 Michael Klowak
Michael Klowak Andrea K. Boggild
Andrea K. Boggild
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
METHODS article
Front. Nutr., 04 July 2023
Sec. Nutrition and Metabolism
Volume 10 - 2023 | https://doi.org/10.3389/fnut.2023.1196470
This article is part of the Research TopicFood as MedicineView all 24 articles
Introduction: Despite effective treatment of leprosy via WHO-approved multi-drug therapy (MDT), patients still suffer from debilitating neuropathic sequelae, including peripheral neuropathic pain (PNP), and continue to develop intercurrent etiologies (such as diabetes), and progressive existing neuropathy over time. Strategies seeking to improve physiological and metabolic wellness, including those that reduce systemic inflammation and enhance immune responsiveness to neurotoxic factors may influence underlying neuropathic etiologies. A whole food plant-based diet (WFPBD) has been shown to be effective in the management of neuropathic pain due to diabetes, limiting severity and relevant symptomology. Diabetes remains a significant sequela of leprosy, as up to 50% of patients in reaction requiring corticosteroids, may develop a biochemical diabetes. As nutritional interventions may modulate both leprosy and diabetes, a specific exploration of these relationships remains relevant.
Objectives: (1) To demonstrate the effect of a WFPBD lifestyle intervention, on neuropathic pain variables in leprosy; and (2) To contextualize the significance of diet in the treatment of chronic sequelae in leprosy by evaluating tolerability and side effect profile.
Methods: A prospective, randomized, controlled, single-blind, multicentre interventional trial is described. Weekly one-hour dietary counseling sessions promoting a WFPBD emphasizing vegetables, fruits, whole-grains, nuts, and legumes, omitting animal products, and limiting fat intake over a six-month duration will be implemented. Participants will be 70 age and sex-matched individuals experiencing active or treated “cured” leprosy and PNP, randomized to either intervention or control groups. Primary outcome measures include efficacy via visual analog scale, subjective questionnaire and objective quantitative sensory testing, as well as safety, tolerability, and harms of a WFPBD on PNP in leprosy. This study will be initiated after Research Ethics Board (REB) approval at all participating sites, and in advance of study initiation, the trial will be registered at ClinicalTrials.gov.
Expected impact: It is hypothesized that WFPBDs will mitigate progression and severity of PNP and potentially reduce the adverse events related to standard corticosteroid treatment of leprosy reactions, thereby reducing disease severity. By examining the effects of WFPBDs on PNP in leprosy, we hope to illuminate data that will lead to the enhanced therapeutic management of this neglected tropical disease.
Leprosy continues to affect nearly 200,000 individuals globally, despite being eliminated as a public health concern by the World Health Organization in 2000 (1). Causative agents, Mycobacterium leprae and Mycobacterium lepromatosis, prevail in low-middle income countries where many barriers to treatment adherence and effective prevention of neuropathic sequelae continue to challenge the clinical management of leprosy (1, 2). Patients experience hypopigmented and inflammatory cutaneous lesions, disabling sensory and motor neuropathies, and debilitating neuropathic pain, often leading to stigma and social ostracization (2–6). Despite the development of effective therapeutics via multidrug therapy (MDT), nerve release surgery, and other immunosuppressives decades ago, treatment of the associated neuropathic pain continues to remain largely ineffective. Standard pharmacological treatment of PNP using antidepressants, anticonvulsants, and opioids, results in a less than 30% reduction of pain (1, 7). Additionally, a significant side effect profile including anticholinergic effects, dizziness, confusion, hypertension, and weight fluctuation, contribute to poor adherence to PNP treatment overall (8). Given these extensive barriers, patients with leprosy sequelae, including PNP, continue to experience a reduced quality of life even with adequate access to gold standard therapeutics (6, 9, 10). In the absence of effective pharmaceuticals, alternative interventions must be explored to bolster patients’ control of leprosy sequelae and the associated morbidity.
Lifestyle interventions have recently emerged as accessible and cost-effective strategies to reduce the burden and severity of neuropathic pain in diabetes. Strategies seeking to improve physiological and metabolic wellness, including those that reduce inflammation and enhance immune responsiveness to neurotoxic factors may influence underlying neuropathic etiologies. Nutrient supplementation has been instrumental in reducing host oxidative stress, strengthening the immune system, and mitigating potential adverse events in both leprosy and diabetes (11–15). Specifically, oral vitamin E and zinc supplementation may confer antioxidant effects, reducing daily analgesic requirements, and decreasing the incidence of leprosy symptoms overall (14, 16, 17). Likewise, studies assessing the use of oral vitamin D3 and omega-3 supplementation in diabetes have shown statistically significant improvements on subjective tests of neuropathy and pain, as well as objective tests of nerve health (11–15). Dietary interventions have also been specifically shown to reduce overall symptomology and improve the quality of life of individuals suffering from PNP due to diabetes (18–22). Many leprosy patients will develop impaired glucose tolerance due to genetic and lifestyle factors alone, and also due to the reliance on corticosteroids for control of inflammatory leprosy reactions (which can occur before, during, and after effective MDT). As patients experiencing leprosy often endure a biochemically induced diabetes, similar rationale may be applied. Prior to a final diagnosis of leprosy, patients are statistically significantly more likely to have diabetes (up to 14.2%) or pre-diabetes (up to 50%), when compared to healthy controls. Likewise, up to 65% of patients require corticosteroid treatment following reactions, resulting in steroid-induced hyperglycemia in up to 47% of individuals who were previously glucose tolerant (23–28). Additionally, given the high population prevalence of diabetes, lifestyle and genetic factors may predispose those with leprosy to diabetic neuropathy independent of corticosteroid use.
A WFPBD emphasizing vegetables, fruits, grains, and legumes, while omitting animal products, and limiting saturated fat intake has recently been shown to reduce diabetes related PNP severity and symptomology (19, 21, 22, 29, 30). In a cohort study assessing a WFPBD in 21 participants with type 2 diabetes, a statistically significant reduction of both serum triglycerides and total cholesterol, alongside a noticeable decrease in pain, weight, and insulin requirements was reported (22). Likewise, data from over 110 observational and clinical trials suggest that dietary patterns similar to a WFPBD are associated with a decreased presence of diabetes and significant improvements in biochemical profiles, including total LDL, and therapeutic requirements, for insulin in particular (21). Finally, a comprehensive randomized control trial seeking to address neuropathic pain management in 34 participants with neuropathy due to diabetes corroborates previous findings. Using both subjective questionnaire and objective quantitative sensory testing (QST), and electrophysiology, a significant decline in weight, body mass index (BMI), and glycemia was observed alongside a statistically significant improvement in neuropathic pain (19). Overall, WFPBDs have proven to be effective in the management of neuropathy due to diabetes, limiting endoneural ischemia, and providing sufficient glycemic control and lipid management, which when uncontrolled seem to exacerbate neuropathic pain. As a result, this phenomenon may translate to the management of PNP in leprosy, where diabetes comorbidity is common, and research has shown that diet and lifestyle interventions may be sufficient to control such steroid-induced hyperglycemia (23–28, 30–32). A WFPBD may also provide enhanced nutritional and antioxidant intake, conferring neuro-protective effects against leprosy alone while patients are actively undergoing antimicrobial MDT.
