
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Nutr., 17 October 2023
Sec. Clinical Nutrition
Volume 10 - 2023 | https://doi.org/10.3389/fnut.2023.1264338
This article is part of the Research TopicIntervention Effects of Food-derived Polyphenols and Bioactive Peptides on Chronic InflammationView all 14 articles
 Xiaopeng Huang
Xiaopeng Huang Jinshan Zhang*
Jinshan Zhang* Yongqiang Zheng
Yongqiang Zheng Xiaofeng LiuYongquan Xu
Xiaofeng LiuYongquan Xu Yangzhen FangZhenyu LinLiang LinHongpeng ZhangZefeng Wang
Yangzhen FangZhenyu LinLiang LinHongpeng ZhangZefeng WangObjective: The objective of this study is to investigate whether alcohol exposure and specific alcoholic drinks are independent risk factors for incident knee surgery in knee osteoarthritis (KOA) patients.
Methods: We identified all patients who were clinically diagnosed as KOA between January 2010 and January 2018 in our outpatient department. Demographic, clinical, and radiographic data were collected from the database of our hospital. Next, we analyzed the association between alcohol consumption and incident knee surgery.
Results: A total of 4,341 KOA patients completed the current study and were included in the final analysis. Incident knee surgery for the purpose of treating osteoarthritis was observed in 242 patients. Incident knee surgery was significantly associated with age (OR [95%CI], 1.023 [1.009–1.039], P = 0.002), BMI (OR [95%CI], 1.086 [1.049–1.123], P < 0.001), baseline K-L grade 3 (OR [95%CI], 1.960 [1.331–2.886], P = 0.001), baseline K-L grade 4 (OR [95%CI], 1.966 [1.230–3.143], P = 0.005), 7.1–14 drinks per week (OR [95%CI], 2.013 [1.282–3.159], P = 0.002), >14 standard drinks per week (OR [95%CI], 2.556 [1.504–4.344], P = 0.001), and the most common alcoholic drink produced by pea (OR [95%CI], 3.133 [1.715–5.723], P < 0.001).
Conclusion: KOA patients who consumed more than seven standard drinks per week were at substantial risk of incident knee surgery. In addition, alcoholic drink produced by pea is also an independent risk factor.
Knee osteoarthritis (KOA) is characterized by three core symptoms (pain, stiffness, and limited function) and accompanied by many structural alterations including degradation of cartilage subchondral bone remodeling, meniscal degeneration, and Hoffa's and effusion synovitis, affecting more than 10% of the overall population globally as estimated (1–3). The disease burden of KOA had been projected to double in the following decades because of the increasing aging of the population (4). Many risk factors for KOA development and progression including female sex, aging, and overweight/obesity have been well-established by previous studies (5, 6). Lifestyle intervention is the cornerstone of KOA management. According to a previous study, weight loss could be beneficial for KOA patients in the long term (7). In addition, increasing physical activities appropriately is also important for KOA patients by increasing lower-limb muscle strength (8–10).
KOA could also be treated with surgical procedures. The efficacy and safety of total knee arthroplasty (TKA), unicompartmental knee arthroplasty (UKA), and high tibial osteotomy (HTO) have been well-established and generally recommended for KOA management (11, 12). In contrast, many high-quality, multicenter, randomized clinical trials have consistently and repeatedly demonstrated that arthroscopic procedures, including lavage, debridement, and arthroscopic partial meniscectomy, are ineffective and even harmful in the long term for KOA patients (13–16). However, this high-quality evidence failed to curb the increase in arthroscopic procedures in KOA patients (13–16). Nevertheless, incident arthroscopic procedures at least reflected poor symptom control and were reasonably considered clinically important events for disease progression.
