
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Nutr. , 22 June 2023
Sec. Clinical Nutrition
Volume 10 - 2023 | https://doi.org/10.3389/fnut.2023.1132191
This article is part of the Research Topic Nutrition and Sustainable Development Goal 3: Good Health and Wellbeing View all 35 articles
 Sadeq Ali Al-Maweri1*
Sadeq Ali Al-Maweri1* Gamilah Al-Qadhi2
Gamilah Al-Qadhi2 Esam Halboub3,4
Esam Halboub3,4 Nader Alaizari5Asma Almeslet6
Nader Alaizari5Asma Almeslet6 Kamran Ali1
Kamran Ali1 Safa A. Azim Osman1
Safa A. Azim Osman1Background: Growing evidence suggests a significant association between vitamin D deficiency and RAS. Hence, the present meta-analysis and trial sequential analysis sought to investigate the potential association between low serum vitamin D levels and RAS.
Methods: PubMed, Scopus, Embase, and Web of Science were comprehensively searched on December 1st, 2022 to retrieve all relevant studies. The grey literature was also searched via ProQuest. All case-control studies on the association between vitamin D and RAS were considered. The quality appraisal of the included studies was done using Newcastle-Ottawa scale. RevMan 5.0 and trial sequential analysis (TSA) programs were used for analyses.
Results: A total of 14 case-control studies with 1468 subjects (721 RAS patients and 747 controls) were included. The pooled data revealed a significant association between low serum levels of vitamin D and the risk of RAS (mean difference = – 8.73, 95% CI: – 12.02 to – 5.44, I2 = 94%, P < 0.00001). Additionally, TSA findings indicated that the current studies surpassed the required information size, confirming that the differences were reliable.
Conclusion: The available evidence suggests that Vitamin D deficiency may have a role in the pathogenesis of RAS. Therefore, evaluation of vitamin D should be considered in RAS patients. Additionally, the results support the possibility of using vitamin D supplements in the management of RAS patients with inadequate serum levels of vitamin D. Future interventional studies are required to evaluate the benefits of vitamin D replacement in prevention and treatment of RAS.
Recurrent aphthous stomatitis (RAS) - also known as recurrent aphthous ulcers or canker sores - is the commonest cause of oral mucosal ulceration (1–3). RAS is a highly prevalent condition affecting up to 25% of the general population, mainly adolescent and young adults, although it can occur at any age (3, 4). It is characterized by recurring, painful, ovoid or round, single or multiple ulcers of the oral mucosa, and primarily affect the non-keratinized mucosa (3, 4). The RAS-associated pain and discomfort might be severe and impact the patients' quality of life adversely by interfering with routine oral functions such as eating, swallowing, and speaking (1, 3, 5). Clinically, there are three variants of RAS: minor (less than 1 cm in diameter), major (more than 1 cm), and herpetiform (2–3 mm across) (2–4). Minor RAS is the most common form accounting for 90% of all RAS cases (1, 3).
Despite the extensive research done on the topic, the exact etiopathogenesis of RAS remains unclear (1). An immunological reaction to an unknown trigger is considered the most plausible mechanism involved in the development of RAS (6, 7). Several systemic and local factors increase predisposition to RAS including psychological stress, genetic makeup, immunological dysfunction, mucosal trauma, gastrointestinal disorders, hematological factors, and nutritional and hematinic deficiencies (1, 3, 6–10). The potential role of nutritional deficiencies of certain vitamins and minerals has been explored extensively in the literature (10). In this regard, numerous studies assessed hematinic and vitamins deficiencies (such as, B-complex vitamins and Folic acid) in RAS patients. However, the results remain inconclusive (11–16).
In recent years, the role of vitamin D in pathogenesis of several oral diseases including RAS has generated a significant level of interest (12, 14, 17, 18). Vitamin D, a lipid soluble secosteroid, plays key biological roles in calcium-phosphorus homeostasis and bone metabolism (17, 19). Recent evidence supports the role of vitamin D in inhibition of inflammatory process: Vitamin D is believed to modulate the immune system through inhibition of maturation of dendritic cells, and establishing a balance between different components of the immune system (17, 20, 21). In regard to systemic health, vitamin D deficiency has been linked to many disorders including hypertension, musculoskeletal disorders, obesity, cancers and autoimmune diseases (17, 22–26). In relation to oral health, a growing body of evidence links vitamin D deficiency to several oral mucosal diseases such as oral lichen planus and RAS (27, 28). In context of the latter, many recent studies investigated the potential association between vitamin D and the risk of RAS but showed inconsistent results (11–14, 28–30). Our previous meta-analysis, which involved all relevant studies published up to June 2019 (n = 5) revealed a significant association between vitamin D deficiency and RAS (31). Since then, numerous case-control studies have investigated the role of vitamin D in RAS, and appeared to report variable results (11–14, 32–35). Hence, we sought to update the available evidence regarding the potential association between low serum levels of vitamin D and RAS, supported by a trial sequential analysis (TSA). TSA is a novel approach used in systematic reviews and meta-analysis to control the random errors in the conventional meta-analysis and identifies the information size and weather further studies are still required or not (36).
The focused research question for this study was: “Is low serum level of vitamin D associated with RAS?
The present meta-analysis followed PRISMA 2020 guidelines and PICO/PECO principles (37), and the protocol was registered in PROSPERO (ID: CRD42022365428).
All case-control and cohort studies that investigated the association between serum levels of vitamin D (25-hydroxycholecalciferol) and RAS, and fulfilled the following criteria were considered eligible: (1) comprised systemically healthy RAS subjects who were compared with systematically healthy control subjects, (2) the outcome measures reported serum levels of vitamin D quantitatively (mean ± SD).
The exclusion criteria were: (1) Lack of control group, (2) experimental studies, (3) case reports (4) case series, (5) missing or inadequate quantitative data (means of vitamin D), (6) editorials, and (7) review papers.
