
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Nutr., 26 September 2022
Sec. Nutritional Epidemiology
Volume 9 - 2022 | https://doi.org/10.3389/fnut.2022.956293
This article is part of the Research TopicHealthy Foods and Dietary Patterns in Modern ConsumerView all 15 articles
 Zohre Foroozanfar1
Zohre Foroozanfar1 Mohsen Moghadami2
Mohsen Moghadami2 Mohammad Ali Mohsenpour3,4Anahita Houshiarrad5
Mohammad Ali Mohsenpour3,4Anahita Houshiarrad5 Azam Farmani6Mohsen Ali Akbarpoor6
Azam Farmani6Mohsen Ali Akbarpoor6 Razieh Shenavar2,6*
Razieh Shenavar2,6*Introduction: Households' dietary habits are affected by their environment and socioeconomic status (SES). This study aims to investigate eating behaviors and determine the factors affecting nutritional status in households in Fars Province in 2018.
Method: In this cross-sectional study, urban and rural households were selected using the multistage sampling method. A questionnaire was employed to interview the mother or householder to record the demographic, SES, and dietary habits of the family for major food items commonly used. A logistic regression model was used to analyze the data. The p-value less than 0.05 was considered significant.
Results: In total, 6,429 households participated in the study. The majority of households use traditional flatbread, low-fat milk, and liquid/cooking oil. Frying was the most prevalent method of cooking. Parents' level of education and SES were associated with type of consumed bread, milk and dairy, methods of food preparation, adding salt at the table, eating out, and fast-food usage. Parents' higher level of education was significantly associated with salt storage in optimal conditions and not using salt before tasting the meal.
Conclusion: Most of the households had healthy practices, especially in consumption of certain oils and methods of preparing their food as well as keeping salt in an optimal condition and using iodized salt. The most important unhealthy nutritional behavior was high consumption of fast food and outdoor food, especially in urban regions. Unhealthy dietary habits were more prevalent in households with low household and regional SES. Both households and regions with higher SES had better dietary habits.
Recently, changes in lifestyle have raised the prevalence of chronic diseases such as cardiovascular disease, hypertension, diabetes, and cancers (1). The most important lifestyle determinants of non-communicable diseases (NCDs) are reduced physical activity and poor eating habits (2).
A healthy dietary habit includes various approaches to the consumption of different food groups, food items, and the preparation of daily meals. Several recommendations are available in order to stick to a healthy dietary habit and, consequently, to prevent NCDs, such as choosing vegetable oils over animal-based oils, consuming fruits and vegetables on a daily basis, and using low-fat dairy products (3). Moreover, the food preparation method is also a major factor affecting health (4). According to the nutritional transitions, fast-food consumption has been increased alarmingly, with its health consequences emerging (3).
In addition, the dietary habits of individuals and households are affected by their environment and socioeconomic status (SES). The association between SES and poorer health has been recognized, and inequalities in nutrition have been associated with inequalities in health. Higher SES environment, education, and income are linked to changing dietary habits, but not always in a desirable way (3). Populations in low SES probably are at a higher risk of unhealthy conditions due to the lack of access to healthcare and poor nutrient intake. Thus, given public health policies, the assessment of eating habits in each population is essential for preventing diseases and nutrient deficiencies (5).
A few studies have been conducted in Iran to comprehensively assess nutritional behavior and its possible determinants for different geographical areas in rural and urban populations. Therefore, we aimed to assess the nutritional behavior of households in rural and urban populations of Fars Province, Iran.
A cross-sectional study was designed to investigate the nutritional behavior of urban and rural populations of Fars Province, Iran. The study protocol was approved by the Shiraz University of Medical Sciences (SUMS), Fars, Iran, under the registration code: IR.SUMS.REC.13940598.
Households residing in the urban and rural areas of Fars Province, covered by the Health Department of SUMS, were included in the study.
Fars Province, a populated province, is located in the southwest area of Iran. SUMS is one of the major universities of medical sciences in Iran, which is placed in Shiraz, the capital of Fars. SUMS Health Department covers 29 out of 36 towns in Fars Province (Figure 1). In this study, a multistage sampling method was used. In the first phase, all 29 towns were considered 29 stages (28 affiliated towns and Shiraz as the center). In the second phase, the towns were divided into two urban and rural communities. In addition, Shiraz was divided into 7 areas, including 5 urban communities (3 districts of Shiraz—northern, central, and southern, and 2 northern and southern suburbs of Shiraz) and 2 rural communities. Subsequently, by means of the maps, urban and rural areas were separated into three clusters of north, center, and south with a maximum spatial accuracy. Finally, we obtained 168 clusters from affiliated towns and 21 clusters from Shiraz. Then, 34 households in each cluster were included using a systematic random sampling method. In this stage, the first household was selected by random selection and sampling was continued from the right side of the house until reaching the predetermined sample size. Thus, a total of 6,426 households were included in this study. The mother of each household was considered the representative in order to respond to the interviewer, or, in the absence of the mother, the householder (the person in the household who is responsible for making decisions and earning money) was interviewed. Figure 1 depicts the sampling procedure of the study.
