 Doris Abra Awudi1†
Doris Abra Awudi1† Anita Nyarkoa Walker1*†
Anita Nyarkoa Walker1*† Mary Makhala Weeto1Christiana Babymay Priddy1
Mary Makhala Weeto1Christiana Babymay Priddy1 Otobong Donald Akan2,3Cynthia Anuseh Baduweh4Bella Abigail Arthur5Salimata Yakubu6Solim Essomandan Clémence Bafei6
Otobong Donald Akan2,3Cynthia Anuseh Baduweh4Bella Abigail Arthur5Salimata Yakubu6Solim Essomandan Clémence Bafei6 Timothy Mobolaji Olagunju6Margaret Zaitoun1Yuxia Zhong1Yucong Feng1Yuandie Zhang1Tao Wei1
Timothy Mobolaji Olagunju6Margaret Zaitoun1Yuxia Zhong1Yucong Feng1Yuandie Zhang1Tao Wei1 Qing Feng1*
Qing Feng1*- 1Department of Nutrition and Food Hygiene, Nanjing Medical University, Nanjing, Jiangsu, China
- 2Microbiology Department, Akwa-Ibom State University, Uyo, Akwa-Ibom State, Nigeria
- 3Food Science and Engineering, Central South University of Forestry and Technology, Hunan, China
- 4School of Public Health, Nanjing Medical University, Nanjing, Jiangsu, China
- 5School of Medicine, Jiangsu University, Zhejiang, Jiangsu, China
- 6Department of Epidemiology and Health Statistics, Nanjing Medical University, Nanjing, Jiangsu, China
Background: The impact of non-communicable diseases (NCDs) is disproportionately felt by immigrants from low- to medium-income countries (LMICs), partly due to their dietary habits. To thrive in their new environment, migrants either omit or consume certain food items, which could lead to nutritional deficits. As a result, most migrants experience more NCDs than their compatriots in their native countries. Therefore, we evaluated the difference in dietary habits, quality, and the influencing factors of overweight or obesity among African migrant students in Nanjing (China) and non-migrant students in Africa using cross-sectional data.
Methods: The researchers used the food frequency questionnaire and the global diet quality score metrics to assess food intake and quality, respectively. Then, cross-tabulation was employed to explore the differences between the groups in meal skipping, eating habits, and diet quality. Finally, the factors associated with overweight or obesity were assessed with binary logistic regression stratified by African students in Nanjing and students in their native countries.
Results: Approximately 678 responses were received, mainly between 18–25 years (46.7%) and 26–36 years (45.4 %). The majority of them (52.3%) were international students. The non-migrant African students' diets lacked citrus fruits (22.2%), deep orange fruits (15.4%), deep orange vegetables (18%), cruciferous vegetables (24.6%), and dark leafy vegetables (26.5%). While the African migrant students consumed more high-fat dairy (50.7%), processed meats (23.9%), sweets and ice creams (51.3%), sugar-sweetened beverages (40.5%), and juice (61.5%), p < 0.001. Furthermore, consuming late-night meals constantly [Exp (B) = 39.607, p = 0.049], eating twice a day [Exp (B) = 6.527, p = 0.036], consuming red meat [Exp (B) = 29.287, p = 0.001], processed meats [Exp (B) = 719.979, p = 0.0011], refined grains and baked foods [Exp (B) = 15.752, p = 0.013], and sweets and ice cream [Exp (B) = 193.633, p = 0.006] were factors inducing overweight or obesity among only African migrant students.
Conclusion: Controlling the what (Western diet and nature of late-night meals) and the when of eating can drastically reduce their influence on obesogenic condition formation in African migrant students in China and elsewhere.
1 Introduction
Migrating from one's country of origin to another might instigate changes in behavior and lifestyle. Food is a critical aspect of cultures; therefore, immigration can drastically change an individual's survival core (1). Interestingly, dietary complications among migrants are mainly the result of changes in diet. A mediating element for the high frequency of nutritional disorders among migrants, besides their low economic situation, is insufficient or lack of knowledge regarding local foods (2, 3). To thrive in their new environment, migrants either omit or consume certain food items, which could lead to nutritional deficits (4). For instance, according to the study by Zhu et al., Chinese international students in South Korea consumed fewer fruits and vegetables, more readymade foods, and mostly missed breakfast (5). However, unhealthy diets and practices such as consuming sugary drinks, fast foods, and fewer fruits and vegetables, skipping meals, particularly breakfast, and binge eating, among others, contribute to weight gain and, as a result, increase the burden of non-communicable diseases (NCDs) globally (6).
Non-communicable diseases, such as overweight or obesity, are prime culprits in a pandemic across the globe. Aside from infectious and chronic diseases being burdensome to people of African origin, with at least 69% of fatalities from infectious diseases, current projections suggest increased death rates from diabetes, cancer, respiratory, and cardiovascular disease-induced NCDs among Africans in the next 10 years (7). Additionally, NCD impacts are disproportionately felt by immigrants from lower-middle-income countries (LMICs) (8). According to a study among African Migrants in Europe, diabetes, obesity, and higher CVD risk are becoming more common among Europe-based Ghanaian migrants compared to their Ghana-based fellow citizens (9, 10). However, observable disparities in diet-induced health issues among immigrant and non-immigrant counterparts in their home countries are not just among Africans. For instance, when consuming foods rich in fats, Chinese living in America also have a greater incidence of long-term illnesses such as excessive weight gain, hypertension, sugar diseases, disease of the heart, and some types of malignancies than Chinese living in China. Suggesting that migration might be a culprit for these health inequalities (11).
The specific nature of food culture for a particular group of people (12) can also account for the dietary problems resulting in NCDs among migrants. For instance, there is a significant difference in the availability of African staple foods such as millet, sorghum, plantains, and cassava, among others, compared to the staples of Asians such as rice and wheat (13). The differences in diet availability pose a severe problem for most African migrants outside of Africa, making them skip meals and consume excessive amounts of fast food. The Pew Research Center has estimated that in 2010, African migrants comprised 80% of all international migrants in other countries, including China (14). However, no study has examined the diet quality of immigrant African students in China and how it affects their weight status. This study's outcome can inform decision-makers and migrant students on how to manage overweight or obesity risks among African students in China.
2 Materials and methods
2.1 Study design, population, and sampling
This study examined the quality of African international students' diets in Nanjing and compared them with those of their compatriot students in their respective African countries. The differences in influencing factors of overweight or obesity across the two groups were also assessed using a cross-sectional study. A purposive and convenient sampling technique was employed to recruit African students in Nanjing, Lesotho, Ghana, and Nigeria. Nanjing is located in the east of China, hosting most international students in Jiangsu province since it is the province's capital and second-largest city. The students from Lesotho attended the National University of Lesotho, situated in the capital of Lesotho. The Ghanaian students were from the University of Cape Coast in Cape Coast, Ghana. Finally, the Nigerian students were from the University of Lagos in Akoka, Nigeria. This study employed an online data collection method for international students in Nanjing and a face-to-face interview for African students in their respective countries. The researchers pretested the questionnaire with ten students from Nanjing Medical University, China; the University of Cape Coast, Ghana; the University of Lagos, Nigeria, and the National University of Lesotho, Lesotho. The final version was then hosted on Wenjuanxing for international students in China and on Google Forms for non-international students.