Two investigators independently conducted extensive online searches on December 1, 2022 in PubMed, Scopus, Embase, and Web of Science databases for all relevant studies from date of inception till and including November 2022. The grey literature was also searched via Proquest. The following Mesh terms and free keywords were used for the electronic searches: “Stomatitis, Aphthous”[Mesh] (for PubMed) OR “recurrent aphthous ulcers” OR “aphthous ulcers” OR “recurrent aphthous stomatitis” OR “recurrent aphthosis” OR “recurrent oral ulcer” Or “aphthous stomatitis” AND “vitamin D” OR “25-hydroxycholecalciferol” (Detailed search strategy is presented in Supplementary Table 1). The online searches were supplemented with a manual search of the references of the included studies. The retrieved studies were then exported to EndNote program, and duplicates were removed.
Two investigators (NA, GA) independently extracted all relevant data using a pre-designed form. The following data were extracted: authors, year of publication, country, study design, sample size, age of participants, the means and SD of serum levels of Vitamin D (ng/mL).
Two investigators (NA, GA) independently assessed the quality of the included studies using the Newcastle-Ottawa Scale (NOS). The quality of each study was evaluated based on the following three domains: selection of cases and controls; comparability of cases and controls; and assessment of the exposure. Subsequently, each study was judged as either high quality (at least 7 stars); moderate quality (4–6 stars); or poor quality (0–3 stars).
Statistical analyses were conducted using Review Manager (RevMan) Version 5.3 (Copenhagen: The Nordic Cochrane Centre, the Cochrane Collaboration, 2014). The mean difference (MD) in vitamin D between the two groups along with 95% confidence interval (CI) were calculated. The heterogeneity across the included studies was evaluated using the Cochrane Q test (χ2 test) and I-squared index (I2). A P-value of < 0.05 was considered statistically significant.
TSA software version 0.9.5.10 beta was used for TSA (www.ctu.dk/tsa). In brief, we used two-sided trial sequential monitoring boundary type, and the required information size (RIS) was estimated (36, 38).
Publication bias was assessed using funnel plot and Egger's test.
A total of 273 records were retrieved from online searches, 161 of which were duplicates and were thus removed (Figure 1). The titles and abstracts of the remaining 112 articles were screened by two independent investigators (SA, GA) for inclusion. Of these, 88 articles were found to be irrelevant and were excluded. The full text of the potentially eligible 24 articles were read by the two investigators, and 10 were excluded for various reasons (Supplementary Table 2). Eventually, 14 studies were included in the present meta-analysis.
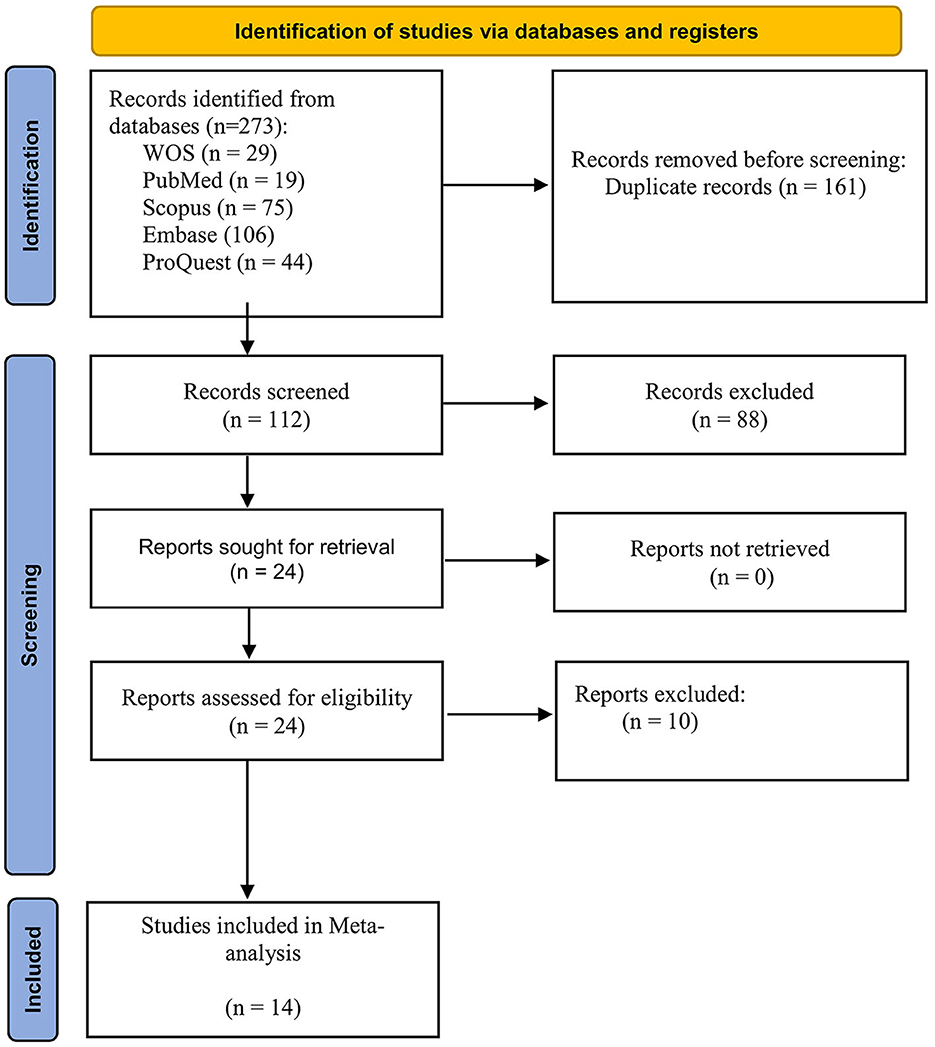
Figure 1. Flowchart of the study search strategy.
