
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Nutr., 30 August 2022
Sec. Nutritional Epidemiology
Volume 9 - 2022 | https://doi.org/10.3389/fnut.2022.987048
This article is part of the Research TopicEnvironmental Factors Implicated in ObesityView all 11 articles
 Nora A. AlFaris1
Nora A. AlFaris1 Naseem M. Alshwaiyat2
Naseem M. Alshwaiyat2 Hana Alkhalidy3
Hana Alkhalidy3 Jozaa Z. AlTamimi1
Jozaa Z. AlTamimi1 Reham I. Alagal4
Reham I. Alagal4 Reem A. Alsaikan4
Reem A. Alsaikan4 Malak A. Alsemari5
Malak A. Alsemari5 Mona N. BinMowyna6
Mona N. BinMowyna6 Nora M. AlKehayez1*
Nora M. AlKehayez1*Background: Adults frequently consume sugar-sweetened beverages. These products are linked to negative health effects such as obesity. Our study was carried out to assess rates of weekly and daily sugar-sweetened beverages consumption in a multi-ethnic population of middle-aged men and association with sociodemographic variables and obesity.
Methods: A sum of 1,800 middle-aged men (36–59 years) living in Riyadh, KSA, participated in this cross-sectional study. Sociodemographic variables and the frequency of sugar-sweetened beverages consumption were gathered from participants using face to face interviews. Weekly and daily consumption of sugar-sweetened beverages were the two binary outcome variables applied in this research. Weight and height were measured following standard procedures.
Results: In this study, 93.8 and 32.6% of participants consumed sugar-sweetened beverages weekly and daily, respectively. The weekly and daily sugar-sweetened beverages consumption was predicted by nationality. Subjects from Pakistan (99.3%) and Yemen (60.0%) reported the greatest rates of weekly and daily consumption, respectively, while Bangladeshi and Sudanese subjects reported the lowest rates of weekly (87%) and daily (2.9%) consumption, respectively. Another factor that predicted weekly sugar-sweetened beverages consumption was obesity. Obese subjects had a significantly greater odds ratio of weekly sugar-sweetened beverages intake than non-obese individuals (OR = 3.80, P = 0.003).
Conclusion: Consumption of sugar-sweetened beverages is common among middle-aged men who live in KSA. Results show connecting sugar-sweetened beverages intake with specific sociodemographic variables and obesity.
Globally, a widespread intake of sugar-sweetened beverages (SSBs) has been documented in adults (1). Common SSBs include regular soda, fruit drinks, and energy drinks. Most of SSBs are manufactured by adding high amounts of various types of free sugars such as sucrose and fructose (2). Consumption of SSBs contributes to daily energy intake due to their high added sugar content (3). Thus, SSBs intake may decline overall diet quality and lower daily intake of essential micronutrients (4). Consumption of SSBs is linked to a greater risk of numerous health problems like obesity, diabetes, cardiovascular disease and dental caries (5–7). Subsequently, SSBs intake has been considered an important public health issue (8). This situation motivated the WHO to create guidelines encouraging adults to limit added sugar intake to 5–10% of typical day calories (9). As SSBs consumption is very common among adults, it is vital to investigate patterns of SSBs intake and related sociodemographic variables to create efficient wellbeing promotion initiatives to minimize their use (10, 11).
In the Kingdom of Saudi Arabia (KSA), adult obesity is a serious health issue accompanied by unhealthy lifestyle choices such as physical inactivity and poor diet, including high consumption of SSBs (12–16). Indeed, KSA is the top oil producer in the Middle East region, and its economy is rising quickly. It should be no surprise that KSA hires people from all over the world. In fact, KSA had a workforce of about 50% foreigners, and 90% of the private sector occupations were held by foreigners (17). About one-third of the people in this country are non-Saudi residents, with men making up roughly three-fourths of them (18). Immigrants from various ethnic backgrounds make exploring the disparities in food habits and connections to wellness and illness in a diverse population exciting. Therefore, the objectives of this study were to determine the rates of weekly and daily SSBs consumption in a population of middle-aged men from various ethnic groups and the association with socioeconomic variables and obesity.
The data for this study were derived from a research project named the Relationship between Obesity, physical Activity, and Dietary pattern among men in KSA (ROAD-KSA) (15, 16, 19–22). It is a cross-sectional research project that took place in Riyadh, KSA, from February to June 2019. The study sample was randomly drawn from Riyadh public areas using a stratified clustered sampling technique. The eligible subjects were middle-aged men aged 36–59 years, living in Riyadh city, without any physical disability (the disability nature may affect body weight and height, which could bias the outcome of obesity diagnosis, and may affect food habits, including SSBs intake which could bias the outcome of SSBs consumption frequency), and having citizenship from one of these countries: KSA, Egypt, Yemen, Syria, Jordan, Sudan, Turkey, Pakistan, Afghanistan, India, Bangladesh, and the Philippines. Before taking part in our study, informed consent was collected from subjects in agreement with the Helsinki Declaration. The present study was authorized by the research ethics committee of Princess Nourah bint Abdulrahman University.
Professional research team gathered sociodemographic data following face to face interviews. The collected data were nationality, age, residency period in KSA, household type, marital status, educational level, and monthly income.
Professional research team measured weight and height of subjects while wearing minimal clothes and no slippers in a complete standup situation. Weight was measured to the closest 0.1 kg using a weight balance (Seca 802, Hamburg, Germany), whilst height was measured to the closest 0.1 cm using a portable stadiometer (Seca 213, Hamburg, Germany). Weight (kg) was divided by height (m2) to find body mass index (BMI) value. Obesity is determined as a BMI ≥ 30 (23).
