 Saeedeh Hosseini Hooshiar1
Saeedeh Hosseini Hooshiar1 Sadegh Jafarnejad
Sadegh Jafarnejad
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CLINICAL TRIAL article
Front. Nutr. , 10 January 2024
Sec. Nutrition and Metabolism
Volume 10 - 2023 | https://doi.org/10.3389/fnut.2023.1298831
Background: Premenstrual syndrome disorder (PMS) is a condition that affects health-related quality of life (HRQoL) and encompasses a variety of symptoms, including psychological, physical, and behavioral symptoms. Some evidence suggests that an increase in body mass index (BMI) can reduce both HRQoL and menstrual quality. This is because the body fat tissue can affect menstrual cycles by changing the estrogen/progesterone ratio. This study investigated the impact of two diets alternate-day modified fasting (ADMF) and daily calorie restriction (DCR) – on PMS syndrome and HRQoL.
Methods: The study was a randomized controlled, open-label trial that lasted for 8 weeks and involved 60 obese/overweight women. Participants were recruited from the Health Service Centers of Kashan University of Medical Sciences using simple random sampling. The study compared the impact of the ADMF and DCR diets on HRQoL and PMS symptoms. Patients were classified based on their BMI and age and then allocated to either the intervention (ADMF) or control (DCR) group using a random numbers table. The study measured HRQoL, PMS severity, weight, BMI, body fat mass, waist circumference, fat-free mass, and skeletal muscle mass before and after the study. The study had an almost 18% dropout rate.
Results: Significant improvements were observed in mood lability (p = 0.044) and expressed anger (p < 0.001) in relation to PMS symptoms. However, no significant differences were detected in the changes of other COPE subscales. The ADMF diet had a significant impact on the 12-item Short-Form Health Survey (SF-12) total score (p < 0.001) and physical function subscales (p = 0.006) as well as mental health (p < 0.001) when compared to the control diet. This implies that the ADMF diet increased both SF-12 total score and its subscales. The intervention led to improvements in HRQoL, physical function, and mental health. Additionally, significant improvements in BMI and weight were observed between the two groups pre- and post-study (p < 0.001). Anthropometric data, including body fat mass and waist circumference, showed a significant improvement (p < 0.001 and p = 0.029, respectively) before and after the study. However, there were no significant changes in fat-free mass (p = 0.936) and skeletal muscle mass (p = 0.841) between the two groups.
Conclusion: The study suggested that ADMF can improve HRQoL, mood lability, and expressed anger. It also showed that ADMF can reduce waist circumference, weight, and body fat mass in obese/overweight women.
Clinical trial registration: The Iranian Registry of Clinical Trials (IRCT20220522054958N1).
PMS is a common health issue among women of childbearing age, which greatly affects their quality (1). This disorder not only impacts women’s psychological health and social relationships but also reduces their work performance due to its physical and behavioral symptoms (2). PMS typically occurs during the luteal phase of the menstrual cycle (3). The prevalence of this disorder is 47.8% worldwide (4), while in Iran, it ranges from 33 to 48% (5). Women with PMS may experience various symptoms, including behavioral, emotional, and physical signs such as depression, isolation, irritability, and bloating (6). While the exact causes of PMS are still unclear, various factors are known to contribute to this condition (7). Age, family history, taking contraceptive pills, smoking, stress, BMI, exercise, and dietary habits are some of the factors that can lead to menstrual problems (8). Therefore, different strategies have been suggested to manage PMS, such as medications, specific supplements, dietary recommendations, psychological methods, and exercise. Research is ongoing to find more effective and safer treatments (9).
Dietary interventions can be safe and effective strategies for managing PMS (10). Research suggests that menstrual disorders are linked to obesity (11). In a study by Ju et al. (12), it was found that overweight/obese and underweight women suffer from menstrual disorders more than normal-weight women. High levels of prostaglandins have been associated with menstrual problems (13), and the levels of body fat can impact the menstrual cycle and normal ovulation, potentially leading to menstrual disorders (14). Obesity can also alter the function of neurotransmitters that affect progesterone and estrogen hormones (15). Studies have shown that every unit of increased BMI increases the risk of PMS by 3% (16). It is possible that abnormal menstruation and irregular ovulation can affect the estrogen/progesterone ratio, leading to an increase in prostaglandins and thus menstrual disorders (17).
Additionally, changes in the levels of progesterone and estrogen during the menstrual cycle may affect brain chemicals such as serotonin, which can influence mood (18). Research has also linked obesity and overweight to reduced quality of life in various populations (19). Quality of life refers to a subjective sense of overall wellbeing and satisfaction with life. HRQoL (health-related quality of life) is a tool that can help assess the functional impact of diseases and has high acceptability (20). Studies have found that the most common problems experienced by young women are related to menstruation (21).
Calorie restriction has been suggested as the primary treatment for overweight or obese individuals (22). However, patients have low adherence to common calorie restriction diets as they need to be followed daily (23). Intermittent fasting diets have been proposed as an alternative weight loss method and have been shown to improve metabolic health (24). Among various intermittent fasting methods, alternate-day modified fasting (ADMF) has been shown to reduce body weight by 3–7% in 2–3 months (25). However, it is unclear how the ADMF or calorie restriction diets affect body composition and anthropometric indices (22). Trepanowski et al. (22, 26) found that intermittent fasting can improve waist circumference more than usual calorie restriction diets but can decrease weight similarly to common diets. Some studies suggest that intermittent fasting diets decrease visceral fat and preserve muscle mass compared to daily calorie restriction diets (27). Other evidence shows that both intermittent fasting and daily calorie restriction diets increase muscle mass and do not change visceral fat tissue (22). Hutchison et al. (28) reported that intermittent fasting leads to higher decreases in body weight and fat tissue than common calorie restriction diets over 2 months. Some trials propose that attempting to lose weight increases the risk of menstrual disorders (29). Other evidence shows that menstrual disorders increase in women with a normal BMI who enter the BMI category of 25 or higher (12).
In a study by Anton et al. (30), it was found that a fasting diet not only led to significant improvements in HRQoL but also resulted in a small yet significant weight loss among participants. Another study by Etemadifar et al. (31) revealed that Ramadan fasting had a positive impact on the HRQoL of multiple sclerosis patients. Interestingly, the fasting diet was observed to enhance the quality of life independently of weight loss (32). Moreover, a few studies have emphasized that a fasting diet is safe and feasible and can boost the quality of life (33). However, Nugraha et al. (34) presented contradictory findings as their research showed that a Ramadan fasting diet did not affect HRQoL as compared to the control. Hence, due to the inconsistencies in the published results and the limitations of the studies conducted in this field, it is crucial to conduct further research to arrive at more conclusive findings. The primary objective of this trial was to evaluate the impact of the two diets, DCR and ADMF, on HRQoL and the severity of PMS. The findings of this trial can potentially be utilized to enhance dietary recommendations.