Excessive alcohol consumption and alcoholism are major global risk factors for increased all-cause mortality and incident morbidities but not limited to cardiovascular diseases, malignancies, neurological diseases, and accidental injuries (17–20). For KOA, a previous study revealed that excessive alcohol drinking was associated with an increased risk of KOA (21). Furthermore, the mechanistic link between alcohol intake and KOA development has been elucidated by a preclinical study (22). A population-based study concluded that alcohol consumption contributed to radiographic change in KOA in Korea (23). Notably, previous studies in KOA patients only focused on the amount of alcohol consumption rather than specific types of alcoholic drinks. This study aimed to investigate whether alcohol exposure and specific alcoholic drinks are independent risk factors for incident knee surgery in KOA patients.
This study followed the Declaration of Helsinki and all local laws and regulations during design and conducted data analysis. We obtained ethics approval for collecting all related data from patients and medical records. We identified all patients who were clinically diagnosed as KOA at a visit to our outpatient department between January 2010 and January 2018 via the hospital information system (HIS). The clinical diagnosis of KOA in the current study was defined as those made by clinical specialists in orthopedic and/or sports medicine. It was generally determined based on patient history, physical examination, and laboratory and radiographic findings (24). As shown in Figure 1, patients were excluded from this study if they had any knee surgery histories (n = 125), concomitant structural knee injuries (fractures, ligament ruptures, meniscal tears, and dislocations; n = 345), missing values for essential baseline variables (n = 567), and declining to participate (n = 1,152).
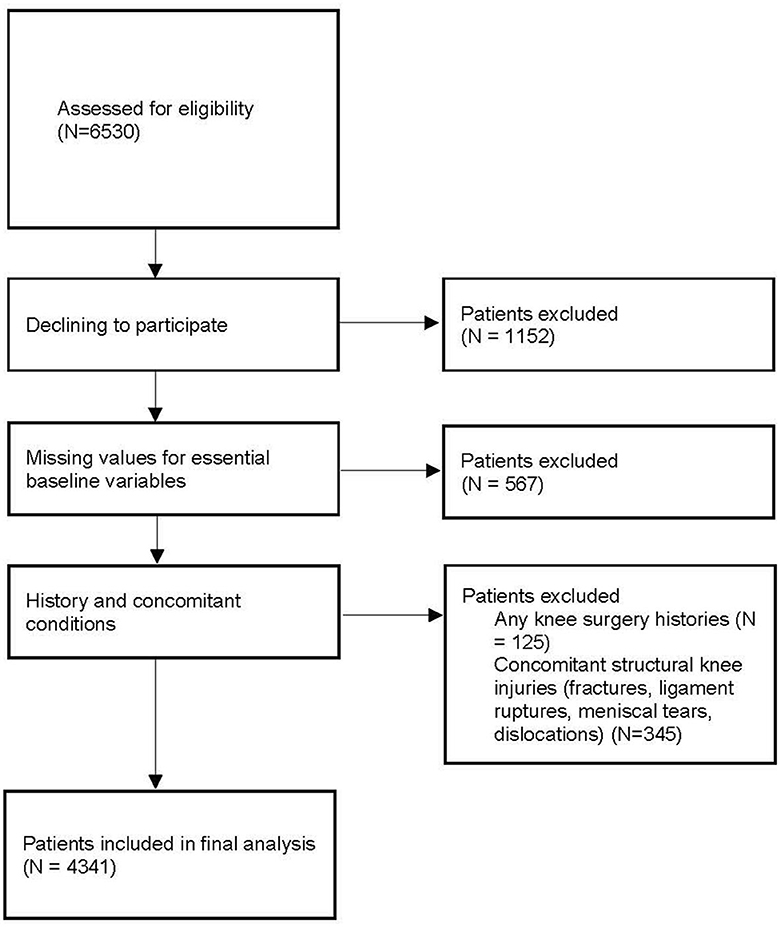
Figure 1. Study screening and enrollment.