The frequency of SSBs intake was determined using a valid and reliable questionnaire. The questionnaire's face validity was assessed using an objective evaluation from five skilled researchers. A test-retest pilot study with a 14 days' time lag was used to judge the questionnaire's reliability. Data were collected by a skilled research team using face to face interviews. In this study, SSBs were defined as artificial beverages with free sugars that are not recognized as diet or low-calorie, excluding coffee, tea, dairy, and alcoholic beverages (11). Consequently, SSBs were classified into three subtypes: regular soda, fruit drinks and energy drinks. Regular soda refers to carbonated beverages with added sugar. Fruit drinks are artificial fruit juices with free sugars, excluding natural fruit juices. Energy drinks are any carbonated beverage with added sugar and a high level of stimulating ingredients such as caffeine. To determine the frequency of SSBs consumption, the participants were questioned about the number of servings (on average 12 fl oz can or bottle) from each SSBs subtype they usually drink per week or day during the preceding year. The frequency of weekly and daily consumption for total SSBs and each SSBs subtype were computed based on replies. Drinking at least one serving per week was considered weekly consumption, while drinking at least one serving per day was considered daily consumption (24).
Data analysis was managed using Statistical Package for the Social Sciences (SPSS) software for Windows, version 26.0 (SPSS Inc., Armonk, NY, USA). This study uses two binary outcome variables: weekly and daily consumption of SSBs. Categorical variables were analyzed using the Chi-square test, and the results were displayed as frequencies and percentages. After adjusting for studied sociodemographic variables and obesity, a multivariate logistic regression analysis was done to investigate variables linked to weekly and daily SSBs consumption. Two-tailed testing was used to determine P-values. Statistical significance was recognized when P < 0.05.
The study subjects came from twelve different countries who lived in KSA. The mean age of study participants was 40.9 ± 3.8 years, and the mean BMI was 26.6 ± 3.6. Table 1 displays the prevalence of weekly SSBs consumption among subjects by sociodemographic variables and obesity. Weekly SSBs consumption was reported in 93.8% of the full study sample, while weekly consumption rates for regular soda, fruit drinks, and energy drinks were 81.9, 58.1, and 32.1%, respectively. When participants were divided into subgroups depending on their nationality, significant differences (P < 0.001) in weekly SSBs consumption rates were observed. The participants from Pakistan have the highest rate of SSBs intake per week (99.3%), while the subjects from Bangladesh have the lowest rate (87%). The highest prevalence of regular soda drinking per week (89.8%) was observed among Afghani subjects, while the lowest prevalence (71.8%) was observed among Jordanian subjects. While Filipino subjects have the highest weekly consumption rates of fruit drinks (85.9%) and energy drinks (53.5%). The lowest rates of fruit drinks (24.0%) and energy drinks (17.8%) were reported among subjects from Bangladesh and Sudan, respectively. Participants who have lived in KSA for more than 5 years had a significantly higher prevalence of weekly SSBs intake (94.4%) than those who have been there for 5 years or less (91.3%). Living within non-family households was correlated with a significantly greater rate of weekly SSBs intake (95.8%) than living within family households (90.5%). Single subjects have significantly higher weekly consumption rates of SSBs (95.5%) and regular soda (88.8%) than married participants (93.4 and 81.2%, respectively). A low education level was correlated with a significantly greater weekly SSBs intake rate (95.9%) than high education level (90.0%). Likewise, low monthly income was connected with a significantly greater weekly consumption rate of SSBs (95.9%) than high monthly income (91.6%). Lastly, obese participants have a significantly greater prevalence of weekly SSBs consumption (97.7%) than non-obese subjects (93.2%).
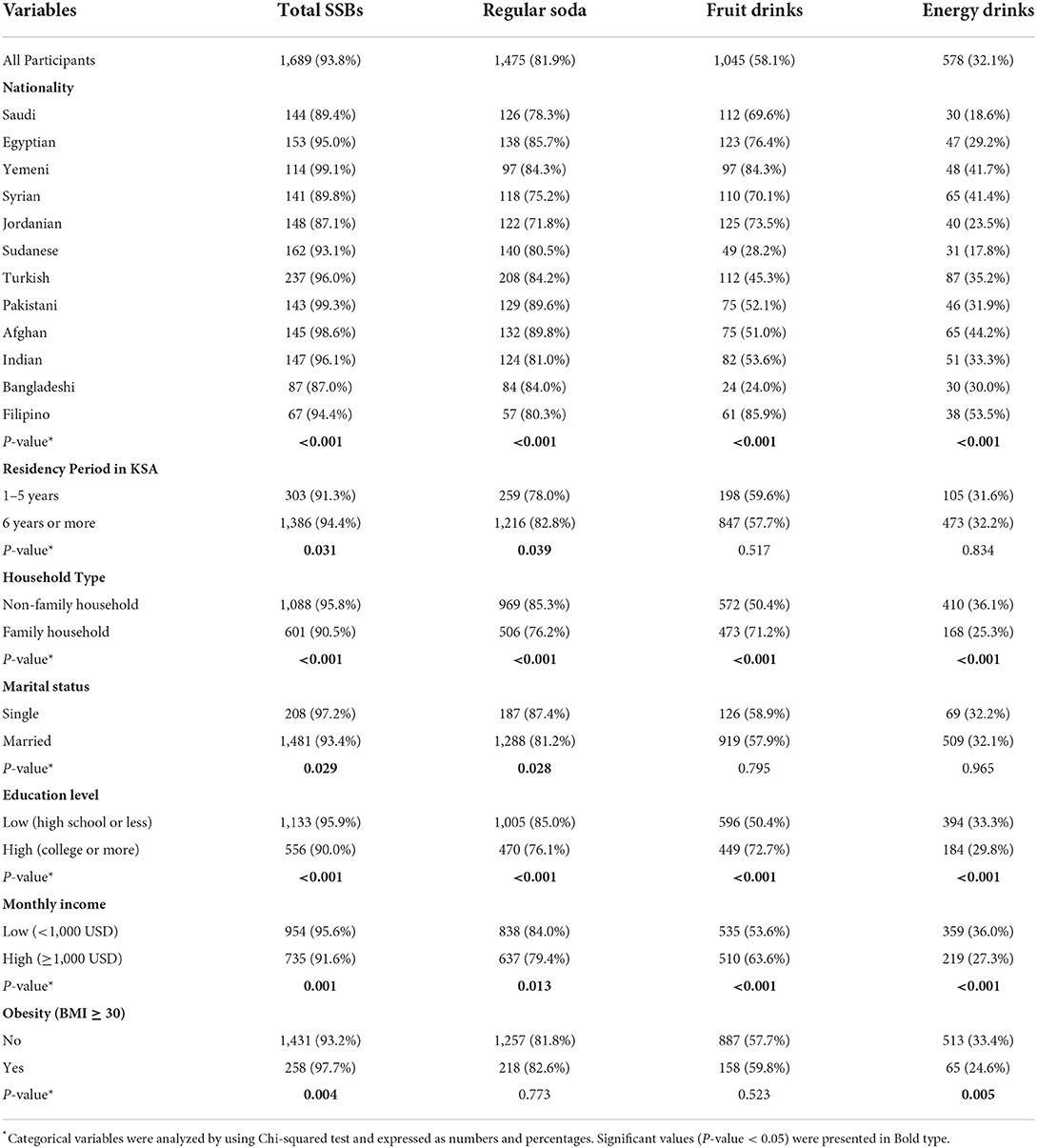
Table 1. Prevalence of weekly sugar-sweetened beverages (SSBs) consumption among study participants (n = 1,800) stratified by sociodemographic variables and obesity.