This is a randomized, controlled, open-label trial. Participants were selected from the health centers of Kashan University of Medical Sciences considering the inclusion and exclusion criteria using a simple random sampling method. The inclusion criteria were women aged between 18 and 50 years, with a BMI equal to or greater than 25 and less than 40, menstrual bleeding lasting between 3 and 8 days, and normal menstrual cycles of 21–35 days. The participants also had PMS based on PSST (premenstrual symptoms screening tool) and agreed to comply with the study methods. The exclusion criteria included chronic disorders such as heart disease, diabetes, hypertension, digestive problems such as gastritis, peptic ulcer, and duodenal ulcer, breastfeeding, pregnancy, alcohol abuse, smoking habit, weight loss of more than 1 to 2 kg in the last month, nutritional supplements to lose weight, adherence to a special diet, and medication use in the last 2 months. Mental or psychiatric disorders such as depression, clinically diagnosed diseases such as infectious cancer, kidney, CVD, liver, neurological, endocrine, and gynecological diseases were also the exclusion criteria. In addition, having surgery in the last 6 months, enduring extreme stress during the trial, taking antidepressants and contraceptives, taking B6 supplements in the past 3 months, and not completing the questionnaire for 3 successive days and 5 non-successive days were other exclusion criteria.
The flow diagram for the study is presented in Figure 1. A total of 60 eligible participants were sorted based on their BMI and age and then randomly assigned to either the “ADMF” (intervention) or “DCR” (control) groups after initial investigations at the start of the study. A statistician created the allocation sequences with a table of random numbers (35). Participants were assessed based on the eligibility criteria by a trained nutritionist and a medical doctor, who then included them in the trial. The trial protocol was explained by the nutritionist, who also obtained informed written consent and maintained contact with the patients via phone at their workplaces or homes throughout the trial.
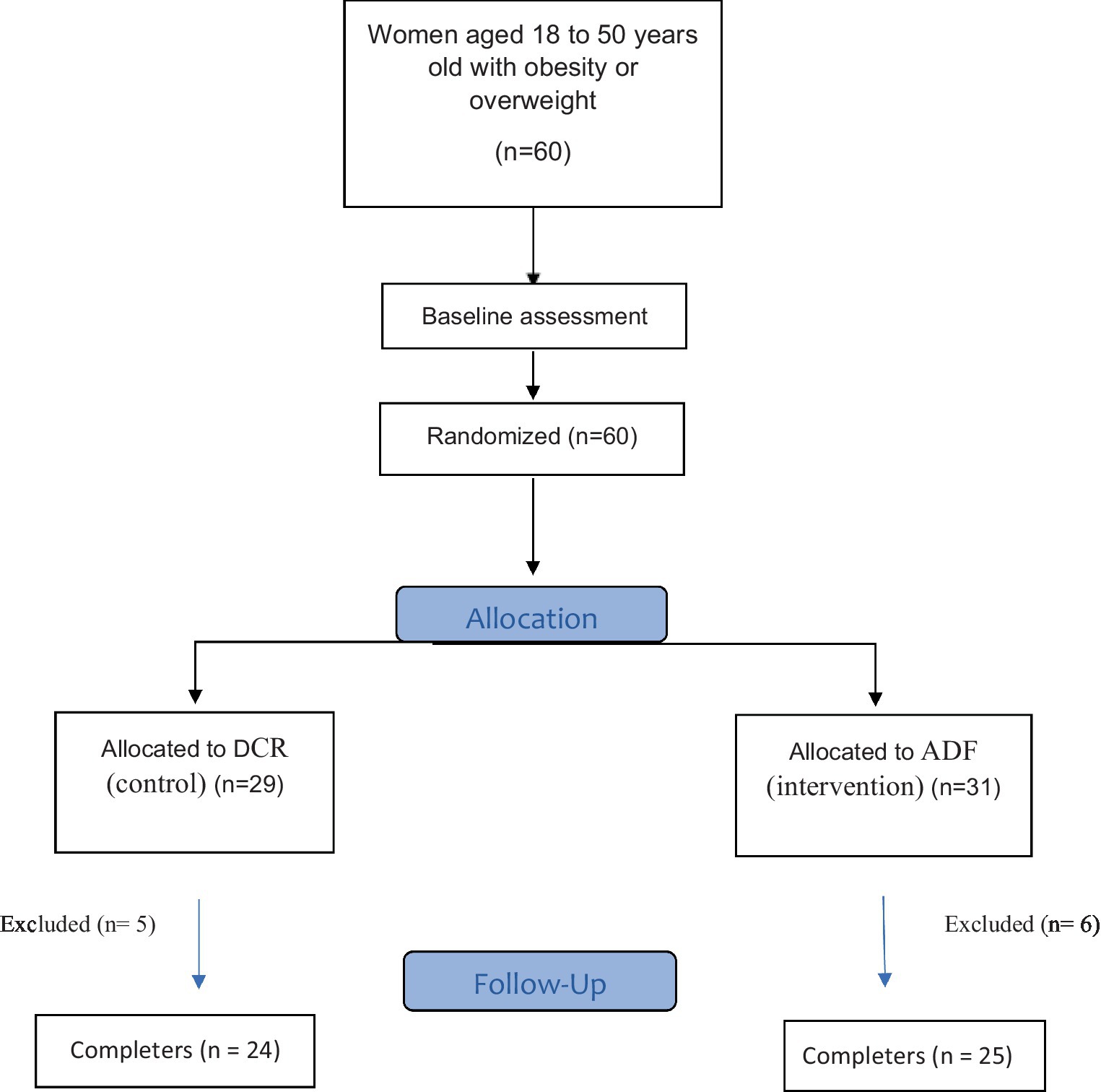
Figure 1. Flow chart of the intervention.
All participants followed their prescribed diet for 8 weeks according to the group they were in and their energy requirements. The energy needs of patients were evaluated using the Mifflin equation (36). A professional dietician provided dietary counseling to patients. Individuals in the control and fasting groups were required to maintain their usual physical activity during the 8-week study period. Participants completed the food record questionnaire 3 days a week (2 days during the week and 1 day off) once every 2 weeks to ensure adherence to the prescribed diet (37). They were asked to complete food records during the week, one fast day, and one feast day. The food record was completed on a day off, whether it was a fast day or a feast day. All participants were taught how to fill in the questionnaires and select appropriate days to complete the questionnaires correctly. Using the home scale guide, the results of the forms were converted to grams and calculated by N4 software (The first Databank Inc.; Hearst Corporation) for Iranian foods. Then, the intake of macronutrients and calories was determined. Participants were considered adherent when the total macronutrients and calorie consumption were between 80 and 110% of the recommended amounts (38). The study researchers regularly made phone calls to participants to encourage them to adhere to their diets. The Ethics Committee of Kashan University of Medical Sciences approved this trial with the ethics code IR.KAUMS.MEDNT.REC.1401.003 and the Iranian Registry of Clinical Trials with the registration code IRCT20220522054958N1. No special side effects were observed during the study.
The ADMF diet consisted of alternating periods of feasting and fasting, starting at midnight every day. During fasting days, participants had a 75% calorie restriction, consuming only a quarter of their daily energy needs between 12:00 PM and 2:00 PM. They were allowed to drink water and other calorie-free drinks, with a daily limit of 400 mg of caffeine. On feasting days, participants consumed their entire daily calorie requirement. The diet was followed for 8 weeks, with a prescribed daily intake of 15% protein, 30% fat, and 55% carbohydrates. Participants were required to maintain their daily routine activities, and all had the same number of contacts with the dietician. The food was prepared at home by the individuals.
During the study, a group of individuals (DCR) were allocated 63% of their daily calorie requirements as the control group. The participants were required to follow their prescribed diet for 8 weeks and cook all their meals at home. The macronutrient composition of the diet was 15% protein, 30% fat, and 55% carbohydrates. The participants were asked to maintain their regular physical activity routine, and all patients had the same number of contacts with the dietician.
