 Jiutian Huang
Jiutian Huang Ziyi He
Ziyi He Minhui Xu
Minhui Xu Jianing Du
Jianing Du Yun-tao Zhao
Yun-tao Zhao
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Nutr. , 13 July 2023
Sec. Nutritional Epidemiology
Volume 10 - 2023 | https://doi.org/10.3389/fnut.2023.1161175
This article is part of the Research Topic Diet Behavior and Heart Health View all 21 articles
Background: Previous studies found that increasing vegetable intake benefits are reduced after adjustment for socioeconomic factors. Using genetic variation as an instrumental variable for vegetable intake and socioeconomic status, we investigated the relationship between vegetable intake and ischemic cardio-cerebral vascular diseases and focused on whether socioeconomic status was a possible confounder.
Methods: From three independent genome-wide association studies, we extracted instrumental variables reflecting raw and cooked vegetable intake, which were used to perform Mendelian randomization analysis. To evaluate the effects of socioeconomic factors on vegetable intake, univariate and multivariate Mendelian randomization analyses were performed using single nucleotide polymorphisms representing education attainment and household income reported in the literature. We also performed outlier assessment and a series of sensitivity analyses to confirm the results.
Results: Genetically predicted raw and cooked vegetable intake were not associated with any ischemic cardio-cerebral vascular diseases and lipid components after Bonferroni correction. Univariate Mendelian randomized analysis revealed that raw vegetable intake was positively correlated with education attainment (β = 0.04, p = 0.029) and household income (β = 0.07, p < 0.001). Multivariate Mendelian randomized model showed a positive correlation between household income and raw vegetable intake (β = 0.06, p = 0.004). Socioeconomic status was closely associated with eating habits and lifestyle related to the risk of cardiovascular diseases.
Conclusion: Genetically determined raw and cooked vegetable intake was not associated with significant benefits in terms of ischemic cardio-cerebral vascular diseases while genetically determined socioeconomic status may have an impact on vegetable intake. Socioeconomic status, which was closely associated with other eating habits and lifestyle, may affect the association between vegetable intake and ischemic cardio-cerebral vascular diseases.
Ischemic cardio-cerebral vascular diseases are the leading cause of death and decreased quality of life worldwide (1–3). Increased vegetable intake is widely recommended in the cardiovascular disease (CVD) field (4, 5). Many observational studies support the benefits of increased vegetable intake (6, 7), including lowering serum lipids and preventing chronic disease. However, the independent effects of raw and cooked vegetables on ischemic cardiovascular disease are poorly understood, and results vary in traditional epidemiological studies (8–12).
Socioeconomic status (SES), such as education attainment and household income, has a significant impact on the occurrence of cardiovascular disease (13). A large study found that those with primary education had an increased risk of cardiovascular disease, cardiovascular event mortality, and all-cause mortality compared with those with higher education (14). Patients with financial barriers are at higher risk of future CVD events (15). Socioeconomic status can limit access to fresh vegetables and fruits due to a lack of health literacy and high prices (16, 17). Several studies found that increasing vegetable intake benefits are reduced after adjustment for socioeconomic factors (8, 10, 18). And the risk of ischemic cardio-cerebral vascular disease is related to various lifestyle factors, including diet, smoking, drinking, physical inactivity, etc. (19–22), which are also closely related to education attainment and household income (14, 23, 24).
The Mendelian randomization (MR) approach has been widely used to assess the causal effects of risk factors on disease. Relying on pooled data from genome-wide association studies (GWAS) (25), the MR approach uses genetic variants, randomly assigned to individuals at conception, as instrumental variables (IVs) to analyze causal relationships between exposure and outcome. When performed carefully, MR analysis largely overcomes the limitations of confounders and avoids the bias of typical observational studies (26). Several previous Mendelian randomization studies (12, 27, 28) have found that vegetable intake did not reduce certain metabolic risk factors and the risk of some cardiovascular events. We aimed to estimate the effects of vegetable intake on ischemic cardio-cerebral vascular disease risk and serum lipids and to focus on the influence of socioeconomic status on vegetable intake, other eating habits, and lifestyle.
We designed a one-sample Mendelian Randomization study to evaluate how vegetable intake was related to ischemic heart disease and ischemic stroke. We selected angina, acute myocardial infarction, chronic ischemic heart disease, and cerebral infarction as our outcome variables. Considering the genetic connection between instrumental variables used for the intake of raw and cooked vegetables, both univariable and multivariable MR studies were used to assess the causal relationship between exposure and outcome. After discovering a lack of clear causal relationship between vegetable intake and ischemic cardiovascular events, we further conducted a multivariable Mendelian Randomization study to estimate the potential impact of socioeconomic status on vegetable intake, and we also attempted to prove that this impact is equally widespread in other dietary habits and lifestyle (Figure 1).
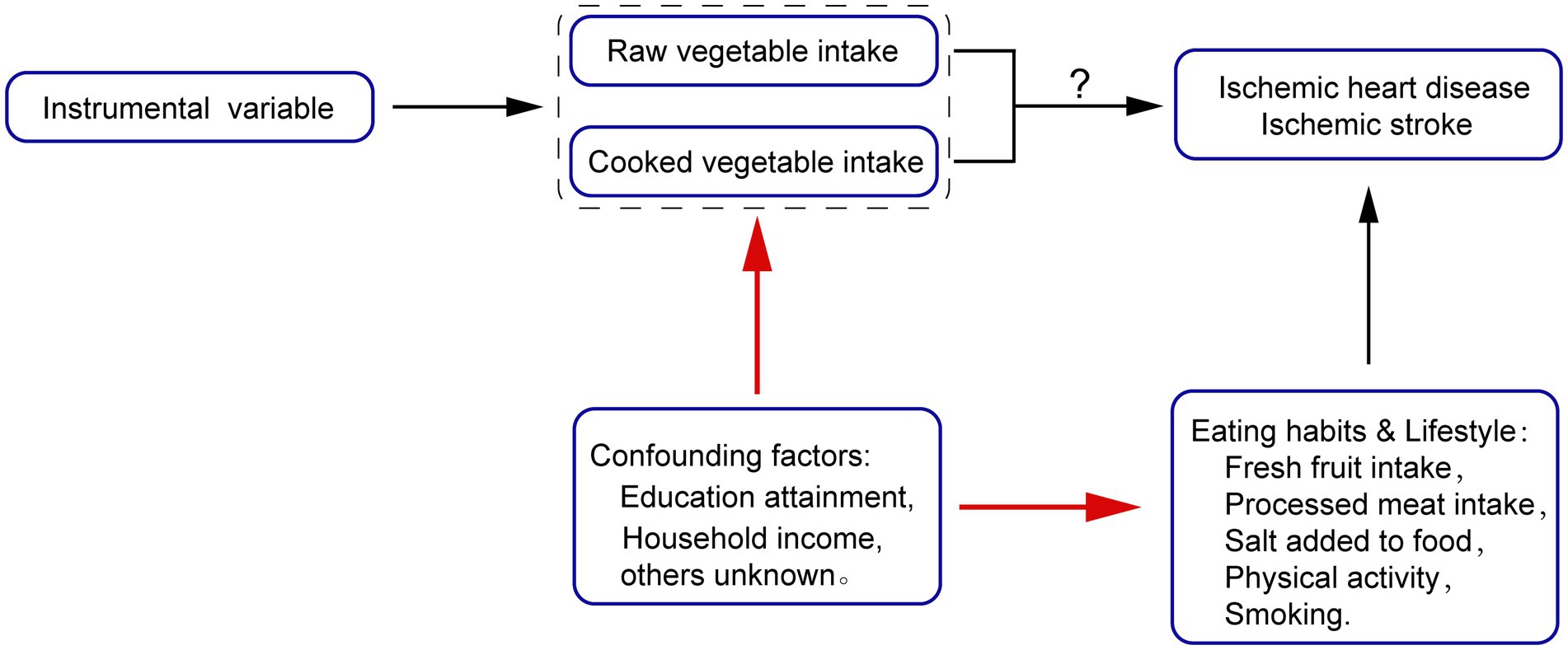
Figure 1. Mendelian Randomization (MR) Model of our study.
