 Rebecca K. Kelly
Rebecca K. Kelly Janet Calhoun2
Janet Calhoun2 Amy Hanus
Amy Hanus Pamela Payne-Foster
Pamela Payne-Foster Ron Stout
Ron Stout Bruce W. Sherman
Bruce W. Sherman- 1Element Health, Inc, Fairhope, AL, United States
- 2Ardmore Institute of Health (AIH), Ardmore, OK, United States
- 3College of Community Health Sciences, University of Alabama, Tuscaloosa, AL, United States
- 4School of Health and Human Sciences, University of North Carolina at Greensboro, Greensboro, NC, United States
Introduction: Prior studies have demonstrated that an intake of foods rich in dietary fiber is associated with a favorable impact on health status and body weight. However, the association between fiber intake and weight loss has not been well-studied in employer settings. This research aimed to assess the relationship between dietary fiber and weight loss among individuals participating in the Full Plate Living (FPL) program.
Methods: The 16-week plant-predominant fiber-rich eating program was delivered to 72 employers, primarily in the Southwest U.S., over 3 years (2017–2019). Participants received weekly video lessons, FPL materials, and additional online resources. A retrospective analysis of repeated measures was conducted using participant data obtained from 4,477 participants, of which 2,792 (62.5%) reduced body weight. Analysis of variance with post hoc analysis was used to assess the statistical significance of the changes between baseline and follow-up measures of dietary fiber intake in each of the food categories, specifically the relationship between changes in individual and combined (composite) daily servings of fruits, vegetables, whole grains, beans, and nuts on body weight measures among three groups at follow-up: those who lost, maintained, or gained weight. Multilevel modeling was used to test the hypothesis that increased intake of fiber was associated with greater weight loss.
Results: The mean weight loss for the weight loss group was 3.28 kg. As compared to the two other groups, the intake of whole fiber-rich foods at follow-up was significantly higher among the weight loss group with fruits (2.45 servings), vegetables (2.99 servings), beans (1.03 servings), and total fiber composites (9.07 servings; P < 0.001). A significant increase in servings of grains was also noted (P < 0.05). Multilevel modeling demonstrated that a higher total fiber composite (Model 1), as well as higher intakes of either vegetables or fruits (Model 2), resulted in greater weight loss.
Discussion: Our findings indicate that the FPL program can be a part of a lifestyle medicine approach to healthy eating and weight loss. Delivering the program in clinical, community, and workplace settings can increase its reach as an effective and low-cost offering.
Introduction
The workplace provides employers with opportunities to identify solutions to enhance employee health, wellbeing, and productivity while maintaining or reducing healthcare costs (1–6). Being overweight and obese is linked to increased healthcare expenditures across adults of all ages and body mass index ranges, particularly for individuals with severe obesity (7). Excess body weight is also linked to numerous comorbid and chronic health conditions including type 2 diabetes, heart disease, stroke, and various types of cancer. The Centers for Disease Control and Prevention Obesity (8) reports that the prevalence of obesity among adults living in the United States is 41.9%, of which ~60% of adults in the US are working (9). With the increased prevalence of obesity in the US, recent studies have expanded our understanding of dietary contributors to weight loss. Factors associated with weight loss are multifaceted and include adjustments in dietary intake of kilocalories, macronutrients, and fiber. Previous research suggests that a higher intake of dietary fiber is a predictor of weight loss and compliance with healthy eating when combined with an overall reduction in kilocalorie intake (10–14). Intake of foods high in fiber has also been associated with improved health, quality of life, and reductions in chronic health conditions (11–19).
Full Plate Living (FPL), a multicomponent nutrition education program, was designed for individuals and groups in clinical, workplace, and community settings. The details and benefits of the FPL program have been previously described (20–22). FPL's simplified healthy eating approach emphasizes small-step habit adoption to include the consumption of plant predominant foods high in fiber, such as fruits, vegetables, beans and legumes, cooked whole grains, and nuts (21). The focus of the FPL plant-predominant nutrition program is to gradually consume 75% of a meal from nutrient-dense, low-calorie foods that are high in fiber, or ~40 g of fiber per day, over time. FPL also emphasizes physical movement, consumption of water, and awareness of satiety cues.