To diagnose PMS, the PSST questionnaire was used (39). The questionnaire has 19 items and consists of two sections. The first section has 14 questions related to physical, behavioral, and psychological symptoms, while the second section evaluates the impact of these symptoms on patients’ lives. This section has five components. Patients were asked to report their symptoms during 5 days before their menstruation (40). Symptoms were rated on a scale of 1 to 4 (1: no symptoms and 4: severe symptoms).
To diagnose PMS, the following criteria were used: (I) a score of 3 or more in at least one of the four items related to feeling irritable, depressed, tearful, or tense; (II) a score of 3 or more in at least one of the five items related to interference with work performance, communication with friends and family, household tasks, or social life; (III) a score of 3 or more in at least four out of the first 14 items. Patients who did not meet these criteria were not included in the research (40).
The study required women with PMS to record their symptoms daily for 3 months using the COPE assessment tool (41). The tool assesses 22 premenstrual symptoms, including 10 somatic and 12 behavioral symptoms, throughout the menstrual cycle (41, 42). Participants were required to rate the severity of their symptoms on a 0–3 point Likert scale (3: severe symptoms, 2: moderate symptoms, 1: mild symptoms, and 0: no symptoms) (43). At the end of each month, the scores for each symptom were totaled, and the PMS severity was determined. Scores less than 30% indicated mild PMS severity, scores between 30 and 50% indicated moderate severity, scores between 50 and 60% indicated severe severity, and scores over 60% indicated very severe PMS severity (44). Participants were required to complete this form for 3 months, i.e., 1 month before starting the study and 2 months during the study.
The Short Form Health Survey is a widely used public questionnaire that is applied globally (45). The SF-12 is a shorter version of the SF-36 questionnaire and consists of only 12 items (46, 47). Each item is scored on a 6-point Likert scale, with higher scores indicating better HRQoL (47, 48). To calculate the subscales of physical and mental health, the scores of certain items were added together. For the mental health subscale, scores of the social functioning, vitality, role restrictions due to emotional problems, and perceived mental health items were added together. For the physical health subscale, scores of physical functioning, bodily pain, role restrictions due to physical problems, and general health items were added together (49).
The study measured the physical activity scale both before and after the experiment. To quantify the physical activity, the physical activity scale questionnaire based on MET (metabolic equivalents) was used which includes nine different levels (rest and sleep with a MET value of 0.9 to intense activity with a MET value greater than 6) (50). The physical activity scale quantifies the average daily amount of physical activity undertaken by individuals.
Participants’ weight was evaluated by the Seca scale which had an accuracy of 0.1 kg, without shoes and wearing light clothes. Their height was measured with a stadiometer that had an accuracy of 0.5 cm, while standing barefoot. Body mass index (BMI) was measured accurately by dividing the participant’s weight (in kg) by the participant’s height squared (in meters). Waist circumference was measured, during exhaling, between the iliac crest and the lowest rib, during normal expiration, with an inelastic tape (51). Other anthropometric data, such as fat-free mass, skeletal muscle mass, waist-to-hip ratio, and body fat mass were calculated using InBody 770 (bioelectrical impedance analysis; InBody Co.). All anthropometric data were collected both before and after the trial.
To assess whether the data distribution is normal, we employed the Kolmogorov–Smirnov test. We used the chi-square test for qualitative data and the independent t-test for quantitative data to compare between groups (intervention and control). For comparing the within-group mean of quantitative variables, we used the paired t-test in normal conditions and the Wilcoxon test in non-normal conditions at the beginning and end of the trial. We used the Mann–Whitney test in non-normal conditions and the t-test in normal conditions to evaluate the mean changes between groups. We analyzed the data using the SPSS software (IBM, version 22) and expressed statistically significant results as a value of p of <0.05.
The flow diagram of this study can be seen in Figure 1. Initially, 60 women were randomly assigned to either the ADMF or calorie restriction groups. During the trial, six participants from the fasting group were excluded due to not adhering to the diet (n = 3), pregnancy (n = 1), and illness (n = 2). Similarly, five women from the control group were excluded due to not adhering to the diet (n = 4) and illness (n = 1). Eventually, 49 women finished the trial and were included in the final analysis. The demographic characteristics of the participants were displayed in Table 1, and no significant difference was observed between the two groups in terms of baseline characteristics, BMI (p = 0.535), age (p = 0.876), and physical activity (p = 0.106). Moreover, there were no significant changes in physical activity at the beginning and end of the study within the intervention (p = 0.353) and control (p = 0.601) groups (Table 1).
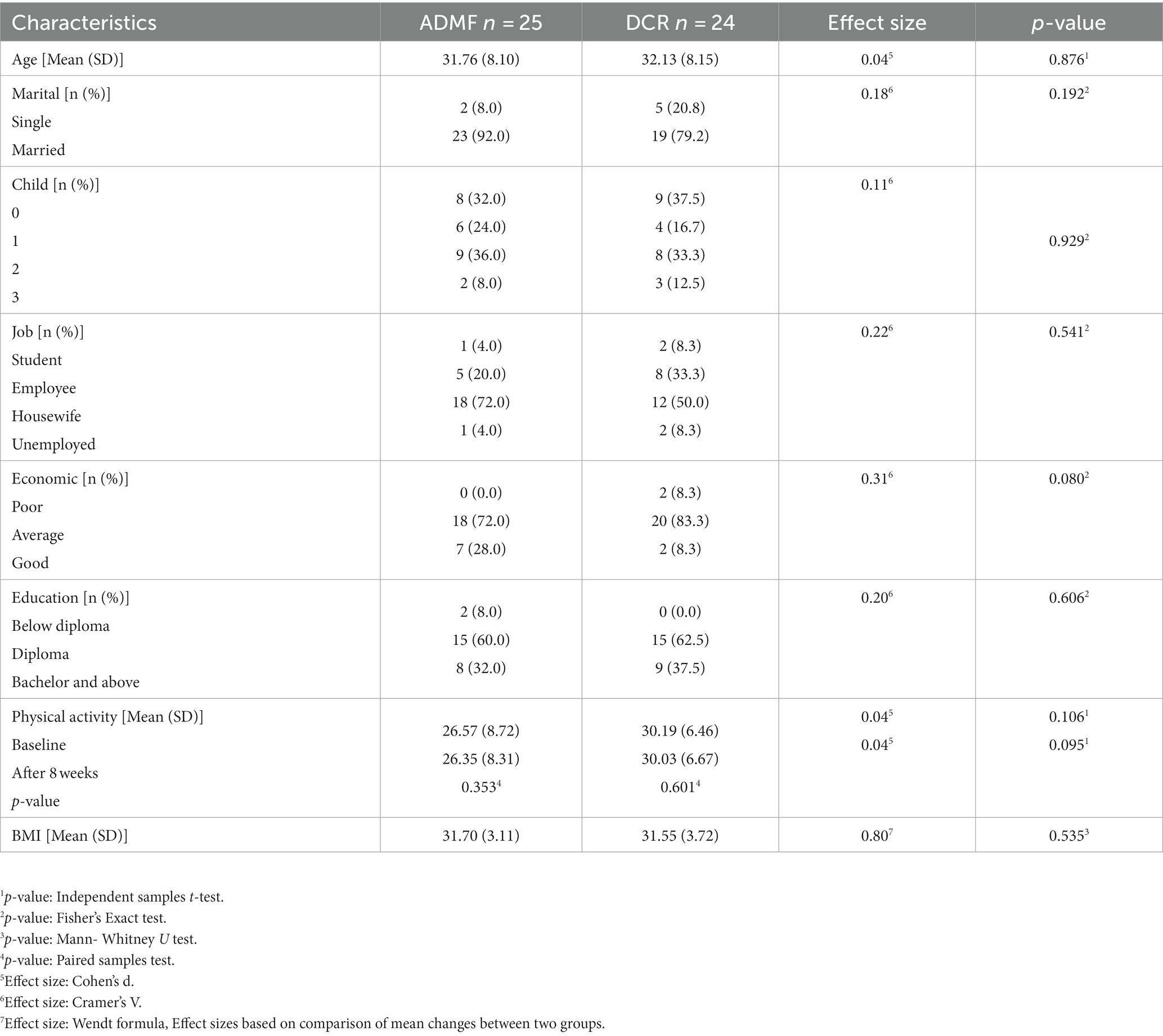
Table 1. General characteristics of study participants.
