 Mariana De Santis Filgueiras
Mariana De Santis Filgueiras Mariane Alves Silva
Mariane Alves Silva Lara Gomes Suhett
Lara Gomes Suhett
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
EDITORIAL article
Front. Nutr., 19 June 2023
Sec. Nutrition and Metabolism
Volume 10 - 2023 | https://doi.org/10.3389/fnut.2023.1229753
This article is part of the Research TopicNutrition, Bone Health, and Cardiometabolic Risk in ChildhoodView all 5 articles
Editorial on the Research Topic
Nutrition, bone health, and cardiometabolic risk in childhood
The prevalence of overweight and obesity in young people is rapidly increasing worldwide. It is estimated that there will be about 206 million children and adolescents aged 5–19 years with obesity in 2025 and 254 million in 2030 (1). This increase has been associated with physical inactivity and poorer diet quality (2) which may also contribute to adverse bone outcomes in pediatric people (3). In this context, childhood obesity has been described as a cardiometabolic risk factor of great magnitude in public health, with negative implications for children's bone health (4). Figure 1 summarizes the relationships between nutrition, bone health, and cardiometabolic risk in children and adolescents.
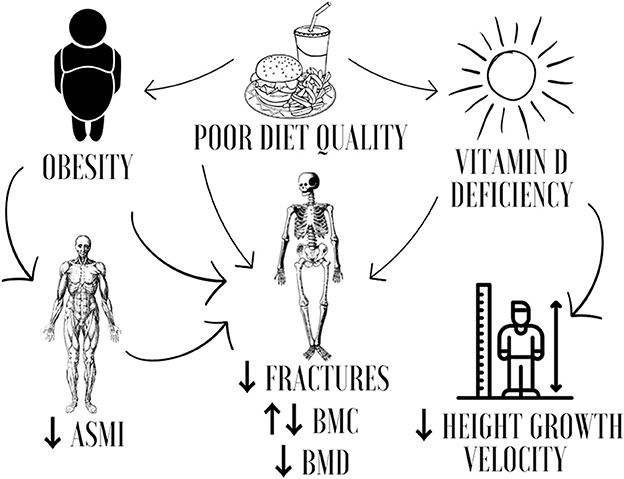
Figure 1. Nutrition, bone health, and cardiometabolic risk in childhood. ASMI, appendicular skeletal muscle mass index; BMC, bone mineral content; BMD, bone mineral density.
Frontiers in Nutrition published four articles that evaluated the association between bone mineral content (BMC) and obesity (n = 2); vitamin D supplementation and overweight (n = 1); and vitamin D levels, height growth velocity, and bone mineral density (BMD) (n = 1) in children and adolescents. The studies were randomized controlled trials (n = 2), cohorts (n = 1), and cross-sectional design (n = 1).
The relationship between overweight/obesity and bone health in children and adolescents may be attributed to change in BMC. Studies have shown that obese children had higher BMC compared to non-obese children [(5); Liang et al.]. On the other hand, Cristi-Montero et al. identified the mediating role of the appendicular skeletal muscle mass index (ASMI) in the inverse association between body fat and BMC in Chilean adolescents. This mediation was slightly higher in girls and adolescents with normal weight. Muscle tissue appears to play a role in preventing excess body fat and impaired bone health (6).
As well as for the BMC, evidence on the occurrence of fractures is contradictory. Liang et al. showed that childhood obesity was associated with a reduced risk of fractures in adulthood, while other studies indicated that overweight/obesity was associated with a higher prevalence of fractures, suggesting worse bone quality in children (7, 8). This may be a result of the greater mechanical load on the bone structure of people with obesity (9) and the imbalance in the secretion of leptin and adiponectin by bone marrow adipocytes, contributing to an increase in osteoblasts (10).
In addition to the changes in the BMC, the relationship between overweight/obesity and bone health may be attributed to vitamin D deficiency, since its prevalence is higher in people with obesity (11). However, overweight may influence the response to vitamin D supplementation in people with a genetic predisposition to lower serum levels of the vitamin D (12, 13). Asghari et al. investigated the influence of the rs2282679 polymorphism on the response of overweight and obese schoolchildren to vitamin D supplementation and identified that there was no interaction between genotype, supplementation, and vitamin D levels after the intervention. The researchers believe that obesity may nullify the association between genetic predisposition and response to vitamin D supplementation.
The vitamin D deficiency is linked to pediatric rickets, which may be directly related to child height growth. In this sense, Xiao et al., when conducting a prospective cohort of 10,450 Chinese children, displayed a non-linear and inverse L-shaped association between serum 25-hydroxy vitamin D [25(OH)D)] concentration and height growth velocity, leveling off to 40–60 nmol/L. Although some previous studies did not show an association between vitamin D and height growth (14, 15), we emphasize that the study by Xiao et al. is prospective, population-based, and with a large sample size. In addition, the investigations have divergences in the form of assessment of height growth, classification of vitamin D levels, and adjustment variables in statistical analyses.
Additionally, Xiao et al. showed that vitamin D sufficiency was associated with a reduced risk of low BMD in children; however, this result was not found among those with overweight and obesity. The authors attributed this difference according to weight status to decreased bioavailability of vitamin D in people with excess body fat, and to increased metabolic clearance of vitamin D due to increased absorption by adipose tissue.
Even though the articles included in this topic did not evaluate the relationship between diet and bone health in pediatric people, it is important to holistically understand the role of diet quality on bone health using different approaches such as dietary patterns, scores, and indices (3). A recent systematic review gathered the available evidence on the association between diet quality and bone health markers in young people. The authors concluded that healthy dietary patterns exert synergistic positive effects on markers of bone health (BMC and BMD), while poor diet quality negatively impacted the bone health in children and adolescents. Additionally, they highlighted that longitudinal research using a specific tool to assess diet quality in relation to bone health is required and further studies should include bone-regulating hormones and markers of bone turnover in the analysis (3).
