 Yinghui Ma
Yinghui Ma Yuying Zhu1
Yuying Zhu1 Lei Li
Lei Li- 1School of Economics and Management, Jiangsu University of Science and Technology, Zhenjiang, China
- 2School of Economics and Management, Beijing Forestry University, Beijing, China
- 3College of Economics and Management, Zhejiang A & F University, Hangzhou, China
- 4Research Academy for Rural Revitalization of Zhejiang, Zhejiang A & F University, Hangzhou, China
Objective: As the global population ages, disability among the elderly presents unprecedented challenges for healthcare systems. However, limited research has examined whether dietary interventions like tea consumption may alleviate and prevent disability in older adults. As an important dietary therapy, the health benefits of tea drinking have gained recognition across research disciplines. Therefore, this study aimed to investigate the association between tea drinking habits and disability levels in the elderly Chinese population.
Methods: Leveraging data from the 2008 to 2018 waves of the Chinese Longitudinal Healthy Longevity Survey, we disaggregated tea drinking frequency and activities of daily living (ADL) measures and deployed fixed-effect ordered logit models to examine the tea-disability association for the first time. We statistically adjusted for potential confounders and conducted stratified analyses to assess heterogeneity across subpopulations.
Results: Multivariable fixed-effect ordered logistic regression suggested tea drinking has protective effects against ADL disability. However, only daily tea drinking was associated with lower risks of basic activities of daily living (BADL) disability [odds ratio (OR) = 0.61; 95% confidence interval (CI), 0.41–0.92] and lower levels of instrumental activities of daily living (IADL) disability (OR = 0.78; 95% CI, 0.64–0.95). Stratified analyses indicated heterogeneous effects across age and income groups. Daily tea drinking protected against BADL (OR = 0.26 and OR = 0.28) and IADL disability (OR = 0.48 and OR = 0.45) for adults over 83 years old and high-income households, respectively.
Conclusion: We found that drinking tea almost daily was protective against disability in elderly people, warranting further research into optimal dosages. Future studies should utilize more rigorous causal inference methods and control for confounders.
1. Introduction
The growing prevalence of disability among the elderly has become a critical global issue. An estimated 100 million older adults suffer from varying degrees of disability (1). Disability in the elderly refers to the loss or limitation of their ability to perform daily activities and maintain living skills (2). Treatable pathological factors, such as diabetes or malnutrition, may cause these disabilities (3–5). Therefore, interventions such as treating diseases or improving nutrition may enhance disability status in the elderly. Neurodegenerative diseases, Alzheimer’s disease, and other cognitive disorders lead to a decline in memory, thinking, and behavior in the elderly, impacting their daily living skills and independence (6, 7). There is no complete solution for the disability caused by these degenerative diseases in the elderly. Therefore, adopting preventive strategies is crucial.
China faces a severe aging crisis, with disability rates among older adults increasing from 7% in 2015 to 7.45% in 2020 (8, 9). Projections from China’s Old Age Association show the disabled elderly population over 65 will grow from approximately 187 million in 2020 to over 520 million by 2050. The proportion of disabled elderly people in the total population will also continue to rise, with the disabled elderly population accounting for approximately 13.68% of the total elderly population in 2050 (10).
Tea contains antioxidants and bioactive compounds, such as flavonoids, catechins, polyphenols, and gallic acid (11). These substances all have biological activities and can reduce the risk of dementia by alleviating oxidative stress and inhibiting inflammatory responses (12). Using data from adults aged 65 years and above in Taiwan, Chiu et al. (13) found that higher tea intake was associated with lower disability levels in both men and women. Tao et al. (14) demonstrated that frequent iced tea and tea drinking had protective effects against ADL disability in the elderly. In a cross-sectional study in China, a lack of tea consumption was identified as one of the predictors of functional disability by Zhang et al. (15).
Apart from the above studies, little research has explored the health impacts of tea drinking on disability. For over 4,000 years, people in China, widely recognized as the origin of tea cultivation, have noted tea’s health benefits and therapeutic properties. Chinese people have been the world’s largest consumers of tea since 2006 (16). Therefore, this study aimed to determine the association between tea drinking and disability levels in older adults, which is important for reducing disability risks, improving quality of life, and alleviating caregiving burdens on families and society for the rapidly aging population.
2. Materials and methods
2.1. Study sample
The Chinese Longitudinal Healthy Longevity Survey (CLHLS), initiated in 1998 by the Center for Healthy Aging and Development Studies at Peking University’s National School of Development, aims to examine the health determinants of individuals aged 65 and above. From 1998 to 2018, approximately half of the counties in 23 provinces, cities, and autonomous regions nationwide were randomly chosen for eight successive surveys, culminating in approximately 113,000 household visits. The survey specifics have been elaborated in previous studies (17, 18). The gathered data encompass demographic and residential information, marital status, lifestyle, socioeconomic attributes, health status, and an extensive array of personal data pertaining to the elderly.
To compensate for participant attrition due to death or loss to follow-up, the CLHLS incorporated new participants, mirroring the characteristics of the departed, to maintain study consistency. All surveys were administered through in-person interviews at the participants’ residences, with each participant providing a signed informed consent form. In cases in which a participant was incapable of signing, a close relative signed on their behalf. This study adhered to the principles of the Declaration of Helsinki.
Data for this study were gleaned from four CLHLS surveys conducted in 2008, 2011, 2014, and 2018, which included the participants who were surveyed about their tea consumption at baseline and followed up afterward. The sample selection process is shown in Figure 1.
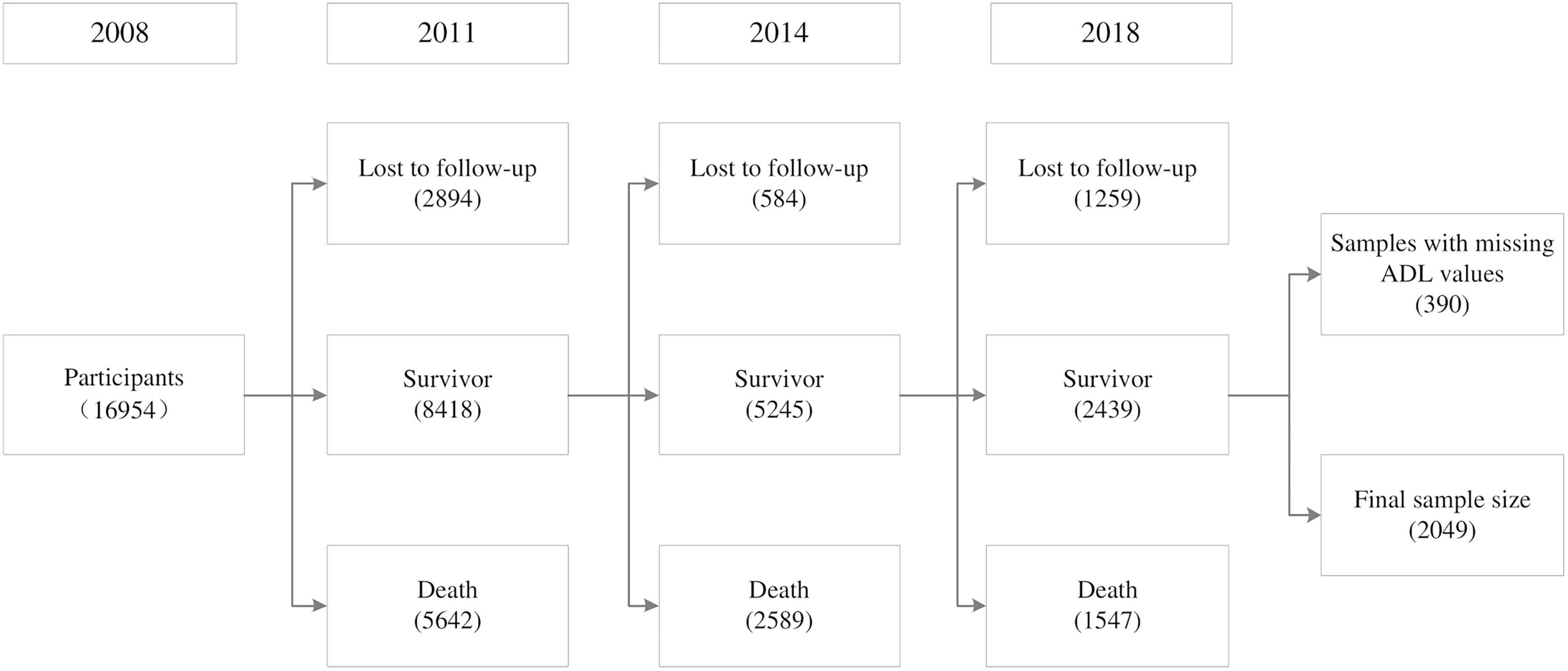
Figure 1. Participant inclusion and exclusion criteria.