Table 2 shows the prevalence of daily SSBs consumption among study participants by sociodemographic variables and obesity. Daily consumption of SSBs was reported in 32.6% of the full study sample, whereas the rates for regular soda, fruit drinks, and energy drinks were 11.7, 2.6, and 0.8%, respectively. When participants are subdivided depending on their nationality, significant variations (P < 0.001) in daily intake rates of SSBs, regular soda and fruit drinks are identified. Yemeni subjects have the highest rates of daily SSBs intake (60.0%) and regular soda (20.9%). In comparison, the highest rates of daily intake of fruit drinks and energy drinks were seen among Filipino (12.7%) and Afghan (2.7%) subjects, respectively. In contrast, the lowest rates of daily consumption of SSBs (2.9%) and regular soda (0.6%) were reported among Sudanese and Jordanian subjects, respectively. However, daily consumption of fruit drinks was not observed among Sudanese, Pakistani, Indian, and Bangladeshi subjects, while daily consumption of energy drinks was not observed among Egyptian, Jordanian, Sudanese, and Bangladeshi subjects. The daily SSBs consumption rates among participants with 5 years or less and more than 5 years of residency in KSA were 36.4 and 31.7%, respectively (P > 0.05). Similarly, the daily SSBs consumption rates among participants who live within non-family and family households were 33.0 and 31.9%, respectively. The daily SSBs consumption rates among single and married participants were 37.4 and 32.0%, respectively. The daily SSBs consumption rates among participants with low and high education levels were 32.3 and 33.2%, respectively. The daily SSBs consumption rates among participants with low and high monthly income were 32.0 and 33.4%, respectively. Finally, the daily SSBs consumption rates among obese and non-obese participants were 28.8 and 33.3%, respectively.
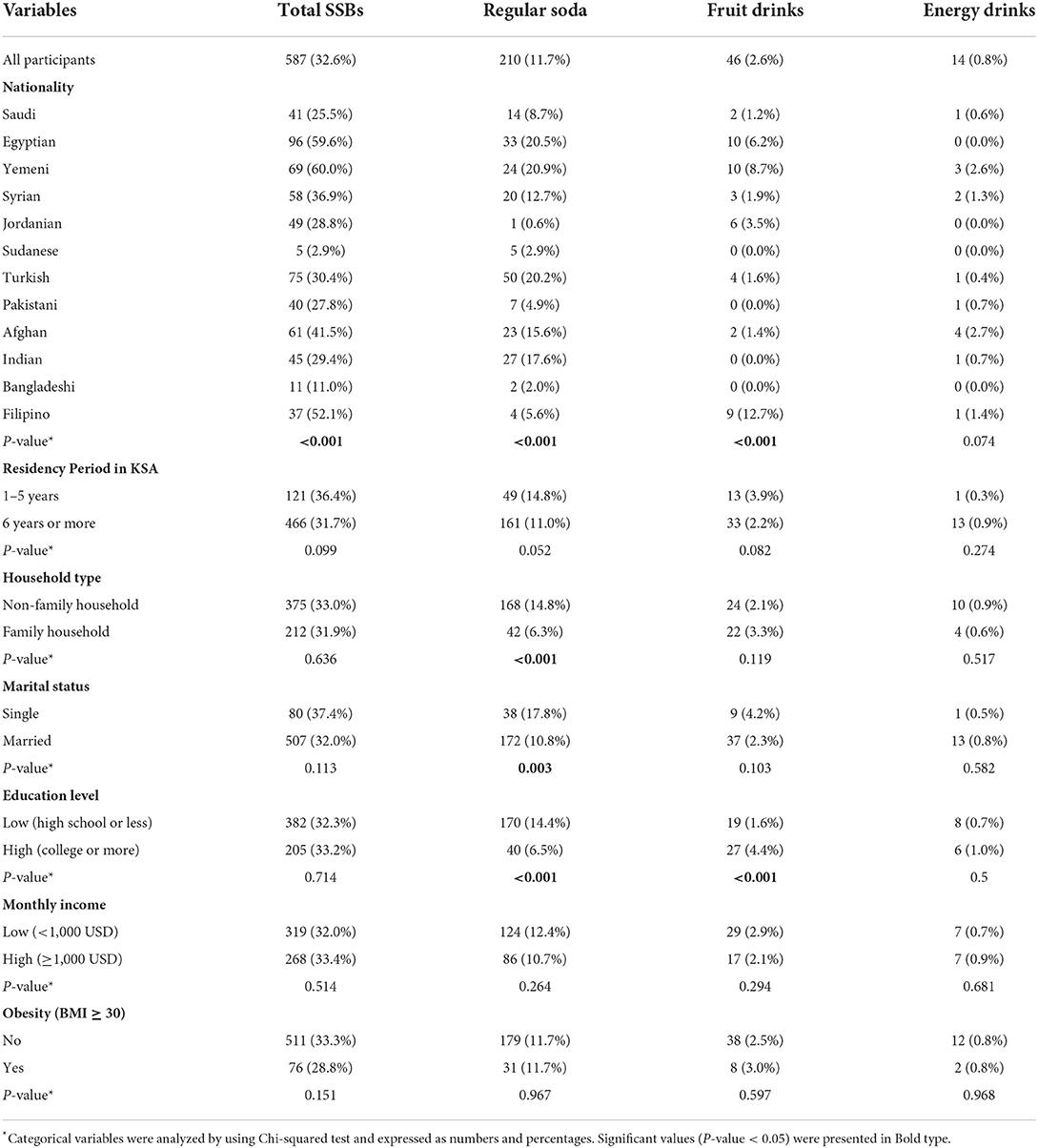
Table 2. Prevalence of daily sugar-sweetened beverages (SSBs) consumption among study participants (n = 1,800) stratified by sociodemographic variables and obesity.