A total of 14 case-controlled studies comprising 1468 subjects (721 RAS patients and 747 controls) were included in this meta-analysis (11–14, 18, 28–30, 32–35, 39, 40). Six studies were conducted in Turkey (12–14, 34, 39, 40), three in Iran (28, 30, 35), one in Poland (18), one in India (33), one in Saudi Arabia (32), one in the United Arab Emirates (11) and one in Iraq (29). The mean age of study participants ranged from 29.26 to 40.60 years, and from 27.44 to 40.80 years in the control groups. Two studies were conducted in children with mean age ranging from 7.6 to 8.7 years (34, 40). Of 721 RAS cases, around 56% (n = 404) were females (Table 1). Eight studies (28–30, 32, 34, 35, 39, 40) included patients with minor RAS, two studies (18, 33) included patients with minor, major, and herpetiform RAS, and one study (12) included patients with minor and major RAS, while three studies (11, 13, 14) did not mention the type of RAS. All the included studies assessed the serum levels of vitamin D, seven of which used ELISA (enzyme-linked immunosorbent assay) (29, 30, 32–35, 40), while four studies (11, 18, 28, 39) used ECLIA (electro-chemiluminescence binding assay). Three studies (12–14) did not mention the type of the assay. With respect to diagnostic criteria of RAS, all studies relied on clinical presentation and history of recurrence of RAS, while one study did not provide sufficient information (14) (Table 1).

Table 1. General characteristics of the included studies.
Concerning the outcome measures, all studies assessed and compared serum levels of vitamin D in RAS and controls, and eight studies also (11, 13, 18, 29, 30, 32, 34, 39) assessed the association between serum levels of vitamin D and RAS variables such as duration, severity, and frequency (Table 2).
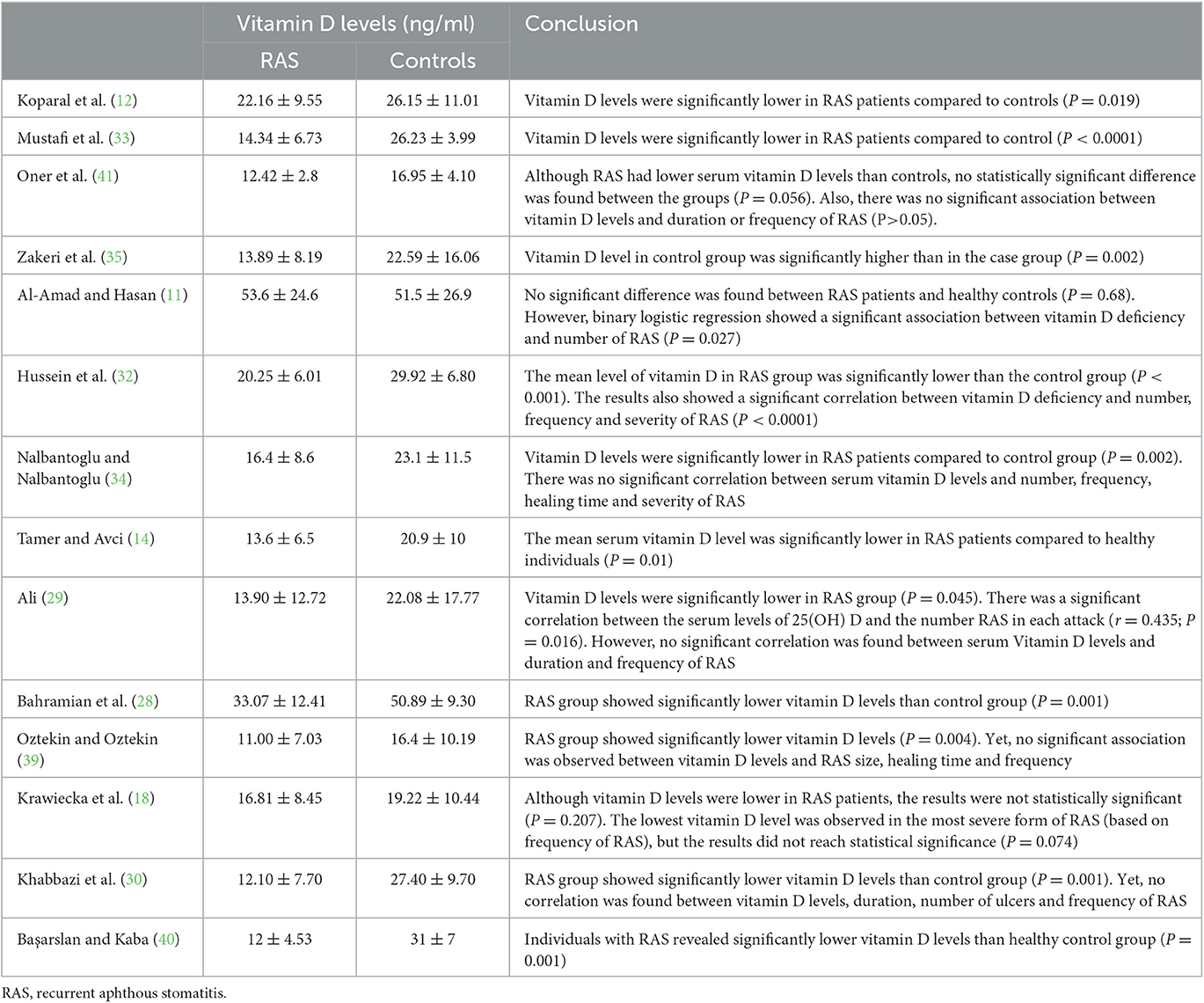
Table 2. Summary of the main outcomes.
A summary of the quality assessment of the included studies is presented in Table 3. Of the included studies, 12 (12–14, 18, 28–30, 32–35, 40) were of moderate quality, while two studies (11, 39) were of high quality.