2.2. Dependent variables
This study used the Katz Index to gauge disability levels among elderly participants, incorporating both basic activities of daily living (BADL) and instrumental activities of daily living (IADL). BADL ability was evaluated based on six items: bathing, dressing, transferring, toileting, eating, and continence. If the respondent could complete an activity without assistance, it was coded as 1 and otherwise as 0, with scores ranging from 0 to 6. A new variable, “BADL,” was calculated as the sum, in which a maximum score was assigned “1” (representing “non-disabled”); a score of 4–5 was assigned “2” (representing “mild disability”); a score of 2–3 was assigned “3” (representing “moderate disability”); and a score of 0–1 was assigned “4” (representing “severe disability”).
The IADL assessment included eight items: visiting neighbors, shopping, cooking, washing, walking 1 km continuously, lifting 5 kg, crouching and standing up three times continuously, and taking public transport alone. Each item was coded as 1 if the respondent could complete it independently and 0 otherwise, with scores ranging from 0 to 8. A new variable “IADL” was calculated as the sum, in which a maximum score was assigned “1” (representing “non-disabled”); a score of 6–7 was assigned “2” (representing “mild disability”); a score of 3–5 was assigned “3” (representing “moderate disability”); and a score of 0–2 was assigned “4” (representing “severe disability”) (19–21).
2.3. Independent variable
The drinking of tea was measured by the question: “How often do you drink tea?” The response options include almost daily; not every day but at least once a week; not every week but at least once a month; not every month but sometimes; and rarely or never. As the study’s independent variable, drinking tea almost daily was assigned a value of 5; not every day but at least once a week was assigned 4; not every week but at least once a month was assigned 3; not every month but sometimes was assigned 2; and rarely or never was assigned 1. Higher scores indicate a higher frequency of tea drinking.
2.4. Covariate measurements
This study critically examines several potential covariates, including sociodemographic factors, socioeconomic status, and health-related behaviors. Sociodemographic characteristics mainly included age (65–75, 75–83, and 83+), gender (male or female), marital status (married or unmarried), education level (illiteracy, primary school or below, or junior high school or above), and residential category (urban, town, or rural). For socioeconomic status, whether retired with a pension (yes or no), financial support (dependence or independence) and household income (≤ RMB 20,000 or > RMB 20,000) were mainly considered. For health behaviors, self-rated health (good, normal, and bad), current alcohol drinking and smoking (yes or no), fruit and vegetable consumption (often, occasionally, or rarely), and physical exercise (yes or no) were mainly considered.
2.5. Statistical analysis
In the 2008 survey, 16,954 respondents participated and were interviewed. In subsequent follow-ups, 4,737 individuals were lost to follow-up, 9,778 died, and 390 had missing ADL scores; these samples were excluded. A total of 2,049 participants completed the survey four times and were eventually included in the balanced panel data analysis (Figure 1). There were 623 missing values for sociodemographic characteristics and socioeconomic status, which we replaced with the individual’s data from the previous year.
Based on the baseline characteristics summarized by tea consumption frequency, we employed the chi-square test and univariate analysis to examine categorical variables, and variance analysis for continuous variables. Taking into account time-invariant individual characteristics, we utilized panel data methods and applied the fixed effect ordered logit model to assess the odds ratio (OR) and 95% confidence interval (95% CI) for the impact of tea consumption on the level of disability in the elderly during the 2008–2018 follow-up period. Model 1 was a univariate analysis without adjustment. Model 2 adjusted for age, gender, marital status, education level, and residence. Model 3 added retirement status, financial support, self-rated health, drinking, smoking, exercise, and fruit and vegetable intake. For subgroup analyses, we grouped age and income by terciles and dichotomy, respectively, and all models adjusted for demographics, socioeconomics, and health behaviors.
Analyses were performed in STATA 17.0. All p-values are two-sided with p < 0.05 considered statistically significant.
3. Results
3.1. Descriptive characteristics
Table 1 displays the baseline descriptive characteristics of the study cohort categorized by tea consumption frequency. The sample consisted of 2,049 respondents with an average age of 75.07 years; 1,072 were female (52.32%), 61.01% were married, and 12.49% resided in urban areas, with the rest living in rural areas. Although the vast majority of the elderly were financially independent (78.28%), 74.82% of them belonged to households with an annual income of less than RMB 20,000. The proportion of the elderly who perceived their health status as good was 56.91% and the proportions of the elderly who smoked and drank were relatively low at 22.99 and 22.69%, respectively. Almost everyone (91.61%) frequently consumed fresh vegetables; only 42.41% ate fresh fruits often and 34.46% engaged in physical exercise. In the total sample, 48.32% of the participants drank tea almost every day and 36.07% rarely or never drank tea. The remaining three categories accounted for only 15.62% of the total sample.
