 Yan-Ming Jiang1
Yan-Ming Jiang1 Xiao-Dong Zhu
Xiao-Dong Zhu
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Nutr., 16 February 2023
Sec. Clinical Nutrition
Volume 10 - 2023 | https://doi.org/10.3389/fnut.2023.1036572
This article is part of the Research TopicSystemic Markers of Muscle LossView all 13 articles
Purpose: This study explored the relationship between the prognostic nutritional index (PNI) and overall survival rate (OS) in patients with nasopharyngeal carcinoma (NPC), and established and validated an effective nomogram to predict clinical outcomes.
Methods: This study included 618 patients newly diagnosed with locoregionally advanced NPC. They were divided into training and validation cohorts at a ratio of 2:1 based on random numbers. The primary endpoint of this study was OS, progression-free survival (PFS) was the second endpoint. A nomogram was drawn from the results of multivariate analyses. Harrell’s concordance index (C-index), area under the receiver operator characteristic curve (AUC), and decision curve analysis (DCA) were used to evaluate the clinical usefulness and predictive ability of the nomogram and were compared to the current 8th edition of the International Union Against Cancer/American Joint Committee (UICC/AJCC) staging system.
Results: The PNI cutoff value was 48.1. Univariate analysis revealed that age (p < 0.001), T stage (p < 0.001), N stage (p = 0.036), tumor stage (p < 0.001), PNI (p = 0.001), lymphocyte-neutrophil ratio (NLR, p = 0.002), and lactate dehydrogenase (LDH, p = 0.009) were significantly associated with OS, age (p = 0.001), T-stage (p < 0.001), tumor stage (p < 0.001), N-stage (p = 0.011), PNI (p = 0.003), NLR (p = 0.051), and LDH (p = 0.03) were significantly associated with PFS. Multivariate analysis showed that age (p < 0.001), T-stage (p < 0.001), N-stage(p = 0.02), LDH (p = 0.032), and PNI (p = 0.006) were significantly associated with OS, age (p = 0.004), T-stage (<0.001), N-stage (<0.001), PNI (p = 0.022) were significantly associated with PFS. The C-index of the nomogram was 0.702 (95% confidence interval [CI]: 0.653–0.751). The Akaike information criterion (AIC) value of the nomogram for OS was 1142.538. The C-index of the TNM staging system was 0.647 (95% CI, 0.594–0.70) and the AIC was 1163.698. The C-index, DCA, and AUC of the nomogram demonstrated its clinical value and higher overall net benefit compared to the 8th edition of the TNM staging system.
Conclusion: The PNI represents a new inflammation-nutrition-based prognostic factor for patients with NPC. In the proposed nomogram, PNI and LDH were present, which led to a more accurate prognostic prediction than the current staging system for patients with NPC.
Nasopharyngeal carcinoma (NPC) is highly prevalent in southern China and Southeast Asia, with an incidence rate of 20-30/100,000/year in some areas (1). Radiotherapy (RT) is the most important treatment for RT. Owing to the use of intensity-modulated radiotherapy (IMRT), the cure rate has significantly improved, particularly in terms of local recurrence-free and overall survival (OS). However, the incidence of distant metastasis remains high and is the main failure mode (2). Although the tumor lymph node metastasis (TNM) staging system is often considered the most valuable prognostic factor for NPC in clinical practice, the heterogeneity of patients at the same stage, who often have different risk factors, limits the ability of the system to differentiate between patients with different prognoses and make accurate treatment choices. Personalized and accurate predictions are challenging. Studies have shown a significant link between inflammatory markers and poor prognosis in patients with various types of tumors (3, 4). Thus, indicators of systemic inflammation, such as the neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), and lymphocyte-to-monocyte ratio (LMR), have received increased attention (5–7). Recent studies have demonstrated a close relationship between immunonutritional status and tumor prognosis (8). The choice of treatment and quality of life are affected by patient nutritional status and immune function. Therefore, monitoring the nutritional and immune status of the body plays an important role in determining curative effects and prognosis (9). Hence, this study aimed to determine the value of inflammatory immune and nutritional indicators in the prognosis of patients with NPC.
Buzey first proposed the prognostic nutritional index (PNI) which is calculated from the serum albumin concentration and peripheral blood lymphocyte count (10). The PNI has been shown to be a valid indicator of a patient’s immune and nutritional status (11). The PNI was designed to assess the periodic operational immunity status and surgical risk in patients undergoing gastrointestinal surgery (12). Although investigators have demonstrated the significant value of PNI in the survival prognosis of many types of malignancy (13–15), few studies have reported the PNI prognosis of NPCs. While several studies have investigated the PNI in metastatic NPC (16, 17), the patients were treated using various regimens. Thus, the association of the PNI with the prognosis of survival, especially in patients with locally advanced NPC undergoing concurrent chemoradiotherapy (CCRT) with or without adjuvant chemotherapy (AC) remains unknown. Therefore, to eliminate therapeutic heterogeneity, the present study investigated the prognostic value of PNI in patients with locally advanced NPC.
Data on patients with NPC who received chemoradiotherapy at Guangxi Medical University Cancer Hospital from 2010 to 2013 were collected and analyzed. NPC was diagnosed based on histological evidence. The inclusion criteria were: (1) patients with NPC who underwent IMRT, (2) received concurrent chemoradiation combined with or without adjuvant chemotherapy, and (3) had no hematology disease, infection, or hyperpyrexia. The exclusion criteria were: (1) multiple cancers at diagnosis, (2) TNM stages I–II and IVb, and (3) missing values in the relevant predictors or follow-up data (Figure 1).
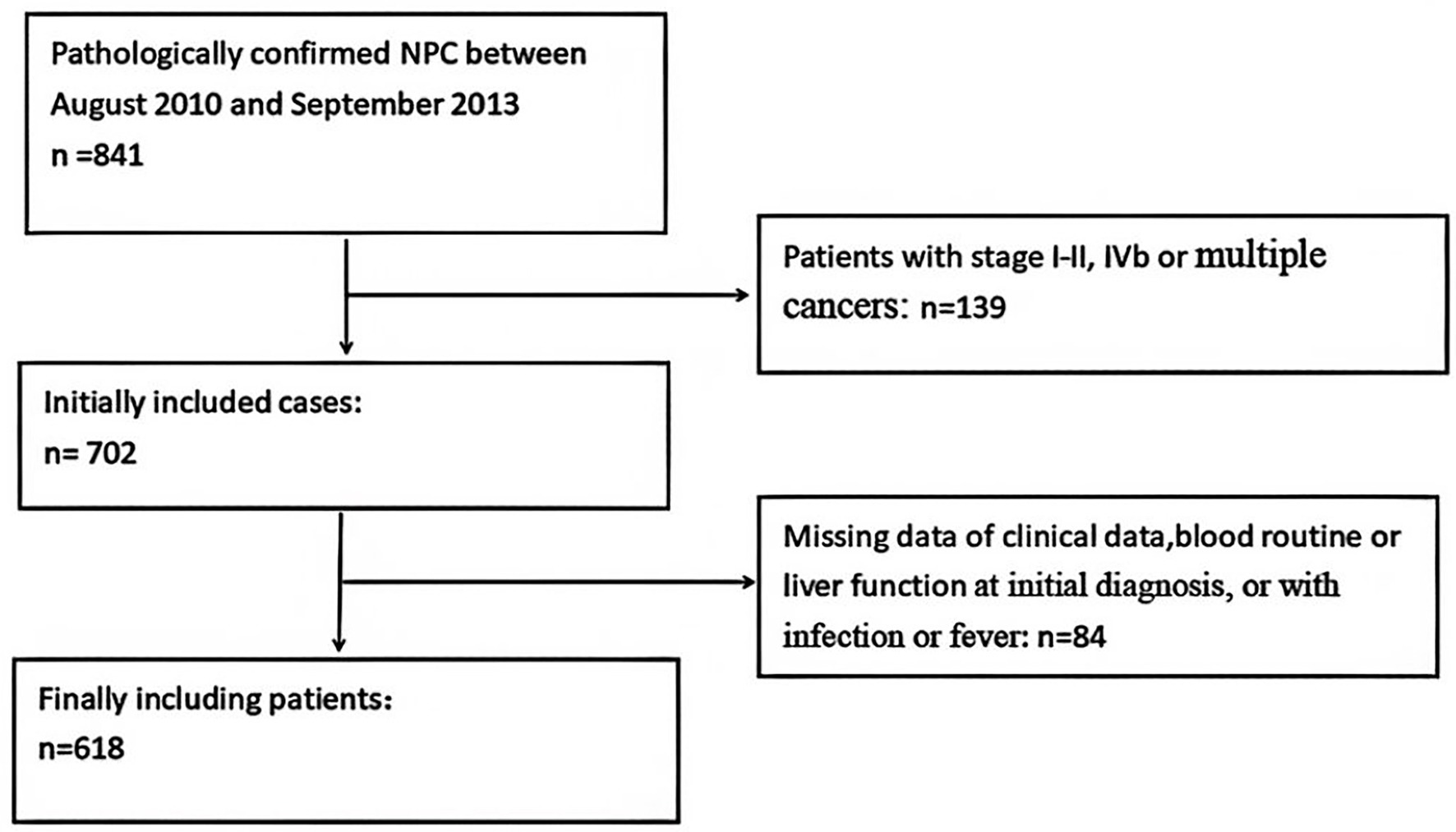
Figure 1. Flow chart of patient inclusion.
The collected clinical data included age, sex, chemotherapy, clinical stage, radiotherapy dose, pretreatment lymphocyte count, pretreatment neutrophil count, pretreatment lactate dehydrogenase (LDH) level, pretreatment platelet count, serum albumin count (ALB), and pretreatment body mass index (BMI), which were calculated for each patient. The neutrophil-to-lymphocyte ratio (NLR) was calculated. The PNI was determined using the formula PNI = ALB+5 × lymphocyte count (g/L). This study was approved by the Ethics Committee of Guangxi Medical University Cancer Hospital (LW2022029). All data were anonymized; therefore, the requirement to obtain informed consent was waived.
Radical IMRT was performed in all patients. Primary nasopharyngeal gross tumor volume (GTVnx) and cervical lymph node tumor volume (GTVnd) were defined as tumors visible on computed tomography (CT), magnetic resonance imaging (MRI), 18F-fluorodeoxyglucose positron emission tomography with computed tomography (PET-CT), and physical examinations. Clinical target volume (CTV1) was determined using the formula CTV1 = GTVnx + (5–10 mm) margins. The CTV2 = CTV1 + (5–10 mm margins) included the GTVnd lymphatic region. The planning target volume (PTV) was calculated as PTV = CTV + 3 mm margins. The prescription dosage was: PGTVnx 70–75.9 Gy/31–32f, PGTVnd 60–73.6 Gy/30–32f, PCTV1 60–68 Gy/30 ~ 31f, and PCTV2 54–57.6 Gy/30–31 f.
All patients were administered concurrent chemotherapy. The chemotherapy regimen comprised cisplatin (2–3 cycles of 80–100 mg/m2 every 21 days). The adjuvant chemotherapy (AC) regimens included PF (cisplatin,80 mg/m2+ 5-fluorouracil 3,000 mg/m2), TPF (docetaxel 60 mg/m2 + cisplatin 60 mg/m2 + 5-fluorouracil 3,000 mg/m2), and TP (docetaxel 75 mg/m2 + cisplatin 75 mg/m2, every 21 days) after CCRT, for at least one cycle.
Patients were reviewed every 3 months for 2 years after the end of treatment. Within 3–5 years of the end of treatment, the reviews were performed every 6 months. Five years after the end of treatment, an annual review was conducted. OS was defined as the primary endpoint and was measured from the date of diagnosis to the date of death or the last follow-up, whichever occurred first.
To assess the sensitivity and specificity of OS, we used X-tile software (version 3.6.1, Yale University 2003-05) to determine the optimal cutoff values for the PNI and NLR (18). We evaluated other clinicopathological variables associated with the risk of progression, including BMI (19), age, and LDH (20), based on clinical significance, basic theoretical knowledge, and predictors identified in previous studies.