Diet is an important modifiable risk factor for chronic diseases, such as obesity (16), and childhood is a crucial phase for the formation of healthy eating habits (17), as well as for the adequate bone mineralization (18). Therefore, investigate the role of diet quality on bone health in the beginning of life can guide actions to prevent bone diseases and their comorbidities in the future.
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
As editors of this Research Topic named Nutrition, Bone Health, and Cardiometabolic Risk in Childhood, were thank all authors and reviewers for their valuable contributions. We are also grateful for Frontiers in Nutrition for the opportunity to write the topic and continuous support.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
2. Mahumud RA, Sahle BW, Owusu-Addo E, Chen W, Morton RL, Renzaho AMN. Association of dietary intake, physical activity, and sedentary behaviours with overweight and obesity among 282,213 adolescents in 89 low and middle income to high-income countries. Int J Obes. (2021) 45:2404–18. doi: 10.1038/s41366-021-00908-0
3. Suhett LG, Filgueiras MS, Novaes JF, Sukumar D. Role of diet quality in bone health in children and adolescents: a systematic review. Nutr Rev. (2023) nuad036. doi: 10.1093/nutrit/nuad036. [Epub ahead of print].
4. Fintini D, Cianfarani S, Cofini M, Andreoletti A, Ubertini GM, Cappa M, et al. The bones of children with obesity. Front Endocrinol. (2020) 11:200. doi: 10.3389/fendo.2020.00200
5. Van Leeuwen J, Koes BW, Paulis WD, van Middelkoop M. Differences in bone mineral density between normal-weight children and children with overweight and obesity: a systematic review and meta-analysis. Obesity Rev. (2017) 18:526–46. doi: 10.1111/obr.12515
6. Kirk B, Feehan J, Lombardi G, Duque G. Muscle, bone, and fat crosstalk: the biological role of myokines, osteokines, and adipokines. Curr Osteoporos Rep. (2020) 18:388–400. doi: 10.1007/s11914-020-00599-y
7. Fornari ED, Suszter M, Roocroft J, Bastrom T, Edmonds EW, Schlechter J. Childhood obesity as a risk factor for lateral condyle fractures over supracondylar humerus fractures. Clin Orthopaed Related Res. (2013) 471:1193–8. doi: 10.1007/s11999-012-2566-2
8. Kessler J, Koebnick C, Smith N, Adams A. Childhood obesity is associated with increased risk of most lower extremity fractures. Clin Orthopaed Relat Res. (2013) 471:1199–207. doi: 10.1007/s11999-012-2621-z
9. Horowitz MC, Berry R, Holtrup B, Sebo Z, Nelson T, Fretz JA, et al. Bone marrow adipocytes. Adipocyte. (2017) 6:193–204. doi: 10.1080/21623945.2017.1367881
10. Pollock NK. Childhood obesity, bone development, and cardiometabolic risk factors. Mol Cell Endocrinol. (2015) 410:52–63. doi: 10.1016/j.mce.2015.03.016
11. Pereira-Santos M, Costa PR, Assis AM, Santos CA, Santos DB. Obesity and vitamin D deficiency: a systematic review and meta-analysis. Obes Rev. (2015) 16:341–9. doi: 10.1111/obr.12239
12. Aguirre Castaneda R, Nader N, Weaver A, Singh R, Kumar S. Response to vitamin D3 supplementation in obese and non-obese Caucasian adolescents. Horm Res Paediatr. (2012) 78:226–31. doi: 10.1159/000343446
13. Krasniqi E, Boshnjaku A, Wagner KH, Wessner B. Association between polymorphisms in Vitamin D pathway-related genes, vitamin D status, muscle mass and function: a systematic review. Nutrients. (2021) 13:3109. doi: 10.3390/nu13093109
14. Huey SL, Acharya N, Silver A, Sheni R, Yu EA, Peña-Rosas JP, et al. Effects of oral vitamin D supplementation on linear growth and other health outcomes among children under five years of age. Cochrane Database Syst Rev. (2020) 12:CD012875. doi: 10.1002/14651858.CD012875.pub2
15. Chowdhury R, Taneja S, Kvestad I, Hysing M, Bhandari N, Strand TA. Vitamin D status in early childhood is not associated with cognitive development and linear growth at 6-9 years of age in North Indian children: a cohort study. Nutr J. (2020) 19:14. doi: 10.1186/s12937-020-00530-2
16. World Health Organization. Diet, Nutrition, and the Prevention of Chronic Diseases: Report of a Joint WHO/FAO Expert Consultation. WHO Technical Report Series 916. Geneva: World Health Organization (2002). 149 p.
17. Issanchou S, Habeat Consortium. Determining factors and critical periods in the formation of eating habits: results from the Habeat Project. Ann Nutr Metab. (2017) 70:251–6. doi: 10.1159/000471514
Keywords: diet, child, adolescent, bone, obesity, vitamin D
Citation: Filgueiras MS, Silva MA and Suhett LG (2023) Editorial: Nutrition, bone health, and cardiometabolic risk in childhood. Front. Nutr. 10:1229753. doi: 10.3389/fnut.2023.1229753
Received: 26 May 2023; Accepted: 08 June 2023;
Published: 19 June 2023.
Edited and reviewed by: Ellen E. Blaak, Maastricht University, Netherlands
Copyright © 2023 Filgueiras, Silva and Suhett. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mariana De Santis Filgueiras, bWRzZmlsZ3VlaXJhc0BnbWFpbC5jb20=
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.