Major dietician groups suggest that a WFPBD is efficacious and superior in most, if not all populations. Dieticians of Canada, the British Dietetic Association, and the American Academy of Nutrition and Dietetics promote WFPBDs, suggesting improvements in weight, cholesterol, and risk of cardiovascular disease and type 2 diabetes (33–35). These groups also endorse that a WFPBD meets or exceeds recommended lipid, vitamin, mineral, fiber, protein, and amino acid requirements, when sufficient caloric intake is achieved (33–35). The wholegrains, nuts, seeds, beans, and fruits and vegetables readily supplied by a WFPBD can maximize intake of thiamine, pyridoxine, cobalamin, omega-3, zinc, and vitamins A, C, and E which are crucial to neurotransmitter and myelin synthesis, action potential propagation, and neuroprotection via capturing free radicals, and reducing oxidative stress (36–39).
We hypothesize that a WFPBD will have a multipronged beneficial effect, providing sufficient nutrient intake, neuro-protective benefits, and glycemic control to enhance host control of leprosy sequelae. A comprehensive prospective, randomized, controlled, single-blind, multicentre trial examining the efficacy, safety, and tolerability of a whole food plant-based diet on PNP in leprosy will inform any association between nutritional interventions and disease severity at the population level. Through reliable and validated techniques, such as comprehensive questionnaires and objective QST, a robust data set and analysis is expected to be generated. Overall, it is hypothesized that WFPBDs will mitigate progression of PNP as well as adverse events related to standard corticosteroid treatment of reactions, resulting in decreased neuropathic pain severity. By evaluating our current knowledge regarding the effects of WFPBDs on neuropathic pain in leprosy, we hope to illuminate data that will lead to enhanced therapeutic management and control of the impact of this neglected tropical disease.
This is a prospective, randomized, controlled, single-blind, multicentre trial examining the efficacy, safety, and tolerability of a WFPBD versus standard diet within a population living with PNP due to leprosy. An analytic framework capturing the target population, intervention, comparator, intermediate and ultimate outcomes to be assessed, as well as the impacts and considerations underpinning such a trial is presented in Figure 1.

Figure 1. Analytic framework. BMI, body mass index; BMR, basal metabolic rate; BP, blood pressure; CAD, coronary artery disease; DALY, disability-adjusted life year; DM2, Type 2 diabetes mellitus; HR, heart rate; HTN, hypertension; LFTs, liver function tests; MCV, mean corpuscular volume; WFPBD, whole foods plant-based diet.
The overall objective of this study is to demonstrate the effect of a dietary lifestyle intervention, specifically a WFPBD, on neuropathic pain variables in leprosy. It is hypothesized that patients may demonstrate a statistically significant improvement in sensory and motor neuropathy, as well as pain, on comprehensive questionnaires and objective QST and muscle testing both within and between groups at study end. Secondary objectives include contextualizing the significance of diet in the treatment of chronic leprosy sequelae by demonstrating high tolerability and a limited side effect profile alongside aforementioned improvements in neuropathic pain. It is hypothesized that a WFPBD has the potential to serve as a low-risk, low-cost, low-tech intervention for chronic neuropathic pain, improving function and reducing overall morbidity of leprosy.
Participants will be enrolled at the Tropical Disease Unit (TDU) in Toronto, Ontario, Canada, and one or more partner tropical medicine institutes, and will include patients experiencing active, or treated “cured” leprosy, as well as any degree of PNP. Inclusion into the trial requires: (1) clinically compatible leprosy based on the presence of thickened peripheral nerves (on physical exam, as well as ultrasound), and hypo- or anesthetic skin lesions; and/or (2) laboratory confirmed leprosy via positive slit skin smears and/or consistent histopathology and/or the presence of acid-fast bacilli on histopathology; and/or (3) a clinically compatible presence of neuropathy on physical exam including but not limited to glove and stocking paresthesia, abnormal touch perception sensations, and subjective pain (40–42) (Table 1). Sensory perception will be evaluated using 0.2–0.6 g Semmes-Weinstein monofilament, and the presence of 2/3 insensate sites will be considered “abnormal” (43). The use of objective QST as a standalone test for inclusion will be dependent on enrolment frequency to better preserve trial specificity. In the event of inadequate enrolment, a negative QST will not exclude patients from the trial to ensure adequate sensitivity, and vice versa. QST unreliably detects small fiber neuropathy, potentially representing a large portion of the target population (44, 45). Therefore, it is unlikely that it will remain a standalone inclusion criterion, however, will still be collected for downstream analysis. Finally, prospective participants who are pregnant, <18 years of age, already following a WFPBD (including vegetarian and vegan diets), and those experiencing neuropathy due to other significant causes alone, will be excluded (Table 1). Leprosy patients who fulfill inclusion criteria experiencing a biochemical diabetes due to corticosteroid therapy will remain eligible for inclusion and will be considered in downstream analysis (23–28). No restriction on language will be implemented as translation services will be made available across study centres.
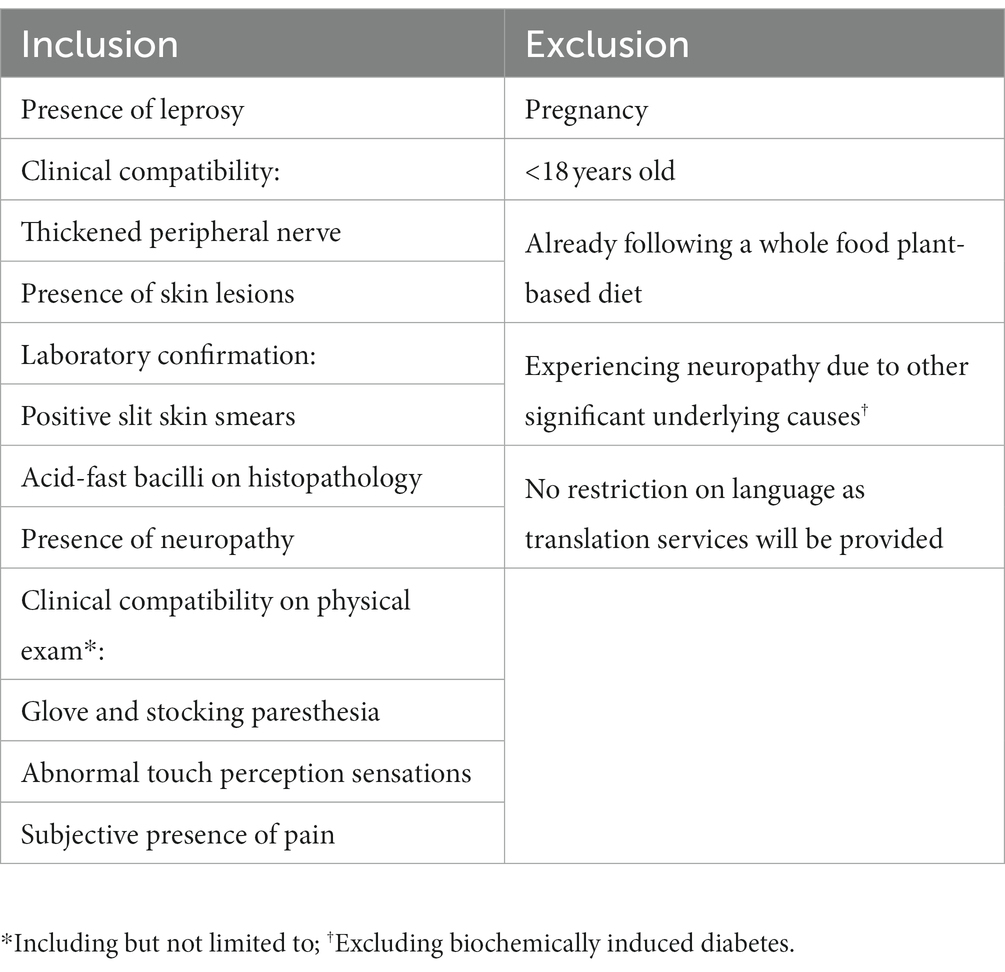
Table 1. Inclusion and exclusion criteria.