Genetic instrumental variables reflecting vegetable intake were derived from three independent UK Biobank-based GWAS (Supplementary Table S1) (29–31). The measures of dietary intake, including vegetable intake, in UK Biobank are based on self-reported questionnaire data. We identified single nucleotide polymorphisms (SNPs) with a genome-wide significant p value (<5 × 10−8) associated with phenotypes. After removing duplicate SNPs, we obtained 39 SNPs reflecting raw vegetable intake, and 25 reflecting cooked vegetable intake. The SNP rs12629972 was excluded because it reflected both raw and cooked vegetable intake. We also excluded palindrome SNPs with intermediate allele frequencies (>0.42) or indel genetic variants. To account for the possibility that the three GWAS may have identified interrelated SNPs as reflecting vegetable intake, we used LDlink to remove SNPs in linkage disequilibrium (32). If a pair of SNPs had LD R2 > 0.01, the SNP with the higher p value was removed. Finally, we used PhenoScanner, a curated database of publicly available results from large-scale genetic association studies in humans (33), to check whether each SNP was associated with potential confounders (p < 5 × 10−8, proxies for European: R2 > 0.8). Rs11191193 was excluded because of its significant genetic association with educational attainment, and rs838133 because it was directly associated with total cholesterol. Finally, we used 18 SNPs reflecting raw vegetable/salad intake and 11 SNPs reflecting cooked vegetable intake for MR analysis (Supplementary Tables S2, S3). Supplementary Figures S1, S2 show the detailed selection process. Proxy SNPs (minimum linkage disequilibrium R2 = 0.8) were used for vegetable intake-associated SNPs that were unavailable in outcome datasets. Some studies have shown that these SNPs may influence people’s dietary preferences and alter genetically determined raw and cooked vegetable intake through senses such as olfaction and taste (34, 35).
In addition, in order to get a more definite conclusion, we also directly extracted the instrumental variables from MRC-IEU. The visualization results of the exposed GWAS can be obtained in Supplementary Figures S3, S4. 18 and 17 SNP were used to reflex raw and cooked vegetables, respectively. Considering that some of the SNPs may have never been reported or used, we calculated the F statistic () for each SNP to test for a weak instrumental variable bias. F statistics for all variables were over 10, and weak instrument bias was avoided in principle (Supplementary Tables S4, S5) (36).
Genetic associations with education attainment were obtained from the GWAS conducted under the auspices of the Social Science Genetic Association Consortium, which reported 74 genome-wide significant loci associated with educational attainment in people of European descent (n = 293,723) (37). Educational attainment was measured by the number of years of schooling completed (EduYears, mean = 14.3, SD = 3.6). 12 loci that were unavailable in the target data-set were removed and the remaining 62 loci have been retained (Supplementary Table S6). The SNPs used as instrumental variables related to household income were derived from Shi et al. (38). The same method was used to extract the genetic association of the 54 SNPs with education attainment and vegetable intake. Of 54 SNPs, 5 were unavailable and removed; the remaining 49 SNPs were retained to perform further analysis (Supplementary Table S7). SNPs associated with education attainment may affect years of education by altering neurodevelopment at different stages. For example, rs4500960 may be related to developmental biology, brain size, and cerebra core methodology, while rs61160187 is closely related to transcription factor binding and negative regulation of signal transmission (37). And SNPs associated with household income are associated with intracranial volume, infant head circumference, and level of cognitive ability (39).
The primary outcomes included ischemic cardio-cerebral vascular diseases diagnosed by the International Classification of Diseases version, Tenth Version, with the following ICD-10 codes: I20 (angina pectoris), I21 (acute myocardial infarction), I25 (chronic ischemic heart disease), and I63 (cerebral infarction). Data were acquired from the UK Biobank summary statistics curated in the MRC-IEU Open GWAS database or provided by Neale Lab (40). Serum lipid and lipoprotein levels were measured using the Nightingale high-throughput NMR metabolomics platform in 2020, and blood samples were provided by UK Biobank. GWAS results based on these metabolic biomarkers can be obtained from MRC-IEU (European, N = 115,078).
The raw and cooked vegetable intake as well as vegetarian alternatives intake used as outcome variables in MVMR were obtained from MRC-IEU. To illustrate the broad impact of education attainment and household income on IHD risk was not limited to the preferences for vegetable intake, we also obtained a series of outcome variables related to diet and lifestyle, including fresh fruit intake, processed meat intake, salt add to food and smoking (from MRC-IEU) and physical activity (from Within family GWAS consortium). Source and relevant information of result variables used in the study can be acquired from Supplementary Table S8.
We used the inverse-variance weighted (IVW) method as the main method to evaluate the causal effect of exposure and outcome. Due to the potential genetic association between raw and cooked vegetables, as well as between education and household income, we used the multivariate Mendelian method to analyze their independent effects. The SNPs used to conduct multivariable MR were combinations of instrumental variables of each exposure in univariable MR. We calculated the odds ratio (OR) and 95% confidence interval (CI). Cochrane’s Q-statistic was used to assess the heterogeneity of SNP effects (Supplementary Tables S15, S16). If significant heterogeneity was observed, a random-effects IVW model was applied. For sensitivity analyses, we used three complementary methods with different assumptions for valid estimates. MR-Egger lacks statistical power for assessment of causal effects and provides wider confidence intervals, but can detect horizontal pleiotropy by p value for its intercept term (Supplementary Table S14) (41). A weighted median method generates homogeneous causal estimates, although >50% of weights derived in the analysis arise from invalid instrumental variables (42). Mendelian Randomization Pleiotropy RESidual Sum and Outlier (MR-PRESSO) can identify outlying SNPs and correct for horizontal pleiotropy through their exclusion (Supplementary Table S13) (43). Additionally, we performed leave-one-out sensitivity analysis to identify potentially highly influential SNPs (Supplementary Figures S5–S12).
All statistical analyses were performed in R (version 4.1.3, R Foundation for Statistical Computing, Vienna, Austria), with MR analyses performed using the TwoSampleMR package (version 0.5.6) (44), MRPRESSO package (version 1.0) (43), and MVMR package (45). Statistical significance was set at a two-sided p value < 0.05. Bonferroni correction of the evidential threshold was based on the number of exposures (p value <0.05/the number of exposures).
Genetically predicted raw and cooked vegetable intake (IVs from three UK biobank based GWAS) were not associated with any ischemic cardiovascular diseases according to IVW analysis (P>0.05) (Table 1). The multivariate MR (IVs from three UK biobank based GWAS) observed a correlation between cooked vegetable intake and an increased risk of Chronic ischemic heart disease (OR 1.02; 95% CI 1.00, 1.04; p = 0.042) (Table 1), but did not exceed the significance level of Bonferroni correction (p > 0.0125). IVW analysis also showed that genetically predicted raw and cooked vegetable intake (IVs from MRC-IEU) were not associated with any ischemic cardiovascular diseases (Supplementary Table S9; Supplementary Figures S13, S14).
