 Kristin Fulgoni
Kristin Fulgoni Victor L. Fulgoni III
Victor L. Fulgoni III- Nutrition Impact, LLC., Battle Creek, MI, United States
A large percentage of daily vegetable intake is attributed to white potatoes, but limited information is available on how potatoes are incorporated into dietary patterns in the US. Therefore, the objective of this study was to determine food patterns that include potatoes and to compare the associated diet quality and association with biomarkers to a food pattern without potatoes. Data from American subjects 2-18 and 19 years and older who participated in the What We Eat in America portion of the National Health and Nutrition Examination Survey cycles 2001-2018 were utilized in the current study. Diet quality was assessed using the Healthy Eating Index-2015. Anthropometric variables included body mass index (BMI), waist circumference, and weight. Biomarkers analyzed included glucose, insulin, triglycerides, HDL-, LDL-, and total cholesterol. Multiple food clusters containing potatoes were identified with several having higher and lower diet quality as compared to a food pattern without potatoes. Children and adolescents in one potato cluster had lower BMI, waist circumference, and body weight compared to those in a no potato dietary pattern, whereas adults in 3 potato clusters had higher anthropometric variables than those in a no potato pattern. In adults, some dietary patterns including potatoes were also associated with lower and higher HDL and total cholesterol and higher insulin levels. The percentage of calories from potatoes across patterns was small, ∼9-12%, suggesting the differences observed in diet quality and biomarkers were due to other food categories consumed in the pattern. This study suggests there are ways to incorporate potatoes as part of a healthy eating pattern but depends more on the other foods included in the diet.
Introduction
Vegetables are an important component in a healthy dietary pattern and are associated with lower risk of all-cause mortality, cardiovascular disease, overweight and obesity, type 2 diabetes, deteriorating bone health, colorectal and breast cancers in adults (1, 2). The Dietary Guidelines for Americans (DGA) recommends between 1 and 2.5 cup equivalents of vegetables per day for children and adults, depending on total calories consumed (1). Potatoes are defined as a starchy vegetable in the DGA, of which 2-5 cups are recommended weekly (1). Potatoes contribute substantially to vegetable intake and are the top source of vegetables in children, representing 34% of vegetables, and one of the top sources in adults, contributing 25% to total vegetable intake (3).
Potatoes are a nutrient dense food that can be included as part of a healthy eating pattern due to high levels of several nutrients including potassium and dietary fiber, both defined as nutrients of public concern (1). Potassium intake has an inverse correlation with blood pressure, whereas higher fiber intake reduces the risk of coronary heart disease (1, 2). Depending on preparation, 100 g of potatoes can provide 535 mg and 2.2 g of potassium and fiber to the diet, respectively, representing 16-23 and 5.8-10.5% of the nutrient adequate intakes for children and adults (4–6). Previous studies have found potatoes contribute 4.0-6.7% and 3.8-6.9% of daily potassium and dietary fiber, respectively, in children and adolescents (7–9). For adults, potatoes have been reported as the 3rd and 4th highest sources of potassium and fiber, respectively, providing 6.7 and 6.4% of daily intake (10). In addition to potassium and fiber, potatoes contributed more than 5% daily intake of vitamins B6 and C, magnesium, copper, thiamin, niacin, and phosphorus while contributing less than 10 and 5% of daily energy and sodium intake, respectively (11, 12).
The association of potatoes with physiological measures and anthropometric variables is inconsistent based on previous studies and differ based on potato preparation. A recent review found positive and neutral associations between potatoes and weight gain, BMI, and waist circumference (13), but studies utilized different covariate sets and had moderate, serious, and critical risk of bias, possibly influencing the findings. Regarding physiological measures, a previous study found no associations between potato intake and blood pressure and BMI, but when focused on fried potato intake, associations were found in US women (14). Analyzing these physiological parameters association with dietary patterns including potatoes may give more clarity to the health impacts of potatoes when incorporated within a diet.
While numerous studies have reported on potato consumption and its impact on nutrient intake (11, 12), diet quality (15), and association with physiological variables (13, 14), there is a lack of information of dietary patterns with and without potatoes being associated with these variables. Therefore, the goal of the current study was to determine potato dietary patterns and how they differ from dietary patterns without potatoes and to assess the association of these patterns with biomarkers, body composition, and diet quality scores. It was hypothesized that dietary patterns including potatoes result in higher Healthy Eating Index 2015 (HEI-2015) scores overall as well as for total vegetables and can positively impact biomarkers and body composition measures.
Materials and methods
Study population and data source
The National Health and Nutrition Examination Survey (NHANES) is now a continuous survey representative of the non-institutionalized United States population that includes a dietary intake component, What We Eat in America (WWEIA). NHANES study designs and methods are available online (16, 17). WWEIA collects detailed information on the dietary intake of participating subjects divided into 15 main food groups, 46 subcategories, and over 150 unique categories. NHANES cycles 2001-2002, 2003-2004, 2005-2006, 2007-2008, 2009-2010, 2011-2012, 2013-2014, 2015-2016, and 2017-2018 were utilized in the current study. Male and female participants defined as either potato consumers or potato non-consumers 2 years and older (with subgroups 2-18 y and 19 + y) with complete 24-h recalls were analyzed in the current study. Pregnant and/or lactating subjects (n = 1,631), those with zero calories (n = 6) and subjects with unreliable dietary reports (n = 10,163), as determined by the USDA, were removed from the sample, resulting in a sample size of 72,584. For participants 12 years and younger, other individuals with the most knowledge of their dietary intake were used as proxies. WWEIA is collected using the Automated Multiple Pass Method (AMPM) (18) which is a five-step process with multiple passes which increases the accuracy of dietary reporting. NHANES protocols have been approved by the Research Ethic Review Board and individual personal information is not included in publicly available NHANES data.