Table 3 demonstrates the odds ratios for weekly and daily SSBs consumption among participants for sociodemographic variables and obesity. Nationality was found to be a predictor of weekly and daily SSBs consumption. Compared to Bangladeshi participants, subjects from Egypt, Yemen, Turkey, Pakistan, Afghanistan, and India had significantly greater odds ratios of SSBs consumption per week [odds ratio (OR) ranged from 2.96 to 29.19, P < 0.05]. Likewise, compared to subjects from Sudan, subjects from the remaining countries had significantly greater odds ratios of daily SSBs consumption (OR ranging from 3.72 to 103.15, P < 0.05). Furthermore, increasing age was significantly associated with lower odds ratios of weekly (OR = 0.88, P < 0.001) and daily (OR = 0.95, P < 0.001) SSBs consumption. Subjects who lived in family households had a significantly lower odds ratio of daily SSBs consumption than those who lived in non-family households (OR = 0.41, P < 0.001). Highly educated subjects had a significantly lower odds ratio of daily SSBs consumption than those with low education (OR = 0.60, P = 0.006). Subjects with a high monthly income had a significantly higher odds ratio of daily SSBs consumption than those with low monthly income (OR = 1.35, P = 0.044). Finally, obese subjects had a significantly higher odds ratio of weekly SSBs consumption than non-obese subjects (OR = 3.80, P = 0.003).
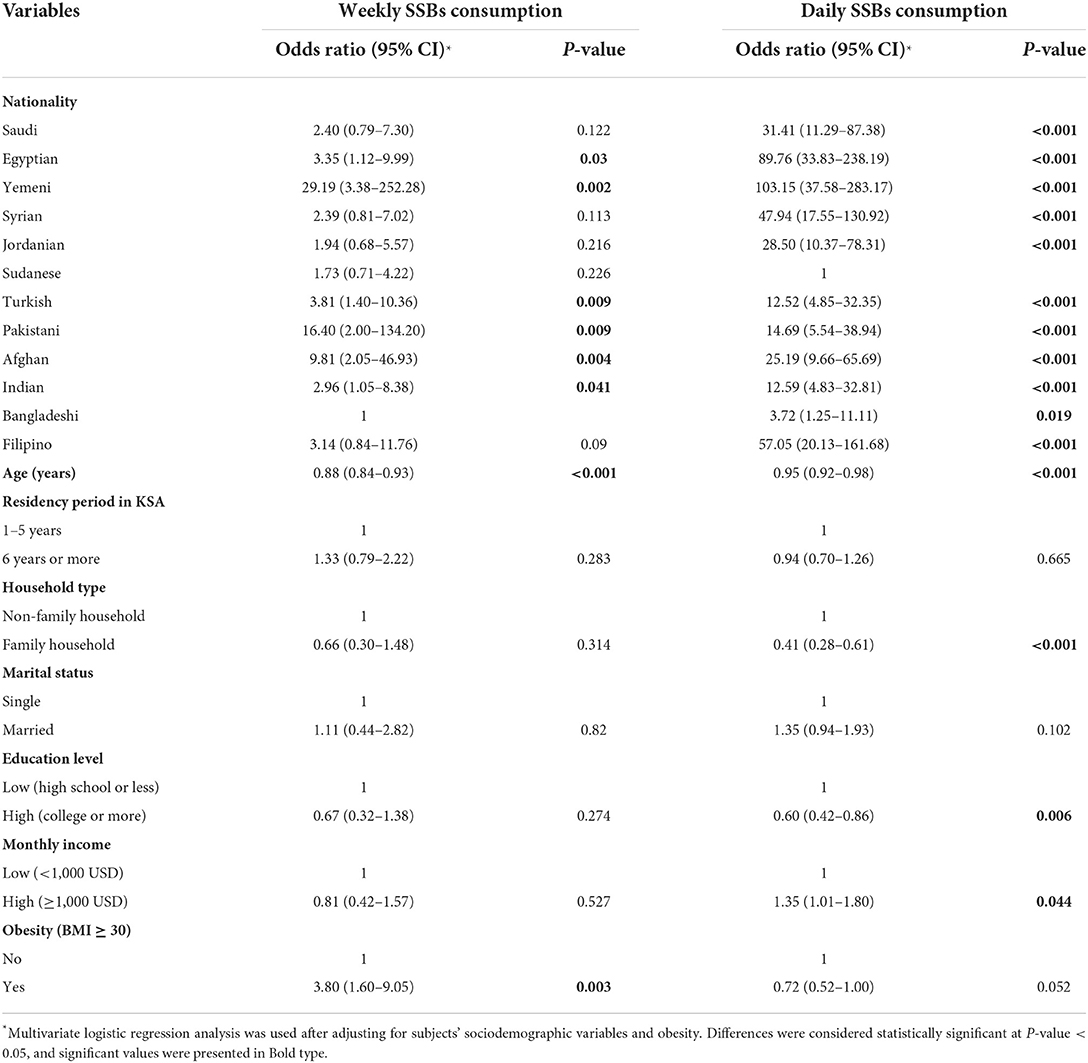
Table 3. Odds ratios of weekly and daily sugar-sweetened beverages (SSBs) consumption among study participants for sociodemographic variables and obesity.