The David Jenkins Portfolio Diet was originally designed to lower blood lipid levels in patients with hypercholesterolemia by emphasizing vegetables, fruits, grains, and legumes, while omitting animal products, and limiting saturated fat intake (46, 47). Specifically, the diet focuses on plant sterols (1 g/1000 kcals) as enriched margarine, soy and vegetable proteins (23 g/1000 kcals) as soy milk, meat alternatives, nuts, beans, chickpeas, and lentils, viscous fibers (9 g/1000 kcal) in the form of oats, barley, and psyllium, and low-calorie fruits and vegetables (46, 47) (Table 2). Following a comprehensive interventional trial in which 13 participants received the portfolio diet, a statistically significant reduction of LDL cholesterol, and coronary artery disease was observed (p < 0.001) alongside high compliance (93%) and acceptability (p = 0.042) (47). Similarly, in recent literature interventional trials have emerged assessing the efficacy of a WFPBD, like that of the portfolio diet, for neuropathic pain in individuals with diabetes. Specifically, in a trial assessing a low-fat plant-based diet, omitting animal products, and limiting fat intake to 20–30 g/day in 34 patients, a statistically significant reduction of pain on subjective neuropathy questionnaires and neuropathy on objective electrophysiology was observed (p < 0.05) (19). WFPBDs have been shown to provide sufficient glycemic control and lipid management which, when left unchecked, can exacerbate diabetes-related neuropathy. Given the absence of literature concerning the intersection of dietary lifestyle interventions and neuropathic pain of leprosy, it is hypothesized that a WFPBD will have similar physiological and neuro-protective benefits in a cohort of patients with leprosy and its neuropathic sequelae, in whom diabetes comorbidity is frequent.
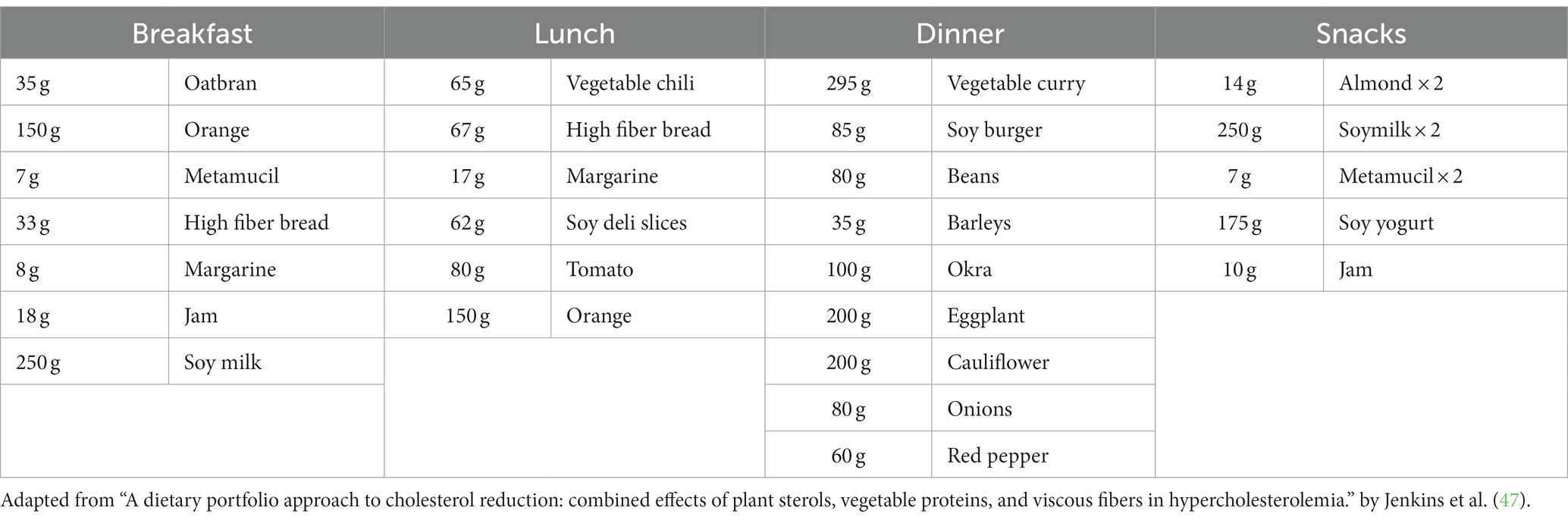
Table 2. Example portfolio diet for one day.
Participants in the intervention group will be instructed to follow a WFPBD for 24 weeks. The study duration was chosen as a conservative estimate of comparable lifestyle-based interventional trials that demonstrated statistically significant improvements in diabetes-related neuropathy outcomes (18, 19). The diet will emphasize vegetables, fruits, whole-grains, nuts, and legumes, while omitting animal products, and limiting fat intake (Table 2). Selection of specific plant-based components may differ across study sites in concordance with local culinary preferences and cultural practices related to food. By tailoring the diet to the unique cultural diaspora affected by leprosy, many of which already endorse plant-based components, we seek to enhance adherence and acceptability to the diet overall. Likewise, current economic projections suggest that diets seeking to reduce animal products are more affordable than current standard diets across all socioeconomic levels – particularly due to inclusion of global staples such as tubers, beans, legumes, and rice – further enhancing accessibility (48–50). Participants will receive weekly support and guidance via 1 h counseling sessions with registered dieticians or the equivalent at each participating site. Sessions will be designed to disseminate comprehensive guidelines for following the WFPBD including culturally acceptable recipes and addressing concerns or knowledge gaps regarding the intervention. Participants in both the intervention group, and control group will be instructed to continue their respective leprosy therapeutics as prescribed throughout the duration of the study. Finally, dietary adherence will be measured via monthly random 24 h dietary recalls, and participants are free to withdraw at any point during the trial if they no longer wish to participate.
Clinical manifestations of leprosy are highly variable, hinging on several geographic, cultural, and genetic underpinnings (2). As such, to maximize the impact of trial outputs, we seek to address the global experience of leprosy through collaboration between the TDU in Toronto, Ontario, Canada, and one or more partner centres for excellence in the care of Hansen’s disease patients abroad. Given migration patterns, selected study centres will account for endemic source countries and regions including the Philippines, the Indian sub-Continent, Southeast Asia, and South America, providing for a more representative data set (2, 51). Trial documents including patient informed consent will be prepared in multiple languages to harmonize procedures across study sites. Likewise, site leads at each respective centre will be responsible for coordinating recruitment, as well as data collection. Oversight will be maintained by a centralized lead at the TDU, who will be responsible for disseminating the randomization protocol, and ensuring overall procedural adherence across sites.