Dietary pattern analysis
Individual food intakes were determined using relevant Food Patterns Equivalent Databases (19). Potato consumers were defined as those with intake from WWEIA food categories potato chips (5002), white potatoes, baked or boiled (6802), French fries and other fried white potatoes (6804), and mashed potatoes and white potato mixtures (6806). Dietary patterns including potatoes and patterns without potatoes were determined using SAS 9.4 (SAS Institute, Cary, NC, USA). The SAS PROC CLUSTER command was utilized based on the percentage of calories from potatoes. The cluster analysis maximizes the differences in the percentage of calories coming from all food groups other than potatoes. Dietary patterns were defined as percentage of calories from potatoes and the 15 main food groups in WWEIA (20): dairy, protein foods, mixed dishes, refined grains, whole grains, snacks/sweets, fruit, vegetables, non-alcohol beverages, and alcoholic beverages. Cluster 0 was defined as the dietary pattern of potato non-consumers. After initial analysis where we examined 1, 2, 4, 6, 8, 10, 12, 14, and 16 clusters, we settled on further evaluation of six dietary clusters as a compromise between the percentage of variation explained as assessed by r-square, sample size of the clusters, and ease of interpretation. Children/adolescents and adults each had 3 unique clusters when compared to each other, therefore further analyses were conducted separately for these groups. The r-squared value for children and adults was of 0.418 and 0.383 in children and adults, respectively.
Diet quality assessment and biomarkers
Diet quality was assessed using the HEI-2015 which measures the adherence to DGA recommendations. High scores are associated with higher intake of food components total vegetables, greens and beans, total fruit, whole fruit, whole grains, dairy, total protein foods, seafood and plant protein, and fatty acid ratio. Higher scores are also associated with lower intakes of foods recommended to be limited; sodium, refined grains, saturated fat, and added sugars. Components total fruits, whole fruits, total vegetables, greens and beans, total protein foods, and seafood and plant protein have a maximum of 5 points each, whereas whole grains, dairy, fatty acid ratio, refined grains, sodium, added sugars, and saturated fats have a maximum score of 10 points. Total scores were calculated as the summation of individual component scores and the maximum score is 100. Biomarkers and body measurements were collected during the Medical Examination Center portion of NHANES survey. Body weight, waist circumference, and BMI were collected with NHANES standardized protocols (16). BMI z-score for subjects 2-18 y was determined using CDC growth charts (21). Biomarkers were collected according to NHANES laboratory protocols and included HDL, LDL, and total cholesterol, fasting plasma glucose, fasting insulin, and fasting triglycerides.
Statistical analyses
All analyses were adjusted for the complex sample design of NHANES. Regression analyses were used to determine differences in HEI-2015 total and component scores, body measures, and biomarker variables across dietary patterns. Covariates used in HEI-2015 analyses and body measures included age, gender, ethnicity, poverty income ratio, physical activity level, and current smoking status. For biomarkers, the above covariate set was used in addition to energy intake and BMI. Examination sample weights were used for intake analyses, anthropometric measures, HDL, and total cholesterol while fasting weights were used for fasting plasma glucose, fasting insulin, and fasting triglycerides. Statistical significance was set at <0.01.
Results
Cluster descriptions
In children, the six clusters identified had a percentage of calories from potatoes ranging from 8.6 and 11.7 percent (Table 1). Subjects in cluster 1 had the highest percentage of calories from protein foods (32.2%) and the lowest percentage from mixed dishes (7.0%). Those in cluster 2 had the highest percentage of calories from milk/dairy (31.1%) and the lowest percentage of calories from beverages (6.5%), while those in cluster 3 had the highest percentage of calories from potatoes (11.7%) as well as the highest percentages of calories from refined grains and beverages (16.3 and 13.8%, respectively). Subjects in cluster 4 had the highest percentage of calories from mixed dishes (51.8%) and the lowest percentages from milk/dairy, protein foods, refined grains and snacks/sweets (4.2, 3.5, 3.0, and 9.0%, respectively). Subjects in cluster 6 had the highest percentage of calories from snacks/sweets (44.5%) and the lowest percentage of calories from potatoes (8.6%).
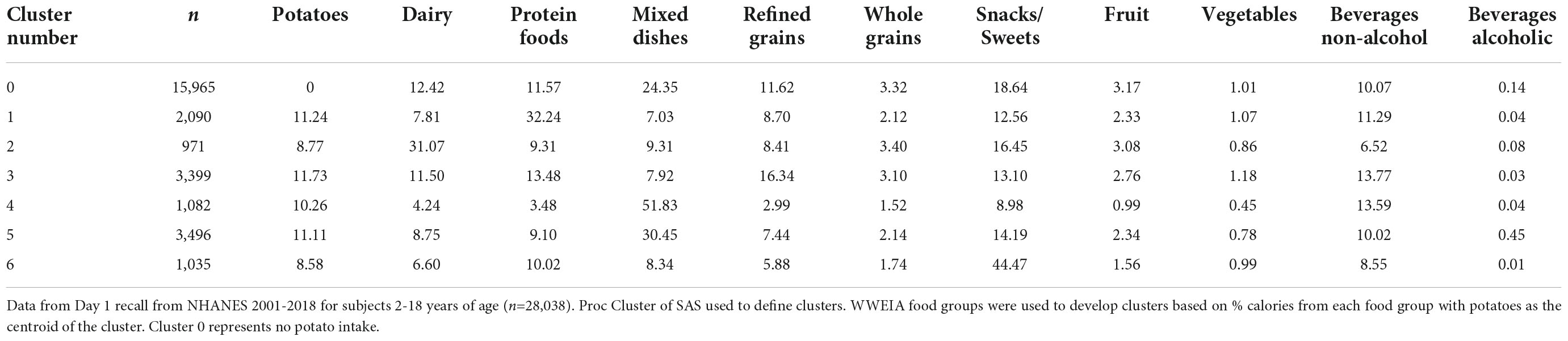
Table 1. Potato dietary patterns of consumption (clusters) and mean percent calories (kcal) within food groups in American children and adolescents.
In adults, the percentage of potatoes in clusters 1-6 ranged from 8.6 to 12.2 percent of calories (Table 2). The adult clusters had a somewhat similar pattern as children and adolescents. Subjects in cluster 1 had the highest percentage of calories from potatoes (12.2%) as well as a high percentage of calories from refined grains and beverages (10.7 and 11.2%, respectively). Those in cluster 2 had the highest percentage of calories from mixed dishes (52%) and the lowest percentages from milk/dairy, protein foods, refined grains, and whole grains (2.5, 4.1, 3.2, and 1.3%, respectively). Subjects in cluster 3 had the highest percentage of calories from protein foods (43.9%) and the lowest percentage from snacks/sweets (5.6%) while those in cluster 6 had the highest percentage of calories from snacks/sweets (37.2%) and the lowest percentage of calories from potatoes (8.6%).