This study explored weekly and daily SSBs consumption rates in a multi-ethnic population of middle-aged men. Our results disclosed that most subjects (93.8%) were weekly consumers of SSBs and about one-third (32.6%) were daily consumers of SSBs. The prevalence of SSBs consumption among adults has been investigated in several studies. According to a recent nationally representative survey from KSA, 71.2% of adults consumed SSBs weekly, while 35.5% consumed SSBs daily. In addition, 65% of middle-aged adults (35–54 years) were weekly SSBs consumers (24). In a national survey of Australian adults, 55.9 and 19.3% of men consumed SSBs weekly and daily, respectively. The rates of weekly and daily SSBs intake in adults aged 31–45 years were 54.7% and 16.3, respectively, while the rates of weekly and daily SSBs intake in adults aged 46–60 years were 41.1 and 12.5%, respectively (10). A Norwegian study reported that SSBs intake rate among adults was 34% (25). Another study indicated that 63.9% of American adults drank SSBs daily. Moreover, the daily consumption rates of regular soda, fruit drinks, and energy/sport drinks were 21, 6.6, and 5.7%, respectively (26). The rate of daily SSBs consumption among British adults was 20.4% (27). Finally, research from New York City reported that 27.5% of adults were daily consumers of SSBs (28).
This study's data showed that participants from different countries consumed SSBs at significantly different rates. This outcome is in line with several earlier research that found a substantial difference in SSBs intake across adults from various countries, regions, or ethnic origins (26, 29, 30). A study that compared the consumption of SSBs across 187 countries spread over 21 global geographical areas discovered significant variation in SSBs consumption. The difference between the top and lowest regional consumption levels was over ten times. East Asia had the lowest intake of SSBs, while the Caribbean had the highest (30). The consumption of SSBs and SSBs subtypes in the United States differed according to where people lived. Adults in the Northeast, South, West, and Midwest consumed daily SSBs at rates of 68.4, 66.7, 61.2, and 58.8%, respectively. According to findings from this study, adults in the Northeast were much more likely (OR = 1.13) to report consuming SSBs on a daily basis than adults in the South, while those in the Midwest (OR = 0.70) and the West (OR = 0.78) were noticeably less likely to do so (26). In another American study, SSBs intake varies depending on ethnicity. Blacks and Hispanic middle-aged and older adults were more likely than Whites to drink SSBs (29). The causes of these differences in SSBs consumption rates by nationality are still unconfirmed. The potential explanations include differences in the ecological factors such as availability and accessibility to SSBs that adults experienced in their original countries during the preceding age stages (31, 32). Other reasons include variations in how they reacted to SSBs marketing advertisements in the country where they lived caused by disparities in language and cultural standards (10, 33). Nevertheless, when initiatives to lower SSBs consumption are developed, disparities in SSBs consumption rates by nationality should be taken into account (34).
Linking SSBs consumption among adults to sociodemographic factors is widely discussed in previous studies (27, 29). Our results observed significant relationships between weekly or daily SSBs consumption and age, household type, education level and monthly income. Our findings agreed with findings from previous studies that reported a higher likelihood of SSBs consumption was linked to younger age (10, 24, 28, 35, 36), living within non-family households (37), and lower education levels (27, 29). Contrarily, our findings conflict with an earlier study which stated that SSBs consumption did not seem to differ between university students living in their family households and those living in non-family households (38), and earlier studies reported that a higher likelihood of SSBs consumption was linked to lower monthly income (27, 29).
Interestingly, our findings supported the link between consuming SSBs every week and obesity. Many adults are affected by obesity, a costly condition with high morbidity and mortality rates (39, 40). Numerous studies support the relationship between SSBs consumption and adulthood obesity and other obesity-related conditions like diabetes and coronary heart disease (6, 41, 42). Several theories have been established to elucidate the relationship between SSBs use and obesity (43). Adults who usually drink SSBs consume significantly more calories, which causes a positive energy balance (44, 45). On any given day, around 50% of United States adults have one or more SSBs servings, and nearly 7% of their daily caloric intake is derived from SSBs (46). Possible mechanisms include decreased satiety, fast fructose absorption, and after-meal hyperglycemia. The absorption of glucose can cause after-meal hyperglycemia when SSBs are drunk, which reduces the carbohydrate-related elevation in serum glucose level (47). Postprandial hyperglycemia causes a cascade of changes, including hyperinsulinemia, glucose uptake by insulin-sensitive tissues, concurrent hypoglycemia to levels lower than fast values, greater appetite driven by the lack of available fuel, and overeating (48). Furthermore, fructose is processed largely in the liver. Fast fructose absorption from SSBs may overload hepatic metabolic processes, promote lipogenesis, and result in physiological abnormalities such as insulin resistance and excessive fat accumulation (49). Fructose consumption switch on hepatic de novo lipogenesis through stimulating two master transcriptional regulators: SREBP-1c and ChREBP. As this process is independent of insulin secretion, fructose consumption can encourage hepatic lipid buildup even in the presence of insulin resistance. Furthermore, fructose intake causes ATP depletion and suppresses the oxidation of fatty acids in the hepatocytes' mitochondria, promoting fat accumulation in the liver and secreting triglycerides-rich VLDL particles. Overall, fructose intake promotes dyslipidemia, cardiometabolic risk factors and insulin resistance, and elevates visceral fat deposit in overweight and obese adults (50, 51).
