Probiotics, Prebiotics, and Synbiotics Improve Uremic, Inflammatory, and Gastrointestinal Symptoms in End-Stage Renal Disease With Dialysis: A Network Meta-Analysis of Randomized Controlled Trials
 Zixian Yu†
Zixian Yu† Jin Zhao
Jin Zhao Yunlong Qin
Yunlong Qin Yumeng Zhang
Yumeng Zhang Shiren Sun
Shiren SunYu, Z., Zhao, J., Qin, Y., Wang, Y., Zhang, Y., and Sun, S. (2022). Front. Nutr. 9:850425. doi: 10.3389/fnut.2022.850425
In the published article, there was an error in Figure 6 as published. The panel C (indole-3-acetic acid, IAA) and panel D (malondialdehyde, MDA) in Figure 6 is the same as the panel C (tumor necrosis factor-α, TNF-α) and panel D (endotoxin) in Figure 4. The corrected Figure 6 and its caption appear below.
FIGURE 6
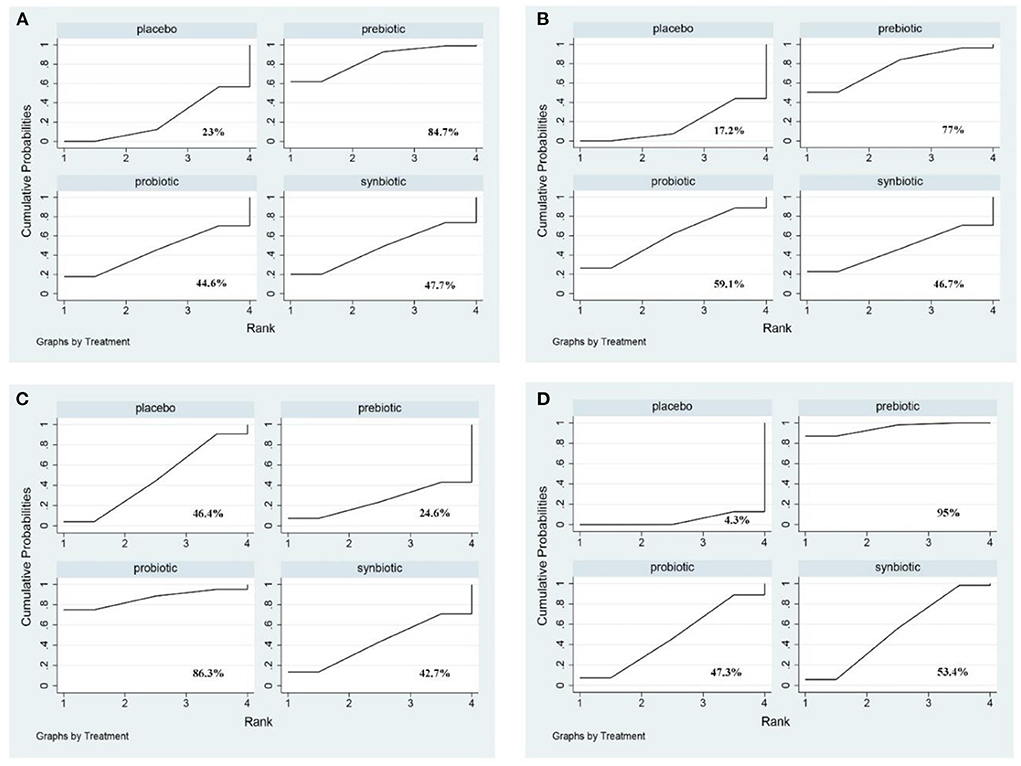
Figure 6. The cumulative ranking area of uremic toxins; Treatment strategies were ranked based on their probability of reducing (A) indoxyl sulfate (IS); (B) p-cresyl sulfate (PCS); (C) indole-3-acetic acid (IAA); (D) malondialdehyde (MDA) by cumulative ranking area (SUCRA). The greater the probability, the better the effect.
In the published article, there was an error in Table 1 as published. The number of males in Liu et al. is wrong, 28 should be changed to 23. The corrected Table 1 and its caption appear below.