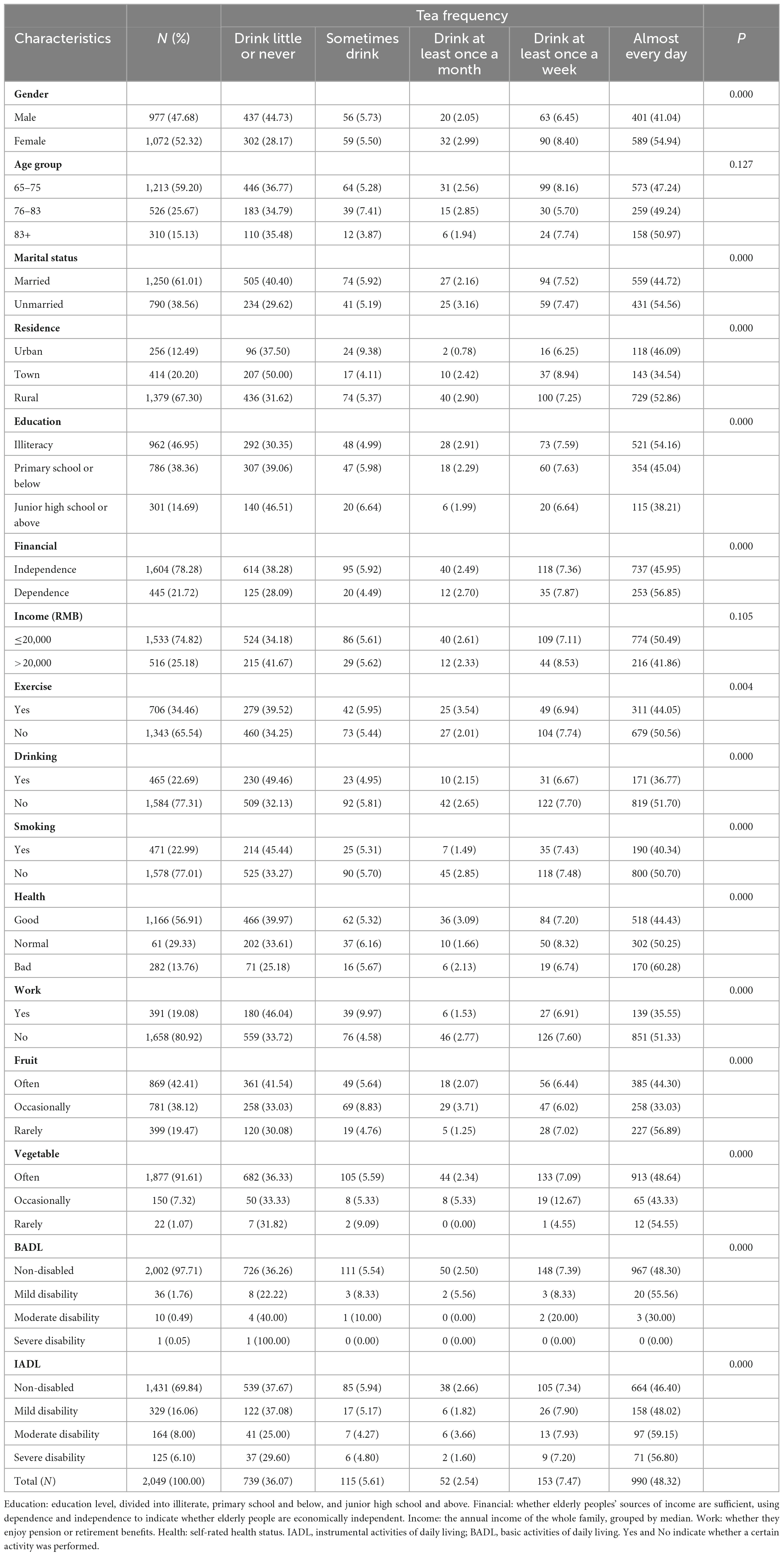
Table 1. Baseline characteristics of participants stratified by tea drinking frequency.
Those who did not benefit from a retirement system were more likely to drink tea almost daily than those who did, a difference that is statistically significant (p = 0.000). Similarly, individuals with higher educational levels and those who did not smoke, drink, and regularly consume fresh fruits and partake in other healthy behaviors were more likely to drink tea, with these differences also being statistically significant (p < 0.01). Only 2.29% of all participants suffered from varying degrees of BADL disability, whereas the incidence rate of IADL disability was as high as 30.16%. Those without disabilities were more inclined to consume tea.
3.2. Logistic regression results
In Table 2, unadjusted fixed effects ordered logit models indicated almost everyday tea drinking protected against BADL (OR = 0.53; 95% CI, 0.34–0.83) and IADL disability (OR = 0.74; 95% CI, 0.61–0.89) compared with drink little or never. After adjusting for sociodemographic characteristics, socioeconomic status, and healthy behaviors, almost everyday tea drinking still had a protective effect against IADL (OR = 0.78; 95% CI, 0.64–0.95) and BADL disability (OR = 0.61; 95% CI, 0.41–0.92).
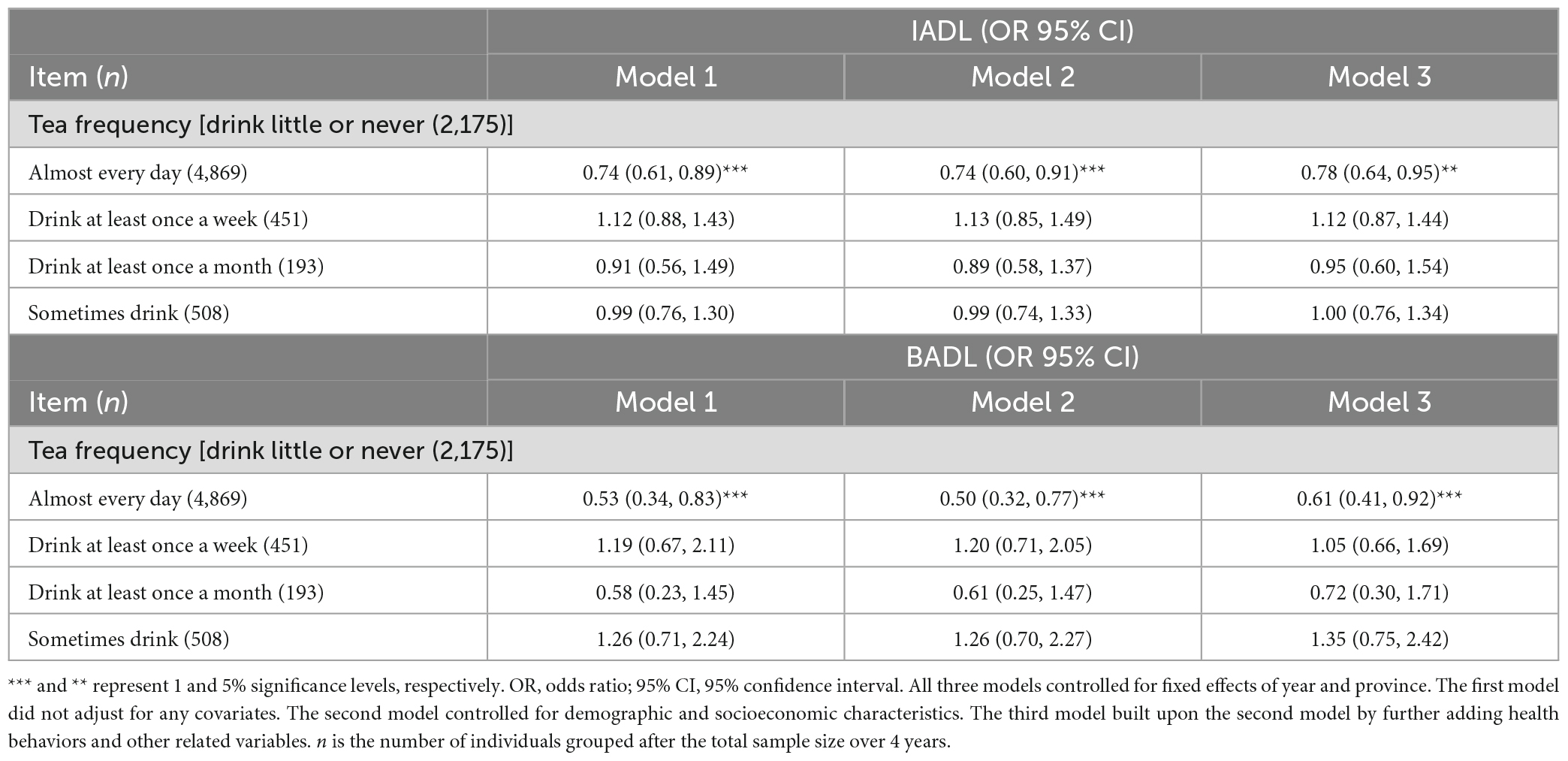
Table 2. Associations between tea drinking and disability among older Chinese people.