For continuous variables, means ± SD or medians are reported. Mann–Whitney U or Kruskal–Wallis tests were used for analysis, as appropriate. Numbers and proportions were reported for categorical variables. χ2 or Fisher’s exact tests were used for the analysis. Cox proportional hazards models were used for univariate and multivariate analyses. All p-values were two-tailed, with p < 0.05 considered statistically significant. IBM SPSS Statistics, version 23.0 (IBM Corp., Armonk, NY, United States) was used for statistical analysis.
Based on the results of the multivariate analysis, we established a nomogram. The predictive accuracy and discriminative ability were used to evaluate the predicted nomogram values. The C-index and calibration plot of the nomogram for 5-year OS were used to evaluate its performance. Harrell’s C-index and calibration plots were used for the external validation of the nomogram, which were compared to the current 8th edition of the International Union Against Cancer/American Joint Committee (UICC/AJCC) staging system based on C-index, receiver operating characteristic (ROC), and decision curve analysis (DCA). All steps were implemented using R software version 4.1.2 (R Foundation for Statistical Computing, Vienna, Austria).
A total of 618 patients were enrolled and randomly assigned to the training and validation cohorts in a 2:1 ratio based on random numbers. The patient characteristics are shown in Table 1. No significant differences were observed between the training and validation cohorts (Table 1).
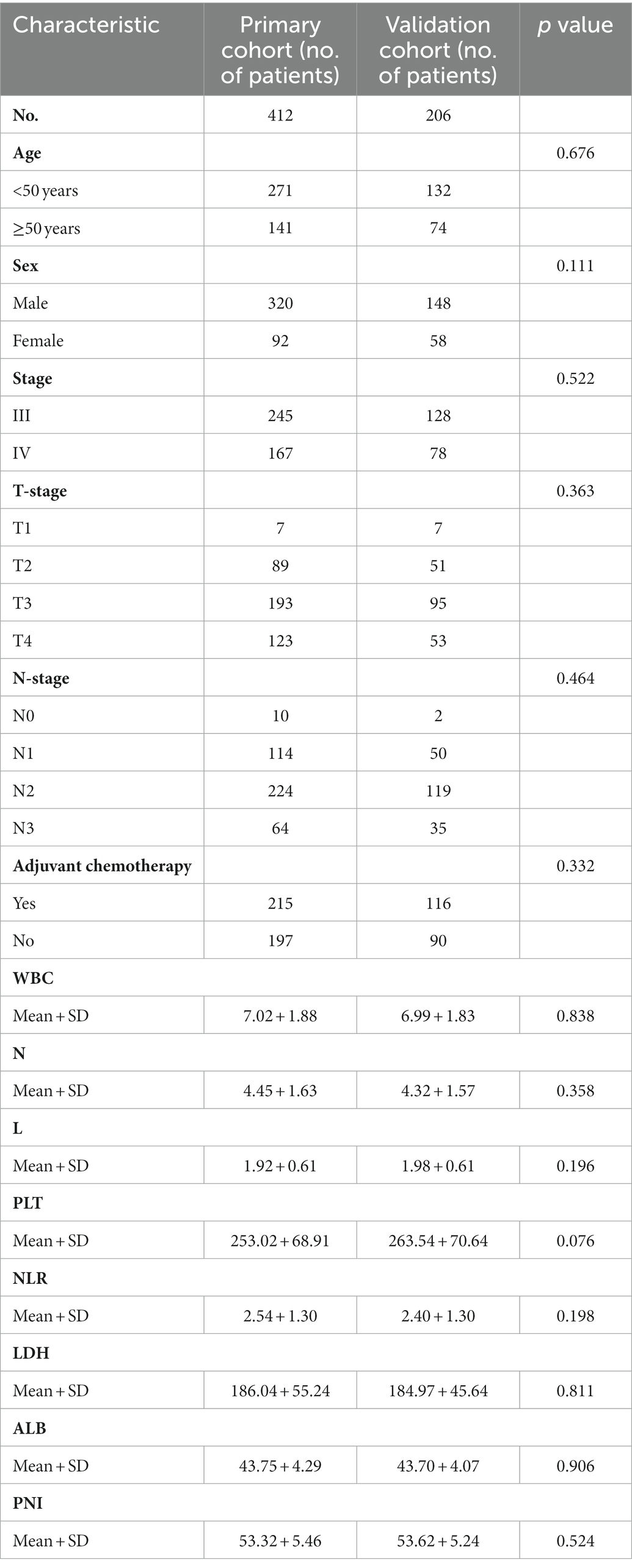
Table 1. Baseline patient characteristics.
The median follow-up duration was 84 (range, 2–125) months. Of the patients, 148 died and 179 had advanced disease at the last follow-up. The 1-, 3-, and 5-year estimated OS rates in all cohorts were 98.5, 89.5, and 82.6%, respectively. The 1-, 3-, and 5-year estimated OS rates in the training cohort were 98.5, 88.3, and 80.9%, respectively, whereas those in the validation cohort were 98.5, 89.4, and 82.9%, respectively.
NLR and PNI were used as test variables and OS as state variables. The X-tile program was used to determine the optimal cutoff values of NLR and PNI (2.7 and 48.1, respectively) (Figure 2). The PNI was significantly associated with age and T stage (Table 2). These findings are similar to those of related studies (21, 22).
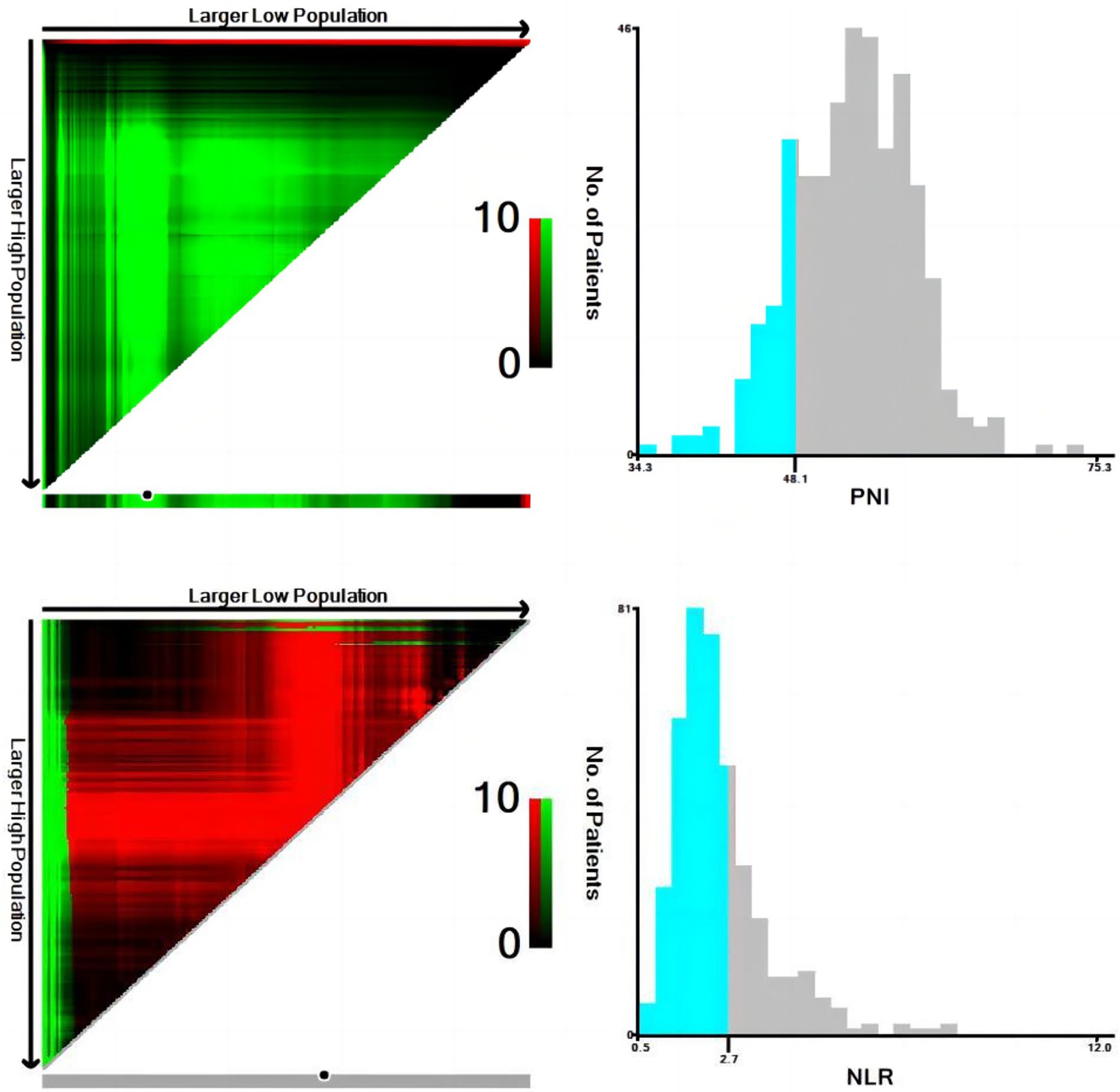
Figure 2. Calculation of optimal cut-off values of neutrophil-to-lymphocyte ratio (NLR) and prognostic nutritional index (PNI) by X-tile software.
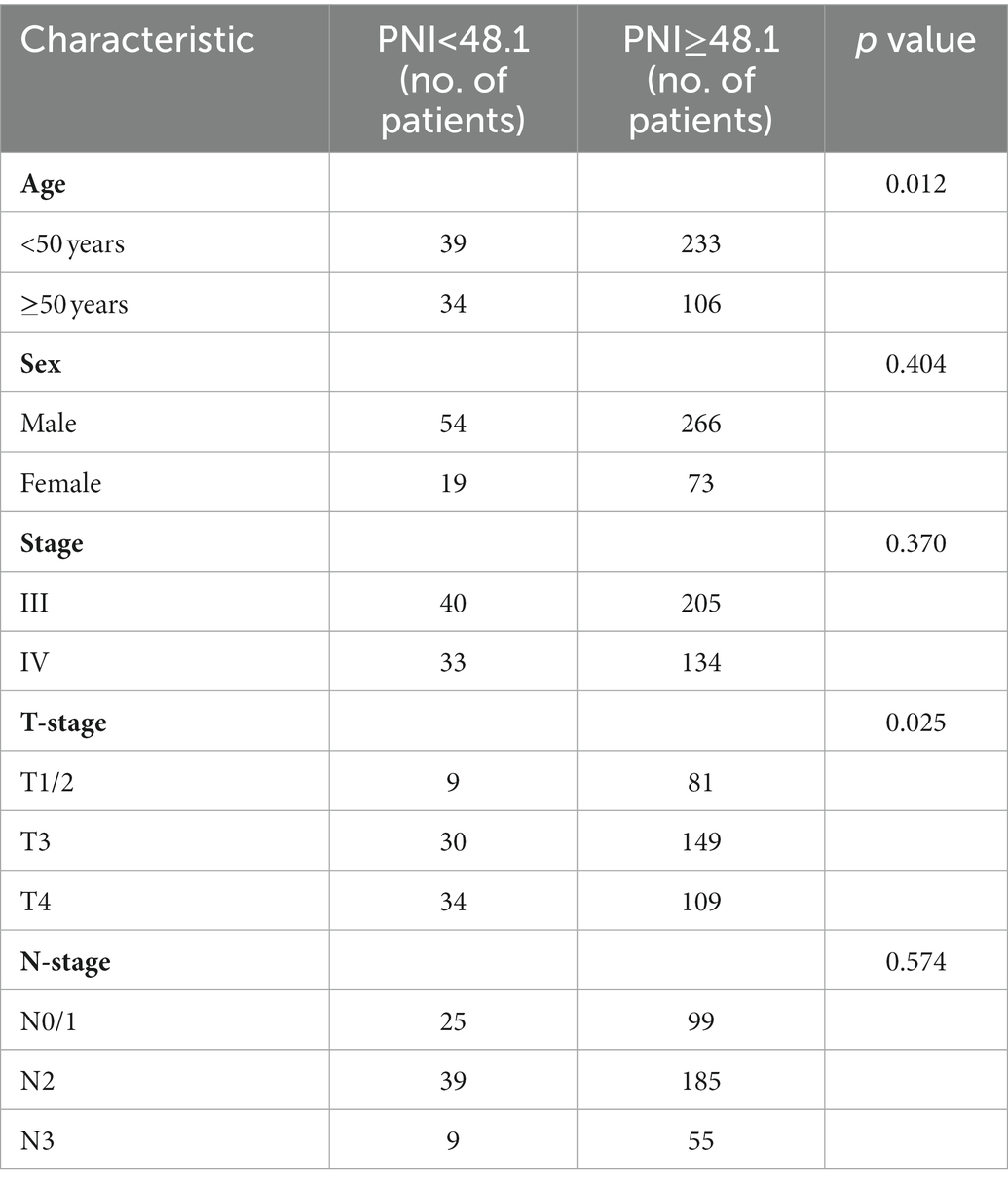
Table 2. Baseline characteristics of patients grouped by PNI.
