 Noha M. Almoraie*
Noha M. Almoraie* Israa M. Shatwan
Israa M. Shatwan Maha A. Althaiban
Maha A. Althaiban Mahitab A. Hanbazaza
Mahitab A. Hanbazaza Huda A. WazzanNajlaa M. Aljefree
Huda A. WazzanNajlaa M. Aljefree- Department of Food and Nutrition, Faculty of Human Sciences and Design, King Abdulaziz University, Jeddah, Saudi Arabia
Objective: We aimed to assess the dietary intake of certain food groups in a representative sample of public-school teachers living in Jeddah city. We also, examined the association of dietary intake with physical activity and obesity among schoolteachers.
Methods: The study was a cross-sectional online survey, conducted among 640 (177 male, 463 female) schoolteachers aged between 20 and 62 years old and working in public primary, intermediate, and high schools in Jeddah. Measurements included gender, weight, height, body mass index (BMI), health problems, and lifestyle behaviours, including physical activity levels, smoking status, and dietary intake.
Results: Based on gender, number of non-smoking women (94%) was higher than number of non-smoking men (57.1%) (P < 0.001). However, men were more active than women (P = 0.03). Regarding BMI, there were more overweight men than women, while obese women numbered more than men (P = 0.003). There was no significant difference in dietary intake between men and women except that men consumed more soft drinks than women (P = 0.002). Lower physically active schoolteachers were less likely to consume salad (OR = 0.6, 95% CI 0.4–0.9; P = 0.02), vegetables (OR = 0.6, 95% CI 0.3–0.9; P = 0.01), beans and legumes (OR = 0.4, 95% CI 0.2–0.7; P = 0.005), wholegrain bread (OR = 0.6, 95% CI 0.4–0.9; P = 0.03), dairy products (OR = 0.6, 95% CI 0.4–0.9; P = 0.01), snacks (OR = 0.5, 95% CI 0.2–0.8; P = 0.01), and fish (OR = 0.4, 95% CI 0.2–0.9; P = 0.04) compared to those with high levels of physical activity. Only fruit intake was considered statistically significant (OR = 0.4, 95% CI 0.3–0.7; P = 0.003). The study found a relationship between the BMI of schoolteachers and food intake. Obese schoolteachers had lower consumption of fruits (OR = 0.3, 95% CI 0.2–0.7; P = 0.007) and white meat (OR = 0.5, 95%CI 0.3–0.9; P = 0.03) than schoolteachers in the normal weight group.
Conclusion: The high prevalence of physical activity, dietary intake and body weight among Saudi teachers is a major public health concern. The present study identified several lifestyle factors associated with body weight that may represent valid targets for the prevention and management of obesity among Saudi school teachers. Promoting active lifestyles and healthy diets would be primary targets for obesity prevention.
1. Introduction
Obesity and overweight are major public health problems that are considered a global pandemic (1) due to disease and biological risk factors linked to non-communicable diseases. The World Health Organization (WHO) defines obesity and overweight as abnormal or excessive accumulation of fat and classifies it according to a body mass index (BMI) of higher than 25 and 30 kg/m2, for overweight and obesity, respectively (2). The prevalence of adult obesity has increased threefold globally in the last four decades (3), according to WHO. There is a growth in obesity rates around the world (>1 billion). In Europe, two thirds of the adult's population is obese (3), whereas, in Saudi Arabia, more than half the adults are considered obese, which is also the case in Arabian gulf countries (4). Obesity and overweight causes are complicated by environmental, genetic, behavioural, and socioeconomic factors. It is well-known that dietary intake and physical activity are risk factors linked with obesity and overweight (5). In Saudi Arabia, obesity and overweight increased due to shifting lifestyles as a result of the growth of the economy, technology, food availability, variety, and changes in the population's living standards. This led to changes in food choice, energy intake and energy expenditure. A high snack frequency (unhealthy crisps, sweets, and carbonated beverages), skipping daily breakfast, and emotional eating are harmful dietary habits significantly associated with a higher BMI that were found in the Saudi population (6). In addition, some Saudis are physically inactive because of the weather, culture, and lack of time and equipment (7). Sedentary lifestyles in the Saudi population as a result of sedentary jobs, long car trips, and watching screens (computer, mobile, television and games) for more than 8 hours per day contribute to the physical inactivity of Saudi adults (7).
Schoolteachers have specific environmental and psychological challenges that require ideal health conditions to meet their job requirements (8). Studies have reported that schoolteachers might not have a healthy dietary intake due to skipping breakfast, eating inadequate breakfast, and consuming foods high in fat and sugar or calorically dense snacks, which is not supported by dietary recommendations (9–11). This dietary behaviour among schoolteachers is more likely to lead to concentration problems and increase the risk of obesity (9). The change in socio-cultural and lifestyle for the Saudi population increase adults' consumption of unhealthy fast foods. The majority of schoolteachers in Saudi Arabia skip breakfast at home, especially females (74%); further, over 76% and 85% of males and females eat breakfast and/or snacks at school (5). A US study (12) found that the most frequently consumed foods by schoolteachers was candy (70%) and 33% of them provided it as a reward for students weekly. However, the consumption of cookies, doughnuts, sweetened drinks, and pizza was at 25%.
Additionally, most schoolteachers are moderately physically active (13–15), irrespective of their role in the classroom, and schoolteachers during teaching (14, 16). Among individuals, including schoolteachers, the obesity risk increases with the degree of physical inactivity, sedentary life, and dietary behaviour (17). The prevalence of obesity among schoolteachers was 30% in a Brazilian study (18) and 40% in a Saudi study in Jeddah (19). Obesity is associated with lifestyle and comorbidities among public school teachers (20). The higher obesity prevalence among schoolteachers may be related to high levels of sedentary behaviour during leisure (20) and the association of prolonged screen time, sedentary behaviour, and unhealthy eating habits (15). In addition, sitting time and watching screen devices are associated with consuming products of high energy density and low nutritional content. Globally, one in four adults is physically inactive (21), compared to one in two in Saudi Arabia (22) and one-third in South Africa (23). A Brazilian study (24) found that more than 50% schoolteachers are physically inactive, and this is as result of low levels of physical activity, high levels of TV viewing and low energy expenditure. Generally, schoolteachers sit in an orthostatic position at school 95% of the time. Furthermore, previous scientific evidence indicated health impact of increased percentages of obesity among different populations including increase rates of associated chronic diseases such as cardiovascular disease, diabetes, hypertension (25), and cancer (26). Also, studies showed other undesirable health impact for obesity including the presence of psychological disorders (27, 28), body dissatisfaction (29). Moreover, the health of schoolteachers affects teaching quality. This may indirectly affect student achievement and students' subsequent success in society due to the role of a teacher in students' lives, especially at this critical age (30). Previous literature illustrated that schoolteachers have been affected by chronic diseases globally. For example, the rates of hypertension were reported by 25%, 29% and 84% among Saudi, Indian, and Nigerian schoolteachers, respectively (31–33).
As schoolteachers are considered role models for students, the dietary intake and physical activity of schoolteachers may influence their students' behaviours. Also, teachers spend ~7 h a day, 5 days per week at schools, working with students, which allows students to copy teachers' food choices during breakfast and snack times. Therefore, schoolteachers should be positive role models for students by setting an example of healthy dietary intake and healthy lifestyle habits (34, 35). Dietary intake, physical activity levels, and obesity are important indicators of health status among schoolteachers, which may affect their work performance. Hence, the current study hypothesises that public schoolteachers who are physically active and have a normal BMI have a healthy dietary intake. To the best of our knowledge, the association between physical activity, obesity status, and dietary intake has not been examined among schoolteachers in Saudi Arabia. Additionally, previous studies regarding school nutrition and health interventions focused considerably on students, not teachers. Therefore, this study aimed to fill this gap and assess the dietary intake of certain food groups in a representative sample of public-school teachers living in Jeddah city. We further examined the association of dietary intake with physical activity and obesity among schoolteachers. The finding of this study will enhance future health interventions in schools and lead policymakers in Saudi Arabia and beyond.
2. Methods
2.1. Study design and participants
This cross-sectional study was conducted between October 2021 and March 2022 on teachers working in public schools in Jeddah, Saudi Arabia. This study was first approved by the Biomedical Ethics Research Committee of King Abdulaziz University (Reference No. 159-21). In order to collect data from schoolteachers in Jeddah city, approvals were also sought from the Education Department of Jeddah.
