 Qi Long
Qi Long Yijie Feng2†
Yijie Feng2† Fei Chen
Fei Chen Wenqiao Wang
Wenqiao Wang Shanshan Mao
Shanshan Mao
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Nutr., 15 August 2022
Sec. Clinical Nutrition
Volume 9 - 2022 | https://doi.org/10.3389/fnut.2022.960006
This article is part of the Research TopicOxidative Stress and Neuroinflammatory Responses Associated with Metal Toxicity in Brain DisordersView all 5 articles
Background and aims: Children with spinal muscular atrophy (SMA) have a high rate of dyslipidaemia, which is a risk factor of vital importance for cardiovascular diseases in adulthood. Studies have demonstrated that the serum zinc level is associated with lipid profiles in the general population as well as in individuals diagnosed with obesity or diabetes. The purpose of this study was to evaluate the relationship between serum zinc level and lipid profiles in children with SMA.
Methods: This cross-sectional study was launched in a tertiary children's medical center in China and involved pediatric patients with SMA under the management of a multidisciplinary team of outpatient services from July 2019 to July 2021. Anthropometric information, general clinical data, serum zinc level, lipid profiles, and body composition data were collected. Multivariate analysis was used for a thorough inquiry on the association between the serum zinc level and lipid profiles.
Results: Among the 112 patients with SMA [median (IQR) age 5.54 years (2.75–8.29), 58.04% female], who fulfilled the inclusion criteria of the study, dyslipidaemia was detected in 60 patients (53.57%). Based on multivariable linear regression, serum zinc level was positively associated with high-density lipoprotein cholesterol (HDL-C; β = 1.63, 95% CI = 0.44–3.22) and apolipoprotein A1 (APO A1; β = 2.94, 95% CI = 0.03–5.85) levels, independently of age, sex, type, activity, percentage of body fat, and body mass index. As the serum zinc level increased by 10 μmol/L, the risk of low APO A1 levels decreased by 35% (OR = 0.65, 95% CI = 0.44–0.97) according to multivariable logistic regression analyses.
Conclusion: Serum zinc concentration was positively correlated with HDL-C and APO A1 levels among children with SMA. We suggest measures to correct the lower level of serum zinc to improve HDL-C and APO A1 levels.
Spinal muscular atrophy (SMA) is a rare genetic neuromuscular disease with an autosomal recessive inheritance pattern. The most common type is 5qSMA, which is caused by a homozygous mutation or deletion in the survival motor neuron 1 gene positioned on chromosome 5q11.2–q13.3 (1). The worldwide incidence of SMA is ~1/10,000 live births, and the carrier frequency is 1/42 in the Chinese population (2, 3). SMA manifests as progressive muscle weakness and atrophy resulting from motor neurons' pathological degeneration in the anterior horn of the spinal cord, which is often accompanied by organ damage in the respiratory, digestive, and skeletal systems (4).
In recent years, drug treatment for SMA has achieved unprecedented progress (5). Despite medication development, experts have unanimously pointed out that SMA standardized treatment and individualized management always require the cooperation of a patient-centered multidisciplinary team and that nutrition management is indispensable (6, 7). Over the last few years, research in SMA nutrition has focused mainly on evaluating the nutritional status, body composition, dietary intake, bone health, and individual energy demand (8, 9). Moreover, recent literature has described metabolic abnormalities in SMA, of which dysregulation of the lipid profiles is the first and most frequently studied issue (10–12). Studies on lipid metabolism in patients with SMA have confirmed abnormal levels of fatty acid oxidative metabolites and increased susceptibility to dyslipidaemia (11, 13).
Prevention and treatment of dyslipidaemia is a challenging clinical issue. The therapeutic management of childhood dyslipidaemia mainly consists of lifestyle adjustment, emphasizing suitable dietary patterns, and increased physical activity for early prevention of atherosclerosis and coronary artery diseases (14–16). However, in children with SMA, improvement through exercise is more difficult because of motor dysfunction.
Zinc is considered one of the essential micronutrients for the human body and plays a significant role in the metabolism of lipids, proteins, and carbohydrates (17). Studies have shown that individuals with an inordinate amount of body fat have lower serum zinc levels (18). Research shows that, in comparison with the general population, patients with SMA often have a decreased fat-free mass and an increased fat mass (19). However, little research has been conducted on serum zinc levels in patients with SMA. It has been implied that zinc insufficiency may disrupt the energy generation process, and thus adipose tissue is shaped (17). Under conditions of low blood zinc level, lipid management is impaired, causing a rise in triglycerides (TG), total cholesterol (TC), and low-density lipoprotein cholesterol (LDL-C), as well as a decrease in high-density lipoprotein cholesterol (HDL-C) levels in adults, which in turn leads to obesity, metabolic syndrome, and diabetes (20–23). Zinc supplementation can improve blood lipid levels, thus reducing morbidity and mortality associated with cardiovascular diseases (24).
This study was designed to explore the potential relationship between serum zinc level and lipid profiles in children with SMA and provides new treatment strategies for reducing the incidence of dyslipidaemia.
