
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Nutr. , 12 April 2023
Sec. Clinical Nutrition
Volume 10 - 2023 | https://doi.org/10.3389/fnut.2023.1172526
This article is part of the Research Topic Intensive Care Unit Acquired Weakness: Potential Role of Medical Nutrition Treatment Quantity, Timing, and Composition View all 9 articles
 Su Wang1†
Su Wang1† Xin Zhao1†
Xin Zhao1† Qian Wang2†
Qian Wang2† Yongran Wu1†
Yongran Wu1† Jiaxin Xu1†Ruiting Li1
Jiaxin Xu1†Ruiting Li1 Ting Zhou1Zheng Lv1Jihong Yang3Le Yang4*Xiaojing Zou1*
Ting Zhou1Zheng Lv1Jihong Yang3Le Yang4*Xiaojing Zou1*Background: Early enteral nutrition (EN) is recommended for critically ill patients. However, the impact of early EN on intubated severe trauma patients remains unclear.
Methods: Severely traumatized adult patients who received invasive mechanical ventilation (MV) for more than 48 h during intensive care unit (ICU) stay at our institution between 2017 and 2022 were retrospectively included. Early EN was defined as EN initiation ≤48 h from ICU admission and late EN >48 h. Propensity score matching (PSM) analysis was used to compare outcomes between the groups. The primary endpoint was the incidence of ventilator-associated pneumonia (VAP). Multivariable logistic regression analysis was performed to identify independent predictors of delayed EN.
Results: For final analysis, 337 intubated severe trauma patients were available, including 204 (60.5%) in the early EN group and 133 (39.5%) in the late EN group. After PSM, early EN patients had a lower incidence of VAP (12.9 vs. 25.8%, p = 0.026) and a shorter length of hospital stay (21 vs. 24 days, p = 0.015) compared to late EN patients. There was no demonstrable difference in mortality between the two groups. Abdominal trauma, massive blood transfusion, and serum albumin were identified as independent risk factors for delayed EN.
Conclusion: Early EN decreased the VAP rate and reduced the length of hospital stay in invasively ventilated patients with severe trauma. Abdominal injury, massive blood transfusion and low albumin were associated with delayed EN.
Severely injured trauma patients who require ventilator support and intensive care unit (ICU) admission are at risk of nosocomial pneumonia development (1). Nosocomial infections in the ICU, particularly ventilator-associated pneumonia (VAP), pose a considerable economic burden globally, as patients often need prolonged mechanical ventilation (MV) and have significantly longer stays in the ICU and hospital (2). VAP occurred more frequently in intubated trauma patients than in other critically ill patients, and contributed to increased morbidity and mortality (3, 4). It has been reported that the incidence of VAP can reach up to 60.6% among severe trauma patients (5). How to effectively prevent VAP in trauma patients remains an important issue.
The responses following the traumatic injuries such as muscle breakdown, immune suppression, and cytokine cascade potentially deteriorate the nutritional status, which predisposes the patients to infectious complications (6). Nutritional support including enteral nutrition (EN) and parenteral nutrition is a crucial factor in the fight against hospital pneumonia (7). However, the reports on the relationship between EN and the development of VAP seem to be conflicting. Some authors have indicated that early EN was associated with increased VAP risk (8, 9), whereas others have observed the opposite (10). To date, in severely traumatized patients, the impact of early EN on VAP is also unclear. Moreover, although early initiation of EN is recommended in the trauma patients, the evidence is also inconsistent as to whether it provides a survival benefit (11, 12).
Here, our primary purpose was to compare the effects of early vs. late EN on VAP occurrence and other clinical outcomes in invasively ventilated patients with severe trauma using a propensity score model. The second purpose was to identify factors that were associated with delayed EN.
This study adhered to the Declaration of Helsinki and was approved by the Ethical Committee of the Union Hospital (No. 0167-1), Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China. Due to the retrospective nature of the study, patient informed consent was waived.
We retrospectively reviewed the medical records of all trauma patients consecutively admitted to the ICU of our institution between January 2017 and December 2022. In this study, the patients were enrolled if they met the following inclusion criteria. (i) Who was an adult patient (≥18 years old). (ii) Who had an injury severity score (ISS) ≥ 16 points (13). (iii) Who received EN. (iv) Who underwent invasive MV for more than 48 h. (v) Who were not confirmed with COVID-19. Excluded patients had been treated with tracheostomy before ICU arrival; had already received invasive MV for at least 12 h before ICU admission; switched to palliative care; had incomplete medical records and missing key data.
We extracted patient data from electronic medical record system in our institution. The parameters were collected in the present study including gender, age, body mass index (BMI), history of smoking, Charlson Comorbidity Index (CCI), initial Glasgow Coma Scale (GCS), brain trauma, abdominal trauma, chest trauma, spinal trauma, pelvic trauma, ICU admission diagnosis of shock and trauma-induced acute respiratory distress syndrome (ARDS), massive blood transfusion, ISS, sequential organ failure assessment (SOFA) and acute physiology and chronic health evaluation II (APACHE II) within 24 h after ICU arrival, serum creatinine, total bilirubin and albumin at ICU admission, and the time to delivery of EN after admission to the ICU.
The primary outcome of our study was the incidence of VAP. Other outcome variables were the duration of invasive MV, the length of ICU and hospital stay, and 28-day mortality.
Body mass index was defined as body weight (kg)/body height (m2). Massive blood transfusion was defined as adults transfused packed red blood cells ≥10 units within 24 h or >4 units within 1 h (14). Early EN was defined as EN initiation within 48 h after ICU admission and late or delayed EN as initiation after 48 h of ICU admission, based on the recommendation of nutrition support therapy guidelines in the adult critically ill patients (15). EN was initiated according to the assessment of the physician in charge at the time. Patients were routinely given EN by a nasogastric feeding tube at our institution, and the gastric tube was considered to be exchanged for a jejunal tube when gastric motility disorder occurred and no improvement was observed after administration of metoclopramide. VAP was defined as a pneumonia arising >48 h after endotracheal intubation. VAP diagnoses were documented by the new onset of fever or leukocytosis and purulent sputum, with new lung infiltrate, and the positive microbiological sample of endotracheal aspirate (≥105 colony-forming units [cfu]/mL) or bronchoalveolar lavage (≥104 cfu/mL) or protected brush specimens (≥103 cfu/mL) (16).
All statistical analyses were performed using IBM SPSS software (version 26.0), and differences were considered statistically significant at p < 0.05 in this study. Normal distribution was checked by Kolmogorov–Smirnov test for all continuous variables. Categorical variables were presented as frequency (percentage) and non-normally distributed continuous variables as medians and interquartile ranges. To compare baseline characteristics between the two groups, chi-square test or Fishers exact test was used for categorical variables, and Mann-Whitney non-parametric test was used for continuous variables with non-normal distributions.