The inclusion criteria were male and female teachers, aged between 18 and 65 years old, working in public primary, intermediate, and high schools in Jeddah city. This study excluded teachers working in private schools. There are six administrative educational offices for public schools in Jeddah: North, East, Centre, Naseem, South, and Safa. According to the Ministry of Education statistics, the total number of male and female teachers working at public schools in Jeddah was as follows: in primary, intermediate, and high schools there were 6,046, 3,777, and 2,189 male teachers and 7,304, 4,323, and 3,219 female teachers, respectively (36). Hence, according to the online sample size calculator (37), the required sample size for the current study was 638 schoolteachers working in public schools in Jeddah.
2.2. Measures
An online self-reported survey was distributed electronically via par code and WhatsApp, e-mail to several educational offices and, in return, to all public schools in their area during the school year. A closed-ended multiple-choice questionnaire was used to collect and assess data in four categories: sociodemographic characteristics, health characteristics, health behaviours, and dietary intake. The online self-reported survey was used because it allowed the collection of data from a large and representative sample in a short time. At the beginning of the online survey, schoolteachers were informed about the research objectives and procedures, and their anonymity and voluntary participation in this research were guaranteed. Since the survey was distributed online, consent was obtained by adding a consent statement, respondents provided consent through this to participate in the research. Thus, only those who agreed to participate were able to complete the survey.
2.2.1. Sociodemographic characteristics
Sociodemographic characteristics of schoolteachers included age (18–65), sex (male; female), marital status (single, married, divorced, widowed), education level (diploma; bachelor; postgraduate), school stage (primary; secondary; high), and years of teaching experience (1–5; 6–10; 11–15;16–20; and above 20 years).
2.2.2. Health characteristics
Self-reported health characteristics, including the presence of chronic disorders (e.g., diabetes, hypertension, coronary heart disease, high cholesterol levels) and self-reported height and weight, were collected to determine body mass index (BMI). BMI in kg/m2 was categorised as normal weight (BMI between 18.5 and 24.99), overweight (BMI ≥ 25.0), or obese (BMI ≥ 30.0). BMI was classified according to the cut-off points of the World Health Organization (WHO) (38).
2.2.3. Health behaviours
Questions were related to participants' health behaviours, including physical activity, cigarette smoking, and dietary intake. For physical activity, questions were adapted from previous study conducted in Saudi Arabia (39). Participants were asked to self-report their physical activity, such as walking, running, or swimming, with the responses being classified as never, rarely, 1–2 per week, 3–4 per week, and more than 5 per week. In the analysis, we categorised them into two groups: low (participants who exercised two times per week or less) and high (participants who exercised more than three times per week) physical activity (39). Smoking was assessed by asking the participants about their cigarette smoking habits during the previous year. The responses were categorised as smoker, ex-smoker, and non-smoker.
2.2.4. Dietary intake
A short, non-quantitative, validated Food Frequency Questionnaire (FFQ) was used to assess the weekly frequency (days/week) of dietary intake for 14 food items, including fruits, fruit juices, salads, vegetables, dairy products, beans and legumes, cereals, wholegrain bread, snacks, sweets, soft drinks, white and red meat, and fish. The validated questionnaire was adopted from Cleghorn et al. (40). Each FFQ item had seven frequency options including (never, once a week, 2 to 4 times per week, 5 to 6 times per week, 1 to 2 times per day, 3 to 4 time per day, or 5 or more times per day). The participants were asked on average how often they consumed these 14 food items during the past 12 months. Based on participants responses, consumption was categorised as “low intake” or “high intake”. A consumption frequency of at least 5 days/week was defined as high intake, whereas low intake was defined as <5 days/week. These categories were based on a study done by Delfino et al. (15).
2.3. Statistical analysis
All of the data presented in the current study were categorical variables. Descriptive data of the study participants are shown in tables as frequencies (n) and percentages (%). Correlations between categorical variables (demographic characteristics, gender, and dietary intake) were examined using the chi-square test. Logistic regression analyses were performed to obtain odds ratios (ORs) and 95% CIs of dietary intake by physical activity levels and BMI status. All models were adjusted for a selected set of covariates, including sex, age, marital status, education level, years of experience, health status, and smoking status. In the analysis model, physical activity and BMI status were considered the explanatory variables, while the dietary intake was considered the outcome variables. For all analyses, the P < 0.05 was considered borderline significant. However, due to multiple testing of 14 food groups, we applied Bonferroni correction, and the statistical significance level was set at P = 0.003. Statistical analyses were performed using SPSS software version 28.0.
3. Results
The demographic characteristics of public-school teachers from Jeddah, Saudi Arabia, based on gender are shown in Table 1. The sample consisted of 640 schoolteachers; 72.3% were female, and 27.7% were male. Among the study participants, 74.1% were married, and 68.2% were aged between 35 and 54 years old. The majority of the study participants (83.6%) held a bachelor's degree. There were significant differences between male and female teacher in marital status and education level. In comparison to men, the percentage of widowed, single, and divorced women teachers was higher than that of men (P = 0.03). A higher percentage of women teachers held diplomas, while a higher percentage of men held postgraduate degree (P < 0.001). Most of the participants (40.9%) taught in high schools, and 36.6% had more than 20 years of teaching experience. Approximately 36.6% of the schoolteachers included in this study were healthy, 13.4% were diagnosed with diabetes, and 10.2% were diagnosed with hypertension. The mean BMI was 27.2 kg/m2 (SD = 4.9), and 34.4% of the participants were in the normal weight range, whereas 40.8% and 24.5% of the participants were overweight and obese, respectively. There were more overweight men teachers than women teachers, while there were more obese women teachers than men teachers (P = 0.003). In general, the percentage of non-smokers was 83.8%. There were more non-smoker women teachers (94%) than non-smoker men teachers (57.1%) (P < 0.001). A total of 53.6% of the participants were classified as highly physically active. Men teachers were more active than women teachers (P = 0.03). Table 2 presented dietary intake according to gender. There was no significant difference in dietary intake between men teachers and women teachers except that men teachers consume more soft drinks than women teachers (P = 0.002).
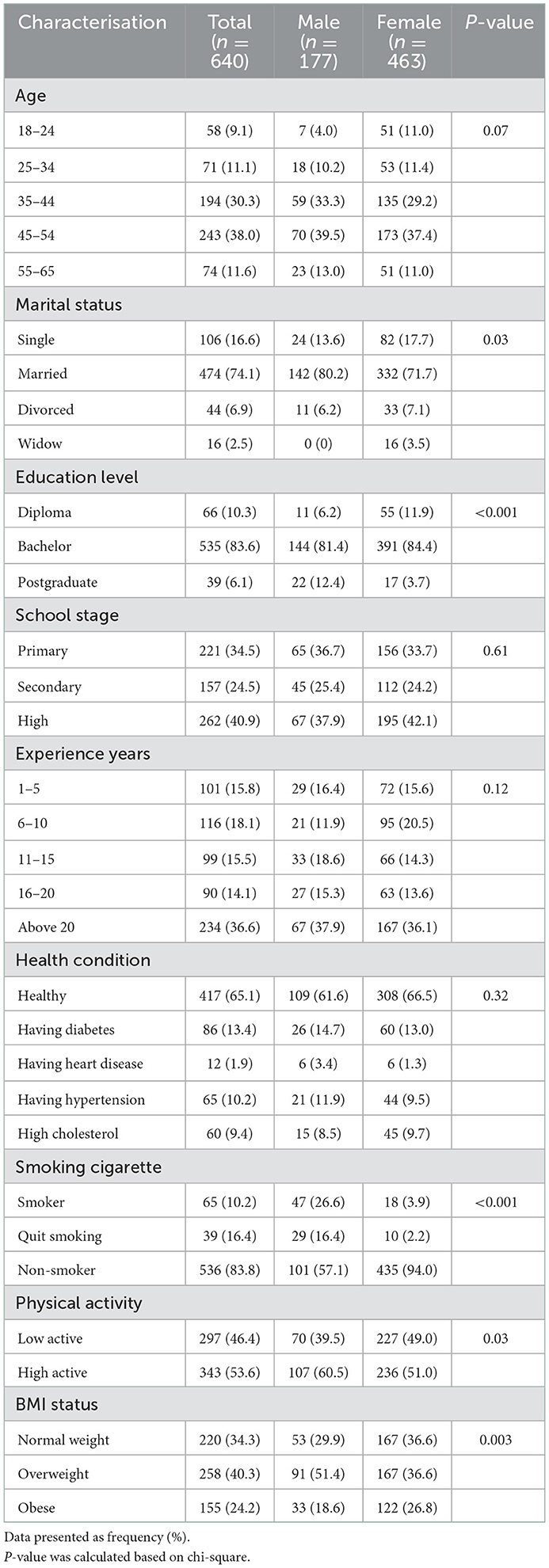
Table 1. Baseline characterisation of schoolteachers from public school stratified by gender.