In the univariate analysis, age (p < 0.001), T-stage (p < 0.001), tumor stage (p < 0.001), N stage (p = 0.011), PNI (p = 0.001), NLR (p = 0.002), and LDH (p = 0.009) were significantly associated with OS. Age (p = 0.001), T-stage (p < 0.001), tumor stage (p < 0.001), N-stage (p = 0.011), PNI (p = 0.003), NLR (p = 0.051), and LDH (p = 0.03) were significantly associated with PFS. In the multivariate analysis, age (p < 0.001), T-stage (p < 0.001), N-stage (p = 0.020), PNI (p = 0.006), and LDH (p = 0.032) were significantly associated with OS. Age (p = 0.004), T-stage (<0.001), N-stage (<0.001), PNI (p = 0.022) were significantly associated with PFS (Tables 3, 4). PNI was an independent prognostic factor for both OS and PFS in nasopharyngeal carcinoma patients (Figures 3, 4).
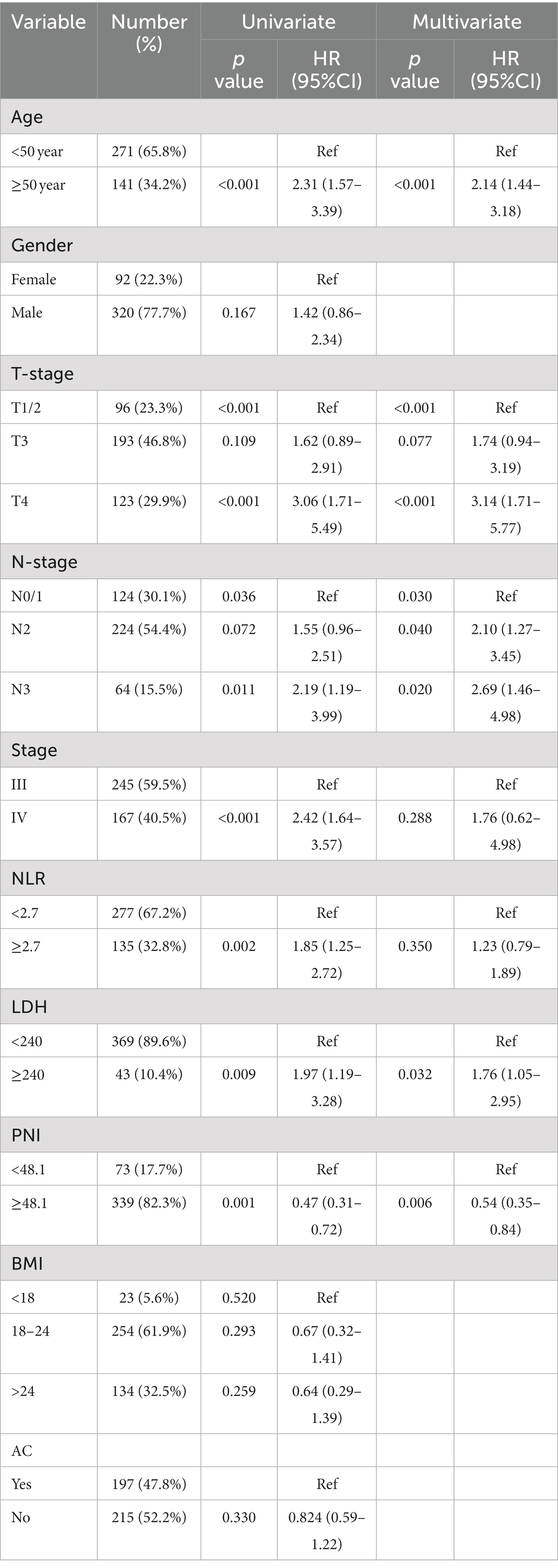
Table 3. Identification of risk factors of overall survival (OS) by univariate and multivariate Cox models.
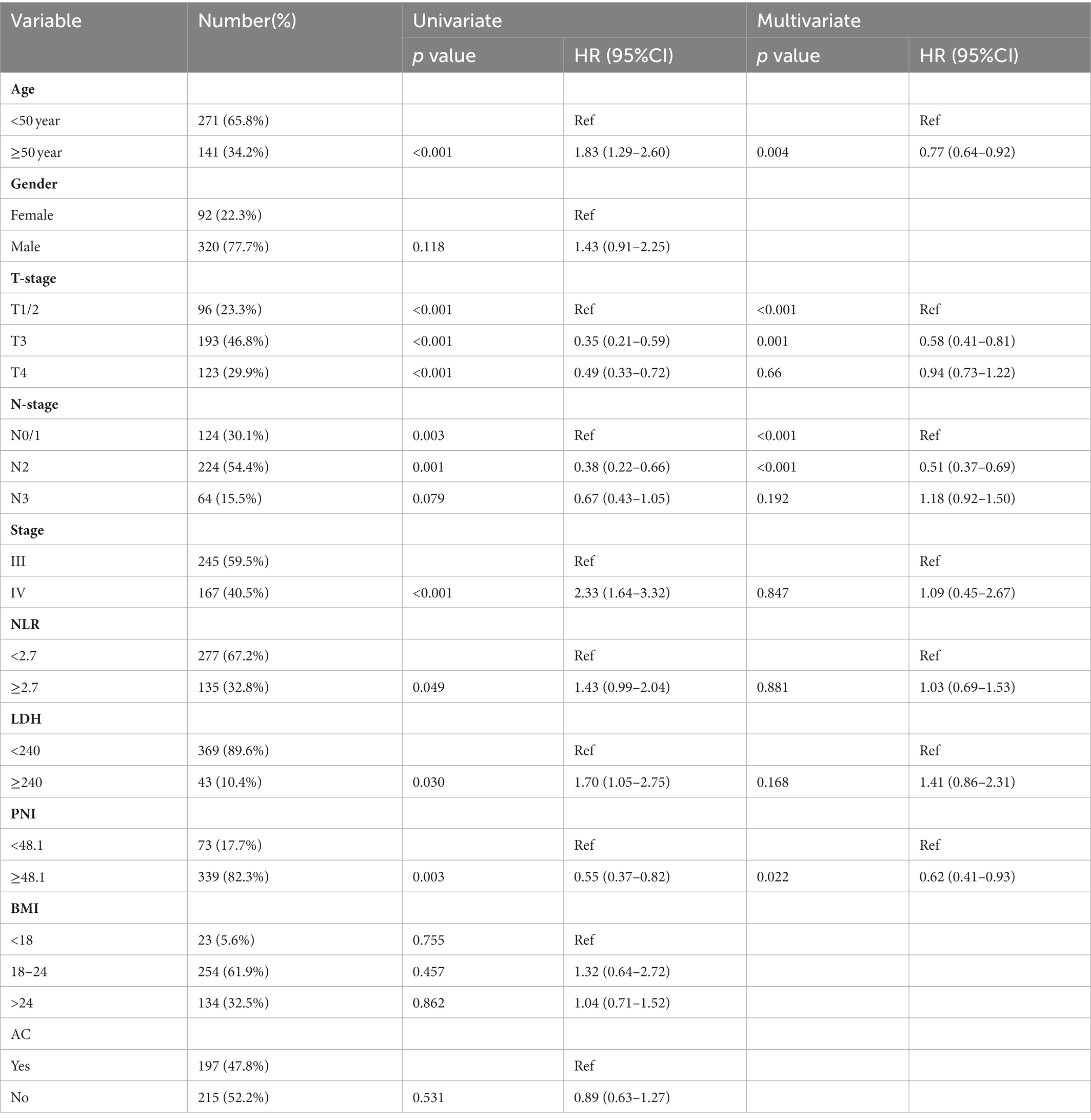
Table 4. Identification of risk factors of PFS by univariate Cox models and multivariate Cox models.
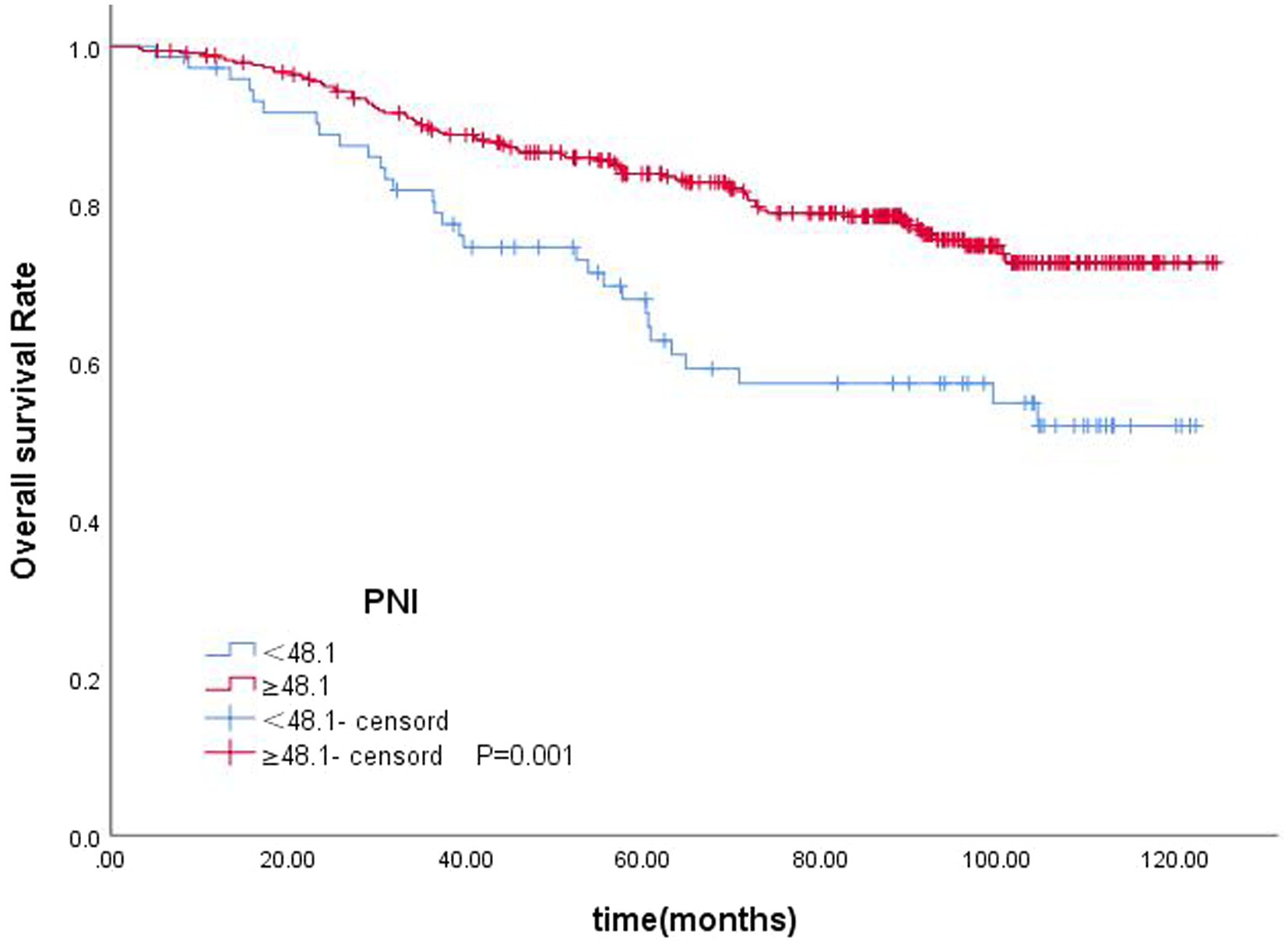
Figure 3. Kaplan–Meier curves for OS according to PNI.
