 Enyu Tong1†
Enyu Tong1† Yiming Chen1†
Yiming Chen1† Yanli Ren1
Yanli Ren1 Yuanyuan Zhou1
Yuanyuan Zhou1 Chunhong Di2
Chunhong Di2 Ying Zhou1Shihan Shao1Shuting Qiu1Yu Hong1
Ying Zhou1Shihan Shao1Shuting Qiu1Yu Hong1 Lei Yang1
Lei Yang1 Xiaohua Tan1*
Xiaohua Tan1*- 1School of Public Health, Hangzhou Normal University, Hangzhou, China
- 2The Affiliated Hospital of Hangzhou Normal University, Hangzhou Normal University, Hangzhou, China
Background: Preoperative carbohydrate loading is an important element of the enhanced recovery after surgery (ERAS) paradigm in adult patients undergoing elective surgery. However, preoperative carbohydrate loading remains controversial in terms of improvement in postoperative outcomes and safety. We conducted a Bayesian network meta-analysis to evaluate the effects and safety of different doses of preoperative carbohydrates administrated in adult patients after elective surgery.
Methods: MEDLINE (PubMed), Web of Science, EMBASE, EBSCO, the Cochrane Central Register of Controlled Trials, and China National Knowledge Infrastructure (CNKI) were searched to identify eligible trials until 16 September 2022. Outcomes included postoperative insulin resistance, residual gastric volume (RGV) during the surgery, insulin sensitivity, fasting plasma glucose (FPG), fasting serum insulin (Fin) level, the serum levels of C-reactive protein (CRP), postoperative scores of pain, patients’ satisfaction, thirst, hunger, anxiety, nausea and vomit, fatigue, and weakness within the first 24 h after surgery and the occurrences of postoperative infection. The effect sizes were estimated using posterior mean difference (continuous variables) or odds ratios (dichotomous variables) and 95 credible intervals (CrIs) with the change from baseline in a Bayesian network meta-analysis with random effect.
Results: Fifty-eight articles (N = 4936 patients) fulfilled the eligibility criteria and were included in the meta-analysis. Both preoperative oral low-dose carbohydrate loading (MD: –3.25, 95% CrI: –5.27 to –1.24) and oral high-dose carbohydrate loading (MD: –2.57, 95% CrI: –4.33 to –0.78) were associated with postoperative insulin resistance compared to placebo/water. When trials at high risk of bias were excluded, association with insulin resistance was found for oral low-dose carbohydrate loading compared with placebo/water (MD: –1.29, 95%CrI: –2.26 to –0.27) and overnight fasting (MD: –1.17, 95%CrI: –1.88 to –0.43). So, there was large uncertainty for all estimates vs. control groups. In terms of safety, oral low-dose carbohydrate administration was associated with the occurrences of postoperative infection compared with fasting by 0.42 (95%Crl: 0.20–0.81). In the other outcomes, there was no significant difference between the carbohydrate and control groups.
Conclusion: Although preoperative carbohydrate loading was associated with postoperative insulin resistance and the occurrences of postoperative infection, there is no evidence that preoperative carbohydrate administration alleviates patients’ discomfort.
Systematic review registration: [https://www.crd.york.ac.uk/PROSPERO/], identifier [CRD42022312944].
Introduction
Surgery, as a form of stress, induces peripheral insulin resistance, which can result in hyperglycemia, which, in turn, may have potentially adverse effects on postoperative patients (1, 2). Efficient management of preoperative interventions could reduce postoperative complications and facilitate recovery.
Enhanced recovery after surgery (ERAS) is a multimodal, multidisciplinary project aimed at improving the recovery of patients undergoing surgery during the entire perioperative period (3). The overall complication occurrences were reduced by up to 50% when the ERAS protocols were used compared with traditional perioperative patient management (4, 5).
The preoperative administration of carbohydrate loading as a part of ERAS protocols reduces insulin resistance and tissue glycosylation, improves postoperative glucose control, and enhances postoperative comfort (6). Several randomized controlled trials (RCTs) and meta-analysis have shown that preoperative carbohydrate loading decreased postoperative insulin resistance and side effects compared with those consuming placebo/water or in a fasted state (7, 8). Other RCTs, however, have shown that perioperative carbohydrate administration had no effect on postoperative insulin resistance (9, 10). Thus, the administration of preoperative carbohydrates remains somewhat controversial.
The conventional pairwise meta-analysis has its limitations. First, the previous meta-analysis cannot compare different controls (such as fasting, placebo, or water) simultaneously, so these meta-analyses need to combine these groups into one treatment arm, thus limited interpretability (8). Second, because of the scarcity of direct head-to-head comparisons of interventions in trials, it is unable to assess the comparative effects of interventions (11).
Therefore, to overcome this limitation, we conducted an updated systematic review and network meta-analysis (NMA) to pool and analyze data comparing different preoperative drinks used for clinical and metabolic postoperative outcomes in adult patients undergoing elective surgery (12).
Materials and methods
Protocol registration
This is a systematic review and NMA of preoperative carbohydrate intervention trials in adult patients undergoing elective surgery. The Preferred Reporting Items for Systematic Reviews (PRISMA) and Meta-analyses for RCTs were used to organize the reporting (13). The study protocol was registered (registration number: CRD42022312944) with the International Prospective Register of Systematic Reviews (PROSPERO) following the standard reporting method.
Data sources
MEDLINE (PubMed), Web of Science, EMBASE, EBSCO, the Cochrane Central Register of Controlled Trials, and China National Knowledge Infrastructure (CNKI) were searched to identify eligible trials. We updated the literature search weekly, and the search was performed from database inception until 16 September 2022 (details are shown in Supplementary Table 1).
Trial selection criteria
Eligible trials included the preoperative administration of at least 10 g carbohydrate loading (orally or intravenously) before 4 h of the surgery started, and with fasting, placebo, or water, undergoing any type of elective surgery in adults. Studies also included carbohydrate-based solutions containing other compounds (such as glutamine and whey protein). Patients with diabetes mellitus or those who were receiving emergency surgery were also excluded.
Trial identification
Two investigators independently screened articles by title, abstract, and full text using the inclusion criteria. The inclusion of a study was decided by consensus between the two investigators. When differences occurred, investigators consulted or discussed with a third one to solve them.
Intervention categories
Five categories were used to classify the preoperative administration for the included RCTs:
(1) Low-dose carbohydrate: The dose of oral carbohydrate is between 10 and 50 g before surgery (10–50 g);
(2) High-dose carbohydrate: The dose of oral carbohydrate is greater than 50 g before surgery (>50 g);
(3) Carbohydrate, iv: preoperative carbohydrate by intravenous perfusion;
(4) Placebo/water (control group);
(5) Fasting (control group).
Outcome measures
The primary outcome was mean change from baseline to the end point (within the first 24 h after surgery) in insulin resistance, as measured by the Homeostasis Model Assessment of Insulin Resistance (HOMA-IR) method according to the following equation: HOMA-IR = [fasting insulin(μU/mL) × fasting glucose (mmol/L)]/22.5)]. Secondary outcomes were included: residual gastric volume (RGV) during the operation; insulin sensitivity (measured by the hyperinsulinemic glucose clamp method) within the first 24 h after surgery; fasting plasma glucose (FPG) within the first 24 h after surgery; fasting serum insulin (Fin) level within the first 24 h after surgery; the serum levels of C-reactive protein (CRP) within the first 24 h after surgery; postoperative pain, patients’ satisfaction, thirst, hunger, anxiety, postoperative nausea and vomit (PONV), fatigue, weakness (all measured on a visual analog scale [VAS]), and the occurrences of postoperative infection.
Data extraction
The following study characteristics were extracted for each eligible study: (1) trial information: the first author, study year, the study country, and trial name; (2) patient characteristics: sample size in each treatment, the type of surgery, and American Society of Anesthesiologists (ASA) grade; (3) intervention details: the type, total dose, administrate route, and timing of each treatment; (4) outcome measures: the primary or secondary outcomes including insulin resistance, RGV, insulin sensitivity, FPG, Fin level, the serum levels of CRP, pain, thirst, hunger, anxiety, nausea and vomit, fatigue, weakness within the first 24 h after surgery, and the occurrences of postoperative infection.
Quality and risk of bias assessment
The quality of every eligible trial was assessed independently by two researchers based on the Cochrane risk of bias 2.0 tool in RCTs in a blind fashion (14), which contains five domains: randomization process, deviations from the intended interventions, missing outcome data, measurement of the outcome, and selection of the reported result. Disagreements were discussed and resolved through consensus.
Data synthesis and analysis
We estimated the effect sizes for group differences with respect to baseline changes. We used the imputation of correlation when standard deviations were not available for the mean change value, but were available for baseline and endpoint values (15). Arithmetic difference between baseline and end point was used when the study did not report mean change. Meta-analytic calculations were conducted using R Version 4.1.2 (RStudio, Boston, MA, USA) (16). We performed a Bayesian network model and all analyses were conducted using the “gemtc” package version 1.0-1 (17) and jagsUI packages version 1.5.2 (18). Network plot command of Stata version 16.0 (StataCorp, College Station, TX 77845, USA) was used to draw the comparison-adjusted funnel (19).