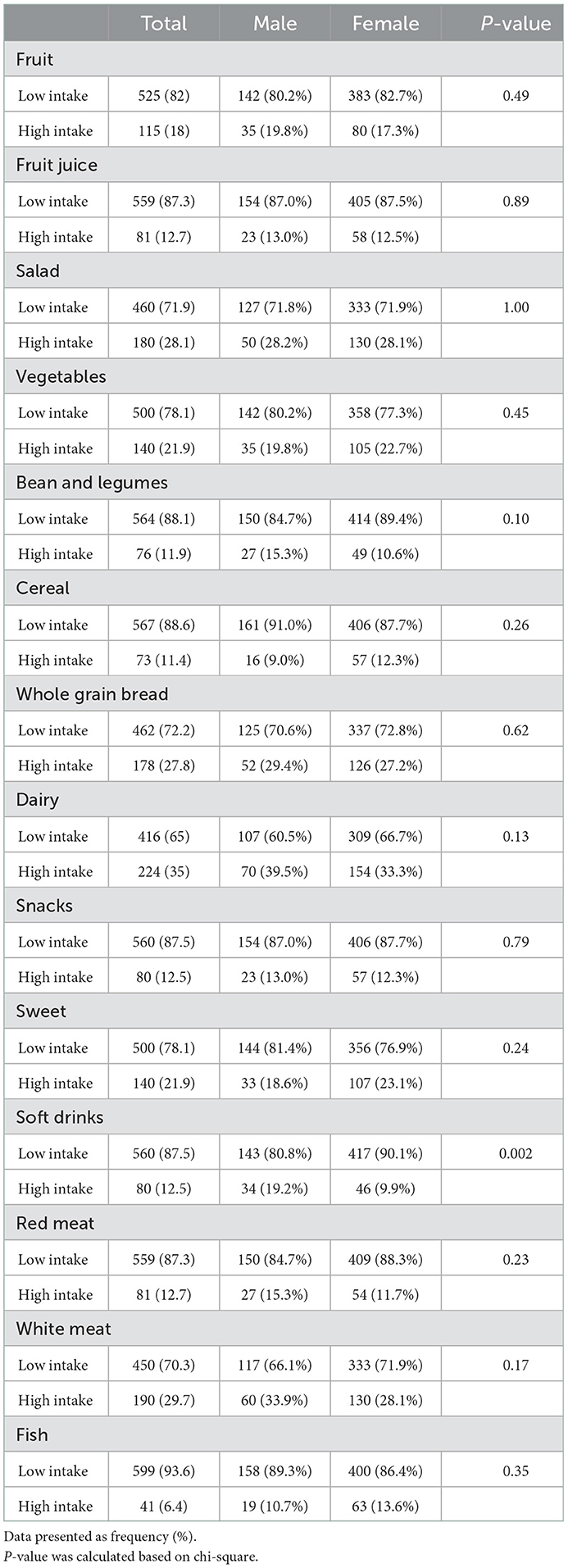
Table 2. Dietary intake based on gender of public schoolteachers.
The association between physical activity levels and dietary intake is shown in Table 3. Schoolteachers with low levels of physical activity exhibited a decreased consumption of salad (OR = 0.6, 95% CI 0.4–0.9; P = 0.02), vegetables (OR = 0.6, 95% CI 0.3–0.9; P = 0.01), beans and legumes (OR = 0.4, 95% CI 0.2–0.7; P = 0.005), wholegrain bread (OR = 0.6, 95% CI 0.4–0.9; P = 0.03), dairy products (OR = 0.6, 95% CI 0.4–0.9; P = 0.01), snacks (OR = 0.5, 95% CI 0.2–0.8; P = 0.01), and fish (OR = 0.4, 95% CI 0.2–0.9; P = 0.04) compared to those with high levels of physical activity. However, the difference was borderline significant. Only fruit intake was considered statistically significant (OR = 0.4, 95% CI 0.3–0.7; P = 0.003). The associations between BMI and dietary intake are shown in Table 4. Obese schoolteachers had a decreased consumption of fruits (OR = 0.3, 95% CI 0.2–0.7; P = 0.007) and white meat (OR = 0.5, 95% CI 0.3–0.9; P = 0.03) than schoolteachers in the normal weight group. Among the enrolled schoolteachers, the risk of being obese was associated with a decreased intake of vegetables (OR = 0.5, 95% CI 0.3–0.9; P = 0.05) compared to the group with normal body weight, but this did not reach statistical significance. However, the difference was borderline significant, and none of these associations were statistically significant.
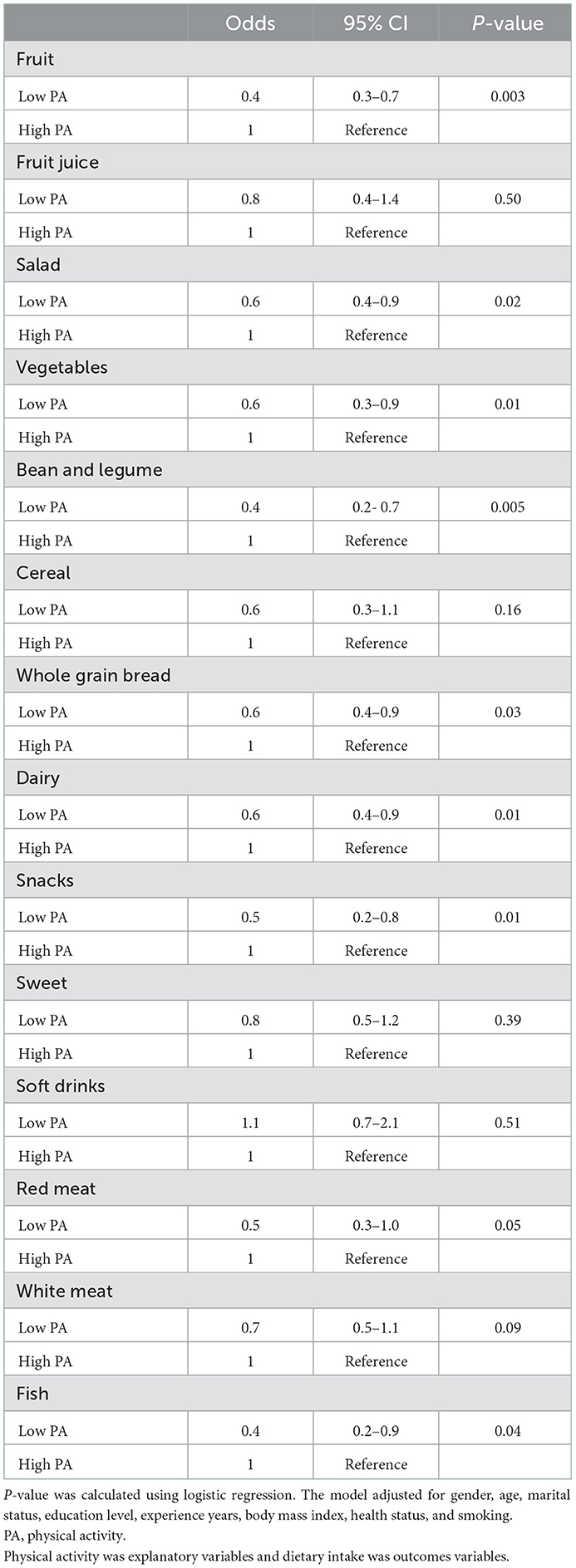
Table 3. Odds ratios and 95% CIs of food group intake according to physical activity levels of public schoolteachers.