TABLE 1
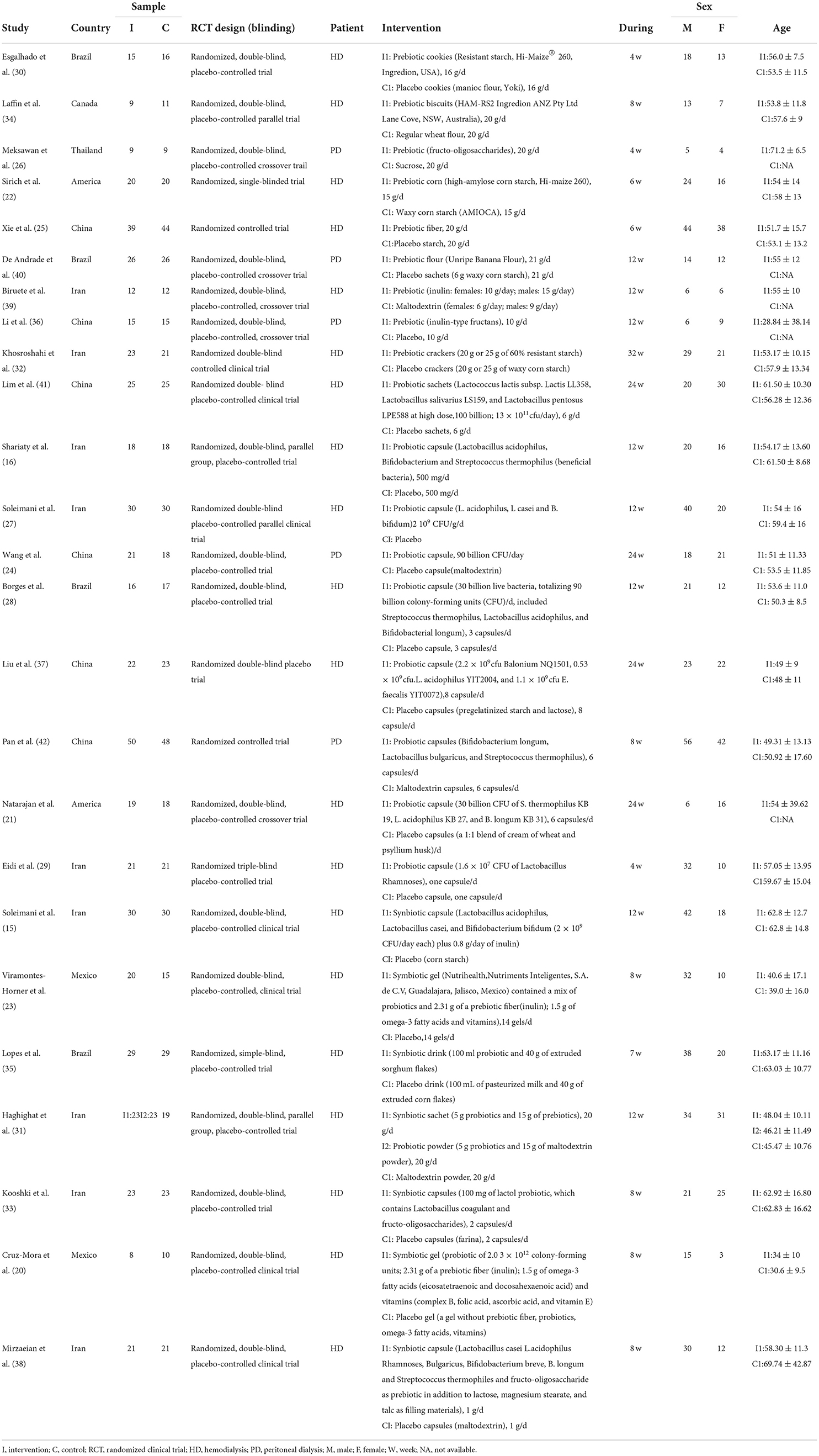
Table 1. Characteristics of included Interventions in dialysis patients.
In the published article, there was an error in Supplementary Figure 6. Panel A (BUN) is the same as panel B (Creatinine). The correct material statement appears below.
Supplementary Figure 6 Results of direct comparisons for other clinical outcomes. Forest plot of the effect of prebiotic, probiotic, and synbiotic supplementation on (A) BUN (mg/dl); (B) Creatinine (mg/dl); (C) Urea (mg/dl); (D) Uric acid (mg/dl).
In the published article, there was an error in Supplementary Figure 15. The figure legend of (E) p-cresyl sulfate (PCS) should be replaced with (E) Malondialdehyde (MDA), and the original material statement was Supplementary Figure 15. Sensitivity analysis. Sensitivity analysis for the network of (A) C-reactive protein (CRP); (B) Interleukin-6(IL-6); (C) tumor necrosis factor-α (TNF-α); (D) Indoxyl sulfate (IS); (E) p-cresyl sulfate (PCS); (F) Urea. The correct material statement appears below.