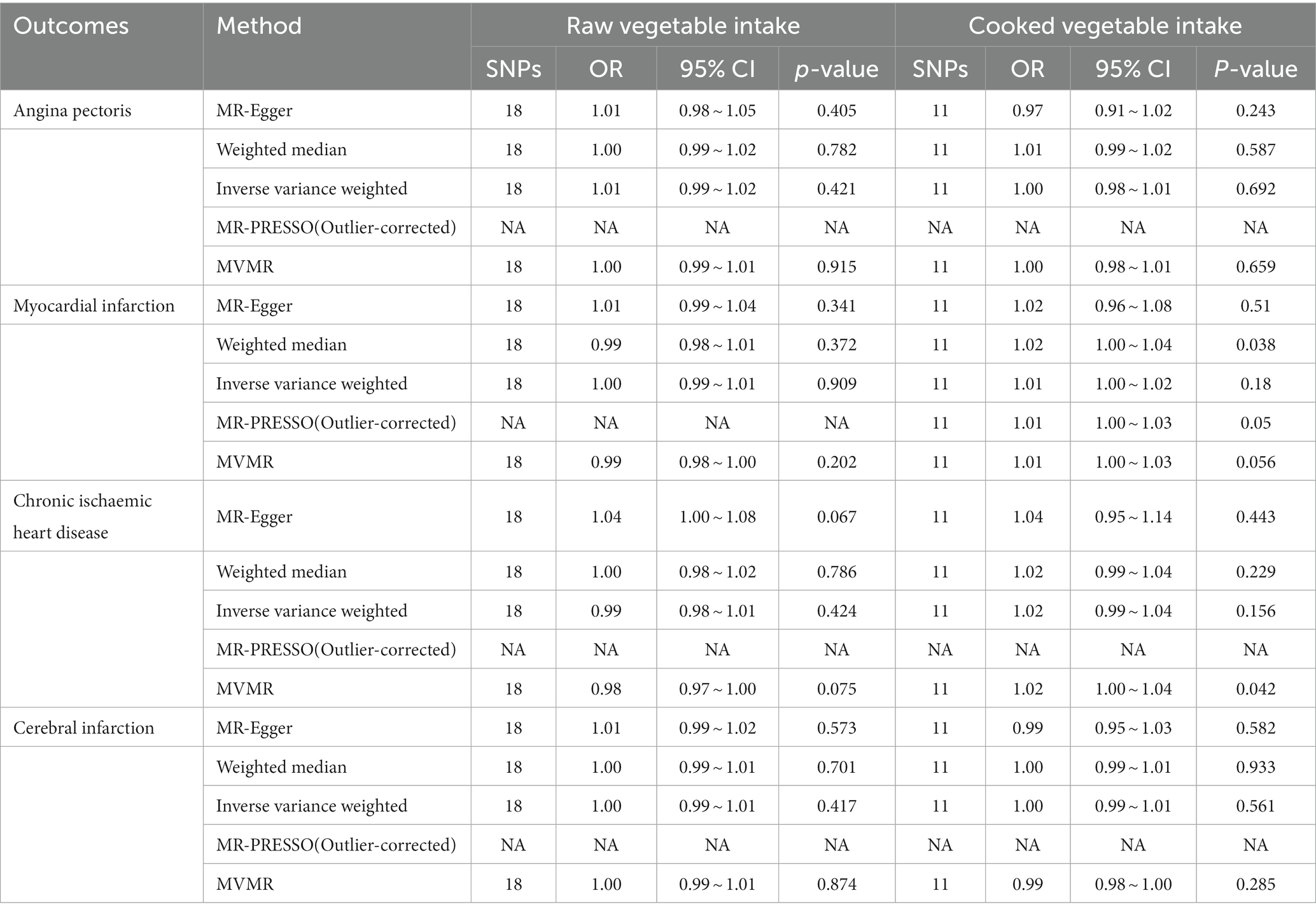
Table 1. Estimates given as odds ratios (ORs) and 95% confidence intervals for the effect of raw and cooked vegetable intake on ischemic cardio-cerebral vascular diseases.
IVW analysis showed that genetically predicted raw vegetable intake (IVs from three UK biobank based GWAS) was associated with reduced low-density lipoprotein cholesterol (LDL-C) (β −0.25; 95% CI −0.44, −0.07; p = 0.006) and apolipoprotein B (ApoB) (β −0.28; 95% CI −0.43, −0.12; p < 0.001) (Supplementary Tables S10, S11). MVMR analysis showed that raw vegetable intake was only associated with reduced ApoB (β −0.22; 95% CI −0.38, −0.06; p = 0.013), but did not exceed the significance level of Bonferroni correction (p > 0.0083) (Supplementary Tables S10, S11). Cooked vegetable intake did not significantly influence serum lipid components according to the IVW and MVMR analysis. Results of Mendelian randomization analysis of genetically predicted vegetable intake (IVs from MRC-EU) and lipid profiles are presented in Supplementary Tables S12; Supplementary Figures S15, S16.
We conducted univariable MR analysis to explore the impact of education attainment and household income on raw and cooked vegetable intake. People with higher education attainment tended to eat more raw vegetables (IVW: β 0.04; 95% CI 0.00, 0.08; p = 0.029). Similarly, people with higher household income tended to eat more raw vegetables (IVW: β 0.07; 95% CI 0.03, 0.11; P<0.001) and vegetarian alternatives intake (IVW: β 0.02; 95% CI 0.00, 0.04; p = 0.042), while we did not find the impact of social-economic conditions on cooked vegetable intake (Figure 2).
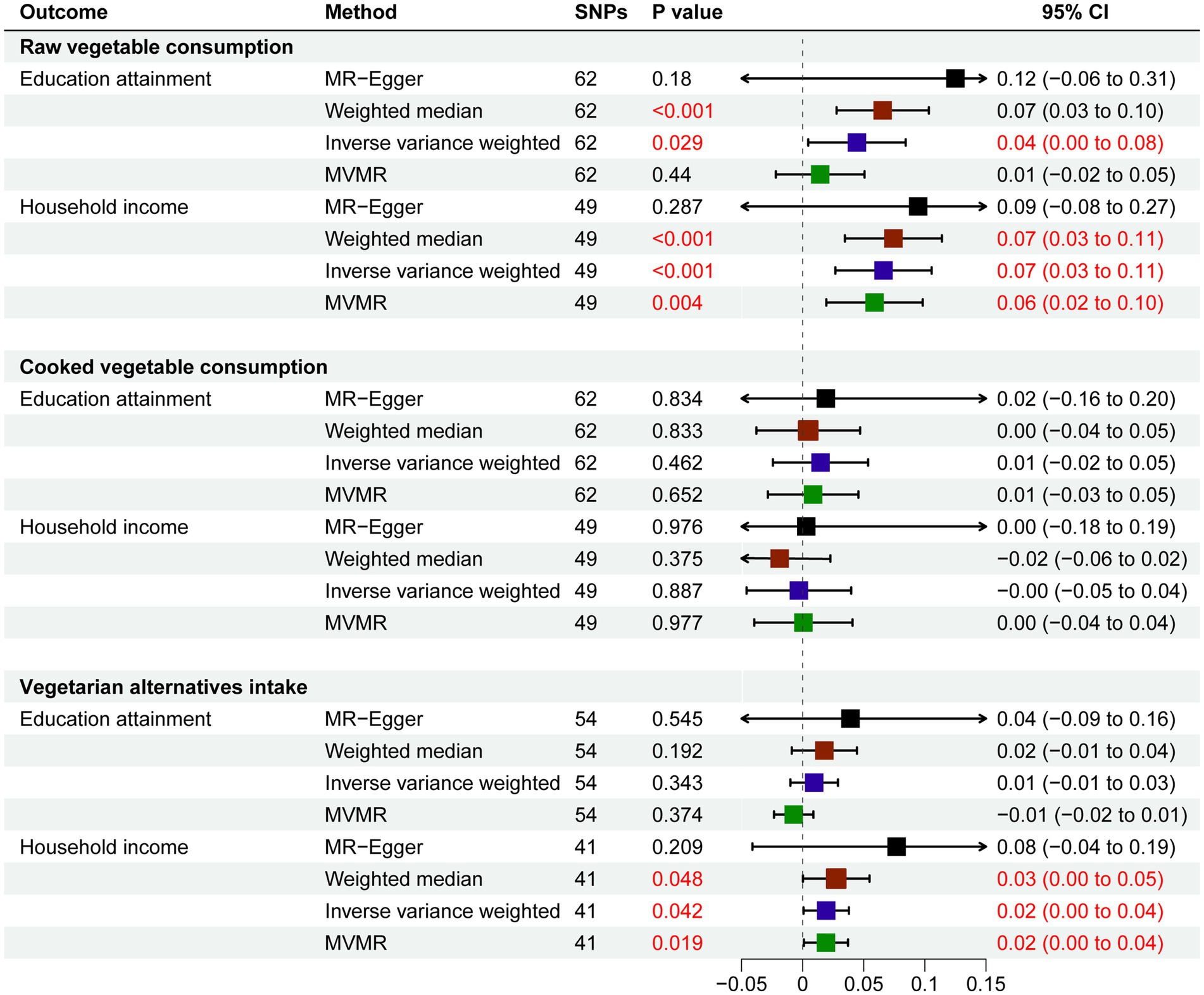
Figure 2. Estimates Given as Beta and 95% Confidence Intervals for the Effect of Education Attainment and Household Income on Vegetable Consumption.