3.3. Subgroup analysis
Previous studies indicate that tea consumption effects on cognition vary by age and economic status in the elderly (22, 23). This section explores whether tea-disability associations differ by age and income. Stratified regression by age (Table 3) showed that drinking frequencies above drink at least once a month have a protective effect against BADL disability in elderly individuals aged 83 and above (OR = 0.36, OR = 0.42, and OR = 0.26). At least once a month (OR = 0.51; 95% CI, 0.2–0.91) and almost everyday drinking (OR = 0.48; 95% CI, 0.33–0.69) were also associated with less IADL disability. These findings indicate that tea drinking may help prevent ADL ability decline and functional deterioration in the oldest section of the population.
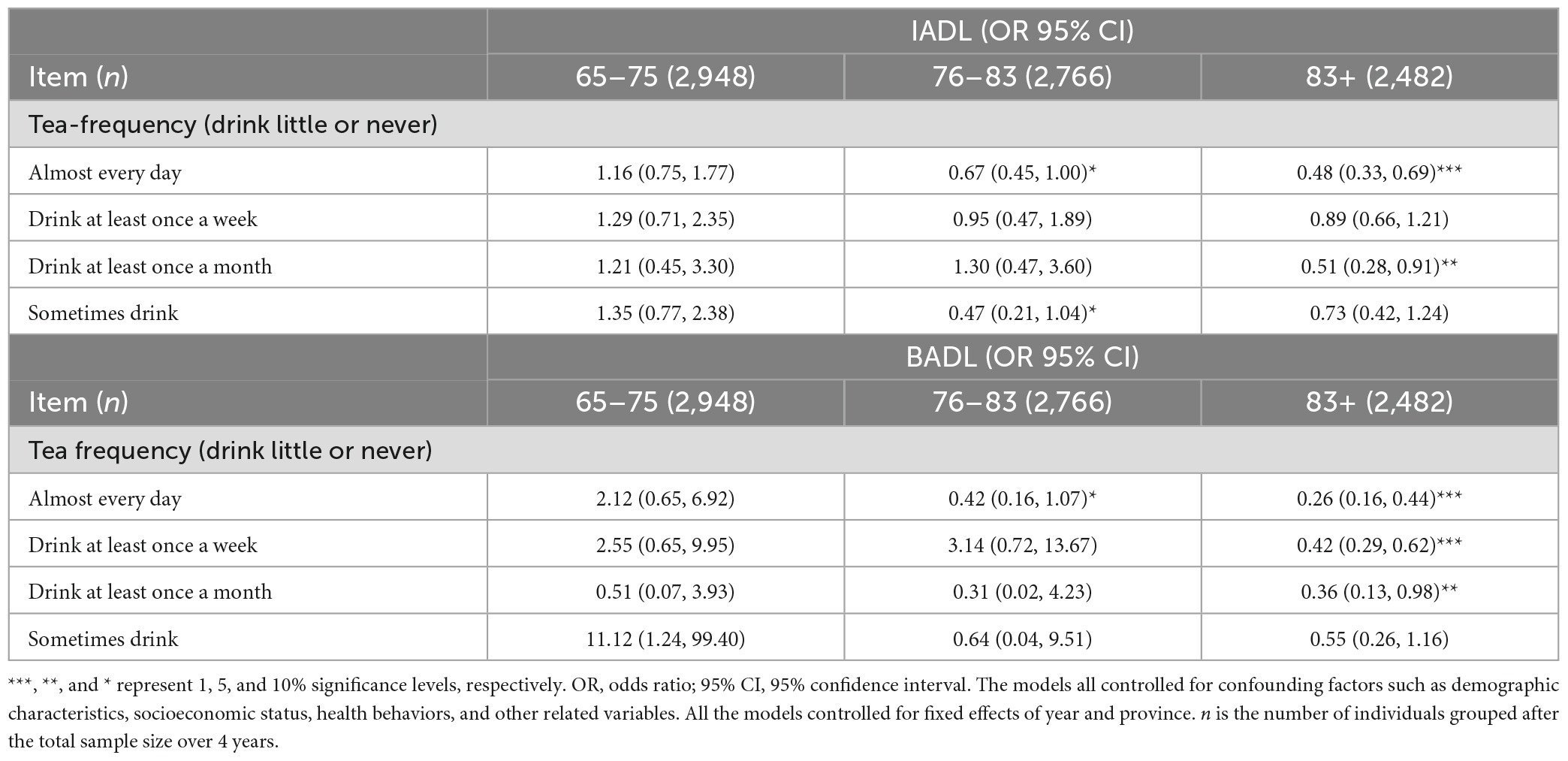
Table 3. The association between tea drinking and disability stratified by age.
Income was dichotomized into high and low groups. Stratified analysis (Table 4) showed that almost everyday tea drinking had a positive protective effect against BADL disability in high-income elderly people (OR = 0.28; 95% CI, 0.15–0.50). Sometimes and almost everyday drinking also protected against IADL disability decline (OR = 0.78 and OR = 0.45, respectively). However, tea drinking did not significantly impact BADL or IADL disability in low-income elderly people.
