
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Nutr. , 05 July 2023
Sec. Clinical Nutrition
Volume 10 - 2023 | https://doi.org/10.3389/fnut.2023.1097860
This article is part of the Research Topic Impact of Diet-Related Disorders on Musculoskeletal Health View all 5 articles
 Guanghui Cui1,2
Guanghui Cui1,2 Shaojie Li3,4
Shaojie Li3,4 Hui Ye1,2
Hui Ye1,2 Yao Yang1,2
Yao Yang1,2 Yingming Chu1,2
Yingming Chu1,2 Xiaofen Jia1,2
Xiaofen Jia1,2 Yue Feng1,2
Yue Feng1,2 Miaomiao Lin1,2
Miaomiao Lin1,2 Xuezhi Zhang1,2*
Xuezhi Zhang1,2*Objectives: Patients with digestive diseases frequently suffer from dyspepsia and malabsorption, which may lead to muscle loss due to malnutrition. However, it is not clear whether digestive diseases are associated with sarcopenia. This study aims to explore the longitudinal association between digestive diseases and sarcopenia in middle-aged and older adults based on a nationally representative survey from China.
Methods: We used a prospective cohort study including 7,025 middle-aged and older adults aged ≥45 years from the 2011 to 2015 waves China Health and Retirement Longitudinal Study (CHARLS). Digestive diseases were identified using self-report. The assessment of sarcopenia was based on the Asian Working Group for Sarcopenia 2019 Consensus and included three components of muscle strength, physical performance, and muscle mass. Cox hazards regression was used to examine the association between digestive diseases and sarcopenia.
Results: The prevalence of digestive diseases and the incidence of sarcopenia in middle-aged and older adults were 22.6% (95% CI = 21.6–23.6%) and 8.5% (95% CI = 7.8–9.1%). After adjusting for 15 covariates composed of three sets (demographic characteristics, lifestyles, and health status), digestive diseases were associated with a higher risk of sarcopenia (HR = 1.241, 95% CI = 1.034–1.490, P < 0.05). The associations were more pronounced among men, older adults aged 60–79, rural residents, and married people. In addition, the association between digestive diseases and sarcopenia was robust in the sensitivity analysis.
Conclusion: Digestive diseases were associated with an increased risk of sarcopenia in middle-aged and older adults aged ≥45 years. Early intervention of digestive diseases may help to reduce the incidence of sarcopenia in middle-aged and older adults.
Sarcopenia refers to a generalized and progressive skeletal muscle disorder including the loss of muscle strength and mass (1). A recent systematic review and meta-analysis indicated that the global prevalence of sarcopenia ranged from 10 to 27%, with the prevalence of severe sarcopenia varying between 2 and 9% (2). Sarcopenia not only decreased the quality of life for individuals but also caused serious economic and medical burdens to society and families. Numerous studies have shown that sarcopenia was associated with increased risks of adverse health outcomes such as falls, fractures (3), and mortality (4). In addition, it was identified as a predictor of increased health service use and healthcare costs according to the evidence from different countries (5, 6). Therefore, exploring its risk factors to achieve precise screening and early prevention has become the focus of interest in the field of clinical practice, geriatric and public health.
Previous studies mainly investigated the associated factors of sarcopenia from the perspective of sociodemographic characteristics (7) and nutritional status (8). In addition to these factors, studies have found that sarcopenia may also be secondary to some long-term diseases or co-exist with these pathological conditions (1, 9). Previous studies suggested an increased prevalence of sarcopenia in those with bone and joint diseases, cancer, chronic heart failure, chronic obstructive pulmonary disease, and diabetes (9). The long-term existence of these diseases would damage the physiological function of the body, lead to long-term chronic inflammation, and metabolic disturbances, and then induce sarcopenia (10). Based on these discovered factors, many studies have explored the intervention measures for sarcopenia, mainly involving exercise and nutritional supplements (11). A systematic review showed that exercise intervention can improve muscle strength and physical function, while the results of nutrition intervention were ambiguous (12), which may be related to the different kinds of nutrients taken. A recent systematic review and meta-analysis of nutrition supplement interventions found that different types of nutrients had different effects on the muscle mass and strength of older adults (13). In addition to the type of nutrients, the effect of nutrition supplements also depends on whether the individual can effectively absorb nutrients, which is directly related to the individual’s digestive and absorption function.
Patients with digestive diseases often have digestive disorders, which may lead to muscle loss due to poor absorption of nutrients. However, few studies have explored whether digestive diseases are associated with an increased risk of sarcopenia. A previous cross-sectional study that enrolled 303 patients with digestive diseases in Japan reported that the prevalence of sarcopenia was 32.0% (14), which indicated patients with digestive diseases often suffer from sarcopenia. However, it was impossible to explore the relationship between digestive diseases and sarcopenia, because this study only selected patients with digestive diseases as samples. Therefore, it is necessary to further examine the association between digestive diseases and sarcopenia to provide scientific evidence for the intervention of sarcopenia in the future. Malnutrition was identified as a highly prevalent complication in patients with digestive diseases such as gastroparesis (15), inflammatory bowel disease (16), pancreatic disease (17), cirrhosis (18), and non-alcoholic fatty liver disease (19). The Belgian population-based cohort study involving 534 community-dwelling older people showed that malnutrition was a strong predictor of the onset of sarcopenia (20). Recently, researchers put forward a view of the gut-muscle axis (21). They believed that the gastrointestinal tract and skeletal muscles interact with each other through hormones, gut microbes, and metabolites (22). This further implies the possible relationship between digestive diseases and sarcopenia.