Patients with a history of leprosy will be pre-screened for inclusion via clinical records prior to routine follow up. Study personnel will approach eligible patients experiencing active or treated (“cured”) leprosy, as well as subjective neuropathic pain at participating tropical disease institutions. Eligible participants will receive a comprehensive in-person review of the trial protocol, including data collection requirements, and will be given the patient consent form. Patients will voluntarily confirm willingness to participate and will be free to withdraw at any point. Upon consent to enrolment, participants will be randomized to either the WFPBD intervention group, or standard of care control group. To ensure equal distribution and matching between study groups, randomization will be carried out using a stratified block method (52). Participants will be assigned to strata primarily by study site, followed by sex (male/female), and lastly age-band (18–65, >65) (Figure 2). Random sequence generation will be carried out using a computer-generated allocation sequence. Study investigators, physicians, and participants will not be blinded to group allocation due to the transparent nature of the dietary intervention and counseling. However, primary end points will be collected by independent study personnel, blinded to group allocation, allowing for a single-blinded protocol.

Figure 2. Stratified, block, randomization protocol. Adapted from: “Randomization in clinical studies.” by Lim and In (52). TDU, Tropical Disease Unit.
This is a novel RCT addressing the implications of a WFPBD on neuropathic outcomes in individuals with leprosy. This relationship has not been directly assessed in the current body of literature, however similar research questions have been assessed in individuals with diabetes mellitus. As such, the sample size calculation herein will utilize this literature as a proxy. The efficacy of a WFPBD diet on neuropathy in a diabetes cohort has been reported via the Michigan Neuropathy Screening Instrument (MNSI), including both subjective (questionnaire) and objective (physical assessment) measures. The sample size calculation was based on the MNSI questionnaire measurement as explicit details pertaining to the MNSI physical assessment were not provided. Specifically, both the type of QST utilized (vibration, perception, both, etc.) and the location the test was carried out (lesion, glove, stocking, etc.) were not mentioned. Therefore, the MNSI questionnaire was preferentially chosen as a proxy. Participants receiving the intervention reported a final mean MNSI questionnaire of 5.3 ± 2.5 compared to 7.1 ± 2.8 in the control group at study end (19). Using an opensource sample size calculator with two independent study groups, continuous endpoints, an alpha of 0.5 and 80% power, a final sample size of approximately 60 participants was ascertained (53, 54). This is a conservative estimate as source literature demonstrated a statistically significant effect on outcomes with a relatively low population of 34 individuals (19). Assuming high acceptability and a 14% withdrawal and/or loss to follow-up rate based on previous literature, a final sample size of ~70 individuals, 35 per group, will be needed to adequately power this trial (19, 47, 55, 56).
Descriptive statistics including reported means ± standard deviation for continuous variables [questionnaires including MNSI-physical assessment, Neuropathy Total Symptom Score (NTSS), modified Medical Research Council Scale (mMRCS), Neuropathic Pain Symptom Inventory (NPSI), McGill Pain Questionnaire (MPQ), Pittsburgh Sleep Quality Index (PSQI), and International Physical Activity Questionnaire (IPAQ) summative scores, visual analog scale (VAS), anthropometrics, diabetes duration, hemoglobin A1c, and serum micronutrient levels] and proportions for categorical variables [number of adverse events, dietary adherence, insulin use, leprosy clinical status (according to the WHO and Ridley Jopling classification systems), frequency and prevalence of inflammatory leprosy reactions, corticosteroid use] will be reported by each study group (57). Between- and within-group comparisons will also be made for continuous variables using the Student’s t-test with reported p-values, and for categorical variables using the chi square or Fisher’s exact tests, reporting p-values with odds ratios and 95% confidence intervals. Statistics will also be reported for all time points including baseline, and end of study. Multivariate logistic regression adjusting for covariates [such as age, sex, PROGRESS+ factors (58, 59), level of physical activity, smoking status, alcohol consumption, comorbidities, diabetes status] and potential effect modifiers (such as change in weight over time, medication de-escalation over time) will be carried out to ascertain the impact of a WFPBD on PNP in leprosy patient sub-populations and under various conditions. All statistical analysis will be carried out using GraphPad Prism 8 (GraphPad, United States).
Outcomes will be collected at both baseline and at study end by dedicated personnel blinded to group allocation. Data will be housed on a password-protected and encrypted database generated on a secure drive which will be locked in the respective study centres. Prior to database entry, all patient and study data will be anonymized, and a master list linking patient identification and consecutive study numbers will be generated, secured, and housed separately to said database and to which only the study investigators will have access. Data collected for this study cannot be linked to a specific patient, and the principal investigator and study researchers will be the only individuals who have access to this information. Following final data collection, data will be pooled across study centres and analysis will be conducted within the research lab of the principal investigator.
The MNSI is a robust assessment of neuropathy identifiers that includes both a subjective questionnaire and objective measurements of perception via QST. Specifically, Semmes-Weinstein monofilaments will be used to measure sensation at the ulnar nerve-innervated dorsum of the hand bilaterally, given this site’s predilection for leprosy associated nerve damage, while a 128 Hz tuning fork will be utilized to test for vibration perception thresholds at the great toe (43, 60). This screening instrument has been widely used and validated in both diabetes and leprosy related neuropathy cohorts (19, 60). Scoring is based on a binomial yes/no response to specific questions where yes = 1 point and no = 0 points. Additionally, any abnormal QST result = 1 point, and a score of 4 or greater indicates the presence of neuropathy (60). The MNSI will be conducted at both baseline and at study end and will be utilized as one of the measurements for sensory neuropathy (Figure 3).

Figure 3. Outcomes, stratifiers, and additional considerations to be collected. AE, adverse events; BMI, body mass index; IPAQ, international physical activity questionnaire; mMRC, modified medical research council scale; MNSI, Michigan neuropathy screening instrument; MPQ, McGill pain questionnaire; NPSI, neuropathic pain symptoms inventory; NTSS, neuropathy total symptom score; PA, physical activity; PSQI, Pittsburgh sleep quality index; RRS, resonance Raman spectroscopy; Stnd, standard of care; VAS, visual analog scale; WFPBD, whole foods plant-based diet.
The Neuropathy Total Symptom Score will also be used to formulate a more robust assessment of sensory neuropathy. Unlike the MNSI, the NTSS includes considerations for both neuropathy intensity and frequency. Based on a summative questionnaire, participants can be assigned a maximum of 21.96 points, indicating greater morbidity, and depicted as a matrix comparing neuropathy intensity (mild, moderate, severe) versus frequency (occasional, often, continuous) (61). This questionnaire has been widely used and validated in cohorts of individuals with diabetes, a common comorbidity of leprosy, and will strengthen the assessment of sensory neuropathy within this trial (23, 61). The NTSS will be carried out at both baseline and study end (Figure 3).
The modified Medical Research Council Scale is a reliable tool that has been commonly used to measure motor neuropathy in patients with leprosy (43). The mMRCS utilizes voluntary muscle testing (VMT) in the assessment of motor nerve function including the facial, ulnar, median, radial, and later popliteal nerves. Patients can be assigned a maximum of 5 points, which may be downgraded by any significant reduction of VMT. A score of less than 5 is indicative of decreased motor nerve function (43). The mMRCS will be utilized at baseline and at the end of study to provide a robust assessment of motor neuropathy in this trial (Figure 3).
The Neuropathic Pain Symptom Inventory incorporates both measures of pain intensity and frequency including common patient pain descriptors such as burning, squeezing, pressure, and stabbing relative to the past 24 h (62). It has most commonly been used in the assessment of neuropathic pain in leprosy cohorts, wherein the higher the score the greater the pain, out of a possible 100 points (62–64). Participants will complete the NPSI questionnaire as part of a comprehensive neuropathic pain assessment at both baseline and at the end of the study (Figure 3).