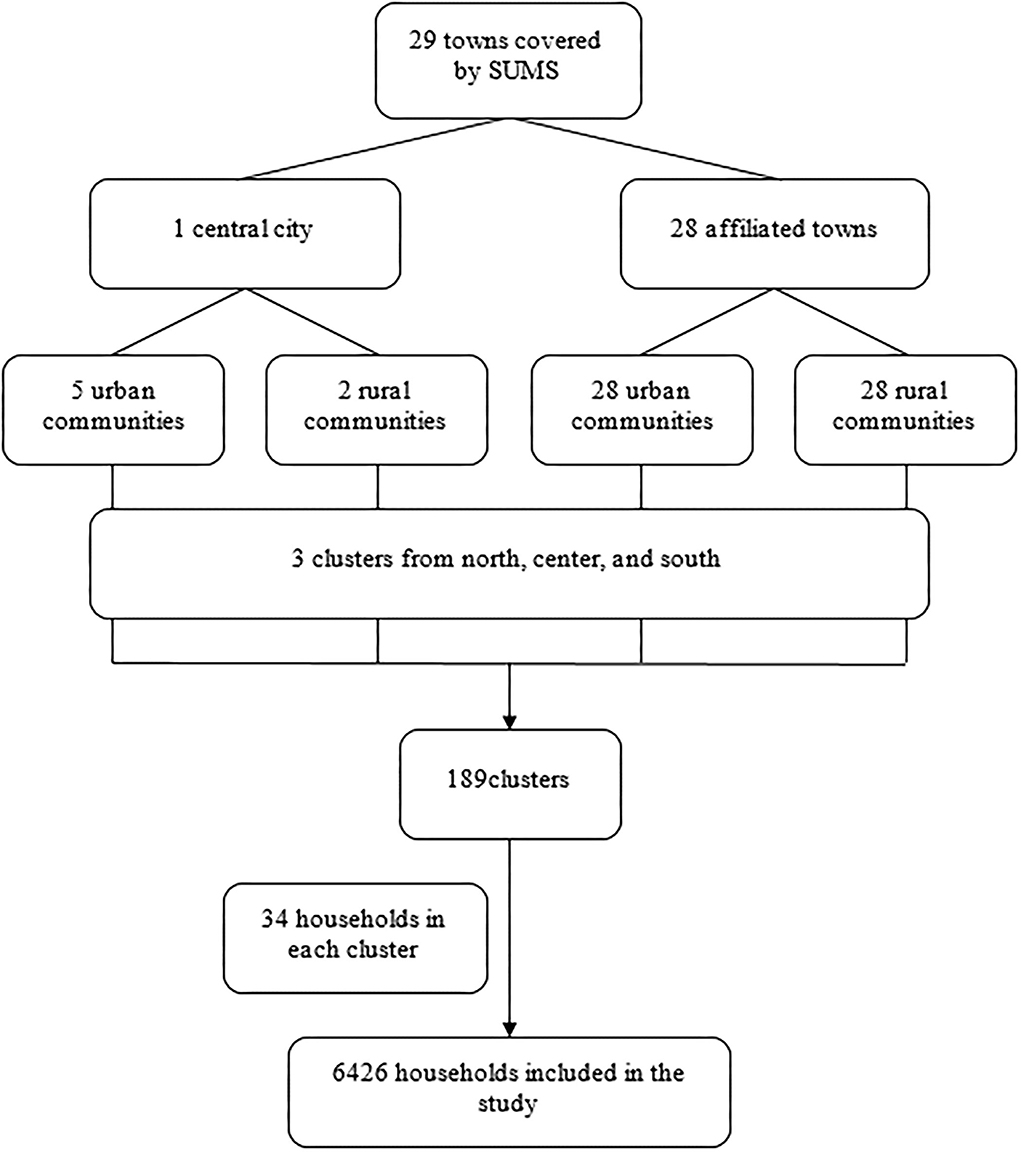
Figure 1. Sampling procedure of the study.
A questionnaire was compiled to assess general and sociodemographic characteristics of the households. The questionnaire asked about the persons who were present in the household for the last 7 days continuously, head of the household, and his/her spouse's level of education (illiterate, elementary level, high school, diploma, graduate, and postgraduate), and job status (unemployed, farmer, full-time worker, daily worker, employed, self-employed, and retired for father and housewife, employed, and self-employed for mother).
The sociodemographic status of the household was calculated by considering the possession of 9 specific items, including home, personal vehicle, washing machine, LCD TV, dishwasher, refrigerator, handmade rug, laptop, and microwave. Based on the number of items possessed by households, the SES was categorized into three groups, namely, low (3 items or less), moderate (4–6 items), and high (more than 7 items) (6).
A nutritional behavior questionnaire was used to investigate the overall food consumption habits of households (1, 7). Interviewers asked about types of consumed milk and dairy (low fat vs. high fat), bread (traditional flatbreads or homemade breads), and oil (different types of vegetable oils or animal oils), in addition to their consumed amount. The frequency of the consumption of vegetables and salad (weekly) and salt consumption habits were assessed by the questionnaire. Interviewers asked about iodized salt consumption, and in case of a positive response, its storage method within the household was investigated to indicate whether the storage is optimal or undesirable. In addition, the habit toward salt was recorded based on using salt at the table and adding salt to the meal before tasting it. Moreover, using dietary habit questionnaires, data were gathered about food preparation methods, including boiling, grilling, steaming, roasting, frying, or, other traditional methods, and consuming fast-food and packaged food.
To describe the quantitative and qualitative characteristics (ordinal and nominal variables) of the households, descriptive statistical procedures including mean ± standard deviation (SD), frequency, and percentage were performed, respectively. To determine the contribution of food habits or consumption and place of residence, the chi-square test was used. In addition, the logistic regression model was used to estimate the association between sociodemographic characteristics and food habits or consumption. All statistical analyses were performed using the SPSS software version 22 (IBM, USA). A p-value of less than 0.05 was considered significant.
A total of 6,429 households were included in the study, of which 5,826 (91.4%) were headed by a father. The mean household size was 3.91 ± 1.38, which was 4.01 ± 1.48 in rural areas and 3.80 ± 1.27 in urban areas. The characteristics of households, householders, and spouse's level of education and job based on place of residence are reported in Table 1.
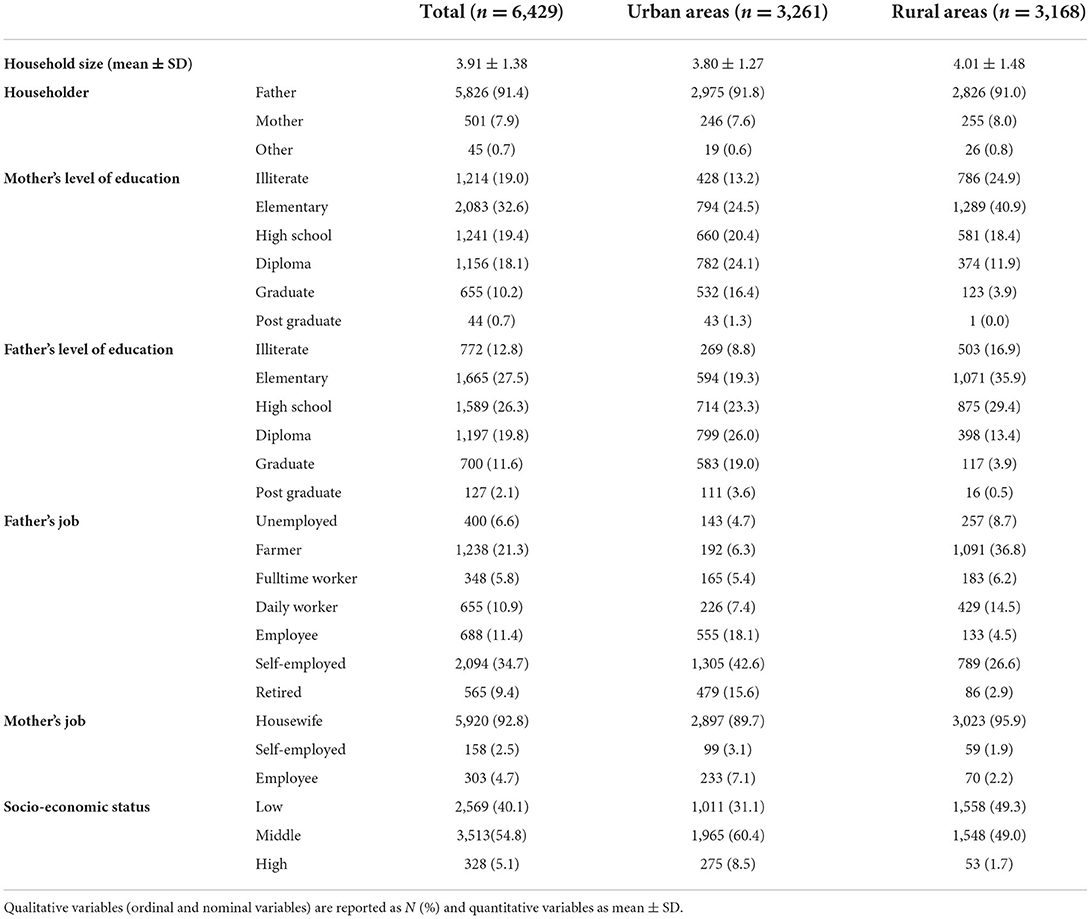
Table 1. Socio-demographic characteristics of households by place of residence.