To minimize the influence of potential confounders, a propensity score matching (PSM) analysis was conducted. The covariates used for propensity matching were the twenty variables presented in Table 1. To create a matched sample, nearest neighbor matching was performed with a caliper width of 0.1 on the propensity-score with a matching ratio of 1:1. A subgroup analysis was also conducted, and we evaluated the treatment-by-covariate interactions to explore potential heterogeneity of the treatment effects relative to the sites of trauma. In this study, the primary outcomes stratified by trauma sites were compared in the PSM cohort and the p-values for the interactions were examined using the Cochran-Mantel-Haenszel test in subgroups. In order to identify the independent risk factors for delayed EN, factors with a p-value of less than 0.05 in the univariable analysis were entered into the multivariable logistic regression analysis with a forward stepwise procedure.
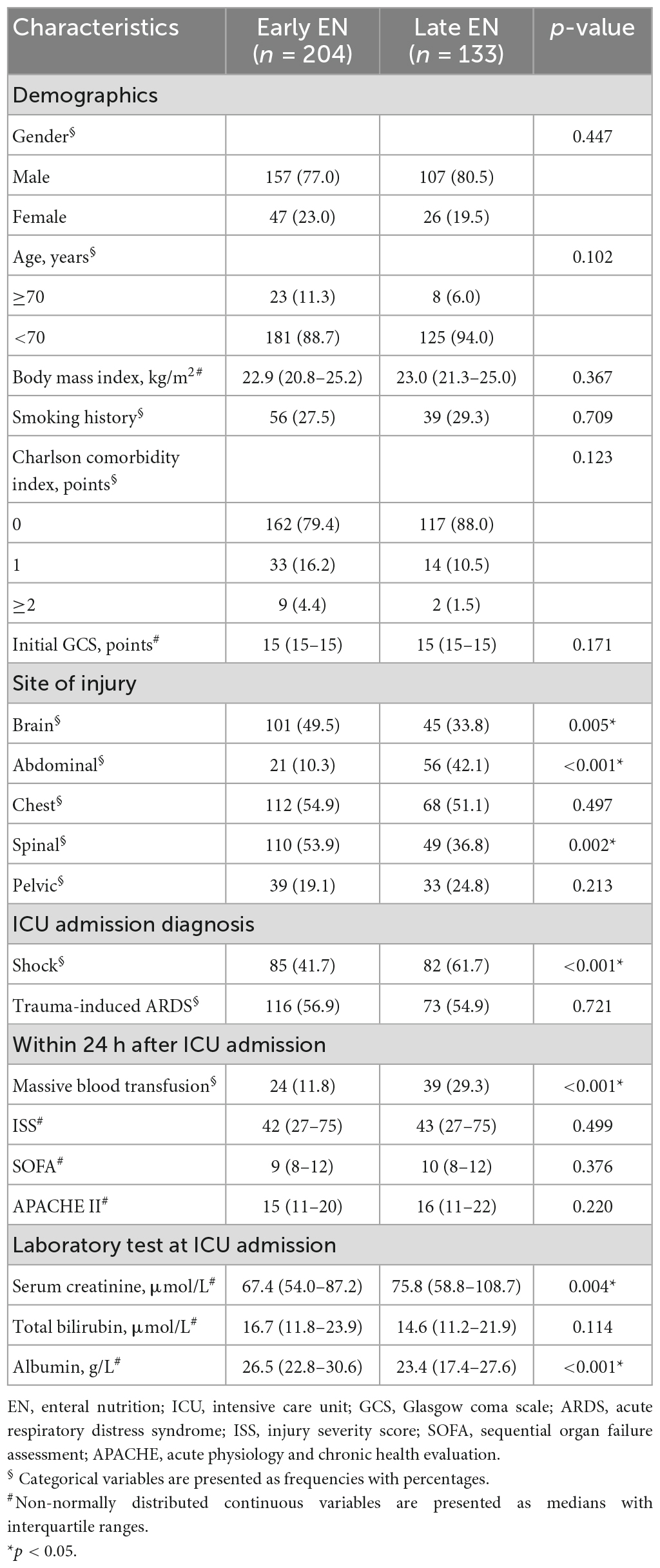
Table 1. Baseline characteristics of the severe trauma patients receiving invasive mechanical ventilation.
A total of 498 mechanically ventilated patients with severe trauma met the inclusion criteria. Among them, 39 patients had been treated with tracheostomy before ICU admission, 73 patients had already received invasive MV for at least 12 h before admission, 15 patients switched to palliative care, and 34 patients had incomplete data records (Figure 1). After excluding the cases based on the exclusion criteria, the remaining 337 cases were further analyzed in this study. Of these patients, 78.3% were male, 9.2% were older than 70 years, 28.2% had a smoking history, 17.2% had a CCI score ≥1, 43.3% suffered a brain injury, 22.8% suffered an abdominal injury, 53.4% suffered a chest injury, 47.2% suffered a spinal injury, 21.4% suffered a pelvic injury, 49.6% occurred the shock, 56.1% occurred the trauma-induced ARDS, 18.7% received massive blood transfusion. The median BMI of the entire study population was 22.9 kg/m2, the median GCS score was 15 points, the median ISS score was 42 points, the median SOFA score was 10 points, the median APACHE II score was 15 points, the median serum creatinine value was 70.0 μmol/L, the median total bilirubin value was 16.0 μmol/L, and the median albumin value was 25.7 g/L.