The McGill Pain Questionnaire will also be used to assess neuropathic pain throughout the trial, given a more robust set of patient pain descriptors. The MPQ classifies over 75 words into 4 descriptive pain categories including sensory, affective, evaluative, and miscellaneous, each with subcategories utilizing a scaled point system to indicate relative severity within each group, as well as over time. A maximum score of 78 points is possible, indicating most chronic and severe pain (65). This questionnaire has been utilized and validated within both diabetes and leprosy cohorts (19, 66). Alongside the NPSI, the MPQ will also be completed at both baseline and at the end of the study to provide the most comprehensive assessment of neuropathic pain possible (Figure 3).
Participants will also subjectively assess pain level on a 10-cm Visual Analog Scale between absolute poles of “No pain” and “Worse possible pain,” both at baseline and at the end of the study. The VAS is a tool commonly used to assess pain given any underlying etiology, including both diabetes and leprosy, and is often utilized as the gold-standard when validating novel questionnaires assessing pain (19, 62, 63).
Additional considerations concerning the longstanding implementation of a WFPBD within this population will also be assessed at each counseling session. Data on safety via the number of adverse events, tolerability via drop-out rate, and emerging harms, against gold standard PNP therapeutics (or non-interventions, such as watchful waiting) will be collected and summarized. Dietary adherence reported as a proportionate yes/no will also be collected to ensure interventional feasibility. Based on the current landscape of the literature a WFPBD is expected to perform as well, if not better, than the current standard of care when considering implementation (19, 47, 55) (Figure 3).
As a dietary lifestyle intervention can have a drastic effect on anthropometrics, height and weight will be measured at both baseline and at the end of the study and will be used to calculate body mass index (BMI) (Figure 3). Likewise, sleep quality has been associated with neuropathy severity, and must be monitored throughout the trial. The Pittsburgh Sleep Quality index is a validated questionnaire, widely used to assess sleep perturbation due to various etiologies. Participants can be assigned a maximum of 21 points indicating severe difficulties in all areas of sleep quality (67). The PSQI will be collected at baseline and at the end of the study. Self-reported physical activity will also be collected at such intervals using the International Physical Activity Questionnaire. The IPAQ includes 27-items designed to gauge the frequency and intensity of physical activity carried out in a 7-day period, encompassing occupational, transportation, housework, and leisure activities. It has been extensively tested and validated throughout 12 countries and has previously been utilized in assessing self-reported physical activity in both diabetes and leprosy cohorts (68–70). To avoid the potentially confounding effects of additional lifestyle levers, such as sleep quality and exercise, these assessments are paramount during downstream analysis. Lastly, in individuals experiencing a biochemical diabetes due to leprosy related corticosteroids, an assessment of diabetes control including duration of illness, therapeutics used, and insulin status will also be carried out to monitor any changes throughout the trial (Figure 3). Standard biochemistry, including serum cholesterol, triglycerides, hemoglobin-A1c, serum glucose, hepatic transaminases, creatinine, and basic micronutrient panel (e.g., serum ferritin, B12) will be taken to measure diabetes parameters and general physiological status. To better ascertain the relationship between the dietary lifestyle intervention and leprosy itself, neuropathy and neuropathic pain outcomes will be stratified by secondary outputs, with specific emphasis on diabetes status, and steroid use.
In order to avoid additional invasive blood draws in at-risk equity-deserving patient populations, alternative yet validated measures of individuals’ micronutrient status will be implemented. Both skin carotenoids and urine metabolites can be utilized to define the baseline dietary habits of all participants. Resonance Raman Spectroscopy (RRS) has emerged as an inexpensive and non-invasive tool commonly used to measure skin carotenoid levels including alpha-carotene, beta-carotene, beta-cryptoxanthin, lycopene, lutein, and zeaxanthin (71, 72). Due to the high concentrations of carotenoids in fruits and vegetables, RRS has been used to reliably estimate dietary intake of such foods (71, 72). Its performance has been assessed across multiple geographies and in patients with varied skin tones, and a statistically significant correlation was not identified (71, 72). Similarly, urine metabolites can be assessed using standard laboratory biochemistry commonly available to study centres and can be utilized to estimate the remaining components of diet (73, 74). Consumption habits of fruits, vegetables, low fiber grains, fish protein, nuts, red meat, shellfish, dietary supplements, caffeine, alcohol, and fats and oils can be estimated and corroborated using relative levels of urine metabolites including methyl glutamate, mannitol, cytosine, suberate, omega 3, tryptophan, xylitol, lysine, creatine, vitamin B2, and vitamin E (73, 74). Micronutrient status assessment will be carried out at baseline and at study end to ensure significant micronutrient derangements have not occurred (Figure 3).
Beyond primary and secondary endpoints, potentially confounding variables will be collected and utilized for downstream data analysis including: (1) demographic data: age, sex, socioeconomic status [relative within country and absolute according to World Bank definitions (75)], occupation (considering level of manual work, repetitive tasks, and prolonged standing/walking/climbing), household membership (living alone vs. with family members), and education level; and (2) lifestyle-related information: level of physical activity (via the international physical activity questionnaire), tobacco and cannabis smoking and alcohol consumption habits (amount consumed/day), and environment (urban vs. rural; meters a.s.l.). Effect modifiers including weight loss over time and de-escalation of medication over time will also be considered. Considerations of intervention cost, feasibility, cultural acceptability, and adherence will also be collected and summarized in a thematic analysis (Figure 3).
In advance of study initiation and following Research Ethics Board (REB) approval at all participating centers, this trial will be registered with ClinicalTrials.gov clinical trial database (76) according to the Interventional Trial Protocol Registration Template.1 Current literature suggests high acceptability, and a limited risk profile associated with a WFPBD (19, 21, 22, 47, 55, 56). As a result, a safety board will not be established, however, data on relevant safety, tolerability, and harms will still be collected for downstream analysis. Iterative updates to the trial protocol will be made available to the REB and trial updates will be populated within the ClinicalTrials.gov website as soon as they become available. Data, protocol updates, and study progress will be made available to relevant stakeholders including the site principal investigators, study personnel, and participants, and will be disseminated in the form of peer-reviewed journal publications, submitted conference abstracts/posters, presentations, and lay-language infographics.
This trial aims to investigate the potential neuro-protective impact of a WFPBD on sensory and motor neuropathy in leprosy, thereby strengthening the literature underpinning dietary lifestyle interventions for chronic diseases. Through comprehensive validated questionnaires and QST, a robust profile of neuropathy progression and the relative impact of a WFPBD will be ascertained. Given this assessment, this trial has the potential to inform on the development of novel guidelines to better manage the sequelae of leprosy, an infectious disease of significant global relevance. Patients experiencing a leprosy infection continue to suffer from debilitating therapeutic side effects and social ostracization, contributing to ever rising disability-adjusted life years (DALYs) lost (6, 77–79). Therefore, a WFPBD in the management of leprosy-related neuropathy may mitigate the significant impact of the disease at both the patient and economic level. A WFPBD has the potential to serve as a low-risk, low-cost, low-tech intervention for chronic neuropathic pain, improving function and reducing the overall morbidity of leprosy. More broadly, this trial will also contribute to the growing literature regarding the importance of dietary lifestyle interventions in disease management and may lead to the continued investigation of this relationship in other diseases of relevance.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
MK contributed to protocol design and was primarily responsible for drafting the manuscript. AB conceived the protocol and contributed to design and writing of the manuscript. All authors provided input and comments on successive drafts of the manuscript, read, and approved the final draft.