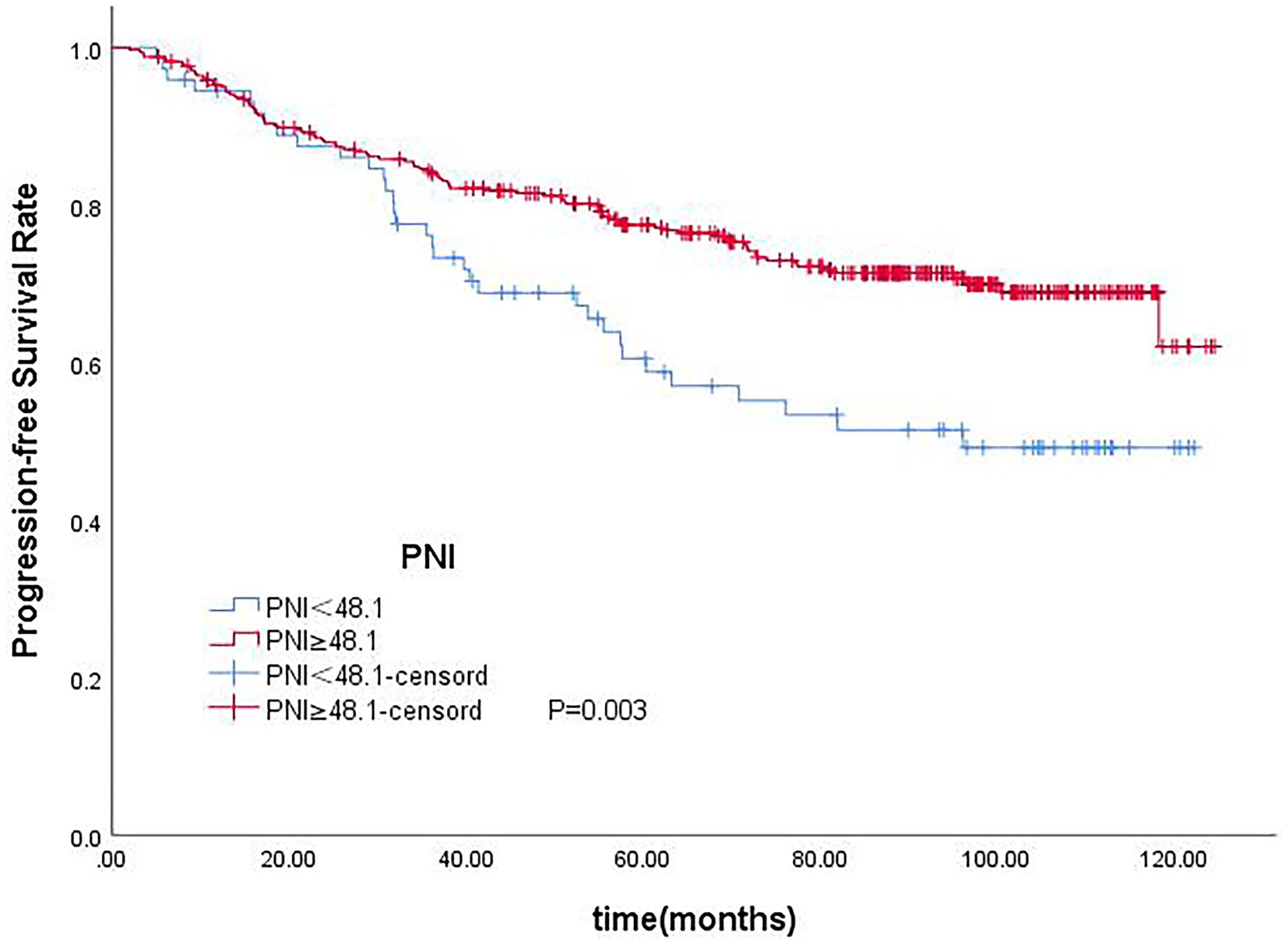
Figure 4. Kaplan–Meier curves for PFS according to PNI.
Based on the results of the multivariate analysis, a nomogram was constructed for predicting OS by the ‘survival’ and ‘rms’ packages in R 4.1.2 (Figure 5). Each variable subtype was assigned a score based on a score table. To predict the 3-and 5-year OS, we summed the scores for each variable, obtained an overall score, and calculated the overall survival. The C-index of the nomogram was 0.702 (95% confidence interval [CI], 0.653–0.751). The Akaike information criterion (AIC) value of the nomogram for OS was 1142.538. Excellent agreement was observed in the calibration graphs between the nomogram-predicted probabilities and actual observations of the 5-year OS (Figure 6). To confirm the accuracy of the nomogram in the validation cohort, the C-index and calibration slope were applied. The C-index was 0.719 (95% CI, 0.580–0.858). The calibration curves for the validation cohort showed optimal agreement between the actual observations and the nomogram prediction of 5-year OS (Figure 7).
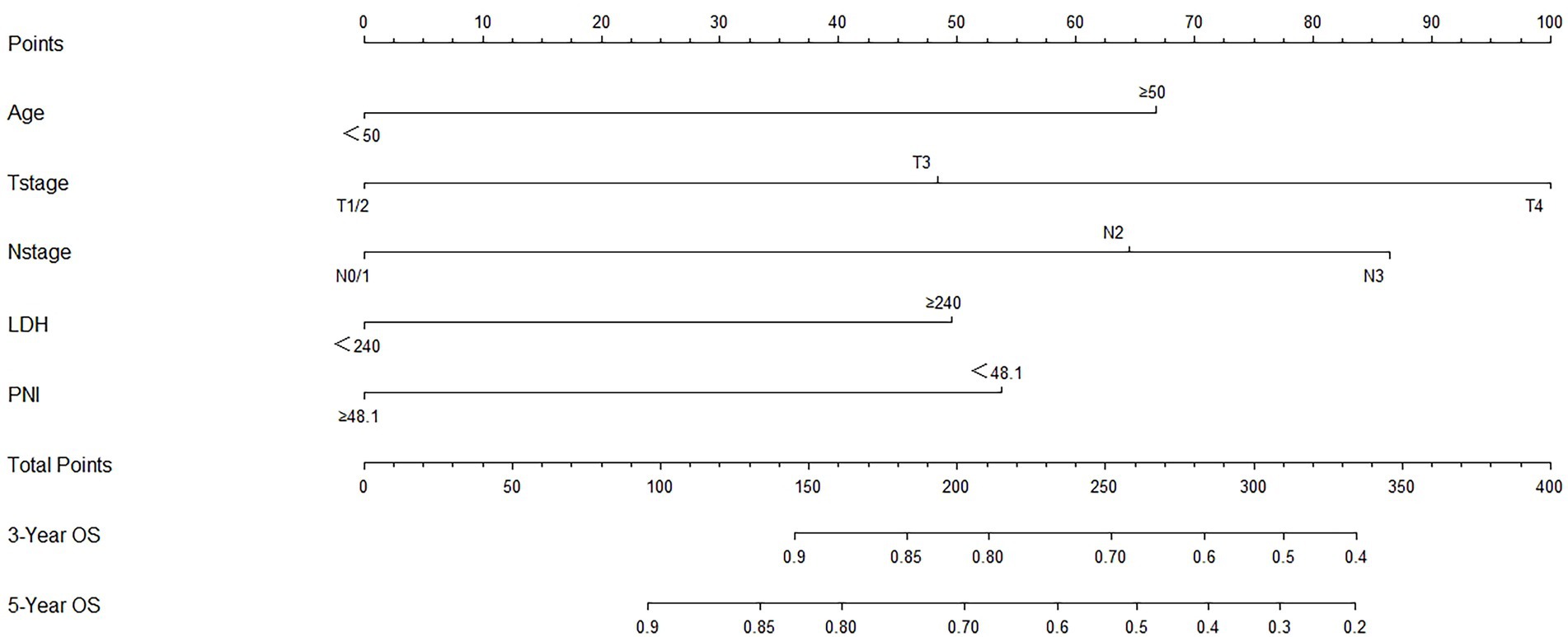
Figure 5. Prognostic nomogram of survival probabilities at 3- and 5-year in patients with nasopharyngeal carcinoma (NPC).
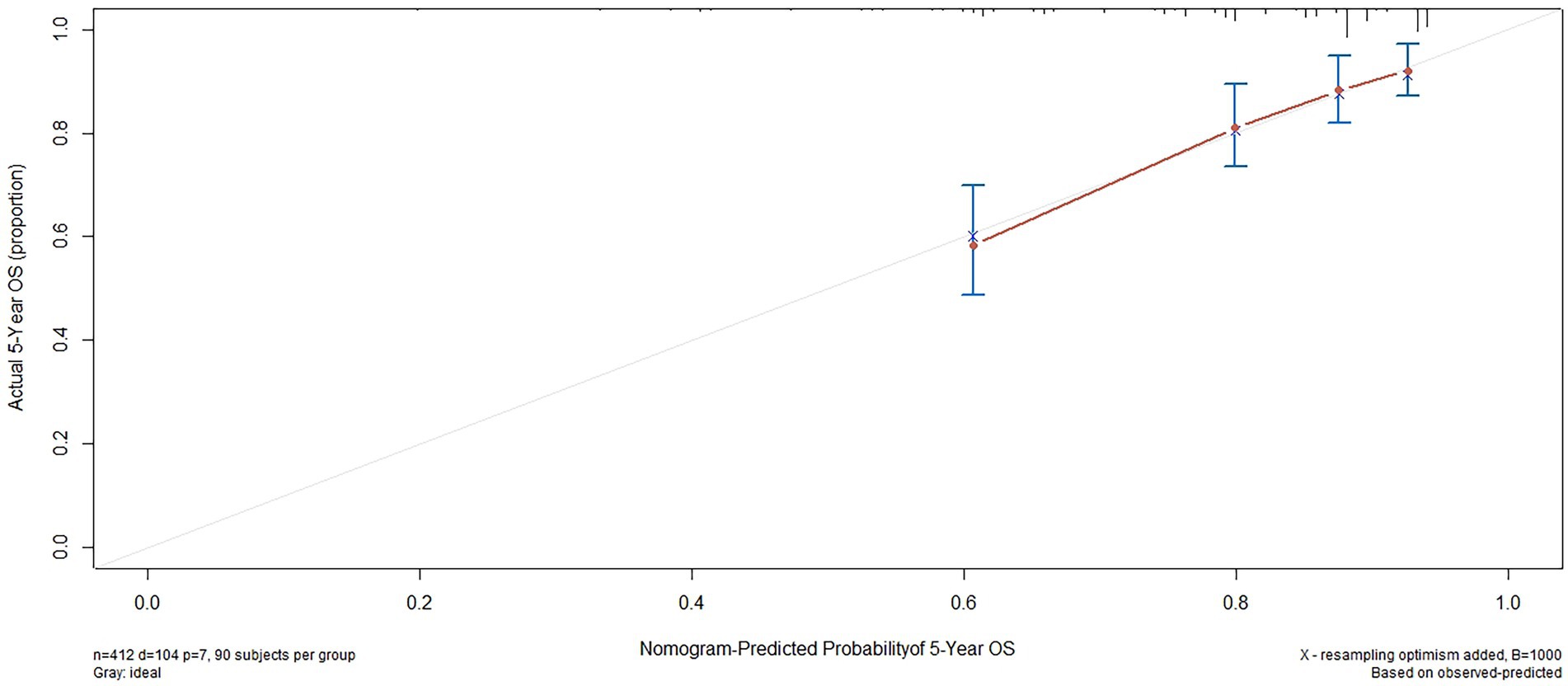
Figure 6. Calibration plots of survival probabilities at 5-year in patients with NPC.