This cross-sectional study was prospectively carried out in an outpatient department of our hospital from July 2019 to July 2021. The inclusion criteria were as follows: (1) diagnosis of 5qSMA by genetic testing; (2) age < 18 years; (3) provision of consent to take part in this study. Those who met the following criteria were excluded: (1) concomitant presence of any other disease or a recent acute medical history; (2) a history of spinal fusion surgery or the presence of metal surgical implants in the body; and (3) having received disease-modifying treatment. Ethical approval was obtained from the Ethics Committee of the Children's Hospital of the Zhejiang University School of Medicine (2019-IRB-171). Written informed consent was acquired from the participants and their guardians. The selection procedure is illustrated in Figure 1; a total of 112 patients were finally included.

Figure 1. Flow chart showing patient selection.
Quantitative analyses of serum zinc levels were performed utilizing a multichannel atomic absorption spectrophotometer-MB5 (Beijing Persee General Instrument Company Limited, Beijing, China).
Blood samples for lipid tests were collected under fasting conditions. Serum TG, TC, APO A1, APO B, HDL-C, and LDL-C levels were measured using an automatic biochemical analyser (Beckman Coulter Inc., USA). The cut-off points for lipids recommended by the National Cholesterol Education Program were as follows: LDL-C ≥130 mg/dl, TG ≥100 mg/dl (0–9 years), TG ≥130 mg/dl (10–19 years), TC ≥200 mg/dl, HDL-C <40 mg/dl, APO B ≥110 mg/dl, and APO A1 <115 mg/dl (25).
The covariates in this study included age, sex, body mass index (BMI), disease classification, activity, and percentage of body fat. Anthropometric data were collected by professionally trained clinical research coordinators. Body weight was measured using a lever scale (electronic scale for babies) with an accuracy of 50 g. Height was measured using a baby height-measuring board for children under 2 years old and a height-measuring instrument with an accuracy of 0.1 cm for patients over 2 years old. When the patient could not stand, the height was replaced by the arm span. The BMI was computed as the ratio of weight to height squared (kg/m2).
Disease classification was performed according to the maximum athletic ability achieved. The degree of activity was based on currently achievable athletic ability. Fat mass was obtained by an InBody S10 body composition analyser (Biospace, Seoul, Korea). This assessment was carried out after at least 8 h of fasting with the patients in a sitting posture with the legs set apart and arms not touching the torso. The fat mass divided by the body weight was used as the percentage of body fat.
Quantitative variables are described as median with range (quartile) or mean ± standard deviation, and frequencies with percentages are used to describe binary variables. The serum zinc level cut-off was taken as 75 μmol/L. We divided the patients into two groups based on their serum zinc median level. To compare the differences between the two groups, we used chi-square tests or Fisher's exact test for categorical variables and Student's t-test or the Mann–Whitney U-test for quantitative variables. Moreover, logistic and linear regression models were applied to analyse the association between the serum zinc level and lipid profiles adjusted for major covariates, including age, sex, BMI, disease classification, activity, and percentage of body fat (univariate and multivariate analyses). Multiple imputations with chained equations accounted for the missing data on the percentage of body fat. Statistical software packages R (http://www.R-project.org, The R Foundation) and Empowerstats (http://www.empowerstats.com, X&Y Solutions, Inc., Boston, MA, USA) were utilized to perform the analyses mentioned above.
A total of 112 participants (65 women and 47 men) were enrolled: 16 with type I, 57 with type II, and 39 with type III SMA. The baseline characteristics of the study participants, divided by the median serum zinc level, are shown in Table 1. No differences were observed in sex, activity, BMI, or percentage of body fat (all P < 0.05), whereas differences in the age and types of SMA between the two groups (all P > 0.05) were found to be significant. Over half (53.57%) of the patients with SMA tested positive for at least one out of the six indicators for laboratory-defined dyslipidaemia (Table 1). The prevalence of abnormal TC, LDL-C, HDL-C, TG, APO A1, and APO B levels ranged from 4.46 to 25.90%. We found that TG, HDL-C, and APO A1 levels in the two groups were significantly different (i.e., serum zinc levels increased with a decrease in TG and an increase in HDL-C and APO A1 levels).