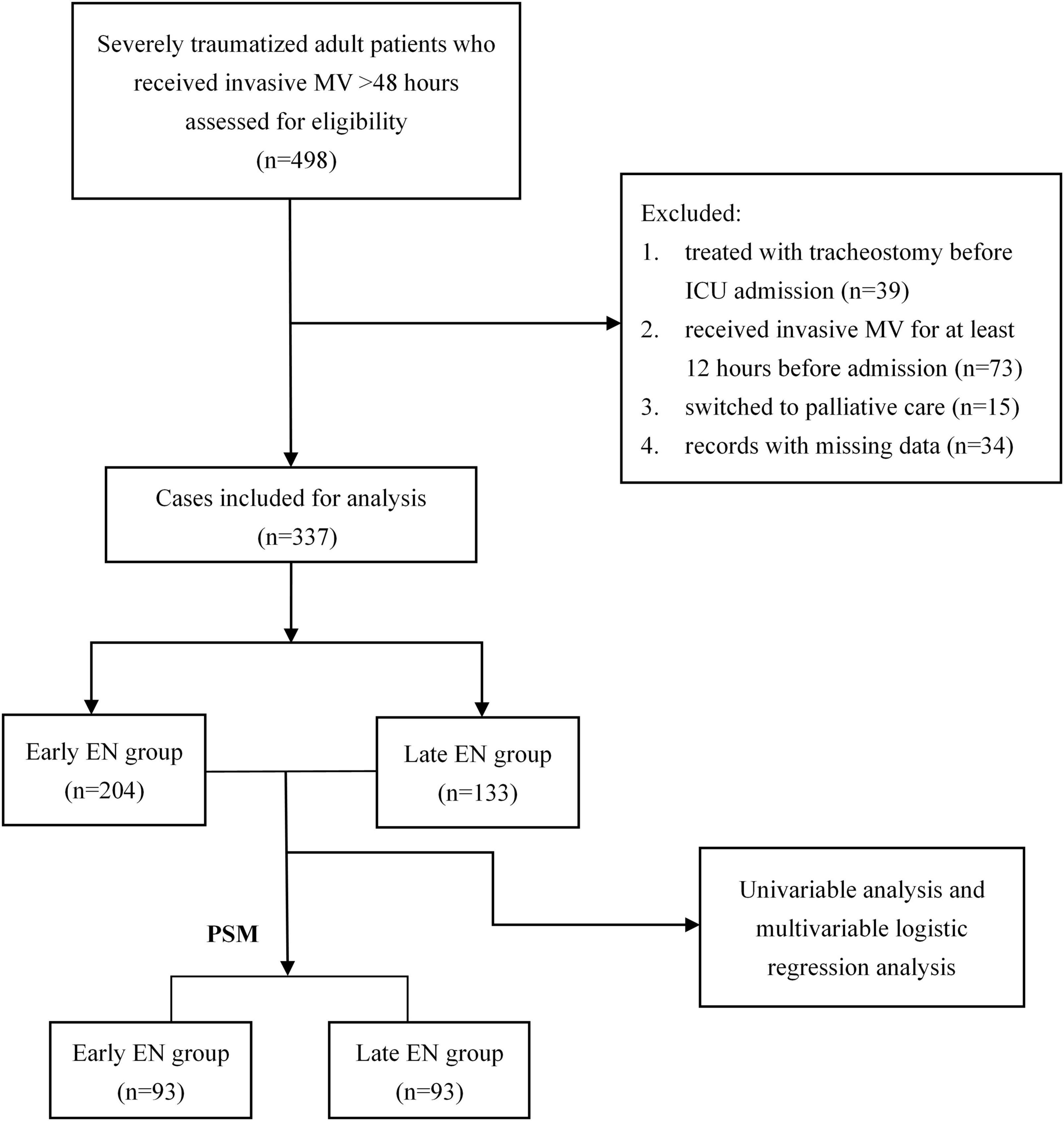
Figure 1. Flow chart of the study. ICU, intensive care unit; EN, enteral nutrition; MV, mechanical ventilation; PSM, propensity score matching.
There were 204 patients (60.5%) delivered with early EN, while 133 patients (39.5%) with late EN. Compared with the late EN group, the early EN group had a lower serum creatinine value (67.4 vs. 75.8 μmol/L, p = 0.004), a higher albumin value (26.5 vs. 23.4 g/L, p < 0.001), a higher proportion of brain injury (49.5 vs. 33.8%, p = 0.005) and spinal injury (53.9 vs. 36.8, p = 0.002), a lower proportion of abdominal injury (10.3 vs. 42.1%, p < 0.001), shock (41.7 vs. 61.7%, p < 0.001) and massive blood transfusion (11.8 vs. 29.3%, p < 0.001). The detailed comparison was presented in the Table 1.
In invasively ventilated patients with severe trauma, we assessed the impact of early EN on the primary outcome of VAP development. The overall incidence of VAP was 21.4% (72/337), and the early EN patients had a lower incidence (16.7 vs. 28.6%, p = 0.009, Table 2) compared to the late EN patients. A significantly shorter length of hospital stay was also observed in the early EN group (21 vs. 26 days, p < 0.001). But no significant effect of early EN on invasive MV time, length of stay in ICU and all-cause mortality rate was demonstrated (Table 2). The 28-day mortality rate for the entire population was 6.2%.
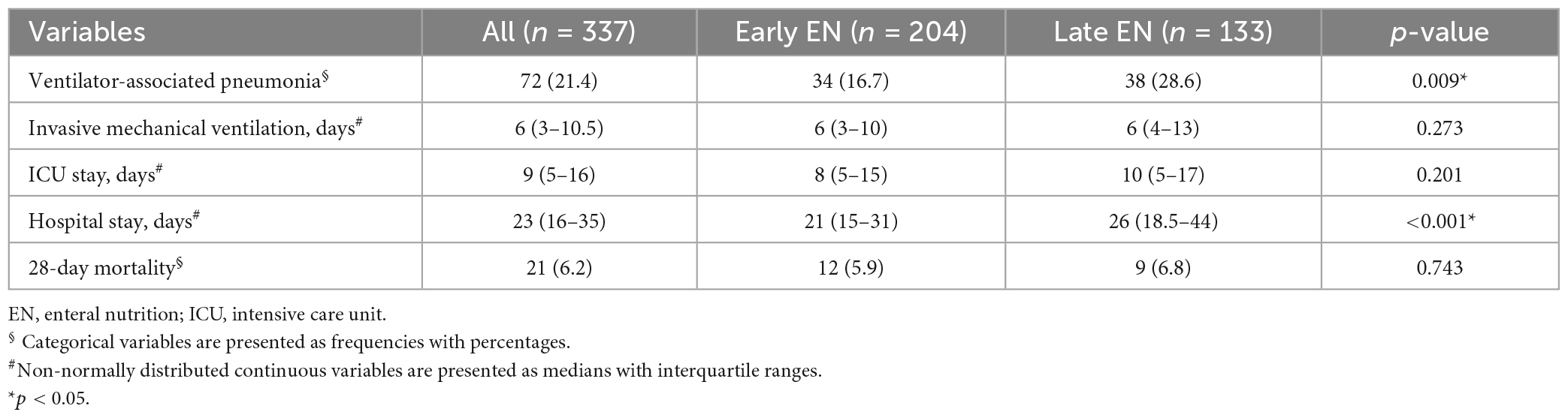
Table 2. Outcomes in early and late enteral nutrition groups.
To further investigate the role of early EN delivery in preventing VAP and improving prognosis in severely traumatized population, we performed PSM to balance clinical factors between the two groups. PSM yielded a cohort of 93 patients in the early EN group and 93 patients in the late EN group. After PSM, between-group differences for all variables were eliminated (Table 3). The significant results between the groups remained similar after matching by propensity score (Table 4), that is, patients with delayed EN had higher VAP rates and longer hospital stays. In the early EN group, shorter invasive ventilator duration, shorter ICU stay and lower mortality were also observed, but no significant differences were present. We did a subgroup analysis, and subgroup results were presented as a forest plot (Figure 2). There were no significant interactions between treatment groups and different sites of trauma in regard to the occurrence of VAP (p-interaction >0.05). The effects of early EN on the primary outcome were similar regardless of trauma sites.