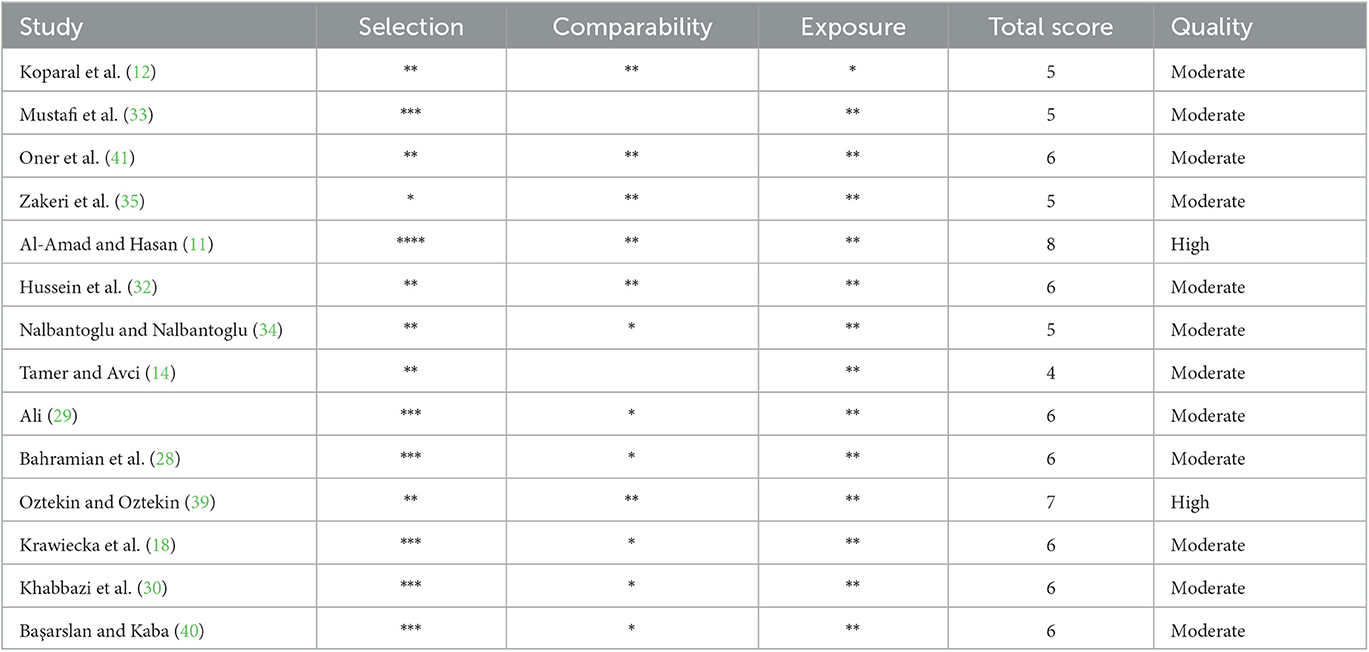
Table 3. Quality of studies assessed by Newcastle Ottawa Scale (case-control studies).
Of the 14 included studies, 11 studies (12, 14, 28–30, 32–35, 39, 40) found significantly lower serum levels of vitamin D in RAS patients compared to the controls (Table 2); one study found insignificant (P = 0.056) lower serum levels of vitamin D in RAS patients (13); while two studies did not find any differences between the two groups (11, 18).
Eight studies (11, 13, 18, 29, 30, 32, 34, 39) assessed the association between serum levels of vitamin D and RAS variables such as duration, severity, and frequency. Five studies (13, 18, 30, 34, 39) found no significant association between vitamin D and duration, frequency, and severity of RAS, while three studies showed a significant association between serum levels of vitamin D and number of RAS (11, 29, 32) (Table 2).
The pooled results of the 14 studies revealed a significant association between low serum levels of vitamin D and the risk of RAS (MD = – 8.73, 95% CI: – 12.02to – 5.44, I2 = 94%, P < 0.00001 (Figure 2).
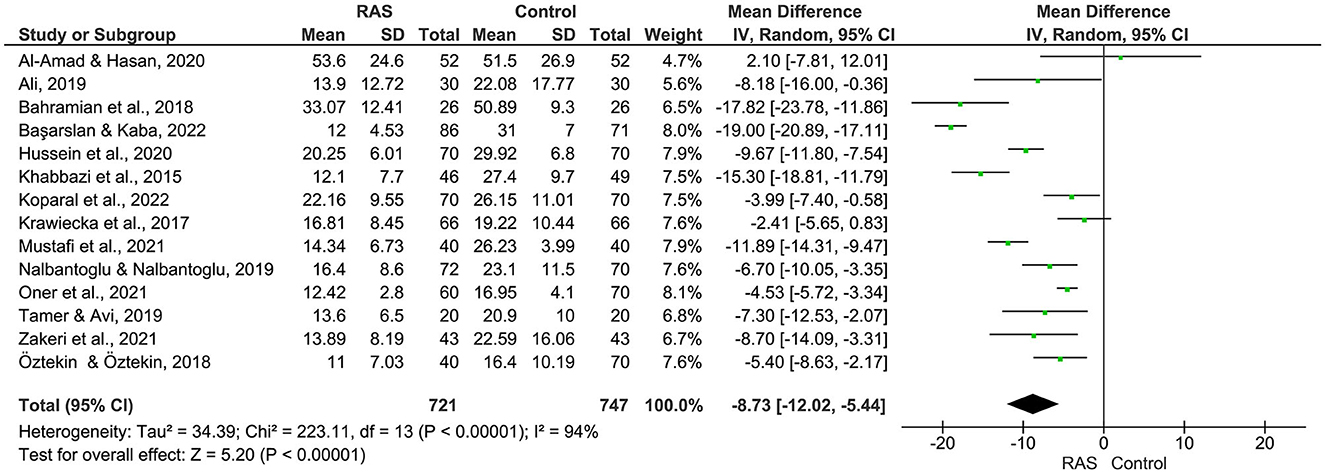
Figure 2. Meta analysis of vitamin D levels between RAS and controls.