We defined the baseline as the time of performing the first knee plain radiograph during the study period. All baseline demographic and clinical data were retrieved from HIS, and the information was further confirmed by contacting patients through on-site interview, telephone, email, and instant message software. The baseline demographic data consisted of demographic information (sex, age, and body mass index [BMI]) calculated by weight, height, and education. The Kellgren–Lawrence (K-L) grades (25) were rated by a radiographic evaluation committee consisting of three radiologists specialized in musculoskeletal radiology. The rating process was conducted without grouping information. The consensus on grading was achieved by the majority of people. When the two knees had different K-L grades, the final K-L grade was recorded according to the more severe side.
The alcohol consumption was self-reported by patients based on their recalling for the last 12 months. Show cards were used to prompt recalling of the number of standard drinks usually consumed per week. Each show card, respectively, illustrated the typical volume of Chinese distilled spirit (25 ml of 50% alcohol/volume), Chinese rice wine (90 ml of 15% alcohol/volume), wine (120 ml of 11% alcohol/volume), and beer (285 ml of 4.5% alcohol/volume) equivalent to 10 g of ethanol, defined as a standard drink (26). For those who reported frequent consumption of other types of alcoholic beverages during the previous year, researchers calculated the weekly consumption after collecting the label information of these alcoholic beverages. The weekly number of standard drinks was recorded in a categorical manner as none, ≤1, 1.1–7, 7.1–14, and >14 standard drinks per week. The researchers also asked the patients for his or her most common alcoholic beverage type (beer, Chinese distilled spirit, Chinese rice wine, wine, and others). We collected label information of the most commonly consumed alcoholic beverages and recorded the raw materials (barley, wheat, grape, rice, kaoliang, pea, and corn) of these alcoholic beverages.
In this study, incident knee surgery was defined as any surgical procedure performed for the purpose of treating KOA no matter whether this type of surgical procedure was recommended or not. The incident knee surgery and types of surgery were reported by patients. In the current study, incident knee surgery included TKA, arthroscopic procedures (ineffective and not recommended), UKA, and HTO.
All statistical analyses were performed using SPSS software (IBM Corp. Released 2019. IBM SPSS Statistics for Windows, version 26.0. Armonk, NY: IBM Corp). The statistical significance was set at a two-sided 0.05. We first tabulated descriptive statistics to summarize the characteristics of the subjects. Continuous and categorical variables were, respectively, presented as means ± standard deviations and counts (percentage), unless otherwise indicated. When the P-value was <0.2 in univariable analysis, the variables along with demographic variables (age, sex, and BMI) were further included in logistic regression for multivariable analysis.
A total of 4,341 KOA patients were included in the final analysis. Incident knee surgery for the purpose of treating osteoarthritis was observed in 242 patients out of 4,341 patients during the study period. Specifically, 65 patients had TKA, 5 had UKA, 162 had arthroscopic procedures, and 10 had high tibial osteotomy. For univariable analyses, incident knee surgery was significantly associated with age, BMI, baseline K-L grades, alcohol consumption, and the most common type of alcoholic beverage produced by pea (Table 1). The logistic regression model included sex, baseline BMI, baseline age, alcohol consumption, most common type of alcoholic beverage produced by pea, and baseline K-L grades.