Mean difference (MD) was used to model continuous variables, whereas dichotomous outcomes were modeled using a binomial likelihood and logit link (20). The outcomes were converted to standard units. Additionally, missing standard deviations were calculated from standard errors, ranges, or interquartile ranges as described in the Cochrane Handbook (21). In this study, a NMA was conducted within a Bayesian framework to assess the relative effectiveness of preoperative carbohydrate loading for recovery after elective surgery.
The consistency model and the inconsistency model were used to analyze all outcomes, and the difference in deviance information criterion (DIC) and I2 was used to compare the overall findings. If the difference in DIC between the two models was ≥ 5, we used the inconsistency model. Both a fixed-effect model and a random model were run for each result, and a lower DIC value indicated a greater model fit.
The Markov chain Monte Carlo (MCMC) algorithm was used to estimate the posterior densities of all unknown parameters in each model. It was based on simulations of 200,000 iterations in each of four chains and provided evidence for confirming the convergence of the models.
The trials we included were tested for consistency and inconsistency. We used the node splitting method to perform to compare the treatment effect direct and indirect comparisons of multiple interventions, and P > 0.05 was considered to indicate good consistency (22, 23).
Probability values were summarized and are reported as the surface under the cumulative ranking (SUCRA) curve. When the intervention was certain to be the worst, the SUCRA value would be 0, and when it was certain to be the best, the SUCRA value would be 1 (24).
To investigate the source of heterogeneity, meta-regression was used to explore and account for the heterogeneity with the risk of bias, the category of surgery, and the blinding of these studies’ designs.
The planned sensitivity analyses of the outcomes were conducted to evaluate the robustness of the model. First, in addition to the Bayesian random effect network, sensitivity analyses were performed using a fixed-effect network. Second, the transitivity assumption was tested by splitting the “water or placebo” group within the network. Third, all analyses were repeated after excluding high-risk trials and data from imputation methods. In addition, for the primary outcome, we planned to add subgroup analyses conducted for different surgical categories, and a comparison-adjusted funnel plot was used to assess the presence of small-study effects bias.
The Confidence in Network Meta-Analysis (CINeMA) methodological framework and application were used to evaluate confidence in NMA effect estimates for all outcomes and treatment comparisons (25, 26).
Results
Study selection
A total of 9411 records were retrieved, of which 58 articles (N = 4936 patients) fulfilled the eligibility criteria and were included in the meta-analysis, the retrieval process is shown in Figure 1. A total of five interventions were included in this meta-analysis: oral low-dose carbohydrate (10–50 g) loading, oral high-dose carbohydrate (more than 50 g) loading, carbohydrate by intravenous perfusion (Carbohydrate, iv), placebo/water, and fasting. Detailed trial and patient characteristics are shown in Table 1.
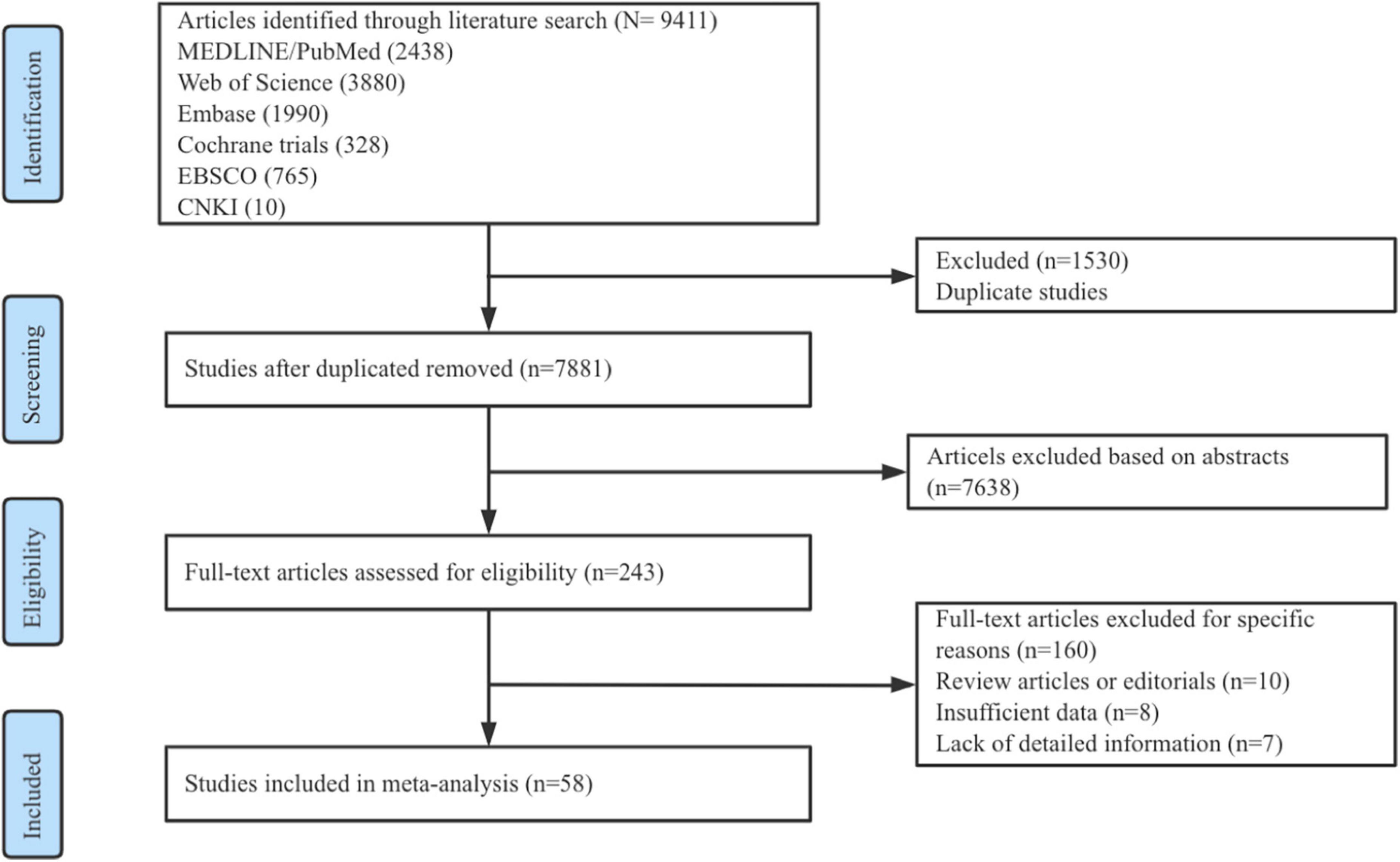
Figure 1. Flow diagram of study identification, screening, eligibility assessment, and inclusion.
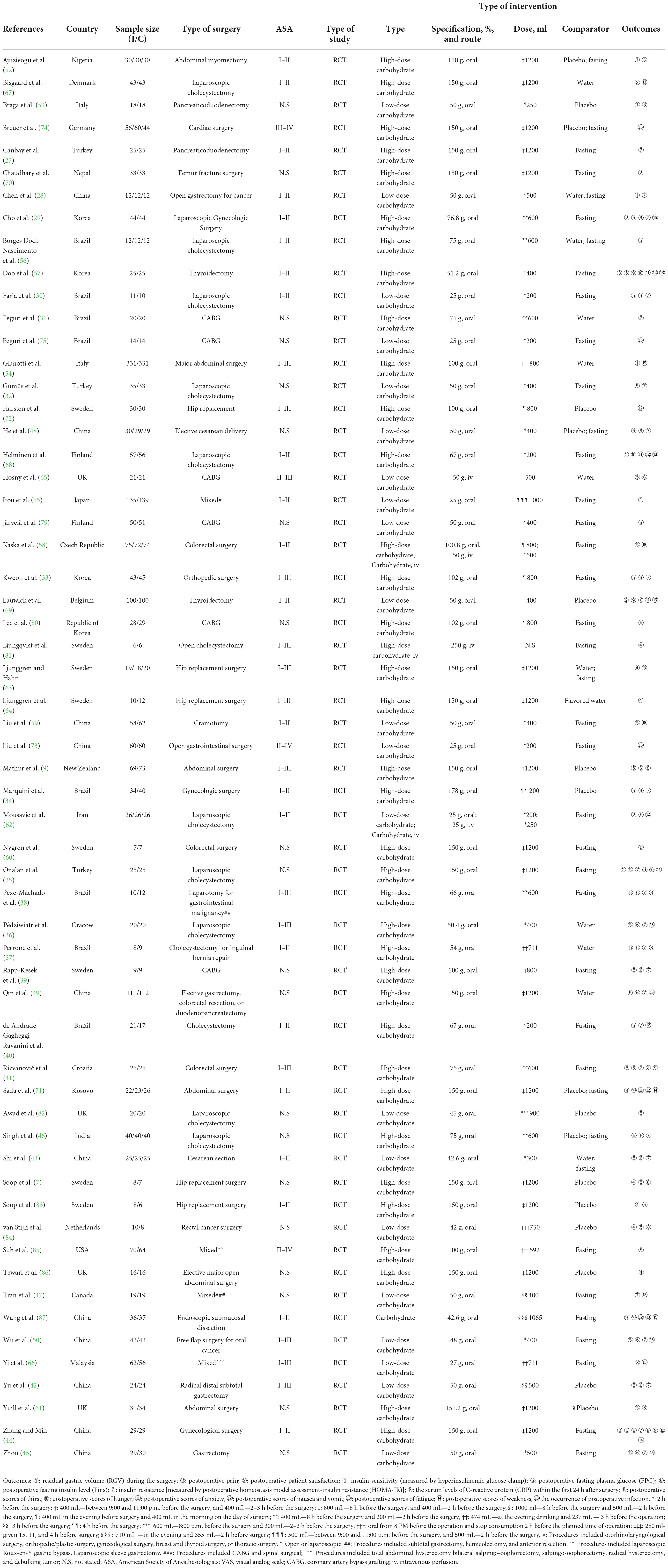
Table 1. Characteristics of the included studies.