Therefore, given the existing research gaps, we used a prospective cohort study to explore the association between digestive diseases and sarcopenia. This will provide evidence based on the Chinese community population level for further examining the association between digestive diseases and sarcopenia. It is contributed to simply targeting high risk populations in community screening and intervention of sarcopenia.
We used the 2011 to 2015 waves of China Health and Retirement Longitudinal Study (CHARLS) data to conduct a prospective cohort study. CAHRLS is a national survey of middle-aged and older adults in China, which adopts a multi-stage stratified probability sampling method and has good national representation (23). CHARLS started the baseline survey in 2011, followed by a follow-up about every 2 years. At present, the survey data for four times in 2011, 2013, 2015, and 2018 have been disclosed. Since the data in 2018 only published questionnaire data, but not biomarker data, we used the data in 2011–2015 to explore the association between digestive system diseases and sarcopenia. In 2011, CHARLS recruited 17,708 participants. After excluding samples under the age of 45 and those with missing data, 10,400 participants were included at baseline. Subsequently, we excluded participants with sarcopenia in 2011 and those who were lost or missing sarcopenia data in the 2013 and 2015 surveys, and finally 7,025 participants entered the final analysis. The sample selection process is shown in Figure 1. CHARLS has been approved by the Ethics Committee of Peking University (No. IRB00001052-11015), and all participants have obtained informed consent.

Figure 1. The selection process of participants.
Digestive diseases were identified using self-report. Participants were asked, “Have you been diagnosed with Stomach or other digestive diseases (except for tumor or cancer) by a doctor?” When participants answered “yes” was determined to have digestive diseases. In this study, we defined digestive diseases as a binary variable (no vs. yes).
The assessment of sarcopenia was based on the Asian Working Group for Sarcopenia 2019 Consensus and includes three components of muscle strength, physical performance, and muscle mass (24). Muscle strength was measured using a standardized handgrip strength meter (Yuejian WL-1000, China). The handgrip strength of men below 28 kg and women below 18 kg is considered low muscle strength (24). Five-time chair stand tests were used to evaluate the individual’s physical performance. The time of 5-time chair stand tests ≥12 s is considered low physical performance (24). The muscle mass was evaluated by the appendicular skeletal muscle mass (ASM). Since CHARLS does not use instruments to measure ASM, we used previously validated anthropometric formulas (ASM = 0.193 × body weight + 0.107 × height − 4.157 × sex (men = 1, women = 2) − 0.037 × age − 2.631) to estimate ASM (25). To reduce the potential impact of height on ASM, we adjust the height of ASM by dividing ASM by the square of height (ASM/Ht2). Referring to the previous study (26), we set the low muscle mass as lower than the 20th percentile of ASM for sex. Low muscle mass + low muscle strength or low physical performance was considered sarcopenia.
Covariates in this study include three sets: demographic characteristics, lifestyles, and health status. Demographic characteristics included age, sex, residence (rural or urban), marital status (married or unmarried), and education level (illiterate, or primary school, or middle school and above). Lifestyles included smoking (current non-smoker or current smoker), drinking (current non-drinker or current drinker), exercise (hardly or regularly), social activity participation (No or Yes), and meal frequency (<3 or ≥3 meals per day). Health status included chronic diseases (No or Yes), cognitive function [cognitive normal or mild cognitive impairment (MCI)], functional limitations (No or Yes), visual impairment (No or Yes), and hearing impairment (No or Yes). More details of the measurement of covariates are in the Supplementary material.
STATA version 17.0 (StataCorp, College Station, TX, USA) was used to perform all statistical analyses. We used the Chi-square test to compare the differences in demographic characteristics, lifestyles, and health status between groups with and without digestive diseases. Cramer’s V statistic was used to estimate the effect size. Cox hazards regression was used to examine the association between digestive diseases and sarcopenia. Hazard Ratio (HR) and 95% confidence interval (CI) were used to estimate the strength of association and statistical significance, respectively. We estimated the following four models: model 1 was unadjusted; model 2 adjusted age, sex, residence, marital status, and education level; model 3 adjusted smoking, drinking, exercise, social activity participation, and meal frequency based on model 2; model 4 further adjusted chronic diseases, cognitive function, functional limitations, hearing impairment, and visual impairment based on model 3. To test the heterogeneity of the results, we conducted subgroup analyses among sex, age, residence, and marital status. Meanwhile, we also examined the interaction of digestive diseases with sex, age, residence, and marital status for associations with sarcopenia. In addition, we excluded individuals with MCI for sensitivity analysis to test the robustness of the association between digestive diseases and sarcopenia. We set P < 0.05 as statistically significant.
The mean age of 7,025 participants was 57.3 years (SD: 9.4). The prevalence of digestive diseases and the incidence of sarcopenia in middle-aged and older adults were 22.6% (95% CI = 21.6–23.6%) and 8.5% (95% CI = 7.8–9.1%). More detailed information regarding the characteristics of participants according to digestive diseases is shown in Table 1.