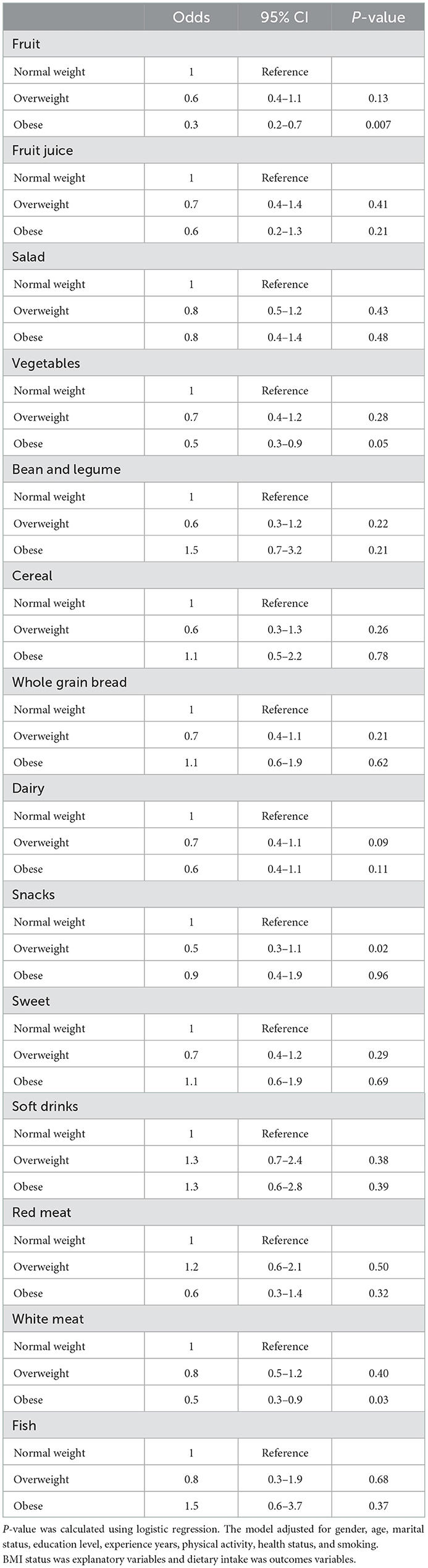
Table 4. Odds ratios and 95% CIs of food group intake according to body mass index categories of public schoolteachers.
4. Discussion
To prevent and control the rise of obesity prevalence and its complications, it is fundamental to establish healthy eating habits in the early development of a child (41). Consequently, the most effective way to promote health in the education system is through schoolteachers who can encourage healthy eating (41). Studies show that being proactive can improve health outcomes and promote healthy lifestyles (42, 43). In addition, the essential aspects of implementing health promotion in schools have been achieved with the aid of teachers' interest and engagement (43, 44). Thus, this study aimed assess the dietary intake of certain food groups in a representative sample of public-school teachers living in Jeddah city. Also, it aimed to examine the association of dietary intake with physical activity and obesity among schoolteachers. The main study findings regarding health behaviours of Saudi public-school teachers showed that the prevalence of overweight and obesity was 65%, the percentage of non-smokers was 84%, and 54% of the study participants met the definition of high physical activity. Our data show that physically active teachers consume more fruits, vegetables, beans, legumes, and dairy products than teachers who are less physically active. Less red meat and fewer snacks were consumed by teachers who were less physically active than by those who were more active. Compared to teachers with normal weight, those with a high BMI consumed fewer fruits, vegetables, snacks, and white meat. Hence, the main hypothesis was confirmed. To the best of our knowledge, no previous studies have examined the association of dietary intake with physical activity and obesity among schoolteachers in Saudi Arabia.
In this study, the obesity prevalence of schoolteachers was twice as high as the global obesity prevalence of adults (24.5 vs. 13.0%), and further analysis of the determinants is needed to investigate this alarming finding. This increased obesity frequency is consistent with earlier findings by Lizana et al. (45) reporting an obesity frequency of 25.7% among 70 rural Chilean teachers. Other studies among different populations, including 305 Tanzanian health workers, teachers, and bankers reported an even higher obesity prevalence (37.8%) with the prevalence of overweight and obesity among teachers reported by 62.6% in Tanzanian (46), which was similar to the results of the current study (65% when considering both overweight and obesity). It should be emphasised that the age of the current study population may have contributed to the increased obesity prevalence, as obesity increases progressively with age, reaching its peak in age groups from 40 to 60 years (47); these age groups were predominant in our study population. The risk of developing a several non-communicable diseases, including obesity, cardiovascular diseases, diabetes and hypertension increases with age (48). The results of the current study also revealed that the number of overweight men teachers was higher than that of women teachers, while that of obese women teachers was higher than that of men teachers (P = 0.003). However, the reason for such a difference may be the hormonal differences between men and women, genetic factors, and variations in clinical severity are also thought to play a role in the interaction influence of sex in the correlations with obesity (48). Previous studies conducted in Saudi Arabia reported similar results as men had higher levels of overweight and women had higher levels of obesity (49).
The present study demonstrated that the level of physical activity in Saudi Arabia has increased, although it is still relatively low. According to the Saudi STEPwise survey, the prevalence of moderate and high levels of physical activity among Saudis aged 15–64 years was 32.3% (50). The level of physical activity reported in this study was 54%. Despite not being comparable to our study in methodology or national representativeness, other studies among Saudi adults aged 15 and older have reported increases in physical activity, ranging from 50 to 70%.(7, 51). According to the WHO, around 30% of the world's population and 30–70% of those living in countries in the eastern Mediterranean region do not meet the recommended minimum level of physical activity (52). In the present study, women teachers were found to be less physically active than men teachers. A possible explanation for this might be that men in Saudi Arabia generally have more opportunities than women to engage in outdoor physical activity especially considering the hot weather in the kingdom, which may affect women who wear hijab to exercise (49). However, there are plenty of health clubs for both sexes; nevertheless, the high cost for health clubs might be an issue that impact practising physical activity (49). It is notable that women in the Middle East have generally been reported to be less physically active than men (53, 54), and lower than that in many developed countries (53).
The current study findings indicated that the consumption of food from various categories was considered poor, as only a small percentage of schoolteachers' food intake met the dietary recommendations. These results were consistent with the findings of a nationally representative survey on the Saudi adult population that revealed that the consumption of fruits, vegetables, beans, legumes, dairy products, and fish did not meet the dietary recommendations (55). Unhealthy eating habits are the leading risk factor for poor health, with an estimated 11.3 million attributed deaths and 241.4 million attributed disability-adjusted life years per annum globally (56). In line with our findings, the Global Burden of Diseases, Injuries, and Risk Factors study reported that in Saudi Arabia, the average intake of fruits, vegetables, nuts, whole grains, and seafood (polyunsaturated and omega 3) fatty acids was considerably below optimal levels, whereas the consumption of red meat, processed meats, saturated fatty acids, sugar-sweetened beverages, and salt was significantly above optimal levels (57). Interventions to enhance teacher eating habits are necessary because they may positively impact both teachers' and students' health-related behaviours. This is because healthier diets are strongly associated with a lower risk of developing chronic diseases (58). This study also reported that the teachers' dietary intake did not differ by gender except that men teachers consume more soft drinks than women teachers (P = 0.002). Previous studies showed similar results revealed similar findings (59, 60). A study that examined the consumption pattern of sugar-sweetened beverages among college students in Jordan and its impact on their body weight, reported that men consumed greater amounts of sugar-sweetened beverages than women (P = 0.016) (59). This might be because women are more aware of the risk factors of soft drinks and are more concerned with their body image than men (61, 62). Another reason for such a difference reported by Xi et al. is that men drink less water than women, which leads to increased sugar-sweetened drink consumption (63). Men are also likely to consume more soft drinks overall since their overall food consumption is larger than that of women (62).
The present study findings showed that schoolteachers with high physical activity consumed more fruits, vegetables, beans, legumes, and dairy products than those with low physical activity. A sufficient degree of physical activity leads to improve health, including decreased overweight and obesity levels. Conversely, a lack of physical exercise is strongly associated with an elevated risk of cardiometabolic and vascular diseases (64). This is probably because most study participants had university degrees (bachelor's and postgraduate), which indicates that people who are well-educated are more aware about nutritional aspects and have a favourable attitude towards leading a healthy lifestyle (54). Previous studies have shown a close relationship between exercise and healthy food choices (65–67), which appears to be associated with improved health knowledge and awareness, as well as perceiving a healthy diet and physical activity requirements as beneficial and practical (68). Similarly, a study concluded that low levels of physical activity were associated with inadequate fruit and vegetable intake among young adults in Brazil (low consumption of fruits and vegetables by 79 and 90% respectively) (69). Additionally, in previous study among college students in Saudi Arabia physically active students tend to consume higher amounts of fruits, vegetables, and dairy products than inactive students (70). Other studies found that adults with an active lifestyle eat healthier diets including more fibre and fruits and vegetables, less saturated fat, and fewer servings of fried food and sweets than sedentary adults (65, 66, 68). Furthermore, in the current study, schoolteachers with low physical activity consumed fewer snacks and less red meat than those with high physical activity. These findings are consistent with a previous study conducted among Polish adults (71). The Polish study reported that adults who considered themselves physically active consumed less red meat and meat products (71). Although, few studies investigated the relationship between physical activity and the consumption of red meat, a previous study in adult women aged 20–50 years old reported that lower physical activity is associated with low consumption of red meat, which is consistent with our findings (72). However, in a study conducted among female undergraduate students, the high consumption of unhealthy snacks was significantly associated with increased levels of physical activity (73), which is the opposite of our findings as the present study showed that those who were physically active had higher intake of healthy food and less intake of unhealthy snacks.