The majority of households (65.7%) used traditional flatbreads, more than half of the households (53.9%) consumed low-fat milk and dairy products, and liquid/cooking oil was the most consumed oil within households (65.9%). Frying was the most prevalent method of cooking (54.2%). In addition, the iodized salt was used in 97.2% of households in comparison with non-iodized salt (2.8%), and storage of salt was in optimal condition in 72.0% of households for total population. Table 2 represents household nutritional behavior in total population based on the place of residence.
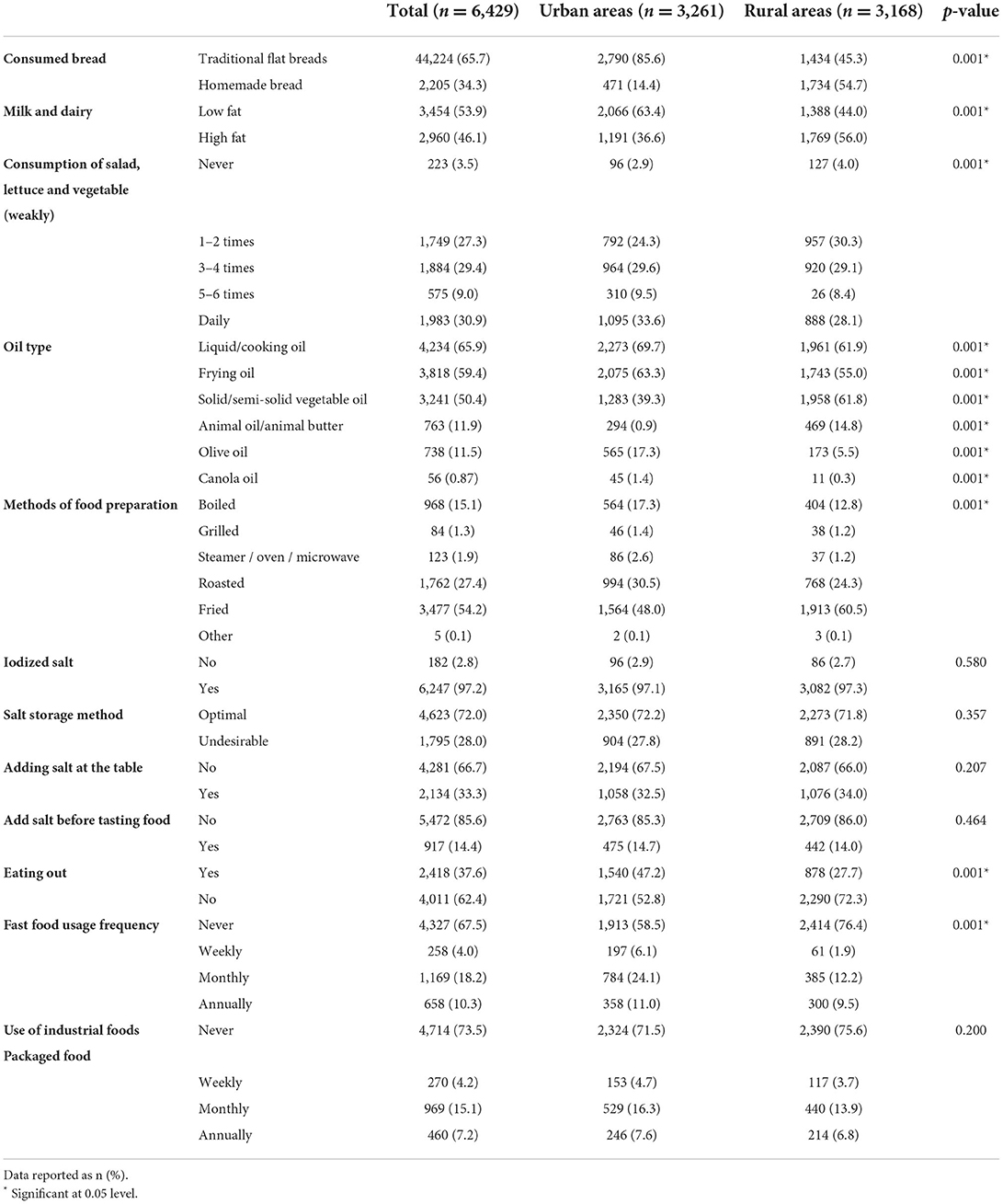
Table 2. Household Food habits in total population as well as place of residence.
As shown in Table 2, there was a significant difference between rural and urban areas in terms of food habits, such as consumed bread, milk and dairy, and oil type (p < 0.001). Food preparation methods, eating out, and fast-food consumption were significantly different between urban and rural communities (p < 0.001).
Higher levels of education of the head of the household and his/her spouse as well as higher SES were significantly associated with reduced consumption of home-made bread, consumption of high-fat dairy products, and frying food. In addition, the larger family size was associated with increased consumption of high-fat dairy products and frying food (p < 0.05). According to our results, a higher level of education was significantly associated with household iodized salt intake (odds ratio [OR] = 1.23, 95% CI: 1.08, 1.39). Moreover, a higher level of education of the head of the household and his/her spouse was significantly associated with salt storage in optimal conditions as well as not using a salt shaker at the table and not using salt before tasting food. Larger family size was associated with salt storage in undesirable conditions (OR = 0.95, 95% CI: 0.91, 0.98), using a salt shaker at the table (OR = 1.09, 95% CI: 1.05, 1.14), and using salt before tasting food (OR = 1.13, 95% CI: 1.08, 1.18). Higher SES was associated with not using a salt shaker at the table (OR = 0.89, 95% CI: 0.82, 0.98). Moreover, higher levels of education of the head of the household and his/her spouse as well as higher SES were significantly associated with increased consumption of outdoor food and fast foods. In addition, a larger family size was associated with increased consumption of fast foods (OR = 1.10, 95% CI: 1.06, 1.15). Table 3 represents the association between dietary habits and related factors.