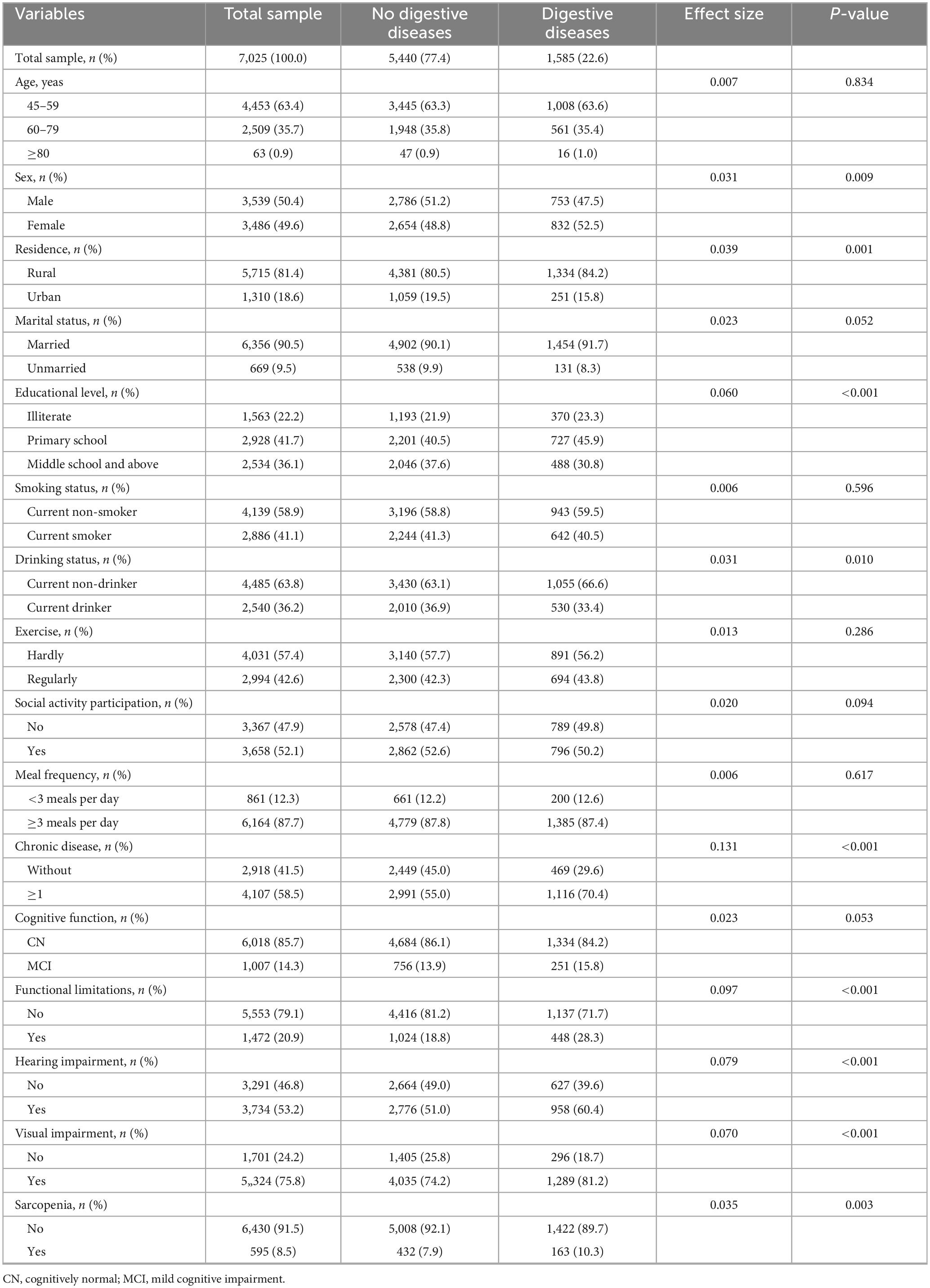
Table 1. Characteristics of participants according to digestive diseases.
Table 2 displays the results of the association between digestive diseases and sarcopenia among the whole sample. Model 1 showed that digestive diseases were significantly associated with a high risk of sarcopenia (HR = 1.304, 95% CI = 1.089–1.562, P < 0.01). After adjusting for age, sex, residence, marital status, and educational level in model 2, the association weakened but was still significant (HR = 1.270, 95% CI = 1.061–1.522, P < 0.01). And then, we further adjusted smoking, drinking, exercise, social activity participation, and meal frequency based on model 2, digestive diseases were also associated with a higher risk of sarcopenia (HR = 1.266, 95% CI = 1.057–1.516, P < 0.05) in model 3. Finally, model 4 shows that digestive diseases still increased the risk of sarcopenia (HR = 1.241, 95% CI = 1.034–1.490, P < 0.05) after adjusting health status.
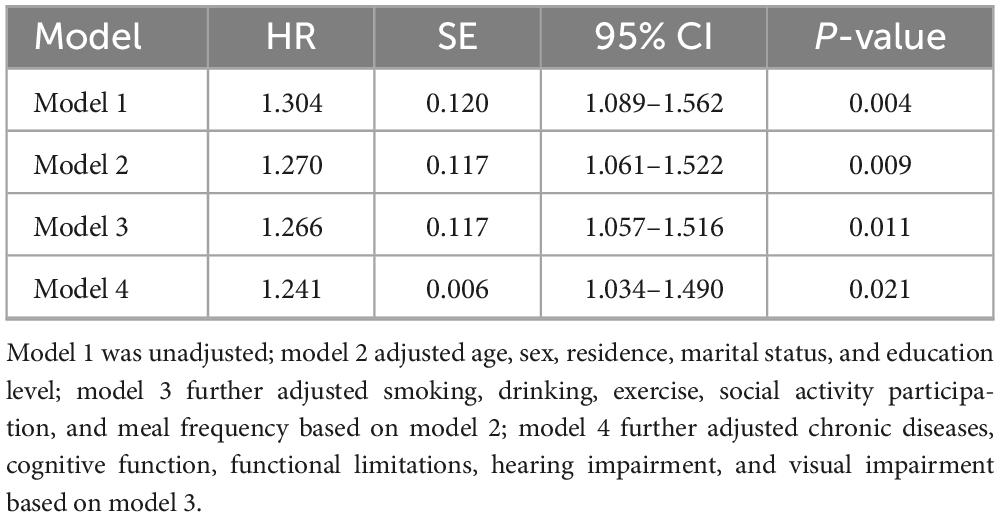
Table 2. Associations between digestive diseases and sarcopenia among whole sample.