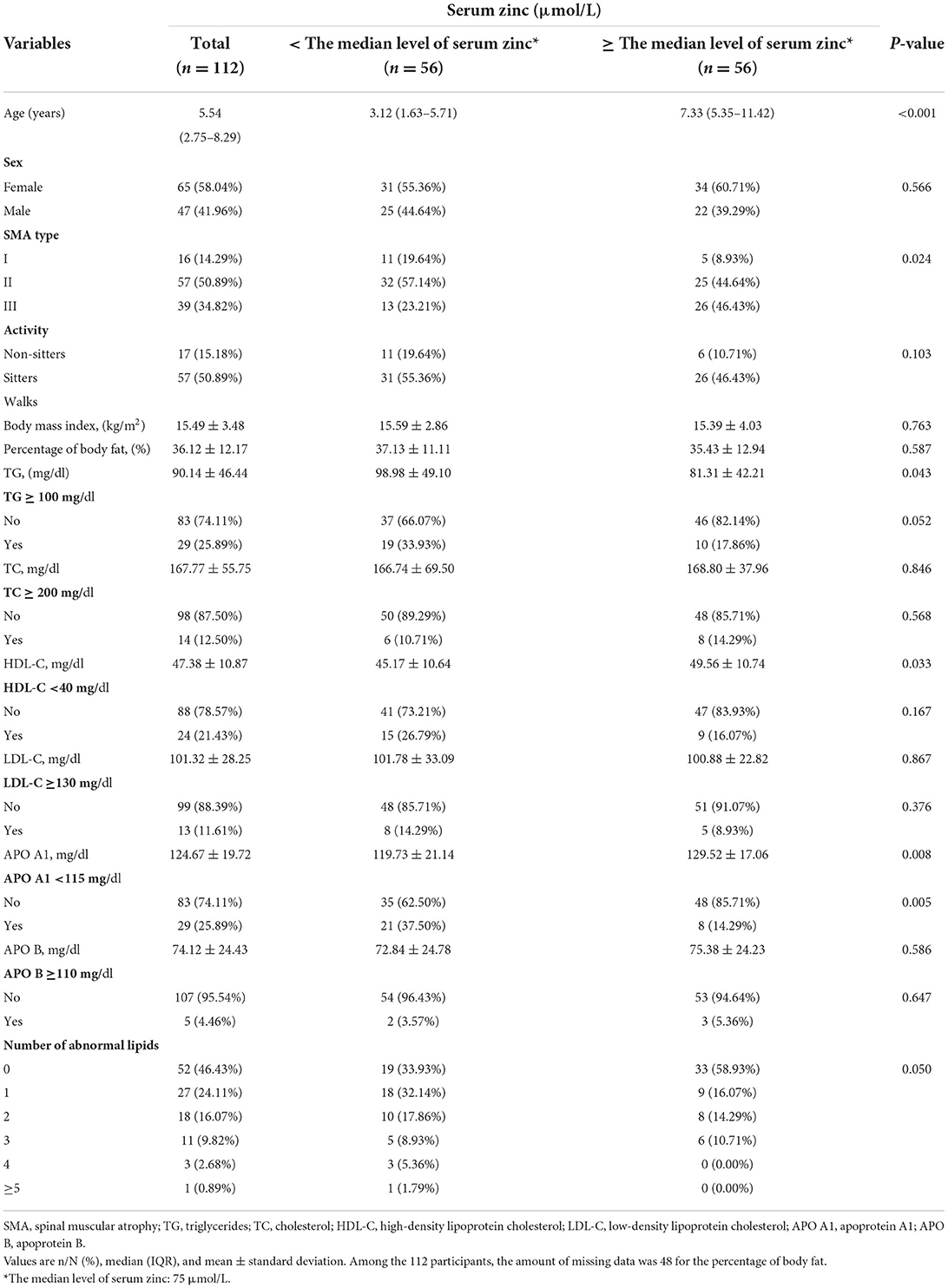
Table 1. Baseline characteristics of the study participants by the median level of serum zinc.
To identify factors related to lipid profiles, we set each of the candidates as independent variables while using lipid profiles as the dependent variable (Table 2). Univariate analysis showed that age (β = −2.79, 95% CI = −4.55 to −1.03), activity (sitters vs. non-sitters: β = −25.68, 95% CI = −50.59 to −0.77), SMA type (type 2 vs. type 1: β: −26.90, 95% CI = −52.39 to −1.41), and zinc level (β = −0.63, 95% CI = −1.17 to −0.09) were associated with TG level. Zinc level was associated with HDL-C (β = 0.16, 95% CI = 0.04–0.29) and APO A1 (β = 0.28, 95% CI = 0.05–0.51) levels.