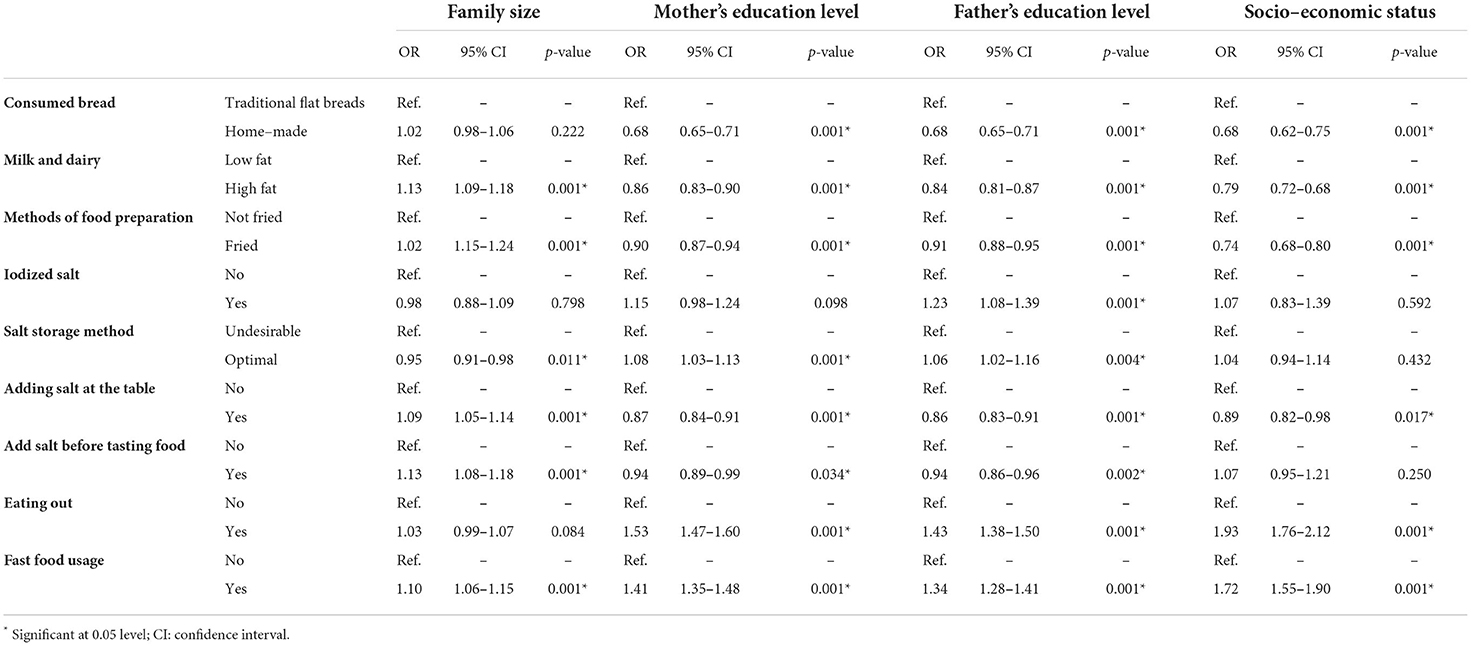
Table 3. Factors associated with food habits in total population.
The association between sociodemographic characteristics of households and food habits in urban and rural areas is reported in Tables 4, 5, respectively. According to the results, in rural areas, a higher level of education was associated with household iodized salt intake, but there was no association between education and iodized salt intake in urban areas. Larger family size was associated with increased consumption of home-made bread in urban areas, but there was no association between size of family and consumption of home-made bread in rural areas.
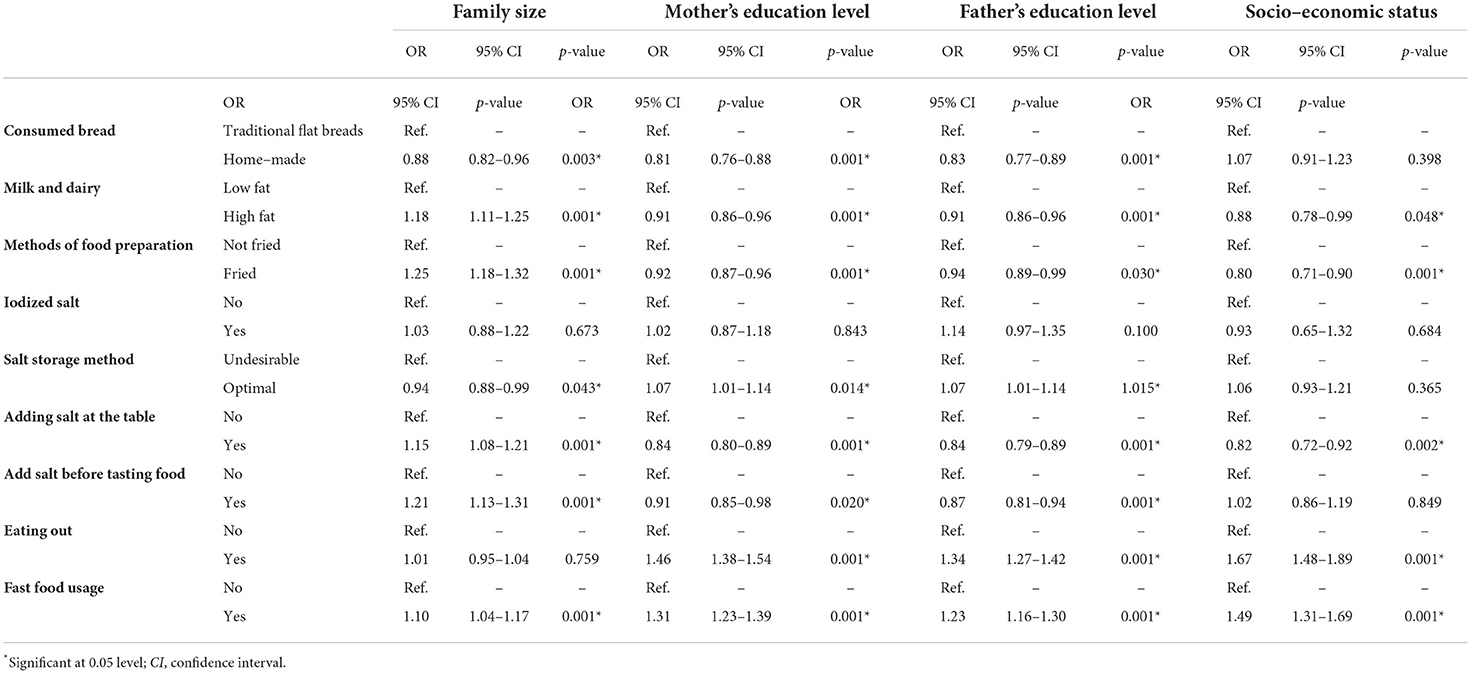
Table 4. Factors associated with food habits in urban population.