Figure 3 depicts the TSA: The cumulative Z curves crossed the conventional boundary and the trial sequential monitoring boundary and surpassed the required information size (n = 443) as well. As such, the evidence is reliable and confirmatory, and further trials are no longer needed.
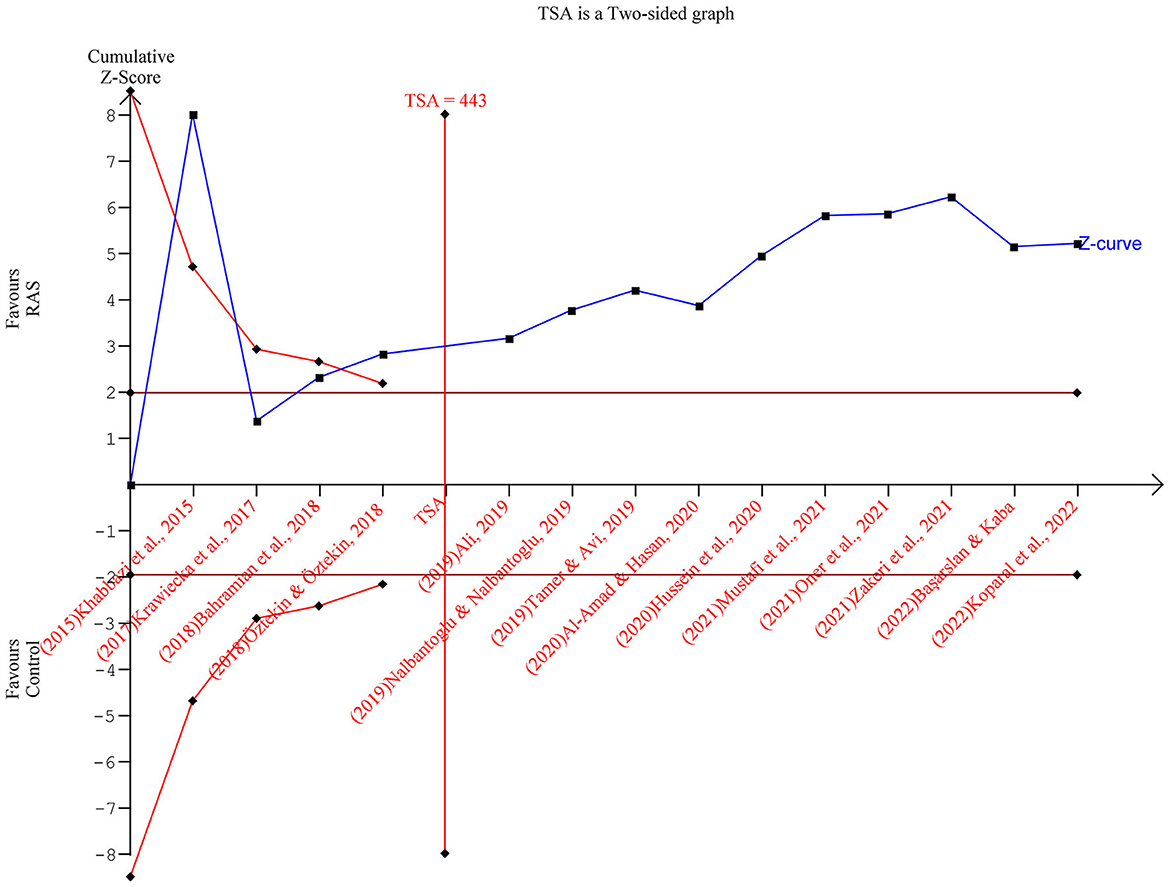
Figure 3. Trial sequential analysis results.
The funnel plot (Figure 4) reveals symmetric distribution of the included studies, indicating no publication bias.
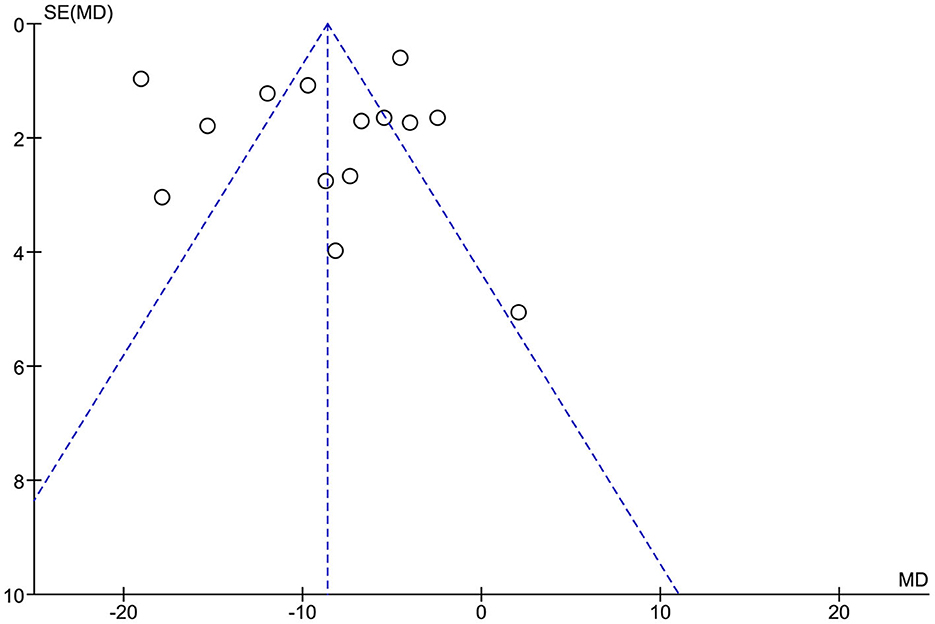
Figure 4. Funnel plots.