Considering that education and income are related genetically and socially, we next performed MVMR. In the MVMR model, education attainment had a weakened influence on raw vegetable intake (β 0.01; 95% CI −0.02, 0.05; p = 0.440). Household income was still positively related to raw vegetable intake (β 0.06; 95% CI 0.02, 0.10; p = 0.004) and vegetarian alternatives intake (IVW: β 0.02; 95% CI 0.00, 0.04; p = 0.019) (Figure 2).
Finally, we conducted univariable MR analysis to explore the impact of education attainment and household income on other eating habits and lifestyle to show that socioeconomic status has an extremely broad impact on ischemic cardio-cerebral vascular diseases. People with higher education attainment and household income tended to eat more fresh fruit intake (IVW: β 0.09; p < 0.001) (IVW: β 0.09; p < 0.001), eat less processed meat (IVW: β −0.06; p = 0.028) (IVW: β −0.10; p = 0.001), add less salt to food (IVW: β −0.15; p < 0.001) (IVW: β −0.14; p < 0.001), have more physical activity (IVW: β 0.07; p = 0.002) (IVW: β 0.06; p = 0.004) and smoke less (IVW: β −0.23; p < 0.001) (IVW: β −0.42; p < 0.001; Figure 3).
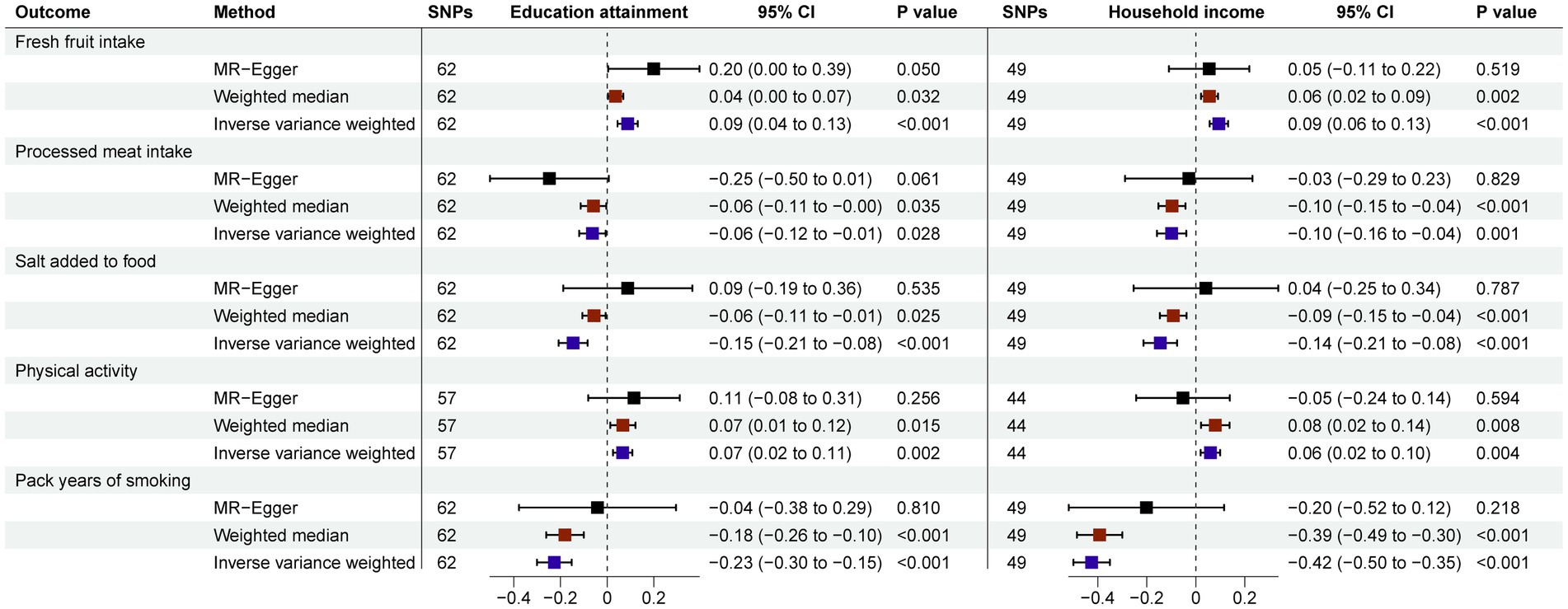
Figure 3. Estimates Given as Beta and 95% Confidence Intervals for the Effect of Education Attainment and Household Income on Eating Habits and Lifestyle.
Our results showed that genetic variant-determined increases in raw or cooked vegetable intake did not confer a benefit in terms of ischemic cardio-cerebral vascular diseases. Increased raw vegetable intake may reduce LDL-C and ApoB levels. In addition, socioeconomic status, including income and education, have positive effects on raw vegetable intake in persons of European ancestry. Meanwhile, socioeconomic status had an extremely broad impact on other eating habits and lifestyle.
Worldwide dietary guidelines (4, 5) include recommendations for increased vegetable intake to reduce the risk of CVD, but the independent effects of raw versus cooked vegetables by different epidemiological studies have yielded inconsistent results. Leenders et al. (9) reported that vegetable intake was associated with lower CVD mortality, with a stronger association for raw vegetables. Miller et al. (10) showed that CVD incidence was only associated with high cooked vegetable intake. In a large prospective cohort study (8), total and raw vegetable intake was inversely associated with cardiovascular disease outcomes. Systematic reviews have shown that total vegetable intake is associated with reduced CVD incidence and stroke risk (46–48). A Mendelian randomization study (27) has found no evidence of an association between cooked and raw vegetable intake and coronary heart disease, heart failure, or atrial fibrillation. Since the Mendelian randomization method can reduce the unknown confounders, different results between conventional epidemiological studies and Mendelian randomization studies may be related to differences in study populations and research methods, and insufficient adjustment for confounding factors in conventional epidemiological studies. High-vegetable diets are generally lower in calories, fat, sodium, and glycemic load, which are well-established risk factors for ischemic cardio-cerebral vascular diseases (11, 49). It may be a lack of significance in merely increasing vegetable intake without controlling for other variables such as salt intake and total energy intake. And the impact of diet on health outcomes is complex. It is important to control for consistency in overall dietary patterns when assessing the health effects of single foods or nutrients (30).