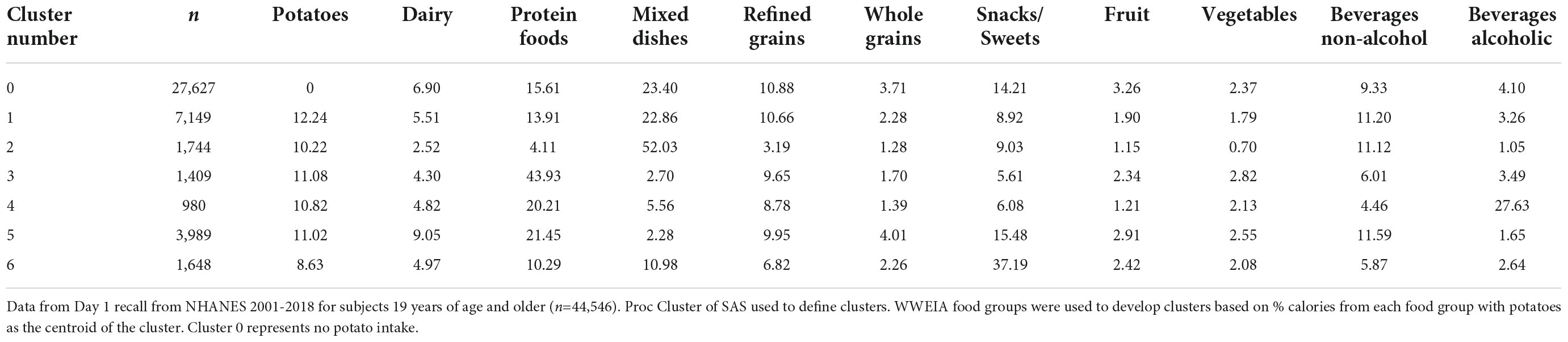
Table 2. Potato dietary patterns of consumption (clusters) and mean percent calories (kcal) within food groups in American adults.
Diet quality measured by Healthy Eating Index 2015
In children, subjects in the no potato cluster had a HEI-2015 total score of 46.4 points (Table 3). Subjects in potato clusters 1, 2, and 3 had higher HEI-2015 total scores and those in clusters 4 and 6 had lower total scores compared to subjects in the no potato cluster. The highest HEI-2015 total score was observed in cluster 1 subjects at 50.5 points. The participants in this cluster had a higher score for components total vegetables, total protein foods, fatty acid ratio, and refined grains as well as lower scores for greens and beans, total fruit, whole fruit, whole grains, dairy, and sodium compared to those in the no potato cluster. Total protein foods, fatty acid ratio, and refined grains contributed 16, 30, and 38% to the difference in total scores, respectively. The lowest HEI-2015 total score was observed in cluster 4 subjects at 43.4 points. Subjects in this cluster had a higher score for total vegetables and fatty acid ratio and lower scores for greens and beans, total fruit, whole fruit, whole grains, dairy, seafood and plant protein, and sodium compared to those in cluster 0. Whole fruit, whole grains, and dairy contributed 16, 22, and 15% to the difference in total scores, respectively.
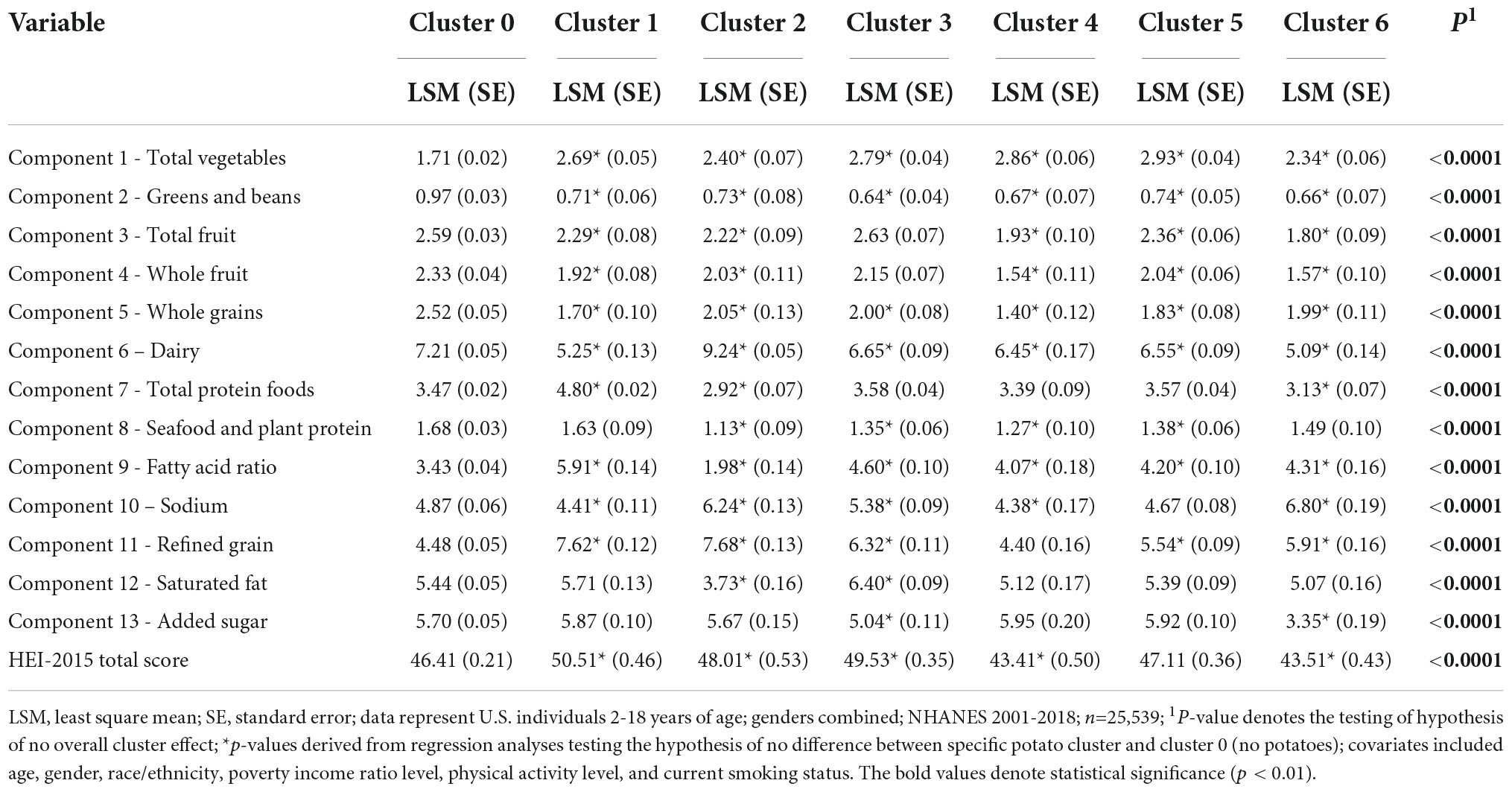
Table 3. Least square mean total and subcomponent Healthy Eating Index 2015 scores by potato cluster in American children and adolescents.