The present study results showed that schoolteachers with high BMI have a decreased consumption of fruits compared to those with normal weight, which is aligned with previous studies (74). These findings are supported by the fact that a higher intake of fruits and vegetables lowers the risk of developing obesity (75). Increasing fruit and vegetable intake may also contribute to weight management because fruits and vegetables are low in energy but high in fibre and water, thereby producing a satiating effect (76). The satiating properties of fruits and vegetables lead to a reduction in energy-dense, nutrient-poor food consumption, thereby reducing overall caloric intake (76, 77). The intake of snacks, depending on the quantity and frequency of consumption, is unlikely to increase body weight. However, our findings showed that schoolteachers with high BMI consumed fewer snacks than schoolteachers with normal weight. Several studies have found that snacking frequency and daily calorie consumption from snacks have a negligible or even inverse relationship with the risk of becoming overweight or obese (78, 79). However, these associations may be confounded due to the underreporting of snacking behaviours among obese people compared to normal-weight respondents (78, 80). The consumption patterns of main meals and the choice of foods and beverages consumed as snacks appear to influence the associations between snacking, diet quality, and body weight (81). In particular, frequent snacks as substitutes for main meals may have a negligible impact on body weight and daily energy balance. Moreover, our findings indicated that less intake of vegetables is associated with increased risk of obesity. Data from the Atlantic Partnership for Tomorrow's Health Study demonstrated that increased fruit and vegetable consumption is inversely associated with BMI risk (82). Previous study showed that low vegetable intake was strongly associated with obesity risk among Japanese patients with type 2 diabetes in both sexes (83). These findings are supported by the results of a systematic review confirming that increased vegetable intake is associated with weight loss of 0.09–0.1 kg over 4 years, decreased risk of weight gain, and lower risk of overweight or obesity (84). Vegetables may contribute to the beneficial effects of weight changes, as they abundantly contain vitamins, minerals, fibres, and proteins (16, 85). In the present study findings, white meat consumption had a negative association with increased BMI. Red meat consumption has been linked to general and abdominal obesity in several epidemiological studies, but the results have been inconsistent (86, 87). Several studies have indicated that red meat consumption is positively associated with obesity (88, 89), whereas others have not found a significant correlation (90, 91). Because red meat and its products are a rich source of protein, cholesterol, and saturated fatty acids, they are considered high-energy-density foods (88). Moreover, the association between white meat consumption and obesity has received less attention in previous studies than red meat consumption, and the results in this regard have been more controversial (92, 93). According to Vergnaud et al., who assessed the association between the consumption of total meat, red meat, poultry, and processed meat in a large European population, higher poultry consumption was found to be associated with a lower risk of obesity (93), whereas Maskarinec et al. found a significant positive relationship between white meat consumption and obesity in Hawaii (94). Furthermore, a longitudinal study of ~90,000 adults whose dietary habits and anthropometric data were measured for 6.5 years showed a statistically significant relationship between the consumption of animal proteins and long-term weight gain (95).
4.1. Strengths and limitations
The main strength of this research is that it is the first study to examine the associations of dietary intake with physical activity and obesity using a representative sample of public school teachers living in Jeddah. In our analysis, we adjusted for socioeconomic factors that may significantly influence dietary intake. However, the current study has certain limitations. First, information about dietary intake, physical activity level, health status and body height and weight were collected using a self-reported questionnaire, which may raise concerns about recall bias, as some participants responded in socially desirable ways for some variables, including dietary intake. Second, the dietary intake was not measured using the semi-quantitative FFQ; only the intake frequency, i.e., the number of days per week, was recorded. Future studies should consider FFQ which captures more food items than the one used in this study. Likewise, future studies should also consider using the semi-quantitative FFQ with both frequency and portion sizes. Another point is that body weight can affect the quantity and quality of food consumed, and vice versa (96); thus, the association between dietary intake and obesity can be ambiguous. Third, the cross-sectional design prevents drawing conclusions about causal relationships. Finally, the study findings cannot be generalised to all schoolteachers in Saudi Arabia, as this study examined only schoolteachers in Jeddah city; thus, extending the findings to other populations is not possible. Future studies should collect data from all regions in Saudi Arabia in order to generalise the findings for all the Kingdom.
5. Conclusions
The current study is one of the first to examine the associations of dietary intake with physical activity and obesity among schoolteachers in Saudi Arabia. Schoolteachers are a vital group that is neglected in scientific research, and they play an important role in promoting health in education systems by encouraging healthy lifestyles and healthy eating habits among students. The findings of this study revealed that more than half of the schoolteachers reported high physical activity levels; however, a high prevalence of overweight and obesity was also reported by the study participants. These high rates of overweight and obesity might increase the current or future risk of non-communicable diseases among schoolteachers. Our results also showed that high physical activity was associated with higher consumption of healthy food, including fruits, vegetables, beans, legumes, and dairy products. Conversely, higher BMI was associated with lower consumption of fruits, vegetables, snacks, and white meat. Adjustments to the lifestyle of teachers are required, aiming to increase their healthy diet and reduce several risk factors leading to cardiovascular disease, dyslipidaemia and diabetes. Schoolteachers are expected to be role models for students and future generations. Healthy schoolteachers influence the health and educational performance of students. However, health promotion interventions at schools focus on students, not teachers. Strategies to reduce the obesity risk among schoolteachers should focus on increasing the intake of a healthy diet, as well as increasing physical activity. Nutrition education programs are vital to encourage schoolteachers in Saudi Arabia to consume healthy food and adopt a healthy lifestyle, thereby enhancing public health.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving human participants were reviewed and approved by Education Department of Jeddah City and the Biomedical Ethics Research Committee of King Abdulaziz University (Reference No. 159-21). The patients/participants provided their written informed consent to participate in this study.
Author contributions
Conceptualisation: NAlm, IS, and NAlj. Methodology: NAlj and NAlm. Formal analysis: IS. Data collection and writing—original draft preparation: NAlm, IS, MA, MH, HW, and NAlj. All authors have read and agreed to the published version of the manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Swinburn BA, Sacks G, Hall KD, McPherson K, Finegood DT, Moodie ML, et al. The global obesity pandemic: shaped by global drivers and local environments. Lancet. (2011) 378:804–14. doi: 10.1016/S0140-6736(11)60813-1
2. Alluhidan M, Alsukait RF, Alghaith T, Shekar M, Alazemi N, Herbst CH. Overweight and Obesity in Saudi Arabia: Consequences and Solutions. International Development in Focus. Washington, DC: World Bank (2022). doi: 10.1596/978-1-4648-1828-8
3. World Health Organization (WHO). Obesity and Overweight. Available online at: Audible.com/start-listentail/obesity-and-overweight. https://www.who.int/news-room/fact-sheets/dehttps://stories (accessed August 05, 2022).