The study included only international African students in Nanjing who accepted to participate. At the same time, the non-international students comprised only students from the selected schools who decided to participate in the survey. Data collection took place between 1 August and 30 December 2022. We provided no incentive for participation. No personal identification information (confidentiality) was collected. The participants could complete the survey within 10–15 min. All study participants provided their consent before participating by selecting “yes” to continue with the study or “no” to withdraw from the study. The School of Public Health, Nanjing Medical University's research committee reviewed the study protocol. However, the ethics committee of Nanjing Medical University exempted the study from obtaining ethical approval because it did not collect biological samples or receive confidential information. Nevertheless, Helsinki's ethical standards and later amendments were adhered to. Furthermore, the heads of schools and departments of the various universities and colleges of the universities in Africa gave their consent before the researchers collected the data from the different schools.
2.2 Dietary intake assessment
Researchers used a proven semi-quantitative food frequency questionnaire (FFQ) specific to our populations (15–19) to access the food consumption of the respondents – the final tool comprised 100 food items for each country. The frequency of consuming food was estimated as “four to six times per day,” “two to three times per day,” “once every day,” “two to six times per week,” “once every week,” “once to three times per month,” and “never.” Specific portion sizes were added to the questionnaire to ensure that the respondents selected the actual amount they consumed. For each frequency option, we used the following values: never = 0; once to three times per month = 2/30; once every week = 1.5/7; two to six times per week = 4/7; once every day = 1; two to three times per day = 2.5; and four to six times per day = 4. Next, the research team estimated the mass consumed per day by multiplying the corresponding value of the frequency of consuming food items by the standard portion size (20).
2.3 Diet quality assessment
We used the Global Diet Quality Score (GDQS), a food-based dietary quality score, to determine the adequacy of our respondents' dietary intake. This index was developed based on the Prime Diet Quality Score. The GDQS aims to explore dietary quality and investigate how the food we eat relates to long-term diseases across the globe. The GDQS includes 25 food groups: 16 healthy food groups, 2 unhealthy groups when consumed in excess, and 7 unhealthy food groups. The detailed components of the food groups are published elsewhere (21). The scoring of the GDQS is based on the quantity of food consumed daily. Positive scores are given to the healthy 16 food groups, and higher scores denote higher consumption. Next, for the unhealthy food groups, except high-fat dairy and red meat, moderate consumption received a higher score, whereas very low or extremely high intakes received a worse score. A higher score on the GDQS, which ranges from 0 to 49 points, indicates higher dietary quality. The GDQS negative (GDQS–) sub-metric is composed of the addition of the score of the unhealthy food categories and ranges from 0 to 17 points, whereas the GDQS positive (GDQS+) sub-metric is composed of the addition of the score of the healthy food groups and ranges from 0 to 32 points (21).
2.4 Eating habits
This aspect was constructed based on existing literature about practices recognized as healthy or unhealthy eating behaviors. The behaviors examined include fast food consumption, binge eating, late-night meals, healthy meal choices, reading food labels, and consuming soda and alcoholic beverages. The responses to these questions were “never,” “sometimes,” “most of the time,” and “always.” This aspect also consisted of whether they skipped meals, the type of meal skipped, and the number of times they ate in a day.
2.5 Other variables
This component was added to collect information on demographic and anthropometric variables. Age, sex, continent of origin, educational level, present residence, and average monthly expenses were among the demographic variables.
The weight (kg) and height (m) of African students in Nanjing were self-reported. However, using a weighing scale, the data collectors weighed the non-international African students in their home nations while dressed in loose clothing and without shoes. We reported their weight and height to be closest to 0.5 kg (1.1 pounds). Before using any measurement equipment for the first time, they calibrated it to ensure that the collected data was accurate. We then calculated their body mass index (BMI) in kg/m2 by dividing their weight by the square of their height. We followed the recommendations of the National Institute of Health to categorize the BMI. Here, underweight is defined as having a BMI of 18.5 or less. A BMI between 18.5 and 24.9 is considered average weight, and a BMI between 25 and 29.9 is defined as overweight while a BMI of 30 or more is defined as obese (22).
2.6 Statistical analyses
The Statistical Package for Social Sciences was used for the analysis (version 26; SPSS Inc., Chicago, IL). The data were described through frequencies, percentages, means, and standard deviations. Then, cross-tabulation was used to determine how meal skipping, eating habits, and diet quality differed among the students in Nanjing and the students in their native countries. The predisposing factors of overweight or obesity were assessed with binary logistic regression stratified by African students in Nanjing and African students in their native countries, with weight status as the outcome variable and diet quality and eating habits as the explanatory variables. All statistical analyses were conducted with a significance level of p < 0.05 Table 1.
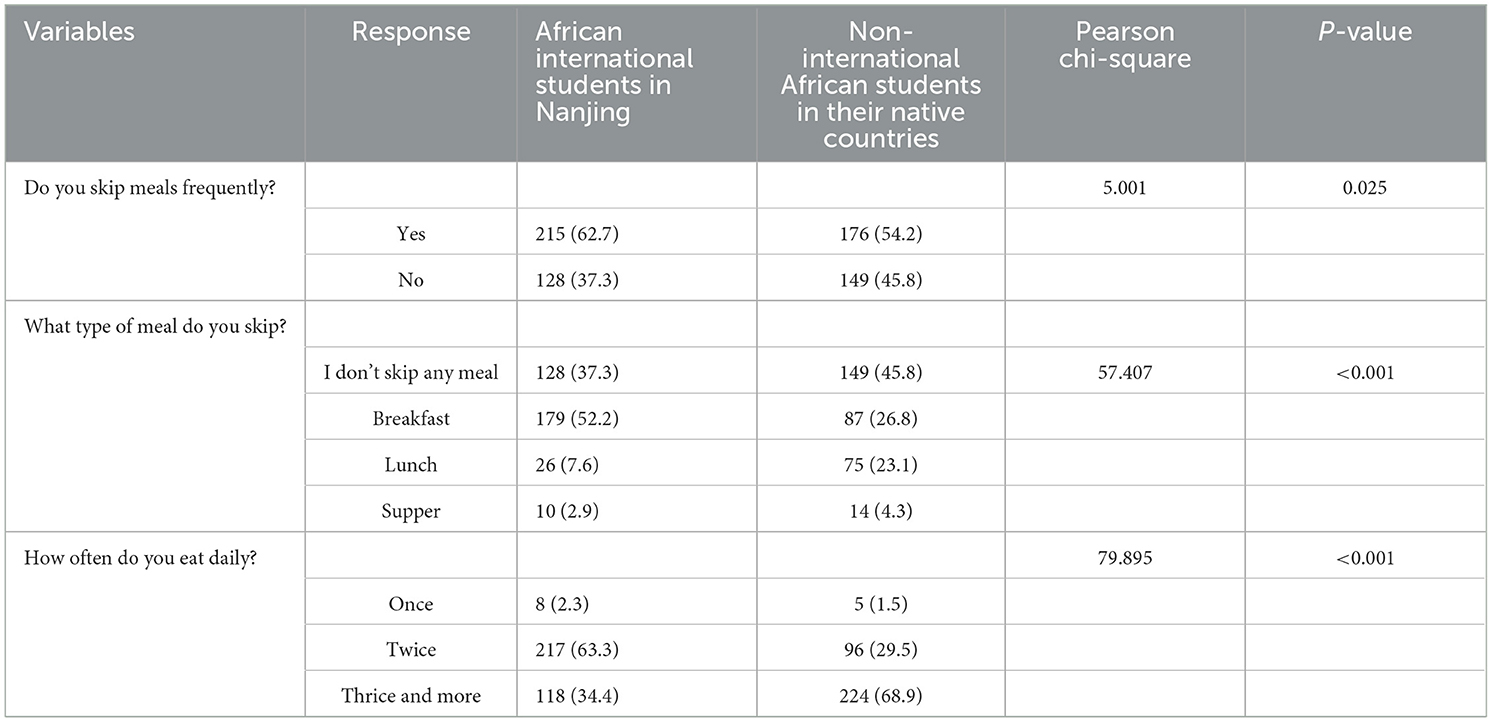
Table 1. How meal-skipping habits vary across African international students in Nanjing and non-international African students in their native countries.