Several environmental and governmental modifications need to be made to lower SSBs use in the community (11). Limiting the availability of these foods in public places and reducing exposure to SSBs commercial advertisements in the media may help reduce SSBs consumption (10). Moreover, raising public knowledge of the harmful health effects of SSBs use through public health education initiatives may aid efforts to restrict overall SSBs intake (8). In addition, campaigns that encourage substituting SSBs with energy-free liquids like water should be considered (52). Global public health organizations have encouraged governments to intervene due to the widespread and fast increases in SSBs intake. Taxing the price of SSBs is one practical solution to decrease SSBs intake (53, 54).
Few limitations apply to our study. The significant associations between outcome measures and their predictors could not be used to infer causality because of the cross-sectional design. Moreover, women were not involved in the present study. Another drawback was using a self-reported frequency approach to collect consumption data, which relied on participants' memories. Compared to evaluating the consumption using a 24-h recall method, this approach can result in an underestimated SSBs intake. The definition of SSBs is diverse across studies limiting the opportunity to compare our results with previous studies. Finally, this study could not account for calorie intake when analyzing the relationship between SSBs consumption and obesity due to a lack of energy intake data. Despite these limitations, this study still presents valuable data about the rates of SSBs consumption and associated determinants.
According to this study, middle-aged men who live in KSA consumed SSBs at relatively high rates. The results demonstrated that middle-aged men from different countries who reside in KSA drink SSBs at noticeably varied rates. The findings also show a connection between SSBs consumption, certain sociodemographic variables, and obesity.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Research Ethics Committee at Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia. The patients/participants provided their written informed consent to participate in this study.
RIA, RAA, NAls, and NAlF: conceptualization. MA, HA, and JA: methodology. NAlK, RIA, and MA: software. MA and MB: validation. HA and NAls: formal analysis. RAA and NAlK: investigation. NAlF and MB: resources. RAA, HA, and NAls: data curation. NAlF, NAlK, JA, and RIA: writing—original draft preparation. RAA, MB, NAls, and HA: writing—review and editing. JA, MA, and MB: visualization. NAlF: supervision. JA: project administration. RIA and NAlK: funding acquisition. All authors have read and agreed to the published version of the manuscript.
This research was funded by Princess Nourah bint Abdulrahman University Researchers Supporting Project number (PNURSP2022R131), Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia.
The authors would like to thank Princess Nourah bint Abdulrahman University Researchers Supporting Project number (PNURSP2022R131), Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia, for supporting this research.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
KSA, Kingdom of Saudi Arabia; BMI, Body Mass index; OR, odds ratio.
1. Bleich SN, Vercammen KA, Koma JW, Li Z. Trends in beverage consumption among children and adults, 2003-2014. Obesity. (2018) 26:432–41. doi: 10.1002/oby.22056
2. CDC. The CDC Guide to Strategies for Reducing the Consumption of Sugar-Sweetened Beverages. Atlanta, GA: Centers for Disease Control and Prevention (2010).
3. Sharkey J, Johnson C, Dean W. Less-healthy eating behaviors have a greater association with a high level of sugar-sweetened beverage consumption among rural adults than among urban adults. Food Nutr Res. (2011) 55:5819. doi: 10.3402/fnr.v55i0.5819
4. Vartanian LR, Schwartz MB, Brownell KD. Effects of soft drink consumption on nutrition and health: a systematic review and meta-analysis. Am J Public Health. (2007) 97:667–75. doi: 10.2105/AJPH.2005.083782
5. Bernabé E, Vehkalahti MM, Sheiham A, Aromaa A, Suominen AL. Sugar-sweetened beverages and dental caries in adults: a 4-year prospective study. J Dent. (2014) 42:952–8. doi: 10.1016/j.jdent.2014.04.011
6. Malik VS, Hu FB. The role of sugar-sweetened beverages in the global epidemics of obesity and chronic diseases. Nat Rev Endocrinol. (2022) 18:205–18. doi: 10.1038/s41574-021-00627-6
7. Monnard CR, Grasser EK. Perspective: cardiovascular responses to sugar-sweetened beverages in humans: a narrative review with potential hemodynamic mechanisms. Adv Nutr. (2018) 9:70–7. doi: 10.1093/advances/nmx023
8. Pomeranz JL. Advanced policy options to regulate sugar-sweetened beverages to support public health. J Public Health Policy. (2012) 33:75–88. doi: 10.1057/jphp.2011.46
9. WHO. Guideline: Sugars Intake for Adults And Children. Geneva: World Health Organization (2015). Available online at: https://www.who.int/publications/i/item/9789241549028 (accessed July 5, 2022).
10. Miller C, Ettridge K, Wakefield M, Pettigrew S, Coveney J, Roder D, et al. Consumption of sugar-sweetened beverages, juice, artificially-sweetened soda and bottled water: an Australian population study. Nutrients. (2020) 12:817. doi: 10.3390/nu12030817
11. Vercammen KA, Moran AJ, Soto MJ, Kennedy-Shaffer L, Bleich SN. Decreasing trends in heavy sugar-sweetened beverage consumption in the United States, 2003 to 2016. J Acad Nutr Diet. (2020) 120:1974–85. doi: 10.1016/j.jand.2020.07.012
12. Al-Rethaiaa AS, Fahmy AEA, Al-Shwaiyat NM. Obesity and eating habits among college students in Saudi Arabia: a cross sectional study. Nutr J. (2010) 9:39. doi: 10.1186/1475-2891-9-39
13. ALFaris NA, Al-Tamimi JZ, Al-Jobair MO, Al-Shwaiyat NM. Trends of fast food consumption among adolescent and young adult Saudi girls living in Riyadh. Food Nutr Res. (2015) 59:26488. doi: 10.3402/fnr.v59.26488
14. Benajiba N, Mahboub SM. Consumption of sugar-sweetened soft drinks among saudi adults: assessing patterns and identifying influencing factors using principal component analysis. Pak J Nutr. (2019) 18:401–7. doi: 10.3923/pjn.2019.401.407
15. AlFaris NA, Alshwaiyat NM, AlTamimi JZ, Alagal RI, Al-Jamal HA, AlKehayez NM. Physical activity levels of a multi-ethnic population of middle-aged men living in Saudi Arabia and factors associated with physical inactivity. Int J Public Health. (2022) 66:1604328. doi: 10.3389/ijph.2021.1604328
16. AlTamimi JZ, Alagal RI, AlKehayez NM, Alshwaiyat NM, Al-Jamal HA, AlFaris NA. Physical activity levels of a multi-ethnic population of young men living in Saudi Arabia and factors associated with physical inactivity. Front Public Health. (2022) 9:734968. doi: 10.3389/fpubh.2021.734968
17. De Bel-Air F. Demography, migration labour market in Saudi Arabia. Gulf Labour Markets Migration. European University Institute (EUI) Gulf Research Center (GRC). GLMM - EN - No. 1/2014 (2014). Available online at: https://cadmus.eui.eu/bitstream/handle/1814/32151/GLMM%20ExpNote_01-2014.pdf (accessed July 5, 2022).