Supplementary Figure 15 Sensitivity analysis. Sensitivity analysis for the network of (A) C-reactive protein (CRP); (B) Interleukin- 6(IL-6); (C) tumor necrosis factor-α (TNF-α); (D) Indoxyl sulfate (IS); (E) Malondialdehyde (MDA); (F) Urea.
In the published article, there was an error. “IAA” should be changed to “MDA,” “96.8%” should be changed to “95%,” “Synbiotics” should be changed to “Probiotics,” “MDA” should be changed to “IAA,” “95.6%” should be changed to “86.3%” in the Results. A correction has been made to Results, Network Meta-Analysis, Uremic Toxins. The corrected sentence appears below:
“Uremic toxins including IS, PCS, IAA, and MDA were evaluated. The outcome revealed prebiotics were superior in declining IS (prebiotics: SMD −0.43; 95% CI [−0.81, −0.05]), prebiotics and synbiotics were effective supplements on the alteration of MDA level (prebiotics: SMD −1.88; 95% CI [−3.02, −0.75]; synbiotics: SMD −0.85; 95% CI [−1.67, −0.02]) but no supplements significantly declined serum PCS, and IAA (Figure 5 and Supplementary Figure 11). With regard to IS, PCS, and MDA, prebiotics were ranked as the first therapeutic option, where the SUCRA were 84.7, 77, and 95%, respectively. Probiotics had the highest possibility in serum IAA level (SUCRA = 86.3%) (Figure 6).”
In the published article, there was an error. “Synbiotics” should be changed to “prebiotics” in the Discussion section, and “respectively” needed to be removed from another sentence. A correction has been made to Discussion, Paragraph 3. The corrected sentence appears below:
“Prebiotics were superior in reducing serum IS, prebiotics were rated as best in reducing MDA level. The accumulation of metabolic toxins in the blood is closely associated with the deteriorating progression of CKD to ESRD, part of the toxins, such as protein-bound uremic toxins, come from intestinal flora, and dialysis is not potentially removed (9, 45). The efficacy of pro/pre/syn-biotics in lowering uremic toxins has been demonstrated by previous meta-analysis (13, 49). Our pairwise comparison found the same results and notably we further suggested that prebiotics and synbiotics are the most effective supplements. Prebiotics are some non-digestible food ingredients, regarded as a vital dietary supplement for ESRD patients with dietary restriction of protein intake, increasing the concentration of short-chain fatty acids (SCFAs), which benefit metabolites produced by gut bacterium (12, 50). Decreased SCFAs were regarded as one of the main mechanisms of the production of uremic toxins, which may also be the reason why prebiotics were more effective than probiotics and synbiotics. MDA is a low-molecular-weight solution that participates in oxidative stress, connecting with the progress of CKD and its cardiovascular complications (51). Seven randomized controlled trials were introduced in the study of Nguyen et al. (14), who found that MDA was significantly reduced in hemodialysis patients after taking three supplements. Several studies also have demonstrated that synbiotics might increase the expression of the antioxidant gene SOD and GPX in the gut by targeting gut bacteria to activate oxidative stability (52, 53). Current studies support the evidence that taking prebiotics and synbiotics have the most beneficial influence in reducing IS and MDA. Whereas, it is of great importance to emphasize that the change of uremic toxins is the result of multiple comparisons among the three drugs, combining small samples of studies and different follow-up times, which declined the strength of evidence, contributing to the accuracy of evidence is low. Thus, launching large clinical trials is important to evaluate the function of pro/pre/syn-biotics in reducing uremic toxins, especially protein-bound uremic toxins.”
The authors apologize for these errors and state that this does not change the scientific conclusions of the article in any way. The original article has been updated.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Keywords: probiotic, prebiotic, synbiotic, network meta-analysis, end-stage renal disease (ESRD)
Citation: Yu Z, Zhao J, Qin Y, Wang Y, Zhang Y and Sun S (2022) Corrigendum: Probiotics, prebiotics, and synbiotics improve uremic, inflammatory, and gastrointestinal symptoms in end-stage renal disease with dialysis: A network meta-analysis of randomized controlled trials. Front. Nutr. 9:984187. doi: 10.3389/fnut.2022.984187
Received: 01 July 2022; Accepted: 11 July 2022;
Published: 27 July 2022.
Edited and reviewed by: Alice Sabatino, University of Parma, Italy
Copyright © 2022 Yu, Zhao, Qin, Wang, Zhang and Sun. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Shiren Sun, sunshiren@medmail.com.cn
†These authors have contributed equally to this work and share first authorship