In the ADMF group, a statistically significant decrease in mood lability was observed (p = 0.002) before and after the study. Additionally, there was a significant difference in the change in mood lability between the two groups (p = 0.044). The fasting group showed a significant change in expressed anger (p < 0.001) compared to the control group. However, there were no significant differences in the changes of other COPE subscales, such as oversensitivity, irritability, anxiety, crying easily, isolation, depression, dizziness, heart palpitation, nausea, poor concentration, forgetfulness, hot flash, headache, fatigue, increased appetite, food craving, acne, breast tenderness, swelling, and bloating, before and after the research between the control and intervention groups (Table 2).
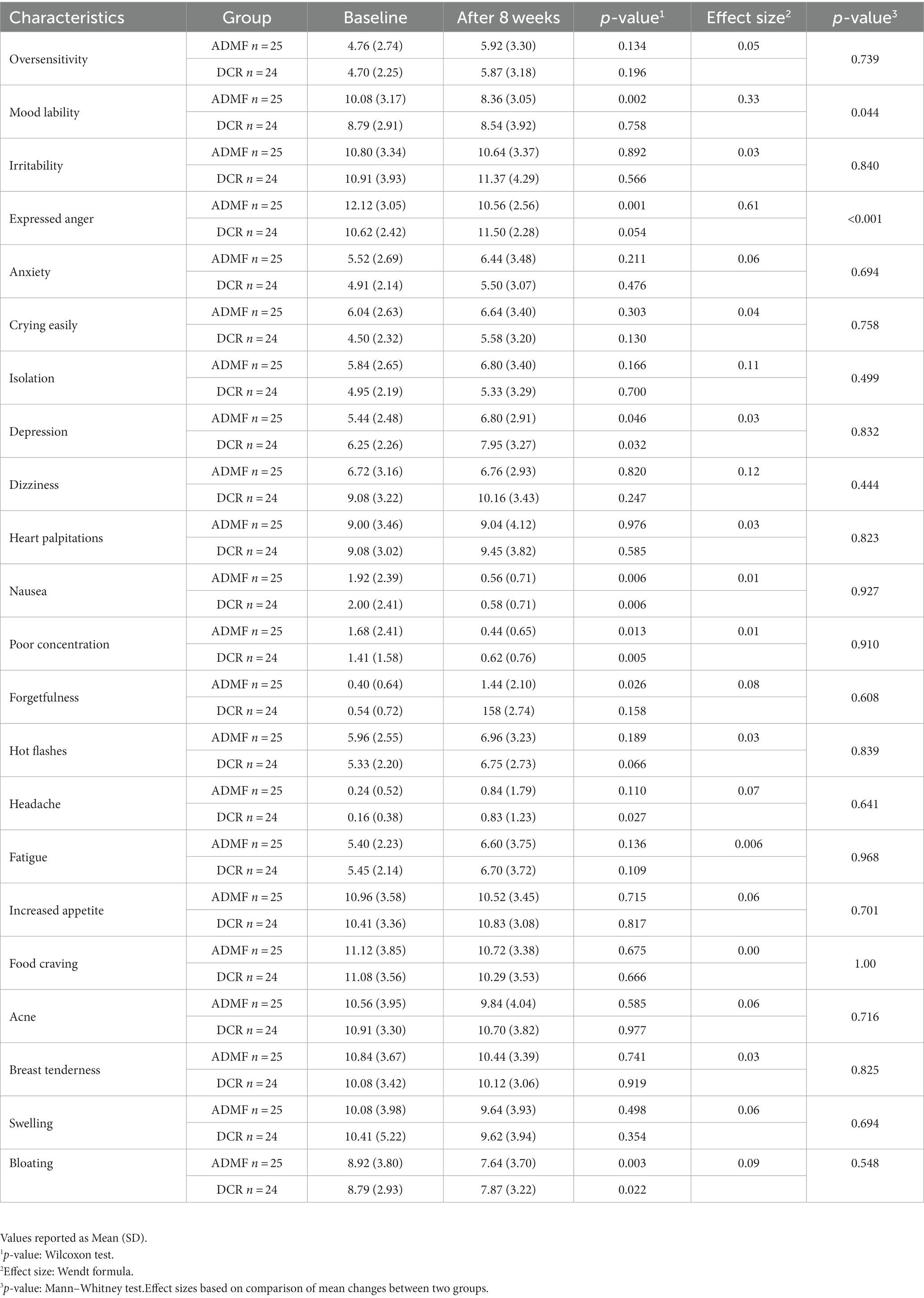
Table 2. The COPE subscales, before and after the study.
Table 3 displays the SF-12 changes before and after the study. The ADMF resulted in significant improvements in the SF-12 total score (p < 0.001) as well as the physical function (p = 0.006) and mental health (p < 0.001) subscales compared to the control diet. This means that the intervention led to improved HRQoL, physical function, and mental health. Moreover, the percentage change in physical function, mental health, and SF-12 total score was higher in the intervention group than in the control group. The HRQoL questionnaire includes a specific subscale that focuses on participants’ physical health, specifically referring to illness and injury experienced in the past 30 days. Although Table 1 indicates similar levels of physical activity between the intervention and control groups, the divergent results observed in HRQoL and its subscales imply that the intervention group exhibited enhancements in both physical and mental wellbeing.