The beneficial impact of FPL on improving eating behaviors and health values has been demonstrated in both community and employer settings (20, 23–25). A recent FPL analysis demonstrated significant improvements in eating behaviors and health status including increased consumption of fiber-rich foods of fruits, vegetables, whole grains, beans, and nuts; improvement in perceived health and energy values; increased confidence values of losing weight and choosing healthy foods, and overall weight loss (20). However, research gaps exist regarding our understanding of the relationship between weight modification and adherence to the FPL plant-predominant eating approach in the workplace.
This study aimed to assess the relationship between servings of whole-food plant-based foods high in fiber and the impact on body weight among employees in a workplace wellness program using the FPL program. More specifically, the present study is attempting to answer the following three questions:
(1) Does participation in the FPL program result in weight modification?
(2) As a result of participating in the FPL program, does total fiber intake or specific high-fiber foods play a role in weight loss; and
(3) To what extent does the FPL program yield differences across the following three groups: weight loss (WL), weight neutral (WN), and weight gain (WG)?
Methods
Study design
The study design, procedures, and intervention have been previously described in detail (20). The 16-week FPL program consisted of individuals receiving weekly online educational videos, FPL program curriculum materials, and online resources to include recipes and meal planning tips. A repeated measures study design was conducted using participant data from the FPL. A 20-question, self-reported confidential online health assessment was completed at both baseline and follow-up (within 3 weeks of program completion) and included questions about eating behaviors, perceived values of energy and health, and confidence values for healthy eating and weight loss. Daily servings of fiber-rich food, including fruits, vegetables, beans, grains, and nuts, were recorded by participants in a food diary. Because this study was a retrospective, post hoc analysis of de-identified data, IRB approval for the study was not obtained.
Subjects
The program was delivered through 72 employers located primarily in the Southwest U.S. from 2017 to 2019. Employee participants were recruited through their organization's wellness program. A total of 6,820 individuals were enrolled in the FPL program, of which 4,477 were included in the analysis as they completed the baseline and follow-up health questionnaires.
Measures
Measures of data-specific variables were previously described (20), including demographic characteristics, food intake, self-perceived health and energy values, confidence scores, and body weight.
Demographic characteristics
Available demographic details were limited to age and gender. Gender was coded as male or female.
Food intake
Food intake was self-reported by asking “How many actual servings of food do you consume each day over the last 2 weeks for each of the following food categories, such as fruits, vegetables, beans, whole grains, nuts?”
Self-perceived health
Responses were coded into five categories: excellent, very good, good, fair, and poor.
Self-perceived energy
The self-perceived energy question was assessed on a 5-point scale by asking “How would you describe your energy level in the past month?” Responses were coded into five categories: very high energy, high energy, moderate energy, low energy, and no energy.
Confidence scores
Participants recorded their confidence for each item on a 10-point scale, ranging from 0 (no confidence) to 10 (complete confidence).
Additional measures were evaluated for this study to include body weight, fiber composite, and overall water intake.
Body weight categories
Body weight was self-reported and provided a comparative measure of pre- and post-program change. Participants were divided into three groups based on their baseline and follow-up program weight change: WL, WN, and WG. Individuals recorded their weight to the nearest pound measurement. Participants who lost >1 pound or 0.45 kg of body weight were included in the WL group. Participants who maintained their weight, <1 pound or 0.45 kg, of body weight change were included in the WN group. Individuals who gained more than one pound or 0.45 kg were included in the WG category.
Fiber composite
A high-fiber food composite was developed by adding the total number of daily servings of fiber-rich foods.
Water intake
Water was assessed based on the number of cups of water consumed per day.
Analyses
Analysis of variance with post hoc analysis was used to assess the statistical significance of the changes between baseline and follow-up measures of dietary fiber intake in each of the food categories, specifically the relationship between changes in individual and combined (composite) servings of fruits, vegetables, grains, beans, and nuts on body weight measures among the three weight groups. The WL group was used as the reference with a comparison to both WN and WG values for the post hoc measures.