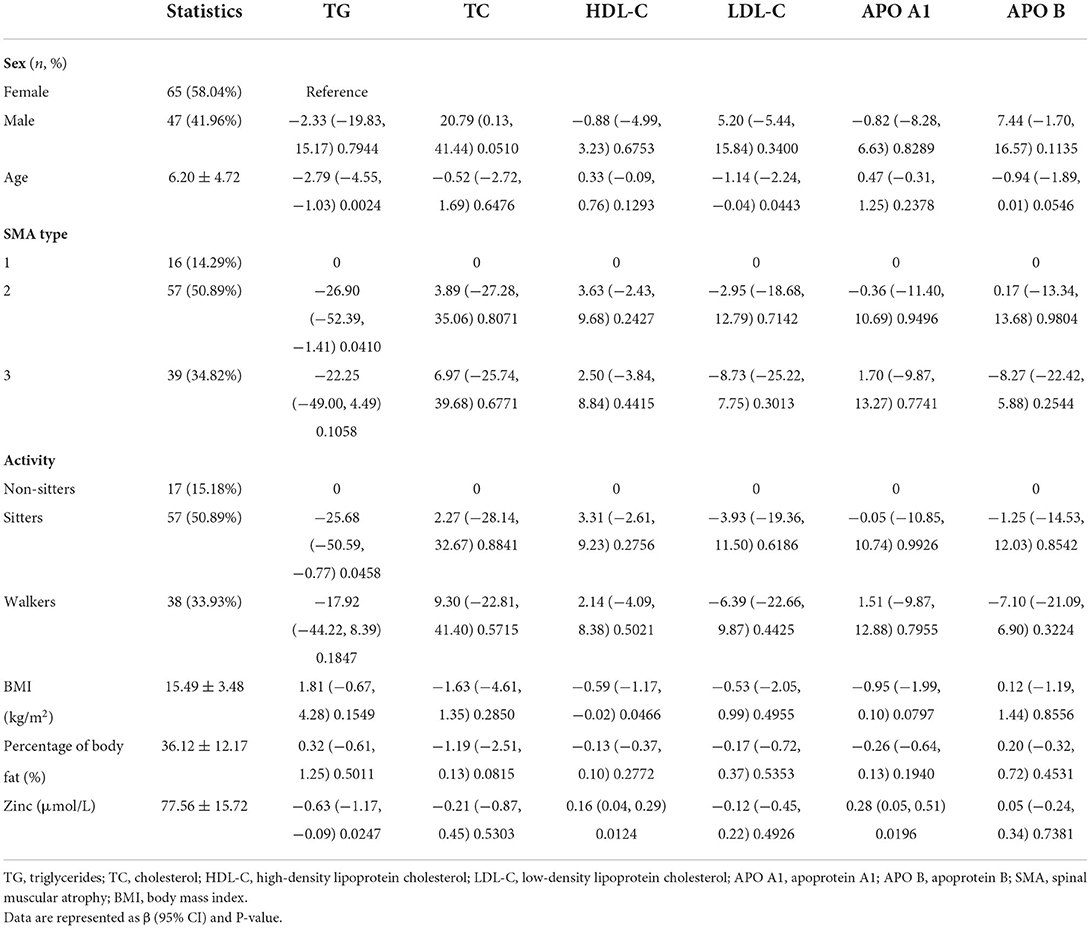
Table 2. Univariate analysis related to lipid profiles.
We employed multivariable logistic regression analysis to demonstrate the association between serum zinc levels and dyslipidaemia (Table 3). The crude model analysis indicated that an increase of 10 μmol/L in serum zinc concentration was accompanied by a 36% decrease in the risk of an APO A1 level <115 mg/dl (OR = 0.64, 95% CI = 0.46–0.89). Further adjustment for age, sex, SMA type, activity, BMI, and percentage of body fat had little impact on the odds ratios of an APO A1 level <115 mg/dl (OR = 0.65, 95% CI = 0.44–0.95). In the crude model, elevated serum zinc levels reduced the risk of TG, HDL-C, LDL-C, and APO B dyslipidaemia, whereas, in models 1 and 2, the association was not significant (crude model; Models 1 and 2 in Table 3).
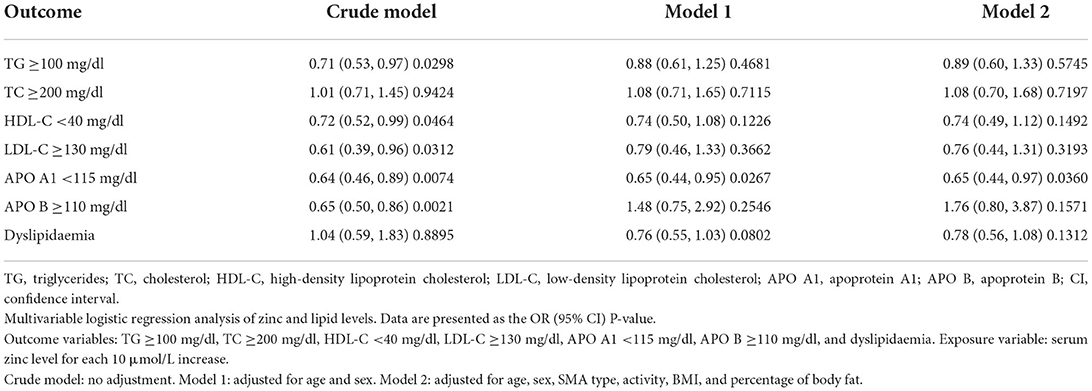
Table 3. Multivariable logistic regression between serum zinc and dyslipidaemia.
We also used multivariable linear regression analysis to determine the association between the levels of serum zinc and lipid profiles (Table 4). In the crude model, serum zinc levels positively correlated with HDL-C (β = 1.63, 95% CI = 0.37–2.88) and APO A1 (β = 2.76, 95% CI = 0.48–5.05). After full adjustment, an increase of 10 μmol/L in serum zinc level led to a 1.63 mg/dl and 2.94 mg/L elevation in serum HDL-C (β = 1.63, 95% CI = 0.44–3.22) and APO A1 (β = 2.94, 95% CI = 0.03–5.85) levels, respectively (Table 4). In the crude model, serum zinc and TG levels were negatively correlated, whereas, in Models 1 and 2, the association was not significant. No linear association was observed between serum zinc and LDL-C, TC, or APO B levels (Table 4).