In adults, subjects in the no potato cluster had a HEI-2015 total score of 50.7 points (Table 4). Adults in potato clusters 3, 4, and 5 had higher HEI-2015 total scores and those in clusters 1, 2, and 6 had lower total scores compared to cluster 0. The highest total score was observed in cluster 4 subjects and was 4.1 points higher than cluster 0. Subjects in this cluster had higher scores for total vegetable, total protein foods, fatty acid ratio, sodium, refined grains, saturated fats, and added sugars and lower scores for greens and beans, total fruit, whole fruit, whole grains, dairy, and seafood and plant protein compared to cluster 0. Sodium, refined grains, saturated fat, and added sugars contributed 17, 32, 14, and 20% of the difference in total scores, respectively. The lowest total score was observed in cluster 2 subjects with 6.8 points less than cluster 0. Participants in this cluster had higher scores for total vegetables and lower scores for greens and beans, total fruit, whole fruit, whole grains, seafood and plant protein, sodium, refined grains, and saturated fat than cluster 0. Whole fruit, whole grains, and saturated fat contributed 12, 15, and 20% to the lower total scores, respectively.
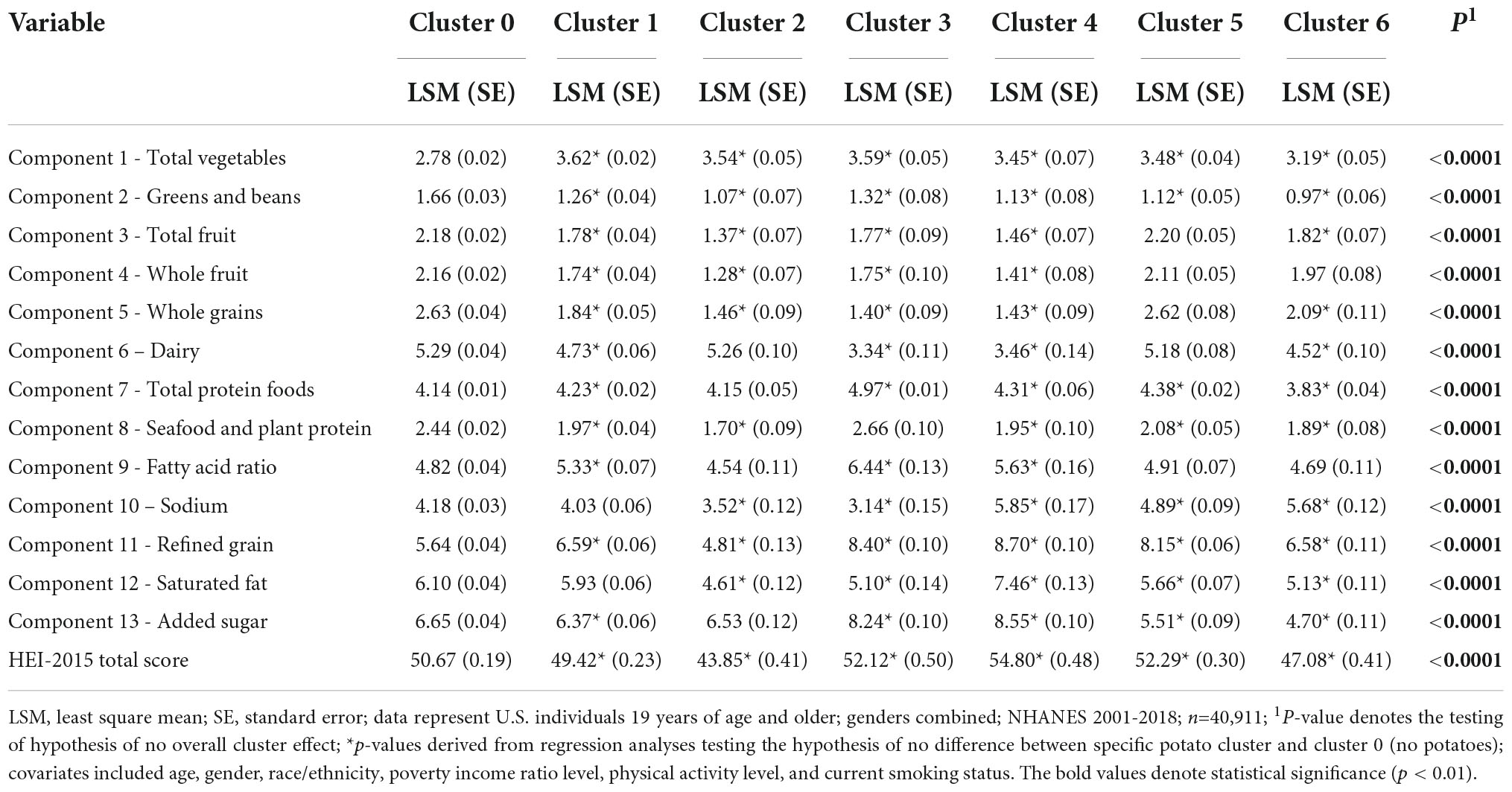
Table 4. Least square mean total and subcomponent Healthy Eating Index (2015) scores by potato cluster in American adults.
Potato clusters association with health biomarkers
In children, differences between subjects in cluster 0 and potato clusters were observed for BMI, waist circumference, weight, and total cholesterol (Table 5). Subjects in cluster 6 had 4, 2, and 5% lower BMI, waist circumference, and weight, respectively, compared to those in cluster 0. Participants in cluster 1 had 2% higher total cholesterol compared to cluster 0.