Multilevel modeling was used to test the hypothesis that increased fiber intake was associated with lower body weight at follow-up (i.e., weight loss). Random-intercept models were estimated with repeated measures nested in subjects. Two models were estimated. Model 1 had fiber composite as the independent variable of main interest. In comparison, Model 2 examined individual high-fiber food categories including vegetables, fruits, nuts, beans, and whole grains. Included as time-varying covariates were water intake, and a variable (time), to capture secular trends. Time-varying variables were person-mean centered to estimate their within-subject association with body weight. With two repeated measures, person-mean centering was equivalent to a change score. Age and gender were included as time-invariant covariates.
Results
The program included 6,820 program participants; of which, 4,477 individuals completed baseline and program self-reported questionnaires; therefore included in the program analysis.
Table 1 presents descriptive statistics for baseline demographic characteristics for all participants (n = 4,447) including subgroups based on body weight category. The average age for all participants was 45.7 (SD + 11.7). Consistent with similar nutrition and weight management studies demonstrating that women participate at rates three times greater than men (26, 27), the majority of study participants were women (87.0%). Of the three weight groups, the WL category was the largest, at 62.5% (n = 2,792), with an additional 22.0% gaining weight (n = 988) and 15.5% maintaining their weight (n = 697). The mean body weight for all female participants was 86.3 kg (SD + 21.8), while the mean body weight for male participants was 101.3 kg (SD + 22.0).
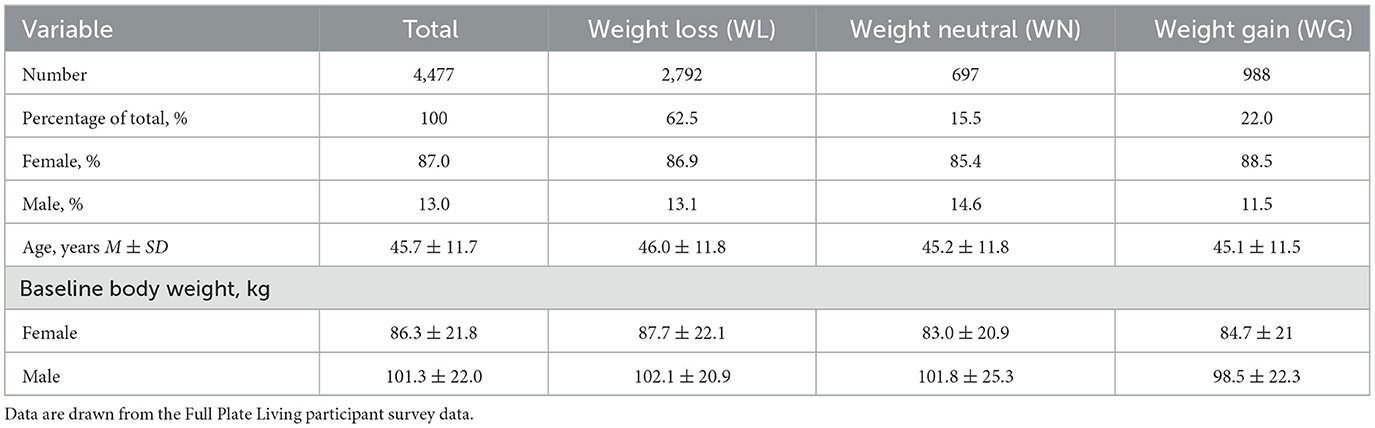
Table 1. Baseline demographic characteristics of participants by weight loss category.
Baseline and follow-up measures of participant eating behaviors, health measures, and confidence levels among all three weight groups are presented in Table 2. Significant weight loss was demonstrated for the WL group, with a mean of 3.28 kg (P < 0.01) for all participants losing weight as compared to an average body weight increase of 2.22 kg in the WG group. Further segmentation by gender among the weight loss group revealed that female participants lost 3.17 kg (P < 0.01) of body weight as compared to male participants at 4.06 kg weight loss (P < 0.01). Both of the WL values were significantly different from those in the WN and WG categories.