The results of the subgroup analysis showed that the association between digestive diseases and sarcopenia was heterogeneous among sex, age, residence, and marital status. Specifically, the association was more pronounced among males, older adults aged 60–79 years, rural residents, and married people. However, we found no significant interaction effects. Details of the subgroup analysis are shown in Figure 2.
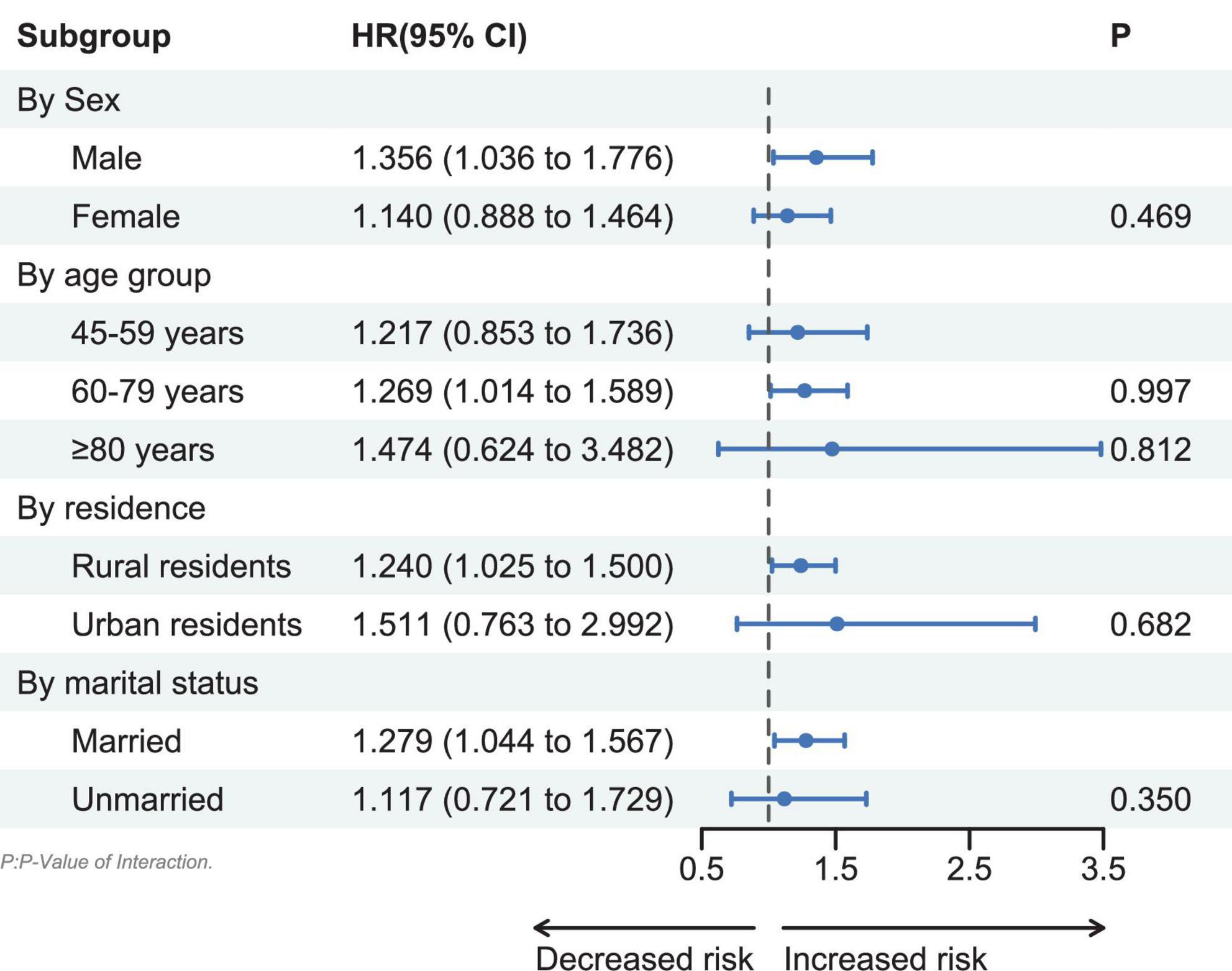
Figure 2. Subgroup analyses of associations between digestive diseases and sarcopenia.
After excluding participants with MCI, digestive diseases were still associated with sarcopenia (HR = 1.387, 95% CI = 1.126–1.707, P = 0.002). This result suggested that the association of digestive diseases with sarcopenia was robust.
Based on a nationally representative survey, this study explored the longitudinal association between digestive diseases and sarcopenia in middle-aged and older adults in China. As far as we know, this is the first study to explore the above association based on the Chinese population. This study found that digestive diseases were associated with a higher risk of sarcopenia among Chinese middle-aged and older adults, which further enriched the relevant factors of sarcopenia, and provided new intervenable factors for future prevention and intervention.