3 Results
We received a total of 678 responses, and 53% were received from women. The bulk of respondents were between the ages of 18 and 25 years (46.7%) and 26 and 36 years (45.4%) and were primarily undergraduates (53.4%). They consisted of African students in Nanjing (52.3%) and African students from Lesotho (29.9%), Nigeria (10.5%) and Ghana (8.2%). Finally, the majority of students were healthy (55.7%), while approximately 38.7% were overweight or obese (Table 2).
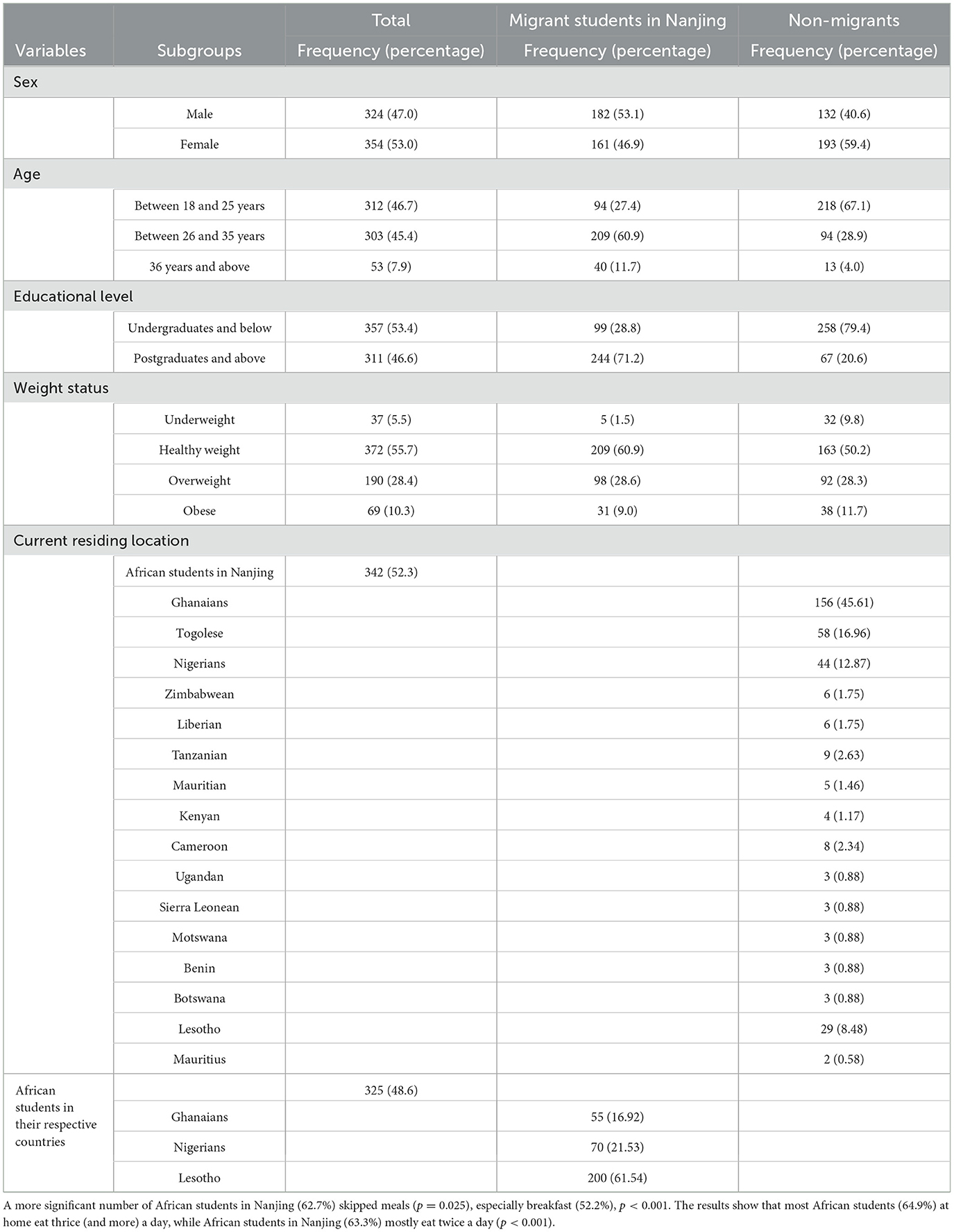
Table 2. The demographic distribution of the students.
The eating habits of African students in Nanjing were found to be less healthy compared to their counterparts in their native countries. The students in Nanjing frequently (93.7%) consumed fast foods such as burgers, pizza, and fries. Additionally, it was found that more international students in Nanjing often consume food during late hours (68.9%) and binge eat (64.5%). However, the late-night meals eaten by a majority of African students in Nanjing were considered healthy (74.5%); they regularly read the food labels of the food they consume (86.3%), This difference was statistically significant (p < 0.001) (Table 3).