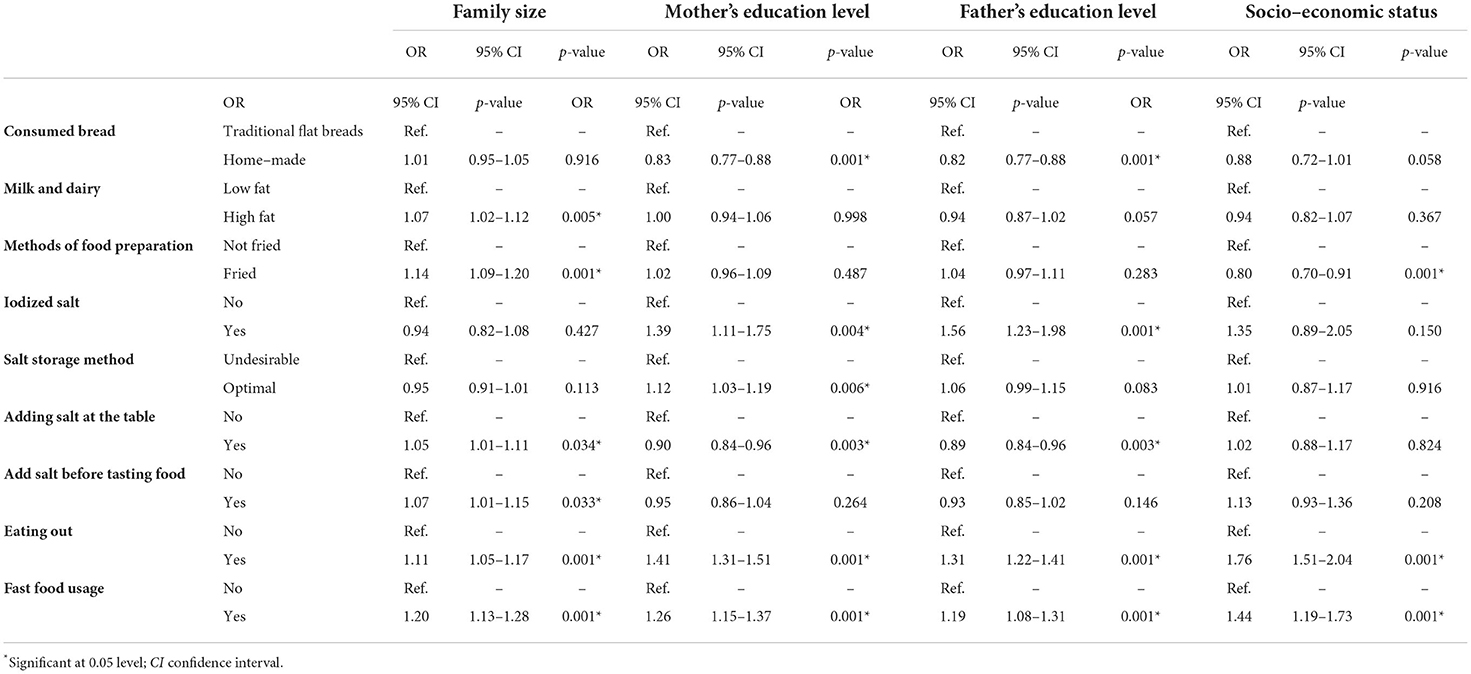
Table 5. Factors associated with food habits in rural population.
In this study, liquid/cooking oils were the most consumed oil type among households (65.9%). In addition, olive and canola oils were consumed by 11.5 and 0.87% of households, respectively. However, consumption of liquid and vegetable oils in Sanandaj Province, Iran, was 26.75% (8). These vegetable oils have shown beneficial properties toward cardiovascular diseases due to their fatty acid composition. Consuming more than 2.5 times mono-unsaturated fatty acids (MUFAs) and poly-unsaturated fatty acids (PUFAs) present in vegetable oils (9) than saturated fatty acids (SFAs) is considered a healthy behavior in the Healthy Eating Index 2015 (10).
In contrast to liquid and vegetable oils, animal meat and high-fat dairy products contain high amounts of SFA. SFA consumption is responsible for various chronic conditions, including cardio heart disease (CHD) (11); thus, it is recommended by the Dietary Guideline for Americans (DGA) to use <10% of daily calorie intake from SFA and replace it with PUFA (11).
Dietary guidelines suggest reducing the consumption of high-fat dairy products (12). In the present survey, almost nearly half of the households (53.9%) consumed low-fat milk and dairy. Although low-fat milk and dairy products were significantly higher, it was observed that a significant difference could be due to the large sample size. As the American meta-analysis reported, high-quality evidence supports favorable associations (i.e., decreased risk) between total dairy intake and hypertension risk and between low-fat dairy and yogurt intake and reduced risk of type 2 diabetes (T2D) and the consequent massive burden of health economics in this area (13). Thus, proper methods of awareness are required to amend dairy product consumption patterns in this area.
In this study, the most common methods of cooking were fried cooking (54.2%). Deep frying with oil negatively changes the fatty acid composition of oil. Frying increases energy density and decreases the water content of the meal. In a case-control study in India, patients with coronary heart disease, when compared with the control group, reported a greater intake of shallow fried food. Data from a case-control study in China showed that the frequency of fried food intake was significantly higher in patients with acute myocardial infarction. Data from the Nurses' Health Study and the Health Professional Follow-Up Study showed that frequent fried food consumption was significantly associated with a higher risk of coronary artery disease (CAD) (14). Thus, health and nutrition education as well as the improvement of healthy snacks and physical activity, especially at schools and kindergarten can change nutritional behaviors in Iranian households.