LDL-C and other apolipoproteins play central roles in ischemic cardio-cerebral vascular disease occurrence and progression (50–52). Increased vegetable intake may improve plasma lipid profiles, potentially protecting against ischemic cardio-cerebral vascular diseases. Our findings indicated that increased vegetable intake did not significantly improve lipoproteins, except that raw vegetable intake may be associated with improved LDL-C and ApoB. Although increased vegetable intake has been associated with lower plasma LDL-C in observational studies (53, 54), randomized controlled trial results suggest that increased vegetable intake has negligible effects on plasma cholesterol component concentrations (55, 56). This suggests that although increased vegetable intake may have some beneficial influence on lipid profile, the benefits may be insufficient to yield clinical effects. There are several possible reasons for the different effects of raw and cooked vegetables on lipoproteins. Cooking vegetables may increase salt and fat intake, which are linked to CVD morbidity and mortality (57, 58). Cooking improves food safety and food digestibility but also impairs food quality, resulting in the loss of certain nutrients (59–61). Moreover, different types of vegetables may be eaten differently (8).
Low socioeconomic status has been associated with the development of ischemic cardio cerebral vascular disease and may confer comparable cardiovascular risks to traditional risk factors (62, 63). A prospective cohort study demonstrated that adults with low SES are at higher risk of CVD mortality and cardiovascular events than adults with high SES, partly mediated by lifestyle (64). The increased CVD burden in low SES populations may be due to a range of biological, behavioral, and psychosocial risk factors (13). In our screening of instrumental variables of vegetable intake, rs11191193 had significant genetic associations with educational attainment. Roos et al. (65) showed that household education level is an important determinant of raw vegetable intake. A large study found that individuals with primary school education had an increased risk of cardiovascular disease and cardiovascular mortality compared with those with higher education (14). An MR study (66) reported an inverse association between genetically determined educational attainment and CAD risk. And there is a strong association between genetically determined educational attainment and risk factors such as smoking, body mass index, and hypertension (66). One analysis suggested that most CHD risk among individuals with low education is due to behavioral and biological risk factors, with the main contributors being smoking, physical inactivity, and hypertension (23). The level of education may affect the ability to develop health literacy and access to healthy lifestyle and dietary recommendations (16, 67), leading to changes in vegetable intake as well as other lifestyle. Income levels have been consistently associated with CVD risk (14). Population analysis studies of atherosclerosis risk in communities have shown that living in deprived areas is associated with a higher incidence of coronary heart disease (68). The increased risk of CVD in low-income groups may be related to poor dietary choices and increased costs of healthy foods. In low-income areas with limited access, there are more fast food restaurants, fewer supermarkets, and fewer brand options, resulting in limited access to fresh fruits and vegetables (17, 69–71). Economic differences can affect not only the availability of resources but also the promotion or maintenance of a healthy lifestyle (72, 73).
Higher income and higher education attainment may be associated with improved health perceptions and lifestyle factors (74, 75), potentially explaining the positive conclusions of studies that did not fully adjust for socioeconomic status. In a large prospective cohort study (8), total and raw vegetable intake was inversely associated with cardiovascular disease outcomes. However, these associations significantly decreased after adjustment for potential confounders, such as socioeconomic status and lifestyle factors. Results from a cohort study (10) showed that higher vegetable intake was inversely associated with major cardiovascular disease, myocardial infarction, and cardiovascular mortality in models adjusted only for age, sex, and center. After multivariable adjustment including socioeconomic status, the association was significantly attenuated, and only non-cardiovascular mortality and total mortality remained significant. Similarly, in another study from China (18), higher vegetable intake was associated with lower CVD mortality risk in a minimally adjusted model, and the association was no longer significant after adjustment for factors such as socioeconomic status. Given the complex interrelationships between socioeconomic status, eating habits, lifestyle, and health outcomes, it is important to adjust for socioeconomic status to reduce bias.
Our study has several strengths. We investigated the independent effects of raw and cooked vegetable intake on ischemic cardio-cerebral vascular diseases and lipid profiles. Compared with traditional observational studies, MR studies reduce the effects of unknown confounders and reverse causality (30). Especially, by using the Mendelian randomization analysis, we examined the impact of socioeconomic factors on vegetable intake, other eating habits, and lifestyle, confirming that the effects of education and income on dietary habits and lifestyle are relatively common and may be extremely important confounders in previous studies.
Our work had several limitations. Our selected GWAS for vegetable intake did not report specific intake characteristics, such as vegetable type. Therefore, we could not perform a stratified MR analysis by vegetable type, which would help draw more valuable causal inferences. Additionally, our MR study was restricted to individuals of European ancestry (76). Due to differences in genetic background and eating habits, similar studies should be conducted on a larger scale around the world. Moreover, the SNPs of the utilized GWAS were all self-reported, which may differ from the actual intake, potentially introducing some bias to the results. Individuals tend to report more healthy foods and less unhealthy foods, and people with a high BMI tend to report less food intake (77, 78). Diet changes over time may also be a potential limitation (79). Furthermore, we selected two sample datasets with a large proportion of the population overlapping, which may increase the bias in the direction of the observed association and the inflation of the Type I error rate and false-positive results (80). Finally, MR relies on assumptions that genetic tools are associated with exposure, independent of potential confounders and that genetic tools are associated with outcomes only through exposure. Although we speculated about the possible mechanism of action of the instrumental variable SNPs, the effect of the SNP on the function of the gene product is unknown and is based only on a statistical association between gene and apparent effect (81). We cannot completely avoid horizontal pleiotropic effects because it is difficult to determine the biological function of exact genetic variants. There remains a need for further high-quality GWAS and MR analyses.
Our results showed that genetically determined raw and cooked vegetable intake was not associated with significant benefits related to ischemic cardio-cerebral vascular disease. Genetically determined socioeconomic status may have an impact on vegetable intake. Additionally, socioeconomic status, which was closely associated with other eating habits and lifestyle, may affect the association between vegetable intake and ischemic cardio-cerebral vascular diseases.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
JH and ZH: design the study and draft the work. MX and JD: data collection and statistical analysis. Y-tZ: design the study and revise it critically for important intellectual content. All authors contributed to the article and approved the submitted version.
We want to acknowledge participants and investigators from the IEU Open GWAS Project and the creator of MRC-IEU UK Biobank GWAS pipeline. If there is no open systematic data platform provided by them, there will be no such research. We do thank Stephen Burgess and Deborah A. Lawlor, for their selfless help with data statistics. We acknowledge Tai-kang Yao and Zhi-fei Li for contributing his ideas and providing suggestions. We thanks to all the participating authors.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnut.2023.1161175/full#supplementary-material
ApoB, apolipoprotein B; CI, confidence interval; CVD, cardiovascular disease; IEU, Integrative Epidemiology Unit; IVs, instrumental variables; IVW, inverse-variance weighted; GWAS, genome-wide association studies; LDL-C, low-density lipoprotein cholesterol; MR, Mendelian randomization; MVMR, multivariable Mendelian randomization; OR, odds ratio; SES, socioeconomic status; SNPs, single nucleotide polymorphisms.