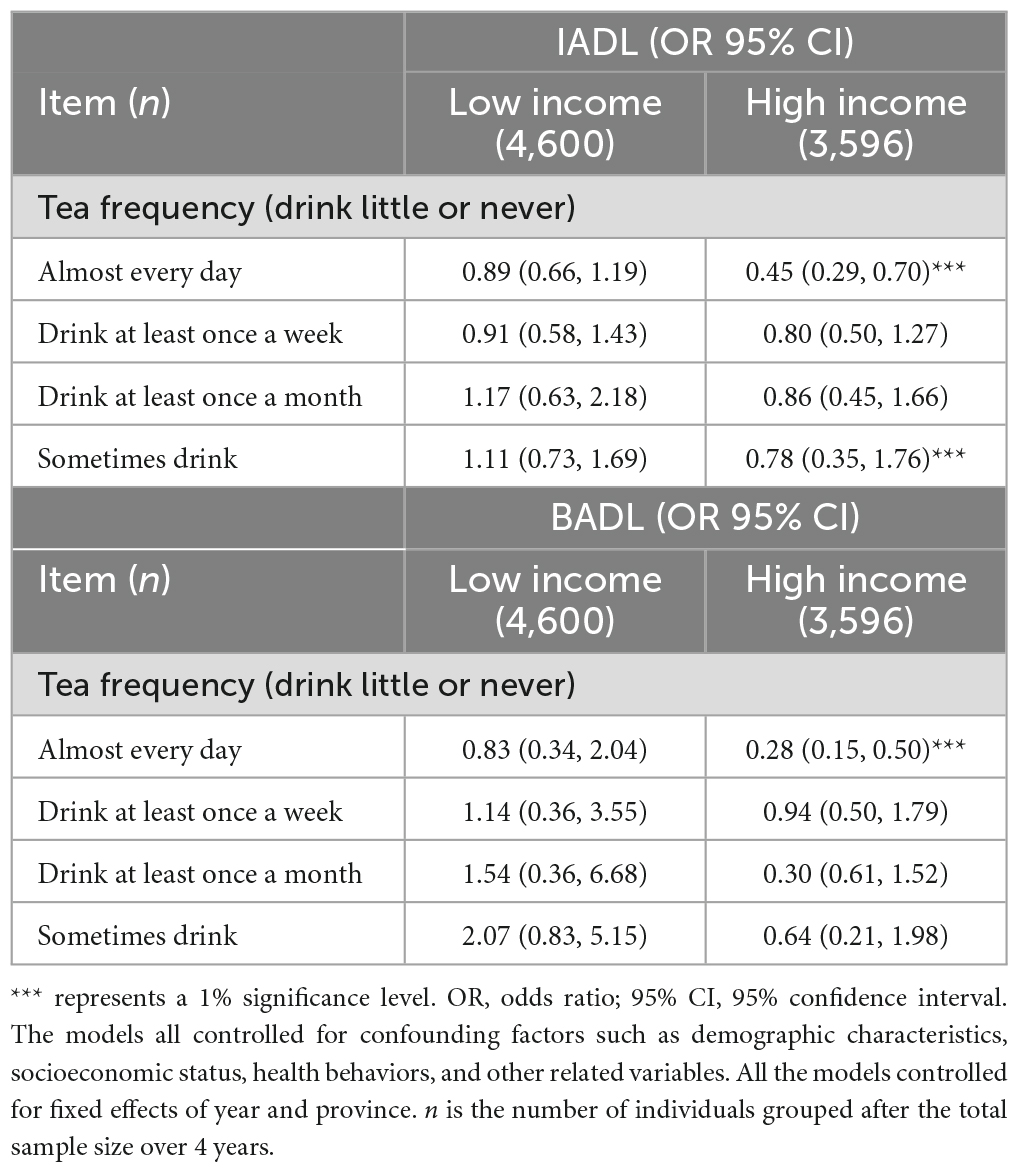
Table 4. The association between tea drinking and disability stratified by income.
4. Discussion
In this large prospective elderly cohort, we found that frequent tea drinking (almost daily) could alleviate the deterioration of daily living activities and lower risks of BADL and IADL disability, whereas occasional tea drinking did not provide protective effects. Our findings provide new evidence that frequent tea consumption could help prevent disability in the elderly.
In the context of widespread tea culture, tea drinking has always been considered as a promising non-pharmacological health strategy and has always been used to assist the management of hypertension, obesity, and diabetes (24). Tea and its components have been extensively used in functional foods and supplements to prevent and treat diverse conditions, including Parkinson’s disease (25), stroke (26), and dementia (12), among others. Certain tea types, including black tea and oolong tea, contain abundant tea polyphenols like catechins and theaflavins, conferring beneficial properties such as antioxidant, anti-inflammatory, and neuroprotective activities that positively associate with health-related quality of life in aging populations (27). White tea is abundant in xanthine glycosides, flavonoid glycosides, and methylated flavan-3-ols, exhibiting antihypertensive and antioxidant actions (28). Rodent experiments by Li et al. (29) revealed white tea extract (WTE) can modulate lipid metabolism in cultured rat adipocytes and hepatocellular carcinoma cells. Shen et al. (30) reported green tea epigallocatechin and epicatechin can stimulate bone formation by modulating osteoblast differentiation and proliferation. These catechins also suppress inflammation and bone resorption to benefit bone health. Animal studies have demonstrated various protective effects of green tea, including antioxidant, anti-inflammatory, antihypertensive, antidiabetic, and hepatoprotective activities (31–33). Sustained tea intake may positively impact physiological health (34), thereby improving quality of life (35) and promoting healthy aging. Consequently, tea drinking may play an important role in disability protection for the elderly population.
The findings of this study demonstrated protective effects of tea drinking on BADL and IADL disability and that almost daily tea drinking was associated with lower levels of disability in older people, a finding that contrasts with several previous studies. Tea contains a variety of molecular compounds, including caffeine, oxalic acid, and tannic acid. Numerous scientific studies have shown that excessive caffeine intake can lead to insomnia, anxiety, rapid heartbeat, and other harmful effects (36). Additionally, high consumption of oxalic acid may adversely impact kidney function (37). The tannic acid in tea may be associated with reduced iron absorption (38). Additionally, lack of sleep and poor kidney function can increase the risk of disability in the elderly (39, 40).
Contrary to the potential negative effects noted earlier, some research indicates that adequate and regular tea drinking may promote health benefits in the elderly population (41). Elderly individuals who regularly drink tea have better cognitive function, and regular tea drinking (at least once a week) is associated with a lower risk of cognitive impairment (22, 42). A diminished capacity for activities of daily living among older adults is associated with cognitive decline (43), which critically predicts functional impairment and disability in this population (44, 45). Elderly people with greater cognitive function encounter a lower disability risk (46), suggesting that tea drinking may reduce disability prevalence by protecting against cognitive decline.
Cognitive decline in elderly people is mainly caused by three factors: neurodegenerative diseases (47), neurotransmitter imbalances (48), and brain atrophy (49), which often have complex interactions with oxidative stress and inflammation. Tea possesses abundant bioactive constituents associated with anti-inflammatory and antioxidant mechanisms (13, 50), which are capable of conferring antioxidant, anti-inflammatory, and neuroprotective properties that may enhance cognitive health and mitigate disability risk in older populations. Tea polyphenols manifest antioxidant, anti-inflammatory, and neuroprotective qualities that help reduce oxidative damage, suppress neuroinflammation, and protect neurons from harm (51). Catechins alleviate oxidative stress and inflammation, decelerating the progression of neurodegenerative diseases (52). Caffeine inhibits brain fatty acid amide hydrolase and decreases amyloid-beta accumulation, thus reducing susceptibility to neurodegenerative conditions like Alzheimer’s disease (53). L-theanine has anxiolytic and antidepressant effects that can alleviate cognitive impairment by regulating neurotransmitters such as GABA, serotonin, and dopamine (54), partially validating the foregoing analysis.
Our stratified regression analysis showed that tea drinking was associated with higher BADL and IADL scores in those over 83 years old. This aligns with previous studies showing that frequent tea drinking is associated with better cognition in Chinese octogenarians (22) and improves cognition in Japanese people over 70 years old who consume green tea (55). Advanced age confers a risk for disability (56). Statistics indicate that the disability rate is nearly three times higher in Chinese people aged 75–84 versus 65–74, with nearly half of the over 85 s eventually developing total disability (57). Our findings suggest that tea consumption helps prevent disability in the very old. IADL represents the ability needed for social interaction activities in middle-aged and elderly people, who are more sensitive to subtle functional defects (58). Assessing IADL enables the early detection of physical and cognitive decline in elderly people, allowing timely intervention.