4. Korkmaz C. Assessment of health-promoting lifestyle profiles and nutritional knowledge levels of pre-service physical education and science teachers: A comparative study example. Educ Q Rev. (2022) 13:564–76. doi: 10.31219/osf.io/7v6m5
5. Elhadd T, Al-Amoudi A, Alzahrani A. Epidemiology, clinical and complications profile of diabetes in Saudi Arabia: a review. Ann Saudi Med. (2007) 27:241. doi: 10.4103/0256-4947.51484
6. Al-Agha A, Mabkhoot Y, Bahwirith A, Mohammed A, Ragbi R, Allhabi E, et al. Various causative factors and associated complications of childhood obesity in Jeddah, Western Region, Saudi Arabia. Ann Afr Med. (2020) 19:15. doi: 10.4103/aam.aam_8_19
7. El Bcheraoui C, Tuffaha M, Daoud F, Kravitz H, Al Mazroa MA, Al Saeedi M, et al. On your mark, get set, go: levels of physical activity in the kingdom of Saudi Arabia, 2013. J Phys Act Health. (2016) 13:231–8. doi: 10.1123/jpah.2014-0601
8. Scheuch K, Haufe E, Seibt R. Teachers' health. Dtsch Arztebl Int. (2015) 112:347–56. doi: 10.3238/arztebl.2015.0347
9. Saroja MM, Priya EMJ. awareness on healthy dietary habits among prospective teachers in Tirunelveli District. Turcomat. (2021) 12:4060–6. doi: 10.17762/turcomat.v12i3.1696
10. Hartline-Grafton HL, Rose D, Johnson CC, Rice JC, Webber LS. Are school employees role models of healthful eating? Dietary intake results from the ACTION worksite wellness trial. J Am Diet Assoc. (2009) 109:1548–56. doi: 10.1016/j.jada.2009.06.366
11. Smith KJ, Gall SL, McNaughton SA, Blizzard L, Dwyer T, Venn AJ. Skipping breakfast: longitudinal associations with cardiometabolic risk factors in the Childhood Determinants of Adult Health Study. Am J Clin Nutr. (2010) 25 92:1316–25. doi: 10.3945/ajcn.2010.30101
12. Kubik MY, Lytle LA, Hannan PJ, Story M, Perry CL. Food-related beliefs, eating behavior, and classroom food practices of middle school teachers. J Sch Health. (2002) 72:339–45. doi: 10.1111/j.1746-1561.2002.tb07921.x
13. Kruger HS, Venter CS, Vorster HH, Margetts BM. Physical inactivity is the major determinant of obesity in black women in the North West Province, South Africa: the THUSA study. Transition and Health During Urbanisation of South Africa. Nutrition. (2002) 18:422–7. doi: 10.1016/S0899-9007(01)00751-1
14. Farahmand BY, Persson PG, Michaëlsson K, Baron JA, Alberts A, Moradi T, et al. Physical activity and hip fracture: a population-based case-control study. Swedish Hip Fracture Study Group. Int J Epidemiol. (2000) 29:308–14. doi: 10.1093/ije/29.2.308
15. Delfino LD, Tebar WR, Gil FC, De Souza JM, Romanzini M, Fernandes RA, et al. Association of sedentary behaviour patterns with dietary and lifestyle habits among public school teachers: a cross-sectional study. BMJ Open. (2020) 10:e034322. doi: 10.1136/bmjopen-2019-034322
16. Vaz M, Bharathi AV. How sedentary are people in'sedentary'occupations? The physical activity of teachers in urban South India. Occup Med. (2004) 54:369–72. doi: 10.1093/occmed/kqg100
17. Brito WF, Santos CL, Marcolongo Ado A, Campos MD, Bocalini DS, Antonio EL, et al. Physical activity levels in public school teachers. Rev Saude Publica. (2012) 46:104–9. doi: 10.1590/S0034-89102012000100013
18. Tebar WR, Gil FCS, Delfino LD, Souza JM, Mota J, Christofaro DGD. Relationship of obesity with lifestyle and comorbidities in public school teachers—a cross-sectional study. Obesities. (2022) 2:52–63. doi: 10.3390/obesities2010006
19. Bakhotmah BA. Teachers dietary practices during school day in Jeddah, western Saudi Arabia. Food Sci Nutr. (2012) 3:1553–60. doi: 10.4236/fns.2012.311203
20. Delfino LD, Tebar WR, Tebar FCSG, De Souza JM, Romanzini M, Fernandes RA, et al. Association between sedentary behavior, obesity and hypertension in public school teachers. Ind Health. (2020) 58:345–53. doi: 10.2486/indhealth.2019-0170
21. Guthold R, Stevens GA, Riley LM, Bull FC. Worldwide trends in insufficient physical activity from 2001 to 2016: a pooled analysis of 358 population-based surveys with 1·9 million participants. Lancet Glob Health. (2018) 6:e1077–86. doi: 10.1016/S2214-109X(18)30357-7
22. Al-Hazzaa HM. Physical inactivity in Saudi Arabia revisited: A systematic review of inactivity prevalence and perceived barriers to active living. Int J Health Sci. (2018) 12:50–64. doi: 10.2196/preprints.9883
23. World Health Organization (WHO). Global Recommendations on Physical Activity for Health. (2010). Available online at: https://apps.who.int/iris/bitstream/handle/10665/44399/9789241599979_eng.pdf;jsessionid=04C423D4CAE804D52D889A6E370BA2ED?sequence=1 (accessed December 26, 2022).
24. de Souza SCS, Campanini MZ, de Andrade SM, González AD, de Melo JM, Mesas AE. Watching television for more than two hours increases the likelihood of reporting poor sleep quality among Brazilian schoolteachers. Physiol Behav. (2017) 179:105–9. doi: 10.1016/j.physbeh.2017.05.029
25. Ramón-Arbués E, Martínez-Abadía B, Gracia-Tabuenca T, Yuste-Gran C, Pellicer-García B, Juárez-Vela R, et al. Prevalence of overweight/obesity and its association with diabetes, hypertension, dyslipidemia and metabolic syndrome: a cross-sectional study of a sample of workers in Aragón, Spain. Nutr Hosp. (2019) 36:51–9. doi: 10.20960/nh.1980
26. De Pergola G, Silvestris F. Obesity as a major risk factor for cancer. J Obes. (2013) 2013:291546. doi: 10.1155/2013/291546
27. Myers J, McAuley P, Lavie CJ, Despres JP, Arena R, Kokkinos P. Physical activity and cardiorespiratory fitness as major markers of cardiovascular risk: their independent and interwoven importance to health status. Prog Cardiovasc Dis. (2015) 57:306–14. doi: 10.1016/j.pcad.2014.09.011
28. Umegaki H, Sakurai T, Arai H. Active life for brain health: a narrative review of the mechanism underlying the protectiveeffects of physical activity on the brain. Front Aging Neurosci. (2021) 13:761674. doi: 10.3389/fnagi.2021.761674
29. Weinberger NA, Kersting A, Riedel-Heller SG, Luck-Sikorski C. Body dissatisfaction in individuals with obesity compared to normal-weight individuals: a systematic review and meta-analysis. Obes Facts. (2016) 9:424–41. doi: 10.1159/000454837
30. Lei H, Cui Y, Chiu MM. The relationship between teacher support and students' academic emotions: a meta-analysis. Front Psychol. (2018) 8:2288. doi: 10.3389/fpsyg.2017.02288
31. Ibrahim NK, Hijazi NA, Al-Bar AA. Prevalence and determinants of prehypertension and hypertension among preparatory and secondary school teachers in Jeddah. J Egypt Public Health Assoc. (2008) 83: 183–203.
32. Girish B, Majgi, SM. A study of hypertension & its risk factors among primary school teachers of Tumkur, Karnataka. Indian J Forensic Community Med. (2017) 4: 53–7. doi: 10.18231/2394-6776.2017.0011
33. Familoni OB. Determinants and perception of cardiovascular risk factors among secondary school teachers in Oyo state Nigeria. Afr J Med Med Sci. (2011) 40: 339–43
34. Fadupin G, Olayiwola I. Prevalence of obesity among adult hypertensive patients attending the Lagos State Hospital, Ikeja South West, Nigeria. Nig J Nutri Sci. (2011) 32:70–8. doi: 10.4314/njns.v32i1.67813
35. Ickes MJ, McMullen J, Haider T, Sharma M. Global school-based childhood obesity interventions: a review. Int J Environ Res Public Health. (2014) 11:8940–61. doi: 10.3390/ijerph110908940
36. Ministry of Education. Statistical Evidence for the Academic year 1438/1439 AH. Jeddah: General Administration of Education in Jeddah Governorate. (2018). p. 5–85. Available online at: https://edu.moe.gov.sa/jeddah/DocumentCentre/Pages/default.aspx?DocId=929d43a6-1e95-48cc-aee0-d198ed2c49c6 (accessed November 11, 2021).
37. Raosoft.com. Sample size calculator by Raosoft, Inc. (2004). Available online at: http://www.raosoft.com/samplesize.html (accessed November 13, 2021)
38. World Health Organization (WHO). Body Mass Index—BMI. Available online at: http://www.euro.who.int/en/health-topics/diseaseprevention/nutrition/a-healthy-lifestyle/body-mass-index-bmi (accessed July 11, 2022).