Risk of bias and quality of evidence
The overall quality of RCTs included in the network was high and moderate. The risk of bias of 58 studies included in the meta-analysis is shown in Figure 2 (details of the risk of bias 2.0 assessment in each trial are shown in Supplementary Figure 1). According to the risk of bias 2.0 tool of Cochrane Collaboration, 25 (43%) studies were high-quality across all domains and 12 RCTs (21%) were at high risk of bias.
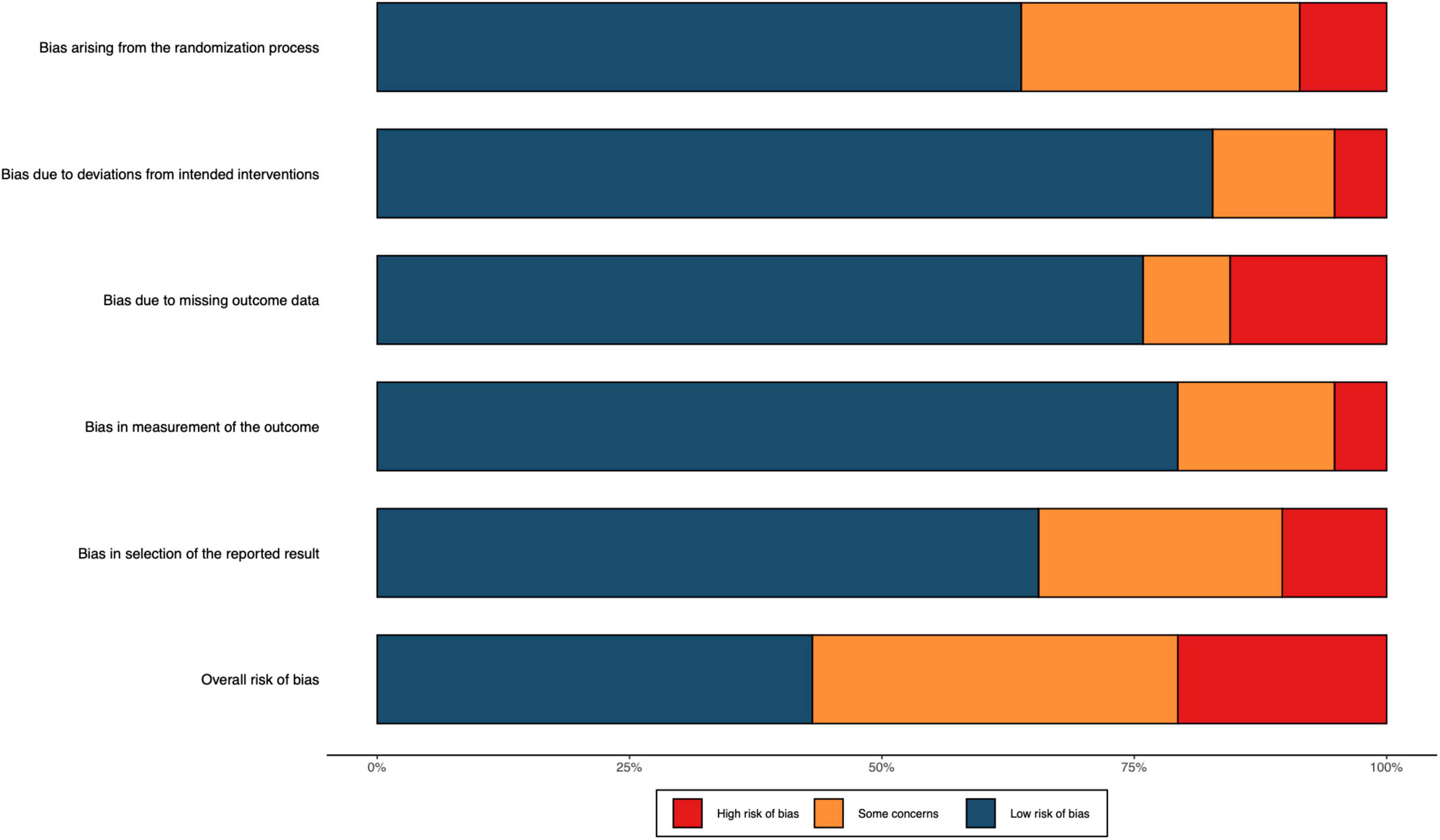
Figure 2. Risk of bias included RCTs. The colors in the bar next to each row/criteria represent the percentage of total studies falling within the high risk of bias/some concerns/low risk of bias.
Primary outcome
The primary outcome of this study was postoperative insulin resistance, and it was measured by the homeostasis model assessment-insulin resistance (HOMA-IR) method. The network plot for the primary outcome is shown in Figure 3. Each circle represented an intervention, and the area of each circle was proportional to the number of patients for which the intervention was accepted and indicated the sample size, and the width of the line was proportional to the number of trials that directly compared the two interventions.
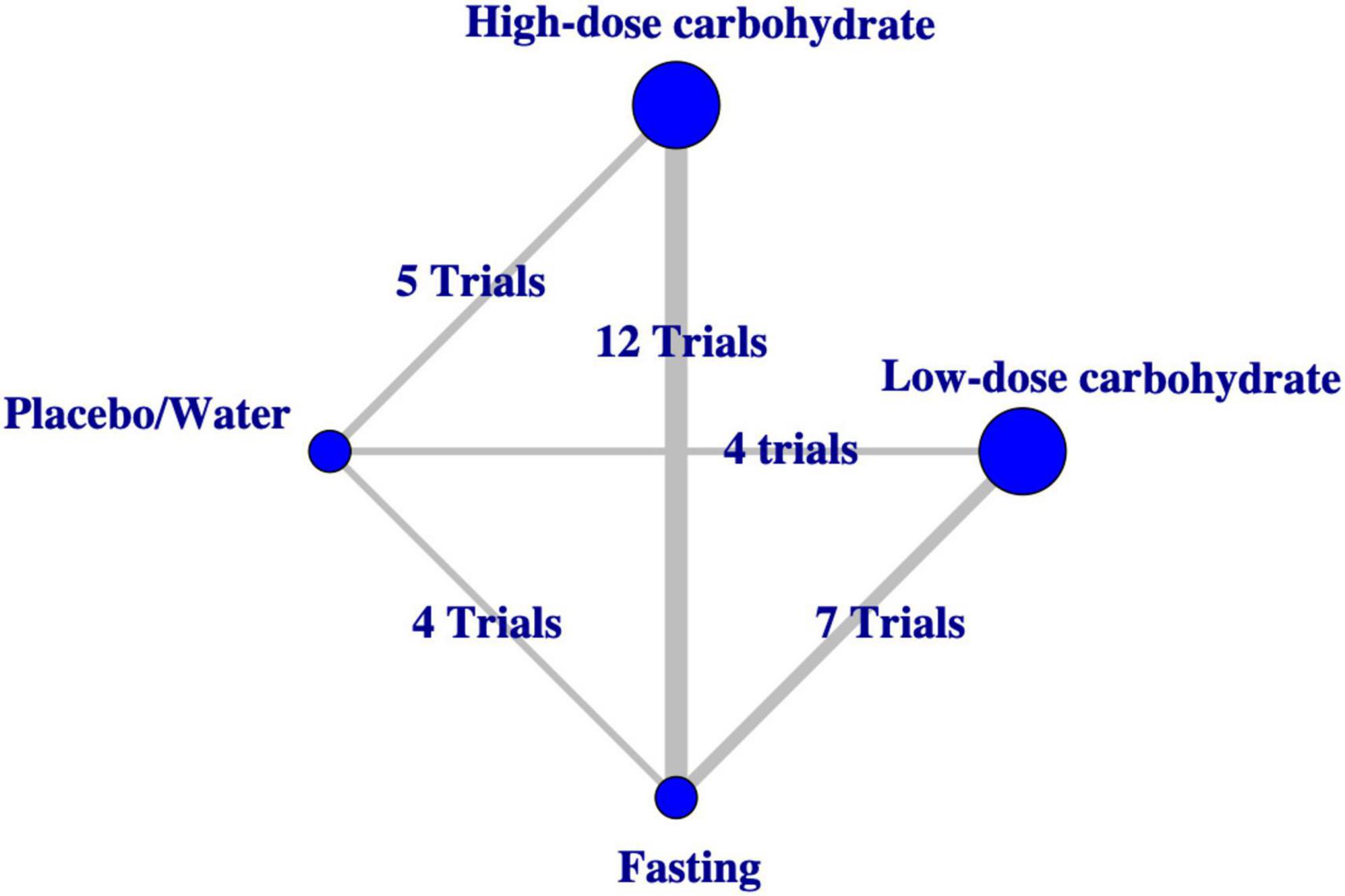
Figure 3. Network plot of evidence comparing different interventions for the primary outcome.