Economic status influences diet (59, 60). Tea consumption and associated health benefits also depend on income (61). Thus, we conducted income-stratified analyses (high vs. low), controlling for socioeconomic factors. The results revealed differing tea-disability patterns by income. Drinking tea almost every day has a protective effect against IADL and BADL disability in elderly people from high-income households, whereas no significant impact was observed in low-income elderly people. This may reflect higher stroke, dementia, and disability rates among those of a lower economic status (62, 63). Although beneficial, tea alone may be insufficient as treatment. Higher tea consumption frequency and quality among high-income elderly likely stems from health motivations, which confer preventive effects (64).
The advantage of our study is the use of a fixed effects ordered logit model to analyze panel data. This controlled for individual heterogeneity and provided more reliable association measurements than Cox models. This model also allowed us to evaluate the treatment effect of tea drinking within individuals, overcoming the limitations of previous studies that did not control for time-invariant unobserved characteristics (65–67). Furthermore, we refined the independent and dependent variables to identify the tea consumption frequency with the greatest impact on disability in the elderly and quantify the protective effects of different frequencies. Using both IADL and BADL provided comprehensive assessments of disability; IADL was more sensitive in capturing mild disability and early functional decline, helping timely discovery and intervention. Our conclusions show that only drinking tea almost every day confers protective effects against disability, rather than casual tea drinking. This study has several limitations. First, owing to the limitations of the questionnaire items, this study used the frequency of drinking tea as the independent variable, and the questionnaire did not include questions regarding the types and doses of tea intake. Future studies can explore the effects of different types of tea and tea doses on disability in elderly people. Second, although this paper selected the ADL scale as an indicator of disability level, the scoring criteria were rather rough due to the limitations of the answer types in the questionnaire.
5. Conclusion and recommendations
Tea drinking among older adults was found to help reduce the risk of increased disability levels. Regular tea drinking exerted a certain protective effect against IADL and BADL disability in the elderly population; daily drinking appeared to be the optimal frequency. The protective effects of tea drinking were more pronounced in the very old and high-income elderly. These findings may have important implications for public health efforts aimed at preventing functional capacity decline in older adults. Additional rigorous observational studies are warranted to further elucidate this relationship, accounting for tea type and potential interactive effects.
Disability can profoundly impact the quality of life and mental wellbeing of older adults and impose tremendous socioeconomic burdens (68), as disabled elderly people often require more care, healthcare, and rehabilitation services, undoubtedly increasing the economic burden on families and society (69). Given global aging trends, the number of disabled older adults continues to rise. Long-term care systems are widely deemed to be fundamental for addressing looming crises in the care of elderly people and protecting health in later life. Our findings may also provide new perspectives on developing better long-term care models.
Data availability statement
Publicly available datasets were analyzed in this study. This data can be found here: https://opendata.pku.edu.cn/dataverse/CHADS.
Ethics statement
The studies involving human participants were reviewed and approved by the Ethical Review Committee of Peking University. The patients/participants provided their written informed consent to participate in this study.
Author contributions
YM: obtained funding, conceptualized the study, assisted with statistical analysis, helped conduct the literature search and review, wrote, and revised the manuscript. YZ: conducted the literature search and review, analyzed the data, assisted with statistical analysis, wrote, and revised parts of the manuscript. DH and HZ: conducted statistical analysis, drafted the manuscript, wrote, and revised parts of the manuscript. LL: contributed to the writing of the final version of the manuscript. All authors have read and agreed to the published manuscript.
Funding
This study was one of mid-term results of the humanities and social science youth project funded by the Ministry of Education of People’s Republic of China, named “Influence Mechanism and Empirical Research of Dealers’ Pre-sales Guidance on Pesticide Use Behavior Under the Disregard of Information Inattention” (21YJC790086). This study was also funded by the Jiangsu University Philosophy and Social Science Research Project “Climate Change, Food Production and Food Security in China” (2019SJA1932); the National Natural Science Foundation of China (42177463); major Humanities and Social Sciences Research Projects in Zhejiang higher education institutions (2023QN096); and the Research Development Fund Project of Zhejiang A & F University (W20220182); and the Major Project of Philosophy and Social Science Research in Universities in Jiangsu Province (2023SJZD010).
Acknowledgments
The authors would like to acknowledge the Chinese Longitudinal Healthy Longevity Survey (CLHLS) team for providing data.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. GBD 2019 Ageing Collaborators. Global, regional, and national burden of diseases and injuries for adults 70 years and older: systematic analysis for the Global Burden of Disease 2019 Study. BMJ. (2022) 376:e068208. doi: 10.1136/bmj-2021-068208
2. Rui T. Analysis of disability status and change of elderly population in China–based on the data of the sixth and seventh national population census. Health Econ Res. (2023) 40:6–11.
3. Joyce GF, Keeler EB, Shang B, Goldman DP. The lifetime burden of chronic disease among the elderly. Health Aff. (2005) 24:R18–29. doi: 10.1377/hlthaff.w5.r18
4. Kim E, Sok SR, Won CW. Factors affecting frailty among community-dwelling older adults: a multi-group path analysis according to nutritional status. Int J Nurs Stud. (2021) 115:103850. doi: 10.1016/j.ijnurstu.2020.103850
5. Mahesh M, Abdin E, Vaingankar JA, Picco L, Jeyagurunathan A, Shafie SB, et al. Disability in Singapore’s elderly population. Ann Acad Med Singap. (2016) 45:284–96.
6. Alzheimer’s Association. 2021 Alzheimer’s disease facts and figures. Alzheimers Dement. (2021) 17:327–406. doi: 10.1002/alz.12328
7. Xiyuan H, Chao G. Effects of chronic disease, disability and dementia on mortality risk in the elderly in China: a population-based prospective cohort study. Chin J Dis Control. (2022) 26:1426–32.
8. Yuejun J, Han L, Yuan L. Quantitative prediction analysis of the number and structure of disabled elderly in China. J Demogr. (2017) 39:81–9.
9. Runlin, H, Xiaojing H, Lilong Z, Xiaoli L. The size, structure and development trend of disabled elderly population in rural China: a study based on CLHLS data and the data of the seventh national population census. Popul Res. (2023) 47:63–77.
10. Jinying W, Natural L. Age pattern of disability in the elderly and prediction of future disability population in China. J Demogr. (2020) 42:57–72.