AB was supported as a Clinician Scientist by the Department of Medicine at the University of Toronto and the University Health Network. MK was supported by the Queen Elizabeth II Graduate Scholarship in Science and Technology and Open Award from the Institute of Medical Science at the University of Toronto.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. ^https://prsinfo.clinicaltrials.gov/Interventional_Study_Protocol_Registration_Template_Jan_2018.pdf
1. World Health Organization. Guidelines for the diagnosis, treatment and prevention of leprosy. Geneva: World Health Organization (2018).
2. Boggild, AK, Correia, JD, Keystone, JS, and Kain, KC. Leprosy in Toronto: an analysis of 184 imported cases. CMAJ. (2004) 170:55–9.
3. Maymone, MBC, Laughter, M, Venkatesh, S, Dacso, MM, Rao, PN, Stryjewska, BM, et al. Leprosy: clinical aspects and diagnostic techniques. J Am Acad Dermatol. (2020) 83:1–14. doi: 10.1016/j.jaad.2019.12.080
4. de Freitas, MRG, and Said, GR. Leprous neuropathy. Handb Clin Neurol. (2013) 115:499–514. doi: 10.1016/B978-0-444-52902-2.00028-X
5. Boggild, AK, Keystone, JS, and Kain, KC. Leprosy: a primer for Canadian physicians. CMAJ. (2004) 170:71–8.
6. Somar, P, Waltz, M, and van Brakel, W. The impact of leprosy on the mental wellbeing of leprosy-affected persons and their family members – a systematic review. Global Mental Health. (2020) 7:7. doi: 10.1017/gmh.2020.3
8. Cavalli, E, Mammana, S, Nicoletti, F, Bramanti, P, and Mazzon, E. The neuropathic pain: an overview of the current treatment and future therapeutic approaches. Int J Immunopathol Pharmacol. (2019) 33:205873841983838. doi: 10.1177/2058738419838383
9. Toh, HS, Maharjan, J, Thapa, R, Neupane, KD, Shah, M, Baral, S, et al. Diagnosis and impact of neuropathic pain in leprosy patients in Nepal after completion of multidrug therapy. PLoS Negl Trop Dis. (2018) 12:e0006610. doi: 10.1371/journal.pntd.0006610
10. Kerstman, E, Ahn, S, Battu, S, Tariq, S, and Grabois, M. Neuropathic pain. Handb Clin Neurol. (2013) 110:175–87. doi: 10.1016/B978-0-444-52901-5.00015-0
11. Durán, AM, Salto, LM, Câmara, J, Basu, A, Paquien, I, Beeson, WL, et al. Effects of omega-3 polyunsaturated fatty-acid supplementation on neuropathic pain symptoms and sphingosine levels in Mexican-Americans with type 2 diabetes. Diabetes Metab Syndr Obes. (2019) 12:109–20. doi: 10.2147/DMSO.S187268
12. Ghadiri-Anari, A, Mozafari, Z, Gholami, S, Khodaei, SA, Aboutorabi-zarchi, M, Sepehri, F, et al. Dose vitamin D supplementations improve peripheral diabetic neuropathy? A before-after clinical trial. Diabetes Metab Syndr. (2019) 13:890–3. doi: 10.1016/j.dsx.2018.12.014
13. Lewis, EJH, Perkins, BA, Lovblom, LE, Bazinet, RP, Wolever, TMS, and Bril, V. Effect of omega-3 supplementation on neuropathy in type 1 diabetes a 12-month pilot trial. Neurology. (2017) 88:2294–301. doi: 10.1212/WNL.0000000000004033
14. Haase, H, Overbeck, S, and Rink, L. Zinc supplementation for the treatment or prevention of disease: current status and future perspectives. Exp Gerontol. (2008) 43:394–408. doi: 10.1016/j.exger.2007.12.002
15. Vijayaraghavan, R, Suribabu, CS, Sekar, B, Oommen, PK, Kavithalakshmi, SN, Madhusudhanan, N, et al. Protective role of vitamin E on the oxidative stress in Hansen’s disease (Leprosy) patients. Eur J Clin Nutr. (2005) 59:1121–8. doi: 10.1038/sj.ejcn.1602221
16. Dwivedi, VP, Banerjee, A, Das, I, Saha, A, Dutta, M, Bhardwaj, B, et al. Diet and nutrition: an important risk factor in leprosy. Microb Pathog. (2019) 137:103714. doi: 10.1016/j.micpath.2019.103714
17. Vázquez, CMP, Netto, RSM, Barbosa, KBF, de Moura, TR, de Almeida, RP, Duthie, MS, et al. Micronutrientes que influyen en la respuesta immune en la lepra. Nutr Hosp. (2014) 29:26–36. doi: 10.3305/nh.2014.29.1.6988
18. Ghavami, H, Radfar, M, Soheily, S, Shamsi, SA, and Khalkhali, HR. Effect of lifestyle interventions on diabetic peripheral neuropathy in patients with type 2 diabetes, result of a randomized clinical trial. Agri. (2018) 30:165–70. doi: 10.5505/agri.2018.45477
19. Bunner, AE, Wells, CL, Gonzales, J, Agarwal, U, Bayat, E, and Barnard, ND. A dietary intervention for chronic diabetic neuropathy pain: a randomized controlled pilot study. Nutr Diabetes. (2015) 5:e158. doi: 10.1038/nutd.2015.8
20. Nathan, DM, Barrett-Connor, E, Crandall, JP, Edelstein, SL, Goldberg, RB, Horton, ES, et al. Long-term effects of lifestyle intervention or metformin on diabetes development and microvascular complications over 15-year follow-up: the diabetes prevention program outcomes study. Lancet Diabetes Endocrinol. (2015) 3:866–75. doi: 10.1016/S2213-8587(15)00291-0
21. Barnard, ND, Katcher, HI, Jenkins, DJA, Cohen, J, and Turner-McGrievy, G. Vegetarian and vegan diets in type 2 diabetes management. Nutr Rev. (2009) 67:255–63. doi: 10.1111/j.1753-4887.2009.00198.x
22. Crane, MG, and Sample, C. Regression of diabetic neuropathy with total vegetarian (vegan) diet. J Nutr Med. (1994) 4:431–9. doi: 10.3109/13590849409003592
23. Saraya, MA, Al-Fadhli, MA, and Qasem, JA. Diabetic status of patients with leprosy in Kuwait. J Infect Public Health. (2012) 5:360–5. doi: 10.1016/j.jiph.2012.08.001
24. de Sousa Oliveira, JS, dos Reis, ALM, Margalho, LP, Lopes, GL, da Silva, AR, de Moraes, NS, et al. Leprosy in elderly people and the profile of a retrospective cohort in an endemic region of the Brazilian Amazon. PLoS Negl Trop Dis. (2019) 13:e0007709. doi: 10.1371/journal.pntd.0007709
25. Boggild, AK, Faust, L, Klowak, M, Macrae, C, Kopalakrishnan, S, and Showler, AJ. Ofloxacin-containing multidrug therapy in ambulatory leprosy patients: a case series. J Cutan Med Surg. (2021) 25:45–52. doi: 10.1177/1203475420952437
26. MacRae, C, Kopalakrishnan, S, Faust, L, Klowak, M, Showler, A, Klowak, SA, et al. Evaluation of safety tool for ambulatory leprosy patients at risk of adverse outcome. Trop Dis Travel Med Vaccines. (2018) 4:1. doi: 10.1186/s40794-018-0061-9
27. Nigam, P, Dayal, SG, Srivastava, P, Joshi, LD, Goyal, BM, Brahma, DU, et al. Diabetic status in leprosy. Hansen Int. (1979) 4:7–14.