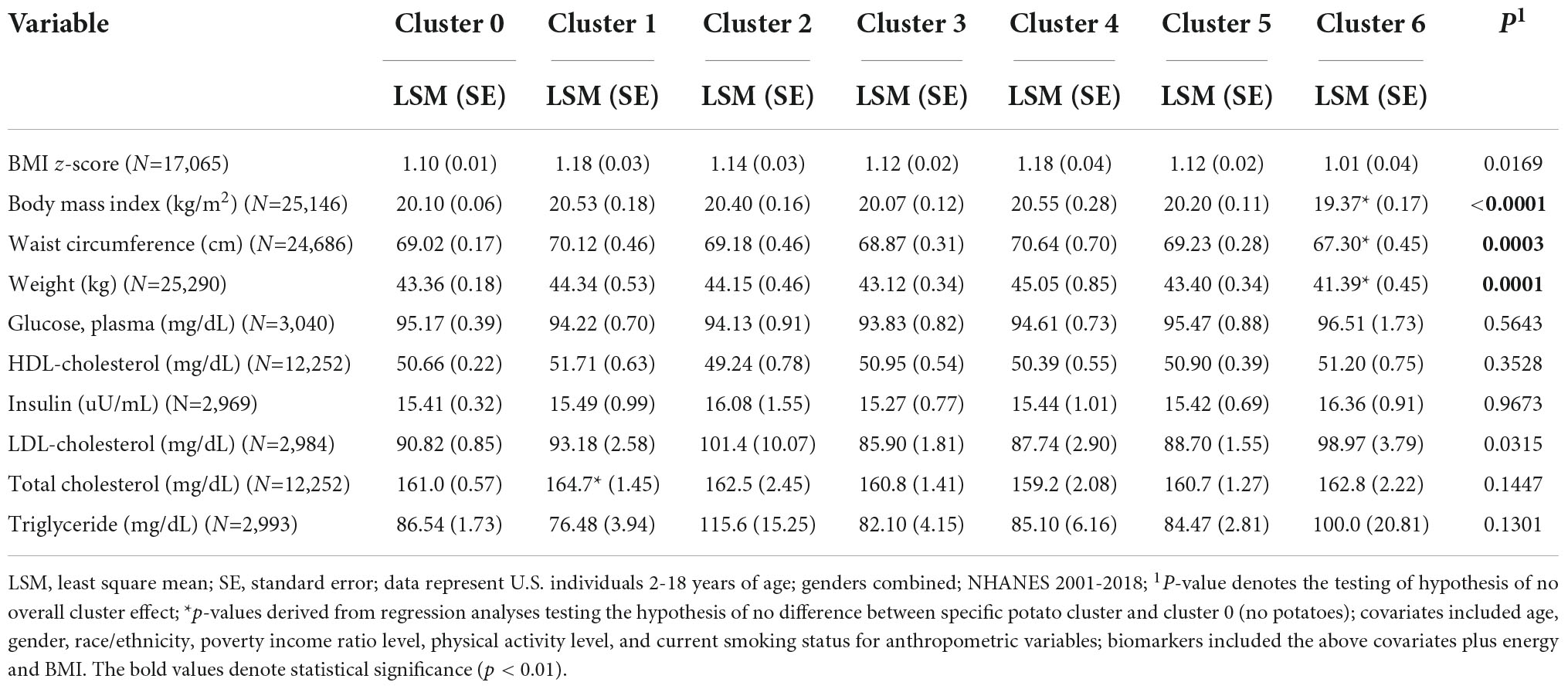
Table 5. Least square mean anthropometrics and biomarkers by potato cluster in American children and adolescents.
For adults, differences between subjects in cluster 0 and potato clusters were observed for BMI, waist circumference, weight, HDL cholesterol, insulin, and total cholesterol (Table 6). Subjects in cluster 2 had the largest differences in BMI, waist circumference, and weight at 5, 4, and 5% higher, respectively, compared to those in cluster 0. Participants in cluster 2 also had the lowest HDL cholesterol compared to those in cluster 0 with a difference of 3%. Cluster 4 subjects had the largest differences in HDL and total cholesterol at 13 and 5% higher, respectively, compared to those in cluster 0. Insulin was 7% higher in cluster 1 subjects, representing the largest difference in insulin compared to those in cluster 0.
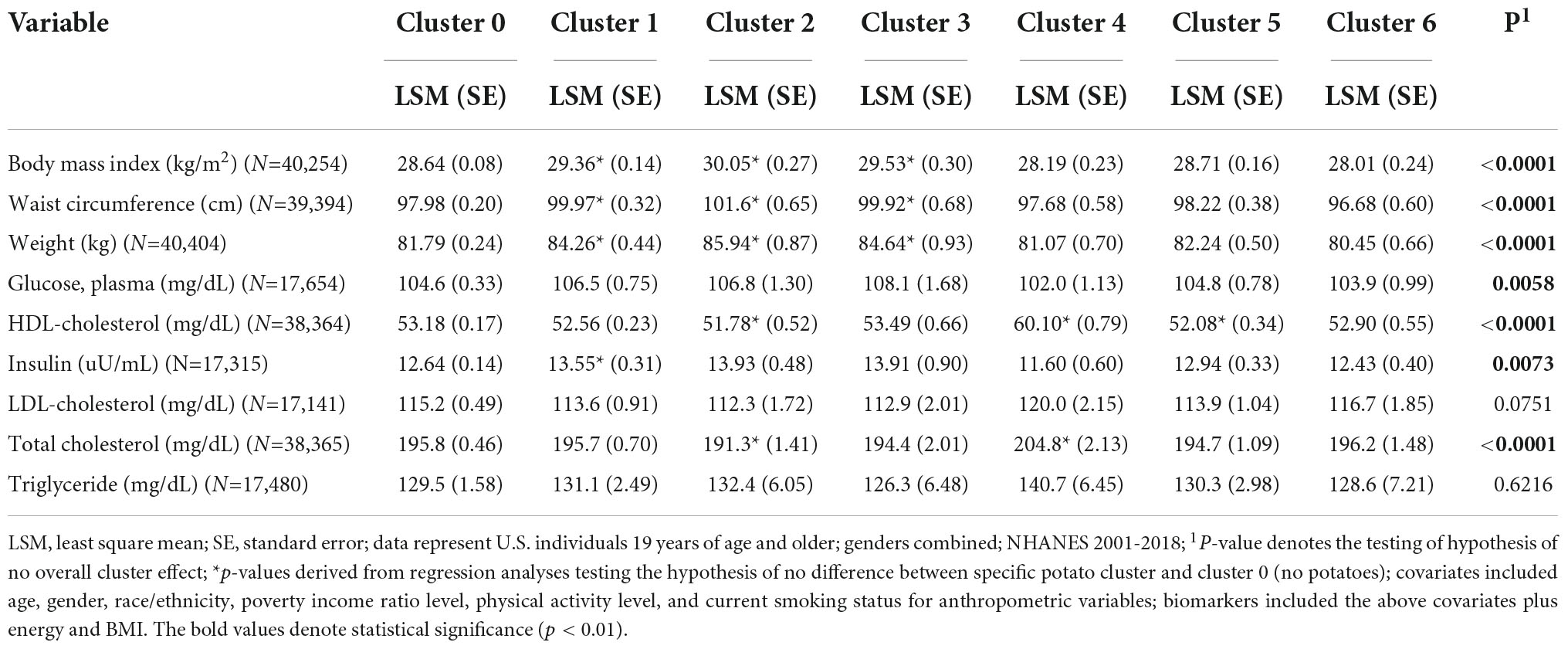
Table 6. Least square mean anthropometrics and biomarkers by potato cluster in American adults.