39. Aljefree NM, Lee P, Alsaqqaf JM, Ahmed F. Association between vitamin D status and coronary heart disease among adults in Saudi Arabia: A case-control study. Healthcare. (2016) 4:77. doi: 10.3390/healthcare4040077
40. Cleghorn CL, Harrison RA, Ransley JK, Wilkinson S, Thomas J, Cade JE. Can a dietary quality score derived from a short-form FFQ assess dietary quality in UK adult population surveys? Public Health Nutr. (2016) 19:2915–23. doi: 10.1017/S1368980016001099
41. Karpushkina AV, Pankratova MS. Strategy for obesity prevention among school-age children (literature review). Probl Endocrinol. (2016) 62:52–60. doi: 10.14341/probl201662252-60
42. Dumitrescu AL, Dogaru BC, Dogaru CD, Manolescu B. The relationship between self-reported oral health, self-regulation, proactive coping, procrastination and proactive attitude. Community Dent Health. (2011) 28, 170–173. doi: 10.1922/CDH_2554Dumitrescu04
43. Graciano AMC, Cardoso NMM, Teixeira SA, Mattos FF, Gomes VE, Borges-Oliveira AC. Health promotion in Brazil: qualitative survey with primary school teachers. Health Promot Int. (2019) 34:e28–35. doi: 10.1093/heapro/day061
44. Herr SW, Telljohann SK, Price JH, Dake JA, Stone GE. High school health-education teachers' perceptions and practices related to teaching HIV prevention. J Sch Health. (2012) 82:514–21. doi: 10.1111/j.1746-1561.2012.00731.x
45. Lizana PA, Aballay J, Vicente-Rodríguez G, Gómez-Bruton A. Low interest in physical activity and higher rates of obesity among rural teachers. Work. (2020) 67:1015–22. doi: 10.3233/WOR-203351
46. Zubery D, Kimiywe J, Martin HD. Prevalence of overweight and obesity, and its associated factors among health-care workers, teachers, and bankers in Arusha City, Tanzania. Diabetes Metab Syndr Obes. (2021) 14:455–65. doi: 10.2147/DMSO.S283595
47. Low S, Chin MC, Deurenberg-Yap M. Review on epidemic of obesity. Ann Acad Med Singap. (2009) 38:57–9. doi: 10.47102/annals-acadmedsg.V38N1p57
48. Mauvais-Jarvis F, Bairey Merz N, Barnes PJ, Brinton RD, Carrero JJ, DeMeo DL, et al. Sex and gender: modifiers of health, disease, and medicine. Lancet. (2020) 396:565–82. doi: 10.1016/S0140-6736(20)31561-0
49. Aljefree N, Ahmed F. Prevalence of cardiovascular disease and associated risk factors among adult population in the gulf region: a systematic review. Adv Public Health. (2015) 2015:1–23. doi: 10.1155/2015/235101
50. Al-Hamdan NA, Kutbi A, Choudhry AJ, Nooh R, Shoukri M, Mujib S. WHO STEPwise Approach to NCD Surveillance. Country-Specific Standard Report: Saudi Arabia. (2005). Available online at: http://www.who.int/chp/steps/2005_SaudiArabia_STEPS_Report_EN.pdf?ua=1 (accessed July 2022).
51. Al-Zalabani AH, Al-Hamdan NA, Saeed AA. The prevalence of physical activity and its socioeconomic correlates in Kingdom of Saudi Arabia: a cross-sectional population-based national survey. J Taibah Univ Med Sci. (2015) 10:208–15. doi: 10.1016/j.jtumed.2014.11.001
52. World Health Organization (WHO). Physical Activity Fact Sheet No. 385. (2015). Available online at: http://www.who.int/mediacentre/factsheets/fs385/en (accessed July 2022).
53. Sharara E, Akik C, Ghattas H, Makhlouf Obermeyer C. Physical inactivity, gender and culture in Arab countries: a systematic assessment of the literature. BMC Public Health. (2018) 18:639. doi: 10.1186/s12889-018-5472-z
54. Raghupathi, V., Raghupathi, W. The influence of education on health: an empirical assessment of OECD countries for the period 1995–2015. Arch Public Health. (2020) 78:20. doi: 10.1186/s13690-020-00402-5
55. Moradi-Lakeh M, El Bcheraoui C, Afshin A, Daoud F, AlMazroa MA, Al Saeedi M, et al. Diet in Saudi Arabia: findings from a nationally representative survey. Public Health Nutr. (2017) 20:1075–81. doi: 10.1017/S1368980016003141
56. GBD 2013 Risk Factors Collaborators, Forouzanfar MH, Alexander L, Anderson HR, Bachman VF, Biryukov S, et al. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks in 188 countries, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. (2015) 386:2287–323. doi: 10.1016/S0140-6736(15)00128-2
57. Afshin A, Micha R, Khatibzadeh S, Fahimi S, Shi P, Powles J, et al. The impact of dietary habits and metabolic risk factors on cardiovascular and diabetes mortality in countries of the Middle East and North Africa in 2010: a comparative risk assessment analysis. BMJ Open. (2015) 5:e006385. doi: 10.1136/bmjopen-2014-006385
58. Parker EA, Feinberg TM, Lane HG, Deitch R, Zemanick A, Saksvig BI, et al. Diet quality of elementary and middle school teachers is associated with healthier nutrition-related classroom practices. Prev Med Rep. (2020) 18:101087. doi: 10.1016/j.pmedr.2020.101087
59. Bawadi H, Khataybeh T, Obeidat B, Kerkadi A, Tayyem R, Banks A, et al. Sugar-sweetened beverages contribute significantly to college students' daily caloric intake in Jordan: soft drinks are not the major contributor. Nutrients. (2019) 11:1058. doi: 10.3390/nu11051058
60. McGreen J, Kemps E, Tiggemann M. The predictive value of evaluative bias, attentional bias, approach bias, and self-regulatory control in soft drink consumption. Appetite. (2022) 168:105771. doi: 10.1016/j.appet.2021.105771
61. Fiorito LM, Marini M, Mitchell DC, Smiciklas-Wright H, Birch LL. Girls' early sweetened carbonated beverage intake predicts different patterns of beverage and nutrient intake across childhood and adolescence. J Am Diet Assoc. (2010) 110: 543–50. doi: 10.1016/j.jada.2009.12.027
62. Perkins JM, Perkins HW, Craig DW. Misperceptions of peer norms as a risk factor for sugar-sweetened beverage consumption among secondary school students. J Am Diet Assoc. (2010) 110:1916–21. doi: 10.1016/j.jada.2010.09.008
63. Xi B, Huang Y, Reilly KH, Li S, Zheng R, Barrio-Lopez MT, et al. Sugar-sweetened beverages and risk of hypertension and CVD: a dose–response meta-analysis. Br J Nutr. (2015) 113:709–17. doi: 10.1017/S0007114514004383
64. Gaesser GA, Angadi SS. Obesity treatment: weight loss versus increasing fitness and physical activity for reducing health risks. Iscience. (2021) 24:102995. doi: 10.1016/j.isci.2021.102995
65. Wirnitzer K, Boldt P, Lechleitner C, Wirnitzer G, Leitzmann C, Rosemann T, et al. Health status of female and male vegetarian and vegan endurance runners compared to omnivores-Results from the NURMI Study (Step 2). Nutrients. (2018) 11:29. doi: 10.3390/nu11010029
66. Cardoso LSM, Gomes CS, Moreira AD, Bernal RTI, Ribeiro ALP, Malta DC. Fruit and vegetable consumption, leisure-time physical activity and binge drinking in Belo Horizonte, Brazil, according to the Health Vulnerability Index. Rev Bras Epidemiol. (2021) 24:e210013. doi: 10.1590/1980-549720210013.supl.1
67. van der Avoort CMT, Ten Haaf DSM, de Vries JHM, Verdijk LB, van Loon LJC, Eijsvogels TMH, et al. Higher levels of physical activitybib are associated with greater fruit and vegetable intake in older adults. J Nutr Health Aging. (2021) 25:230–41. doi: 10.1007/s12603-020-1520-3
68. de Visser RO, Conroy D, Davies E, Cooke R. Understanding motivation to adhere to guidelines for alcohol intake, physical activity, and fruit and vegetable intake among U.K. university students. Health Educ Behav. (2021) 48:480–7. doi: 10.1177/1090198120988251