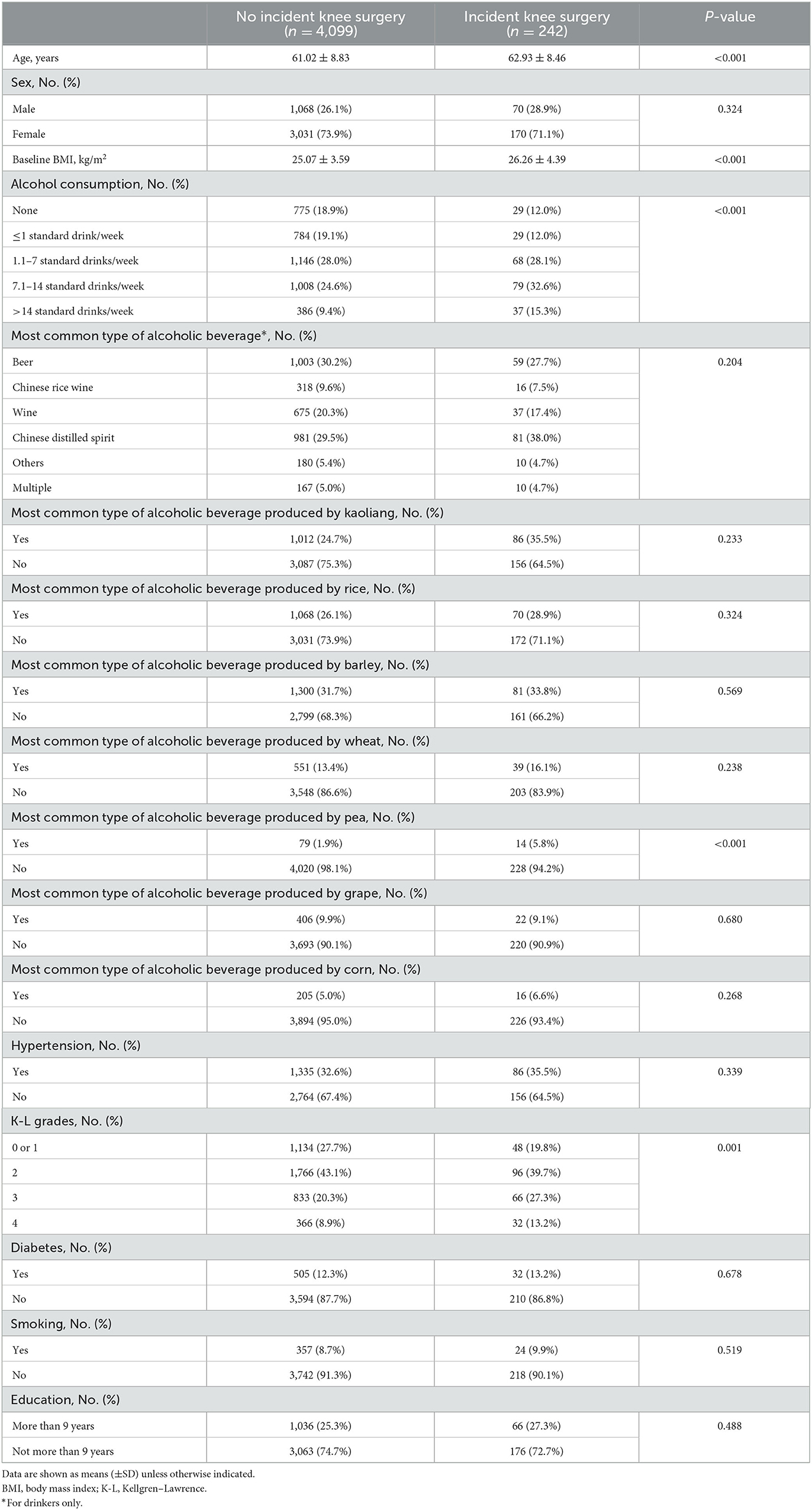
Table 1. Univariable analysis on characteristics grouped by incident knee surgery.
After adjustment with the multivariable logistic regression, incident knee surgery was significantly associated age (OR [95%CI], 1.023 [1.009–1.039], P = 0.002), BMI (OR [95%CI], 1.086 [1.049–1.123], P < 0.001), baseline K-L grade 3 (OR [95%CI], 1.960 [1.331–2.886], P = 0.001), baseline K-L grade 4 (OR [95%CI], 1.966 [1.230–3.143], P = 0.005), 7.1–14 drinks per week (OR [95%CI], 2.013 [1.282–3.159], P = 0.002), >14 standard drinks per week (OR [95%CI], 2.556 [1.504–4.344], P = 0.001), and the most common alcoholic drink produced by pea (OR [95%CI], 3.133 [1.715–5.723], P < 0.001; Table 2).