11. Teixeira AM, Sousa C. A review on the biological activity of camellia species. Molecules. (2021) 26:2178. doi: 10.3390/molecules26082178
12. Ide K, Yamada H, Takuma N, Kawasaki Y, Harada S, Nakase J, et al. Effects of green tea consumption on cognitive dysfunction in an elderly population: a randomized placebo-controlled study. Nutr J. (2016) 15:49. doi: 10.1186/s12937-016-0168-7
13. Chiu C-J, Li M-L, Chou C-Y. Trends and biopsychosocial correlates of physical disabilities among older men and women in Taiwan: examination based on ADL, IADL, mobility, and frailty. BMC Geriatr. (2022) 22:148. doi: 10.1186/s12877-022-02838-6
14. Tao L, Liao J, Zheng R, Zhang X, Shang H. Association of drinking herbal tea with activities of daily living among elderly: a latent class analysis. Nutrients. (2023) 15:2796. doi: 10.3390/nu15122796
15. Zhang X, Chen S, Li X, Gao X, Xu Y, Cao Q. Prevalence of functional dependence in Chinese centenarians and its relationship with serum vitamin D status. J Alzheimers Dis. (2018) 64:1277–86. doi: 10.3233/JAD-180103
16. Wang J, Wei Q, Wan X. Does tea drinking promote health of older adults: evidence from the China Health and Nutrition Survey. J Prev Alzheimers Dis. (2021) 8:194–8. doi: 10.14283/jpad.2020.67
17. Du M, Tao L, Zhu L, Liu J. Association between biomass fuel use and the risk of cognitive impairment among older populations in China: a population-based cohort study. Environ Health. (2021) 20:21. doi: 10.1186/s12940-021-00706-1
18. Zeng Y, Feng Q, Hesketh T, Christensen K, Vaupel JW. Survival, disabilities in activities of daily living, and physical and cognitive functioning among the oldest-old in China: a cohort study. Lancet. (2017) 389:1619–29. doi: 10.1016/S0140-6736(17)30548-2
19. He C, Yan L, Xiaolan W, Xiaochun QA. A comparative study on the level of disability in the elderly in China–based on four national survey data. South Popul. (2021) 36:1–12.
20. Min C, Yaoguang Z, Xueqin X, Shiyong W. Analysis of disability and influencing factors of elderly people aged 60 and above in China. China Hosp Stat. (2021) 28:389–94.
21. Roehrig B, Hoeffken K, Pientka L, Wedding U. How many and which items of Activities of Daily Living (ADL) and Instrumental Activities of Daily Living (IADL) are necessary for screening. Crit Rev Oncol Hematol. (2007) 62:164–71. doi: 10.1016/j.critrevonc.2006.12.002
22. Feng L, Li J, Ng TP, Lee TS, Kua EH, Zeng Y. Tea drinking and cognitive function in oldest-old Chinese. J Nutr Health Aging. (2012) 16:754–8. doi: 10.1007/s12603-012-0077-1
23. Gu YJ, He CH, Li S, Zhang SY, Duan SY, Sun HP, et al. Tea consumption is associated with cognitive impairment in older Chinese adults. Aging Ment Health. (2018) 22:1232–8. doi: 10.1080/13607863.2017.1339779
24. Dong XX, Wang RR, Liu JY, Ma QH, Pan CW. Habitual tea consumption and 5-year incident metabolic syndrome among older adults: a community-based cohort study. BMC Geriatr. (2021) 21:728. doi: 10.1186/s12877-021-02707-8
25. Li X, Yu C, Guo Y, Bian Z, Si J, Yang L, et al. Tea consumption and risk of ischaemic heart disease. Heart. (2017) 103:783–9. doi: 10.1136/heartjnl-2016-310462
26. Zhao LG, Li HL, Sun JW, Yang Y, Zheng W, Xiang YB. Green tea consumption and cause-specific mortality: results from two prospective cohort studies in China. J Epidemiol. (2017) 27:36–41. doi: 10.1016/j.je.2016.08.004
27. Pan C, Ma Q, Sun HP, Xu Y, Luo N, Wang P. Tea consumption and health-related quality of life in elderly adults. J Nutr Health Aging. (2017) 21:480–6. doi: 10.1007/s12603-016-0784-0
28. Hajiaghaalipour F, Kanthimathi MS, Sanusi J, Rajarajeswaran J. White tea (Camellia sinensis) inhibits proliferation of the colon cancer cell line, HT-29, activates caspases and protects DNA of normal cells against oxidative damage. Food Chem. (2015) 166:561–70. doi: 10.1016/j.foodchem.2014.07.009
29. Li N, Zhou X, Wang J, Chen J, Lu Y, Sun Y, et al. White tea alleviates non-alcoholic fatty liver disease by regulating energy expenditure and lipid metabolism. Gene. (2022) 805:146553. doi: 10.1016/j.gene.2021.146553
30. Shen CL, Yeh JK, Cao JJ, Wang JS. Green tea and bone health: evidence from laboratory studies. Food Res Int. (2011) 44:1002–9. doi: 10.1016/j.foodres.2010.11.036
31. Zhang X, Zhou X, Wang J, Chen J. Preventive efficiency of green tea and its components on nonalcoholic fatty liver disease. J Nutr. (2019) 18:46. doi: 10.1186/s12937-019-0448-7
32. Xing L, Zhang H, Qi R, Tsao R, Mine Y. Recent advances in the understanding of the health benefits and molecular mechanisms associated with green tea polyphenols. J Agric Food Chem. (2019) 67:1029–43. doi: 10.1021/acs.jafc.8b06146
33. Sasaki GY, Chen C, O’Sullivan J, Heinrichs A, Liu C, Wang J-S. Green tea extract treatment in obese mice with nonalcoholic steatohepatitis restores the hepatic metabolome in association with limiting endotoxemia-TLR4-NFκB-mediated inflammation. Mol Nutr Food Res. (2019) 63:e1900811. doi: 10.1002/mnfr.201900811
34. Shang A, Li J, Zhou DD, Gan RY, Li HB. Molecular mechanisms underlying health benefits of tea compounds. Free Radic Biol Med. (2021) 172:181–200. doi: 10.1016/j.freeradbiomed.2021.06.006
35. Shi Z, Zhang T, Byles J, Martin S, Avery JC, Taylor AW. Food habits, lifestyle factors and mortality among oldest old chinese: the Chinese Longitudinal Healthy Longevity Survey (CLHLS). Nutrients. (2015) 7:7562–79. doi: 10.3390/nu7095353
36. Temple JL, Bernard C, Lipshultz SE, Czachor JD, Westphal JA, Mestre MA. The safety of ingested caffeine: a comprehensive review. Front Psychiatry. (2017) 8:80. doi: 10.3389/fpsyt.2017.00080
37. Hesse A, Siener R. Current aspects of epidemiology and nutrition in urinary stone disease. World J Urol. (1997) 15:165–71. doi: 10.1007/BF02201853
38. Zijp IM, Korver O, Tijburg LB. Effect of tea and other dietary factors on iron absorption. Crit Rev Food Sci Nutr. (2000) 40:371–98. doi: 10.1080/10408690091189194
39. Foley D, Ancoli-Israel S, Britz P, Walsh J. Sleep disturbances and chronic disease in older adults: results of the 2003 National Sleep Foundation Sleep in America Survey. J Psychosom Res. (2004) 56:497–502. doi: 10.1016/jjpsychores.2004.02.010
40. Boltz M, Kuzmik A, Resnick B, Trotta R, Mogle J, BeLue R, et al. Reducing disability via a family centered intervention for acutely ill persons with Alzheimer’s disease and related dementias: protocol of a cluster-randomized controlled trial (Fam-FFC study). Trials. (2018) 19:496. doi: 10.1186/s13063-018-2875-1
41. Hodge A, Almeida OP, English DR, Giles GG, Flicker L. Patterns of dietary intake and psychological distress in older Australians: benefits not just from a Mediterranean diet. Int Psychogeriatr. (2013) 25:456–66. doi: 10.1017/S1041610212001986
42. Feng L, Gwee X, Kua EH, Ng TP. Cognitive function and tea consumption in community dwelling older Chinese in Singapore. J Nutr Health Aging. (2010) 14:433–8.