Twenty-four studies with 1,390 patients reported insulin resistance during the study period (27–51). Both interventions associated insulin resistance compared with placebo/water, with MD ranging from –3.25 (95%CrI, –5.27 to –1.24) for administrated oral low-dose carbohydrate to –2.57 (95%CrI, –4.33 to –0.78) for oral high-dose carbohydrate loading before surgery. The subgroup analysis based on the category of surgery revealed that the association of oral low-dose carbohydrate compared to placebo/water would correlate with insulin resistance (MD, –4.37 [95%CrI, –8.42 to –0.47]) for patients undergoing major abdominal surgery. Figure 4 shows the results. The result of CineMA represents the confidence in this estimate was low (Supplementary Table 2).
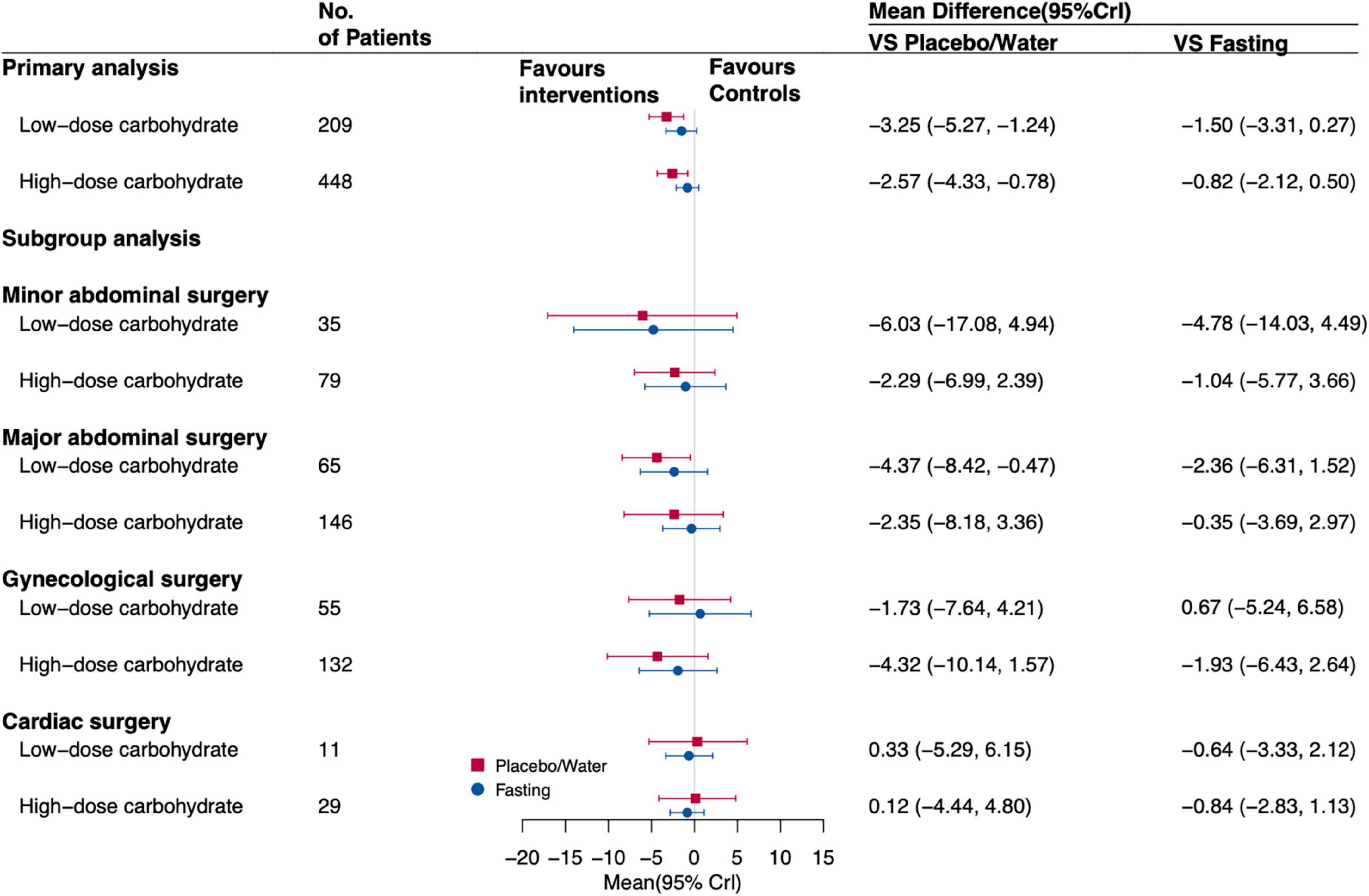
Figure 4. Forest plot for the estimates of different interventions on IR of postoperative patients. Values are mean differences (MDs) with 95% confidence intervals (Crls).
Among all trials included, oral low-dose carbohydrate loading had the highest probability of being the best intervention (SUCRA value of 0.74 compared with other interventions). The corresponding results of SUCRA values are shown in Figure 5. Inconsistency analysis calculated by the node split method showed no significant difference between direct and indirect evidence of this network model, with P-value ranging from 0.05 to 0.32 (Supplementary Table 3). The result of the network meta-regression shows that the covariates we included may not affect the value of insulin resistance (Supplementary Table 4).
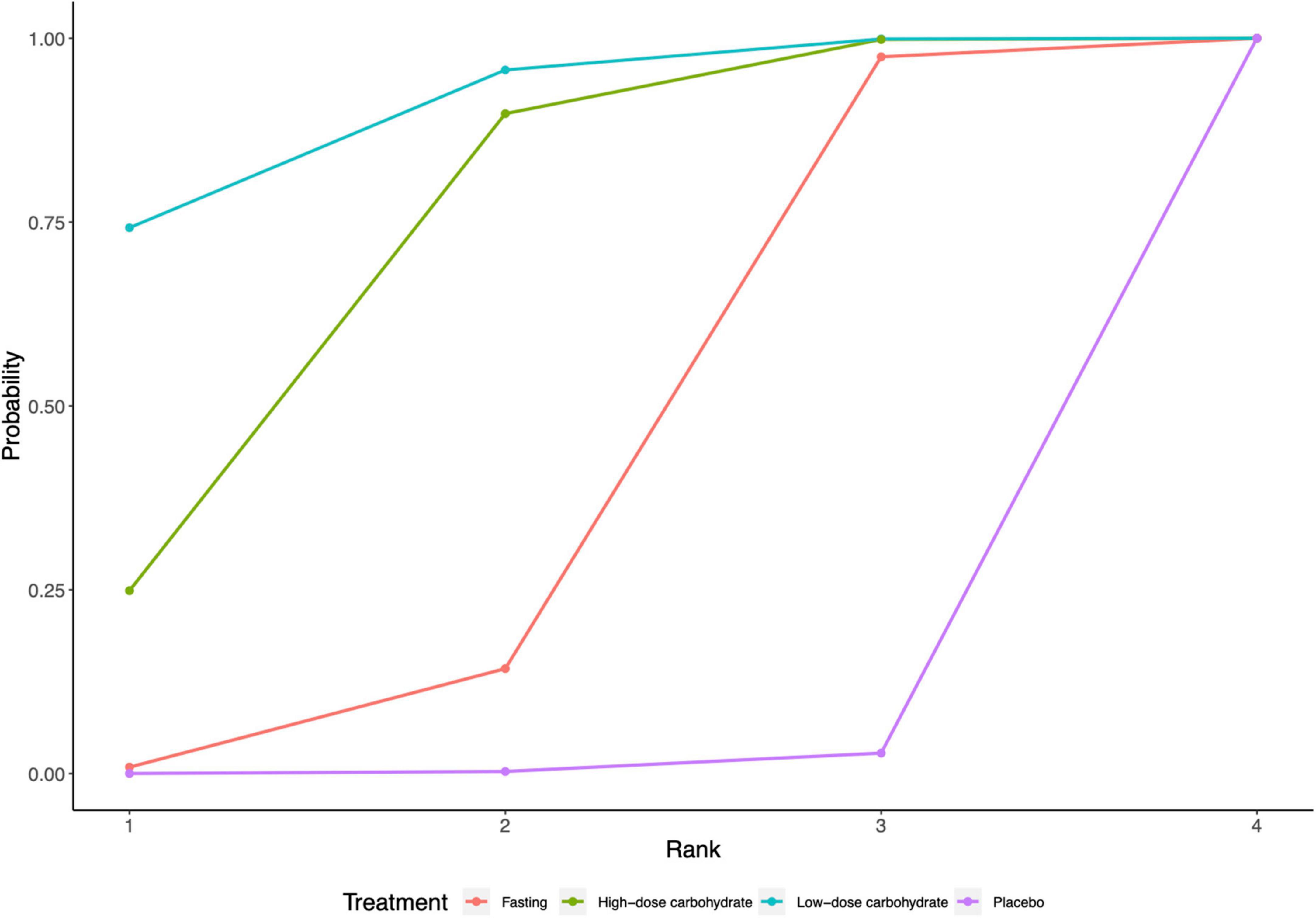
Figure 5. Surface under the cumulative ranking curve (SUCRA) for HOMA-IR.