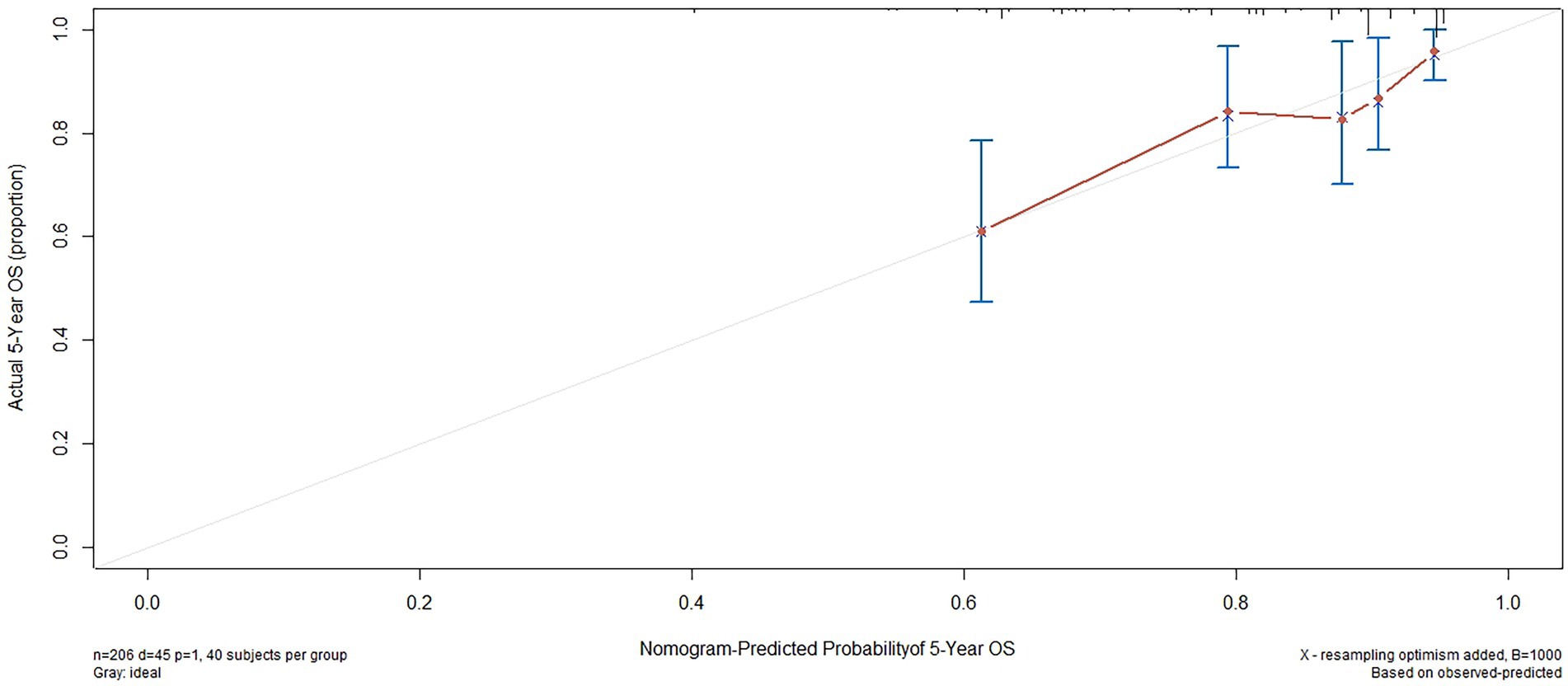
Figure 7. External validation of the nomogram to predict 5-year OS likelihoods in patients with NPC in the validation cohort.
We compared the accuracy of the prediction of 5-year OS between the nomogram and the TNM staging system. The C-index and AIC of the TNM staging system were 0.647 (95% CI, 0.594–0.70) and 1163.698, respectively, while those for the nomogram were 0.702 and 1142.538, respectively. Furthermore, the results of the DCA and time-dependent ROC analysis also indicated a higher net benefit of the clinical application of the nomogram in predicting OS compared to the 8th edition of the TNM staging system (Figures 8–11).
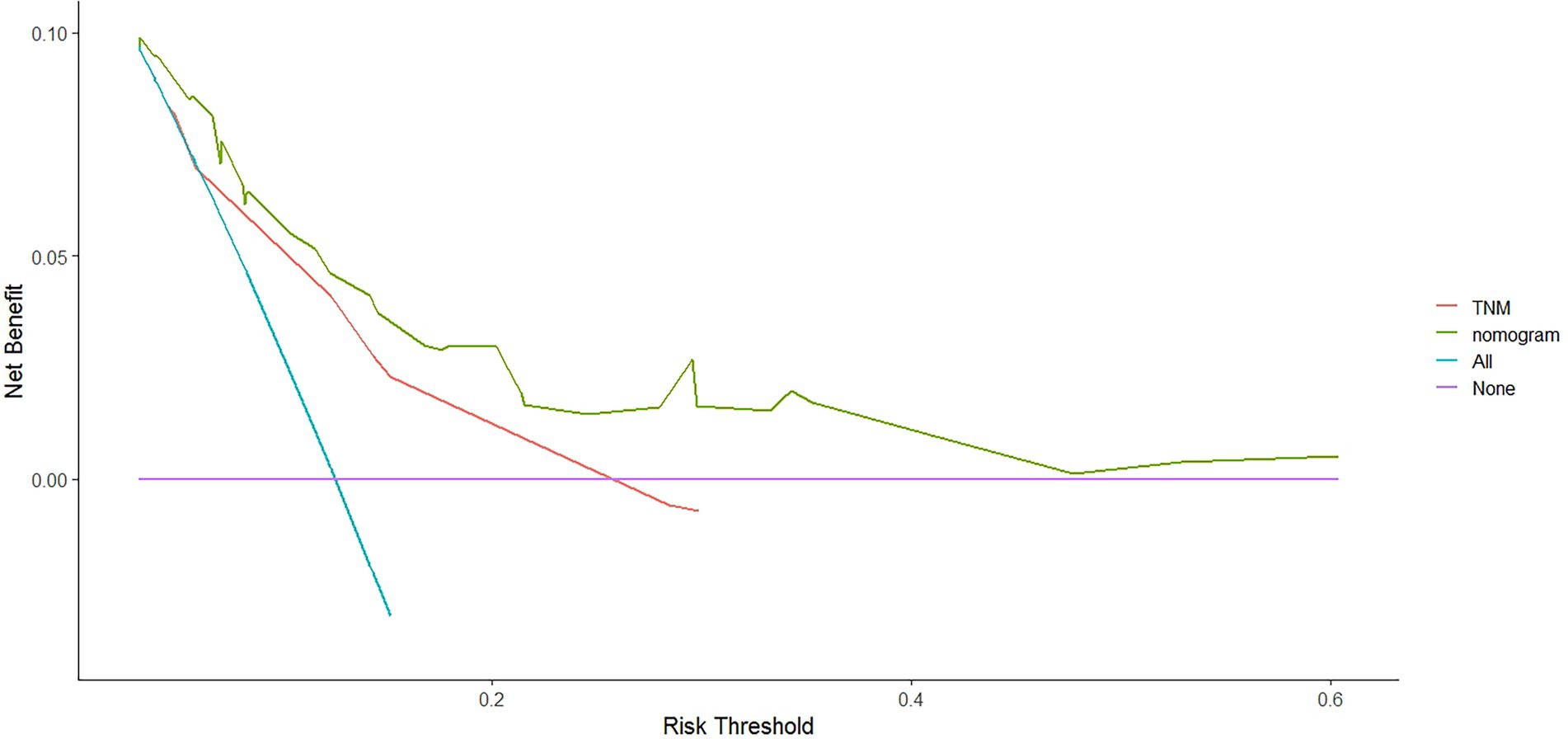
Figure 8. The decision curves (DCA) of OS at 3-year by the nomogram and the TNM staging system.
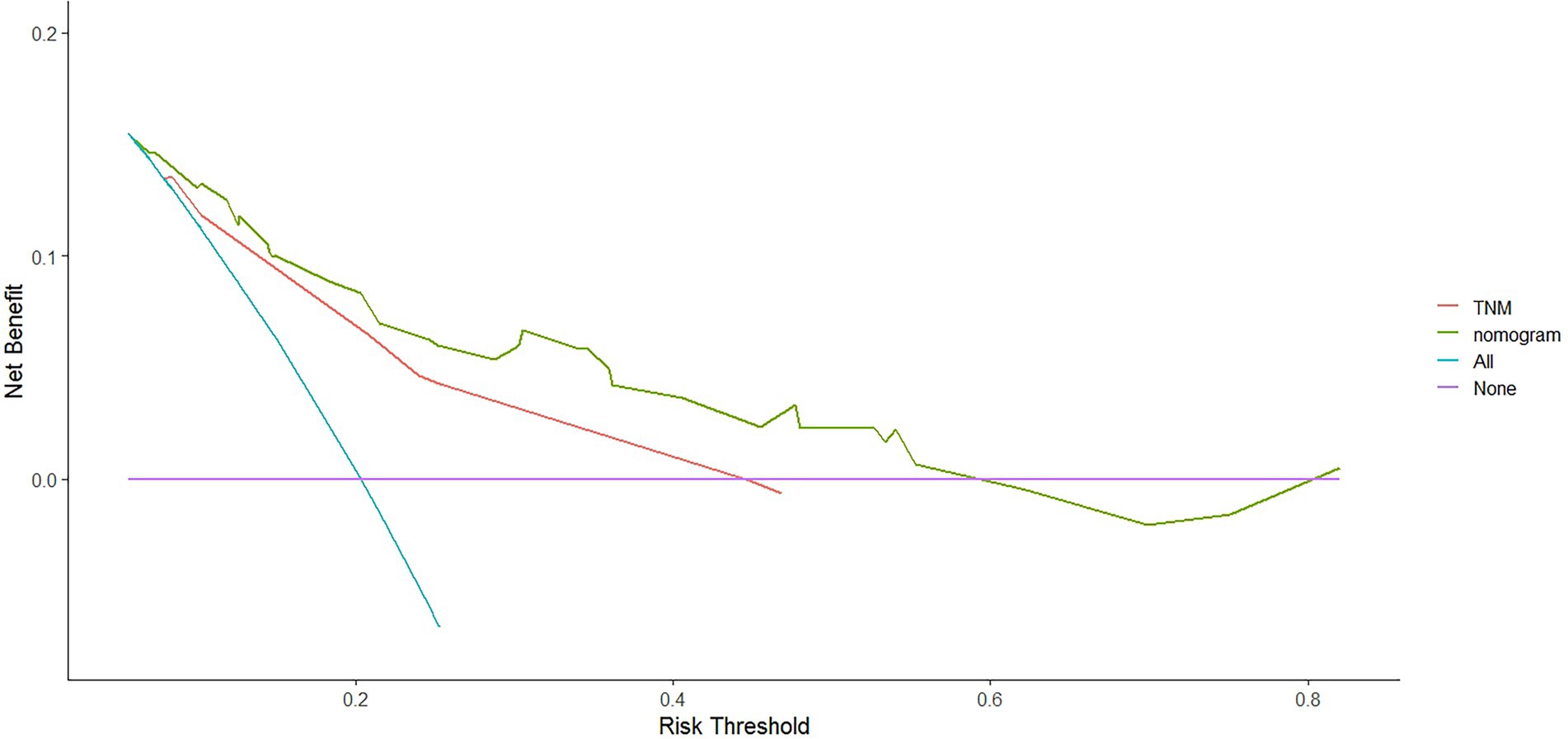
Figure 9. The decision curves (DCA) of OS at 5-year by the nomogram and the TNM staging system.