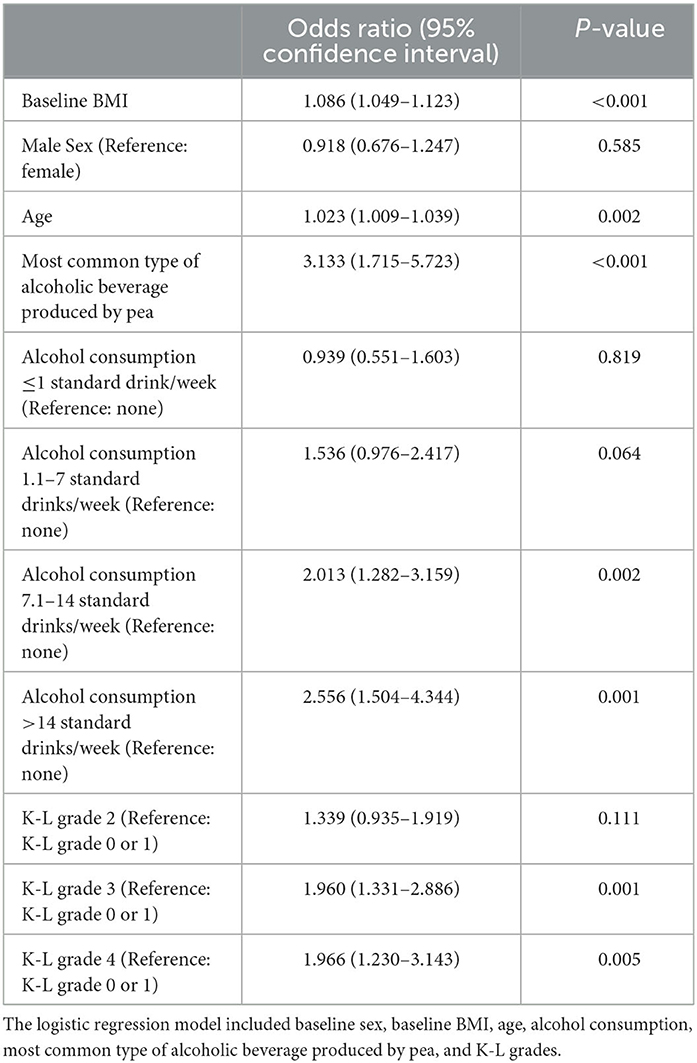
Table 2. Multivariable analysis on characteristics grouped by incident knee surgery.
A previous study using data from the Osteoarthritis Initiative study revealed that excessive alcohol drinking was associated with an increased risk of both radiographic and symptomatic KOA (21). Similarly, a population-based and longitudinal study conducted in Korea found that alcohol consumption contributed to the radiographic progression of KOA (23). For osteoarthritis in other anatomic sites, researchers reported that alcohol exposure is associated with structural destruction and inflammatory features of hand osteoarthritis (27). Notably, previous studies in KOA patients only focused on the amount of alcohol consumption rather than specific types of alcoholic drinks.
The underlying mechanism between alcohol drinking and osteoarthritis remains greatly unclear, while many plausible hypotheses and theories have been proposed. As revealed by many preclinical investigations, alcohol intake is capable of inducing pro-inflammatory states in joints and is thus believed to be a contributing factor to the development and progression of KOA (22). In a mouse model, chronic alcohol consumption also increases cartilage loss in large joints by impairing extracellular matrix production and accelerating the degradation (28). In addition, alcohol could increase the level of inflammatory mediator interleukin-6 (IL-6), an important cytokine in KOA development and progression (29).
The most important and novel finding of the current study is the unexpected association between incident knee surgery and exposure to pea-derived alcoholic beverages in KOA patients. To the best of our knowledge, only some types of Chinese distilled spirit (most of them are made by a fermentation technique called “Daqu”) use pea as a major raw material worldwide. Daqu is one of the oldest and most widely used fermentation technique for spirit-making (30). In addition to alcohol, fermentation with the Daqu technique often produces substantial amount and various types of chemicals with unknown effects on humans (30–32). Clearly, microbiota (molds, yeasts, and bacteria) are responsible for the final chemicals. However, in the current study, we are unable to further determine whether certain microorganisms are involved in this phenomenon. Nevertheless, our finding provides a unique and exciting insight into the pathogenesis of osteoarthritis.