Discussion
The current study objectives were to determine dietary patterns of potato consumers and non-consumers and their differences in diet quality, anthropometric variables, and biomarkers. This is the first study to analyze dietary patterns including potatoes to our knowledge. We defined six dietary patterns using a cluster analysis technique. In terms of diet quality, subjects in three potato clusters had higher HEI-2015 total scores compared to those with non-potato diets. Subjects in two and three potato clusters also had lower total scores in children and adults, respectively. Participants in the potato dietary patterns with the highest HEI-2015 total scores had higher component scores for refined grains, fatty acid ratio, and saturated fat. Subjects with the lowest total scores were mostly the result of low whole fruit and whole grains component scores. In children and adolescents, subjects in one potato cluster had lower BMI, waist circumference, and body weight compared to those in the no potato dietary pattern. On the other hand, in adults, subjects in three potato clusters had higher anthropometric variables compared to those in the no potato cluster. In adults, several differences in biomarkers were observed between participants in potato patterns and those in the non-potato pattern including both lower and higher HDL or total cholesterol levels and higher insulin levels in one cluster.
While total dietary quality scores were within 11 points of each other, patterns including differing levels of potatoes resulted in subjects having both higher and lower HEI-2015 total scores than those with dietary patterns without potatoes. Significant increases and decreases in component scores were present between dietary patterns with potatoes as compared to one without potatoes. These significant differences are small changes (approximately 11-32% of the maximum subcomponent scores) to component scores as compared to previous studies on individual foods such as oatmeal and apples (22, 23). The previous studies focused on foods that are more consistent with one or more specific subcomponents as compared to potatoes. The percentage of calories from potatoes across all clusters was within a small range (8.6 – 12.2%) in both children and adults suggesting the change in diet quality observed is attributable to foods other than potatoes. In the current study, the lowest HEI-2015 score was found for subjects in a potato cluster which had a middle range percentage of calories from potatoes and highest from mixed dishes in both children and adults. Subjects in clusters with high mixed dishes also were associated with higher body weight, waist circumference, and BMI in adults. Potatoes, especially fried potatoes, are commonly consumed as a side dish or incorporated into meals with high levels of refined grains and/or added sugars including sugar-sweetened beverages, burgers, meats, etc. (14). The most common mixed dishes during NHANES 2007-2018 included pasta excluding macaroni and cheese, rice mixed dishes, vegetable mixed dishes, and other Mexican mixed dishes which contain high levels of nutrients the DGA suggest to consume in moderation (1, 20). The food patterns observed maximized the differences in food categories other than potatoes and resulted in differing diet qualities. The DGA as well as previous dietary pattern studies (1, 24), in combination with these results suggest that typically one specific food or food category cannot be solely responsible for improved or decreased diet quality. The entirety of the meal/diet must be taken into account when assessing the impact of potato consumption on dietary quality and associations with body measures/biomarkers.
Similar to diet quality, the anthropometric differences observed in subjects with dietary patterns including potatoes compared to no potatoes may also be due to presence or absence of other foods consumed within the pattern and possibly due to preparation methods. In children and adolescents, one potato cluster was associated with lower BMI, waist circumference, and body weight compared to the no potato cluster. This dietary pattern included the lowest percentage of potatoes (8.58% of calories) and approximately 44% of calories from snacks and sweets. Findings on snack intake within children is controversial with studies reporting direct, inverse, and no relationships between snack intake and anthropometric variables depending on the type, amount, and energy density of the snack (25–28). The content of snacks is important to consider when determining their impact on body weight, BMI, and waist circumference. It’s possible the snacks consumed in this potato cluster were higher in protein, fiber, and/or whole grains which have been found to increase satiety, possibly resulting in less total energy consumption throughout the day (25). In regards to preparation methods, several reviews have reported both positive and inverse associations of potato intake with BMI, weight, and waist circumference (13, 29). More consistent findings are observed when looking specifically at French fry intake and adiposity, with higher intake being associated with weight gain and BMI, whereas findings for total or baked, boiled, and mashed potatoes and BMI are less consistent (13, 14, 30). The current study did not focus on the type of snack included in the dietary pattern nor preparation methods which may affect the associations found.
Differences were observed in biomarkers between subjects in potato clusters and those in the no potato dietary pattern. Interestingly, the highest HDL cholesterol was found in a cluster with subjects consuming 10.8% of calories from potatoes and 27.6% calories from alcoholic beverages. It is difficult to determine the food or food category that attributed this beneficial effect on cholesterol levels. Studies focused on the relationship between potato consumption and cholesterol are scarce with a recent review identifying two studies that found no difference in total, HDL, and LDL cholesterol between high and low potato consumption (29). Another source of increased HDL cholesterol may be the high percentage of alcohol intake in the cluster, although the percentage of alcohol in this dietary pattern is well above the recommended limits (1). Alcohol potentially has a favorable impact on HDL-cholesterol, but is dependent on the amount consumed as well as the type of alcohol (31, 32). In addition to differences in HDL cholesterol, subjects in one potato cluster had higher insulin levels than those in the no potato cluster. Participants in this dietary pattern had the highest percentage of calories from potatoes as well as the second highest percentage of calories from refined grains as well as non-alcoholic beverages. Both non-alcoholic beverages, which are typically sugar-sweetened beverages that contribute high levels of added sugars (33), and refined grains have been associated with higher insulin in previous studies (34). Similar to diet quality, the totality of the diet must be taken into consideration when assessing specific food and food categories relationships with biomarkers and cannot be attributed to potatoes alone.