1. GBD 2017 Causes of Death Collaborators. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. (2018) 392:1736–88. doi: 10.1016/S0140-6736(18)32203-7
2. Celermajer, DS, Chow, CK, Marijon, E, Anstey, NM, and Woo, KS. Cardiovascular disease in the developing world: prevalences, patterns, and the potential of early disease detection. J Am Coll Cardiol. (2012) 60:1207–16. doi: 10.1016/j.jacc.2012.03.074
3. Thomas, H, Diamond, J, Vieco, A, Chaudhuri, S, Shinnar, E, Cromer, S, et al. Global atlas of cardiovascular disease 2000-2016: the path to prevention and control. Glob Heart. (2018) 13:143–63. doi: 10.1016/j.gheart.2018.09.511
4. National Health and Medical Research Council. Australian dietary guidelines. Available at: https://www.eatforhealth.gov.au/guidelines (2013).
5. United States Department of Agriculture. 2015 – 2020 dietary guidelines for Americans. 8th ed Available at: http://health.gov/dietaryguidelines/2015/guidelines/ (2015).
6. Wang, DD, Li, Y, Bhupathiraju, SN, Rosner, BA, Sun, Q, Giovannucci, EL, et al. Fruit and vegetable intake and mortality: results from 2 prospective cohort studies of US men and women and a meta-analysis of 26 cohort studies. Circulation. (2021) 143:1642–54. doi: 10.1161/CIRCULATIONAHA.120.048996
7. Alissa, EM, and Ferns, GA. Dietary fruits and vegetables and cardiovascular diseases risk. Crit Rev Food Sci Nutr. (2017) 57:1950–62. doi: 10.1080/10408398.2015.1040487
8. Feng, Q, Kim, JH, Omiyale, W, Besevic, J, Conroy, M, May, M, et al. Raw and cooked vegetable consumption and risk of cardiovascular disease: a study of 400,000 adults in UK biobank. Front Nutr. (2022) 9:831470. doi: 10.3389/fnut.2022.831470
9. Leenders, M, Sluijs, I, Ros, MM, Boshuizen, HC, Siersema, PD, Ferrari, P, et al. Fruit and vegetable consumption and mortality: European prospective investigation into cancer and nutrition. Am J Epidemiol. (2013) 178:590–602. doi: 10.1093/aje/kwt006
10. Miller, V, Mente, A, Dehghan, M, Rangarajan, S, Zhang, X, Swaminathan, S, et al. Fruit, vegetable, and legume intake, and cardiovascular disease and deaths in 18 countries (PURE): a prospective cohort study. Lancet. (2017) 390:2037–49. doi: 10.1016/S0140-6736(17)32253-5
11. Aune, D, Giovannucci, E, Boffetta, P, Fadnes, LT, Keum, N, Norat, T, et al. Fruit and vegetable intake and the risk of cardiovascular disease, total cancer and all-cause mortality-a systematic review and dose-response meta-analysis of prospective studies. Int J Epidemiol. (2017) 46:1029–56. doi: 10.1093/ije/dyw319
12. Kobylecki, CJ, Afzal, S, Davey Smith, G, and Nordestgaard, BG. Genetically high plasma vitamin C, intake of fruit and vegetables, and risk of ischemic heart disease and all-cause mortality: a Mendelian randomization study. Am J Clin Nutr. (2015) 101:1135–43. doi: 10.3945/ajcn.114.104497
13. Schultz, WM, Kelli, HM, Lisko, JC, Varghese, T, Shen, J, Sandesara, P, et al. Socioeconomic status and cardiovascular outcomes: challenges and interventions. Circulation. (2018) 137:2166–78. doi: 10.1161/CIRCULATIONAHA.117.029652
14. Woodward, M, Peters, SA, Batty, GD, Ueshima, H, Woo, J, Giles, GG, et al. Socioeconomic status in relation to cardiovascular disease and cause-specific mortality: a comparison of Asian and Australasian populations in a pooled analysis. BMJ Open. (2015) 5:e006408. doi: 10.1136/bmjopen-2014-006408
15. Parikh, PB, Yang, J, Leigh, S, Dorjee, K, Parikh, R, Sakellarios, N, et al. The impact of financial barriers on access to care, quality of care and vascular morbidity among patients with diabetes and coronary heart disease. J Gen Intern Med. (2014) 29:76–81. doi: 10.1007/s11606-013-2635-6
16. Luepker, RV, Rosamond, WD, Murphy, R, Sprafka, JM, Folsom, AR, McGovern, PG, et al. Socioeconomic status and coronary heart disease risk factor trends. The Minnesota Heart Survey. Monograph. (1993) 88:2172–9. doi: 10.1161/01.CIR.88.5.2172
17. Alwitt, LF, and Donley, TD. Retail Stores in Poor Urban Neighborhoods. J Consum Aff. (1997) 31:139–64. doi: 10.1111/j.1745-6606.1997.tb00830.x
18. Liu, W, Hu, B, Dehghan, M, Mente, A, Wang, C, Yan, R, et al. Fruit, vegetable, and legume intake and the risk of all-cause, cardiovascular, and cancer mortality: a prospective study. Clin Nutr. (2021) 40:4316–23. doi: 10.1016/j.clnu.2021.01.016
19. Mozaffarian, D. Dietary and policy priorities for cardiovascular disease, diabetes, and obesity: a comprehensive review. Circulation. (2016) 133:187–225. doi: 10.1161/CIRCULATIONAHA.115.018585
20. Larsson, S, Mason, A, Bäck, M, Klarin, D, Damrauer, S, Michaëlsson, K, et al. Genetic predisposition to smoking in relation to 14 cardiovascular diseases. Eur Heart J. (2020) 41:3304–10. doi: 10.1093/eurheartj/ehaa193
21. Bell, S, Daskalopoulou, M, Rapsomaniki, E, George, J, Britton, A, Bobak, M, et al. Association between clinically recorded alcohol consumption and initial presentation of 12 cardiovascular diseases: population based cohort study using linked health records. BMJ. (2017) 356:j909. doi: 10.1136/bmj.j909
22. Piché, M, Tchernof, A, and Després, J. Obesity phenotypes, diabetes, and cardiovascular diseases. Circ Res. (2020) 126:1477–500. doi: 10.1161/CIRCRESAHA.120.316101
23. Kershaw, KN, Droomers, M, Robinson, WR, Carnethon, MR, Daviglus, ML, and Monique Verschuren, WM. Quantifying the contributions of behavioral and biological risk factors to socioeconomic disparities in coronary heart disease incidence: the MORGEN study. Eur J Epidemiol. (2013) 28:807–14. doi: 10.1007/s10654-013-9847-2
24. Stirbu, I, Looman, C, Nijhof, GJ, Reulings, PG, and Mackenbach, JP. Income inequalities in case death of ischaemic heart disease in the Netherlands: a national record-linked study. J Epidemiol Community Health. (2012) 66:1159–66. doi: 10.1136/jech-2011-200924
25. Hemani, G, Tilling, K, and Davey Smith, G. Orienting the causal relationship between imprecisely measured traits using GWAS summary data. PLoS Genet. (2017) 13:e1007081. doi: 10.1371/journal.pgen.1007081
26. Davey Smith, G. Use of genetic markers and gene-diet interactions for interrogating population-level causal influences of diet on health. Genes Nutr. (2011) 6:27–43. doi: 10.1007/s12263-010-0181-y
27. Feng, Q, Grant, AJ, Yang, Q, Burgess, S, Bešević, J, Conroy, M, et al. Vegetable intake and cardiovascular risk: genetic evidence from Mendelian randomization. medRxiv. (2022)
28. Feng, Q, and Bešević, J. Vegetable intake and metabolic risk factors: a Mendelian randomization study. medRxiv. (2022)