The current study had several limitations. First, future confirmation of our observation by prospective and larger cohort studies should be performed. If so, mechanistic studies are urgently needed to explore why pea-derived alcoholic beverages are associated with osteoarthritis progression. Notably, this is the first study reporting this phenomenon, and thus, we are currently unable to propose a reasonable hypothesis without future mechanistic studies. Second, because of the observational nature, the decision on whether to receive surgical treatment in this study lacked transparency for us and readers. Finally, because the drinking pattern and specific types of alcoholic beverages may largely vary by age, sex, and socioeconomic status in a general population (33, 34), future studies on alcohol consumption and KOA should further explore these factors. Extrapolation of our conclusion to a different setting should be cautious.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
The studies involving humans were approved by the Ethics Committee at Jinjiang Municipal Hospital. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
XH: Data curation, Investigation, Writing—original draft. JZ: Conceptualization, Funding acquisition, Methodology, Project administration, Supervision, Validation, Writing—review and editing. YZ: Data curation, Investigation, Writing—original draft. XL: Data curation, Investigation, Writing—original draft. YX: Data curation, Investigation, Writing—original draft. YF: Data curation, Investigation, Writing—original draft. ZL: Data curation, Investigation, Writing—original draft. LL: Data curation, Investigation, Writing—original draft. HZ: Data curation, Investigation, Writing—original draft. ZW: Data curation, Investigation, Writing—original draft.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was supported by the Science and Technology Project of Quanzhou City (2020N079s).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Cross M, Smith E, Hoy D, Nolte S, Ackerman I, Fransen M, et al. The global burden of hip and knee osteoarthritis: estimates from the global burden of disease 2010 study. Ann Rheum Dis. (2014) 73:1323–30. doi: 10.1136/annrheumdis-2013-204763
2. Zhu H, Zhou L, Wang Q, Cai Q, Yang F, Jin H, et al. Glucagon-like peptide-1 receptor agonists as a disease-modifying therapy for knee osteoarthritis mediated by weight loss: findings from the Shanghai Osteoarthritis Cohort. Ann Rheum Dis. (2023) 82:1218–26. doi: 10.1136/ard-2023-223845
3. GBD 2019 Risk Factors Collaborators. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. (2020) 396:1223–49. doi: 10.1016/S0140-6736(20)30752-2
4. Long H, Liu Q, Yin H, Wang K, Diao N, Zhang Y, et al. Prevalence trends of site-specific osteoarthritis from 1990 to 2019: findings from the global burden of disease study 2019. Arthritis Rheumatol. (2022) 74:1172–83. doi: 10.1002/art.42089
6. Kan HS, Chan PK, Chiu KY, Yan CH, Yeung SS, Ng YL, et al. Non-surgical treatment of knee osteoarthritis. Hong Kong Med J. (2019) 25:127–33. doi: 10.12809/hkmj187600
7. Wang Q, Runhaar J, Kloppenburg M, Boers M, Bijlsma JWJ, Bierma-Zeinstra SMA. Diagnosis of early stage knee osteoarthritis based on early clinical course: data from the CHECK cohort. Arthritis Res Ther. (2021) 23:217. doi: 10.1186/s13075-021-02598-5