As discussed earlier, RAS is a common mucosal disease that may impact adversely on the patients' quality of life (5). Despite a large body of research on the topic, the exact etiopathogenesis of RAS remains unclear (1, 6, 10). Given the lack of a specific etiology, RAS management is challenging (2, 42–44). In light of the mounting evidence regarding the potential role of vitamin D in the pathogenesis of certain oral mucosal diseases including RAS (13, 29, 31, 35), the present meta-analysis was conducted to answer the following focused question: Is low serum levels of vitamin D associated with higher risk of RAS? Overall, the results of the pooled 14 studies revealed a significant association between low serum levels of vitamin D and the risk of RAS. Additionally, the result of the meta-analysis was supported by the TSA findings, which showed that the current studies surpassed the required information size, confirming that the differences were reliable. However, the qualitative analysis revealed conflicting results regarding the association between serum levels of vitamin D and severity and frequency of RAS.
The results of the present updated meta-analysis confirm our original meta-analysis (31), and substantiate many previous systematic reviews and meta-analyses that found significant associations between vitamin D deficiency and several autoimmune diseases and dermatological conditions such as lupus erythematosus, vitiligo, autoimmune bullous dermatoses, rheumatoid arthritis, and primary Sjögren's syndrome (22–26). Interestingly, our results are in accord with a recent clinical trial which investigated the efficacy of vitamin D supplementations in RAS patients with vitamin D deficiency, and reported a significant reduction in the frequency of RAS episodes, number of ulcers, and duration of healing time after one year (45). The exact mechanism behind the effects of vitamin D on RAS is still unclear yet, but may be explained by its immunomodulatory effects. Studies confirmed that vitamin D has strong immunomodulatory effects on both innate and acquired immunity responses, as well as on cytokines levels (20, 46, 47), all of which are thought to be involved in the pathogenesis of RAS (6, 7, 10).
It is recognized that the level of any evidence obtained from each meta-analysis is largely dependent on the quality of the included studies. Hence, we meticulously scrutinized the quality of all included studies using NOS, a reliable and validated appraisal tool. The results showed that two studies were of high quality (low risk of bias), and 11 were of moderate quality, and no study was with low quality, suggesting fair evidence. Additionally, the result of the meta-analysis was further substantiated by TSA results, which further confirmed the reliability and conclusiveness of the results (36).
The present updated meta-analysis has some limitations that should be considered. The main limitation is the marked heterogeneity across the included studies in terms of geography, age of the participants, methods of vitamin D ascertainment, types of RAS included, among others. This in turn may have biased the results. Additionally, although the included studies were conducted in different parts of the world and involved large samples (721 RAS cases and 747 controls), five studies (around 40% of the included studies) came from one country, Turkey, and thus the generalization of the results may not be appropriate.
In conclusion, the present updated meta-analysis confirms the association between low serum levels of vitamin D and the risk of RAS. Hence, vitamin D assessment may be considered in RAS patients. The results also support the use of vitamin D supplementations in RAS patients with inadequate serum levels of vitamin D. However, future interventional studies (for prevention and/or treatment purposes) investigating the effect of vitamin D supplements on RAS patients are required.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
SA: study concept, search strategy, and drafting the manuscript. GA-Q: data extraction, quality appraisal, and drafting the manuscript. EH: concept of the study and critically revised and edited the paper. NA: data extraction, quality appraisal, and drafting the manuscript. AA: concept of the study, data analysis, and critically revised and edited the paper. KA: concept of the study and critically revised and edited the paper. SO: data curation and critically revised and edited the paper. All authors approved the final version.
Open Access funding provided by the Qatar National Library.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnut.2023.1132191/full#supplementary-material
1. Bilodeau EA, Lalla RV. Recurrent oral ulceration. Etiology, classification, management, and diagnostic algorithm. Periodontol. (2019) 80:49–60. doi: 10.1111/prd.12262
2. Lau CB, Smith GP. Recurrent aphthous stomatitis. A comprehensive review and recommendations on therapeutic options. Dermatol Ther. (2022) 35:e15500. doi: 10.1111/dth.15500
3. Tarakji B, Gazal G, Al-Maweri SA, Azzeghaiby SN, Alaizari N. Guideline for the diagnosis and treatment of recurrent aphthous stomatitis for dental practitioners. J Int Oral Health. (2015) 7:74–80.