18. General Authority of Statistics of Saudi Arabia. Population by Gender, Age Groups and Nationality (Saudi/Non-Saudi), The Fifth Saudi Census. (2010). Available online at: https://www.stats.gov.sa/sites/default/files/ar-census2010-dtl-result_2_1.pdf (accessed July 5, 2022).
19. Alagal RI, AlFaris NA, AlTamimi JZ, Alshwaiyat NM, Ahmad A, Alzaheb RA, et al. Differences in overweight and obesity prevalence among young men from twelve middle Eastern and Asian countries living in Saudi Arabia. Healthcare. (2022) 10:690. doi: 10.3390/healthcare10040690
20. AlFaris NA, Alshwaiyat NM, Alkhalidy H, Alagal RI, AlTamimi JZ, AlKehayez NM. Breakfast skipping in a multi-ethnic population of middle-aged men and relationship with sociodemographic variables and weight status. Front Nutr. (2022) 8:761383. doi: 10.3389/fnut.2021.761383
21. AlTamimi JZ, Alshwaiyat NM, AlFaris NA, AlKehayez NM, Ahmad A, Alagal RI. Differences in overweight and obesity prevalence in middle-aged men from twelve middle eastern and Asian countries living in Saudi Arabia. Int J Gen Med. (2022) 15:3333–43. doi: 10.2147/IJGM.S359639
22. AlTamimi JZ, Alshwaiyat NM, Alkhalidy H, AlFaris NA, AlKehayez NM, Alagal RI. Breakfast skipping among a multi-ethnic population of young men and relationship with sociodemographic determinants and weight status. Int J Environ Res Public Health. (2022) 19:2903. doi: 10.3390/ijerph19052903
24. Al-Hanawi MK, Ahmed MU, Alshareef N, Qattan AMN, Pulok MH. Determinants of sugar-sweetened beverage consumption among the Saudi adults: findings from a nationally representative survey. Front Nutr. (2022) 9:744116. doi: 10.3389/fnut.2022.744116
25. Paulsen MM, Myhre JB, Andersen LF. Beverage consumption patterns among Norwegian adults. Nutrients. (2016) 8:561. doi: 10.3390/nu8090561
26. Park S, McGuire LC, Galuska DA. Regional differences in sugar-sweetened beverage intake among US adults. J Acad Nutr Diet. (2015) 115:1996–2002. doi: 10.1016/j.jand.2015.06.010
27. Barrett P, Imamura F, Brage S, Griffin SJ, Wareham NJ, Forouhi NG. Sociodemographic, lifestyle and behavioural factors associated with consumption of sweetened beverages among adults in Cambridgeshire, UK: the Fenland Study. Public Health Nutr. (2017) 20:2766–77. doi: 10.1017/S136898001700177X
28. Rehm CD, Matte TD, Van Wye G, Young C, Frieden TR. Demographic and behavioral factors associated with daily sugar-sweetened soda consumption in New York City adults. J Urban Health. (2008) 85:375–85. doi: 10.1007/s11524-008-9269-8
29. Han E, Powell LM. Consumption patterns of sugar-sweetened beverages in the United States. J Acad Nutr Diet. (2013) 113:43–53. doi: 10.1016/j.jand.2012.09.016
30. Singh GM, Micha R, Khatibzadeh S, Shi P, Lim S, Andrews KG, et al. Global, regional, and national consumption of sugar-sweetened beverages, fruit juices, and milk: a systematic assessment of beverage intake in 187 countries. PLoS ONE. (2015) 10:e0124845. doi: 10.1371/journal.pone.0124845
31. Elfassy T, Adjoian T, Lent M. Sugary drink consumption among NYC children, youth, and adults: disparities persist over time, 2007–2015. J Community Health. (2019) 44:297–306. doi: 10.1007/s10900-018-0587-9
32. Fiorito LM, Marini M, Mitchell DC, Smiciklas-Wright H, Birch LL. Girls' early sweetened carbonated beverage intake predicts different patterns of beverage and nutrient intake across childhood and adolescence. J Am Diet Assoc. (2010) 110:543–50. doi: 10.1016/j.jada.2009.12.027
33. Morley BC, Niven PH, Dixon HG, Swanson MG, McAleese AB, Wakefield MA. Controlled cohort evaluation of the LiveLighter mass media campaign's impact on adults' reported consumption of sugar-sweetened beverages. BMJ Open. (2018) 8:e019574. doi: 10.1136/bmjopen-2017-019574
34. Levy DT, Friend KB, Wang YC. A review of the literature on policies directed at the youth consumption of sugar sweetened beverages. Adv Nutr. (2011) 2:182S−200S. doi: 10.3945/an.111.000356
35. Pollard CM, Meng X, Hendrie GA, Hendrie D, Sullivan D, Pratt IS, et al. Obesity, socio-demographic and attitudinal factors associated with sugar-sweetened beverage consumption: Australian evidence. Aust N Z J Public Health. (2016) 40:71–7. doi: 10.1111/1753-6405.12482
36. Mendy VL, Vargas R, Payton M, Cannon-Smith G. Association between consumption of sugar-sweetened beverages and sociodemographic characteristics among Mississippi adults. Prev Chronic Dis. (2017) 14:E137. doi: 10.5888/pcd14.170268