Iodine plays an essential role in the functions of thyroid hormones. The prevention of iodine deficiency disorders (IDDs) is one of the most important health programs in Iran. Based on our results, 97.2% of households used iodized salt. The World Health Organization (WHO) and International Council for Iodine Deficiency Disorders (ICCIDD) standards state that the elimination of IDD will be possible if more than 90% of households consume adequately iodized salt (15). The Iodized Salt Coverage Study 2010 shows that the availability of adequately iodized salt in the households in Orissa has almost doubled from 32.4%, conducted by the National Food and Health Survey (NFHS) 3 in 2005–2006 to 59% in 2010. Consumption of iodized salt has increased, but it is still way behind the universal salt iodization (USI) target of 90% of households consuming adequately iodized salt (16, 17). In a study by Srivastava et al., two-thirds (65.2%) of the households were adequately consuming iodized salt, while about one-fifth (21.5%) of the households were consuming iodized salt inadequately (18).
In this study, a higher level of education was significantly associated with reduced consumption of fried food and high-fat dairy products, although, in such families, traditional flatbreads and fast food were consumed more.
In addition, a large-scale meta-analysis investigated 15 European countries and determined that the parents' higher level of education was associated with healthy diet behaviors. A similar result was reported in a Danish survey too (19). The analysis of demographic and socioeconomic data determined that education is usually the strongest component of socioeconomic differences (20). In contrast, Aslam et al. reported that consumption of all groups, healthy and unhealthy foods such as sugar and fast foods, was highly associated with the level of education (21).
In this study, a higher level of education of the head of the household and his/her spouse was significantly associated with iodized salt storage in optimal conditions as well as not using a salt shaker and not using salt before tasting food. Valexi et al. showed that women and men with a high level of education knew how to store iodized salt (22). However, Azizi et al. showed that the level of education was not significantly associated with the storage of salt (23). Higher levels of education may also improve the ability to believe or understand health-related information, in general, or dietary practice, in particular, needed to develop health-promoting skills and beliefs in the field of food habits. It is believed that with a higher level of education, there is more knowledge about healthy food items (20, 24).
In this study, higher SES was significantly associated with reduced consumption of fried food and high-fat dairy products but fast food/outdoor food was increased. A similar result was found in the Kelishadi's study, suggesting that families with higher SES had healthier dietary practices (2). Esghinia et al. (23)and Rezazadeh et al. (25) found a rising trend toward healthy and nutritive behaviors with the increase in SES.
According to previous studies, SES is one of the most important determinants of diet quality in children and adolescents. This can be due to higher nutritional knowledge in high SES regions and limited access and affordability for some fast foods in low SES regions (26).
In this study, SES was not significantly associated with iodized salt intake. However, a study in Tehran showed that the SES influenced iodized salt consumption (27). In studies conducted by Kouhi et al. (28), Sharifirad et al. (29), and Yarmohammadi et al. (30) on students, there was a direct relationship between economic status and fast-food consumption (31). It can be concluded that good income acts as a double-edged sword. Although a favorable economic status can cause the consumption of healthy snacks and healthy nutrition, it can increase their purchasing power for junk foods.
Based on our findings, an unhealthier dietary pattern may exist among the households who are in lower socioeconomic level in Iran. The relationship between SES and nutritional performance has been studied (32). Many studies have determined that eating patterns of people in low SES groups threaten public health (33–37). People in the low SES group, due to a lack of accessibility to healthcare, improper living conditions, less education, and greater psychological stress, may be at a greater risk of poorer health status than others (38). Thus, appropriate policies, interventions, and efforts aimed at improving nutrition-related health, especially in high-risk groups, are necessary.
In this study, daily consumption of vegetables was close to 30%. A healthier dietary pattern is believed to include a higher consumption of fruits and vegetables and a lower consumption of fat and meat. Thus, people with a higher socioeconomic level tend to show a higher consumption of vegetables, fruits, and fiber products, and a lower consumption of meat, meat products, and fats in comparison with people with a lower socioeconomic level (20). Abdollahi et al. showed that with the increase in knowledge and occupational level of the heads of households, consumption of high-dense calories and lower healthy groups decreased. A large-scale meta-analysis from 15 European countries also showed that higher levels of literacy were associated with higher consumption of vegetables and fruits (1, 20, 39). One of the main principles of healthy diet is the daily intake of vegetables that are effective in preventing NCDs. Therefore, certain interventions are necessary to increase vegetable consumption per capita, including increasing access to this group of food and promoting vegetable consumption from childhood.
In this study, family size was associated with increasing consumption of fast food, high-fat dairy products, and fried food, while larger family size was significantly associated with iodized salt storage in undesirable condition as well as using a salt shaker and using salt before tasting food. It is obvious that family size can affect dietary behaviors in the household. When family size increases, the eating habits of a person in the family can affect all members of the family and show itself as the eating behavior of the family. It is to be expected that family members have different eating habits, but unhealthy eating habits are usually more pronounced than other eating habits.
In this study, almost all eating practices were significantly different between rural and urban areas. According to the results, in rural areas, higher levels of knowledge of the head of the household and his/her spouse were associated with household iodized salt intake, but in urban areas, there was no association between knowledge of the head of the household and his/her spouse and iodized salt intake. A larger family size was associated with decreased consumption of home-made bread in urban areas, but there was no association between size of family and consumption of home-made bread in rural areas. Consumption of fast food was significant in both urban and rural areas in this study.
Kelishadi et al. did not report any significant differences between urban and rural areas for salt intake. This finding is probably because of the main sources of salt intake, i.e., bread, cheese, and many junk foods such as cheese puffs and potato chips, which are regularly consumed by all Iranian people and are not limited to urban areas or a kind of socioeconomic categories. On the contrary, a survey in Ethiopia and Sudan showed that individuals in urban areas were 9 times more likely to be aware of iodized salt consumption than those who lived in rural areas (40).
Participants in regions with higher SES had healthier nutritional behaviors, but some nutritional behaviors, such as consumption of fast food less often, were similar in areas with the lowest and highest SES. This can be due to higher health knowledge in high SES regions, and inaccessibility and limited affordability for some fast foods in low SES regions (2).
Despite the expectation that increased knowledge of the head of the household and his/her spouse may create a negative attitude toward eating unhealthy food by being more aware of the importance of healthy nutrition for families, the tendency toward consuming more unhealthy diets and fast food, especially among the adolescents, has increased in households in today's urban communities as a result of longer working hours, more busy educated parents in outdoor work environments, as well as time limitations.
One of the strengths of this study is that it was a comprehensive study with a large sample size, so that the samples represent the whole community. In addition, this study examined all aspects of household dietary behaviors and considered all factors affecting eating habits. The main limitation of this study was that we did not assess the disease and anthropometric data of the households. Therefore, future studies are suggested to obtain more information, including disease and anthropometric data.