4. Jurge S, Kuffer R, Scully C, Porter SR. Mucosal disease series. Number VI Recurrent aphthous stomatitis. Oral Dis. (2006) 12:1–21. doi: 10.1111/j.1601-0825.2005.01143.x
5. Rivera C, Muñoz-Pastén M, Núñez-Muñoz E, Hernández-Olivos R. Recurrent aphthous stomatitis affects quality of life. A case-control study. Clin Cosmet Investig Dent. (2022) 14:217–23. doi: 10.2147/CCIDE.S369481
6. Kounoupis V, Andreadis D, Georgaki M, Albanidou-Farmaki E, Daniilidis M, Markopoulos A, et al. IL-10 and TGF-β1 gene polymorphisms in Greek patients with recurrent aphthous stomatitis. Med Oral Patol Oral Cir Bucal. (2022) 27:e426–33. doi: 10.4317/medoral.25352
7. Ruan HH Li GY, Duan N, Jiang HL, Fu YF, Song YF, Zhou Q, et al. Frequencies of abnormal humoral and cellular immune component levels in peripheral blood of patients with recurrent aphthous ulceration. J Dent Sci. (2018) 13:124–30. doi: 10.1016/j.jds.2017.09.003
8. Al-Maweri SA, Halboub E, Al-Sharani HM, Shamala A, Al-Kamel A, Al-Wesabi M, et al. Association between serum zinc levels and recurrent aphthous stomatitis. A meta-analysis with trial sequential analysis. Clin Oral Investig. (2021) 25:407–15. doi: 10.1007/s00784-020-03704-8
9. Bao ZX, Shi J, Yang XW, Liu LX. Hematinic deficiencies in patients with recurrent aphthous stomatitis. Variations by gender and age. Med Oral Patol Oral Cir Bucal. (2018) 23:e161–7. doi: 10.4317/medoral.21885
10. Chiang CP, Yu-Fong Chang J, Wang YP, Wu YH, Wu YC, Sun A. Recurrent aphthous stomatitis—Etiology, serum autoantibodies, anemia, hematinic deficiencies, and management. J Formos Med Assoc. (2019) 118:1279–89. doi: 10.1016/j.jfma.2018.10.023
11. Al-Amad SH, Hasan H. Vitamin D and hematinic deficiencies in patients with recurrent aphthous stomatitis. Clin Oral Investig. (2020) 24:2427–32. doi: 10.1007/s00784-019-03102-9
12. Koparal M, Ege B, Dogan EI, Kurt MY, Bayazit S. Evaluation of biochemical variables in patients with recurrent aphthous stomatitis. J Stomatol Oral Maxillofac Surg. (2022). doi: 10.1016/j.jormas.2022.09.015
13. Öner m, Öner F, Kurt O, Özdemir S. The role of hematologic parameters in recurrent aphthous stomatitis. Ann Med Res. (2020) 27:495.
14. Tamer F, Avci E. Decreased serum ferritin and vitamin D levels in patients with recurrent aphthous stomatiti. Our Dermatol Online. (2019) 10:229–33. doi: 10.7241/ourd.20193.1
15. Chen H, Sui Q, Chen Y, Ge L, Lin M. Impact of haematologic deficiencies on recurrent aphthous ulceration. A meta-analysis. Br Dent J. (2015) 218:E8. doi: 10.1038/sj.bdj.2015.100
16. Piskin S, Sayan C, Durukan N, Senol M. Serum iron, ferritin, folic acid, and vitamin B12 levels in recurrent aphthous stomatitis. J Eur Acad Dermatol Venereol. (2002) 16:66–7. doi: 10.1046/j.1468-3083.2002.00369.x
17. Khammissa RAG, Fourie J, Motswaledi MH, Ballyram R, Lemmer J, Feller L. The biological activities of vitamin D and its receptor in relation to calcium and bone homeostasis, cancer, immune and cardiovascular systems, skin biology, and oral health. Biomed Res Int. (2018) 2018:9276380. doi: 10.1155/2018/9276380
18. Krawiecka E, Slebioda Z, Szponar E, Kowalska A, Dorocka-Bobkowska B. Vitamin D status in recurrent aphthous stomatitis. Postepy Dermatol Alergol. (2017) 34:612–7. doi: 10.5114/pdia.2017.69683
19. Luo T, Lin Y, Lu J, Lian X, Guo Y, Han L, et al. Effects of vitamin D supplementation during pregnancy on bone health and offspring growth. A systematic review and meta-analysis of randomized controlled trials. PLoS ONE. (2022) 17:e0276016. doi: 10.1371/journal.pone.0276016
20. Alsufiani HM, AlGhamdi SA, AlShaibi HF, Khoja SO, Saif SF, Carlberg C. A single vitamin D(3) Bolus supplementation improves vitamin D status and reduces proinflammatory cytokines in healthy females. Nutrients. (2022) 14:3963. doi: 10.3390/nu14193963
21. Dziedzic EA, Gasior JS, Tuzimek A, Dabrowski M, Jankowski P. The association between serum vitamin D concentration and new inflammatory biomarkers-systemic inflammatory index (SII) and systemic inflammatory response (SIRI)-in patients with ischemic heart disease. Nutrients. (2022) 14:4212. doi: 10.3390/nu14194212
22. Kuo CY, Huang YC, Lin KJ, Tsai TY. Vitamin D deficiency is associated with severity of dry eye symptoms and primary sjögren's syndrome. A systematic review and meta-analysis. J Nutr Sci Vitaminol. (2020) 66:386–8. doi: 10.3177/jnsv.66.386
23. Lee YH, Bae SC. Vitamin D level in rheumatoid arthritis and its correlation with the disease activity. A meta-analysis. Clin Exp Rheumatol. (2016) 34:827–33.
24. Yang M, Wu H, Zhao M, Long H, Lu Q. Vitamin D status in patients with autoimmune bullous dermatoses. A meta-analysis. J Dermatolog Treat. (2022) 33:1356–67. doi: 10.1080/09546634.2020.1810606
25. Islam MA, Khandker SS, Alam SS, Kotyla P, Hassan R. Vitamin D status in patients with systemic lupus erythematosus (SLE). A systematic review and meta-analysis. Autoimmun Rev. (2019) 18:102392. doi: 10.1016/j.autrev.2019.102392
26. Upala S, Sanguankeo A. Low 25-hydroxyvitamin D levels are associated with vitiligo. A systematic review and meta-analysis. Photodermatol Photoimmunol Photomed. (2016) 32:181–90. doi: 10.1111/phpp.12241
27. Slebioda Z, Szponar E, Dorocka-Bobkowska B. Vitamin D and its relevance in the etiopathogenesis of oral cavity diseases. Arch Immunol Ther Exp (Warsz). (2016) 64:385–97. doi: 10.1007/s00005-016-0384-z
28. Bahramian A, Falsafi P, Abbasi T, Ghanizadeh M, Abedini M, Kavoosi F, et al. Comparing serum and salivary levels of vitamin d in patients with recurrent aphthous stomatitis and healthy individuals. J Dent Shiraz Univ Med Sci. (2018) 19:5.