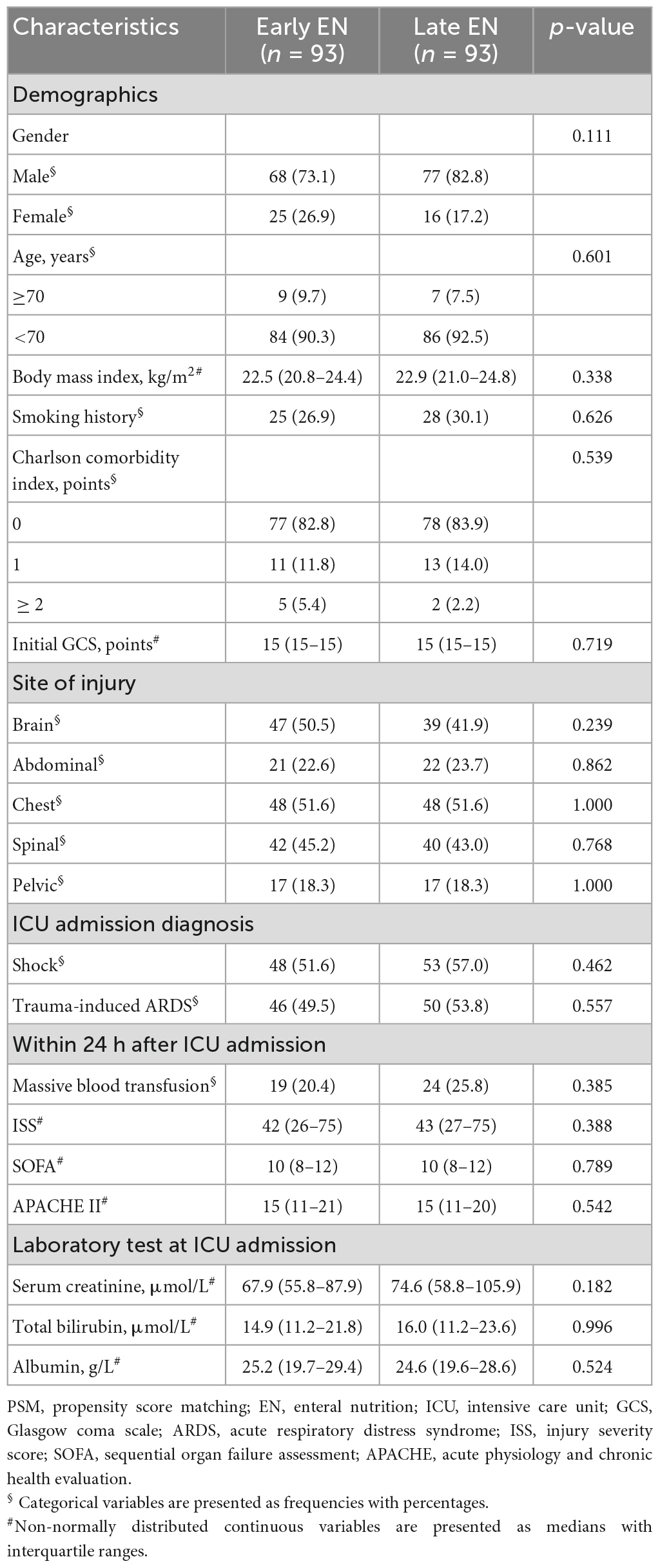
Table 3. Comparison of baseline characteristics in early and late enteral nutrition groups after PSM.
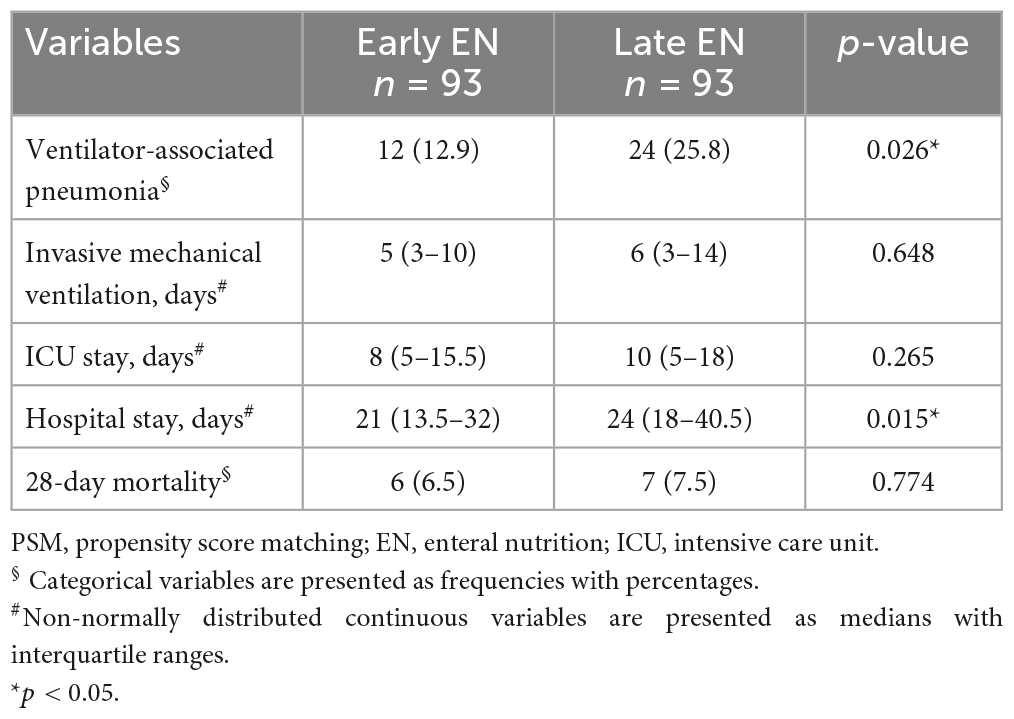
Table 4. Comparison of outcomes in early and late enteral nutrition groups after PSM.