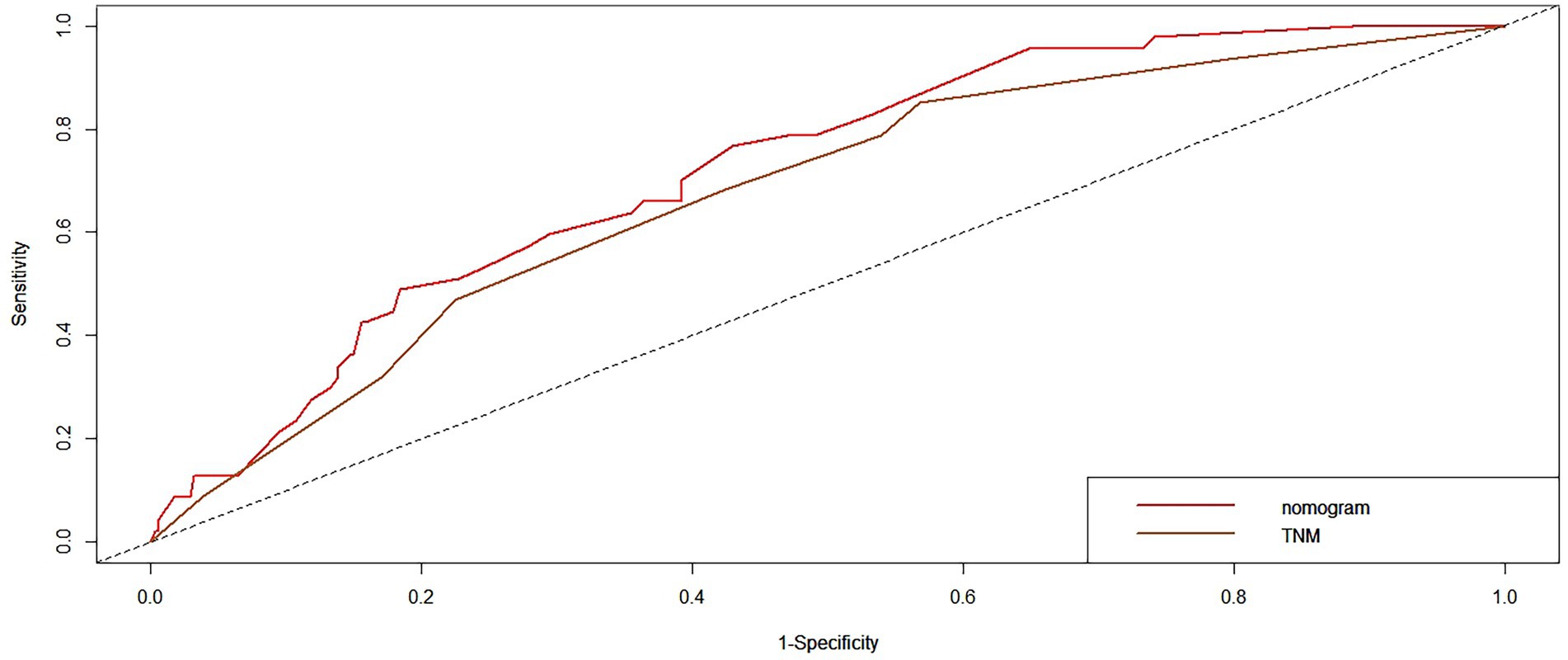
Figure 10. The time-dependent receiver operating characteristic (ROC) curves of OS at 3-year by the nomogram and the TNM staging system.
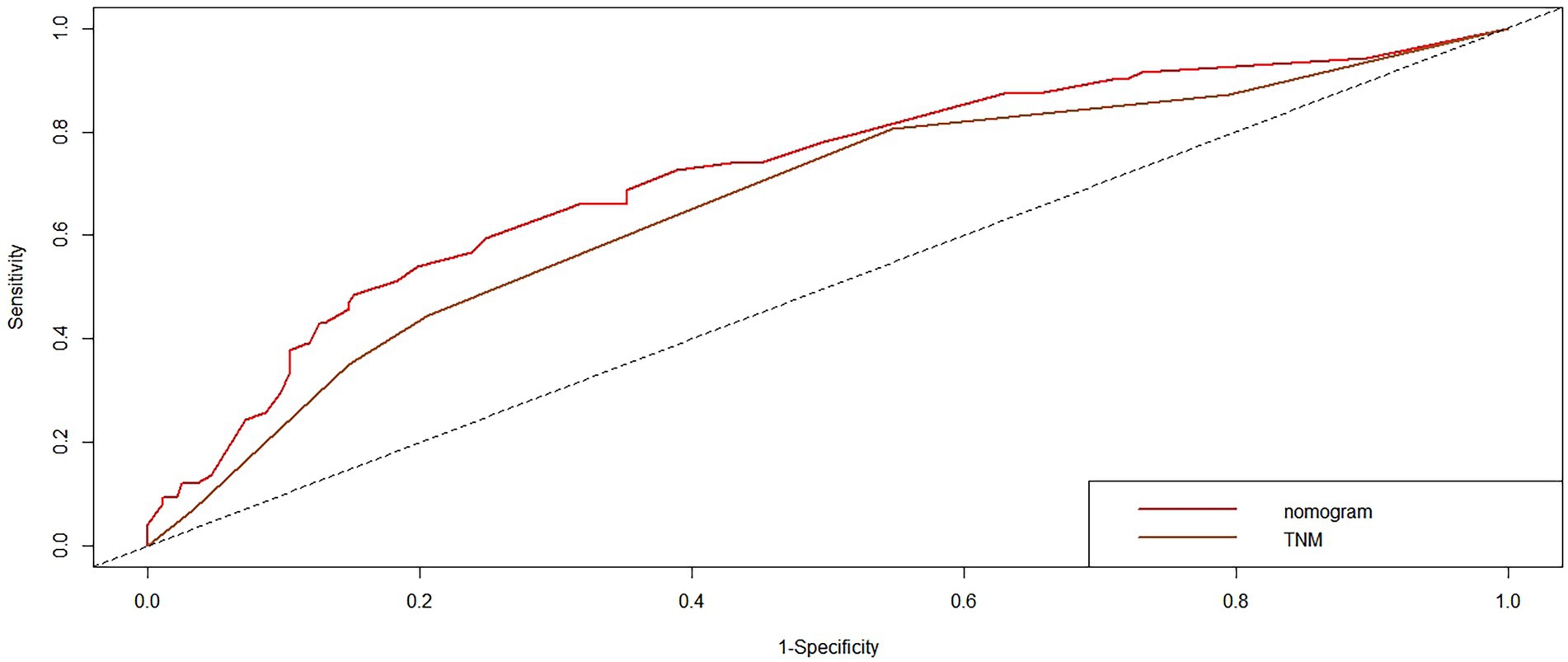
Figure 11. The time-dependent ROC curves of OS at 5-year by the nomogram and the TNM staging system.
Previously, tumor progression was thought to be related to genetic background. An increasing number of studies have demonstrated the key role of inflammation in tumor cell survival and proliferation, novel angiogenesis, apoptosis resistance, immune evasion, metastasis to distant regions and metastasis, and therapy resistance (23). Moreover, some studies have demonstrated that nutritional status plays a decisive role in tumorigenesis and progression. Therefore, the effects of inflammation and nutrition in patients with cancer, including diffuse large B-cell lymphoma (15), osteosarcoma (24) and pancreatic cancer (25).
We collected data on pre-treatment systemic inflammatory and nutritional markers (including BMI, PNI, and NLR) in patients with NPC to examine their clinical and prognostic value and to compare their predictive accuracy. To our knowledge, this is the first study to investigate the prognostic value of inflammatory and nutritional indicators in patients with NPC based on the 8th edition of the AJCC staging system. Our results showed that pre-treatment PNI and NLR had a significant impact on survival in patients with NPC. To effectively distinguish the two prognostic groups, we identified an optimal PNI cutoff point of 48.1. This value was comparable to those reported previously (26–28). Miao et al. (16) suggested that the PNI is an independent reliable prognostic factor in patients with NPC undergoing IMRT. In patients with stage II–IVb disease and PNI ≤ 52.0, CCRT alone did not provide satisfactory results, and additional treatments were required. That study was based on the 7th edition of the UICC/AJCC staging system. However, the 8th edition of the AJCC staging system for NPC has been released and is now widely used. Wei et al. (17) also observed a significantly lower OS in patients with a high PNI (>51) compared to that in patients with metastatic NPC. In their propensity score-matched analysis, Lin (29) confirmed that patients with non-metastatic NPC with PNI <51 were more likely to develop distant metastases. However, that study used the 7th edition of the AJCC/UICC TNM system for clinical staging and did not provide a detailed description of the radiotherapy technology.
Clinicians evaluate prognosis according to the TNM stage and then choose from among therapeutic options. Therefore, accurate staging is important. Although many studies have confirmed that the 7th edition staging system of NPC accurately predicts survival prognosis, and it has been widely internationally adopted (30, 31), this edition has ambiguous definitions that lead to challenges in clinical practice (32, 33). This version of the staging system is primarily based on studies using traditional 2D/3D techniques. However, the widespread use of IMRT and MRI have allowed significant improvements in the survival of patients with NPC, making the 7th edition outdated. Fortunately, these limitations improved in the 8th edition. To our knowledge, this is the first study on the prognosis of PNI in patients with NPC undergoing CCRT with or without AC based on the 8th staging system.
Recent studies have increasingly focused on the effect of nutrition and immune status on the prognosis of patients with cancer (8, 9, 11, 34). The value of NLR in the prognosis of NPC has been supported by many reviews (35–37). The prognostic value of PNI has also been demonstrated in various malignancies (10, 11, 25, 38). However, few studies have determined which prediction value is greater. Lin (29) reported that the PNI had a better discriminatory ability for predicting 1-, 3-, and 5-year DMFS than other inflammatory scores. The results of the present study also showed better discernment of the PNI in predicting the 5-year OS than the NLR. Several indicators of inflammation were included (NLR and PNI); however, only the PNI was an independent prognostic factor for locally advanced NPC. Therefore, the PNI may represent a novel prognostic factor for patients with NPC, which is based on inflammation and nutrition. PNI is an independent prognostic factor even in middle-aged and elderly patients with non-metastatic NPC (22). Although the pre-treatment PNI is an excellent prognostic marker for NPC patients, the post-treatment PNI is also an independent prognostic marker for OS. PNI dynamics are independent prognostic indicators for OS (21).
The PNI can predict tumor survival because (1) lymphocytes are the major component of participants in the immune response and play an important role in inhibiting tumor cell proliferation and metastasis (39). Lymphocyte counts represent the strength of the immune system; the lower the lymphocyte count, the weaker the systemic immunity. Thus, cancer cells easily evade immune surveillance, which augments their activity as cancer cells. (2) Serum albumin level is the most direct indicator of nutritional status in the human body. Albumin has been linked to tumor necrosis because pro-inflammatory cytokines reduce albumin production (38).
In this study, LDH was significantly associated with OS in univariate analysis (p = 0.032). These results are consistent with those previously reported. Xiong (40) observed that pretreatment PNI and LDH were not only statistically significantly associated with survival prognosis in patients with locally advanced NPC. Moreover, their combination, superior to individual scores, complemented the traditional TNM staging systems. The results of a meta-analysis of 18 studies, including 13,789 patients, suggested that high serum LDH levels are associated with worse outcomes in patients with NPC (41). Although numerous studies have confirmed the prognostic value of LDH, the molecular mechanisms linking LDH to distant metastasis remain unclear (42–44). Firstly, it is thought to be linked to glycolysis in cancer cells, which utilize different metabolic pathways than normal cells. Despite the presence of oxygen, cancer cells preferentially utilize the anaerobic glycolysis pathway to produce energy, a phenomenon histologically known as the Warburg effect (45). In anaerobic environments, LDH promotes the conversion of pyruvate to lactic acid, which plays a key role in anaerobic glycolysis. As large amounts of lactic acid are produced, adjusting LDH levels upward ensures efficient activity. Second, the immunosuppressive effect of lactic acidosis is strong enough to mediate tumor immune evasion (46). In addition, in many cases, tumor tissues show extensive cellular damage and release more extracellular enzymes than normal tissues, including LDH (47).