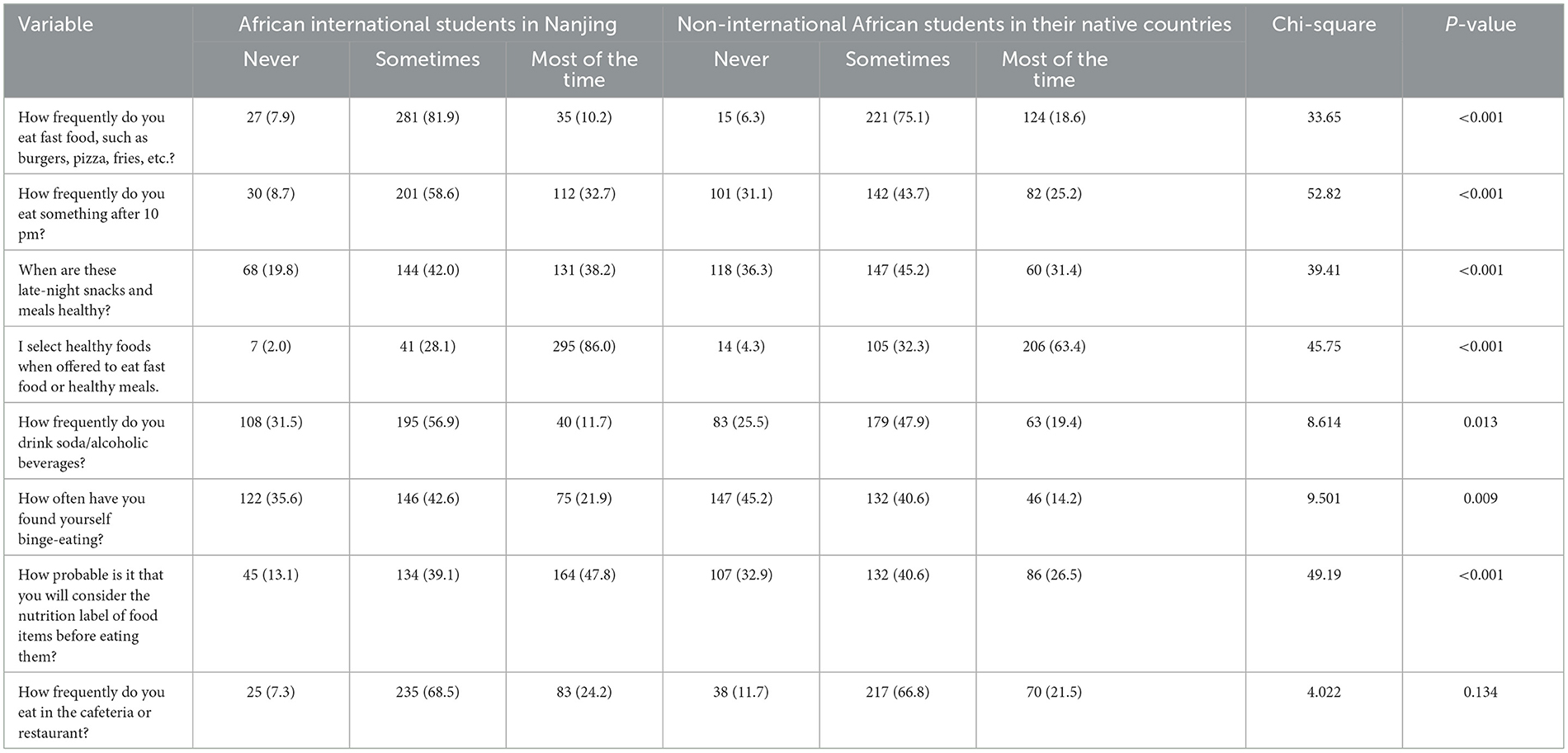
Table 3. How eating habits vary across African international students in Nanjing and non-international African students in their native countries.
For each of the 25 food groups in the GDQS, the average amount consumed is shown in Table 4. The quality of the diet of the students varied significantly across the African students in Nanjing and their counterparts in their respective countries. Here, the diets of African students in their respective countries suffered more from inadequate intake of citrus fruits (22.2%), deep orange fruits (15.4%), deep orange vegetables (18%), cruciferous vegetables (24.6%), and dark leafy vegetables (26.5%). Moreover, the African international students in Nanjing's consumption of legumes (47.8%) and fish and shellfish (44%) were inadequate. On the other hand, they also consumed excessive amounts of high-fat dairy (50.7%), processed meats (23.9%), sweets and ice creams (51.3%), sugar-sweetened beverages (40.5%), and juice (61.5%), and purchased deep fried foods (11.9%), p < 0.001.
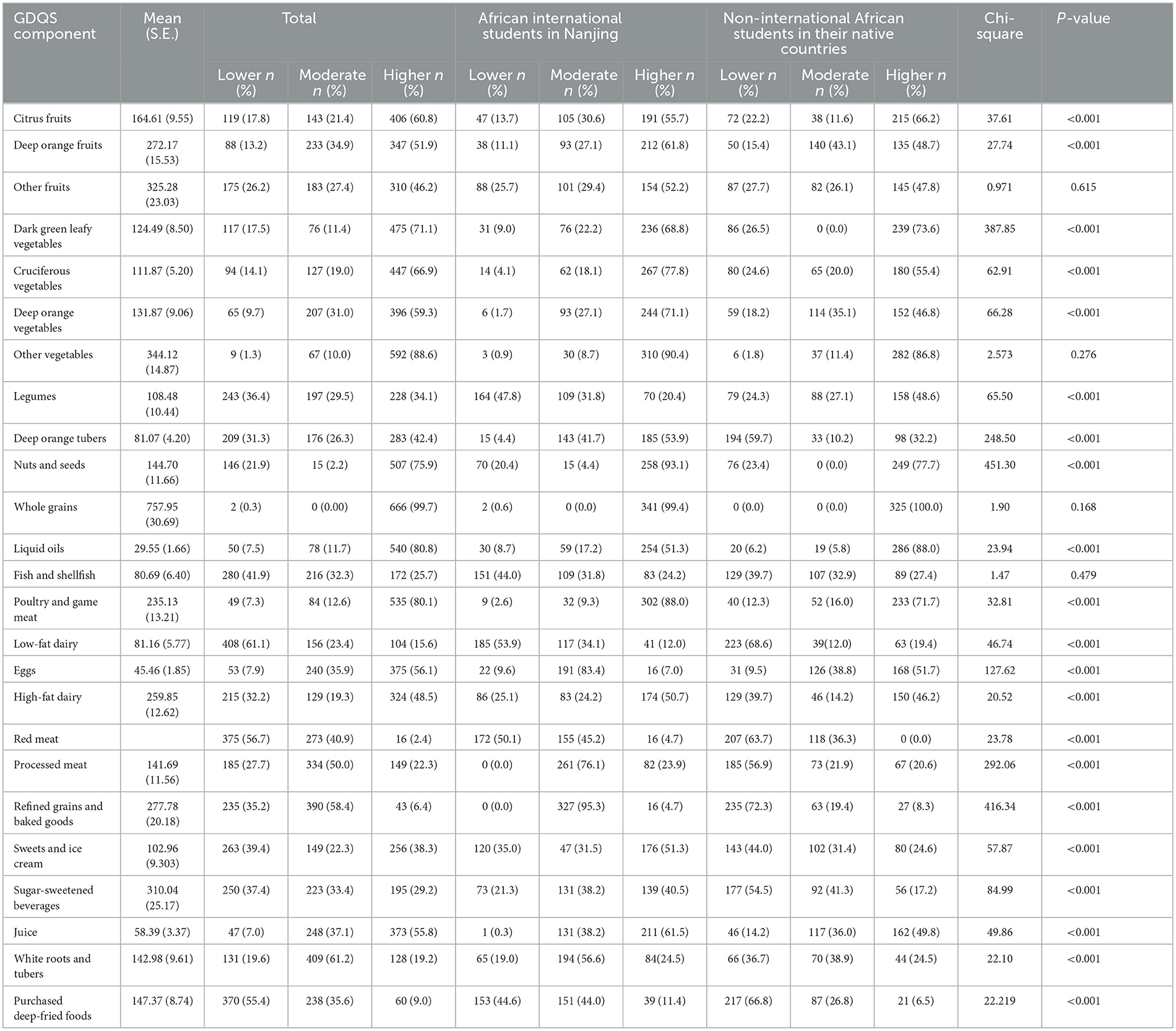
Table 4. The mean consumption for each of the 25 GDQS food groups.