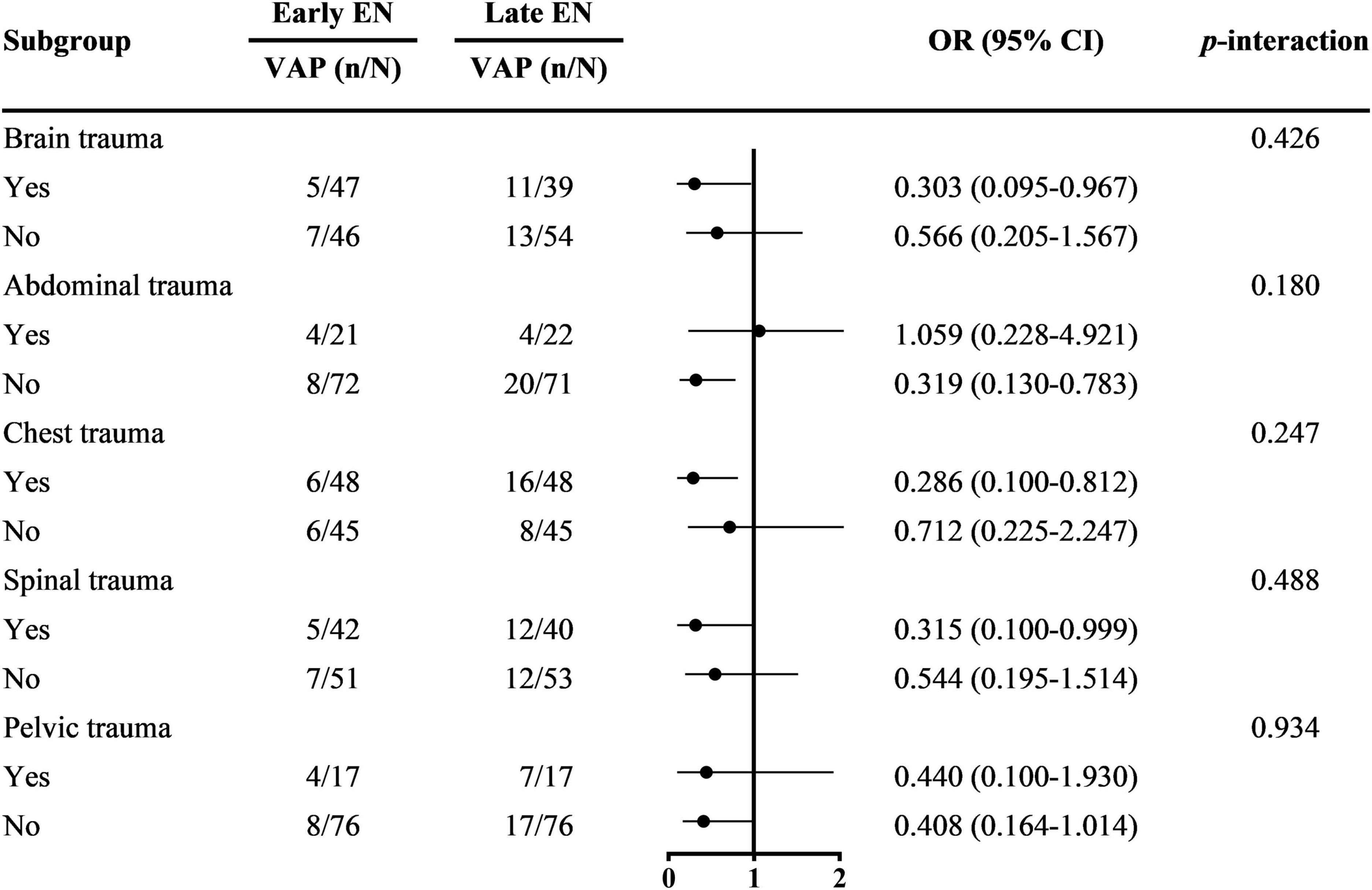
Figure 2. Treatment effect on VAP by subgroup. VAP, ventilator-associated pneumonia; EN, enteral nutrition; OR, odds ratio; CI, confidence interval.
A multivariable logistic regression analysis was carried out to identify the independent risk factors for delayed EN. Seven statistically significant variables in the univariable analysis were included for the further multivariable regression analysis. The results showed that the variables independently associated with delayed EN were abdominal trauma [odds ratio (OR): 6.087; 95% confidence interval (CI): 3.384, 10.949; p < 0.001], massive blood transfusion (OR: 2.657; 95% CI: 1.409, 5.010; p = 0.003), and serum albumin (OR: 0.953; 95% CI: 0.918, 0.988; p = 0.010; Table 5).

Table 5. Multivariable analysis of independent risk factors for delayed enteral nutrition.
Multiple studies have shown that the burden of VAP in trauma patients is significant (17, 18). The observed incidence rate of VAP among the severely traumatized patients in the present study was within the range (11.9–28.3%) previously reported (19, 20). As VAP is known to result in escalating the cost of care and increasing length of stay and mortality, studies have explored the effect of some treatment strategies on reducing its prevalence, such as use of probiotic preparation (20). Nutritional intervention is also considered to be an alternative means to influence the prognosis of trauma patients. Over the past two decades, there has been a growing body of clinical studies surrounding the application of EN to reduce the risk of VAP (21). Regrettably, the impact of early EN support on VAP development in the trauma population has not been well recognized yet.
To our knowledge, this is the first study with a propensity score-matching method to report superiority for early EN over late EN in reducing VAP occurrence in invasively ventilated patients with severe trauma. Our findings also indicated that early EN delivery exerted no significant effect on mortality of these patients, but significantly decreased the length of hospital stay. The risk factors for delayed EN were further analyzed in this study, and the multivariable analysis revealed that abdominal trauma, massive blood transfusion on the first day after ICU admission and lower albumin prevented early delivery of EN.
In this study, even after PSM, provision of early EN to the severe trauma patients significantly decreased the VAP rate. A study based on a nationwide inpatient database found that early EN application in patients with severe traumatic brain injury reduced nosocomial pneumonia (22). Similar effect was observed in acute pancreatitis patients, and the nutritional status of patients was also improved (23). Distinctive and complex metabolic changes after trauma make severe trauma patients more susceptible for developing malnutrition (6, 24). One review further indicated that depending on the severity of injury, energy expenditure increased by 20–50% in trauma patients compared with patients after elective surgery (6). However, numerous studies have revealed that malnutrition in hospitalized patients was related to the increased complications and mortality and prolonged hospital stays (25, 26). In addition to providing protein and calories for critically ill trauma patients, EN also produces non-nutritional benefits. Early enteral feeding following trauma can prevent intestinal mucosa atrophy which can occur rapidly after injury (27). Studies have indicated that early EN maintains the functional gut integrity and prevents bacterial translocation, thereby reducing the risk of systemic infections (28, 29). Moreover, it has been found that stress hyperglycemia mediated by stress-induced insulin resistance following severe trauma is associated with both infection and death in critically injured patients (30), whereas enteral feeding modulates metabolic responses, attenuating the insulin resistance (31). Therefore, early EN application might help reduce the risk of infections.