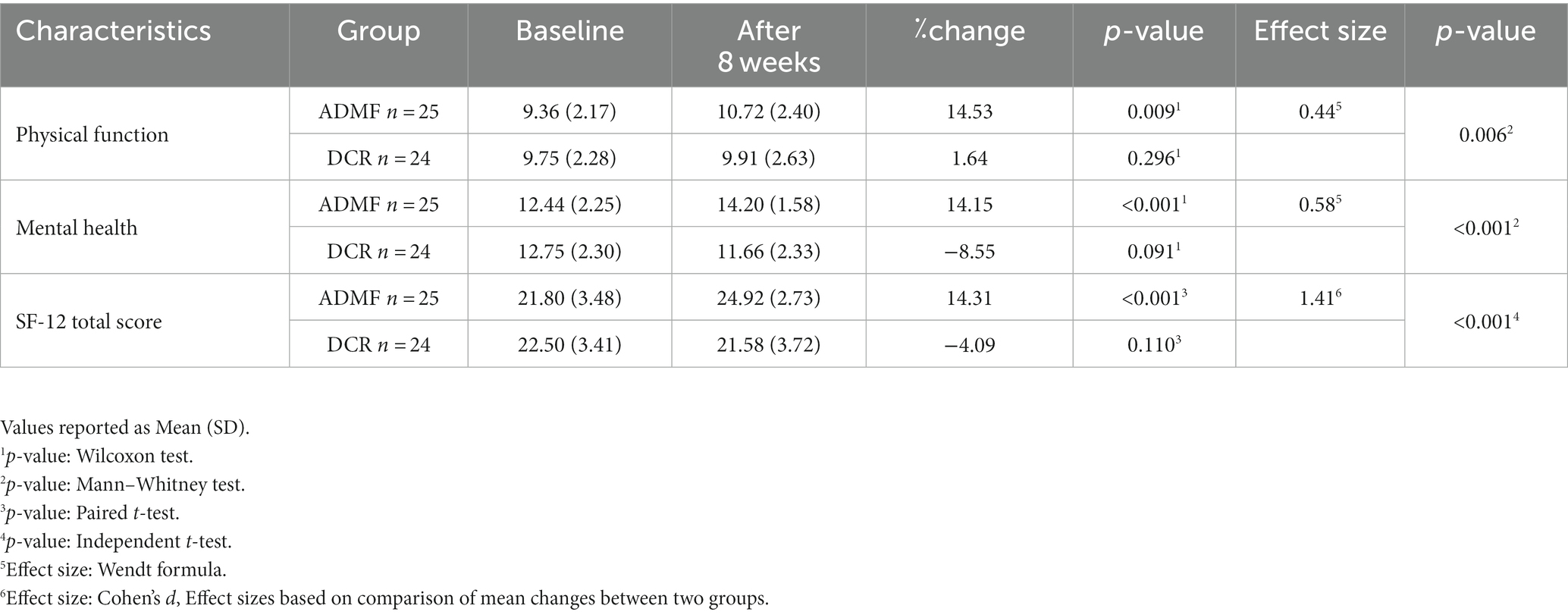
Table 3. The SF-12, physical function, and mental health before and after the study.
At the end of an 8-week intervention, the body weight and BMI of both control and intervention groups showed a significant decrease before and after the study (p < 0.001 and p < 0.001, respectively). Furthermore, the BMI and weight changes between the two groups were significant both before and after the study (p < 0.001). The intervention group had a higher percentage change in body weight compared to the control group (−6.68% vs. −3.72%). However, there were no significant changes in fat-free mass (p = 0.936) and skeletal muscle mass (p = 0.841) between the two groups. Other anthropometric data, including BFM (p < 0.001) and waist circumference (p = 0.029), showed significant differences at the beginning and end of the study between the two groups. Additionally, the percentage change of BFM and WC was higher in the fasting group than the control group (Table 4).
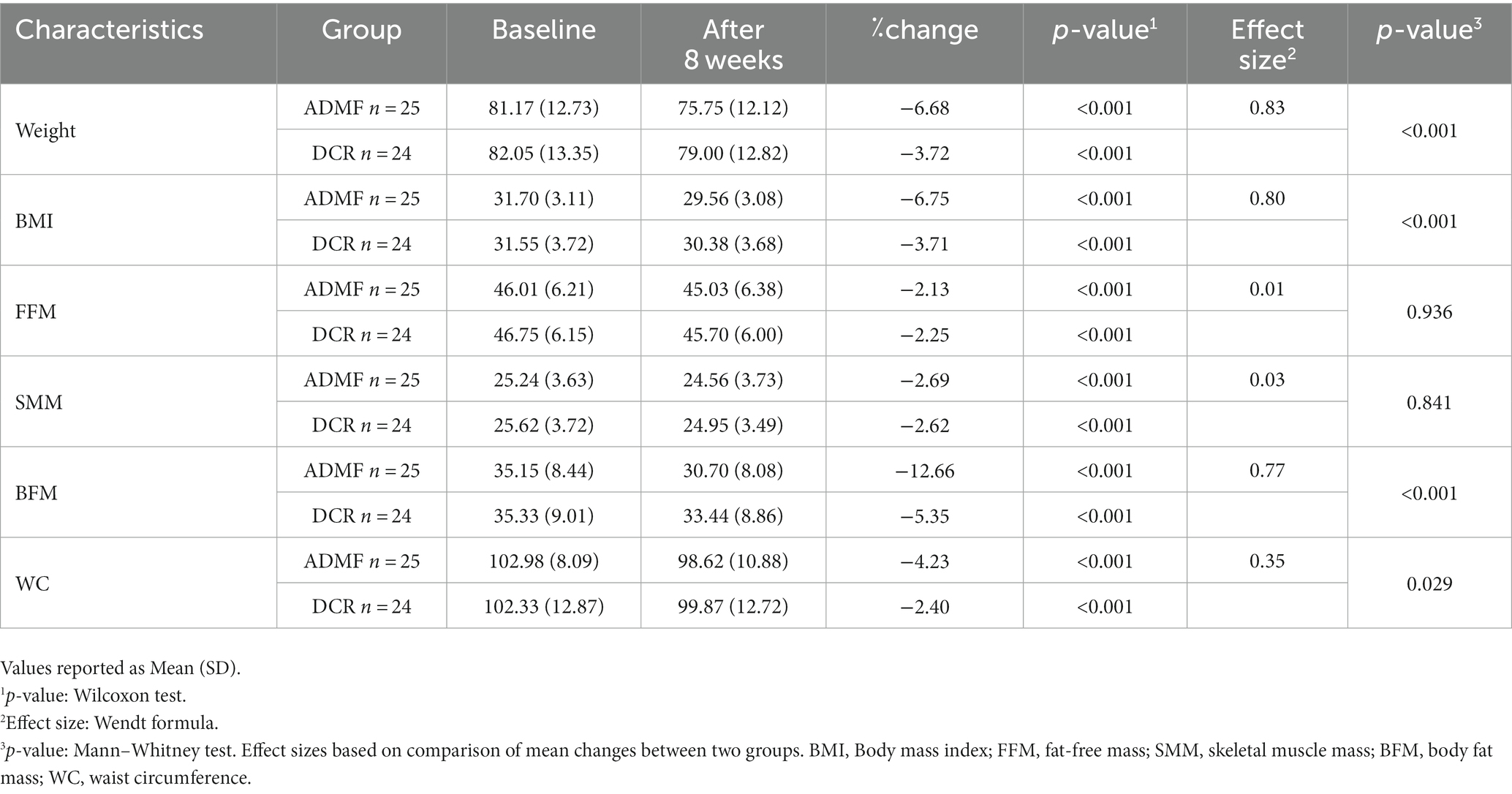
Table 4. The anthropometric indices, at baseline and after the 8-week.
Our trial has shown that following an ADMF diet for 8 weeks can lead to significant improvements in mood lability and reduced expression of anger. Mood swings can be caused by hormonal fluctuations of progesterone and estrogen, which in turn affect the levels of serotonin, dopamine, and γ-aminobutyric acid. These hormones can also impact the renin-angiotensin system. The periodic effect of progesterone and estrogen is also mentioned as the cause of some PMS symptoms such as bloating, weight gain, and swelling (52). However, studies have shown that levels of progesterone and estrogen do not have a significant change between women with PMS and healthy women (53). Therefore, it is unknown why some women suffer from PMS while others do not. Several studies have suggested that women with PMS have greater sensitivity to hormonal differences within the menstrual cycle (54). If post-menopausal patients who previously suffered from PMS are treated with progesterone, the PMS symptoms will recur in them (54).