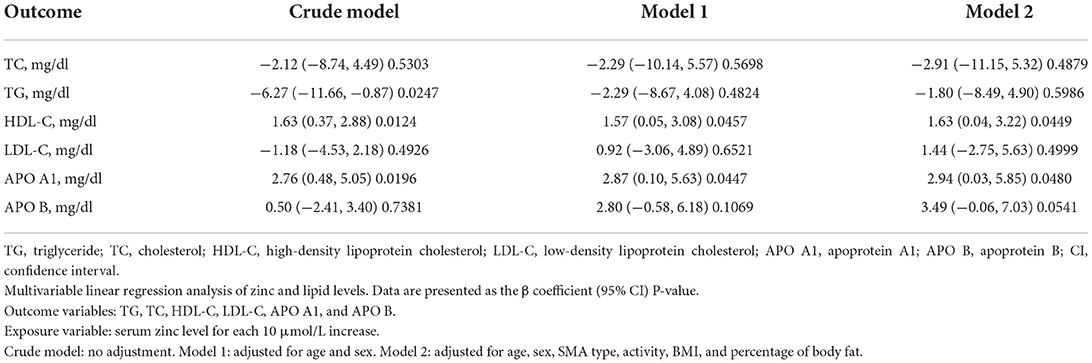
Table 4. Multivariable linear regression about serum zinc and lipid profiles.
This study, to the best of our knowledge, is the first study in this field to explore the association between serum lipids and serum zinc levels in children with SMA by adjusting for the effects of as many covariates as possible. Through the study, it was found that in our children patients with SMA, their serum lipid indicators level of them has different degrees of abnormality. Through the further detailed statistical analysis, we found that low serum zinc levels were significantly correlated with low levels of HDL-C and APO A1, which could provide a practical basis for further exploration of the influencing factors of lipid metabolism of SMA and management strategies for related complications.
Emerging studies have identified metabolic dysfunctions in patients with SMA, including lipid metabolic abnormalities, impaired glucose tolerance, and muscle mitochondrial defects (11, 12, 26). Studies have mostly focused on metabolic disorders involving fatty acid oxidation; however, some isolated studies have improved our understanding of fat metabolism. In a cohort study in Canada by Deguise et al. (13), the current prevalence of dyslipidaemia in 72 patients with SMA (16 with type 1, 52 with type 2, and 6 with type 3) was estimated to be 37.5%. Djordjevic et al. (26) determined the serum lipid profiles of 22 children with SMA type 2 and 15 with SMA type 3 and found 11 children (29.7%) with at least one indicator of abnormal lipid levels. Our study showed a higher incidence of dyslipidaemia (53.6%) than the previous two. This difference may be due to our larger sample size and the inclusion of APO A1 abnormalities in dyslipidaemia; 13% of the patients had over three laboratory-defined indicators of dyslipidaemia, similar to the prevalence reported in the cohort from Canada (14%) (13). In view of the large sample size and consistent results of the Canadian study with ours, we estimate that dyslipidaemia is an important yet undervalued feature of SMA. Dyslipidaemia can further complicate clinical conditions, leading to non-alcoholic fatty liver disease, cirrhosis, and cardiovascular and cerebrovascular diseases in adolescence and adulthood (14). Routine screening and management of SMA in patients with dyslipidaemia are necessary to reduce potential complications.
Zinc, an essential trace element and micronutrient, plays a pivotal role in human growth and development and participates in various physiological processes (17). The total prevalence of zinc deficiency in the general pediatric population is ~20%. There are still very few studies that have determined the dietary intake of zinc and serum zinc levels in patients with SMA. Our previous study confirmed that the frequency of insufficient zinc intake was 83.3% (27). Additionally, studies have consistently reported an increased fat mass and decreased fat-free mass in patients with SMA compared with healthy control subjects (28–30). Excess body fat conduces to increased cortisol synthesis and inflammation, which in turn induces Zip14 and metallothionein expression, causing a decrement in plasma zinc levels (21). Indeed, many studies have confirmed the lower levels of serum zinc in individuals who are overweight and who have obesity and diabetes (20, 21, 31).
Recently, researchers have also extended the correlation between zinc and blood lipid metabolism in the general population, adiposity, and patients with diabetes. However, these results remain controversial. No association (neither linear nor non-linear) was found between serum zinc levels and the risk of dyslipidaemia in participants in a National Health and Nutrition Examination Survey (32). A study by Rios-Lugo et al. (20) did not show any association between zinc concentration and cholesterol or TG levels in patients who were overweight and obese. In contrast, some studies demonstrated that serum zinc level was inversely associated with blood lipid levels (LDL, TG, and TC) and positively associated with HDL-C level in patients with diabetes type 1 or 2 (22, 23). In this study of 112 individuals with SMA, the association between zinc and APO A1/HDL-C levels was linear; that is, as the serum zinc level increases by 10 μmol/L, the HDL-C, and APO A1 levels will correspondingly increase by 1.63 and 2.95 mg/dl, respectively. It is also shown in this study that every 10 μmol/L increase in serum zinc level is associated with a 35% decrease in the incidence of APO A1 dyslipidaemia. However, in this model, the association between zinc levels and those of TC, LDL-C, TG, or APO B was not significant.