Enteral nutrition could elicit immunologic changes, and immunologic communication between the gastrointestinal (GI) tract and mucosal surfaces throughout the body might exist via a common mucosal immunity (32). The transfer of immune cells between the gut and the lungs might play a beneficial role in enhancing the capacity of the host to fight infection (33). In addition, the transport of soluble microbial components and metabolites via the circulation is one means of communication between the gut microbiota and the lungs (33). Samuelson et al. also suggested that the GI microbiota played a crucial role in immune adaptation and initiation at the distal mucosal sites, such as the lung (34). Moreover, studies have indicated that lack of enteral feeding could lead to loss of established anti-viral and anti-bacterial defenses within the respiratory tract, and impaired ability to cope with new infectious challenges (35). Although it was pointed out that nasogastric tube EN increased the risk of reflux and aspiration of gastric contents and reduced the prevention of VAP (36), our findings supported the benefits of early EN application in the severely traumatized population. Besides, Croce et al. demonstrated that use of the ventilator bundle could not work well to prevent VAP in trauma patients (37). Hence, the early delivery of EN may be a useful strategy.
Despite EN delivery being an important part of standard care for critically ill patients, it has been documented that only one third of patients have EN initiated within the 48-h recommendation (38). Approximately 21.0% of patients receiving delayed EN in the medical ICU was reported (39). Moreover, a higher proportion (64%) of patients with severe traumatic brain injury had delayed EN (22), compared with our study population. It is obvious that patient factors may influence the success of early EN delivery.
As a complex injury within a complex cavity, abdominal trauma was a potent risk factor for delayed EN in our study, with an adjusted OR of 6. Yin et al. expressed that their hesitation to introduce early EN in abdominal trauma patients was due to fear of feeding intolerance, although EN could be delivered at 12 h after operation or 24 h after injury in these patients (40). Perhaps our result could also be explained by this. Their study, however, showed that early EN did not increase feeding intolerance and was related to reduced infectious complications (40). In addition, abdominal viscera exposure has led to EN withheld by some clinicians in patients with open abdomen due to the concerns about paralytic ileus and subsequent aspiration and bowel dilation risk (41). Nonetheless, Dissanaike et al. have suggested that early EN appears safe and is associated with the reduction in pneumonia in this patient population (42). Unless contraindicated, late initiation of enteral feeding may be unwise.
Another independent risk factor of delaying EN was massive blood transfusion. Hemorrhage is the most common cause of early death in trauma patients, and massive blood transfusion is required to resuscitate traumatically injured patients with complex physiologic derangements (43). Physiologically, shock shunts blood flow away from the GI tract, however, gut perfusion remains depressed in spite of effective shock resuscitation (44). Thus, there is a concern that EN in shock further harms the already impaired splanchnic perfusion (12), which may partially explain the relatively high proportion of patients with massive blood transfusion receiving late EN. However, one review indicated that early EN in patients with shock was well tolerated and was related to preserved splanchnic blood flow and improved clinical outcomes (45). Moreover, previous study has demonstrated that massive transfusion is independently associated with VAP among critically ill trauma patients (46). Torrance et al. noted that the transfusion of blood products enhanced immunosuppressive inflammatory response caused by polytrauma with resultant increased susceptibility to nosocomial infection (47). Therefore, we speculate that providing early EN support to trauma patients with massive transfusions may have potential benefits.
Critical illness is characterized by inflammation, and hepatic reprioritization of protein synthesis results in lower serum concentrations of albumin (48). Similarly, a low overall albumin level occurred in severe trauma population of this study. According to our results, the lower the albumin value, the more likely it is to delay EN application. This may be interpreted by the consideration of hypoalbuminemia inducing delayed gastric emptying and abnormal intestinal peristalsis (49), while enteral feeding may increase the risk for regurgitation, pulmonary aspiration, and eventual VAP when GI dysfunction is present (50).
This work was constrained by several limitations. First, it was a retrospective study with its inherent biases, and was performed in a single-center setting without a large sample size. Second, the method of PSM was used for this study, however, we could not control for the balance of all potential confounding variables. A prospective study with a large number of patients is required. Third, the different routes for EN support may influence the outcomes (51). Fourth, due to the limited sample size, subgroup analyses may have been underpowered. Last, VAP is difficult to diagnose. The prevalence of VAP varies according to the different diagnostic criteria, and its use affects the time to diagnosis and associated mortality rate (52).
The present study of early vs. late EN showed that early EN decreased the risk of VAP developing and reduced the duration of hospital stay in invasively ventilated patients with severe trauma. Abdominal injury, massive blood transfusion and lower albumin level were associated with delayed EN. Despite applying PSM to adjust for bias in the current study, randomized controlled trial is crucial to further corroborate the results.
The original contributions presented in this study are included in the article/supplementary material, further inquiries can be directed to the corresponding authors.
The studies involving human participants were reviewed and approved by the Ethics Committee of the Union Hospital (No. 0167-1), Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
XjZ, LY, and SW: conceptualization. XjZ and LY: supervision. RL, TZ, and ZL: investigation. QW, YW, JX, ZL, and JY: data curation. SW, XZ, QW, and YW: methodology. SW, XZ, and JX: writing–original draft preparation. XjZ, LY, RL, and TZ: writing–review and editing. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
ARDS, acute respiratory distress syndrome; APACHE II, acute physiology and chronic health evaluation II; BMI, body mass index; CCI, Charlson comorbidity index; CI, confidence interval; EN, enteral nutrition; GCS, Glasgow coma scale; GI, gastrointestinal; ICU, intensive care unit; ISS, injury severity score; MV, mechanical ventilation; OR, odds ratio; PSM, propensity score matching; SOFA, sequential organ failure assessment; VAP, ventilator-associated pneumonia.