Although previous studies have not directly explored the above associations, some studies have investigated the association between gastrointestinal diseases and the components of sarcopenia. A longitudinal study based on UK Biobank showed that gastrointestinal diseases predicted a decline in grip strength after 9 years of follow-up (27). This further supported our findings and provided evidence from observational studies for the theory of the gut-muscle axis. It should be noted that our study excluded digestive system cancer from digestive diseases, because cachexia and sarcopenia are very common complications of cancer patients (28), which may introduce the potential bias. This study also found that the association between digestive diseases and sarcopenia was different in sex, age, residence, and marital status. This association only applied to males, older adults aged 60–79 years, rural residents, and married people. To begin with, it is found in males, rural residents, and married people that there were significant associations between digestive diseases and sarcopenia, which may be related to lower health services utilization. The previous national survey of older adults in China found that males, rural residents, and married people were less likely to use outpatient and inpatient services than females, urban residents, and the unmarried (29), which may make them unable to get timely treatment when they were ill, thus increasing the harm of digestive diseases to health. Secondly, the association between digestive diseases and sarcopenia was found only in participants aged 60–79 years, which may be due to the lower incidence of sarcopenia in middle-aged people aged 45–59 and the lower number of the oldest-old over 80 years old. In statistical analysis, a low incidence rate and sample size may lead to insufficient statistical power. However, since no significant interactions were found, the differences in these subgroup analyses may be due to a reduction in sample size after grouping. In the future, larger sample studies are needed to analyze the results of different subgroups.
The mechanism of association between digestive diseases and an increased risk of sarcopenia may involve an imbalance of gut microbiota, malnutrition, and long-term inflammatory condition. Firstly, most digestive diseases have changes in gut microbiota, which may play a role in the pathophysiological process of muscle mass decline. The gut microbiota of patients with chronic liver disease showed a change of decreasing abundance of Firmicutes (Ruminococcaceae and Lachnospiraceae), Prevotellaceae, and an increase of Enterobacteriaceae, Proteobacteria (30). The gut microbiota of patients with IBD showed a change of decreasing abundance of Firmicutes (Eubacterium, Christensenellaceae, and Faecalibacterium prausnitzii), and an increase of Actinomyces, Escherichia coli (31). Moreover, other digestive diseases including Helicobacter pylori infection were also associated with alterations in the gut microbiome (32, 33). Researchers analyzed the gut microbiome of subjects with sarcopenia or low skeletal muscle mass, and the results indicated that the abundance of Firmicutes (Eubacterium, Ruminococcaceae, Lachnospiraceae, F. prausnitzii) decreased (34, 35). These changes were consistent with the characteristics of gut microbes in patients with liver and gastrointestinal diseases to a certain extent. The microbes decreased in digestive diseases may produce some metabolites such as short-chain fatty acids (SCFAs), secondary bile acids (BAs), and some amino acids. They promoted skeletal muscle health by activating G protein-coupled receptors (GPR41/13/43) and inhibiting HDACs to further regulate the signal pathways related to insulin resistance, inflammatory response, and oxidative stress (36).
Secondly, patients with digestive diseases often face the risk of malnutrition. It was reported that 32.0–61.5% of patients with various digestive diseases suffer from malnutrition (17, 37, 38). Anorexia and abdominal discomfort are the main symptoms of patients with digestive diseases, which may lead to a decrease in their dietary intake and mean a lack of raw materials for muscle protein synthesis. In addition, various pathological changes associated with digestive diseases, such as digestive enzyme deficiency, decreased synthesis or secretion of conjugated BAs, reduced intestinal absorptive area, and dysbacteriosis can cause maldigestion and malabsorption, making nutrients unable to be used for skeletal muscle metabolism (39). In addition, the association between digestive diseases and sarcopenia may also be related to the reduction of nutrient absorption caused by taking medicine in patients with digestive diseases. Proton pump inhibitors (PPIs) have become the first choice for the treatment of acid-related digestive diseases, thus the use of PPI has been increasing in recent decades (40, 41). A large number of studies have found that the use of PPI was related to the reduced absorption of micronutrients such as vitamins C, D, and magnesium (42, 43). Meanwhile, more and more studies have shown that low micronutrient intake was associated with an increased risk of sarcopenia (44).
Thirdly, chronic low-grade inflammation is an important pathological mechanism for the development of sarcopenia. Gastritis, pancreatitis, chronic liver disease, inflammatory bowel disease, irritable bowel syndrome, and other digestive diseases infected were often accompanied by inflammation and caused elevated levels of proinflammatory cytokines such as tumor necrosis factor-alpha (TNF-α), interleukin 6 (IL-6), and myostatin (22, 45, 46). TNF-α, IL-6, and myostatin may activate the expression of the muscle-specific E3 ligases muscle RING-finger protein-1 (MuRF-1) and muscle atrophy F-Box (MAFbx) through regulating the p38 mitogen-activated protein kinase (MAPK) pathway and the nuclear factor-kappa B (NF-κB) pathway (47). MuRF-1 and MAFbx can further activate the ubiquitin proteasomal system (UPS) to promote protein degradation or proteolysis of skeletal muscle (47). The abnormal autophagy enhanced by phosphoinositide 3-kinase (PI3K)/protein kinase B (AKT)/mammalian target of rapamycin (mTOR) pathway was also associated with the process of muscle atrophy mediated by inflammation (48). These mechanisms provide a possible explanation for the relationship between digestive system diseases and sarcopenia. This also suggests that it is necessary to include intestinal flora or inflammatory factors in future research to explore whether these biomarkers can mediate the relationship between digestive diseases and sarcopenia.
It is worth noting that our study has several advantages. First of all, based on a nationally representative data, we explored the association between digestive diseases and sarcopenia using a prospective cohort study for the first time, which has good extrapolation and a higher level of evidence. Secondly, we controlled a set of covariates such as the social demographic characteristics, health conditions, and lifestyles to make the research results more stable. In particular, we have controlled the prevalence of chronic diseases, and the results showed that digestive diseases still significantly increased the risk of sarcopenia, which indicates that digestive diseases were significantly correlated with sarcopenia independently of other chronic diseases. In addition, we also conducted a subgroup analysis, which will help to find vulnerable groups more easily in the early prevention of sarcopenia in the future. Finally, we also conducted a sensitivity analysis, and the results suggested that the association between digestive diseases and sarcopenia was robust. The results of this study provide new ideas for early screening and prevention of sarcopenia in middle-aged and older people in community settings in the future. Community health workers can predict the incidence of sarcopenia 4 years later by asking middle-aged and older people if they have digestive diseases. Considering the availability of self-reported digestive diseases, this study has significant public health implications for reducing the burden of sarcopenia.