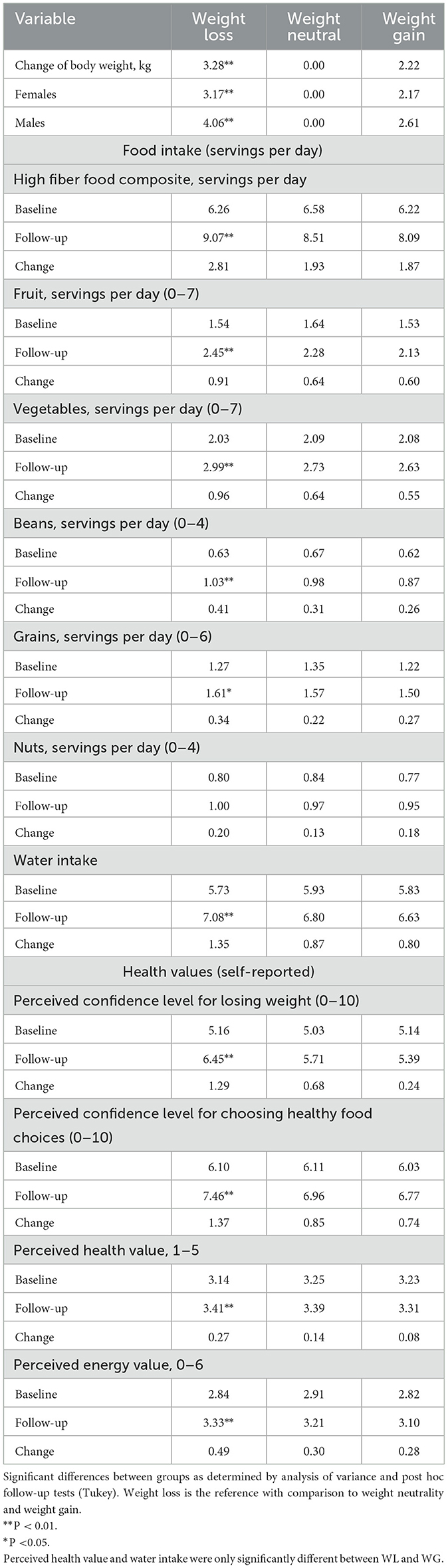
Table 2. Change in health measures, eating behaviors, and confidence values by weight loss category.
Previous studies demonstrated that FPL participants had statistically significant improvements in eating behaviors of fiber-rich foods between baseline and follow-up (20). Unique to this study was the development of a total fiber composite. As a result of the FPL program, participants in the WL group significantly increased their daily total intake of high-fiber foods by 2.81 servings to 9.07 daily servings (P < 0.01) as compared to 8.51 servings for WN and 8.09 servings for the WG group.
Daily servings of fruits, vegetables, beans, and grains were also significantly higher for the WL category at follow-up as compared to the WN and WG categories. The greatest change occurred in daily servings of fruits (0.91), vegetables (0.96), beans (0.41), and grains (0.34). The WL category recorded significantly higher servings of fruits, vegetables, and beans at 2.45 (P < 0.01), 2.99 (P < 0.01), and 1.03 (P < 0.01) as compared to the WN and WG groups. The WL group also had a significantly higher daily intake of whole grains at 1.61 servings compared to the WN and WG groups of 1.57 and 1.50 servings, respectively (P < 0.01). There was no significant difference among servings of nuts at follow-up across the body weight categories.
Confidence levels in losing weight were significantly higher for the WL group at 6.45 (P < 0.01) as compared to the categories of WN at 5.71 and WG at 5.39. The WL group confidence levels in making healthy choices were also significantly higher at 7.46 (P < 0.01) as compared to the categories of WN at 6.96 and WG at 6.77. The self-perceived health values for the WL group were significantly higher at 3.41 than the WG group at 3.31 but not of the WN group at 3.39. Self-perceived energy values were significantly different for the WL group at 3.33 (P < 0.01) as compared to the WN group at 3.21 and 3.10 for the WG group.