HDL-C and its main protein component, APO A1, play important roles in cholesterol homeostasis. The general functions of HDL-C and APO A1 are plasma-cholesterol transport, anti-inflammatory properties, and protection from oxidative damage. Low HDL-C and APO A1 levels are associated with the development of atherosclerosis (33). Patients with type III SMA who have entered adulthood may also experience coronary heart disease symptoms, such as angina pectoris, palpitations, syncope, and exertional dyspnoea (34). With the advent of targeted drugs for SMA, the lifespan of patients with SMA will be prolonged, and cardiovascular disease may probably become more prominent. Improving HDL-C level may contribute to reducing the incidence of coronary heart diseases in adults with SMA.
The potential mechanism through which zinc affects the lipid profile is still unclear. However, it has been proved that the biological mechanism of zinc involves lipid metabolism, suppression of reactive oxygen species production, and reduction in oxidative stress (17, 35). Therefore, appropriate zinc concentration may be essential for maintaining normal lipid levels. A meta-analysis has initially revealed that supplementation of zinc can increase HDL-C and reduce TC, LDL-C, and TG levels (24). Another review pointed out that zinc is an indispensable factor in regulating zinc alpha 2-glycoprotein (ZAG) homeostasis, which is considered an adipokine with anti-inflammatory and lipid-mobilizing activity (17, 18). Appropriate blood zinc concentrations are also relevant in maintaining appropriate ZAG activity as zinc facilitates the binding of adipokines to substrates, promoting lipolysis and lipid utilization (36). Tisdale et al. (37) demonstrated that ZAG could induce lipolysis both in vivo and in vitro by regulating triacylglycerol hydrolysis and free fatty acid release through signal transduction modulation in adipose tissue. A high level of ZAG can also increase HDL-C level in vivo, thereby participating in blood lipid metabolism (38). Combined with the above previous studies, the conclusion of our study preliminarily suggests that an appropriate increase in blood zinc levels in patients with SMA may help to regulate levels of blood lipids, providing evidence for the daily management of metabolism in children with SMA and for the research on the regulation mechanism of lipid metabolism in the future.
Our study had several limitations. First, as it was a cross-sectional observational survey, the cause– or time–effect relationships between serum zinc and lipid levels could not be clarified. Moreover, 42% of the patients did not complete BIA, and the accuracy of body composition analysis using BIA was not determined. However, we used multiple imputations with chained equations to account for the missing data on the percentage of body fat. We have adjusted for probability variables that may influence the result concerning the association between serum zinc and lipid levels. The results of the multivariable linear and logistic regressions were consistent, which further confirmed the relationship between zinc, HDL-C, and APO A1.
Our findings show that among patients with SMA, low serum zinc level is frequent and associated with low levels of HDL-C and APO A1. Therefore, restored serum zinc levels may reduce the incidence of low HDL-C and APO A1 levels. Further studies are warranted to explore strategies to help reduce potential related complications of SMA.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by the Ethics Committee of the Children's Hospital of the Zhejiang University School of Medicine (2019-IRB-171). Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
SM and MM contributed to the conception and design of the research. QL contributed to the statistical analyses and manuscript writing. YF contributed to data collection and manuscript revision. FC and WW contributed to the data collection. All authors read and critically revised the manuscript and approved the final submission.
This study was supported by the Key R&D Program of Zhejiang (2022C03167), the Zhejiang Province Public Welfare Technology Application Research Project (LGC21H090001), and the Key Technologies Research and Development Program of Zhejiang Province (2021C03099).