After excluding studies with a high risk of bias and data of trials with imputation methods (network plot is shown in Supplementary Figure 2), there was an association of oral low-dose carbohydrate loading (MD, –1.29 [95%CrI, –2.26 to –0.27]) with insulin resistance for postoperative patients compared with placebo/water remained. Oral low-dose carbohydrate loading (MD, –1.17 [95% CrI, –1.88 to –0.43]) administration was associated with insulin resistance compared with fasting. The subgroup analysis showed that when patients undergoing major abdominal surgery, administrated oral low-dose carbohydrates before surgery was associated with insulin resistance (MD, –1.35 [95% CrI, –2.64 to –0.01]) compared with fasting. Figure 6 shows the forest plot results. And the SUCRA followed a similar pattern, with oral low-dose carbohydrates having the highest probability of being the best intervention when compared with other interventions; the SUCRA value is 0.88 (Supplementary Table 5).
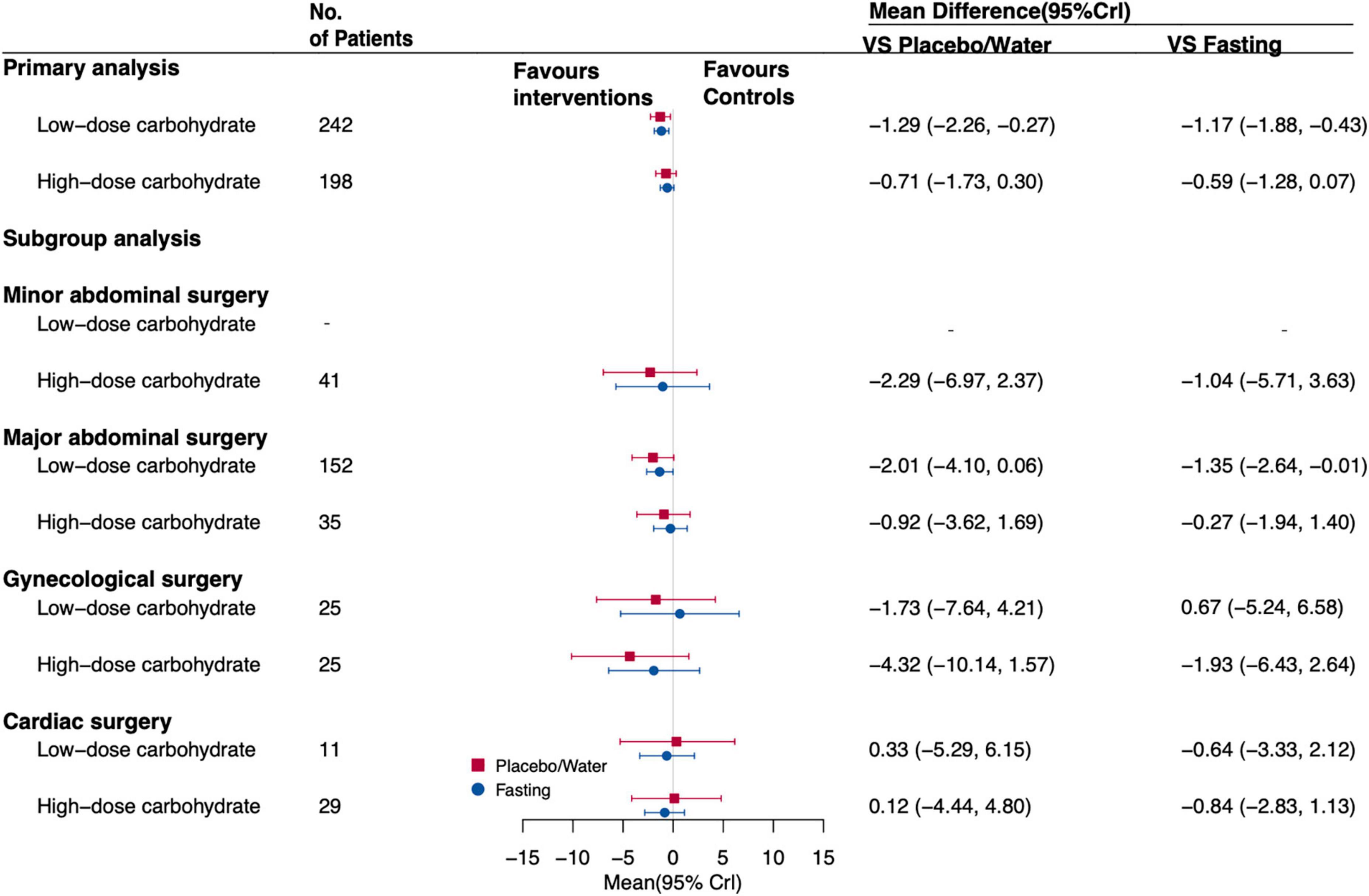
Figure 6. Forest plot for the estimates of different interventions on IR of postoperative patients that excluded trials at high risk of bias and data for the imputation methods. Values are mean differences (MDs) with 95% confidence intervals (CrIs).
A comparison-adjusted funnel plot for postoperative insulin resistance implies the presence of publication bias between the carbohydrate groups and controls (Supplementary Figure 3).
Secondary outcomes
Supplementary Figure 4 represents network plots for each secondary outcome. The confidence in these estimates was generally moderate to very low (Supplementary Table 6).
Residual gastric volume during the surgery (mL)
Four studies reported RGV of intraoperative, involving 1,062 participants (52–55). The multiple-treatments meta-analysis results are shown in Table 2. There was no statistically significant difference between the groups in the network.
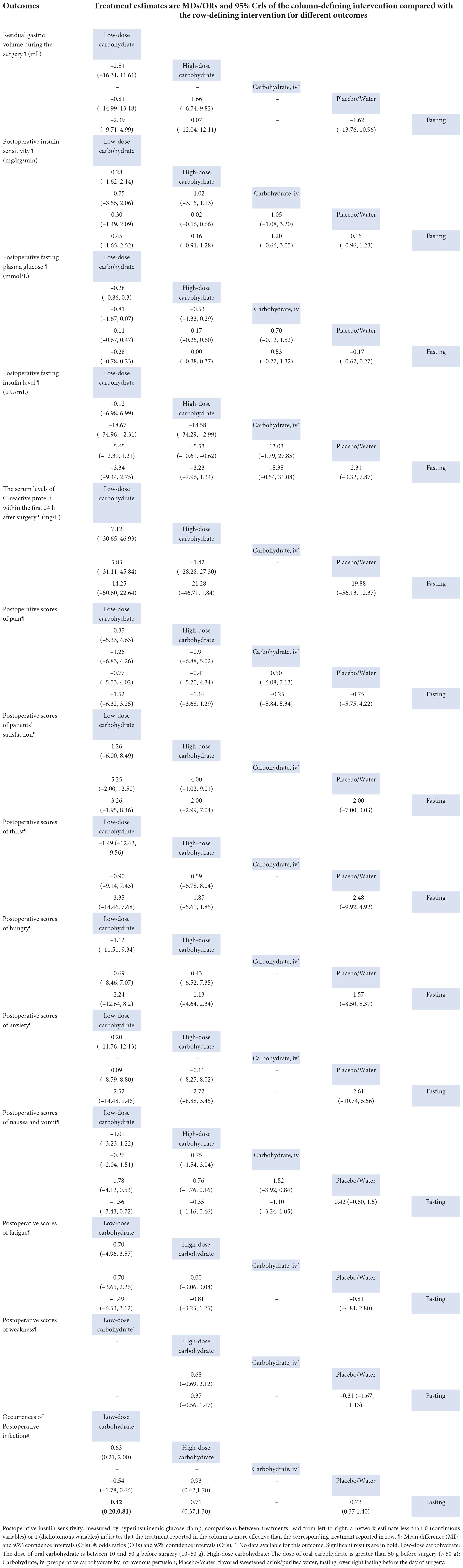
Table 2. Network meta-analysis matrix of secondary outcomes.
Postoperative insulin sensitivity (mg/kg/min)
Seven trials measured insulin sensitivity by hyperinsulinaemic–euglycaemic clamp method, involving 170 participants. The results showed carbohydrate loading dose had no significant differences in any of the comparisons (Table 2).
Postoperative fasting plasma glucose (mmol/L)
Twenty-seven trials reported the FPG of patients after surgery, involving 1886 participants (30–37, 40–50, 56–65). Compared with the control groups, preoperative carbohydrate loading had no significant effect on postoperative FPG. Table 2 shows the results.
Postoperative Fin level (μU/mL)
Twenty-two studies were included, with data available for 1,379 participants (9, 29, 30, 33, 34, 36–46, 48–50, 61, 64, 65). Compared with placebo or water, high-dose carbohydrate loading before surgery was associated with a decrease in Fin level (MD, –5.53 [95%Crl, –10.61 to –0.62]). However, because the confidence interval was wide and close to insignificance, the results should be interpreted with caution. Table 2 displays the results of the multiple-treatments meta-analysis.