According to Table 5, the predisposing factors of overweight or obesity differed between the two groups. Harmful eating habits such as consuming late-night meals always [Exp (B) = 39.607, p = 0.049], eating twice a day [Exp (B) = 6.527, p = 0.036], consuming red meat [Exp (B) = 29.287, p = 0.001], processed meats [Exp (B) = 719.979, p = 0.0011], refined grains and baked foods [Exp (B) = 15.752, p = 0.013], and sweets and ice cream [Exp (B) = 193.633, p = 0.006] all increased the likelihood of being overweight or obese among African international students in Nanjing compared to African students in their home countries. However, there was a decreased risk of becoming overweight or obese when healthy late-night snacks were consumed always [Exp (B) = 0.082, p = 0.0021], sometimes [Exp (B) = 0.032, p = 0.002], or never [Exp (B) = 0.033, p = 0.008]. Furthermore, avoiding cafeteria and restaurant food [Exp (B) = 0.015, p = 0.001], avoiding binge eating [Exp (B) = 0.002, p = 0.01], avoiding consuming deep-fried foods purchased from a store [Exp (B) = 0.027, p = 0.014], and avoiding consuming sugar-sweetened beverages [Exp (B) = 0.0235, p = 0.0037] all decreased the likelihood of being overweight or obese. Finally, a higher global diet quality score also reduced the chance of being overweight or obese [Exp (B) = 0.010, p = 0.001] among African international students in Nanjing compared to African students in their respective countries.
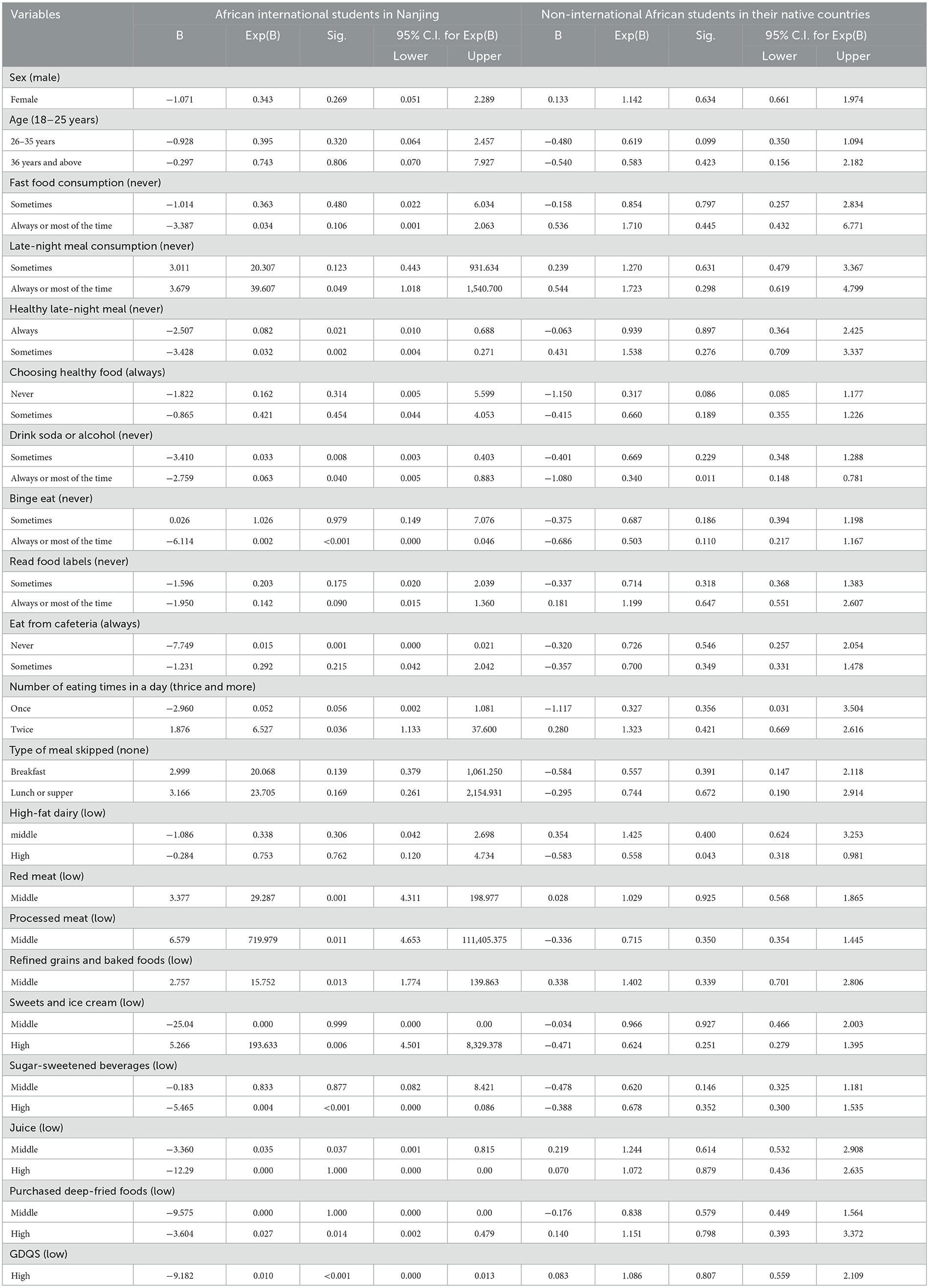
Table 5. The elements that influence our population's chance of being overweight or obese utilizing binary logistic regression.
4 Discussion
This study aimed to investigate whether there was a relationship between the obesity and overweight risk and the dietary quality and eating behaviors of students from a varied population, specifically, African migrant students in Nanjing and African students in their native countries. A cross-sectional study design was utilized in this investigation. The study discovered that African students in Nanjing practice poor eating behaviors more frequently than in their home countries, which affects their risk of being overweight or obese.
Most migrant students, like those in other studies, miss meals, especially breakfast, consume more fast food, and eat at irregular hours (beyond 10:00 pm) (23, 24). The increase level of breakfast skipping can be attributed to the nature of chinese breakfast which is difficult to consume. Students also skip meals due to the stress of studying abroad, especially when learning a new language (25, 26). Notwithstanding, they were always mindful of the food's nutritional information, and their late-night meals were generally healthy. Due to their higher levels of education—the majority of whom were postgraduates and doctoral students as opposed to non-migrant undergraduates—the migrants may exhibit healthier behaviors than their native-born counterparts (27). In addition, the level of nutritional understanding can be increased by extensive nutrition education programs. Developed nations, such as China, continually promote healthy eating habits and encourage their residents to read food labels.