Numerous nomograms or prognostic models have been developed for NPC, but few clinicians have used them in the clinic. There are several reasons for this: (1) Some prognostic models incorporate indicators that are not routinely used in clinical practice, such as C-reactive protein (CRP) (48), high-sensitivity-CRP (hs-CRP) (49), and positron emission tomography (PET)/CT (50), and have limitations in clinical promotion. (2) Some models are based on previous old staging systems (51), such as the UICC2002 TNM stage system, and the latest edition staging system has been widely adopted in clinical practice. (3) Some prognostic models include patients treated with mixed radiotherapy techniques, including intensity-modulated and two-dimensional radiotherapy techniques (48, 49). (4) Some models have not been externally validated (52). Formally, because current prognostic models are more or less flawed, new prognostic models are constantly being developed to improve and modify them. The search is ongoing for the best and most clinically applicable models that can be widely used. We constructed a nomogram based on inflammatory biomarkers and nutritional indicators (53), including Epstein–Barr virus (EBV)-DNA. However, this is not a routine screening program in some centers, and not all patients have these data available, particularly in some basic hospitals. Furthermore, differences in the standards for EBV-DNA assays. All these factors have limited clinical applications. Therefore, we combined the factors identified in this study (age, PNI, and LDH) to develop and validate a nomogram to predict OS in patients with NPC that is more practical in the clinical setting. The nomogram showed a more accurate prognostic capability compared to the conventional TNM staging system, which is anatomically informative and does not consider tumor heterogeneity. The individualized stratification and precise treatment of tumors have some deficiencies. We used the C-index and AUC to compare the accuracy of nomogram and TNM staging system predictions. The nomogram and TNM staging system had C-indices of 0.702 and 0.647, respectively. The nomogram had a higher AUC than that of the TNM staging system. In addition to the C-index and AUC, we used AIC and DCA to compare the two models. The lower the AIC, the higher the discriminatory ability of the model. In our study, the nomogram was associated with a lower corrected AIC (1142.54) compared to the TNM staging system (1163.70). Moreover, the results of the decision curve analysis showed that the nomogram had a higher net benefit in predicting OS clinical utilization compared to the 8th edition TNM staging system. Thus, our results demonstrate the better prediction accuracy of the nomogram.
The present investigation has several limitations. First, this retrospective study was conducted at a single center. Second, we could not examine other markers such as EBV-DNA and CRP. Moreover, because the related data were insufficient or inappropriate, we were unable to analyze them. Although plasma EBV-DNA is an important marker of survival and has been confirmed in numerous studies (54–56), the current use of plasma EBV-DNA has some limitations. (1) Not all patients with pathologically confirmed NPC have detectable plasma EBV-DNA; moreover, studies have shown that even in endemic areas, plasma EBV-DNA is still undetectable in 12–29% of confirmed cases at initial diagnosis (57–59). (2) Owing to the wide variation in copy number determined by quantitative assays of EBV-DNA in plasma performed in different clinical laboratories, there remains no consistent standard or standardized method of analysis. The EBV-DNA copy number is highly variable between laboratories, and there remains no uniform standard. (3) The lowest detection limit also varies widely among different institutions, resulting in variations in false-negative rates and recommended cutoff values. Only 28.4% of the journal articles clearly stated the lower detection limit of their EBV-DNA assays, ranging from 0 to 1,000 copies/ml (60). The recommended cut-off value for classifying patients into different risk groups varies considerably, from 500 to 4,000 copies/ml (61, 62). Thus, there is a need for the standardization of EBV-DNA serological assays to allow the comparison of results between different laboratories and populations in different translational studies (63). Third, this study only explored the relationship between PNI and prognosis at a single pre-treatment time point and did not address the relationship between PNI kinetics and prognosis. Finally, validation in a single institution has certain limitations; therefore, validation in external and prospective populations is required.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
This study was approved by the Ethics Committee of Guangxi Medical University Cancer Hospital (LW2022029), in compliance with the Declaration of Helsinki. The patients/participants provided their written informed consent to participate in this study.
Y-MJ and X-DZ studied conception and design. Y-MJ, X-BP, and J-LM: data acquisition. X-BP and S-TH: data analysis and interpretation. S-TH and J-LM: quality control of data and algorithms. Y-MJ: manuscript writing. X-BP, S-TH, and X-DZ: manuscript reviewing and approving. All authors contributed to the article and approved the submitted version.
This work was supported by the Health Commission of Guangxi Zhuang Autonomous Region (no. Z-A20220684).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1.Chen, YP, Chan, ATC, Le, QT, Blanchard, P, Sun, Y, and Ma, J. Nasopharyngeal carcinoma. Lancet. (2019) 394:64–80. doi: 10.1016/S0140-6736(19)30956-0
2.Peng, G, Wang, T, Yang, KY, Zhang, S, Zhang, T, Li, Q, et al. A prospective, randomized study comparing outcomes and toxicities of intensity-modulated radiotherapy vs. conventional two-dimensional radiotherapy for the treatment of nasopharyngeal carcinoma. Radiother Oncol. (2012) 104:286–93. doi: 10.1016/j.radonc.2012.08.013
3.Cedrés, S, Torrejon, D, Martínez, A, Martinez, P, Navarro, A, Zamora, E, et al. Neutrophil to lymphocyte ratio (NLR) as an indicator of poor prognosis in stage IV non-small cell lung cancer. Clin Transl Oncol. (2012) 14:864–9. doi: 10.1007/s12094-012-0872-5
4.Xia, WK, Liu, ZL, Shen, D, Lin, QF, Su, J, and Mao, WD. Prognostic performance of pre-treatment NLR and PLR in patients suffering from osteosarcoma. World J Surg Oncol. (2016) 14:127. doi: 10.1186/s12957-016-0889-2
5.Diem, S, Schmid, S, Krapf, M, Flatz, L, Born, D, Jochum, W, et al. Neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR) as prognostic markers in patients with non-small cell lung cancer (NSCLC) treated with nivolumab. Lung Cancer. (2017) 111:176–81. doi: 10.1016/j.lungcan.2017.07.024
6.Trinh, H, Dzul, SP, Hyder, J, Jang, H, Kim, S, Flowers, J, et al. Prognostic value of changes in neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR) and lymphocyte-to-monocyte ratio (LMR) for patients with cervical cancer undergoing definitive chemoradiotherapy (dCRT). Clin Chim Acta. (2020) 510:711–6. doi: 10.1016/j.cca.2020.09.008
7.Hu, C, Bai, Y, Li, J, Zhang, G, Yang, L, Bi, C, et al. Prognostic value of systemic inflammatory factors NLR, LMR, PLR and LDH in penile cancer. BMC Urol. (2020) 20:57. doi: 10.1186/s12894-020-00628-z
8.Sun, K, Chen, S, Xu, J, Li, G, and He, Y. The prognostic significance of the prognostic nutritional index in cancer: a systematic review and meta-analysis. J Cancer Res Clin Oncol. (2014) 140:1537–49. doi: 10.1007/s00432-014-1714-3
9.Pastore, CA, Orlandi, SP, and Gonzalez, MC. The inflammatory-nutritional index; assessing nutritional status and prognosis in gastrointestinal and lung cancer patients. Nutr Hosp. (2014) 29:629–34. doi: 10.3305/nh.2014.29.3.7195
10.Buzby, GP, Mullen, JL, Matthews, DC, Hobbs, CL, and Rosato, EF. Prognostic nutritional index in gastrointestinal surgery. Am J Surg. (1980) 139:160–7. doi: 10.1016/0002-9610(80)90246-9
11.Okadome, K, Baba, Y, Yagi, T, Kiyozumi, Y, Ishimoto, T, Iwatsuki, M, et al. Prognostic nutritional index, tumor-infiltrating lymphocytes, and prognosis in patients with esophageal cancer. Ann Surg. (2020) 271:693–700. doi: 10.1097/SLA.0000000000002985
12.Lien, YC, Hsieh, CC, Wu, YC, Hsu, HS, Hsu, WH, Wang, LS, et al. Preoperative serum albumin level is a prognostic indicator for adenocarcinoma of the gastric cardia. J Gastrointest Surg. (2004) 8:1041–8. doi: 10.1016/j.gassur.2004.09.033
13.Nakatani, M, Migita, K, Matsumoto, S, Wakatsuki, K, Ito, M, Nakade, H, et al. Prognostic significance of the prognostic nutritional index in patients with recurrent esophageal squamous cell carcinoma. Nutr Cancer. (2018) 70:467–73. doi: 10.1080/01635581.2018.1445771
14.Ida, N, Nakamura, K, Saijo, M, Kusumoto, T, and Masuyama, H. Prognostic nutritional index as a predictor of survival in patients with recurrent cervical cancer. Mol. Clin. Oncol. (2018) 8:257–63. doi: 10.3892/mco.2017.1508
15.Shen, Z, Wang, F, He, C, Li, D, Nie, S, Bian, Z, et al. The value of prognostic nutritional index (PNI) on newly diagnosed diffuse large B-cell lymphoma patients: a multicenter retrospective study of HHLWG based on propensity score matched analysis. J Inflamm Res. (2021) 14:5513–22. doi: 10.2147/JIR.S340822
16.Miao, J, Xiao, W, Wang, L, Han, F, Wu, H, Deng, X, et al. The value of the prognostic nutritional index (PNI) in predicting outcomes and guiding the treatment strategy of nasopharyngeal carcinoma (NPC) patients receiving intensity-modulated radiotherapy (IMRT) with or without chemotherapy. J Cancer Res Clin Oncol. (2017) 143:1263–73. doi: 10.1007/s00432-017-2360-3
17.Wei, G-B, Lu, Y-Y, Liao, R-W, Chen, Q-S, and Zhang, K-Q. Prognostic nutritional index predicts prognosis in patients with metastatic nasopharyngeal carcinoma. Onco Targets Ther. (2016) 9:5955–61. doi: 10.2147/OTT.S114382
18.Camp, RL, Dolled-Filhart, M, and Rimm, DL. X-tile: a new bio-informatics tool for biomarker assessment and outcome-based cut-point optimization. Clin. Cancer Res. (2004) 10:7252–9. doi: 10.1158/1078-0432.CCR-04-0713
19.Peng, R-R, Liang, Z-G, Chen, K-H, Li, L, Qu, S, and Zhu, X-D. Nomogram based on lactate dehydrogenase-to-albumin ratio (LAR) and platelet-to-lymphocyte ratio (PLR) for predicting survival in nasopharyngeal carcinoma. J Inflamm Res. (2021) 14:4019–33. doi: 10.2147/JIR.S322475
20.Huang, L, Sim, AYL, Wu, Y, Liang, Z, Li, K, Du, Y, et al. Lactate dehydrogenase kinetics predict chemotherapy response in recurrent metastatic nasopharyngeal carcinoma. Ther. Adv. Med. Oncol. (2020) 12:175883592097005. doi: 10.1177/1758835920970050
21.Kucukarda, A, Erdogan, B, Gokyer, A, Sayin, S, Gokmen, I, Ozcan, E, et al. Prognostic nutritional index and its dynamics after curative treatment are independent prognostic factors on survival in non-metastatic nasopharyngeal carcinoma. Support Care Cancer. (2022) 30:2131–9. doi: 10.1007/s00520-021-06627-6