1. Cavalcanti M, Ferrer M, Ferrer R, Morforte R, Garnacho A, Torres A. Risk and prognostic factors of ventilator-associated pneumonia in trauma patients. Crit Care Med. (2006) 34:1067–72. doi: 10.1097/01.Ccm.0000206471.44161.A0
2. Ferrer M, Torres A. Epidemiology of ICU-acquired pneumonia. Curr Opin Crit Care. (2018) 24:325–31. doi: 10.1097/mcc.0000000000000536
3. Mangram A, Sohn J, Zhou N, Hollingworth A, Ali-Osman F, Sucher J, et al. Trauma-associated pneumonia: time to redefine ventilator-associated pneumonia in trauma patients. Am J Surg. (2015) 210:1056–61; discussion 1061–2. doi: 10.1016/j.amjsurg.2015.06.029
4. Marjanovic N, Boisson M, Asehnoune K, Foucrier A, Lasocki S, Ichai C, et al. Continuous pneumatic regulation of tracheal cuff pressure to decrease ventilator-associated pneumonia in trauma patients who were mechanically ventilated: the AGATE multicenter randomized controlled study. Chest. (2021) 160:499–508. doi: 10.1016/j.chest.2021.03.007
5. Esnault P, Nguyen C, Bordes J, D’Aranda E, Montcriol A, Contargyris C, et al. Early-Onset ventilator-associated pneumonia in patients with severe traumatic brain injury: incidence, risk factors, and consequences in cerebral oxygenation and outcome. Neurocrit Care. (2017) 27:187–98. doi: 10.1007/s12028-017-0397-4
6. Dijkink S, Meier K, Krijnen P, Yeh D, Velmahos G, Schipper I. Malnutrition and its effects in severely injured trauma patients. Eur J Trauma Emerg Surg. (2020) 46:993–1004. doi: 10.1007/s00068-020-01304-5
7. Dhaliwal R, Heyland D. Nutrition and infection in the intensive care unit: what does the evidence show? Curr Opin Crit Care. (2005) 11:461–7. doi: 10.1097/01.ccx.0000176693.85260.cd
8. Artinian V, Krayem H, DiGiovine B. Effects of early enteral feeding on the outcome of critically ill mechanically ventilated medical patients. Chest. (2006) 129:960–7. doi: 10.1378/chest.129.4.960
9. Reignier J, Darmon M, Sonneville R, Borel A, Garrouste-Orgeas M, Ruckly S, et al. Impact of early nutrition and feeding route on outcomes of mechanically ventilated patients with shock: a post hoc marginal structural model study. Intensive Care Med. (2015) 41:875–86. doi: 10.1007/s00134-015-3730-4
10. Kompan L, Vidmar G, Spindler-Vesel A, Pecar J. Is early enteral nutrition a risk factor for gastric intolerance and pneumonia? Clin Nutr. (2004) 23:527–32. doi: 10.1016/j.clnu.2003.09.013
11. Doig G, Heighes P, Simpson F, Sweetman E. Early enteral nutrition reduces mortality in trauma patients requiring intensive care: a meta-analysis of randomised controlled trials. Injury. (2011) 42:50–6. doi: 10.1016/j.injury.2010.06.008
12. Reintam Blaser A, Starkopf J, Alhazzani W, Berger M, Casaer M, Deane A, et al. Early enteral nutrition in critically ill patients: ESICM clinical practice guidelines. Intensive Care Med. (2017) 43:380–98. doi: 10.1007/s00134-016-4665-0
13. Wang Y, Liu H, Wang Y, Zhang Y, Zhang J, Huang W, et al. Establishment of trauma treatment teams within a regional severe trauma treatment system in China: study protocol for a national cluster-randomised trial. BMJ Open. (2018) 8:e023347. doi: 10.1136/bmjopen-2018-023347
14. Akaraborworn O, Siribumrungwong B, Sangthong B, Thongkhao K. Massive blood transfusion for trauma score to predict massive blood transfusion in trauma. Crit Care Res Pract. (2021) 2021:3165390. doi: 10.1155/2021/3165390
15. McClave S, Taylor B, Martindale R, Warren M, Johnson D, Braunschweig C, et al. Guidelines for the provision and assessment of nutrition support therapy in the adult critically Ill patient: society of critical care medicine (SCCM) and American society for parenteral and enteral nutrition (A.S.P.E.N.). JPEN J Parenter Enteral Nutr. (2016) 40:159–211. doi: 10.1177/0148607115621863
16. Kalil A, Metersky M, Klompas M, Muscedere J, Sweeney D, Palmer L, et al. Management of adults with hospital-acquired and ventilator-associated Pneumonia: 2016 clinical practice guidelines by the infectious diseases society of America and the American thoracic society. Clin Infect Dis. (2016) 63:e61–111. doi: 10.1093/cid/ciw353
17. Rello J, Ollendorf D, Oster G, Vera-Llonch M, Bellm L, Redman R, et al. Epidemiology and outcomes of ventilator-associated pneumonia in a large US database. Chest. (2002) 122:2115–21. doi: 10.1378/chest.122.6.2115
18. Cook D, Walter S, Cook R, Griffith L, Guyatt G, Leasa D, et al. Incidence of and risk factors for ventilator-associated pneumonia in critically ill patients. Ann Intern Med. (1998) 129:433–40. doi: 10.7326/0003-4819-129-6-199809150-00002
19. Arumugam S, Mudali I, Strandvik G, El-Menyar A, Al-Hassani A, Al-Thani H. Risk factors for ventilator-associated pneumonia in trauma patients: a descriptive analysis. World J Emerg Med. (2018) 9:203–10. doi: 10.5847/wjem.j.1920-8642.2018.03.007
20. Tsilika M, Thoma G, Aidoni Z, Tsaousi G, Fotiadis K, Stavrou G, et al. A four-probiotic preparation for ventilator-associated pneumonia in multi-trauma patients: results of a randomized clinical trial. Int J Antimicrob Agents. (2022) 59:106471. doi: 10.1016/j.ijantimicag.2021.106471
21. Chen S, Bie R, Lai Y, Shi H, Ung C, Hu H. Trends and development in enteral nutrition application for ventilator associated pneumonia: a scientometric research study (1996-2018). Front Pharmacol. (2019) 10:246. doi: 10.3389/fphar.2019.00246
22. Ohbe H, Jo T, Matsui H, Fushimi K, Yasunaga H. Early enteral nutrition in patients with severe traumatic brain injury: a propensity score-matched analysis using a nationwide inpatient database in Japan. Am J Clin Nutr. (2020) 111:378–84. doi: 10.1093/ajcn/nqz290
23. Jin M, Zhang H, Lu B, Li Y, Wu D, Qian J, et al. The optimal timing of enteral nutrition and its effect on the prognosis of acute pancreatitis: a propensity score matched cohort study. Pancreatology. (2017) 17:651–7. doi: 10.1016/j.pan.2017.08.011
24. Kirsch R, Matthews K, Williams V. Using global criteria to detect malnutrition: application in disease states. Nutr Clin Pract. (2020) 35:85–97. doi: 10.1002/ncp.10444
25. Mogensen K, Robinson M, Casey J, Gunasekera N, Moromizato T, Rawn J, et al. Nutritional status and mortality in the critically Ill. Crit Care Med. (2015) 43:2605–15. doi: 10.1097/ccm.0000000000001306
26. Correia M, Waitzberg D. The impact of malnutrition on morbidity, mortality, length of hospital stay and costs evaluated through a multivariate model analysis. Clin Nutr. (2003) 22:235–9. doi: 10.1016/s0261-5614(02)00215-7