43. Xi J, Yang Y, Xie M. Correlation between cognitive function and daily living ability of elderly people in nursing institutions. Chin J Gerontol. (2019) 39:2010–2.
44. Yaffe K, Falvey C, Harris TB, Newman A, Satterfield S, Koster A, et al. Effect of socioeconomic disparities on incidence of dementia among biracial older adults: prospective study. BMJ. (2013) 347:f7051. doi: 10.1136/bmj.f7051
45. Liu-Seifert H, Siemers E, Sundell K, Cummings J, Raskin J, Mohs R. Cognitive and functional decline and their relationship in patients with mild Alzheimer’s dementia. J Alzheimers Dis. (2015) 43:949–55. doi: 10.3233/JAD-140792
46. Ngandu T, Lehtisalo J, Solomon A, Levälahti E, Ahtiluoto S, Bäckman L, et al. A 2 year multidomain intervention of diet, exercise, cognitive training, and vascular risk monitoring versus control to prevent cognitive decline in at-risk elderly people (FINGER): a randomised controlled trial. Lancet. (2015) 385:2255–63. doi: 10.1016/S0140-6736(15)60461-5
47. Winblad B, Amouyel P, Andrieu S, Ballard C, Brayne C, Brodaty H, et al. Defeating Alzheimer’s disease and other dementias: a priority for European science and society. Lancet Neurol. (2016) 15:455–532. doi: 10.1016/S1474-4422(16)00062-4
48. Liu AK, Chang RC, Pearce RK, Gentleman SM. Nucleus basalis of meynert revisited: anatomy, history and differential involvement in Alzheimer’s and Parkinson’s disease. Acta Neuropathol. (2015) 129:527–40. doi: 10.1007/s00401-015-1392-5
49. Romero JE, Coupe P, Lanuza E, Catheline G, Manjón JV. Toward a unified analysis of cerebellum maturation and aging across the entire lifespan: a MRI analysis. Hum Brain Mapp. (2021) 42:1287–303. doi: 10.1002/hbm.25293
50. Li H, Ding F, Xiao L, Shi R, Wang H, Han W, et al. Food-derived antioxidant polysaccharides and their pharmacological potential in neurodegenerative diseases. Nutrients. (2017) 9:778. doi: 10.3390/nu9070778
51. Mancini E, Beglinger C, Drewe J, Zanchi D, Lang UE, Borgwardt S. Green tea effects on cognition, mood and human brain function: a systematic review. Phytomedicine. (2017) 34:26–37. doi: 10.1016/j.phymed.2017.07.008
52. Wang Y, Wang B, Du F, Su X, Sun G, Zhou G, et al. Epigallocatechin-3-gallate attenuates oxidative stress and inflammation in obstructive nephropathy via NF-κB and Nrf2/HO-1 signalling pathway regulation. Basic Clin Pharmacol Toxicol. (2015) 117:164–72. doi: 10.1111/bcpt.12383
53. Kim YS, Kwak SM, Myung SK. Caffeine intake from coffee or tea and cognitive disorders: a meta-analysis of observational studies. Neuroepidemiology. (2015) 44:51–63. doi: 10.1159/000371710
54. Li Y, Wang Y, Li X, Zhang Z. EGCG ameliorates the reduction of TH-positive neuron number in the locus coeruleus of stressed mice. J Neural Transm. (2019) 126:1485–94. doi: 10.1007/s00702-019-02065-6
55. Kuriyama S, Hozawa A, Ohmori K, Shimazu T, Nagatomi R, Arai H, et al. Green tea consumption and cognitive function: a cross-sectional study from the Tsurugaya Project 1. Am J Clin Nutr. (2006) 83:355–61. doi: 10.1093/ajcn/83.2.355
56. Yuan WP, Xue Y, Cai Y, Juan Y. Investigation on the prevalence and self-care ability of multiple chronic diseases in the elderly. Mod Prev Med. (2021) 48: 2590–3.
57. Zhang W, Fu M. Disability risk and care time of the elderly in long-term care insurance system—An analysis based on Barthel index. Insur Res. (2020) 385:80–93.
58. Lawton MP, Brody EM. Assessment of older people: self-maintaining and instrumental activities of daily living. Gerontologist. (1969) 9:179–86.
59. Vieux F, Maillot M, Rehm CD, Drewnowski A. Tea consumption patterns in relation to diet quality among children and adults in the United States: analyses of NHANES 2011–2016 data. Nutrients. (2019) 11:2635. doi: 10.3390/nu11112635
60. Yao Y, Chen H, Chen L, Ju S-Y, Yang H, Zeng Y, et al. Type of tea consumption and depressive symptoms in Chinese older adults: a longitudinal analysis. BMC Geriatr. (2021) 21:331. doi: 10.1186/s12877-021-02203-z
61. French S, Shimotsu S, Wall M, Gerlach A. Capturing the spectrum of household food and beverage purchasing behavior: a review. J Am Diet Assoc. (2008) 108:2051–8. doi: 10.1016/j.jada.2008.09.001
62. Yu S, Qian L, Ma J. The influence of gender and wealth inequality on Alzheimer’s disease among the elderly: a global study. Heliyon. (2023) 9:e14677. doi: 10.1016/j.heliyon.2023.e14677
63. Huang X, Zhang M, Fang J. Growth patterns of activity of daily living disability and associated factors among the Chinese elderly: a twelve-year longitudinal study. Arch Gerontol Geriatr. (2022) 99:104599. doi: 10.1016/j.archger.2021.104599
64. Villaño D, Pecorari M, Testa MF, Raguzzini A, Stalmach A, Crozier A, et al. Unfermented and fermented rooibos teas (Aspalathus linearis) increase plasma total antioxidant capacity in healthy humans. Food Chem. (2015) 168:366–71. doi: 10.1016/j.foodchem.2010.05.032
65. Therneau TM, Grambsch PM. Modeling Survival Data: Extending the Cox Model. New York, NY: Springer (2000). doi: 10.1007/978-1-4757-3294-8
66. Zheng J, Zhou R, Li F, Chen L, Wu K, Huang J, et al. Association between dietary diversity and cognitive impairment among the oldest-old: findings from a nationwide cohort study. Clin Nutr. (2021) 40:1452–62. doi: 10.1016/j.clnu.2021.02.041
68. Chatterji S, Byles J, Cutler D, Seeman T, Verdes E. Health, functioning, and disability in older adults–present status and future implications. Lancet. (2015) 385:563–75. doi: 10.1016/S0140-6736(14)61462-8
Keywords: tea drinking, disability levels, elderly, IADL, BADL
Citation: Ma Y, Zhu Y, Hong D, Zhao H and Li L (2023) Association between tea drinking and disability levels in older Chinese adults: a longitudinal analysis. Front. Nutr. 10:1233664. doi: 10.3389/fnut.2023.1233664
Received: 02 June 2023; Accepted: 12 October 2023;
Published: 31 October 2023.
Edited by:
Enbo Ma, Fukushima Medical University, JapanReviewed by:
Shi-Hui Cheng, University of Nottingham Malaysia Campus, MalaysiaVenkataraghavan Ramamoorthy, Baptist Health South Florida, United States
Copyright © 2023 Ma, Zhu, Hong, Zhao and Li. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lei Li, bGlsZWljZW1AemFmdS5lZHUuY24=