69. Silva DAS, Silva RJdS. Association between physical activity level and consumption of fruit and vegetables among adolescents in northeast Brazil. Revista Paulista de Pediatria (English Edition). Rev Paul Pediatr. (2015) 33:167–73. doi: 10.1016/S2359-3482(15)30047-6
70. Shatwan IM, Aljefree NM, Almoraie NM. Snacking pattern of college students in Saudi Arabia: a cross-sectional study. BMC Nutr. (2022) 8:49. doi: 10.1186/s40795-022-00544-5
71. Jezewska-Zychowicz M, Gebski J, Guzek D, Swiatkowska M, Stangierska D, Plichta M, et al. The associations between dietary patterns and sedentary behaviors in Polish adults (LifeStyle study). Nutrients. (2018) 10:1004. doi: 10.3390/nu10081004
72. Mofrad MD, Mozaffari H, Sheikhi A, Zamani B, Azadbakht L. The association of red meat consumption and mental health in women: a cross-sectional study. Complemen Ther Med. (2021) 56:102588. doi: 10.1016/j.ctim.2020.102588
73. Petersen JM, Prichard I, Kemps E, Tiggemann M. The effect of snack consumption on physical activity: a test of the Compensatory Health Beliefs Model. Appetite. (2019) 141:104342. doi: 10.1016/j.appet.2019.104342
74. Mellendick K, Shanahan L, Wideman L, Calkins S, Keane S, Lovelady C. Diets rich in fruits and vegetables are associated with lower cardiovascular disease risk in adolescents. Nutrients. (2018) 10:136. doi: 10.3390/nu10020136
75. Howarth NC, Saltzman E, Roberts SB. Dietary fiber and weight regulation. Nutr Rev. (2001) 59:129–39. doi: 10.1111/j.1753-4887.2001.tb07001.x
76. Aljefree NM, Shatwan IM, Almoraie NM. Impact of the intake of snacks and lifestyle behaviors on obesity among university students living in Jeddah, Saudi Arabia. Healthcare. (2022) 10:400. doi: 10.3390/healthcare10020400
77. Rolls BJ. The relationship between dietary energy density and energy intake. Physiol Behav. (2009) 97:609–15. doi: 10.1016/j.physbeh.2009.03.011
78. Murakami K, Livingstone MB. Associations between energy density of meals and snacks and overall diet quality and adiposity measures in British children and adolescents: the National Diet and Nutrition Survey. Br J Nutr. (2016) 116:1633–45. doi: 10.1017/S0007114516003731
79. McCrory MA, Howarth NC, Roberts SB, Huang TT. Eating frequency and energy regulation in free-living adults consuming self-selected diets. J Nutr. (2011) 141:148–53. doi: 10.3945/jn.109.114991
80. Sebastian RS, Wilkinson Enns C, Goldman JD. US adolescents and MyPyramid: associations between fast-food consumption and lower likelihood of meeting recommendations. J Am Diet Assoc. (2009) 109:226–35. doi: 10.1016/j.jada.2008.10.053
81. Vatanparast H, Islam N, Patil RP, Shafiee M, Smith J, Whiting S. Snack consumption patterns among Canadians. Nutrients. (2019) 11:1152. doi: 10.3390/nu11051152
82. Yu ZM, DeClercq V, Cui Y, Forbes C, Grandy S, Keats M, et al. Fruit and vegetable intake and body adiposity among populations in Eastern Canada: the Atlantic Partnership for Tomorrow's Health Study. BMJ Open. (2018) 8:e018060. doi: 10.1136/bmjopen-2017-018060
83. Hatta M, Horikawa C, Takeda Y, Ikeda I, Yoshizawa Morikawa SY, Kato N, et al. Association between obesity and intake of different food groups among Japanese with type 2 diabetes mellitus-Japan diabetes clinical data management study (JDDM68). Nutrients. (2022) 14:3034. doi: 10.3390/nu14153034
84. Nour M, Lutze SA, Grech A, Allman-Farinelli M. The relationship between vegetable intake and weight outcomes: a systematic review of cohort studies. Nutrients. (2018) 10:1626. doi: 10.3390/nu10111626
85. Bertoia ML, Mukamal KJ, Cahill LE, Hou T, Ludwig DS, Mozaffarian D, et al. Changes in intake of fruits and vegetables and weight change in United States men and women followed for up to 24 years: analysis from three prospective cohort studies. PLoS Med. (2015) 12:e1001878. doi: 10.1371/journal.pmed.1001878
86. Xu F, Yin XM, Tong SL. Association between excess bodyweight and intake of red meat and vegetables among urban and rural adult Chinese in Nanjing, China. Asia Pac J Public Health. (2007) 19:3–9. doi: 10.1177/101053950701900302
87. Rouhani MH, Salehi-Abargouei A, Surkan PJ, Azadbakht L. Is there a relationship between red or processed meatintake and obesity? A systematic review and meta-analysis ofobservational studies. Obes Rev. (2014) 15:740–8. doi: 10.1111/obr.12172
88. Hashemipour S, Esmailzadehha N, Mohammadzadeh M, Ziaee A. Association of meat and dairy consumption with normal weight metabolic obesity in men: the Qazvin Metabolic Diseases Study. Eat Weight Disord. (2016) 21:419–25. doi: 10.1007/s40519-015-0250-8
89. Wang Z, Zhang B, Zhai F, Wang H, Zhang J, Du W, et al. Fatty and lean red meat consumption in China: differential association with Chinese abdominal obesity. Nutr Metab Cardiovasc Dis. (2014) 24:869–76. doi: 10.1016/j.numecd.2014.03.002
90. Wagemakers JJ, Prynne CJ, Stephen AM, Wadsworth ME. Consumption of red or processed meat does not predict risk factors for coronary heart disease; results from a cohort of British adults in 1989 and 1999. Eur J Clin Nutr. (2009) 63:303–11. doi: 10.1038/sj.ejcn.1602954
91. Babio N, Sorlí M, Bulló M, Basora J, Ibarrola-Jurado N, Fernández-Ballart J, et al. Association between red meat consumption and metabolic syndrome in a Mediterranean population at high cardiovascular risk: cross-sectional and 1-year follow-up assessment. Nutr Metab Cardiovasc Dis. (2012) 22:200–7. doi: 10.1016/j.numecd.2010.06.011
92. Cocate PG, Natali AJ, de Oliveira A, Alfenas Rde C, Peluzio Mdo C, Longo GZ, et al. Red but not white meat consumption is associated with metabolic syndrome, insulin resistance and lipid peroxidation in Brazilian middle-aged men. Eur J Prev Cardiol. (2015) 22:223–30. doi: 10.1177/2047487313507684
93. Vergnaud AC, Norat T, Romaguera D, Mouw T, May AM, Travier N, et al. Meat consumption and prospective weight change in participants of the EPIC-PANACEA study. Am J Clin Nutr. (2010) 92:398–407. doi: 10.3945/ajcn.2009.28713
94. Maskarinec G, Takata Y, Pagano I, Carlin L, Goodman MT, Le Marchand L, et al. Trends and dietary determinants of overweight and obesity in a multiethnic population. Obes Silver Spring. (2006) 14:717–26. doi: 10.1038/oby.2006.82
95. Perna M, Hewlings S. Saturated fatty acid chain length and risk of cardiovascular disease: a systematic review. Nutrients. (2022) 15:30. doi: 10.3390/nu15010030
Keywords: obesity, dietary behaviour, diet, physical activity, schoolteachers
Citation: Almoraie NM, Shatwan IM, Althaiban MA, Hanbazaza MA, Wazzan HA and Aljefree NM (2023) Associations between dietary intake, physical activity, and obesity among public school teachers in Jeddah, Saudi Arabia. Front. Nutr. 10:1081928. doi: 10.3389/fnut.2023.1081928
Received: 27 October 2022; Accepted: 09 January 2023;
Published: 24 January 2023.
Edited by:
Antonios Koutelidakis, University of the Aegean, GreeceReviewed by:
Konstantina Argyri, University of Peloponnese, GreeceStavroula Stoupi, Metropolitan College, Greece
Copyright © 2023 Almoraie, Shatwan, Althaiban, Hanbazaza, Wazzan and Aljefree. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Noha M. Almoraie,  bmFsbW9yaWVAa2F1LmVkdS5zYQ==
bmFsbW9yaWVAa2F1LmVkdS5zYQ==