27. Alexander J. Nutrition and translocation. JPEN J Parenter Enteral Nutr. (1990) 14(5 Suppl):170s–4s. doi: 10.1177/014860719001400505
28. Jabbar A, Chang W, Dryden G, McClave S. Gut immunology and the differential response to feeding and starvation. Nutr Clin Pract. (2003) 18:461–82. doi: 10.1177/0115426503018006461
29. Lee J, Williams G, Kozar R, Kao L, Mueck K, Emerald A, et al. Multitargeted feeding strategies improve nutrition outcome and are associated with reduced pneumonia in a Level 1 trauma intensive care unit. JPEN J Parenter Enteral Nutr. (2018) 42:529–37. doi: 10.1177/0148607117699561
30. Bochicchio G, Bochicchio K, Joshi M, Ilahi O, Scalea T. Acute glucose elevation is highly predictive of infection and outcome in critically injured trauma patients. Ann Surg. (2010) 252:597–602. doi: 10.1097/SLA.0b013e3181f4e499
31. McClave S, Heyland D. The physiologic response and associated clinical benefits from provision of early enteral nutrition. Nutr Clin Pract. (2009) 24:305–15. doi: 10.1177/0884533609335176
32. Kudsk K. Current aspects of mucosal immunology and its influence by nutrition. Am J Surg. (2002) 183:390–8. doi: 10.1016/s0002-9610(02)00821-8
33. Wypych T, Wickramasinghe L, Marsland B. The influence of the microbiome on respiratory health. Nat Immunol. (2019) 20:1279–90. doi: 10.1038/s41590-019-0451-9
34. Samuelson D, Welsh D, Shellito J. Regulation of lung immunity and host defense by the intestinal microbiota. Front Microbiol. (2015) 6:1085. doi: 10.3389/fmicb.2015.01085
35. Kang W, Kudsk K. Is there evidence that the gut contributes to mucosal immunity in humans? JPEN J Parenter Enteral Nutr. (2007) 31:246–58. doi: 10.1177/0148607107031003246
36. Lin Y, Sun Z, Wang H, Liu M. The effects of gastrointestinal function on the incidence of ventilator-associated pneumonia in critically Ill patients. Open Med (Wars). (2018) 13:556–61. doi: 10.1515/med-2018-0082
37. Croce M, Brasel K, Coimbra R, Adams C Jr., Miller P, Pasquale M, et al. National trauma institute prospective evaluation of the ventilator bundle in trauma patients: does it really work? J Trauma Acute Care Surg. (2013) 74:354–60; discussion 60–2. doi: 10.1097/TA.0b013e31827a0c65
38. Stewart M, Biddle M, Thomas T. Evaluation of current feeding practices in the critically ill: a retrospective chart review. Intensive Crit Care Nurs. (2017) 38:24–30. doi: 10.1016/j.iccn.2016.05.004
39. Rupert A, Seres D, Li J, Faye A, Jin Z, Freedberg D. Factors associated with delayed enteral nutrition in the intensive care unit: a propensity score-matched retrospective cohort study. Am J Clin Nutr. (2021) 114:295–302. doi: 10.1093/ajcn/nqab023
40. Yin J, Wang J, Zhang S, Yao D, Mao Q, Kong W, et al. Early versus delayed enteral feeding in patients with abdominal trauma: a retrospective cohort study. Eur J Trauma Emerg Surg. (2015) 41:99–105. doi: 10.1007/s00068-014-0425-4
41. Moore S, Burlew C. Nutrition support in the open abdomen. Nutr Clin Pract. (2016) 31:9–13. doi: 10.1177/0884533615620420
42. Dissanaike S, Pham T, Shalhub S, Warner K, Hennessy L, Moore E, et al. Effect of immediate enteral feeding on trauma patients with an open abdomen: protection from nosocomial infections. J Am Coll Surg. (2008) 207:690–7. doi: 10.1016/j.jamcollsurg.2008.06.332
43. Chow J, Richards J, Galvagno S, Coleman P, Lankford A, Hendrix C, et al. The algorithm examining the risk of massive transfusion (ALERT) score accurately predicts massive transfusion at the scene of injury and on arrival to the trauma bay: a retrospective analysis. Shock. (2021) 56:529–36. doi: 10.1097/shk.0000000000001772
44. McQuiggan M, Kozar R, Sailors R, Ahn C, McKinley B, Moore F. Enteral glutamine during active shock resuscitation is safe and enhances tolerance of enteral feeding. JPEN J Parenter Enteral Nutr. (2008) 32:28–35. doi: 10.1177/014860710803200128
45. Patel J, Rice T, Heyland D. Safety and outcomes of early enteral nutrition in circulatory shock. JPEN J Parenter Enteral Nutr. (2020) 44:779–84. doi: 10.1002/jpen.1793
46. Younan D, Delozier S, Adamski J, Loudon A, Violette A, Ustin J, et al. Factors predictive of ventilator-associated Pneumonia in critically Ill Trauma patients. World J Surg. (2020) 44:1121–5. doi: 10.1007/s00268-019-05286-3
47. Torrance H, Brohi K, Pearse R, Mein C, Wozniak E, Prowle J, et al. Association between gene expression biomarkers of immunosuppression and blood transfusion in severely injured polytrauma patients. Ann Surg. (2015) 261:751–9. doi: 10.1097/sla.0000000000000653
48. Evans D, Corkins M, Malone A, Miller S, Mogensen K, Guenter P, et al. The use of visceral proteins as nutrition markers: an ASPEN position paper. Nutr Clin Pract. (2021) 36:22–8. doi: 10.1002/ncp.10588
49. Doweiko J, Nompleggi D. The role of albumin in human physiology and pathophysiology, Part III: albumin and disease states. JPEN J Parenter Enteral Nutr. (1991) 15:476–83. doi: 10.1177/0148607191015004476
50. Elke G, Felbinger T, Heyland D. Gastric residual volume in critically ill patients: a dead marker or still alive? Nutr Clin Pract. (2015) 30:59–71. doi: 10.1177/0884533614562841
51. Zhu Y, Yin H, Zhang R, Ye X, Wei J. Gastric versus postpyloric enteral nutrition in elderly patients (age =?75 years) on mechanical ventilation: a single-center randomized trial. Crit Care. (2018) 22:170. doi: 10.1186/s13054-018-2092-z
Keywords: early enteral nutrition, ventilator-associated pneumonia, severe trauma patients, invasive mechanical ventilation, propensity score matching (PSM)
Citation: Wang S, Zhao X, Wang Q, Wu Y, Xu J, Li R, Zhou T, Lv Z, Yang J, Yang L and Zou X (2023) Impact of early enteral nutrition on ventilator associated pneumonia in intubated severe trauma patients: A propensity score-matched study. Front. Nutr. 10:1172526. doi: 10.3389/fnut.2023.1172526
Received: 23 February 2023; Accepted: 28 March 2023;
Published: 12 April 2023.
Edited by:
Aurora Serralde, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán (INCMNSZ), MexicoReviewed by:
Carlo Pedrolli, Azienda Provinciale per i Servizi Sanitari (APSS), ItalyCopyright © 2023 Wang, Zhao, Wang, Wu, Xu, Li, Zhou, Lv, Yang, Yang and Zou. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xiaojing Zou, MjQ5MTI2NzM0QHFxLmNvbQ==; Le Yang, MjQ5MTIzNTcwQHFxLmNvbQ==
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.