The authors thank all the volunteers and patients who participated in the clinical study. We thank Bob for the critical review and editing of the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Groen E, Talbot K, Gillingwater TH. Advances in therapy for spinal muscular atrophy: promises and challenges. Nat Rev Neurol. (2018) 14:214–24. doi: 10.1038/nrneurol.2018.4
2. Su YN, Hung CC, Lin SY, Chen FY, Chern JP, Tsai C, et al. Carrier screening for spinal muscular atrophy (SMA) in 107,611 pregnant women during the period 2005-2009: a prospective population-based cohort study. PLoS ONE. (2011) 6:e17067. doi: 10.1371/journal.pone.0017067
3. Verhaart I, Robertson A, Wilson IJ, Aartsma-Rus A, Cameron S, Jones CC, et al. Prevalence, incidence and carrier frequency of 5q-linked spinal muscular atrophy - a literature review. Orphanet J Rare Dis. (2017) 12:124. doi: 10.1186/s13023-017-0671-8
4. Hamilton G, Gillingwater TH. Spinal muscular atrophy: going beyond the motor neuron. Trends Mol Med. (2013) 19:40–50. doi: 10.1016/j.molmed.2012.11.002
5. Wirth B. Spinal muscular atrophy: in the challenge lies a solution. Trends Neurosci. (2021) 44:306–22. doi: 10.1016/j.tins.2020.11.009
6. Mercuri E, Finkel RS, Muntoni F, Wirth B, Montes J, Main M, et al. Diagnosis and management of spinal muscular atrophy: part 1: recommendations for diagnosis, rehabilitation, orthopedic and nutritional care. Neuromuscul Disord. (2018) 28:103–15. doi: 10.1016/j.nmd.2017.11.005
7. Finkel RS, Mercuri E, Meyer OH, Simonds AK, Schroth MK, Graham RJ, et al. Diagnosis and management of spinal muscular atrophy: part 2: pulmonary and acute care; medications, supplements and immunizations; other organ systems; and ethics. Neuromuscul Disord. (2018) 28:197–207. doi: 10.1016/j.nmd.2017.11.004
8. Moore GE, Lindenmayer AW, McConchie GA, Ryan MM, Davidson ZE. Describing nutrition in spinal muscular atrophy: a systematic review. Neuromuscul Disord. (2016) 26:395–404. doi: 10.1016/j.nmd.2016.05.005
9. Chou E, Lindeback R, Sampaio H, Farrar MA. Nutritional practices in pediatric patients with neuromuscular disorders. Nutr Rev. (2020) 78:857–65. doi: 10.1093/nutrit/nuz109
10. Corsello A, Scatigno L, Pascuzzi MC, Calcaterra V, Dilillo D, Vizzuso S, et al. Nutritional, gastrointestinal and endo-metabolic challenges in the management of children with spinal muscular atrophy Type 1. Nutrients. (2021) 13:2400. doi: 10.3390/nu13072400
11. Li Y, Chen T, Wu Y, Tseng Y. Metabolic and nutritional issues associated with spinal muscular atrophy. Nutrients. (2020) 12:3842. doi: 10.3390/nu12123842
12. Deguise M, Chehade L, Kothary R. Metabolic dysfunction in spinal muscular atrophy. Int J Mol Sci. (2021) 22:5913. doi: 10.3390/ijms22115913
13. Deguise MO, Baranello G, Mastella C, Beauvais A, Michaud J, Leone A, et al. Abnormal fatty acid metabolism is a core component of spinal muscular atrophy. Ann Clin Transl Neurol. (2019) 6:1519–32. doi: 10.1002/acn3.50855
14. Pires A, Sena C, Seica R. Dyslipidemia and cardiovascular changes in children. Curr Opin Cardiol. (2016) 31:95–100. doi: 10.1097/HCO.0000000000000249
15. Yoon JM. Dyslipidemia in children and adolescents: when and how to diagnose and treat? Pediatr Gastroenterol Hepatol Nutr. (2014) 17:85–92. doi: 10.5223/pghn.2014.17.2.85
16. Peterson AL, McBride PE. A review of guidelines for dyslipidemia in children and adolescents. Wis Med J. (2012) 111:274.
17. Olechnowicz J, Tinkov A, Skalny A, Suliburska J. Zinc status is associated with inflammation, oxidative stress, lipid, and glucose metabolism. J Physiol Sci. (2018) 68:19–31. doi: 10.1007/s12576-017-0571-7
18. Banaszak M, Górna I, Przysławski J. Zinc and the innovative zinc-α2-glycoprotein adipokine play an important role in lipid metabolism: a critical review. Nutrients. (2021) 13:2023. doi: 10.3390/nu13062023
19. Martinez EE, Quinn N, Arouchon K, Anzaldi R, Tarrant S, Ma NS, et al. Comprehensive nutritional and metabolic assessment in patients with spinal muscular atrophy: opportunity for an individualized approach. Neuromuscul Disord. (2018) 28:512–9. doi: 10.1016/j.nmd.2018.03.009
20. Rios-Lugo MJ, Madrigal-Arellano C, Gaytán-Hernández D, Hernández-Mendoza H, Romero-Guzmán ET. Association of serum zinc levels in overweight and obesity. Biol Trace Elem Res. (2020) 198:51–7. doi: 10.1007/s12011-020-02060-8
21. Severo JS, Morais JBS, Beserra JB, Dos Santos LR, de Sousa Melo SR, de Sousa GS, et al. Role of zinc in zinc-α2-glycoprotein metabolism in obesity: a review of literature. Biol Trace Elem Res. (2020) 193:81–8. doi: 10.1007/s12011-019-01702-w