Most households follow healthy practices, especially types of oils consumed, methods of preparing their food as well as keeping salt in an optimal condition and consuming iodized salt. The most important unhealthy nutritional behavior was the high consumption of fast food and outdoor food, especially in urban regions. Unhealthy nutritional behaviors were more prevalent in households with low household and regional SES. It is suggested to consider community nutrition education and socioeconomic disparities should be considered for public health interventions aiming to improve food habits.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving research study participants were approved by the Shiraz University of Medical Sciences (SUMS), Fars, Iran, under the registration code: IR.SUMS.REC.13940598. The consent form was pre-designed and for all interviewed households, before the research questions, the consent form was completed and if the head of the household or the interviewee was satisfied, the study questionnaire was completed. The patients/participants provided their written informed consent to participate in this study.
ZF: analysis and interpretation of data and writing the original draft. MM: writing the original draft. MAM: research idea and study design. AH: questionnaire design, analysis interpretation of data, and review and editing. AF: collect and clear data and review editing. MA: research idea and study design. RS: research idea and study design, patient enrolment, and writing the original draft. All authors have read the final version of the manuscript and approved it.
This project was discussed by the research committee of the Shiraz University of Medical Sciences and approved, and the proposed budget was allocated in the proposal through the same committee in several stages and after the submission of the work report.
All the nutrition experts in the field of health of the Shiraz University of Medical Sciences and the deputy of health during the research helped us in conducting this study. In addition, the research team examining the food consumption patterns of the National Nutrition Research Institute and the Health Research Institute of Shiraz University of Medical Sciences is thanked and appreciated.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Heshmat R, Abdollahi Z, Ghotbabadi FS, Rostami M, Qorbani M, Homami MR, et al. Nutritional knowledge, attitude and practice toward micronutrients among Iranian households: the NUTRI-KAP survey. J Diabet Metab Disord. (2015) 15:1–5. doi: 10.1186/s40200-016-0260-8
2. Kelishadi R, Qorbani M, Motlagh ME, Ardalan G, Heshmat R, Hovsepian S. Socioeconomic disparities in dietary and physical activity habits of Iranian children and adolescents: the CASPIAN-IV study. Arch Iran Med. (2016) 19:530–7. doi: 10.1515/jpem-2016-0041
3. Czarnocinska J, Wadolowska L, Lonnie M, Kowalkowska J, Jezewska-Zychowicz M, Babicz-Zielinska E. Regional and socioeconomic variations in dietary patterns in a representative sample of young polish females: a cross-sectional study (GEBaHealth project). Nutr J. (2020) 19:1–14. doi: 10.1186/s12937-020-00546-8
4. Guallar-Castillón P, Rodríguez-Artalejo F, Fornés NS, Banegas JR, Etxezarreta PA, Ardanaz E, et al. Intake of fried foods is associated with obesity in the cohort of spanish adults from the European prospective investigation into cancer and nutrition. Am J Clin Nutr. (2007) 86:198–205. doi: 10.1093/ajcn/86.1.198
5. Junger WL III, YokooIV EM, Pereirav RA, Sichieri R III. Macronutrient consumption and inadequate micronutrient intake in adults. Rev Saúde Pública. (2013) 47:177s−189s. doi: 10.1590/s0034-89102013000700004
6. Safarpour M, Dorosty Motlagh A, Hosseini SM, Ranjbar Noshari F, Safarpour M, Daneshi Maskooni M, et al. Prevalence and outcomes of food insecurity and its relationship with some socioeconomic factors. Knowl Health. (2014) 8:193–8. doi: 10.1234/knh.v0i0.388
7. Azemati B, Heshmat R, Sanaei M, Salehi F, Sadeghi F, Ghaderpanahi M, et al. Nutritional knowledge, attitude and practice of Iranian households and primary health care staff: NUTRIKAP survey. J Diabet Metab Disord. (2013) 12:1–4. doi: 10.1186/2251-6581-12-12
8. Salehzadeh H, Soori MM, Sadeghi S, Shahsawari S, Mohammadi S, Saifi M, et al. The type and amount of household oil consumption and the influential factors in Sanandaj city, Iran. J Adv Environ Health Res. (2019) 7:1–7.
9. Ganesan K, Sukalingam K, Xu B. Impact of consumption and cooking manners of vegetable oils on cardiovascular diseases-A critical review. Trends Food Sci Technol. (2018) 71:132–54. doi: 10.1016/j.tifs.2017.11.003
10. Krebs-Smith SM, Pannucci TE, Subar AF, Kirkpatrick SI, Lerman JL, Tooze JA, et al. Update of the healthy eating index: HEI-2015. J Acad Nutr Diet. (2018) 118:1591–602. doi: 10.1016/j.jand.2018.05.021
11. Haugsgjerd TR, Egeland GM, Nygård OK, Igland J, Sulo G, Lysne V, et al. Intake of carbohydrates and SFA and risk of CHD in middle-age adults: the Hordaland health study (HUSK). Public Health Nutr. (2020) 25:1-15. doi: 10.1017/S1368980020003043
12. Dietary Guidelines for Americans 2020-2025 9, editor (2020). Available online at: https://health.gov/our-work/nutrition-physical-activity/dietary-guidelines
13. Drouin-Chartier J-P, Brassard D, Tessier-Grenier M, Côté JA, Labonté M-È, Desroches S, et al. Systematic review of the association between dairy product consumption and risk of cardiovascular-related clinical outcomes. Adv Nutr. (2016) 7:1026–40. doi: 10.3945/an.115.011403
14. Gadiraju TV, Patel Y, Gaziano JM, Djoussé L. Fried food consumption and cardiovascular health: a review of current evidence. Nutrients. (2015) 7:8424–30. doi: 10.3390/nu7105404
15. Gebremariam HG, Yesuf ME, Koye DN. Availability of adequately iodized salt at household level and associated factors in Gondar town, Northwest Ethiopia. Int Sch Res Notices. (2013) 2013:1–6. doi: 10.1155/2013/160582
16. Kumma WP, Haji Y, Abdurahmen J, Mehretie Adinew Y. Factors affecting the presence of adequately iodized salt at home in Wolaita, Southern Ethiopia: community based study. Int J Food Sci. (2018) 2018:4394908. doi: 10.1155/2018/4394908
17. Jacky M Knowles GSG 4 Jonathan Gorstein 5 Roland Kupka 6 Ruth Situma 6 Kapil Yadav 7 Rizwan Yusufali CP 7 Grant J Aaron 4 and the Universal Salt Iodization Coverage Team S. Household coverage with adequately iodized salt varies greatly between countries and by residence type and socioeconomic status within countries: results from 10 national coverage surveys. J Nutr. (2017) 147:1004S−14S. doi: 10.3945/jn.116.242586
18. Kshatri JS, Karmee N, Tripathy RM. Prevalence and predictors of poor iodine nutrition in rural South Odisha: a comparative study between coastal and hilly districts. Natl J Commun Med. (2017) 8:41–6.