In addition, our study has some limitations. The cohort study cannot infer the causal relationship between digestive diseases and sarcopenia, which is our first limitation. In the future, causal inference methods are needed to enhance the causal effect of the above results. Second, we used self-reported digestive diseases instead of being diagnosed by doctors themselves, which may lead to evaluation bias. Although the survey has emphasized the need for participants to report diseases based on previous doctors’ diagnoses, it is undeniable that there may be bias. Due to the data limitations of CHARLS, previous studies (49, 50) have also used digestive diseases assessment methods consistent with this study, and have emphasized the limitations of self-reported bias and measurement bias. However, on the other side, given the scarcity of primary medical resources, if the risk of sarcopenia in middle-aged and older adults after 4 years can be determined based on self-reported digestive diseases, this may be of great value for early intervention and prevention of sarcopenia, as self-reported digestive diseases are very easy to obtain and do not require accurate medical equipment diagnosis. In addition, we have not collected subtypes of digestive diseases, such as gastritis, gastric ulcer, and inflammatory bowel disease. It is necessary to further explore the relationship between specific digestive diseases and sarcopenia in the future. Moreover, sarcopenia may be closely related to the diet of participants, however, since the CHARLS did not involve specific dietary assessments, we only included daily dietary frequency as a covariate, which may result in confounding bias. Finally, we excluded some missing data in the process of sample selection, which may introduce selection bias. However, due to the large number of samples included in our study, the impact of selection bias may be small.
Digestive diseases were associated with an increased risk of sarcopenia in middle-aged and older adults aged ≥45 years. Early intervention of digestive diseases may help to reduce the incidence of sarcopenia in middle-aged and older adults.
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found below: the data used in this study can be obtained from CHARLS official website (https://charls.pku.edu.cn/en/).
The studies involving human participants were reviewed and approved by the Ethics Committee of Peking University. The patients/participants provided their written informed consent to participate in this study.
GC, SL, and XZ: conceptualization. GC and SL: methodology, validation, and formal analysis. GC: software and writing—original draft preparation. HY, GC, SL, and XZ: writing—review and editing. XZ: supervision. YY, YF, YC, XJ, and ML: project administration. All authors had read and agreed to the published version of the manuscript.
The study was supported by the Qi-Huang Scholar Chief Scientist Program of National Administration of Traditional Chinese Medicine Leading Talents Support Program (2021).
The authors thank all the participants and investigators for the CHARLS.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnut.2023.1097860/full#supplementary-material
1. Cruz-Jentoft A, Bahat G, Bauer J, Boirie Y, Bruyère O, Cederholm T, et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. (2019) 48:16–31. doi: 10.1093/ageing/afy169
2. Petermann-Rocha F, Balntzi V, Gray S, Lara J, Ho F, Pell J, et al. Global prevalence of sarcopenia and severe sarcopenia: a systematic review and meta-analysis. J Cachexia Sarcopenia Muscle. (2022) 13:86–99. doi: 10.1002/jcsm.12783
3. Yeung S, Reijnierse E, Pham V, Trappenburg M, Lim W, Meskers C, et al. Sarcopenia and its association with falls and fractures in older adults: a systematic review and meta-analysis. J Cachexia Sarcopenia Muscle. (2019) 10:485–500.
4. Spexoto M, Ramírez P, de Oliveira Máximo R, Steptoe A, de Oliveira C, Alexandre T. European Working Group on Sarcopenia in Older People 2010 (EWGSOP1) and 2019 (EWGSOP2) criteria or slowness: which is the best predictor of mortality risk in older adults? Age Ageing. (2022) 51:afac164.
5. Norman K, Otten L. Financial impact of sarcopenia or low muscle mass – A short review. Clin Nutr. (2019) 38:1489–95. doi: 10.1016/j.clnu.2018.09.026
6. Bruyère O, Beaudart C, Ethgen O, Reginster J, Locquet M. The health economics burden of sarcopenia: a systematic review. Maturitas. (2019) 119:61–9. doi: 10.1016/j.maturitas.2018.11.003
7. Gao Q, Hu K, Yan C, Zhao B, Mei F, Chen F, et al. Associated factors of sarcopenia in community-dwelling older adults: a systematic review and meta-analysis. Nutrients. (2021) 13:4291. doi: 10.3390/nu13124291
8. Santiago E, Roriz A, Ramos L, Ferreira A, Oliveira C, Gomes-Neto M. Comparison of calorie and nutrient intake among elderly with and without sarcopenia: a systematic review and meta-analysis. Nutr Rev. (2021) 79:1338–52. doi: 10.1093/nutrit/nuaa145
9. Cruz-Jentoft A, Sayer A. Sarcopenia. Lancet. (2019) 393:2636–46. doi: 10.1016/S0140-6736(19)31138-9
10. Lena A, Hadzibegovic S, von Haehling S, Springer J, Coats A, Anker M. Sarcopenia and cachexia in chronic diseases: from mechanisms to treatment. Polish Arch Inter Med. (2021) 131:16135. doi: 10.20452/pamw.16135
11. Wu P, Huang K, Chen K, Chou C, Tu Y. Exercise, nutrition, and combined exercise and nutrition in older adults with sarcopenia: a systematic review and network meta-analysis. Maturitas. (2021) 145:38–48.