Table 3 shows the relationship between fiber intake and body weight through the development of two models. Model 1 demonstrates that a higher intake of total high-fiber foods (composite) at follow-up was associated with lower body weight (P < 0.01). Model 2 revealed that of the individual food categories of high-fiber foods (fruits, vegetables, beans, whole grains, and nuts), a higher intake of vegetables or fruits was associated with weight loss (P < 0.01). As a result of the multilevel modeling analysis, increases in the intake of nuts, beans, or grains were not associated with weight change during the study period (P > 0.15).
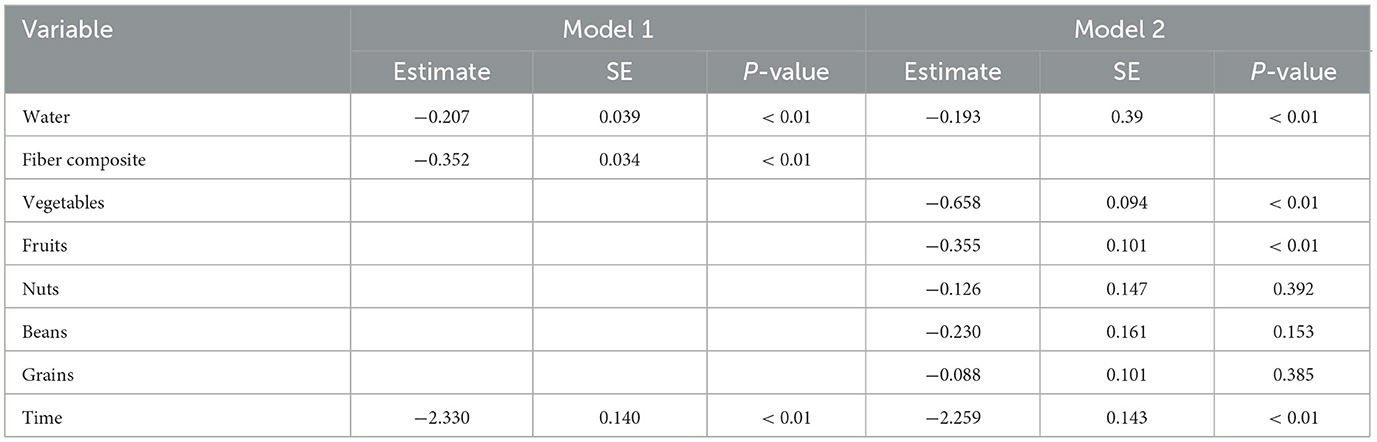
Table 3. Within-subject associations between intake of fiber-rich food composition, individuals' fiber-rich food categories, and body weight.
Discussion
Research has demonstrated that an intake of foods high in fiber is associated with a favorable impact on health status and body weight. This study adds to the body of literature examining the impact of a plant predominant fiber-rich eating approach and its relationship to weight loss in employer settings. More specifically, this study examines the relationship of dietary fiber among individuals participating in the FPL program. As demonstrated in previous studies, there is a direct relationship between the intake of dietary fiber and weight loss (10, 11, 14–17).
The initial finding confirms that the 16-week FPL program results in weight loss among the majority of participants, with 62.5% reporting weight loss. These results can help to address the adverse impact of obesity on health and productivity in the workplace and community by providing a low-cost healthy eating program (21). FPL promotes a healthy nutrition eating approach through a small-step adoption of improved eating habits through the gradual consumption of 75% of nutrients from plant-based whole foods while incorporating sustained adoption of healthy living and nutrition principles.
Further analysis evaluated the difference between three weight groups: those who lost weight, maintained weight, and gained weight. Of the WL group, there was a significant increase in total and individual servings of high-fiber foods including fruits, vegetables, beans, whole grains, and nuts. The WL group consumed 9.07 total daily servings, which was an increase of 0.56 over the WN group, and 0.98 serving more than the WG group. More specifically, the greatest intake of fiber-rich foods came from vegetables at 2.99 or 0.26 and 0.36 servings more than the WN and WG groups, respectively. As a result, our second finding demonstrated that as a result of participating in the FPL program, both the total intake of high-fiber foods, as well as select fiber-rich foods, play a significant role in body weight loss as higher daily servings resulted in greater weight loss. As with previous studies (28–30), individuals who consume higher amounts of vegetables and fruits have greater weight loss as these foods are high in fiber but lower in calories than other high-fiber foods such as beans, grains, and nuts.