Studies have shown that obesity affects the levels of progesterone and estrogen hormones by altering the function of neurotransmitters that regulate them (15). In an 8-week study, an ADMF diet was found to be effective in improving weight, BMI, BFM, and WC. These results were consistent with the findings of another study by Bhutani et al., which showed that ADMF reduced fat mass and weight more than DCR (25). Although both ADMF and DCR resulted in weight loss after 8 weeks, the fasting diet was more effective in reducing BMI and weight than the control. These results were consistent with the results of previous studies, such as Razavi et al. (55) and Johnson et al. (56). Participants in ADMF groups have been found to be more compliant with their prescribed diet compared to those on DCR (57). In traditional diets, food consumption is restricted every day, (58) whereas in ADMF diets, calorie intake is restricted every other day, which leads to greater adherence to the diet (57). This adherence to fasting diets leads to more weight loss compared to traditional diets. In the fasting diet, a significant part of decreased weight is associated with the reduction of fat tissue, while fat-free mass is commonly retained (59). Since participants in ADMF diets have a fast for 3–4 days a week, greater weight loss is often seen compared to the control (60). During fasting hours, the body uses ketones and fat as the primary sources of energy, leading to a reduction in fat tissue and body weight (61, 62). People on fasting diets have reported a decrease in appetite during fasting. The change in appetite may be due to the change in appetite-regulating hormones, such as an increase in adiponectin levels and a decrease in leptin and resistin levels, as seen in animal experiments (63).
Our study found that following the ADMF diet resulted in a significant improvement in the SF-12 total score, as well as the physical function and mental health subscales, when compared to the control diet. Previous studies assessing HRQoL using the SF-12 in various populations have suggested that PMS symptoms can have an impact on HRQoL, including mental and physical subscales (64). In our study, the HRQoL and subscale scores of the ADMF group were better than those of the CRD group, which was likely due to the fasting group’s improved physical and mental health. This result was consistent with previous findings that have reported an increase in quality of life and a decrease in fatigue in gynecological cancer patients (65) as well as other studies indicating that intermittent fasting resulted in an improvement in quality of life and physical and mental fatigue in healthy individuals (66).
One of the limitations of our trial was that the assessment of premenstrual syndrome and quality of life was based on self-reported forms, which could cause inaccuracies. Additionally, this study did not investigate the long-term outcomes of the ADMF diet. Our study had a notable limitation; in that, we performed a per-protocol analysis. As a result, we recommend that future studies also consider alternative analyses, such as intention-to-treat analysis, to enhance the robustness of the findings. By doing so, a more comprehensive understanding of the research outcomes can be achieved. To assess adherence to the recommended diet, we utilized food record forms. It is important to note that collecting food records for only 3 days a week may not provide a comprehensive representation of participants’ dietary intake for the entire week. However, this approach was deliberately chosen to minimize the burden on participants and ensure compliance with the study protocol. Additionally, we conducted regular phone interviews with patients throughout the trial period as an additional measure of control and to enhance data accuracy. Furthermore, this was the first research to assess the effect of an ADMF diet on PMS symptoms. This trial assessed an extensive range of health outcomes, including PMS severity, multiple anthropometric indices, and health-related quality of life measures.
Weight loss is a promising method for controlling PMS, and ADMF has been proposed as an effective diet for weight loss and improving metabolic status. Our study found that ADMF is a safe diet for weight loss and BMI management in overweight and obese women. It could also improve HRQoL, mood lability, and expressed anger. However, further studies are needed to establish causality and generalize the findings to other populations.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by Ethics Committee of Kashan University of Medical Sciences. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
SH: Data curation, Methodology, Writing – original draft. AY: Data curation, Formal analysis, Methodology, Software, Validation, Writing – review & editing. SJ: Conceptualization, Investigation, Methodology, Project administration, Supervision, Validation, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was funded by the Kashan University of Medical Sciences funded this trial.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Steiner, M , and Born, L . Diagnosis and treatment of premenstrual dysphoric disorder: an update. Int Clin Psychopharmacol. (2000) 15 Suppl 3:S5–S17. doi: 10.1016/S0140-6736(00)02749-5
2. Maharaj, S , and Trevino, K . A comprehensive review of treatment options for premenstrual syndrome and premenstrual dysphoric disorder. J Psychiatr Pract. (2015) 21:334–50. doi: 10.1097/PRA.0000000000000099
3. Singh, B , Berman, B , Simpson, R , and Annechild, A . Incidence of premenstrual syndrome and remedy usage: a national probability sample study. Altern Ther Health Med. (1998) 4:75–9.
4. Direkvand-Moghadam, A , Sayehmiri, K , Delpisheh, A , and Kaikhavandi, S . Epidemiology of premenstrual syndrome (PMS)-a systematic review and meta-analysis study. J Clin Diagn Res. (2014) 8:106. doi: 10.7860/JCDR/2014/8024.4021
5. Maleki, F , Pourshahbaz, A , Asadi, A , and Yoosefi, A . The impact of premenstrual disorders on health-related quality of life (HRQOL). practice in clinical psychology. (2014) 2:77–84.
6. Halbreich, U , O’Brien, P , Eriksson, E , Bäckström, T , Yonkers, KA , and Freeman, EW . Are there differential symptom profiles that improve in response to different pharmacological treatments of premenstrual syndrome/premenstrual dysphoric disorder? CNS Drugs. (2006) 20:523–47. doi: 10.2165/00023210-200620070-00001
7. Nworie, KM , Aluh, DO , and Onyekwum, CA . Assessment of premenstrual syndrome among female students in Southeast Nigeria. J Obstetr Gynecol Investig. (2018) 1:55–61. doi: 10.5114/jogi.2018.79426
8. Rafique, N , and Al-Sheikh, MH . Prevalence of menstrual problems and their association with psychological stress in young female students studying health sciences. Saudi Med J. (2018) 39:67–73. doi: 10.15537/smj.2018.1.21438
9. Freeman, EW . Therapeutic management of premenstrual syndrome. Expert Opin Pharmacother. (2010) 11:2879–89. doi: 10.1517/14656566.2010.509344
10. Kia, AS , Amani, R , and Cheraghian, B . The association between the risk of premenstrual syndrome and vitamin D, calcium, and magnesium status among university students: a case control study. Health Promot Perspect. (2015) 5:225–30. doi: 10.15171/hpp.2015.027
11. Snehalata, T , and Mahesh, M . Relationship between body mass composition and primary dysmenorrhea. Indian J Physiother Occup Ther. (2016) 10:76–81. doi: 10.5958/0973-5674.2016.00017.4
12. Ju, H , Jones, M , and Mishra, GD . A U-shaped relationship between body mass index and dysmenorrhea: a longitudinal study. PLoS One. (2015) 10:e0134187. doi: 10.1371/journal.pone.0134187
13. Chan, W , Dawood, MY , and Fuchs, F . Prostaglandins in primary dysmenorrhea: comparison of prophylactic and nonprophylactic treatment with ibuprofen and use of oral contraceptives. Am J Med. (1981) 70:535–41. doi: 10.1016/0002-9343(81)90576-3
14. Frisch, RE . 1 the right weight: body fat, menarche and ovulation. Baillieres Clin Obstet Gynaecol. (1990) 4:419–39. doi: 10.1016/S0950-3552(05)80302-5
15. Sutariya, S , Talsania, N , Shah, C , and Patel, M . An interventional study (calcium supplementation & health education) on premenstrual syndrome-effect on premenstrual and menstrual symptoms. Nat J Commun Med. (2011) 2:100–4.