37. Nicklas TA, Baranowski T, Cullen KW, Berenson G. Eating patterns, dietary quality and obesity. J Am Coll Nutr. (2001) 20:599–608. doi: 10.1080/07315724.2001.10719064
38. Bawadi H, Khataybeh T, Obeidat B, Kerkadi A, Tayyem R, Banks AD, et al. Sugar-sweetened beverages contribute significantly to college students' daily caloric intake in Jordan: soft drinks are not the major contributor. Nutrients. (2019) 11:1058. doi: 10.3390/nu11051058
39. Blüher M. Obesity: global epidemiology and pathogenesis. Nat Rev Endocrinol. (2019) 15:288–98. doi: 10.1038/s41574-019-0176-8
40. Alshwaiyat NM, Ahmad A, Wan Hassan WMR, Al-Jamal HAN. Association between obesity and iron deficiency (review). Exp Ther Med. (2021) 22:1268. doi: 10.3892/etm.2021.10703
41. De Koning L, Malik VS, Rimm EB, Willett WC, Hu FB. Sugar-sweetened and artificially sweetened beverage consumption and risk of type 2 diabetes in men. Am J Clin Nutr. (2011) 93:1321–7. doi: 10.3945/ajcn.110.007922
42. De Koning L, Malik VS, Kellogg MD, Rimm EB, Willett WC, Hu FB. Sweetened beverage consumption, incident coronary heart disease, and biomarkers of risk in men. Circulation. (2012) 125:1735–41. doi: 10.1161/CIRCULATIONAHA.111.067017
43. Pereira MA. The possible role of sugar-sweetened beverages in obesity etiology: a review of the evidence. Int J Obes. (2006) 30:S28–36. doi: 10.1038/sj.ijo.0803489
44. Bachman CM, Baranowski T, Nicklas TA. Is there an association between sweetened beverages and adiposity? Nutr Rev. (2006) 64:153–74. doi: 10.1111/j.1753-4887.2006.tb00199.x
45. Malik VS, Pan A, Willett WC, Hu FB. Sugar-sweetened beverages and weight gain in children and adults: a systematic review and meta-analysis. Am J Clin Nutr. (2013) 98:1084–102. doi: 10.3945/ajcn.113.058362
46. Kit BK, Fakhouri TH, Park S, Nielsen SJ, Ogden CL. Trends in sugar-sweetened beverage consumption among youth and adults in the United States: 1999–2010. Am J Clin Nutr. (2013) 98:180–8. doi: 10.3945/ajcn.112.057943
47. Ebbeling CB. Sugar-sweetened beverages and body weight. Curr Opin Lipidol. (2014) 25:1–7. doi: 10.1097/MOL.0000000000000035
48. Ludwig DS. The glycemic index: physiological mechanisms relating to obesity, diabetes, and cardiovascular disease. JAMA. (2002) 287:2414–23. doi: 10.1001/jama.287.18.2414
49. Ludwig DS. Examining the health effects of fructose. JAMA. (2013) 310:33–4. doi: 10.1001/jama.2013.6562
50. Stanhope KL, Schwarz JM, Keim NL, Griffen SC, Bremer AA, Graham JL, et al. Consuming fructose-sweetened, not glucose-sweetened, beverages increases visceral adiposity and lipids and decreases insulin sensitivity in overweight/obese humans. J Clin Invest. (2009) 119:1322–34. doi: 10.1172/JCI37385
51. Taskinen MR, Söderlund S, Bogl LH, Hakkarainen A, Matikainen N, Pietiläinen KH, et al. Adverse effects of fructose on cardiometabolic risk factors and hepatic lipid metabolism in subjects with abdominal obesity. J Intern Med. (2017) 282:187–201. doi: 10.1111/joim.12632
52. Colchero MA, Molina M, Guerrero-López CM. After Mexico implemented a tax, purchases of sugar-sweetened beverages decreased and water increased: difference by place of residence, household composition, and income level. J Nutr. (2017) 147:1552–7. doi: 10.3945/jn.117.251892
53. Roberto CA, Lawman HG, LeVasseur MT, Mitra N, Peterhans A, Herring B, et al. Association of a beverage tax on sugar-sweetened and artificially sweetened beverages with changes in beverage prices and sales at chain retailers in a large urban setting. JAMA. (2019) 321:1799–810. doi: 10.1001/jama.2019.4249
Keywords: sugar-sweetened beverages, multi-ethnic, middle-aged men, sociodemographic, obesity
Citation: AlFaris NA, Alshwaiyat NM, Alkhalidy H, AlTamimi JZ, Alagal RI, Alsaikan RA, Alsemari MA, BinMowyna MN and AlKehayez NM (2022) Sugar-sweetened beverages consumption in a multi-ethnic population of middle-aged men and association with sociodemographic variables and obesity. Front. Nutr. 9:987048. doi: 10.3389/fnut.2022.987048
Received: 05 July 2022; Accepted: 04 August 2022;
Published: 30 August 2022.
Edited by:
Evelyn Frias-Toral, Catholic University of Santiago de Guayaquil, EcuadorReviewed by:
Claudia Vetrani, University of Naples Federico II, ItalyCopyright © 2022 AlFaris, Alshwaiyat, Alkhalidy, AlTamimi, Alagal, Alsaikan, Alsemari, BinMowyna and AlKehayez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Nora M. AlKehayez, bm1hbGtlaGF5ZXpAcG51LmVkdS5zYQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.