The serum levels of C-reactive protein within the first 24 h after surgery
Seven studies collected blood samples to assess the serum levels of CRP, with data available for 443 participants (9, 37, 38, 41, 44, 53, 66). Multiple-treatments meta-analysis shows no significant difference in any of the companions (Table 2).
Postoperative scores of pain
Eight studies reported postoperative scores of pain scores using a VAS, with data available on 739 participants (29, 35, 44, 62, 67–70). The results found no statistically significant difference after surgery (Table 2).
Postoperative scores of patients’ satisfaction
This was reported by two studies using a VAS, with data available on 140 participants (52, 57). Multiple-treatments meta-analysis found no significant difference in any of the treatments within the network (Table 2).
Postoperative scores of thirst
Six studies reported postoperative thirst scores using a VAS, with data available on 539 participants (35, 44, 57, 68, 69, 71). The results found no statistically significant difference after surgery (Table 2).
Postoperative scores of hungry
This was reported by six studies using a VAS, with data available on 539 participants (35, 44, 57, 68, 69, 71). Multiple-treatments meta-analysis found no significant difference in any of the treatments within the network (Table 2).
Postoperative scores of anxiety
Three studies reported postoperative anxiety scores; all trials used a VAS, with data available on 318 participants (35, 69, 71). The results found no statistically significant difference after surgery (Table 2).
Postoperative scores of nausea and vomit
Seven studies reported postoperative nausea and vomiting scores; all trials used a VAS, and data on 527 participants were available (40, 46, 57, 62, 68, 71, 72). Multiple-treatments meta-analysis found no significant difference in any of the treatments within the network (Table 2).
Postoperative scores of fatigue
This was reported by four studies using a VAS, with data available on 449 participants (57, 67–69). Multiple-treatments meta-analysis found no significant difference in any of the treatments within the network (Table 2).
Postoperative scores of weakness
Two studies reported postoperative weakness scores using a VAS, with data available on 126 participants (44, 71). The results found no statistically significant difference after surgery (Table 2).
The occurrences of postoperative infection
Eleven studies reported the occurrences of postoperative infection, with data available on 1,765 participants (36, 45, 49, 50, 54, 58, 59, 66, 73–75) (Table 2). The NMA result revealed that compared with fasting, low-dose carbohydrate could reduce the occurrences of postoperative infection with statistical significance (odds ratio, 0.42 [95%Crl: 0.20–0.81]). The results of the network meta-regression shows that the covariates we included may not affect the value of secondary outcomes, except the postoperative FPG (Supplementary Table 7).
The value of SUCRA represented that oral low-dose carbohydrate loading had the highest probability of being the best intervention relative to other interventions in patients’ postoperative comfort except for postoperative insulin sensitivity (mg/kg/min), fasting insulin levels (μU/mL), postoperative satisfaction, and weakness (Supplementary Table 8).
Network meta-regression showed that the covariates did not, indeed, influence the value of primary and secondary outcomes (Supplementary Table 9). When trials with a high risk of bias and imputed data were excluded, the results for the secondary outcomes were similar (Supplementary Table 11).
Sensitivity analyses
A summary of clinical and statistical sensitivity analyses is given in Supplementary Tables 10, 11. In the clinical sensitivity, after splitting the “water/placebo” group into two separate arms, postoperative insulin resistance reported a significant MD of –4.02 (95% CrI [–6.46, –1.63]) for low-dose carbohydrate vs. placebo, and MD of –3.65 (95% CrI [–6.24, –1.06]) for high-dose carbohydrate vs. placebo, and the sensitivity analyses were consistent with the main analysis of the secondary outcomes. In the statistical sensitivity analyses, when excluding trials at high risk of bias and data for the imputation methods, oral low-dose carbohydrate loading compared to placebo/water associated with postoperative insulin resistance (MD, –1.29 [95% CrI, –2.26 to –0.27]) for postoperative patients, and compared with fasting, insulin resistance was correlated with oral low-dose carbohydrate (MD, –1.17 [95% CrI, –1.88 to –0.43]). The other results did not differ significantly.
Discussion
Summary of findings
The latest practice guidelines for preoperative fasting recommend that clear liquids may be ingested for up 2 h before an operation; however, it reported less thirst and hunger for fasting time of 2–4 h compared to more than 4 h of fasting, however, it reported equivocal findings for RGV, blood glucose values, hunger, and thirst of nutritional or carbohydrate drinks at 2–4 h relative to more than 4 h of fasting (1).
This NMA represents the most comprehensive analysis of currently available data regarding preoperative carbohydrate loading for patients undergoing elective surgery. We combined direct and indirect evidence from 58 trials comparing four different intervention arms in 4,936 patients undergoing elective surgery. The study that included sufficient numbers of patients to prove a potential association in clinical outcomes was of patients undergoing elective surgery, and it included the most patients available in the current literature. To maintain the homogeneity of interventions, our research divided the dose of carbohydrate loading into low dose (10–50 g) and high dose (>50 g). Our main findings indicate that among patients undergoing elective surgery, preoperative low-dose carbohydrate loading has been found to be associated with insulin resistance and postoperative infection rates.
Three published meta-analyses explored the influence of low-carbohydrate loading on postoperative outcomes (2, 8, 12). However, reports of the effects of carbohydrate loading on insulin sensitivity remain inconsistent. Smith et al. (8) conducted that no significant association was between carbohydrate loading and insulin resistance An earlier NMA of 43 RCTs found that only high-dose carbohydrate administration resulted in a statistically significant associated with insulin resistance compared with fasting, and water or placebo, but with wide confidence intervals so the results are not credible (12). A recent meta-analysis has investigated that compared with fasting, preoperative administration of carbohydrate associated with insulin resistance (2). In our study, we found that oral carbohydrate loading was associated with insulin resistance compared with placebo or water, and the association was still observed in an analysis of excluded high-risk trials and data for the imputation methods. A separate subgroup analysis based on the surgical categories identified the true effect of low-dose carbohydrate loading on insulin resistance, especially those undergoing major abdominal surgery that would otherwise be confounded by other surgical categories. This effect might be due to the preoperative carbohydrate loading, which stimulates an endogenous insulin release and switches off the overnight fasting metabolic state, toward anabolism (63). It should be mentioned that the confidence effect estimate is low or very low, and the significant heterogeneity among studies (different categories of surgery, different types of carbohydrates, and different populations); therefore, the result regarding the effect of carbohydrate loading on insulin resistance must be interpreted with caution.
The present meta-analysis found that oral high-dose carbohydrate (>50 g) was more effective in postoperative outcomes than relative to low-dose carbohydrate, and there is no dose–response relationship between carbohydrate and postoperative outcomes. This may be related to the fact that there is less data available in the network for low-dose carbohydrate comparisons, so some results have wider confidence intervals than in high-dose comparisons.
The gold standard of insulin sensitivity is measured by the hyperinsulinemic–euglycemic clamp method in humans (76). However, we found a small number of studies (n = 7) for this outcome, which could be due to the fact that it is a time-consuming, labor-intensive, and invasive procedure. The multiple-treatments meta-analysis found no evidence that carbohydrate loading was more or less effective in reducing insulin sensitivity compared with placebo/water or fasting. Therefore, more randomized controlled trials need to be included in future analyses to further confirm this outcome.
A recent meta-analysis has investigated that compared with fasting, preoperative administration of carbohydrates decreased patients’ thirst, hungry, and pain (2). Meanwhile, in our study, there was no difference in postoperative patients’ comfort between the administration of preoperative carbohydrates and control groups, and no other significant differences were found in any of the other secondary outcomes. However, some of these results had wide confidence intervals, indicating that data availability is limited. Future well-designed randomized studies will need to examine the biochemical effects and recovery of preoperative carbohydrate loading in elective surgery.
Strengths and limitations
This review has some strengths: First, a comprehensive search was conducted to identify eligible trials; independent study selection, data extraction, and risk of bias assessment were performed by two reviewers; and the CINeMA was used to assess confidence in the NMA results. Second, we also conducted a network meta-regression to evaluate which variables might influence the postoperative outcomes. This review used a Bayesian framework to overcame the tendency of the frequentist approach to be unstable in parameter estimation and obtain biased results (77). Third, we tested different model assumptions to verify the reliability of outcomes in this NMA. Fourth, a NMA is performed to analyze the effect of preoperative carbohydrate loading on various postoperative recovery indicators among elective surgery patients, compensating for the lack of direct comparison between them.
This study has several limitations. First, the results of this meta-analysis are highly dependent on the quality of the trials included. According to the CINeMA results, the evaluation of the credibility of results was from moderate to very low, and there was large uncertainty regarding all the estimates. Second, although 58 RCTs were retrieved, only 21 trials reported postoperative low-dose carbohydrate administration in the network, two studies reported preoperative carbohydrate by intravenous perfusion, and there were relatively few direct comparisons. Third, this may, however, be a type II error (false-negative findings), as only a few trials are available to assess postoperative outcome indicators in many second outcomes. Fourth, small trials tend to report larger beneficial effects than large trials; however, only three trials in our review included more than 100 patients per arm, which may introduce bias due to small-study effects (78). Fifth, the SUCRA value was used to estimate a ranking probability of comparative effectiveness between the different interventions. Sixth, many trials, lack good design, resulting in combining different types of carbohydrates into one group and placebo and water into one group for the main analysis. Finally, double-blinding was not applied in many trials designs included, which may affect the results, but this is also difficult to resolve because fasting and drinking are easily known by the participants, and subsequent experiments need to be further refined.