16. Masho, SW , Adera, T , and South-Paul, J . Obesity as a risk factor for premenstrual syndrome. J Psychosom Obstet Gynecol. (2005) 26:33–9. doi: 10.1080/01443610400023049
17. Zahradnik, H , and Breckwoldt, M . Contribution to the pathogenesis of dysmenorrhea. Arch Gynecol. (1984) 236:99–108. doi: 10.1007/BF02134006
18. Jahanfar, S , Lye, M-S , and Krishnarajah, IS . The heritability of premenstrual syndrome. Twin Res Hum Genet. (2011) 14:433–6. doi: 10.1375/twin.14.5.433
19. Kolotkin, RL , and Andersen, JR . A systematic review of reviews: exploring the relationship between obesity, weight loss and health-related quality of life. Clin Obes. (2017) 7:273–89. doi: 10.1111/cob.12203
20. Sahin, S , Ozdemir, K , and Unsal, A . Evaluation of premenstrual syndrome and quality of life in university students. J Pak Med Assoc. (2014) 64:915–22.
21. Taşçı, K . Evaluation of nursing students’ premenstrual symptoms. TAF Preven Med Bull. (2006) 5:434–43.
22. Trepanowski, JF , Kroeger, CM , Barnosky, A , Klempel, M , Bhutani, S , Hoddy, KK, et al. Effects of alternate-day fasting or daily calorie restriction on body composition, fat distribution, and circulating adipokines: secondary analysis of a randomized controlled trial. Clin Nutr. (2018) 37:1871–8. doi: 10.1016/j.clnu.2017.11.018
23. Moreira, EAM , Most, M , Howard, J , and Ravussin, E . Dietary adherence to long-term controlled feeding in a calorie-restriction study in overweight men and women. Nutr Clin Pract. (2011) 26:309–15. doi: 10.1177/0884533611405992
24. Hoddy, KK , Marlatt, KL , Çetinkaya, H , and Ravussin, E . Intermittent fasting and metabolic health: from religious fast to time-restricted feeding. Obesity. (2020) 28:S29–37. doi: 10.1002/oby.22829
25. Bhutani, S , Klempel, MC , Kroeger, CM , Trepanowski, JF , and Varady, KA . Alternate day fasting and endurance exercise combine to reduce body weight and favorably alter plasma lipids in obese humans. Obesity. (2013) 21:1370–9. doi: 10.1002/oby.20353
26. Trepanowski, J , Kroeger, C , Klempel, M , Calvo, Y , and Varady, K . Alternateday fasting versus daily calorie restriction for weight loss and cardio-protection (120.6). FASEB J. (2014) 28:120.6. doi: 10.1096/fasebj.28.1_supplement.120.6
27. Gotthardt, JD , Verpeut, JL , Yeomans, BL , Yang, JA , Yasrebi, A , Roepke, TA, et al. Intermittent fasting promotes fat loss with lean mass retention, increased hypothalamic norepinephrine content, and increased neuropeptide Y gene expression in diet-induced obese male mice. Endocrinology. (2016) 157:679–91. doi: 10.1210/en.2015-1622
28. Hutchison, AT , Liu, B , Wood, RE , Vincent, AD , Thompson, CH , O’Callaghan, NJ, et al. Effects of intermittent versus continuous energy intakes on insulin sensitivity and metabolic risk in women with overweight. Obesity. (2019) 27:50–8. doi: 10.1002/oby.22345
29. Hailemeskel, S , Demissie, A , and Assefa, N . Primary dysmenorrhea magnitude, associated risk factors, and its effect on academic performance: evidence from female university students in Ethiopia. Int J Women's Health. (2016) 8:489–96. doi: 10.2147/IJWH.S112768
30. Anton, SD , Lee, SA , Donahoo, WT , McLaren, C , Manini, T , Leeuwenburgh, C, et al. The effects of time restricted feeding on overweight, older adults: a pilot study. Nutrients. (2019) 11:1500. doi: 10.3390/nu11071500
31. Etemadifar, M , Sayahi, F , Alroughani, R , Toghianifar, N , Akbari, M , and Nasr, Z . Effects of prolonged fasting on fatigue and quality of life in patients with multiple sclerosis. Neurol Sci. (2016) 37:929–33. doi: 10.1007/s10072-016-2518-9
32. Kesztyüs, D , Fuchs, M , Cermak, P , and Kesztyüs, T . Associations of time-restricted eating with health-related quality of life and sleep in adults: a secondary analysis of two pre-post pilot studies. BMC Nutr. (2020) 6:76–8. doi: 10.1186/s40795-020-00402-2
33. Choi, IY , Piccio, L , Childress, P , Bollman, B , Ghosh, A , Brandhorst, S, et al. A diet mimicking fasting promotes regeneration and reduces autoimmunity and multiple sclerosis symptoms. Cell Rep. (2016) 15:2136–46. doi: 10.1016/j.celrep.2016.05.009
34. Nugraha, B , Ghashang, SK , Hamdan, I , and Gutenbrunner, C . Effect of Ramadan fasting on fatigue, mood, sleepiness, and health-related quality of life of healthy young men in summer time in Germany: a prospective controlled study. Appetite. (2017) 111:38–45. doi: 10.1016/j.appet.2016.12.030
35. Wilcox, S , Sharpe, PA , Parra-Medina, D , Granner, M , and Hutto, B . A randomized trial of a diet and exercise intervention for overweight and obese women from economically disadvantaged neighborhoods: sisters taking action for real success (STARS). Contemp Clin Trials. (2011) 32:931–45. doi: 10.1016/j.cct.2011.08.003
36. Mifflin, MD , St Jeor, ST , Hill, LA , Scott, BJ , Daugherty, SA , and Koh, YO . A new predictive equation for resting energy expenditure in healthy individuals. Am J Clin Nutr. (1990) 51:241–7. doi: 10.1093/ajcn/51.2.241
37. Parvaresh, A , Razavi, R , Abbasi, B , Yaghoobloo, K , Hassanzadeh, A , Mohammadifard, N, et al. Modified alternate-day fasting vs. calorie restriction in the treatment of patients with metabolic syndrome: a randomized clinical trial. Complement Ther Med. (2019) 47:102187. doi: 10.1016/j.ctim.2019.08.021
38. Razo-Olvera, D , Mabel, F , Martin-Vences, AJ , Brito-Córdova, GX , Elías-López, D , Landa-Anell, MV, et al. Primary barriers of adherence to a structured nutritional intervention in patients with dyslipidemia. Nutrients. (2021) 13:1744. doi: 10.3390/nu13061744
39. Steiner, M , Macdougall, M , and Brown, E . The premenstrual symptoms screening tool (PSST) for clinicians. Arch Womens Ment Health. (2003) 6:203–9. doi: 10.1007/s00737-003-0018-4
40. del Mar Fernández, M , Regueira-Méndez, C , and Takkouche, B . Psychological factors and premenstrual syndrome: a Spanish case-control study. PLoS One. (2019) 14:e0212557. doi: 10.1371/journal.pone.0212557
41. Mortola, J , Girton, L , Beck, L , and Yen, S . Diagnosis of premenstrual syndrome by a simple, prospective, and reliable instrument: the calendar of premenstrual experiences. Obstet Gynecol. (1990) 76:302–7.