The non-migrant African students' main dietary issue is their lack of fruit and vegetable consumption. Citrus fruits, deep orange vegetables, cruciferous vegetables, and dark green vegetables were among the foods that non-migrants ate less often. Worldwide, reports of young adults who do not eat enough fruit and vegetables are known (28–30). Additionally, as compared to people in other regions with comparable levels of development, Africans spend the most on food, according to data from the African Union Commission (AUC), the United Nations Economic Commission for Africa (UNECA), and the Food and Agriculture Organization (FAO). As a result, they find it challenging to consume nutrient-dense meals due to their higher cost compared to staples such as cereals and starchy roots (31). Despite this, these foods contain several advantages, including dietary fiber, vitamins, minerals, antioxidants, phytoestrogens, and anti-inflammatory agents, essential for a person's overall health and illness prevention (32). Therefore, measures are required to guarantee that most of the population, particularly students, can access these dietary categories.
Furthermore, the migrant students engaged in an excessive amount of Westernized dining. In particular, they bought and consumed a lot of deep-fried items and processed meat, sweets, ice cream, and beverages with added sugar. This trend in meal consumption is similar to that of other migrants, whose main dietary trends after migration included a significant increase in energy and fat intake and a decrease in carbohydrates, along with switching from whole cereals and beans to more refined types of carbohydrates, meat, and dairy products (33). Additionally, the fact that China is more industrialized than the African nations from which the participants came may have contributed to the rise in consumption (34, 35). However, the increase in consumption of this food group among African migrants in China is detrimental to their health and the world as Westernized diets are connected to many ailments, including type 2 diabetes, obesity, cardiovascular disease, high cholesterol, dementia, and attention deficit hyperactivity disorder (ADHD) (36–38). Due to the effects mentioned above, migrant students must be made aware of the need to create a balanced diet free of or low in Western foods to safeguard their health and the environment.
As anticipated, the risk of becoming overweight or obese among the African migrants increased with their increased consumption of red meat, processed meat, refined grains, baked goods, sweets, and ice cream. These foods are high in saturated fats, the primary cause of most non-communicable disorders such as obesity or being overweight, because they increase low-density lipoprotein (LDL-C) levels (39). The intake of such foods and the increased risk for obesity and other diet-related non-communicable diseases are not recent trends among migrants (40–42). The severe impact this diet is having on migrants' health requires immediate action.
Additionally, unhealthy eating patterns, including regularly eating late at night and eating only twice daily, were effective predictors of being overweight or obese. This result is consistent with a recent study, which indicated that having dinner later in the evening increases various factors that can contribute to obesity (43). Furthermore, Brigham and Women's Hospital researchers discovered that eating after midnight decreases calorie expenditure, increases hunger, and alters fat tissue, which might lead to weight gain (44). Eating less frequently is also linked to an irregular eating pattern that may result in weight gain, like an increase in hormones connected to hunger and, eventually, a metabolic disruption that could raise cardiovascular risk (45). Furthermore, the high risk of being overweight or obese among African migrants who eat twice a day can be attributed to breakfast skipping (46). It is vital to remind migrant students that missing meals would reduce the quantity and quality of nutrients they need each day, and eating unhealthy late-night snacks is detrimental to their health.
Interestingly, consistently eating a healthy late-night snack decreased the likelihood of African migrants being overweight or obese. Only the type of diet taken will determine how harmful late-night meals are to health. Research suggests that eating late-night meals rich in protein, fiber, healthy fats, iron, vitamins A, C, E, folate, and probiotics can help prevent weight gain (47). Even though late-night eating has adverse health effects, young people like our participants cannot entirely break the practice. As a result, informing them about healthy late-night snacks to eat is essential. In addition to late-night snacking, people who avoided eating at cafeterias and restaurants were less likely to be obese or overweight. Research shows that dining at restaurants and cafes harms weight loss and BMI (48). This is because restaurant meals tend to be energy-dense, delicious, and frequently paired with sugary drinks. Moreover, these meals are offered at discounted prices, in large portion sizes, and in appealing packaging, all of which encourage the consumption of larger portions (49). Thus, avoiding eating at restaurants or cafeterias is essential to prevent the risk of weight gain.
A higher global diet quality score also decreased the probability of being overweight or obese. A higher GDQS score indicates a better diet, which can help reduce non-communicable nutrition-related diseases (21). According to the GDQS, people are less likely to gain weight when they consume more plant-based foods that are low in processed grains, red and processed meats, and added sugar. Similar to our findings, U.S. women who experienced a rise in the GDQS reduced the risk of obesity and concurrent weight gain (50). Likewise, Mexican women showed a reduced tendency to gain weight and a smaller waist circumference with increased GDQS (51). Therefore, to prevent weight gain among migrant African students in Nanjing that may lead to overweight or obesity, students should be advised to eat meals high in fruits, vegetables, whole grains, and fish and to cut back on refined grains, red and processed meats, added sugar, and carbonated beverages.
This study is the first to compare eating habits, diet quality, and risk factors for overweight or obesity between non-migrant African students in their respective countries and African migrant students in Nanjing (China). It does, however, have several limitations that should be taken into account when evaluating the results. The migrant students in Nanjing self-reported their weight and height, which could lead to recall bias. Nevertheless, previous research has shown that self-reported weight and height are adequate for calculating BMI (52). Second, because this was a cross-sectional study, a causal association between eating habits, the quality of the diet, and overweight or obesity cannot be proven. Additionally, these findings cannot be generalized to all African students or all African migrant students in China because the sample size was restricted to only African students in Nanjing and African students in specific universities from only three African countries. Finally, the sampling technique was convenient but could not represent the entire population.
5 Conclusion
Different nutritional issues affect migrant students in Nanjing compared to their fellow citizens in their home nations. While various fruits and vegetables are absent from the diet of the non-migrants, the Nanjing migrant students tend to engage in more Westernized diets, including deep-fried snacks, sugar-sweetened beverages, processed meat, high-fat dairy, and ice cream, in addition to eating late at night, skipping meals, especially breakfast, and eating once or twice daily. Furthermore, the African migrant students were more likely to be overweight or obese than the non-migrant students due to these unhealthy eating habits, such as eating late at night, eating twice daily, and consuming red meat, processed meats, refined grains, baked goods, sweets, and ice cream. Controlling the what (Western diet and nature of late-night meals) and when of eating can drastically reduce their influence on obesogenic condition formation in African migrant students in China and elsewhere.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The requirement of ethical approval was waived by the Nanjing Medical University, School of Public Health. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
AW: Writing—original draft, Data curation, Methodology, Supervision, Conceptualization, Formal analysis, Project administration, Validation, Investigation, Funding acquisition. MW: Data curation, Investigation, Writing—review & editing. CP: Investigation, Writing—review & editing, Data curation, Software. OA: Investigation, Writing—review & editing. CB: Investigation, Writing—review & editing, Methodology. BA: Investigation, Writing—review & editing, Data curation. SY: Investigation, Methodology, Writing—review & editing. DA: Writing—review & editing, Data curation, Methodology, Project administration, Visualization. SB: Data curation, Investigation, Software, Writing—review & editing. TO: Data curation, Investigation, Writing—review & editing. MZ: Investigation, Validation, Writing—review & editing. YZho: Validation, Visualization, Writing—review & editing. YF: Software, Validation, Writing—review & editing. YZha: Software, Visualization, Writing—review & editing. TW: Validation, Visualization, Writing—review & editing. QF: Conceptualization, Funding acquisition, Project administration, Resources, Supervision, Writing—review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
The authors would like to thank Dr. Eric Ofori and Dr. Kingsley Pereko, University of Cape Coast, Ghana, for supporting with data collection.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Ramírez AS, Golash-Boza T, Unger JB, Baezconde-Garbanati L. Questioning the dietary acculturation paradox: a mixed-methods study of the relationship between food and ethnic identity in a group of Mexican-American women. J Acad Nutr Diet. (2018) 118:431–9. doi: 10.1016/j.jand.2017.10.008
2. Alakaam A, Willyard A. Eating habits and dietary acculturation effects among international college students in the United States. AIMS Public Health. (2020) 7:228–40. doi: 10.3934/publichealth.2020020
3. Edwards JSA, Hartwell HL, Brown L. Changes in food neophobia and dietary habits of international students. J Hum Nutr Dietet. (2010) 23:301–11. doi: 10.1111/j.1365-277X.2010.01066.x
4. Satia-Abouta J, Patterson RE, Neuhouser ML, Elder J. Dietary acculturation: applications to nutrition research and dietetics. J Am Diet Assoc. (2002) 102:1105–18. doi: 10.1016/S0002-8223(02)90247-6
5. Zhu JF. Lifestyle changes and acculturative stress of Chinese international students living in Korea. Chung-Ang University. (2012).