Conclusion
In summary, when compared with fasting and placebo/water, preoperative carbohydrate appears to be associated with some postoperative outcomes; however, more research into these drinks, preferably multi-types carbohydrate trials are required to improve the strength of the evidence and inform clinical practice.
Data availability statement
The original contributions presented in this study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
ET, YC, YR, and YYZ designed and conducted the research. ET completed the first draft of the manuscript. YZ, SS, and SQ analyzed the data and performed the statistical analyses. CD, YH, and LY substantively revised it. XT critically reviewed the manuscript. All authors contributed to the design of the research (project conception, development of the overall research plan) and approved the final manuscript.
Funding
This study was supported by grants from the Natural Science Foundation of Zhejiang Province (grant nos. LQ18H190003 and LY12H16028) and the National Natural Science Foundation of China (grant no. 81772168).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnut.2022.951676/full#supplementary-material
References
1. American Society of Anesthesiologists Committee. Practice guidelines for preoperative fasting and the use of pharmacologic agents to reduce the risk of pulmonary aspiration: application to healthy patients undergoing elective procedures: an updated report by the American society of anesthesiologists task force on preoperative fasting and the use of pharmacologic agents to reduce the risk of pulmonary aspiration. Anesthesiology. (2017) 126:376–93. doi: 10.1097/aln.0000000000001452
2. Cheng P-L, Loh E-W, Chen J-T, Tam K-W. Effects of preoperative oral carbohydrate on postoperative discomfort in patients undergoing elective surgery: a meta-analysis of randomized controlled trials. Langenbecks Arch Surg. (2021) 406:993–1005. doi: 10.1007/s00423-021-02110-2
3. Engelman DT, Ben Ali W, Williams JB, Perrault LP, Reddy VS, Arora RC, et al. Guidelines for perioperative care in cardiac surgery: enhanced recovery after surgery society recommendations. JAMA Surg. (2019) 154:755–66. doi: 10.1001/jamasurg.2019.1153
4. Thiele RH, Rea KM, Turrentine FE, Friel CM, Hassinger TE, McMurry TL, et al. Standardization of care: impact of an enhanced recovery protocol on length of stay, complications, and direct costs after colorectal surgery. J Am Coll Surg. (2015) 220:430–43. doi: 10.1016/j.jamcollsurg.2014.12.042
5. Ljungqvist O, Scott M, Fearon KC. Enhanced recovery after surgery: a review. JAMA Surg. (2017) 152:292–8. doi: 10.1001/jamasurg.2016.4952
6. Ljungqvist O. Modulating postoperative insulin resistance by preoperative carbohydrate loading. Best Pract Res Clin Anaesthesiol. (2009) 23:401–9.
7. Soop M, Nygren J, Myrenfors P, Thorell A, Ljungqvist O. Preoperative oral carbohydrate treatment attenuates immediate postoperative insulin resistance. Am J Physiol Endocrinol Metab. (2001) 280:E576–83. doi: 10.1152/ajpendo.2001.280.4.E576
8. Smith MD, McCall J, Plank L, Herbison GP, Soop M, Nygren J. Preoperative carbohydrate treatment for enhancing recovery after elective surgery. Cochrane Database Syst Rev (2014) 8:CD009161.
9. Mathur S, Plank LD, McCall JL, Shapkov P, McIlroy K, Gillanders LK, et al. Randomized controlled trial of preoperative oral carbohydrate treatment in major abdominal surgery. Br J Surg. (2010) 97:485–94. doi: 10.1002/bjs.7026
10. Brady MC, Kinn S, Stuart P, Ness V. Preoperative fasting for adults to prevent perioperative complications. Cochrane Database Syst Rev. (2003) 4:CD004423.
11. Higgins JP, Welton NJ. Network meta-analysis: a norm for comparative effectiveness? Lancet. (2015) 386:628–30. doi: 10.1016/s0140-6736(15)61478-7
12. Amer MA, Smith MD, Herbison GP, Plank LD, McCall JL. Network meta-analysis of the effect of preoperative carbohydrate loading on recovery after elective surgery. Br J Surg. (2016) 104:187–97. doi: 10.1002/bjs.10408
13. Hutton B, Salanti G, Caldwell DM, Chaimani A, Schmid CH, Cameron C, et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann Intern Med. (2015) 162:777–84. doi: 10.7326/m14-2385
14. Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. (2019) 366:l4898. doi: 10.1136/bmj.l4898
15. Abrams KR, Gillies CL, Lambert PC. Meta-analysis of heterogeneously reported trials assessing change from baseline. Stat Med. (2005) 24:3823–44. doi: 10.1002/sim.2423
16. RStudio Team,. RStudio Team RStudio Integrated Development for R. Boston, MA: RStudio Team (2020).
17. van Valkenhoef G. Gemtc: Network Meta-Analysis Using Bayesian Methods: R Package Version 1.0-1. (2021).
19. Chaimani A, Higgins JP, Mavridis D, Spyridonos P, Salanti G. Graphical tools for network meta-analysis in STATA. PLoS One. (2013) 8:e76654. doi: 10.1371/journal.pone.0076654
20. Doi SAR, Barendregt JJ. A generalized pairwise modelling framework for network meta-analysis. Int J Evid Based Healthc. (2018) 16:187–94. doi: 10.1097/xeb.0000000000000140
21. Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al. Cochrane Handbook for Systematic Reviews of Interventions. New York, NY: John Wiley & Sons (2019).
22. van Valkenhoef G, Dias S, Ades AE, Welton NJ. Automated generation of node-splitting models for assessment of inconsistency in network meta-analysis. Res Synth Methods. (2016) 7:80–93. doi: 10.1002/jrsm.1167
23. Ades AE, Sculpher M, Sutton A, Abrams K, Cooper N, Welton N, et al. Bayesian methods for evidence synthesis in cost-effectiveness analysis. Pharmacoeconomics. (2006) 24:1–19. doi: 10.2165/00019053-200624010-00001
24. Salanti G, Ades AE, Ioannidis JP. Graphical methods and numerical summaries for presenting results from multiple-treatment meta-analysis: an overview and tutorial. J Clin Epidemiol. (2011) 64:163–71. doi: 10.1016/j.jclinepi.2010.03.016
25. Nikolakopoulou A, Higgins JPT, Papakonstantinou T, Chaimani A, Del Giovane C, Egger M, et al. CINeMA: an approach for assessing confidence in the results of a network meta-analysis. PLoS Med. (2020) 17:e1003082. doi: 10.1371/journal.pmed.1003082
26. Papakonstantinou T, Nikolakopoulou A, Higgins JP, Egger M, Salanti G. Cinema: software for semiautomated assessment of the confidence in the results of network meta-analysis. Campbell Syst Rev. (2020) 16:e1080.
27. Canbay Ö, Adar S, Karagöz AH, Çelebi N, Bilen CY. Effect of preoperative consumption of high carbohydrate drink (Pre-Op) on postoperative metabolic stress reaction in patients undergoing radical prostatectomy. Int Urol Nephrol. (2014) 46:1329–33. doi: 10.1007/s11255-013-0612-y
28. Chen J, Cheng L, Xie Z, Li Z. The effect of the preoperative oral intake of 10% glucose solution on postoperative insulin resistance in patients undergoing gastric cancer resection. J Perianesth Nurs. (2014) 34:1562–5.