A strength of the current study includes the use of a large sample size representative of the US population from NHANES separated into two age groups. A second strength was the utilization of a previously used technique to understand dietary patterns through cluster analysis (24). The current study has several limitations. NHANES depends on self-reported dietary intake which are subject to misreporting (35). Proxies were used for children under 12 who may have limited information on foods consumed outside the house, further adding to misreporting. Although covariates commonly used in intake studies were used, residual confounding may still be present. As with all observational studies, cause and effect could not be determined. Finally, the analyses focused solely on dietary patterns with and without potatoes so other foods within the diet likely have influenced the current results.
The current study identified several dietary patterns in children and adults that included potato consumption with varying levels of other food categories. Diet quality differed between subjects with food patterns including various levels of potatoes with clusters showing both improved and decreased diet quality as compared to food patterns without potatoes even though the percentage of calories from potatoes in all potato clusters was within a finite range (from 8.6-12% in both children and adults). Similar results were observed with biomarkers. Participants in several potato food patterns had decreased anthropometric variables in children compared to those with food patterns excluding potatoes. In adults, differences were observed in both anthropometric and physiological variables including HDL-, total cholesterol, and insulin. Given the finite range of calories from potatoes in clusters, these results suggest the differences in diet quality and biomarkers observed in the current study are likely attributed to the presence or absence of other food categories in the dietary patterns. These data also suggest potatoes can be a part of healthy dietary patterns when balanced with other nutrient-rich foods consistent with dietary recommendations.
Data availability statement
Publicly available datasets were analyzed in this study. This data can be found here: National Health and Nutrition Examination Survey 2001-2018, https://wwwn.cdc.gov/nchs/nhanes.
Ethics statement
The NHANES study procedures were reviewed and approved by the NCHS Ethics Review Board (for more details on specific protocols see https://www.cdc.gov/nchs/nhanes/irba98.htm). Written informed consent was obtained from all participants for their participation in this study.
Author contributions
VF: conceptualization, methodology, and analyses. KF: writing – original draft preparation. VF and KF: writing – review and editing. Both authors read and agreed to the published version of the manuscript.
Funding
This research was funded by the Alliance for Potato Research & Education (APRE). APRE had no role in analyses/interpretation of results and did not review the manuscript prior to submission.
Acknowledgments
This study and the writing of the manuscript were supported by Alliance for Potato Research & Education (APRE).
Conflict of interest
Authors KF and VF were employed by Nutrition Impact, LLC., a food and nutrition consulting firm which analyses NHANES data for numerous food and beverage companies and related entities.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. U.S. Department of Agriculture, U.S. Department of Health and Human Services,. Dietary Guidelines for Americans, 2020-2025. 9th ed. (2020). Available online at: http://DietaryGuidelines.gov (accessed February 11, 2022).
2. Dietary Guidelines Advisory Committee. Scientific Report of the 2020 Dietary Guidelines Advisory Committee: Advisory Report to the Secretary of Agriculture and the Secretary of Health and Human Services. Washington, DC: U.S. Department of Agriculture, Agricultural Research Service (2020).
3. U.S. Department of Agriculture, Agricultural Research Service. Food Patterns Equivalents Intakes from Food: Mean Amounts Consumed per Individual, by Gender and Age, What We Eat in America, NHANES 2017-2018. (2020). Available online at: www.ars.usda.gov/nea/bhnrc/fsrg (accessed September 19, 2021).
4. U.S. Department of Agriculture, Agricultural Research Service. FoodData Central. (2019). Available online at: fdc.nal.usda.gov (accessed February 11, 2022).
5. Institute of Medicine. Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids. Washington, DC: The National Academies Press (2005). doi: 10.17226/10490
6. National Academies of Sciences, Engineering, and Medicine. Dietary Reference Intakes for Sodium and Potassium. Washington, DC: The National Academies Press (2019). doi: 10.17226/25353
7. Leme A, Baranowski T, Thompson D, Philippi S, O’Neil C, Fulgoni V, et al. Food sources of shortfall nutrients among US adolescents: national health and nutrition examination survey (NHANES) 2011-2014. Fam Community Health. (2019) 43:59–73. doi: 10.1097/FCH.0000000000000243
8. O’Neil CE, Nicklas TA, Fulgoni VL. Food sources of energy and nutrients of public health concern and nutrients to limit with a focus on milk and other dairy foods in children 2 to 18 years of age: national health and nutrition examination survey, 2011–2014. Nutrients. (2018) 10:1050. doi: 10.3390/nu10081050
9. Keast D, Fulgoni V, Nicklas T, O’Neil C. Food sources of energy and nutrients among children in the United States: national health and nutrition examination survey 2003–2006. Nutrients. (2013) 5:283–301. doi: 10.3390/nu5010283
10. O’Neil C, Keast D, Fulgoni V, Nicklas T. Food sources of energy and nutrients among adults in the US: NHANES 2003–2006. Nutrients. (2012) 4:2097–120. doi: 10.3390/nu4122097
11. Freedman MR, Keast DR. Potatoes, including french fries, contribute key nutrients to diets of U.S. adults: NHANES 2003-2006. J Nutr Ther. (2012) 1:1–11. doi: 10.6000/1929-5634.2012.01.01.1
12. Freedman MR, Keast DR. White potatoes, including French fries, contribute shortfall nutrients to children’s and adolescents’ diets. Nutr Res. (2011) 31:270–7. doi: 10.1016/j.nutres.2011.03.006
13. Borch D, Juul-Hindsgaul N, Veller M, Astrup A, Jaskolowski J, Raben A. Potatoes and risk of obesity, type 2 diabetes, and cardiovascular disease in apparently healthy adults: a systematic review of clinical intervention and observational studies. Am J Clin Nutr. (2016) 104:489–98. doi: 10.3945/ajcn.116.132332
14. Aljuraiban GS, Pertiwi K, Stamler J, Chan Q, Geleijnse JM, Van Horn L, et al. Potato consumption, by preparation method and meal quality, with blood pressure and body mass index: the intermap study. Clin Nutr. (2020) 39:3042–8. doi: 10.1016/j.clnu.2020.01.007
15. Agarwal S, Fulgoni VL. Intake of potatoes is associated with higher diet quality, and improved nutrient intake and adequacy among US adolescents: NHANES 2001–2018 Analysis. Nutrients. (2021) 13:2614. doi: 10.3390/nu13082614
16. NHANES Questionnaires,. Datasets, and Related Documentation. (n.d.). Available online at: https://wwwn.cdc.gov/nchs/nhanes/Default.aspx (accessed January 24, 2021).