42. Mortola, J , Girton, L , and Fischer, U . Successful treatment of severe premenstrual syndrome by combined use of gonadotropin-releasing hormone agonist and estrogen/progestin. J Clin Endocrinol Metabol. (1991) 72:252–252F. doi: 10.1210/jcem-72-2-252
43. Feuerstein, M , and Shaw, WS . Measurement properties of the calendar of premenstrual experience in patients with premenstrual syndrome. J Reprod Med. (2002) 47:279–89.
44. Khajehei, M , Abdali, K , Parsanezhad, ME , and Tabatabaee, HR . Effect of treatment with dydrogesterone or calcium plus vitamin D on the severity of premenstrual syndrome. Int J Gynecol Obstet. (2009) 105:158–61. doi: 10.1016/j.ijgo.2009.01.016
45. Bullinger, M . German translation and psychometric testing of the SF-36 health survey: preliminary results from the IQOLA project. Soc Sci Med. (1995) 41:1359–66. doi: 10.1016/0277-9536(95)00115-N
46. Ware, JE Jr, Kosinski, M , and Keller, SD . A 12-item short-form health survey: construction of scales and preliminary tests of reliability and validity. Med Care. (1996) 34:220–33. doi: 10.1097/00005650-199603000-00003
47. Ware, J , Kosinski, M , and Keller, S . SF-36 physical and mental health summary scales: a user’s manual. Boston, MA: Health Assessment Lab (1994).
48. Lim, LL , Seubsman, S-a , and Sleigh, A . Thai SF-36 health survey: tests of data quality, scaling assumptions, reliability and validity in healthy men and women. Health Qual Life Outcomes. (2008) 6:52–9. doi: 10.1186/1477-7525-6-52
49. Montazeri, A , Vahdaninia, M , Mousavi, SJ , and Omidvari, S . The Iranian version of 12-item short form health survey (SF-12): factor structure, internal consistency and construct validity. BMC Public Health. (2009) 9:1–10. doi: 10.1186/1471-2458-9-341
50. Aadahl, M , and Jørgensen, T . Validation of a new self-report instrument for measuring physical activity. Med Sci Sports Exerc. (2003) 35:1196–202. doi: 10.1249/01.MSS.0000074446.02192.14
51. World Health Organization . Waist circumference and waist-hip ratio: report of a WHO expert consultation. Geneva: World Health Organization (2011).
52. Davis, C , Sloan, M , and Tang, C . Premenstrual distress among Caucasian, African-American and Chinese women. J Women’s Health Care. (2014) 3:181. doi: 10.4172/2167-0420.1000181
53. Potter, J , Bouyer, J , Trussell, J , and Moreau, C . Premenstrual syndrome prevalence and fluctuation over time: results from a French population-based survey. J Women's Health. (2009) 18:31–9. doi: 10.1089/jwh.2008.0932
54. Dennerstein, L , Lehert, P , and Heinemann, K . Global study of women's experiences of premenstrual symptoms and their effects on daily life. Menopause Int. (2011) 17:88–95. doi: 10.1258/mi.2011.011027
55. Razavi, R , Parvaresh, A , Abbasi, B , Yaghoobloo, K , Hassanzadeh, A , Mohammadifard, N, et al. The alternate-day fasting diet is a more effective approach than a calorie restriction diet on weight loss and HS-CRP levels. Int J Vitam Nutr Res. (2021) 91:242–50. doi: 10.1024/0300-9831/a000623
56. Johnson, JB , Summer, W , Cutler, RG , Martin, B , Hyun, D-H , Dixit, VD, et al. Alternate day calorie restriction improves clinical findings and reduces markers of oxidative stress and inflammation in overweight adults with moderate asthma. Free Radic Biol Med. (2007) 42:665–74. doi: 10.1016/j.freeradbiomed.2006.12.005
57. Varady, KA , and Hellerstein, MK . Alternate-day fasting and chronic disease prevention: a review of human and animal trials. Am J Clin Nutr. (2007) 86:7–13. doi: 10.1093/ajcn/86.1.7
58. Malik, VS , and Hu, FB . Popular weight-loss diets: from evidence to practice. Nat Clin Pract Cardiovasc Med. (2007) 4:34–41. doi: 10.1038/ncpcardio0726
59. Alhamdan, B , Garcia-Alvarez, A , Alzahrnai, A , Karanxha, J , Stretchberry, D , Contrera, K, et al. Alternate-day versus daily energy restriction diets: which is more effective for weight loss? A systematic review and meta-analysis. Obes Sci Pract. (2016) 2:293–302. doi: 10.1002/osp4.52
60. Barnosky, AR , Hoddy, KK , Unterman, TG , and Varady, KA . Intermittent fasting vs daily calorie restriction for type 2 diabetes prevention: a review of human findings. Transl Res. (2014) 164:302–11. doi: 10.1016/j.trsl.2014.05.013
61. El Ati, J , Beji, C , and Danguir, J . Increased fat oxidation during Ramadan fasting in healthy women: an adaptative mechanism for body-weight maintenance. Am J Clin Nutr. (1995) 62:302–7. doi: 10.1093/ajcn/62.2.302
62. De Cabo, R , and Mattson, MP . Effects of intermittent fasting on health, aging, and disease. N Engl J Med. (2019) 381:2541–51. doi: 10.1056/NEJMra1905136
63. Varady, KA , Allister, CA , Roohk, DJ , and Hellerstein, MK . Improvements in body fat distribution and circulating adiponectin by alternate-day fasting versus calorie restriction. J Nutr Biochem. (2010) 21:188–95. doi: 10.1016/j.jnutbio.2008.11.001
64. Yang, M , Wallenstein, G , Hagan, M , Guo, A , Chang, J , and Kornstein, S . Burden of premenstrual dysphoric disorder on health-related quality of life. J Women’s Health. (2008) 17:113–21. doi: 10.1089/jwh.2007.0417
65. Bauersfeld, SP , Kessler, CS , Wischnewsky, M , Jaensch, A , Steckhan, N , Stange, R, et al. The effects of short-term fasting on quality of life and tolerance to chemotherapy in patients with breast and ovarian cancer: a randomized cross-over pilot study. BMC Cancer. (2018) 18:1–10. doi: 10.1186/s12885-018-4353-2
Keywords: intermittent fasting, alternate-day modified fasting, calorie restriction, premenstrual syndrome, PMS, health-related quality of life, obesity, overweight
Citation: Hooshiar SH, Yazdani A and Jafarnejad S (2024) Does an alternate-day modified fasting diet improve premenstrual syndrome symptoms and health-related quality of life in obese or overweight women with premenstrual syndrome? A randomized, controlled trial. Front. Nutr. 10:1298831. doi: 10.3389/fnut.2023.1298831
Edited by:
Eric Gumpricht, Isagenix International, LLC, United StatesReviewed by:
Vali Musazadeh, Tabriz University of Medical Sciences, IranCopyright © 2024 Hooshiar, Yazdani and Jafarnejad. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sadegh Jafarnejad, c2phZmFybmVqYWRAYWx1bW51cy50dW1zLmFjLmly
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.