6. Wong SS, Dixon LB, Gilbride JA, Kwan TW, Stein RA. Measures of acculturation are associated with cardiovascular disease risk factors, dietary intake, and physical activity in older Chinese Americans in New York City. J Immigr Minor Health. (2013) 15:560–8. doi: 10.1007/s10903-012-9669-4
7. Kolling M, Winkley K, von Deden M. “For someone who's rich, it's not a problem”. Insights from Tanzania on diabetes health-seeking and medical pluralism among Dar es Salaam's urban poor. Global Health. (2010) 6:8. doi: 10.1186/1744-8603-6-8
8. Agyemang C, Addo J, Bhopal R, de Graft Aikins A, Stronks K. Cardiovascular disease, diabetes and established risk factors among populations of sub-Saharan African descent in Europe: a literature review. Global Health. (2009) 5:7. doi: 10.1186/1744-8603-5-7
9. Agyemang C, Meeks K, Beune E, Owusu-Dabo E, Mockenhaupt FP, Addo J, et al. Obesity and type 2 diabetes in sub-Saharan Africans - Is the burden in today's Africa similar to African migrants in Europe? The RODAM study. BMC Med. (2016) 14:166. doi: 10.1186/s12916-016-0709-0
10. Boateng D, Agyemang C, Beune E, Meeks K, Smeeth L, Schulze M, et al. Migration and cardiovascular disease risk among ghanaian populations in Europe: the RODAM study (research on obesity and diabetes among african migrants). Circulation. (2017) 10:e004013. doi: 10.1161/CIRCOUTCOMES.117.004013
11. Liu S, Fu MR, Hu SHL, Wang VY, Crupi R, Qiu JM, et al. Obesity indicators and chronic illness among Chinese Americans: a pilot study. J Obes Weight Loss Ther. (2015) 5:270.
12. Sibal V. Food: Identity of culture and religion. Wathi. (2020). Available online at: https://www.wathi.org/food-identity-of-culture-and-religion-researchgate/ (accessed July 4, 2023).
13. Food and Agricultural Organization. Food Staples- What do you eat. National Geographic. (2023). Available online at: https://education.nationalgeographic.org/resource/food-staple/ (accessed July 4, 2023).
14. The Pew Research Center. At Least a Million Sub-Saharan Africans Moved to Europe Since 2010. Pew Research Center. (2018). Available online at: https://www.pewresearch.org/global/2018/03/22/at-least-a-million-sub-saharan-africans-moved-to-europe-since-2010/ (accessed July 4, 2023).
15. Abizari A-R, Ali Z. Dietary patterns and associated factors of schooling Ghanaian adolescents. J Health Popul Nutr. (2019) 38:5. doi: 10.1186/s41043-019-0162-8
16. Abubakari A, Jahn A. Maternal dietary patterns and practices and birth weight in northern Ghana. PLoS ONE. (2016) 11:e0162285. doi: 10.1371/journal.pone.0162285
17. Ene-Obong HN, Sanusi RA, Udenta EA, Williams IO, Anigo KM, Chibuzo EC, et al. Data collection and assessment of commonly consumed foods and recipes in six geo-political zones in Nigeria: important for the development of a National Food Composition Database and Dietary Assessment. Food Chem. (2013) 140:539–46. doi: 10.1016/j.foodchem.2013.01.102
18. Lupi S, Bagordo F, Stefanati A, Grassi T, Piccinni L, Bergamini M, et al. Assessment of lifestyle and eating habits among undergraduate students in northern Italy. Annali Dell'Istituto Superiore Di Sanita. (2015) 51:154–61.
19. Sheehy T, Kolahdooz F, Mtshali TL, Khamis T, Sharma S. Development of a quantitative food frequency questionnaire for use among rural South Africans in KwaZulu-Natal. J Hum Nutr Dietet. (2014) 27:443–9. doi: 10.1111/jhn.12166
20. Sauvageot N, Alkerwi A, Albert A, Guillaume M. Use of food frequency questionnaire to assess relationships between dietary habits and cardiovascular risk factors in NESCAV study: validation with biomarkers. Nutr J. (2013) 12:143. doi: 10.1186/1475-2891-12-143
21. Bromage S, Batis C, Bhupathiraju SN, Fawzi WW, Fung TT, Li Y, et al. Development and validation of a novel food-based global diet quality score (GDQS). J Nutr. (2021) 151, 75S−92S. doi: 10.1093/jn/nxab244
22. BMI. Clinical guidelines on the identification, evaluation, and treatment of overweight and obesity in adults–the evidence report. Obesity Res. (1998) 2:6.
23. Gao RR, Kim JH. Changes in dietary life and health-related lifestyle by stress level in Chinese international students in Korea. J Korean Dietet Assoc. (2018) 24:75–91. doi: 10.14373/JKDA.2018.24.1.75
24. Lee J, Gao R-R, Kim J-H. Acculturation and changes in dietary behavior and anthropometric measures among Chinese international students in South Korea. Nutr Res Pract. (2015) 9:304–12. doi: 10.4162/nrp.2015.9.3.304
25. Tseng M, Fang CY. Stress is associated with unfavorable patterns of dietary intake among female Chinese immigrants. Ann Behav Med. (2011) 41:324–32. doi: 10.1007/s12160-010-9259-4
26. Wang J, Kang Y, Lee SY. Stress and dietary behavior by acculturation level among Chinese students living in Korea. J East Asian Soc Diet Life. (2019). doi: 10.17495/easdl.2019.2.29.1.42
27. Finger JD, Tylleskär T, Lampert T, Mensink GBM. Dietary behaviour and socioeconomic position: the role of physical activity patterns. PLoS ONE. (2013) 8:e78390. doi: 10.1371/journal.pone.0078390
28. Conner TS, Thompson LM, Knight RL, Flett JAM, Richardson AC, Brookie KL. The role of personality traits in young adult fruit and vegetable consumption. Front Psychol. (2017) 8:119. doi: 10.3389/fpsyg.2017.00119
29. Mello Rodrigues V, Bray J, Fernandes AC, Luci Bernardo G, Hartwell H, Secchi Martinelli S, et al. Vegetable consumption and factors associated with increased intake among college students: a scoping review of the last 10 years. Nutrients. (2019) 11:1634. doi: 10.3390/nu11071634
30. Nour M, Sui Z, Grech A, Rangan A, McGeechan K, Allman-Farinelli M. The fruit and vegetable intake of young Australian adults: a population perspective. Public Health Nutr. (2017) 20:2499–512. doi: 10.1017/S1368980017001124
31. UNECA and FAO. New report finds fruit, vegetables, protein remain out of reach for most Africans. (2021). Available online at: https://www.uneca.org/stories/new-report presented in the report shows that nearly, essential vitamins and minerals to maintain basic Health.