28. Ghosh, A. A Central India perspective on leprosy and its association with diabetes mellitus. J Soc Health Diabetes. (2019) 07:37–8. doi: 10.1055/s-0039-1692334
29. McGoey-Smith, KJECMSA. Reversal of pulmonary hypertension, diabetes, and retinopathy, after adoption of a whole food plant-based diet. Int J Dis Reversal Prev. (2019) 1:10. doi: 10.22230/ijdrp.2019v1n2a41
30. Storz, MA, and Küster, O. Plant-based diets and diabetic neuropathy: a systematic review. Lifestyle Med. (2020) 1:e6. doi: 10.1002/lim2.6
31. Aberer, F, Hochfellner, DA, Sourij, H, and Mader, JK. A practical guide for the management of steroid induced hyperglycaemia in the hospital. J Clin Med MDPI. (2021) 10:2154. doi: 10.3390/jcm10102154
32. Bonaventura, A, and Montecucco, F. Steroid-induced hyperglycemia: an underdiagnosed problem or clinical inertia? A narrative review. Diabetes Res Clin Practice. (2018) 139:203–20. doi: 10.1016/j.diabres.2018.03.006
33. Government of Canada. Canada’s dietary guidelines for health professionals and policy makers. Ottawa: Health Canada (2019).
34. BDA: The Association of UK Dietitians. Plant-based diet: food fact sheet. (2017). Available at: https://www.bda.uk.com/resource/plant-based-diet.html (Accessed January 17, 2021).
35. Melina, V, Craig, W, and Levin, S. Position of the academy of nutrition and dietetics: vegetarian diets. J Acad Nutr Diet. (2016) 116:1970–80. doi: 10.1016/j.jand.2016.09.025
36. Calderón-Ospina, CA, and Nava-Mesa, MO. B vitamins in the nervous system: current knowledge of the biochemical modes of action and synergies of thiamine, pyridoxine, and cobalamin. CNS Neurosci Ther. (2020) 26:5–13. doi: 10.1111/cns.13207
37. Zhang, AC, de Silva, MEH, MacIsaac, RJ, Roberts, L, Kamel, J, Craig, JP, et al. Omega-3 polyunsaturated fatty acid oral supplements for improving peripheral nerve health: a systematic review and meta-analysis. Nutr Rev. (2020) 78:323–41. doi: 10.1093/nutrit/nuz054
38. Wintergerst, ES, Maggini, S, and Hornig, DH. Immune-enhancing role of vitamin C and zinc and effect on clinical conditions. Ann Nutr Metab. (2006) 50:85–94. doi: 10.1159/000090495
39. Gladman, SJ, Huang, W, Lim, SN, Dyall, SC, Boddy, S, Kang, JX, et al. Improved outcome after peripheral nerve injury in mice with increased levels of endogenous Omega-3 polyunsaturated fatty acids. J Neurosci. (2012) 32:563–71. doi: 10.1523/JNEUROSCI.3371-11.2012
40. Centers for Disease Control and Prevention. Hansens disease (leprosy): laboratory diagnostics. (2017). Available at: https://www.cdc.gov/leprosy/health-care-workers/laboratory-diagnostics.html (Accessed November 16, 2021).
41. Sreejith, K, Sasidharanpillai, S, Ajithkumar, K, Mani, RM, Chathoth, AT, Menon, PS, et al. High-resolution ultrasound in the assessment of peripheral nerves in leprosy: a comparative cross-sectional study. Indian J Dermatol Venereol Leprol. (2021) 87:199–206. doi: 10.25259/IJDVL_106_20
42. Wheat, SW, Stryjewska, B, and Cartwright, MS. A hand-held ultrasound device for the assessment of peripheral nerves in leprosy. J Neuroimaging. (2021) 31:76–8. doi: 10.1111/jon.12797
43. Haroun, OMO, Vollert, J, Lockwood, DN, Bennett, DLH, Pai, VV, Shetty, V, et al. Clinical characteristics of neuropathic pain in leprosy and associated somatosensory profiles: a deep phenotyping study in India. Pain Rep. (2019) 4:e743. doi: 10.1097/PR9.0000000000000743
44. Devigili, G, Rinaldo, S, Lombardi, R, Cazzato, D, Marchi, M, Salvi, E, et al. Diagnostic criteria for small fibre neuropathy in clinical practice and research. Brain. (2019) 142:3728–36. doi: 10.1093/brain/awz333
45. Cazzato, D, and Lauria, G. Small fibre neuropathy. Curr Opin Neurol. (2017) 30:490–9. doi: 10.1097/WCO.0000000000000472
46. Ramprasath, VR, Jenkins, DJA, Lamarche, B, Kendall, CWC, Faulkner, D, Cermakova, L, et al. Consumption of a dietary portfolio of cholesterol lowering foods improves blood lipids without affecting concentrations of fat soluble compounds. Nutr J. (2014) 13:101. doi: 10.1186/1475-2891-13-101
47. Jenkins, DJA, Kendall, CWC, Faulkner, D, Vidgen, E, Trautwein, EA, Parker, TL, et al. A dietary portfolio approach to cholesterol reduction: combined effects of plant sterols, vegetable proteins, and viscous fibers in hypercholesterolemia. Metabolism. (2002) 51:1596–604. doi: 10.1053/meta.2002.35578
48. Springmann, M, Clark, MA, Rayner, M, Scarborough, P, and Webb, P. The global and regional costs of healthy and sustainable dietary patterns: a modelling study. Lancet Planet Health. (2021) 5:e797–807. doi: 10.1016/S2542-5196(21)00251-5
49. Chen, C, Chaudhary, A, and Mathys, A. Dietary change scenarios and implications for environmental, nutrition, human health and economic dimensions of food sustainability. Nutrients. (2019) 11:856. doi: 10.3390/nu11040856
50. Arrieta, EM, Fischer, CG, Aguiar, S, Geri, M, Fernández, RJ, Coquet, JB, et al. The health, environmental, and economic dimensions of future dietary transitions in Argentina. Sustain Sci. (2022) 15:1–17. doi: 10.1007/s11625-021-01087-7
51. Matsuoka, M, Zhang, L, Morris, MF, Legua, P, and Wiens, C. Polymorphism in the rpoT gene in Mycobacterium leprae isolates obtained from Latin American countries and its possible correlation with the spread of leprosy. FEMS Microbiol Lett. (2005) 243:311–5. doi: 10.1016/j.femsle.2004.12.031
52. Lim, CY, and In, J. Randomization in clinical studies. Korean J Anesthesiol. (2019) 72:221–32. doi: 10.4097/kja.19049
53. ClinCalc. Sample size calculator. (2019). Available at: https://clincalc.com/stats/samplesize.aspx (Accessed November 16, 2021).
54. Kittelson, JM. A review of: fundamentals of biostatistics, 7th ed., by B. Rosner. J Biopharm Stat. (2011) 21:1046–8. doi: 10.1080/10543406.2011.592364
55. Barnard, ND, Scialli, AR, Turner-Mcgrievy, G, and Lanou, AJ. Acceptability of a low-fat vegan diet compares favorably to a step II diet in a randomized. Controlled Trial J Cardiopulm Rehabil Prev. (2004) 24:229–35. doi: 10.1097/00008483-200407000-00004
56. Barnard, ND, Gloede, L, Cohen, J, Jenkins, DJA, Turner-McGrievy, G, Green, AA, et al. A low-fat vegan diet elicits greater macronutrient changes, but is comparable in adherence and acceptability, compared with a more conventional diabetes diet among individuals with type 2 diabetes. J Am Diet Assoc. (2009) 109:263–72. doi: 10.1016/j.jada.2008.10.049
57. Klowak, M, and Boggild, AK. A review of nutrition in neuropathic pain of leprosy. Ther Adv Infect Dis. (2022) 9:204993612211026. doi: 10.1177/20499361221102663
58. World Health Organization. Handbook on health inequality monitoring: with a special focus on low- and middle-income countries. Geneva: World Health Organization (2013).