22.Wu, B, Ni, LQ, Wang, Y, Yang, HH, and Zhao, SK. Low prognostic nutritional index is associated with poor outcome in middle-aged and elderly patients with non-metastatic nasopharyngeal carcinoma: a retrospective cohort study. Support Care Cancer. (2022) 30:8895–904. doi: 10.1007/s00520-022-07286-x
23.Dougan, M, and Dranoff, G. Immune therapy for cancer. Annu Rev Immunol. (2009) 27:83–117. doi: 10.1146/annurev.immunol.021908.132544
24.Huang, X, Hu, H, Zhang, W, and Shao, Z. Prognostic value of prognostic nutritional index and systemic immune-inflammation index in patients with osteosarcoma. J Cell Physiol. (2019) 234:18408–14. doi: 10.1002/jcp.28476
25.Geng, Y, Qi, Q, Sun, M, Chen, H, Wang, P, and Chen, Z. Prognostic nutritional index predicts survival and correlates with systemic inflammatory response in advanced pancreatic cancer. Eur J Surg Oncol. (2015) 41:1508–14. doi: 10.1016/j.ejso.2015.07.022
26.Topkan, E, Yucel Ekici, N, Ozdemir, Y, Besen, AA, Mertsoylu, H, Sezer, A, et al. Baseline low prognostic nutritional index predicts poor survival in locally advanced nasopharyngeal carcinomas treated with radical concurrent chemoradiotherapy. Ear Nose Throat J. (2021) 100:Np69–np76. doi: 10.1177/0145561319856327
27.Du, X-J, Tang, L-L, Mao, Y-P, Guo, R, Sun, Y, Lin, A-H, et al. Value of the prognostic nutritional index and weight loss in predicting metastasis and long-term mortality in nasopharyngeal carcinoma. J Transl Med. (2015) 13:364. doi: 10.1186/s12967-015-0729-0
28.Oei, RW, Ye, L, Kong, F, Du, C, Zhai, R, Xu, T, et al. Prognostic value of inflammation-based prognostic index in patients with nasopharyngeal carcinoma: a propensity score matching study. Cancer Manag Res. (2018) 10:2785–97. doi: 10.2147/CMAR.S171239
29.Williams, BO, Yang, L, Xia, L, Wang, Y, Hong, S, Chen, H, et al. Low prognostic nutritional index (PNI) predicts unfavorable distant metastasis-free survival in nasopharyngeal carcinoma: a propensity score-matched analysis. PLoS One. (2016) 11:e0158853. doi: 10.1371/journal.pone.0158853
30.Pan, J, Xu, Y, Qiu, S, Zong, J, Guo, Q, Zhang, Y, et al. A comparison between the Chinese 2008 and the 7th edition AJCC staging systems for nasopharyngeal carcinoma. Am J Clin Oncol. (2015) 38:189–96. doi: 10.1097/COC.0b013e31828f5c96
31.Chen, L, Mao, YP, Xie, FY, Liu, LZ, Sun, Y, Tian, L, et al. The seventh edition of the UICC/AJCC staging system for nasopharyngeal carcinoma is prognostically useful for patients treated with intensity-modulated radiotherapy from an endemic area in China. Radiother Oncol. (2012) 104:331–7. doi: 10.1016/j.radonc.2011.10.009
32.Yue, D, Xu, YF, Zhang, F, Lin, L, Mao, YP, Li, WF, et al. Is replacement of the supraclavicular fossa with the lower level classification based on magnetic resonance imaging beneficial in nasopharyngeal carcinoma? Radiother Oncol. (2014) 113:108–14. doi: 10.1016/j.radonc.2014.08.036
33.Sze, H, Chan, LL, Ng, WT, Hung, AW, Lee, MC, Chang, AT, et al. Should all nasopharyngeal carcinoma with masticator space involvement be staged as T4? Oral Oncol. (2014) 50:1188–95. doi: 10.1016/j.oraloncology.2014.09.001
34.Shen, LJ, Chen, C, Li, BF, Gao, J, and Xia, YF. High weight loss during radiation treatment changes the prognosis in under−/normal weight nasopharyngeal carcinoma patients for the worse: a retrospective analysis of 2433 cases. PLoS One. (2013) 8:e68660. doi: 10.1371/journal.pone.0068660
35.Su, L, Zhang, M, Zhang, W, Cai, C, and Hong, J. Pretreatment hematologic markers as prognostic factors in patients with nasopharyngeal carcinoma: a systematic review and meta-analysis. Medicine (Baltimore). (2017) 96:e6364. doi: 10.1097/MD.0000000000006364
36.Takenaka, Y, Kitamura, T, Oya, R, Ashida, N, Shimizu, K, Takemura, K, et al. Prognostic role of neutrophil-lymphocyte ratio in nasopharyngeal carcinoma: a meta-analysis. PLoS One. (2017) 12:e0181478. doi: 10.1371/journal.pone.0181478
37.Yao, JJ, Zhu, FT, Dong, J, Liang, ZB, Yang, LW, Chen, SY, et al. Prognostic value of neutrophil-to-lymphocyte ratio in advanced nasopharyngeal carcinoma: a large institution-based cohort study from an endemic area. BMC Cancer. (2019) 19:37. doi: 10.1186/s12885-018-5236-2
38.Mohri, Y, Inoue, Y, Tanaka, K, Hiro, J, Uchida, K, and Kusunoki, M. Prognostic nutritional index predicts postoperative outcome in colorectal cancer. World J Surg. (2013) 37:2688–92. doi: 10.1007/s00268-013-2156-9
39.Hanahan, D, and Weinberg, RA. Hallmarks of cancer: the next generation. Cells. (2011) 144:646–74. doi: 10.1016/j.cell.2011.02.013
40.Xiong, Y, Shi, LL, Zhu, LS, and Peng, G. Prognostic value of pretreatment prognostic nutritional index and lactated dehydrogenase in locally advanced nasopharyngeal carcinoma patients. Ann. Palliat. Med. (2021) 10:4122–33. doi: 10.21037/apm-20-2033
41.Zhai, C, Gu, K, Zhai, X, Wang, J, and Zhang, J. Prognostic value of serum lactate dehydrogenase in patients with nasopharyngeal carcinoma: a meta-analysis. Clin Lab. (2017) 63:1777–85. doi: 10.7754/Clin.Lab.2017.170323
42.Mishra, D, and Banerjee, D. Lactate dehydrogenases as metabolic links between tumor and stroma in the tumor microenvironment. Cancers (Basel). (2019) 11:750. doi: 10.3390/cancers11060750
43.Cairns, RA, Harris, IS, and Mak, TW. Regulation of cancer cell metabolism. Nat Rev Cancer. (2011) 11:85–95. doi: 10.1038/nrc2981
44.Gallo, M, Sapio, L, Spina, A, Naviglio, D, Calogero, A, and Naviglio, S. Lactic dehydrogenase and cancer: an overview. Front Biosci (Landmark Ed). (2015) 20:1234–49. doi: 10.2741/4368
45.Liberti, MV, and Locasale, JW. The Warburg effect: how does it benefit cancer cells? Trends Biochem Sci. (2016) 41:211–8. doi: 10.1016/j.tibs.2015.12.001
46.Siska, PJ, Singer, K, Evert, K, Renner, K, and Kreutz, M. The immunological Warburg effect: can a metabolic-tumor-stroma score (MeTS) guide cancer immunotherapy? Immunol Rev. (2020) 295:187–202. doi: 10.1111/imr.12846
47.Certo, M, Tsai, CH, Pucino, V, Ho, PC, and Mauro, C. Lactate modulation of immune responses in inflammatory versus tumour microenvironments. Nat Rev Immunol. (2021) 21:151–61. doi: 10.1038/s41577-020-0406-2
48.Yang, L, Hong, S, Wang, Y, Chen, H, Liang, S, Peng, P, et al. Development and external validation of Nomograms for predicting survival in nasopharyngeal carcinoma patients after definitive radiotherapy. Sci Rep. (2015) 5:15638. doi: 10.1038/srep15638
49.Tang, LQ, Li, CF, Li, J, Chen, WH, Chen, QY, Yuan, LX, et al. Establishment and validation of prognostic Nomograms for endemic nasopharyngeal carcinoma. J Natl Cancer Inst. (2016) 108:djv291. doi: 10.1093/jnci/djv291
50.Peng, H, Dong, D, Fang, MJ, Li, L, Tang, LL, Chen, L, et al. Prognostic value of deep learning PET/CT-based Radiomics: potential role for future individual induction chemotherapy in advanced nasopharyngeal carcinoma. Clin. Cancer Res. (2019) 25:4271–9. doi: 10.1158/1078-0432.CCR-18-3065
51.Wu, S, Xia, B, Han, F, Xie, R, Song, T, Lu, L, et al. Prognostic Nomogram for patients with nasopharyngeal carcinoma after intensity-modulated radiotherapy. PLoS One. (2015) 10:e0134491. doi: 10.1371/journal.pone.0134491
52.Xia, WX, Zhang, HB, Shi, JL, Lu, X, Wang, L, Ye, YF, et al. A prognostic model predicts the risk of distant metastasis and death for patients with nasopharyngeal carcinoma based on pre-treatment serum C-reactive protein and N-classification. Eur J Cancer. (2013) 49:2152–60. doi: 10.1016/j.ejca.2013.03.003
53.Zhao, R, Liang, Z, Chen, K, and Zhu, X. Nomogram based on inflammatory biomarkers and nutritional indicators for predicting overall survival in Locoregionally advanced nasopharyngeal carcinoma. J Inflamm Res. (2022) 15:2971–81. doi: 10.2147/JIR.S366299
54.Liu, TB, Zheng, ZH, Pan, J, Pan, LL, and Chen, LH. Prognostic role of plasma Epstein-Barr virus DNA load for nasopharyngeal carcinoma: a meta-analysis. Clin Invest Med. (2017) 40:E1–e12. doi: 10.25011/cim.v40i1.28049
55.Song, Y, Xiao, H, Yang, Z, Geng, M, Ma, J, Ren, Y, et al. The predictive value of pre-and post-induction chemotherapy plasma EBV DNA level and tumor volume for the radiosensitivity of locally advanced nasopharyngeal carcinoma. EXCLI J. (2017) 16:1268–75. doi: 10.17179/excli2017-752
56.Liu, LT, Tang, LQ, Chen, QY, Zhang, L, Guo, SS, Guo, L, et al. Mai HQ the prognostic value of plasma Epstein-Barr viral DNA and tumor response to Neoadjuvant chemotherapy in advanced-stage nasopharyngeal carcinoma. Int J Radiat Oncol Biol Phys. (2015) 93:862–9. doi: 10.1016/j.ijrobp.2015.08.003
57.Kim, KY, Le, QT, Yom, SS, Ng, RHW, Chan, KCA, Bratman, SV, et al. Clinical utility of Epstein-Barr virus DNA testing in the treatment of nasopharyngeal carcinoma patients. Int J Radiat Oncol Biol Phys. (2017) 98:996–1001. doi: 10.1016/j.ijrobp.2017.03.018
58.Nicholls, JM, Lee, VH, Chan, SK, Tsang, KC, Choi, CW, Kwong, DL, et al. Negative plasma Epstein-Barr virus DNA nasopharyngeal carcinoma in an endemic region and its influence on liquid biopsy screening programmes. Br J Cancer. (2019) 121:690–8. doi: 10.1038/s41416-019-0575-6
59.Zoto Mustafayev, T, and Ozyar, E. In regard to Kim et al. Int J Radiat Oncol Biol Phys. (2017) 99:1306–7. doi: 10.1016/j.ijrobp.2017.08.034
60.Lee, AWM, Lee, VHF, Ng, WT, Strojan, P, Saba, NF, Rinaldo, A, et al. A systematic review and recommendations on the use of plasma EBV DNA for nasopharyngeal carcinoma. Eur J Cancer. (2021) 153:109–22. doi: 10.1016/j.ejca.2021.05.022
61.Lee, VH, Kwong, DL, Leung, TW, Choi, CW, O'Sullivan, B, Lam, KO, et al. The addition of pretreatment plasma Epstein-Barr virus DNA into the eighth edition of nasopharyngeal cancer TNM stage classification. Int J Cancer. (2019) 144:1713–22. doi: 10.1002/ijc.31856
62.Chan, AT, Lo, YM, Zee, B, Chan, LY, Ma, BB, Leung, SF, et al. Plasma Epstein-Barr virus DNA and residual disease after radiotherapy for undifferentiated nasopharyngeal carcinoma. J Natl Cancer Inst. (2002) 94:1614–9. doi: 10.1093/jnci/94.21.1614
63.Le, QT, Zhang, Q, Cao, H, Cheng, AJ, Pinsky, BA, Hong, RL, et al. An international collaboration to harmonize the quantitative plasma Epstein-Barr virus DNA assay for future biomarker-guided trials in nasopharyngeal carcinoma. Clin. Cancer Res. (2013) 19:2208–15. doi: 10.1158/1078-0432.CCR-12-3702
Keywords: nasopharyngeal carcinoma, PNI, prognosis, nomogram, LDH
Citation: Jiang Y-M, Huang S-T, Pan X-B, Ma J-L and Zhu X-D (2023) The prognostic nutritional index represents a novel inflammation-nutrition-based prognostic factor for nasopharyngeal carcinoma. Front. Nutr. 10:1036572. doi: 10.3389/fnut.2023.1036572
Edited by:
Gabriela Salim de Castro, University of São Paulo, BrazilReviewed by:
Taha Koray Sahin, Hacettepe University, TürkiyeCopyright © 2023 Jiang, Huang, Pan, Ma and Zhu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xiao-Dong Zhu, ✉ emh1eGlhb2RvbmdneG11QDE2My5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.