22. Wolide AD, Zawdie B, Alemayehu T, Tadesse S. Association of trace metal elements with lipid profiles in type 2 diabetes mellitus patients: a cross sectional study. BMC Endocr Disord. (2017) 17:64. doi: 10.1186/s12902-017-0217-z
23. Peruzzu A, Solinas G, Asara Y, Forte G, Bocca B, Tolu F, et al. Association of trace elements with lipid profiles and glycaemic control in patients with type 1 diabetes mellitus in northern Sardinia, Italy: an observational study. Chemosphere. (2015) 132101–107. doi: 10.1016/j.chemosphere.2015.02.052
24. Ranasinghe P, Wathurapatha WS, Ishara MH, Jayawardana R, Galappatthy P, Katulanda P, et al. Effects of zinc supplementation on serum lipids: a systematic review and meta-analysis. Nutr Metab. (2015) 12:491. doi: 10.1186/s12986-015-0023-4
25. National Cholesterol Education Program (NCEP): highlights of the report of the expert panel on blood cholesterol levels in children and adolescents. Pediatrics. (1992) 89:495–501. doi: 10.1542/peds.89.3.495
26. Djordjevic SA, Milic-Rasic V, Brankovic V, Kosac A, Dejanovic-Djordjevic I, Markovic-Denic L, et al. Glucose and lipid metabolism disorders in children and adolescents with spinal muscular atrophy types 2 and 3. Neuromuscul Disord. (2021) 31:291–9. doi: 10.1016/j.nmd.2021.02.002
27. Long Q, Yao M, Xia Y, Ma M, Zhang T, Wang W, et al. Nutritional status of children with spinal muscular atrophy. Chin J Clin Nut. (2020) 28:177–81. doi: 10.3760/cma.j.cn115822-20200427-00112
28. Bertoli S, De Amicis R, Mastella C, Pieri G, Giaquinto E, Battezzati A, et al. Spinal muscular atrophy types I and II: what are the differences in body composition and resting energy expenditure? Clin Nutr. (2017) 36:1674–80. doi: 10.1016/j.clnu.2016.10.020
29. Davis RH, Godshall BJ, Seffrood E, Marcus M, LaSalle BA, Wong B, et al. Nutritional practices at a glance: spinal muscular atrophy type I nutrition survey findings. J Child Neurol. (2014) 29:1467–72. doi: 10.1177/0883073813503988
30. Poruk KE, Davis RH, Smart AL, Chisum BS, LaSalle BA, Chan GM, et al. Observational study of caloric and nutrient intake, bone density, and body composition in infants and children with spinal muscular atrophy type I. Neuromuscul Disord. (2012) 22:966–73. doi: 10.1016/j.nmd.2012.04.008
31. Marreiro DN, Fisberg M, Cozzolino SM. Zinc nutritional status in obese children and adolescents. Biol Trace Elem Res. (2002) 86:107–22. doi: 10.1385/BTER:86:2:107
32. Qu X, Yang H, Yu Z, Jia B, Qiao H, Zheng Y, et al. Serum zinc levels and multiple health outcomes: implications for zinc-based biomaterials. Bioact Mater. (2020) 5:410–22. doi: 10.1016/j.bioactmat.2020.03.006
33. Frikke-Schmidt R. HDL cholesterol and apolipoprotein A-I concentrations and risk of atherosclerotic cardiovascular disease: human genetics to unravel causality. Atherosclerosis. (2020) 29953–55. doi: 10.1016/j.atherosclerosis.2020.03.005
34. Roos M, Sarkozy A, Chierchia GB, De Wilde P, Schmedding E, Brugada P. Malignant ventricular arrhythmia in a case of adult onset of spinal muscular atrophy (Kugelberg-Welander disease). J Cardiovasc Electrophysiol. (2009) 20:342–4. doi: 10.1111/j.1540-8167.2008.01327.x
35. Singh N, Yadav KK, Rajasekharan R. Effect of zinc deprivation on the lipid metabolism of budding yeast. Curr Genet. (2017) 63:977–82. doi: 10.1007/s00294-017-0704-9
36. Wei X, Liu X, Tan C, Mo L, Wang H, Peng X, et al. Expression and function of zinc-alpha2-glycoprotein. Neurosci Bull. (2019) 35:540–50. doi: 10.1007/s12264-018-00332-x
37. Tisdale MJ. Zinc-alpha2-glycoprotein in cachexia and obesity. Curr Opin Support Palliat Care. (2009) 3:288–93. doi: 10.1097/SPC.0b013e328331c897
Keywords: spinal muscular atrophy, dyslipidaemia, serum zinc, children, high-density lipoprotein cholesterol, apolipoprotein A1
Citation: Long Q, Feng Y, Chen F, Wang W, Ma M and Mao S (2022) Association between serum zinc level and lipid profiles in children with spinal muscular atrophy. Front. Nutr. 9:960006. doi: 10.3389/fnut.2022.960006
Received: 02 June 2022; Accepted: 22 July 2022;
Published: 15 August 2022.
Edited by:
Gregory C. Henderson, Purdue University, United StatesReviewed by:
Vedrana Milic-Rasic, University of Belgrade, SerbiaCopyright © 2022 Long, Feng, Chen, Wang, Ma and Mao. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Shanshan Mao, NjMwNzAwM0B6anUuZWR1LmNu
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.