29. Cole, JB, Florez, JC, and Hirschhorn, JN. Comprehensive genomic analysis of dietary habits in UK biobank identifies hundreds of genetic associations. Nat Commun. (2020) 11:1467. doi: 10.1038/s41467-020-15193-0
30. Pirastu, N, McDonnell, C, Grzeszkowiak, EJ, Mounier, N, Imamura, F, Merino, J, et al. Using genetic variation to disentangle the complex relationship between food intake and health outcomes. PLoS Genet. (2022) 18:e1010162. doi: 10.1371/journal.pgen.1010162
31. Niarchou, M, Byrne, EM, Trzaskowski, M, Sidorenko, J, Kemper, KE, McGrath, JJ, et al. Genome-wide association study of dietary intake in the UK biobank study and its associations with schizophrenia and other traits. Transl Psychiatry. (2020) 10:51. doi: 10.1038/s41398-020-0688-y
32. Machiela, MJ, and Chanock, SJ. LDlink: a web-based application for exploring population-specific haplotype structure and linking correlated alleles of possible functional variants. Bioinformatics. (2015) 31:3555–7. doi: 10.1093/bioinformatics/btv402
33. Kamat, MA, Blackshaw, JA, Young, R, Surendran, P, Burgess, S, Danesh, J, et al. PhenoScanner V2: an expanded tool for searching human genotype-phenotype associations. Bioinformatics. (2019) 35:4851–3. doi: 10.1093/bioinformatics/btz469
34. Jaeger, SR, McRae, JF, Bava, CM, Beresford, MK, Hunter, D, Jia, Y, et al. A Mendelian trait for olfactory sensitivity affects odor experience and food selection. Curr Biol. (2013) 23:1601–5. doi: 10.1016/j.cub.2013.07.030
35. McRae, JF, Jaeger, SR, Bava, CM, Beresford, MK, Hunter, D, Jia, Y, et al. Identification of regions associated with variation in sensitivity to food-related odors in the human genome. Curr Biol. (2013) 23:1596–600. doi: 10.1016/j.cub.2013.07.031
36. Burgess, S, and Thompson, SG. Avoiding bias from weak instruments in Mendelian randomization studies. Int J Epidemiol. (2011) 40:755–64. doi: 10.1093/ije/dyr036
37. Okbay, A, Beauchamp, JP, Fontana, MA, Lee, JJ, Pers, TH, Rietveld, CA, et al. Genome-wide association study identifies 74 loci associated with educational attainment. Nature. (2016) 533:539–42. doi: 10.1038/nature17671
38. Shi, X, Yuan, W, Cao, Q, and Cui, W. Education plays a crucial role in the pathway from poverty to smoking: a Mendelian randomization study. Addiction. (2022) 118:128–39. doi: 10.1111/add.16019
39. Hill, WD, Hagenaars, SP, Marioni, RE, Harris, SE, Liewald, DCM, Davies, G, et al. Molecular genetic contributions to social deprivation and household income in UK biobank. Curr Biol. (2016) 26:3083–9. doi: 10.1016/j.cub.2016.09.035
40. Mitchell, R, Elsworth, BL, Mitchell, R, Raistrick, CA, Paternoster, L, Hemani, G, et al. MRC-IEU UK biobank GWAS pipeline version 2. Bristol: University of Bristol.
41. Bowden, J, Davey Smith, G, and Burgess, S. Mendelian randomization with invalid instruments: effect estimation and bias detection through egger regression. Int J Epidemiol. (2015) 44:512–25. doi: 10.1093/ije/dyv080
42. Bowden, J, Davey Smith, G, Haycock, PC, and Burgess, S. Consistent estimation in Mendelian randomization with some invalid instruments using a weighted median estimator. Genet Epidemiol. (2016) 40:304–14. doi: 10.1002/gepi.21965
43. Verbanck, M, Chen, CY, Neale, B, and Do, R. Detection of widespread horizontal pleiotropy in causal relationships inferred from Mendelian randomization between complex traits and diseases. Nat Genet. (2018) 50:693–8. doi: 10.1038/s41588-018-0099-7
44. Hemani, G, Zheng, J, Elsworth, B, Wade, KH, Haberland, V, Baird, D, et al. The MR-base platform supports systematic causal inference across the human phenome. elife. (2018) 7:7. doi: 10.7554/eLife.34408
45. Sanderson, E, Davey Smith, G, Windmeijer, F, and Bowden, J. An examination of multivariable Mendelian randomization in the single-sample and two-sample summary data settings. Int J Epidemiol. (2019) 48:713–27. doi: 10.1093/ije/dyy262
46. Zhan, J, Liu, YJ, Cai, LB, Xu, FR, Xie, T, and He, QQ. Fruit and vegetable consumption and risk of cardiovascular disease: a meta-analysis of prospective cohort studies. Crit Rev Food Sci Nutr. (2017) 57:1650–63. doi: 10.1080/10408398.2015.1008980
47. Bechthold, A, Boeing, H, Schwedhelm, C, Hoffmann, G, Knuppel, S, Iqbal, K, et al. Food groups and risk of coronary heart disease, stroke and heart failure: a systematic review and dose-response meta-analysis of prospective studies. Crit Rev Food Sci Nutr. (2019) 59:1071–90. doi: 10.1080/10408398.2017.1392288
48. Oude Griep, LM, Verschuren, WM, Kromhout, D, Ocké, MC, and Geleijnse, JM. Raw and processed fruit and vegetable consumption and 10-year stroke incidence in a population-based cohort study in the Netherlands. Eur J Clin Nutr. (2011) 65:791–9. doi: 10.1038/ejcn.2011.36
49. Kanter, M, Angadi, S, and Slavin, J. Glycemic index, glycemic load, and cardiovascular disease and mortality. N Engl J Med. (2021) 385:378–80. doi: 10.1056/NEJMc2107926
50. Ference, BA, Graham, I, Tokgozoglu, L, and Catapano, AL. Impact of lipids on cardiovascular health: JACC health promotion series. J Am Coll Cardiol. (2018) 72:1141–56. doi: 10.1016/j.jacc.2018.06.046
51. Ference, BA, Ginsberg, HN, Graham, I, Ray, KK, Packard, CJ, Bruckert, E, et al. Low-density lipoproteins cause atherosclerotic cardiovascular disease. 1. Evidence from genetic, epidemiologic, and clinical studies. A consensus statement from the European atherosclerosis society consensus panel. Eur Heart J. (2017) 38:2459–72. doi: 10.1093/eurheartj/ehx144
52. Holmes, MV, Millwood, IY, Kartsonaki, C, Hill, MR, Bennett, DA, Boxall, R, et al. Lipids, lipoproteins, and metabolites and risk of myocardial infarction and stroke. J Am Coll Cardiol. (2018) 71:620–32. doi: 10.1016/j.jacc.2017.12.006
53. Fornés, NS, Martins, IS, Hernan, M, Velásquez-Meléndez, G, and Ascherio, A. Frequency of food consumption and lipoprotein serum levels in the population of an urban area, Brazil. Rev Saude Publica. (2000) 34:380–7. doi: 10.1590/S0034-89102000000400011
54. Djoussé, L, Arnett, DK, Coon, H, Province, MA, Moore, LL, and Ellison, RC. Fruit and vegetable consumption and LDL cholesterol: the national heart, lung, and blood institute family heart study. Am J Clin Nutr. (2004) 79:213–7. doi: 10.1093/ajcn/79.2.213
55. John, JH, Ziebland, S, Yudkin, P, Roe, LS, and Neil, HA. Effects of fruit and vegetable consumption on plasma antioxidant concentrations and blood pressure: a randomised controlled trial. Lancet. (2002) 359:1969–74. doi: 10.1016/S0140-6736(02)98858-6