The third finding of this study supports the hypothesis that dietary fiber is associated with weight loss. In our analysis, the change in fiber intake from baseline to 16 weeks was a consistent and strong predictor of weight loss. The association between increased fiber intake in the total fiber composite (Model 1) as well as and Model 2, the increased intake of vegetables or fruits, while controlling for water intake. Weight loss increases as total fiber intake, or more specifically fruit or vegetable intake increases.
Additional findings demonstrated that individuals within the WL group also had higher values of perceived energy and confidence values for losing weight and making healthier choices as compared to the other groups. Individuals who improve their health and lose weight have also been shown to have great self-efficacy (31).
There were notable limitations to the study. First, the study was 16 weeks in length and may not be reflective of long-term results. Second, as noted in previous FPL studies (20, 23, 24), self-reported survey data were used for analysis, inclusive of estimated servings of food in place of a daily food log and corresponding analysis. Third, demographic data were limited to age and gender, preventing stratification or adjustment of participant data based on race, ethnicity, and/or socioeconomic status. Finally, attrition bias is one of the major challenges in nutrition and weight management programs, consistent with this study. Future studies of the FPL program should include a longer-term program evaluation period with improved survey instruments, standardized weight measurement, comparison group, and analysis of exercise-related impact.
Despite these limitations, the study has implications for nutrition interventions. Specifically, FPL program interventions delivered at the workplace have been demonstrated to improve weight loss and therefore overall health. Due to these benefits, the FPL program may offer employers a strategy to improve both workplace productivity and healthcare costs. Programs such as FPL are also beneficial to be delivered in clinical and community settings as they may improve patient and community health. The FPL program has been found to improve overall eating habits, and for individuals who consume significant increases in fiber intake, there is corresponding weight loss. In summary, this study identified that the FPL program was effective in improving weight loss as a result of increased intake of high-fiber foods, including the consumption of total fiber and fruits and vegetables. In addition, improvements were significantly higher for confidence in losing weight, confidence in making healthy choices, and perceived health and energy values for the WL group. Future studies could focus on exploring dietary fiber intake and weight loss as part of a longer-term program in multiple settings. In addition, fiber's role in improving health through the measurement of additional clinical markers should be considered in future FPL studies.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. The ethics committee waived the requirement of written informed consent for participation.
Author contributions
RKK: conceptualization, methodology, design and formal analysis, writing, reviewing, editing, and ongoing communications. AH, JC, and RS: data collection, design analysis assistance, manuscript review and editing, and liaisons of the data and background literature. PP-F: ongoing review and edits to the manuscript. BWS: conceptualization, design analysis assistance, writing, reviewing, and editing. All authors contributed to the article and approved the submitted version.
Conflict of interest
RKK, PP-F, and BWS were paid consultants of Ardmore Institute of Health. RKK was employed by Element Health, Inc. AH, JC, and RS were employed by Ardmore Institute of Health.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Goetzel RZ, Henke RM, Tabrizi M, Pelletier KR, Loeppke R, Ballard DW, et al. Do workplace health promotion (wellness) programs work? J Occup Environ Med. (2014) 56:927–34. doi: 10.1097/JOM.0000000000000276