17. Dwyer J, Picciano MF, Raiten DJ. Members of the steering committee. collection of food and dietary supplement intake data: what we eat in America–NHANES. J Nutr. (2003) 133:590S–600S. doi: 10.1093/jn/133.2.590S
18. Moshfegh AJ, Rhodes DG, Baer DJ, Murayi T, Clemens JC, Rumpler WV, et al. The US department of agriculture automated multiple-pass method reduces bias in the collection of energy intakes. Am J Clin Nutr. (2008) 88:324–32. doi: 10.1093/ajcn/88.2.324
19. United States Department of Agriculture. Agricultural Research Service Food Patterns equivalents Database. (2021). Available online at: https://www.ars.usda.gov/northeast-area/beltsville-md-bhnrc/beltsville-human-nutrition-research-center/food-surveys-research-group/docs/fped-databases (accessed April 26, 2021).
20. U.S. Department of Agriculture, Agricultural Research Service. What We Eat in America Food Categories 2017-2018. (2020). Available online at: www.ars.usda.gov/nea/bhnrc/fsrg (accessed February 2, 2022).
21. Centers for Disease Control and Prevention, Division of Nutrition, Physical Activity, and Obesity. A SAS Program for the 2000 CDC Growth Charts (ages 0 to <20 years). (2022). Available online at: https://www.cdc.gov/nccdphp/dnpao/growthcharts/resources/sas.htm (accessed on May 4, 2022).
22. Fulgoni VL, Chu Y, O’Shea M, Slavin JL, DiRienzo MA. Oatmeal consumption is associated with better diet quality and lower body mass index in adults: the national health and nutrition examination survey (NHANES), 2001-2010. Nutr Res. (2015) 35:1052–9. doi: 10.1016/j.nutres.2015.09.015
23. O’Neil CE, Nicklas TA, Fulgoni VL. Consumption of apples is associated with a better diet quality and reduced risk of obesity in children: national health and nutrition examination survey (NHANES) 2003–2010. Nutr J. (2015) 14:48. doi: 10.1186/s12937-015-0040-1
24. Papanikolaou Y, Fulgoni VL III. Patterns of egg consumption can help contribute to nutrient recommendations and are associated with diet quality and shortfall nutrient Intakes. Nutrients. (2021) 13:4094. doi: 10.3390/nu13114094
25. Njike VY, Smith TM, Shuval O, Shuval K, Edshteyn I, Kalantari V, et al. Snack food, satiety, and weight123. Adv Nutr. (2016) 7:866–78. doi: 10.3945/an.115.009340
26. Keast DR, Nicklas TA, O’Neil CE. Snacking is associated with reduced risk of overweight and reduced abdominal obesity in adolescents: national health and nutrition examination survey (NHANES) 1999–2004. Am J Clin Nutr. (2010) 92:428–35. doi: 10.3945/ajcn.2009.28421
27. Tripicchio GL, Kachurak A, Davey A, Bailey RL, Dabritz LJ, Fisher JO. Associations between snacking and weight status among adolescents 12–19 years in the United States. Nutrients. (2019) 11:1486. doi: 10.3390/nu11071486
28. Larson NI, Miller JM, Watts AW, Story MT, Neumark-Sztainer DR. Adolescent snacking behaviors are associated with dietary intake and weight status. J Nutr. (2016) 146:1348–55. doi: 10.3945/jn.116.230334
29. So J, Avendano EE, Raman G, Johnson EJ. Potato consumption and risk of cardio-metabolic diseases: evidence mapping of observational studies. Syst Rev. (2020) 9:274. doi: 10.1186/s13643-020-01519-y
30. Linde JA, Utter J, Jeffery RW, Sherwood NE, Pronk NP, Boyle RG. Specific food intake, fat and fiber intake, and behavioral correlates of BMI among overweight and obese members of a managed care organization. Int J Behav Nutr Phys Act. (2006) 3:42. doi: 10.1186/1479-5868-3-42
31. Day E, Rudd JHF. Alcohol use disorders and the heart. Addiction. (2019) 114:1670–8. doi: 10.1111/add.14703
32. Tverdal A, Høiseth G, Magnus P, Næss Ø, Selmer R, Knudsen GP, et al. Alcohol consumption, HDL-cholesterol and incidence of colon and rectal cancer: a prospective cohort study including 250,010 participants. Alcohol Alcohol. (2021) 56:718–25. doi: 10.1093/alcalc/agab00728
33. Ricciuto L, Fulgoni VL, Gaine PC, Scott MO, DiFrancesco L. Trends in added sugars intake and sources among US children, adolescents, and teens using NHANES 2001–2018. J Nutr. (2022) 152:568–78. doi: 10.1093/jn/nxab395
34. Sanders LM, Zhu Y, Wilcox ML, Koecher K, Maki KC. Whole grain intake, compared to refined grain, improves postprandial glycemia and insulinemia: a systematic review and meta-analysis of randomized controlled trials. Crit Rev Food Sci Nutr. (2021) 1–19. [Epub ahead of print]. doi: 10.1080/10408398.2021.2017838
Keywords: NHANES, potatoes, Healthy Eating Index, dietary patterns, biomarkers
Citation: Fulgoni K and Fulgoni VL III (2022) Certain dietary patterns including potatoes are associated with higher and lower diet quality and physiological measures in children and adults, NHANES 2001-2018. Front. Nutr. 9:987861. doi: 10.3389/fnut.2022.987861
Received: 06 July 2022; Accepted: 12 October 2022;
Published: 10 November 2022.
Edited by:
Donato Angelino, University of Teramo, ItalyReviewed by:
Saeed Mohammadi, Golestan University of Medical Sciences, IranConnie M. Weaver, San Diego State University, United States
Copyright © 2022 Fulgoni and Fulgoni. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Victor L. Fulgoni III, dmljM3JkQGFvbC5jb20=