56. Zino, S, Skeaff, M, Williams, S, and Mann, J. Randomised controlled trial of effect of fruit and vegetable consumption on plasma concentrations of lipids and antioxidants. BMJ. (1997) 314:1787–91. doi: 10.1136/bmj.314.7097.1787
57. He, FJ, Li, J, and Macgregor, GA. Effect of longer term modest salt reduction on blood pressure: Cochrane systematic review and meta-analysis of randomised trials. BMJ. (2013) 346:f1325. doi: 10.1136/bmj.f1325
58. Unhapipatpong, C, Shantavasinkul, PC, Kasemsup, V, Siriyotha, S, Warodomwichit, D, Maneesuwannarat, S, et al. Tropical oil consumption and cardiovascular disease: an umbrella review of systematic reviews and meta analyses. Nutrients. (2021) 13:1549. doi: 10.3390/nu13051549
59. Palermo, M, Pellegrini, N, and Fogliano, V. The effect of cooking on the phytochemical content of vegetables. J Sci Food Agric. (2014) 94:1057–70. doi: 10.1002/jsfa.6478
60. Lee, S, Choi, Y, Jeong, HS, Lee, J, and Sung, J. Effect of different cooking methods on the content of vitamins and true retention in selected vegetables. Food Sci Biotechnol. (2018) 27:333–42. doi: 10.1007/s10068-017-0281-1
61. van Boekel, M, Fogliano, V, Pellegrini, N, Stanton, C, Scholz, G, Lalljie, S, et al. A review on the beneficial aspects of food processing. Mol Nutr Food Res. (2010) 54:1215–47. doi: 10.1002/mnfr.200900608
62. Franks, P, Winters, PC, Tancredi, DJ, and Fiscella, KA. Do changes in traditional coronary heart disease risk factors over time explain the association between socio-economic status and coronary heart disease? BMC Cardiovasc Disord. (2011) 11:28. doi: 10.1186/1471-2261-11-28
63. Stringhini, S, Carmeli, C, Jokela, M, Avendaño, M, Muennig, P, Guida, F, et al. Socioeconomic status and the 25 × 25 risk factors as determinants of premature mortality: a multicohort study and meta-analysis of 1·7 million men and women. Lancet. (2017) 389:1229–37. doi: 10.1016/S0140-6736(16)32380-7
64. Zhang, YB, Chen, C, Pan, XF, Guo, J, Li, Y, Franco, OH, et al. Associations of healthy lifestyle and socioeconomic status with mortality and incident cardiovascular disease: two prospective cohort studies. BMJ. (2021) 373:n604. doi: 10.1136/bmj.n604
65. Roos, EB, Hirvonen, T, Mikkilä, V, Karvonen, S, and Rimpelä, M. Household educational level as a determinant of consumption of raw vegetables among male and female adolescents. Prev Med. (2001) 33:282–91. doi: 10.1006/pmed.2001.0882
66. Zeng, L, Ntalla, I, Kessler, T, Kastrati, A, Erdmann, J, Group UKBCCCW, et al. Genetically modulated educational attainment and coronary disease risk. Eur Heart J. (2019) 40:2413–20. doi: 10.1093/eurheartj/ehz328
67. Cajita, MI, Cajita, TR, and Han, HR. Health literacy and heart failure: a systematic review. J Cardiovasc Nurs. (2016) 31:121–30. doi: 10.1097/JCN.0000000000000229
68. Diez Roux, AV, Merkin, SS, Arnett, D, Chambless, L, Massing, M, Nieto, FJ, et al. Neighborhood of residence and incidence of coronary heart disease. N Engl J Med. (2001) 345:99–106. doi: 10.1056/NEJM200107123450205
69. Giang, T, Karpyn, A, Laurison, HB, Hillier, A, and Perry, RD. Closing the grocery gap in underserved communities: the creation of the Pennsylvania fresh food financing initiative. J Public Health Manag Pract. (2008) 14:272–9. doi: 10.1097/01.PHH.0000316486.57512.bf
70. Block, JP, Scribner, RA, and DeSalvo, KB. Fast food, race/ethnicity, and income: a geographic analysis. Am J Prev Med. (2004) 27:211–7. doi: 10.1016/S0749-3797(04)00139-4
71. Block, D, and Kouba, J. A comparison of the availability and affordability of a market basket in two communities in the Chicago area. Public Health Nutr. (2006) 9:837–45. doi: 10.1017/PHN2005924
72. Christine, PJ, Auchincloss, AH, Bertoni, AG, Carnethon, MR, Sánchez, BN, Moore, K, et al. Longitudinal associations between neighborhood physical and social environments and incident type 2 diabetes mellitus: the multi-ethnic study of atherosclerosis (MESA). JAMA Intern Med. (2015) 175:1311–20. doi: 10.1001/jamainternmed.2015.2691
73. Creatore, MI, Glazier, RH, Moineddin, R, Fazli, GS, Johns, A, Gozdyra, P, et al. Association of neighborhood walkability with change in overweight, obesity, and diabetes. JAMA. (2016) 315:2211–20. doi: 10.1001/jama.2016.5898
74. Bedford, JL, and Barr, SI. Diets and selected lifestyle practices of self-defined adult vegetarians from a population-based sample suggest they are more 'health conscious'. Int J Behav Nutr Phys Act. (2005) 2:4. doi: 10.1186/1479-5868-2-4
75. Chang-Claude, J, Hermann, S, Eilber, U, and Steindorf, K. Lifestyle determinants and mortality in German vegetarians and health-conscious persons: results of a 21-year follow-up. Cancer Epidemiol Biomark Prev. (2005) 14:963–8. doi: 10.1158/1055-9965.EPI-04-0696
76. Fry, A, Littlejohns, TJ, Sudlow, C, Doherty, N, Adamska, L, Sprosen, T, et al. Comparison of sociodemographic and health-related characteristics of UK Biobank participants with those of the general population. Am J Epidemiol. (2017) 186:1026–34. doi: 10.1093/aje/kwx246
77. Livingstone, MB, and Black, AE. Markers of the validity of reported energy intake. J Nutr. (2003) 133:895s–920s. doi: 10.1093/jn/133.3.895S
78. Tooze, JA, Subar, AF, Thompson, FE, Troiano, R, Schatzkin, A, and Kipnis, V. Psychosocial predictors of energy underreporting in a large doubly labeled water study. Am J Clin Nutr. (2004) 79:795–804. doi: 10.1093/ajcn/79.5.795
79. Stevenson, RJ. Psychological correlates of habitual diet in healthy adults. Psychol Bull. (2017) 143:53–90. doi: 10.1037/bul0000065
80. Pierce, BL, and Burgess, S. Efficient design for Mendelian randomization studies: subsample and 2-sample instrumental variable estimators. Am J Epidemiol. (2013) 178:1177–84. doi: 10.1093/aje/kwt084
Keywords: vegetable intake, socioeconomic status, ischemic cardiovascular disease, ischemic cerebrovascular disease, Mendelian randomization
Citation: Huang J, He Z, Xu M, Du J and Zhao Y-t (2023) Socioeconomic status may affect association of vegetable intake with risk of ischemic cardio-cerebral vascular disease: a Mendelian randomization study. Front. Nutr. 10:1161175. doi: 10.3389/fnut.2023.1161175
Edited by:
Yong Zhao, Chongqing Medical University, ChinaReviewed by:
Jesús Francisco García-Gavilán, CIBER Fisiopatología Obesidad y Nutrición (CIBEROBN), SpainCopyright © 2023 Huang, He, Xu, Du and Zhao. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yun-tao Zhao, cmFhc0Boc2MucGt1LmVkdS5jbg==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.