12. Cruz-Jentoft A, Landi F, Schneider S, Zúñiga C, Arai H, Boirie Y, et al. Prevalence of and interventions for sarcopenia in ageing adults: a systematic review. Report of the International Sarcopenia Initiative (EWGSOP and IWGS). Age Ageing. (2014) 43:748–59. doi: 10.1093/ageing/afu115
13. Gielen E, Beckwée D, Delaere A, De Breucker S, Vandewoude M, Bautmans I. Nutritional interventions to improve muscle mass, muscle strength, and physical performance in older people: an umbrella review of systematic reviews and meta-analyses. Nutr Rev. (2021) 7:121–47. doi: 10.1093/nutrit/nuaa011
14. Onishi S, Shiraki M, Nishimura K, Hanai T, Moriwaki H, Shimizu M. Prevalence of sarcopenia and its relationship with nutritional state and quality of life in patients with digestive diseases. J Nutr Sci Vitaminol. (2018) 64:445–53.
15. Limketkai B, LeBrett W, Lin L, Shah N. Nutritional approaches for gastroparesis. Lancet Gastroenterol Hepatol. (2020) 5:1017–26.
16. Liu J, Ge X, Ouyang C, Wang D, Zhang X, Liang J, et al. Prevalence of malnutrition, its risk factors, and the use of nutrition support in patients with inflammatory bowel disease. Inflamm Bowel Dis. (2022) 28(Suppl. 2):S59–66. doi: 10.1093/ibd/izab345
17. Rivelsrud M, Paur I, Sygnestveit K, Nilsen R, Tangvik R. Nutritional treatment is associated with longer survival in patients with pancreatic disease and concomitant risk of malnutrition. Clin Nutr. (2021) 40:2128–37. doi: 10.1016/j.clnu.2020.09.037
18. Bunchorntavakul C, Reddy K. Review article: malnutrition/sarcopenia and frailty in patients with cirrhosis. Aliment Pharmacol Ther. (2020) 51:64–77. doi: 10.1111/apt.15571
19. Bauer K, Littlejohn P, Ayala V, Creus-Cuadros A, Finlay B. Nonalcoholic fatty liver disease and the gut-liver axis: exploring an undernutrition perspective. Gastroenterology. (2022) 162:58. doi: 10.1053/j.gastro.2022.01.058
20. Beaudart C, Sanchez-Rodriguez D, Locquet M, Reginster J, Lengelé L, Bruyère O. Malnutrition as a strong predictor of the onset of sarcopenia. Nutrients. (2019) 11:2883. doi: 10.3390/nu11122883
21. Ticinesi A, Lauretani F, Milani C, Nouvenne A, Tana C, Del Rio D, et al. Aging gut microbiota at the cross-road between nutrition, physical frailty, and sarcopenia: is there a gut-muscle axis? Nutrients. (2017) 9:1303. doi: 10.3390/nu9121303
22. Ehlers L, Bannert K, Rohde S, Berlin P, Reiner J, Wiese M, et al. Preclinical insights into the gut-skeletal muscle axis in chronic gastrointestinal diseases. J Cell Mol Med. (2020) 24:8304–14. doi: 10.1111/jcmm.15554
23. Zhao Y, Hu Y, Smith J, Strauss J, Yang G. Cohort profile: the China Health and Retirement Longitudinal Study (CHARLS). Int J Epidemiol. (2014) 43:61–8. doi: 10.1093/ije/dys203
24. Chen L, Woo J, Assantachai P, Auyeung T, Chou M, Iijima K, et al. Asian working group for sarcopenia: 2019 consensus update on sarcopenia diagnosis and treatment. J Am Med Directors Assoc. (2020) 21:300–7.e2. doi: 10.1016/j.jamda.2019.12.012
25. Wen X, Wang M, Jiang C, Zhang Y. Anthropometric equation for estimation of appendicular skeletal muscle mass in Chinese adults. Asia Pac J Clin Nutr. (2011) 20:551–6.
26. Wu X, Li X, Xu M, Zhang Z, He L, Li Y. Sarcopenia prevalence and associated factors among older Chinese population: findings from the China Health and Retirement Longitudinal Study. PLoS One. (2021) 16:e0247617. doi: 10.1371/journal.pone.0247617
27. Hurst C, Murray J, Granic A, Hillman S, Cooper R, Sayer A, et al. Long-term conditions, multimorbidity, lifestyle factors and change in grip strength over 9 years of follow-up: Findings from 44,315 UK biobank participants. Age Ageing. (2021) 50:2222–9. doi: 10.1093/ageing/afab195
28. von Haehling S, Anker M, Anker S. Prevalence and clinical impact of cachexia in chronic illness in Europe, USA, and Japan: facts and numbers update 2016. J Cachexia Sarcopenia Muscle. (2016) 7:507–9. doi: 10.1002/jcsm.12167
29. Zeng Y, Wan Y, Yuan Z, Fang Y. Healthcare-seeking behavior among chinese older adults: patterns and predictive factors. Int J Environ Res Public Health. (2021) 18:2969. doi: 10.3390/ijerph18062969
30. Albillos A, de Gottardi A, Rescigno M. The gut-liver axis in liver disease: Pathophysiological basis for therapy. J Hepatol. (2020) 72:558–77. doi: 10.1016/j.jhep.2019.10.003
31. Pittayanon R, Lau J, Leontiadis G, Tse F, Yuan Y, Surette M, et al. Differences in gut microbiota in patients with vs. without inflammatory bowel diseases: a systematic review. Gastroenterology. (2020) 158:294. doi: 10.1053/j.gastro.2019.11.294
32. Chen C, Liou J, Lee Y, Hong T, El-Omar E, Wu M. The interplay between and gastrointestinal microbiota. Gut Microbes. (2021) 13:1–22. doi: 10.1080/19490976.2021.1909459
33. Ticinesi A, Lauretani F, Tana C, Nouvenne A, Ridolo E, Meschi T. Exercise and immune system as modulators of intestinal microbiome: implications for the gut-muscle axis hypothesis. Exerc Immunol Rev. (2019) 25:84–95.