32. Slavin JL, Lloyd B. Health benefits of fruits and vegetables. Adv Nutr. (2012) 3:506–16. doi: 10.3945/an.112.002154
33. Holmboe-Ottesen G, Wandel M. Changes in dietary habits after migration and consequences for health: a focus on South Asians in Europe. Food Nutr Res. (2012) 56:18891. doi: 10.3402/fnr.v56i0.18891
35. Popkin BM, Adair LS, Ng SW. Global nutrition transition and the pandemic of obesity in developing countries. Nutr Rev. (2012) 70:3–21. doi: 10.1111/j.1753-4887.2011.00456.x
36. Howard AL, Robinson M, Smith GJ, Ambrosini GL, Piek JP, Oddy WH. ADHD is associated with a “Western” dietary pattern in adolescents. J Atten Disord. (2011) 15:403–11. doi: 10.1177/1087054710365990
37. Rakhra V, Galappaththy SL, Bulchandani S, Cabandugama PK. Obesity and the western diet: how we got here. Mo Med. (2020) 117:536–8.
38. Ugai T, Sasamoto N, Lee H-Y, Ando M, Song M, Tamimi RM, et al. Is early-onset cancer an emerging global epidemic? Current evidence and future implications. Nat Rev Clin Oncol. (2022) 19:656–73. doi: 10.1038/s41571-022-00672-8
39. Astrup A, Teicholz N, Magkos F, Bier DM, Brenna JT, King JC, et al. Dietary saturated fats and health: are the U.S. guidelines evidence-based? Nutrients. (2021) 13:3305. doi: 10.3390/nu13103305
40. Agyemang C, Owusu-Dabo E, de Jonge A, Martins D, Ogedegbe G, Stronks K. Overweight and obesity among Ghanaian residents in The Netherlands: how do they weigh against their urban and rural counterparts in Ghana? Public Health Nutr. (2009) 12:909–16. doi: 10.1017/S1368980008003510
41. Mennen LI, Jackson M, Sharma S, Mbanya JCN, Cade J, Walker S, et al. Habitual diet in four populations of African origin: a descriptive paper on nutrient intakes in rural and urban Cameroon, Jamaica and Caribbean migrants in Britain. Public Health Nutr. (2001) 4:765–72. doi: 10.1079/PHN2000117
42. Saleh A, Amanatidis S, Samman S. The effect of migration on dietary intake, type 2 diabetes and obesity: the Ghanaian health and nutrition analysis in Sydney, Australia (Ghanaisa). Ecol Food Nutr. (2002) 41:255–70. doi: 10.1080/0367-020291909778
43. Dashti HS, Gómez-Abellán P, Qian J, Esteban A, Morales E, Scheer FAJL, et al. Late eating is associated with cardiometabolic risk traits, obesogenic behaviors, and impaired weight loss. Am J Clin Nutr. (2021) 113:154–61. doi: 10.1093/ajcn/nqaa264
44. Vujović N, Piron MJ, Qian J, Chellappa SL, Nedeltcheva A, Barr D, et al. Late isocaloric eating increases hunger, decreases energy expenditure, and modifies metabolic pathways in adults with overweight and obesity. Cell Metabol. (2022) 34:1486–1498.e7. doi: 10.1016/j.cmet.2022.09.007
45. Paoli A, Tinsley G, Bianco A, Moro T. The influence of meal frequency and timing on health in humans: the role of fasting. Nutrients. (2019) 11:719. doi: 10.3390/nu11040719
46. Okada C, Imano H, Muraki I, Yamada K, Iso H. The association of having a late dinner or bedtime snack and skipping breakfast with overweight in Japanese women. J Obes. (2019) 2019:2439571. doi: 10.1155/2019/2439571
47. Njike VY, Smith TM, Shuval O, Shuval K, Edshteyn I, Kalantari V, et al. Snack food, satiety, and weight. Adv Nutr. (2016) 7:866–78. doi: 10.3945/an.115.009340
48. León-Muñoz LM, García-Esquinas E, Soler-Vila H, Guallar-Castillón P, Banegas JR, Rodríguez-Artalejo F. Unhealthy eating behaviors and weight gain: a prospective study in young and middle-aged adults. Obesity. (2016) 24:1178–1184. doi: 10.1002/oby.21477
49. Roberts SB, Das SK, Suen VMM, Pihlajamäki J, Kuriyan R, Steiner-Asiedu M, et al. The measured energy content of frequently purchased restaurant meals: multi-country cross-sectional study. BMJ. (2018) 363:k4864. doi: 10.1136/bmj.k4864
50. Fung TT, Li Y, Bromage S, Bhupathiraju SN, Batis C, Fawzi W, et al. Higher global diet quality score is associated with less 4-year weight gain in U.S. women. J Nutr. (2021) 151:162S−167S. doi: 10.1093/jn/nxab170
51. Angulo E, Stern D, Castellanos-Gutiérrez A, Monge A, Lajous M, Bromage S, et al. Changes in the global diet quality score, weight, and waist circumference in Mexican women. J Nutr. (2021) 151:152S−61S. doi: 10.1093/jn/nxab171
Keywords: global diet quality score, overweight or obesity, eating habits, Africans, western diet, China, students, diet quality
Citation: Awudi DA, Walker AN, Weeto MM, Priddy CB, Akan OD, Baduweh CA, Arthur BA, Yakubu S, Bafei SEC, Olagunju TM, Zaitoun M, Zhong Y, Feng Y, Zhang Y, Wei T and Feng Q (2024) Unhealthy diets increase the likelihood of being overweight or obese among African migrant students in China, but not among African non-migrant students: a cross-sectional study. Front. Nutr. 11:1291360. doi: 10.3389/fnut.2024.1291360
Received: 09 September 2023; Accepted: 12 February 2024;
Published: 15 March 2024.
Edited by:
Georgina Gómez, University of Costa Rica, Costa RicaReviewed by:
Diana Nur Afifah, Diponegoro University, IndonesiaMojca Korošec, University of Ljubljana, Slovenia
Copyright © 2024 Awudi, Walker, Weeto, Priddy, Akan, Baduweh, Arthur, Yakubu, Bafei, Olagunju, Zaitoun, Zhong, Feng, Zhang, Wei and Feng. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Anita Nyarkoa Walker, d2Fsa2VyYW5pdGEzMEBnbWFpbC5jb20=; Qing Feng, cWluZ2ZlbmdAbmptdS5lZHUuY24=
†These authors share first authorship