19. Dynesen AW, Haraldsdottír J, Holm L, Astrup A. Sociodemographic differences in dietary habits described by food frequency questions—results from Denmark. Eur J Clin Nutr. (2003) 57:1586–97. doi: 10.1038/sj.ejcn.1601728
20. Abdollahi M, Mohammadi NF, Houshiarrad A, Ghafarpour M, Ghodsi D, Kalantari N. Socio-economic differences in dietary intakes: the comprehensive study on household food consumption patterns and nutritional status of IR Iran. Nutr Food Sci Res. (2014) 1:19–26.
21. Aslam HM, Alvi AA, Mughal A, Haq Z, Qureshi WA, Haseeb A, et al. Association of socioeconomic classes with diet, stress and hypertension. JPMA J Pak Med Assoc. (2013) 63:289–94.
22. Valeix P, Faure P, Péneau S, Estaquio C, Hercberg S, Bertrais S. Lifestyle factors related to iodine intakes in French adults. Public Health Nutr. (2009) 12:2428–37. doi: 10.1017/S1368980009005515
23. Azizi A, Amirian F, Amirian M. Effects of knowledge, attitude and practice of married women with community oriented medical education in City of Kermanshah City on Iodized salt consumption. Iran J Endocrinol Metab. (2004). 2008:205–10.
24. Karimi-Shahanjarini A, Sharifi M, Bashirian S, Moghimbeigi A, Pour N. Determinants of healthy snacks choice by mothers of 1–5 years old children in Hamadan based on social cognitive theory (SCT). Iran J Nutr Sci Food Technol. (2015) 9:19–26.
25. Rezazadeh A, Rashidkhani B, Omidvar N. Association of major dietary patterns with socioeconomic and lifestyle factors of adult women living in Tehran, Iran. Nutrition. (2010) 26:337–41. doi: 10.1016/j.nut.2009.06.019
26. Kelishadi R, Gheisari A, Zare N, Farajian S, Shariatinejad K. Salt intake and the association with blood pressure in young Iranian children: first report from the middle East and north Africa. Int J Prev Med. (2013) 4:475.
27. Sarlak F, Nabizadeh R, Yunesian M, Rastkari N. Investigate the iodine content in table salts used by families covered by health services of Tehran University of medical sciences in year 2017. Iran J Health Environ. (2019) 11:529–46.
28. Mirhadyan L, Moradi Latreyi S, Pasha A, Kazem Nejad Leili E. Junk food consumption and its associated factors in high school students in Rasht in 2017. J Res Dev Nurs Midwifery. (2020) 17:52–66. doi: 10.29252/jgbfnm.17.1.52
29. Sharifirad G, Yarmohammadi P, Azadbakht L, Morowatisharifabad MA, Hassanzadeh A. Determinants of fast food consumption among Iranian high school students based on planned behavior theory. J Obes. (2013) 2013:147589. doi: 10.1155/2013/147589
30. Yarmohammadi P, Sharifirad GR, Azadbakht L, Morovati SMA, Hassanzadeh A. Predictors of fast food consumption among high school students based on the theory of planned behavior. Health Syst Res. (2011) 7.
31. Ghafari MEL, Ramzankhani A, Souri H. Fast food consumption and its related factors among students: a cross-sectional study. J Health Syst Res. (2013) 8:981–90.
32. Heshmat R, Salehi F, Qorbani M, Rostami M, Shafiee G, Ahadi Z, et al. Economic inequality in nutritional knowledge, attitude and practice of Iranian households: The NUTRI-KAP study. Med J Islam Repub Iran. (2016) 30:426.
33. Kaplan GA, Keil JE. Socioeconomic factors and cardiovascular disease: a review of the literature. Circulation. (1993) 88:1973–98. doi: 10.1161/01.CIR.88.4.1973
34. Turrell G, Mathers CD. Socioeconomic status and health in Australia. Med J Aust. (2000) 172:434–8. doi: 10.5694/j.1326-5377.2000.tb124041.x
35. Grimes CA, Campbell KJ, Riddell LJ, Nowson CA. Is socioeconomic status associated with dietary sodium intake in Australian children? A cross-sectional study. BMJ Open. (2013) 3:1–7. doi: 10.1136/bmjopen-2012-002106
36. Bauer KW, Larson NI, Nelson MC, Story M, Neumark-Sztainer D. Socio-environmental, personal and behavioural predictors of fast-food intake among adolescents. Public Health Nutr. (2009) 12:1767–74. doi: 10.1017/S1368980008004394
37. Mazur RE, Marquis GS, Jensen HH. Diet and food insufficiency among Hispanic youths: acculturation and socioeconomic factors in the third national health and nutrition examination survey. Am J Clin Nutr. (2003) 78:1120–7. doi: 10.1093/ajcn/78.6.1120
38. Adler NE, Boyce T, Chesney MA, Cohen S, Folkman S, Kahn RL, et al. Socioeconomic status and health: the challenge of the gradient. Am Psychol. (1994) 49:15. doi: 10.1037/0003-066X.49.1.15
39. Eshghinia S, Khodarahmi M, Bartimar R, Lashkarboluki F, Asadi J, Saneei P, et al. Socio-economic status versus dietary habits in women living in northeastern Iran. Iran J Nutr Sci Food Technol. (2014) 9:31–9.
Keywords: nutrition behaviors, socio-economic status, level of education, Iran, households
Citation: Foroozanfar Z, Moghadami M, Mohsenpour MA, Houshiarrad A, Farmani A, Akbarpoor MA and Shenavar R (2022) Socioeconomic determinants of nutritional behaviors of households in Fars Province, Iran, 2018. Front. Nutr. 9:956293. doi: 10.3389/fnut.2022.956293
Received: 30 May 2022; Accepted: 30 August 2022;
Published: 26 September 2022.
Edited by:
Prisco Piscitelli, Istituto Scientifico Biomedico Euro Mediterraneo (ISBEM), ItalyReviewed by:
Neha Rathi, Banaras Hindu University, IndiaCopyright © 2022 Foroozanfar, Moghadami, Mohsenpour, Houshiarrad, Farmani, Akbarpoor and Shenavar. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Razieh Shenavar, c2hlbmF2YXIucmF6aWVoQHlhaG9vLmNvbQ==; cnNoZW5hdmFyMTM4N0BnbWFpbC5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.