8. Brennan AM, Standley RA, Anthony SJ, Grench KE, Helbling NL, DeLany JP, et al. Weight loss and exercise differentially affect insulin sensitivity, body composition, cardiorespiratory fitness, and muscle strength in older adults with obesity: a randomized controlled trial. J Gerontol A Biol Sci Med Sci. (2022) 77:1088–97. doi: 10.1093/gerona/glab240
9. McCrimmon RJ, Catarig AM, Frias JP, Lausvig NL, le Roux CW, Thielke D, et al. Effects of once-weekly semaglutide vs once-daily canagliflozin on body composition in type 2 diabetes: a substudy of the SUSTAIN 8 randomised controlled clinical trial. Diabetologia. (2020) 63:473–85. doi: 10.1007/s00125-019-05065-8
10. Aroda VR. A review of GLP-1 receptor agonists: evolution and advancement, through the lens of randomised controlled trials. Diabetes Obes Metab. (2018) 20(Suppl. 1):22–33. doi: 10.1111/dom.13162
11. Glyn-Jones S, Palmer AJ, Agricola R, Price AJ, Vincent TL, Weinans H, et al. Osteoarthritis. Lancet. (2015) 386:376–87. doi: 10.1016/S0140-6736(14)60802-3
12. Martel-Pelletier J, Barr AJ, Cicuttini FM, Conaghan PG, Cooper C, Goldring MB, et al. Osteoarthritis. Nat Rev Dis Primers. (2016) 2:16072. doi: 10.1038/nrdp.2016.72
13. Moseley JB, O'Malley K, Petersen NJ, Menke TJ, Brody BA, Kuykendall DH, et al. A controlled trial of arthroscopic surgery for osteoarthritis of the knee. N Engl J Med. (2002) 347:81–8. doi: 10.1056/NEJMoa013259
14. Sihvonen R, Paavola M, Malmivaara A, Itälä A, Joukainen A, Kalske J, et al. Arthroscopic partial meniscectomy for a degenerative meniscus tear: a 5 year follow-up of the placebo-surgery controlled FIDELITY (Finnish Degenerative Meniscus Lesion Study) trial. Br J Sports Med. (2020) 54:1332–9. doi: 10.1136/bjsports-2020-102813
15. Stahel PF, Wang P, Hutfless S, McCarty E, Mehler PS, Osgood GM, et al. Surgeon practice patterns of arthroscopic partial meniscectomy for degenerative disease in the united states: a measure of low-value care. JAMA Surg. (2018) 153:494–6. doi: 10.1001/jamasurg.2017.6235
16. Rickert J. On patient safety: orthopaedic surgeons must stop performing arthroscopic partial meniscectomy on patients with arthritic knees. Clin Orthop Relat Res. (2020) 478:28–30. doi: 10.1097/CORR.0000000000001072
18. Anderson P, Chisholm D, Fuhr DC. Effectiveness and cost-effectiveness of policies and programmes to reduce the harm caused by alcohol. Lancet. (2009) 373:2234–46. doi: 10.1016/S0140-6736(09)60744-3
19. Roerecke M, Rehm J. Alcohol consumption, drinking patterns, and ischemic heart disease: a narrative review of meta-analyses and a systematic review and meta-analysis of the impact of heavy drinking occasions on risk for moderate drinkers. BMC Med. (2014) 12:182. doi: 10.1186/s12916-014-0182-6
20. Barbería-Latasa M, Gea A, Martínez-González MA. Alcohol, drinking pattern, and chronic disease. Nutrients. (2022) 14:1954. doi: 10.3390/nu14091954
21. Liu T, Xu C, Driban JB, McAlindon T, Eaton CB, Lu B. Excessive alcohol consumption and the risk of knee osteoarthritis: a prospective study from the osteoarthritis initiative. Osteoarthr Cartil. (2022) 30:697–701. doi: 10.1016/j.joca.2022.01.011
22. Kc R, Voigt R, Li X, Forsyth CB, Ellman MB, Summa KC, et al. Induction of osteoarthritis-like pathologic changes by chronic alcohol consumption in an experimental mouse model. Arthritis Rheumatol. (2015) 67:1678–80. doi: 10.1002/art.39090