34. Han D, Wu W, Liu P, Yang Y, Hsu H, Kuo C, et al. Differences in the gut microbiome and reduced fecal butyrate in elders with low skeletal muscle mass. Clin Nutr. (2022) 41:1491–500. doi: 10.1016/j.clnu.2022.05.008
35. Kang L, Li P, Wang D, Wang T, Hao D, Qu X. Alterations in intestinal microbiota diversity, composition, and function in patients with sarcopenia. Sci Rep. (2021) 11:4628. doi: 10.1038/s41598-021-84031-0
36. Giron M, Thomas M, Dardevet D, Chassard C, Savary-Auzeloux I. Gut microbes and muscle function: can probiotics make our muscles stronger? J Cachexia Sarcopenia Muscle. (2022) 13:1460–76. doi: 10.1002/jcsm.12964
37. Knudsen A, Naver A, Bisgaard K, Nordgaard-Lassen I, Becker U, Krag A, et al. Nutrition impact symptoms, handgrip strength and nutritional risk in hospitalized patients with gastroenterological and liver diseases. Scand J Gastroenterol. (2015) 50:1191–8. doi: 10.3109/00365521.2015.1028994
38. Lindqvist C, Slinde F, Majeed A, Bottai M, Wahlin S. Nutrition impact symptoms are related to malnutrition and quality of life – A cross-sectional study of patients with chronic liver disease. Clin Nutr. (2020) 39:1840–8. doi: 10.1016/j.clnu.2019.07.024
39. Montoro-Huguet M, Belloc B, Domínguez-Cajal M. Small and large intestine (i): malabsorption of nutrients. Nutrients. (2021) 13:1254. doi: 10.3390/nu13041254
40. Savarino E, Marabotto E, Zentilin P, Furnari M, Bodini G, Pellegatta G, et al. A safety review of proton pump inhibitors to treat acid-related digestive diseases. Expert Opin Drug Safety. (2018) 17:785–94. doi: 10.1080/14740338.2018.1497155
41. Savarino V, Marabotto E, Zentilin P, Furnari M, Bodini G, De Maria C, et al. The appropriate use of proton-pump inhibitors. Minerva Med. (2018) 109:386–99. doi: 10.23736/s0026-4806.18.05705-1
42. Gommers L, Hoenderop J, de Baaij J. Mechanisms of proton pump inhibitor-induced hypomagnesemia. Acta Physiol. (2022) 235:e13846. doi: 10.1111/apha.13846
43. Vinke P, Wesselink E, van Orten-Luiten W, van Norren K. The use of proton pump inhibitors may increase symptoms of muscle function loss in patients with chronic illnesses. Int J Mol Sci. (2020) 21:10323. doi: 10.3390/ijms21010323
44. Robinson S, Granic A, Sayer A. Micronutrients and sarcopenia: current perspectives. Proc Nutr Soc. (2021) 80:311–8. doi: 10.1017/s0029665121001956
45. Nardone O, de Sire R, Petito V, Testa A, Villani G, Scaldaferri F, et al. Inflammatory bowel diseases and sarcopenia: the role of inflammation and gut microbiota in the development of muscle failure. Front Immunol. (2021) 12:694217. doi: 10.3389/fimmu.2021.694217
46. Yang Y, Kim D. An overview of the molecular mechanisms contributing to musculoskeletal disorders in chronic liver disease: osteoporosis, sarcopenia, and osteoporotic sarcopenia. Int J Mol Sci. (2021) 22:2604. doi: 10.3390/ijms22052604
47. Wiedmer P, Jung T, Castro J, Pomatto L, Sun P, Davies K, et al. Sarcopenia – Molecular mechanisms and open questions. Ageing Res Rev. (2021) 65:101200. doi: 10.1016/j.arr.2020.101200
48. Liu J, Dong S, Shen H, Yang D, Chen B, Ma X, et al. Multi-omics research in sarcopenia: Current progress and future prospects. Ageing Res Rev. (2022) 76:101576. doi: 10.1016/j.arr.2022.101576
49. Zhang H, Xia Y, Chang Q, Zhang X, Zhao Y. Association between water source and chronic gastrointestinal diseases in Chinese: A cross-sectional and longitudinal study. Front Public Health. (2022) 10:992462. doi: 10.3389/fpubh.2022.992462
Keywords: digestive diseases, sarcopenia, middle-aged and older adults, China, CHARLS
Citation: Cui G, Li S, Ye H, Yang Y, Chu Y, Jia X, Feng Y, Lin M and Zhang X (2023) Association between digestive diseases and sarcopenia among Chinese middle-aged and older adults: a prospective cohort study based on nationally representative survey. Front. Nutr. 10:1097860. doi: 10.3389/fnut.2023.1097860
Received: 05 December 2022; Accepted: 20 June 2023;
Published: 05 July 2023.
Edited by:
Caterina Conte, Università Telematica San Raffaele Roma, ItalyReviewed by:
Irma Ruslina Defi, Padjadjaran University, IndonesiaCopyright © 2023 Cui, Li, Ye, Yang, Chu, Jia, Feng, Lin and Zhang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xuezhi Zhang, emhhbmcueHVlemhpQDI2My5uZXQ=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.