59. World Health Organization. Evidence to recommendations: methods used for assessing health equity and human rights considerations in COVID-19 and aviation. Interim guidance. Geneva: World Health Organization (2020).
60. Herman, WH, Pop-Busui, R, Braffett, BH, Martin, CL, Cleary, PA, Albers, JW, et al. Use of the Michigan neuropathy screening instrument as a measure of distal symmetrical peripheral neuropathy in Type1 diabetes: results from the diabetes control and complications trial/epidemiology of diabetes interventions and complications. Diabet Med. (2012) 29:937–44. doi: 10.1111/j.1464-5491.2012.03644.x
61. Bastyr, EJ. Development and validity testing of the neuropathy total symptom score-6: questionnaire for the study of sensory symptoms of diabetic peripheral neuropathy. Clin Ther. (2005) 27:1278–94. doi: 10.1016/j.clinthera.2005.08.002
62. Bouhassira, D, Attal, N, Fermanian, J, Alchaar, H, Gautron, M, Masquelier, E, et al. Development and validation of the neuropathic pain symptom inventory. Pain. (2004) 108:248–57. doi: 10.1016/j.pain.2003.12.024
63. Raicher, I, Stump, PRNAG, Harnik, SB, de Oliveira, RA, Baccarelli, R, Marciano, LHSC, et al. Neuropathic pain in leprosy: symptom profile characterization and comparison with neuropathic pain of other etiologies. Pain Rep. (2018) 3:e638. doi: 10.1097/PR9.0000000000000638
64. Ramos, JM, Alonso-Castañeda, B, Eshetu, D, Lemma, D, Reyes, F, Belinchón, I, et al. Prevalence and characteristics of neuropathic pain in leprosy patients treated years ago. Pathog Glob Health. (2014) 108:186–90. doi: 10.1179/2047773214Y.0000000140
65. Melzack, R. The McGill pain questionnaire: major properties and scoring methods. Pain. (1975) 1:277–99. doi: 10.1016/0304-3959(75)90044-5
66. Stump, PR, Baccarelli, R, Marciano, LH, Lauris, JR, Teixeira, MJ, Ura, S, et al. Neuropathic pain in leprosy patients. Int J Lepr Other Mycobact Dis. (2004) 72:134–8. doi: 10.1489/1544-581X(2004)072<0134:NPILP>2.0.CO;2
67. Buysse Charles, F, Reynolds Ill, DJ, Monk, TH, Berman, SR, and Kupfer, DJ. The Pittsburgh sleep quality index: a new instrument for psychiatric practice and research. Psychiatry Res. (1988) 28:193–213. doi: 10.1016/0165-1781(89)90047-4
68. Craig, CL, Marshall, AL, Sjöström, M, Bauman, AE, Booth, ML, Ainsworth, BE, et al. International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exerc. (2003) 35:1381–95. doi: 10.1249/01.MSS.0000078924.61453.FB
69. Nolan, RC, Raynor, AJ, Berry, NM, and May, EJ. Self-reported physical activity using the international physical activity questionnaire (IPAQ) in Australian adults with type 2 diabetes, with and without peripheral neuropathy. Can J Diabetes. (2016) 40:576–9. doi: 10.1016/j.jcjd.2016.05.013
70. Dias do Prado, G, Bilion Ruiz Prado, R, Soares Camargo Marciano, LH, Maria Tonelli Nardi, S, Antonio Cordeiro, J, and Luiz Monteiro, H. WHO disability grade does not influence physical activity in Brazilian leprosy patients. Lepr Rev. (2011) 82:270–8. doi: 10.47276/lr.82.3.270
71. Ermakov, I, Ermakova, M, Sharifzadeh, M, Gorusupudi, A, Farnsworth, K, Bernstein, PS, et al. Optical assessment of skin carotenoid status as a biomarker of vegetable and fruit intake. Arch Biochem Biophys. (2018) 646:46–54. doi: 10.1016/j.abb.2018.03.033
72. Mayne, ST, Cartmel, B, Scarmo, S, Jahns, L, Ermakov, I, and Gellermann, W. Resonance Raman spectroscopic evaluation of skin carotenoids as a biomarker of carotenoid status for human studies. Arch Biochem Biophys. (2013) 539:163–70. doi: 10.1016/j.abb.2013.06.007
73. Garcia-Perez, I, Posma, JM, Chambers, ES, Mathers, JC, Draper, J, Beckmann, M, et al. Dietary metabotype modelling predicts individual responses to dietary interventions. Nat Food. (2020) 1:355–64. doi: 10.1038/s43016-020-0092-z
74. Playdon, MC, Sampson, JN, Cross, AJ, Sinha, R, Guertin, KA, Moy, KA, et al. Comparing metabolite profiles of habitual diet in serum and urine. Am J Clin Nutr. (2016) 104:776–89. doi: 10.3945/ajcn.116.135301
76. Government of Canada. Health Canada’s clinical trials database. (2016). Available at: https://www.canada.ca/en/health-canada/services/drugs-health-products/drug-products/health-canada-clinical-trials-database.html (Accessed November 6, 2021).
77. Das, N, De, A, Naskar, B, Sil, A, Das, S, Sarda, A, et al. A quality of life study of patients with leprosy attending the dermatology OPD of a tertiary care center of Eastern India. Indian J Dermatol. (2020) 65:42–6. doi: 10.4103/ijd.IJD_729_18
78. Finotti, RFC, Andrade, ACS, and Souza, DPO. Transtornos mentais comuns e fatores associados entre pessoas com hanseníase: análise transversal em Cuiabá, 2018. Epidemiol Serv Saude. (2020) 29:e2019279. doi: 10.5123/S1679-49742020000400006
79. Gómez, LJ, van Wijk, R, van Selm, L, Rivera, A, Barbosa, MC, Parisi, S, et al. Stigma, participation restriction and mental distress in patients affected by leprosy, cutaneous leishmaniasis and Chagas disease: a pilot study in two co-endemic regions of eastern Colombia. Trans R Soc Trop Med Hyg. (2020) 114:476–82. doi: 10.1093/trstmh/trz132

Keywords: leprosy, neglected tropical disease, peripheral neuropathic pain, nutrition, whole foods plant-based diet, portfolio diet, randomized control trial protocol
Citation: Klowak M and Boggild AK (2023) The efficacy of a whole foods, plant-based dietary lifestyle intervention for the treatment of peripheral neuropathic pain in leprosy: a randomized control trial protocol. Front. Nutr. 10:1196470. doi: 10.3389/fnut.2023.1196470
Edited by:
Ellen E. Blaak, Maastricht University, NetherlandsReviewed by:
Bernard Naafs, Stichting Global Dermatology, NetherlandsCopyright © 2023 Klowak and Boggild. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Andrea K. Boggild, YW5kcmVhLmJvZ2dpbGRAdXRvcm9udG8uY2E=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.