23. Kang AH, Kim MR, Shin JS, Lee J, Lee YJ, Park Y, et al. Association between alcohol consumption and osteoarthritis prevalence in Korea as assessed by the alcohol use disorders identification test (AUDIT): a cross-sectional study. BMC Public Health. (2020) 20:227. doi: 10.1186/s12889-020-8326-4
24. Skou ST, Koes BW, Grønne DT, Young J, Roos EM. Comparison of three sets of clinical classification criteria for knee osteoarthritis: a cross-sectional study of 13,459 patients treated in primary care. Osteoarthr Cartil. (2020) 28:167–72. doi: 10.1016/j.joca.2019.09.003
25. Kohn MD, Sassoon AA, Fernando ND. Classifications in brief: Kellgren-Lawrence classification of osteoarthritis. Clin Orthop Relat Res. (2016) 474:1886–93. doi: 10.1007/s11999-016-4732-4
26. Kerr WC, Stockwell T. Understanding standard drinks and drinking guidelines. Drug Alcohol Rev. (2012) 31:200–5. doi: 10.1111/j.1465-3362.2011.00374.x
27. Magnusson K, Mathiessen A, Hammer HB, Kvien TK, Slatkowsky-Christensen B, Natvig B, et al. Smoking and alcohol use are associated with structural and inflammatory hand osteoarthritis features. Scand J Rheumatol. (2017) 46:388–95. doi: 10.1080/03009742.2016.1257736
28. Lorenz J, Schäfer N, Bauer R, Jenei-Lanzl Z, Springorum RH, Grässel S. Norepinephrine modulates osteoarthritic chondrocyte metabolism and inflammatory responses. Osteoarthr Cartil. (2016) 24:325–34. doi: 10.1016/j.joca.2015.08.007
29. Lu B, Solomon DH, Costenbader KH, Keenan BT, Chibnik LB, Karlson EW. Alcohol consumption and markers of inflammation in women with preclinical rheumatoid arthritis. Arthritis Rheum. (2010) 62:3554–9. doi: 10.1002/art.27739
30. Liu H, Sun B. Effect of fermentation processing on the flavor of Baijiu. J Agric Food Chem. (2018) 66:5425–32. doi: 10.1021/acs.jafc.8b00692
31. Shi X, Zhao S, Chen S, Han X, Yang Q, Zhang L, et al. Tetramethylpyrazine in Chinese baijiu: Presence, analysis, formation, and regulation. Front Nutr. (2022) 9:1004435. doi: 10.3389/fnut.2022.1004435
32. Wu XH, Zheng XW, Han BZ, Vervoort J, Nout MJ. Characterization of Chinese liquor starter, “Daqu”, by flavor type with 1H NMR-based nontargeted analysis. J Agric Food Chem. (2009) 57:11354–9. doi: 10.1021/jf902881p
33. Allen L, Williams J, Townsend N, Mikkelsen B, Roberts N, Foster C, et al. Socioeconomic status and non-communicable disease behavioural risk factors in low-income and lower-middle-income countries: a systematic review. Lancet Glob Health. (2017) 5:e277–89. doi: 10.1016/S2214-109X(17)30058-X
Keywords: knee osteoarthritis, alcoholic drink, Kellgren-Lawrence (K-L) grades, total knee arthroplasty (TKA), unicompartmental knee arthroplasty (UKA), high tibial osteotomy
Citation: Huang X, Zhang J, Zheng Y, Liu X, Xu Y, Fang Y, Lin Z, Lin L, Zhang H and Wang Z (2023) Alcoholic drink produced by pea is a risk factor for incident knee surgery in patients with knee osteoarthritis. Front. Nutr. 10:1264338. doi: 10.3389/fnut.2023.1264338
Received: 21 July 2023; Accepted: 21 September 2023;
Published: 17 October 2023.
Edited by:
Danila Cianciosi, Università Politecnica delle Marche, ItalyReviewed by:
Mahsa Jalili, University of Copenhagen, DenmarkCopyright © 2023 Huang, Zhang, Zheng, Liu, Xu, Fang, Lin, Lin, Zhang and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jinshan Zhang, emhhbmdqaW5zaGFuMTkzQHNpbmEuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.