2. O'Donnell MP. Health Promotion in the Workplace. Troy, MI: Art & Science Of Health Promotion Institute (2017).
3. Edington DW, Burton WN, Schultz AB. Health and economics of lifestyle medicine strategies. Am J Lifestyle Med. (2020) 14:274–7. doi: 10.1177/1559827620905782
4. Dement JM, Epling C, Joyner J, Cavanaugh K. Impacts of workplace health promotion and wellness programs on health care utilization and costs. J Occup Environ Med. (2015) 57:1159–69. doi: 10.1097/JOM.0000000000000555
5. Unsal N, Weaver G, Bray J, Bibeau D. A scoping review of economic evaluations of workplace wellness programs. Public Health Rep. (2021) 136:003335492097655. doi: 10.1177/0033354920976557
6. Newman LS, Stinson KE, Metcalf D, Fang H, Brockbank CS, Jinnett K, et al. Implementation of a worksite wellness program targeting small businesses. J Occup Environ Med. (2015) 57:14–21. doi: 10.1097/JOM.0000000000000279
7. Ward ZJ, Bleich SN, Long MW, Gortmaker SL. Association of body mass index with health care expenditures in the United States by age and sex. PLOS ONE. (2021) 16:e0247307. doi: 10.1371/journal.pone.0247307
8. Bryan S, Afful J, Carroll M, Te-Ching C, Orlando D, Fink S, et al . NHSR 158. National Health Nutrition Examination Survey 2017–March 2020 Pre-pandemic Data Files. Centers for Disease Control Prevention. National Center for Health Statistics U.S. (2021). Available online at: https://stacks.cdc.gov/view/cdc/106273 (accessed October 14, 2022).
9. Bureau of Labor Statistics. The Employment Situation - March 2022. Bureau of Labor Statistics. Bureau Of Labor Statistics. (2022). Available online at: https://www.bls.gov/news.release/pdf/empsit.pdf (accessed October 14, 2022).
10. Miketinas DC, Bray GA, Beyl RA, Ryan DH, Sacks FM, Champagne CM. Fiber intake predicts weight loss and dietary adherence in adults consuming calorie-restricted diets: the POUNDS lost (preventing overweight using novel dietary strategies) study. J Nutr. (2019) 149:1742–8. doi: 10.1093/jn/nxz117
11. Sylvetsky AC, Edelstein SL, Walford G, Boyko EJ, Horton ES, Ibebuogu UN, et al. A high-carbohydrate, high-fiber, low-fat diet results in weight loss among adults at high risk of type 2 diabetes. J Nutr. (2017) 147:jn252395. doi: 10.3945/jn.117.252395
12. Michaud TL, Nyman JA, Jutkowitz E, Su D, Dowd B, Abraham JM. Effect of workplace weight management on health care expenditures and quality of life. J Occup Environ Med. (2016) 58:1073–8. doi: 10.1097/JOM.0000000000000864
13. Bozzetto L, Costabile G, Della Pepa G, Ciciola P, Vetrani C, Vitale M, et al. Dietary fibre as a unifying remedy for the whole spectrum of obesity-associated cardiovascular risk. Nutrients. (2018) 10:943. doi: 10.3390/nu10070943
14. Mishra S, Xu J, Agarwal U, Gonzales J, Levin S, Barnard ND, et al. multicenter randomized controlled trial of a plant-based nutrition program to reduce body weight and cardiovascular risk in the corporate setting: the GEICO study. Eur J Clin Nutr. (2013) 67:718–24. doi: 10.1038/ejcn.2013.92
15. Veronese N, Solmi M, Caruso MG, Giannelli G, Osella AR, Evangelou E, et al. Dietary fiber and health outcomes: an umbrella review of systematic reviews and meta-analyses. Am J Clin Nutr. (2018) 107:436–44. doi: 10.1093/ajcn/nqx082
16. Partula V, Deschasaux M, Druesne-Pecollo N, Latino-Martel P, Desmetz E, Chazelas E, et al. Associations between consumption of dietary fibers and the risk of cardiovascular diseases, cancers, type 2 diabetes, and mortality in the prospective NutriNet-Santé cohort. Am J Clin Nutr. (2020) 112:195–207. doi: 10.1093/ajcn/nqaa063
17. Dahl WJ, Stewart ML. Position of the academy of nutrition and dietetics: health implications of dietary fiber. J Acad Nutr Diet. (2015) 115:1861–70. doi: 10.1016/j.jand.2015.09.003
18. Xu X, Zhang J, Zhang Y, Qi H, Wang P. Associations between dietary fiber intake and mortality from all causes, cardiovascular disease and cancer: a prospective study. J Transl Med. (2022) 20:344. doi: 10.1186/s12967-022-03558-6
19. Kurnik-Łucka M, Grońska D, Wojnarski M, Pasieka P, Rzasa-Duran E, Gil K. Health-related quality of life in relation to fruit and vegetable intake among polish pharmacists. Healthcare. (2022) 10:930. doi: 10.3390/healthcare10050930
20. Kelly R, Hanus A, Payne-Foster P, Calhoun J, Stout R, Sherman BW. Health benefits of a 16-week whole food, high fiber, plant predominant diet among U.S. employees. Am J Health Promot. (2022) 0:089011712211160. doi: 10.1177/08901171221116066
21. Hanus A,. Full Plate Living. Ardmore Institute of Health (2022). Available from: https://www.ardmoreinstituteofhealth.org/full-plate-living (accessed October 30, 2022).