29. Ali NSM. Serum vitamin D levels in a sample of Iraqi female patients. Ind J Public Health Res Develop. (2019) 10:5. doi: 10.5958/0976-5506.2019.00178.5
30. Khabbazi A, Ghorbanihaghjo A, Fanood F, Kolahi S, Hajialiloo M, Rashtchizadeh N, et al. comparative study of vitamin D serum levels in patients with recurrent aphthous stomatitis. Egypt Rheumatol. (2015) 37:133–7. doi: 10.1016/j.ejr.2014.07.005
31. Al-Maweri SA, Halboub E, Al-Sufyani G, Alqutaibi AY, Shamala A, Alsalhani A. Is vitamin D deficiency a risk factor for recurrent aphthous stomatitis? A systematic review and meta-analysis. Oral Dis. (2019). doi: 10.1111/odi.13189
32. Hussein F, Elmarssafy L, Sadek H, Alqahtani M. Relationship between serum vitamin D level and recurrent aphthous ulcer. Egypt Dent J. (2020) 66:1015–23. doi: 10.21608/edj.2020.25583.1069
33. Mustafi S, Saha A, Sinha R, Sarkar S, Giri D, Yadav P. Comparative estimation of serum levels of vitamin A, vitamin B12, vitamin D and vitamin E in patients with recurrent aphthous stomatitis and normal individuals—A case-control study. J Indian Acad Oral Med Radiol. (2021) 33:21. doi: 10.4103/jiaomr.jiaomr_50_21
34. Nalbantoglu B, Nalbantoglu A. Vitamin D levels in children with recurrent aphthous stomatitis. Ear Nose Throat J. (2020) 99:460–3. doi: 10.1177/0145561319882783
35. Zakeri M, Parsian H, Bijani A, Shirzad A, Neamati N. Serum levels of vitamin D in patients with recurrent aphthous stomatitis. Dent Med Probl. (2021) 58:27–30. doi: 10.17219/dmp/126360
36. Wetterslev J, Jakobsen JC, Gluud C. Trial Sequential Analysis in systematic reviews with meta-analysis. BMC Med Res Methodol. (2017) 17:39. doi: 10.1186/s12874-017-0315-7
37. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement. an updated guideline for reporting systematic reviews. Bmj. (2021) 372:n71. doi: 10.1136/bmj.n71
38. Brok J, Thorlund K, Wetterslev J, Gluud C. Apparently conclusive meta-analyses may be inconclusive—Trial sequential analysis adjustment of random error risk due to repetitive testing of accumulating data in apparently conclusive neonatal meta-analyses. Int J Epidemiol. (2009) 38:287–98. doi: 10.1093/ije/dyn188
39. Oztekin A, Oztekin C. Vitamin D levels in patients with recurrent aphthous stomatitis. BMC Oral Health. (2018) 18:186. doi: 10.1186/s12903-018-0653-9
40. Başarslan F, Kaba I. Evaluation of vitamin D levels in pediatric patients with recurrent aphthous stomatitis. Cureus. (2022) 14:11. doi: 10.7759/cureus.32064
41. Öner m, Öner F, Kurt O, Özdemir S. The role of hematologic parameters in recurrent aphthous stomatitis. Ann Med Res. (2021) 28:290–5. doi: 10.5455/annalsmedres.2020.05.495
42. Al-Maweri SA, Alaizari N, Alanazi RH, Ashraf S, Alanazi RH, Al-Sharani HM, et al. Efficacy of hyaluronic acid for recurrent aphthous stomatitis. a systematic review of clinical trials/ Clin Oral Investig. (2021) 25:6561–70. doi: 10.1007/s00784-021-04180-4
43. Al-Maweri SA, Halboub E, Ashraf S, Alqutaibi AY, Qaid NM, Yahya K, et al. Single application of topical doxycycline in management of recurrent aphthous stomatitis. A systematic review and meta-analysis of the available evidence. BMC Oral Health. (2020) 20:231. doi: 10.1186/s12903-020-01220-5
44. Halboub E, Al-Maweri SA, Parveen S, Al-Wesabi M, Al-Sharani HM, Al-Sharani A, et al. Zinc supplementation for prevention and management of recurrent aphthous stomatitis. A systematic review. J Trace Elem Med Biol. (2021) 68:126811. doi: 10.1016/j.jtemb.2021.126811
45. Hussein FF, Sadek H, Elmarssafy LH. Impact of vitamin D3 supplementation on recurrent aphthous ulcer. Indian J Pharmaceut Sci. (2022) 3:255–265. doi: 10.36468/pharmaceutical-sciences.spl.440
46. Staeva-Vieira TP, Freedman LP. 1,25-dihydroxyvitamin D3 inhibits IFN-gamma and IL-4 levels during in vitro polarization of primary murine CD4+ T cells. J Immunol. (2002) 168:1181–9. doi: 10.4049/jimmunol.168.3.1181
Keywords: aphthous stomatitis, vitamin D, association, risk factor, meta-analyses
Citation: Al-Maweri SA, Al-Qadhi G, Halboub E, Alaizari N, Almeslet A, Ali K and Osman SAA (2023) Vitamin D deficiency and risk of recurrent aphthous stomatitis: updated meta-analysis with trial sequential analysis. Front. Nutr. 10:1132191. doi: 10.3389/fnut.2023.1132191
Received: 27 December 2022; Accepted: 06 June 2023;
Published: 22 June 2023.
Edited by:
Miroslava Rossenova Atanassova, Møreforsking AS, NorwayReviewed by:
Reza Rastmanesh, Independent Researcher, Tehran, IranCopyright © 2023 Al-Maweri, Al-Qadhi, Halboub, Alaizari, Almeslet, Ali and Osman. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sadeq Ali Al-Maweri, c2FkYWxpMDVAaG90bWFpbC5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.