22. Hanus A. Healthy 25% Picks - Here's What We Recommend. (2022). Available online at: https://www.fullplateliving.org/blog/healthy-25-picks (accessed October 30, 2022).
23. Downes LS, Buchholz SW, Bruster B, Girimurugan SB, Fogg LF, Frock MS. Delivery of a community-based nutrition education program for minority adults. J Am Assoc Nurse Pract. (2019) 31:269–77. doi: 10.1097/JXX.0000000000000144
24. Downes LS, Buchholz SW, Fogg LF. Impact of a nutrition education program on health behaviors in a university workplace wellness program. J Am Assoc Nurse Pract. (2021) 13:1198–206. doi: 10.1097/JXX.0000000000000553
25. Joachim-Célestin M, Rockwood NJ, Clarke C, Montgomery SB. Evaluating the Full Plate Living lifestyle intervention in low-income monolingual Latinas with and without food insecurity. Womens Health. (2022) 18:1–15. doi: 10.1177/17455057221091350
26. Robertson C, Avenell A, Boachie C, Stewart F, Archibald D, Douglas F, et al. Should weight loss and maintenance programmes be designed differently for men? A systematic review of long-term randomised controlled trials presenting data for men and women: the ROMEO project. Obes Res Clin Pract. (2016) 10:70–84. doi: 10.1016/j.orcp.2015.04.005
27. Crane MM, Jeffery RW, Sherwood NE. Exploring gender differences in a randomized trial of weight loss maintenance. Am J Mens Health. (2016) 11:369–75. doi: 10.1177/1557988316681221
28. Dreher ML, Ford NA. A comprehensive critical assessment of increased fruit and vegetable intake on weight loss in women. Nutrients. (2020) 12:1919. doi: 10.3390/nu12071919
29. Nour M, Lutze S, Grech A, Allman-Farinelli M. The relationship between vegetable intake and weight outcomes: a systematic review of cohort studies. Nutrients. (2018) 10:1626. doi: 10.3390/nu10111626
30. Sartorelli DS, Franco LJ, Cardoso MA. High intake of fruits and vegetables predicts weight loss in Brazilian overweight adults. Nutr Res. (2008) 28:233–8. doi: 10.1016/j.nutres.2008.02.004
Keywords: workplace, nutrition, dietary fiber, plant predominant, weight loss, whole food, intervention
Citation: Kelly RK, Calhoun J, Hanus A, Payne-Foster P, Stout R and Sherman BW (2023) Increased dietary fiber is associated with weight loss among Full Plate Living program participants. Front. Nutr. 10:1110748. doi: 10.3389/fnut.2023.1110748
Received: 29 November 2022; Accepted: 20 March 2023;
Published: 17 April 2023.
Edited by:
Andrea K. Boggild, University of Toronto, CanadaReviewed by:
Ceren Gezer, Eastern Mediterranean University, TürkiyeSwana Kopalakrishnan, Western University, Canada
Copyright © 2023 Kelly, Calhoun, Hanus, Payne-Foster, Stout and Sherman. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Amy Hanus, YW15QGZ1bGxwbGF0ZWxpdmluZy5jb20=