29. Cho EA, Lee NH, Ahn JH, Choi WJ, Byun JH, Song T. Preoperative oral carbohydrate loading in laparoscopic gynecologic surgery: a randomized controlled trial. J Minim Invasive Gynecol. (2021) 28:1086–94.e1. doi: 10.1016/j.jmig.2020.12.002
30. Faria MS, de Aguilar-Nascimento JE, Pimenta OS, Alvarenga LC Jr, Dock-Nascimento DB, Slhessarenko N. Preoperative fasting of 2 hours minimizes insulin resistance and organic response to trauma after video-cholecystectomy: a randomized, controlled, clinical trial. World J Surg. (2009) 33:1158–64. doi: 10.1007/s00268-009-0010-x
31. Feguri GR, Lima PR, Lopes AM, Roledo A, Marchese M, Trevisan M, et al. Clinical and metabolic results of fasting abbreviation with carbohydrates in coronary artery bypass graft surgery. Rev Bras Cir Cardiovasc. (2012) 27:7–17. doi: 10.5935/1678-9741.20120004
32. Gümüs K, Pirhan Y, Aydın G, Keloglan S, Tasova V, Kahveci M. The effect of preoperative oral intake of liquid carbohydrate on postoperative stress parameters in patients undergoing laparoscopic cholecystectomy: an experimental study. J Perianesth Nurs. (2021) 36:526–31. doi: 10.1016/j.jopan.2020.10.012
33. Kweon S-H, Park JS, Lee YC. Oral carbohydrate administration in patients undergoing cephalomedullary nailing for proximal femur fractures: an analysis of clinical outcomes and patient satisfaction. Geriatr Orthop Surg Rehabil. (2020) 11:2151459320958609. doi: 10.1177/2151459320958609
34. Marquini GV, da Silva Pinheiro FE, da Costa Vieira AU, da Costa Pinto RM, Kuster Uyeda MGB, Girão M, et al. Preoperative fasting abbreviation (Enhanced Recovery After Surgery protocol) and effects on the metabolism of patients undergoing gynecological surgeries under spinal anesthesia: a randomized clinical trial. Nutrition. (2020) 77:110790. doi: 10.1016/j.nut.2020.110790
35. Onalan E, Andsoy II, Ersoy OF. The effect of preoperative oral carbohydrate administration on insulin resistance and comfort level in patients undergoing surgery. J Perianesth Nurs. (2019) 34:539–50. doi: 10.1016/j.jopan.2018.07.007
36. Pêdziwiatr M, Pisarska M, Matłok M, Major P, Kisielewski M, Wierdak M, et al. Randomized clinical trial to compare the effects of preoperative oral carbohydrate loading versus placebo on insulin resistance and cortisol level after laparoscopic cholecystectomy. Pol Przegl Chir. (2015) 87:402–8. doi: 10.1515/pjs-2015-0079
37. Perrone F, da-Silva-Filho AC, Adôrno IF, Anabuki NT, Leal FS, Colombo T, et al. Effects of preoperative feeding with a whey protein plus carbohydrate drink on the acute phase response and insulin resistance. A randomized trial. Nutr J. (2011) 10:66. doi: 10.1186/1475-2891-10-66
38. Pexe-Machado PA, de Oliveira BD, Dock-Nascimento DB, de Aguilar-Nascimento JE. Shrinking preoperative fast time with maltodextrin and protein hydrolysate in gastrointestinal resections due to cancer. Nutrition. (2013) 29:1054–9. doi: 10.1016/j.nut.2013.02.003
39. Rapp-Kesek D, Stridsberg M, Andersson LG, Berne C, Karlsson T. Insulin resistance after cardiopulmonary bypass in the elderly patient. Scand Cardiovasc J. (2007) 41:102–8. doi: 10.1080/14017430601050355
40. de Andrade Gagheggi Ravanini G, Portari Filho PE, Abrantes Luna R, Almeida de Oliveira V. Organic inflammatory response to reduced preoperative fasting time, with a carbohydrate and protein enriched solution; A randomized trial. Nutr Hosp. (2015) 32:953–7. doi: 10.3305/nh.2015.32.2.8944
41. Rizvanović N, Nesek Adam V, Čaušević S, Dervišević S, Delibegović S. A randomised controlled study of preoperative oral carbohydrate loading versus fasting in patients undergoing colorectal surgery. Int J Colorectal Dis. (2019) 34:1551–61. doi: 10.1007/s00384-019-03349-4
42. Yu Y, Zhou YB, Liu HC, Cao SG, Zahng J, Wang ZH. Effects of preoperative oral carbohydrate on postoperative insulin resistance in radical gastrectomy patients. Zhonghua Wai Ke Za Zhi. (2013) 51:696–700.
43. Shi Y, Dong B, Dong Q, Zhao Z, Yu Y. Effect of preoperative oral carbohydrate administration on patients undergoing cesarean section with epidural anesthesia: a pilot study. J Perianesth Nurs. (2021) 36:30–5. doi: 10.1016/j.jopan.2020.05.006
44. Zhang Y, Min J. Preoperative carbohydrate loading in gynecological patients undergoing combined spinal and epidural anesthesia. J Invest Surg. (2020) 33:587–95. doi: 10.1080/08941939.2018.1546352
45. Zhou H. Effect of Oral Glucose Solution Two Hours before Operation on Patients with Gastric Cance. Jiangsu: Yangzhou University (2018).
46. Singh BN, Dahiya D, Bagaria D, Saini V, Kaman L, Kaje V, et al. Effects of preoperative carbohydrates drinks on immediate postoperative outcome after day care laparoscopic cholecystectomy. Surg Endosc. (2015) 29:3267–72. doi: 10.1007/s00464-015-4071-7
47. Tran S, Wolever TM, Errett LE, Ahn H, Mazer CD, Keith M. Preoperative carbohydrate loading in patients undergoing coronary artery bypass or spinal surgery. Anesth Analg. (2013) 117:305–13. doi: 10.1213/ANE.0b013e318295e8d1
48. He Y, Liu C, Han Y, Huang Y, Zhou J, Xie Q. The impact of oral carbohydrate-rich supplement taken two hours before caesarean delivery on maternal and neonatal perioperative outcomes – a randomized clinical trial. BMC Pregnancy Childbirth. (2021) 21:682. doi: 10.1186/s12884-021-04155-z
49. Qin H, Ji J, Miao Y, Liu T, Zhao D, Jia Z, et al. Efficacy of the oral administration of maltodextrin fructose before major abdominal surgery: a prospective, multicenter clinical study. World J Surg. (2022) 46:2132–40. doi: 10.1007/s00268-022-06455-7
50. Wu HY, Yang XD, Yang GY, Cai ZG, Shan XF, Yang Y. Preoperative oral carbohydrates in elderly patients undergoing free flap surgery for oral cancer: randomized controlled trial. Int J Oral Maxillofac Surg. (2022) 51:1010–5. doi: 10.1016/j.ijom.2022.02.014
51. Castela I, Rodrigues C, Ismael S, Barreiros-Mota I, Morais J, Araújo JR, et al. Intermittent energy restriction ameliorates adipose tissue-associated inflammation in adults with obesity: a randomised controlled trial. Clin Nutr. (2022) 41:1660–6. doi: 10.1016/j.clnu.2022.06.021
52. Ajuzieogu OV, Amucheazi AO, Nwagha UI, Ezike HA, Luka SK, Abam DS. Effect of routine preoperative fasting on residual gastric volume and acid in patients undergoing myomectomy. Niger J Clin Pract. (2016) 19:816–20. doi: 10.4103/1119-3077.180049
53. Braga M, Bissolati M, Rocchetti S, Beneduce A, Pecorelli N, Di Carlo V. Oral preoperative antioxidants in pancreatic surgery: a double-blind, randomized, clinical trial. Nutrition. (2012) 28:160–4. doi: 10.1016/j.nut.2011.05.014
54. Gianotti L, Biffi R, Sandini M, Marrelli D, Vignali A, Caccialanza R, et al. Preoperative oral carbohydrate load versus placebo in major elective abdominal surgery (PROCY): a randomized, placebo-controlled, multicenter, phase III trial. Ann Surg. (2018) 267:623–30. doi: 10.1097/sla.0000000000002325
55. Itou K, Fukuyama T, Sasabuchi Y, Yasuda H, Suzuki N, Hinenoya H, et al. Safety and efficacy of oral rehydration therapy until 2 h before surgery: a multicenter randomized controlled trial. J Anesth. (2012) 26:20–7. doi: 10.1007/s00540-011-1261-x
56. Borges Dock-Nascimento D, Aguilar-Nascimento JE, Caporossi C, Sepulveda Magalhães Faria M, Bragagnolo R, Caporossi FS, et al. Safety of oral glutamine in the abbreviation of preoperative fasting: a double-blind, controlled, randomized clinical trial. Nutr Hosp. (2011) 26:86–90.
57. Doo AR, Hwang H, Ki M-J, Lee J-R, Kim D-C. Effects of preoperative oral carbohydrate administration on patient well-being and satisfaction in thyroid surgery. Korean J Anesthesiol. (2018) 71:394–400. doi: 10.4097/kja.d.18.27143
58. Kaska M, Grosmanová T, Havel E, Hyspler R, Petrová Z, Brtko M, et al. The impact and safety of preoperative oral or intravenous carbohydrate administration versus fasting in colorectal surgery–a randomized controlled trial. Wien Klin Wochenschr. (2010) 122:23–30. doi: 10.1007/s00508-009-1291-7
59. Liu B, Wang Y, Liu S, Zhao T, Zhao B, Jiang X, et al. A randomized controlled study of preoperative oral carbohydrate loading versus fasting in patients undergoing elective craniotomy. Clin Nutr. (2019) 38:2106–12. doi: 10.1016/j.clnu.2018.11.008
60. Nygren J, Soop M, Thorell A, Sree Nair K, Ljungqvist O. Preoperative oral carbohydrates and postoperative insulin resistance. Clin Nutr. (1999) 18:117–20. doi: 10.1054/clnu.1998.0019
61. Yuill KA, Richardson RA, Davidson HI, Garden OJ, Parks RW. The administration of an oral carbohydrate-containing fluid prior to major elective upper-gastrointestinal surgery preserves skeletal muscle mass postoperatively–a randomised clinical trial. Clin Nutr. (2005) 24:32–7. doi: 10.1016/j.clnu.2004.06.009
62. Mousavie SH, Negahi A, Hosseinpour P, Mohseni M, Movassaghi S. The effect of preoperative oral versus parenteral dextrose supplementation on pain, nausea, and quality of recovery after laparoscopic cholecystectomy. J Perianesth Nurs. (2021) 36:153–6. doi: 10.1016/j.jopan.2020.07.002
63. Ljunggren S, Hahn RG. Oral nutrition or water loading before hip replacement surgery; a randomized clinical trial. Trials. (2012) 13:97. doi: 10.1186/1745-6215-13-97
64. Ljunggren S, Hahn RG, Nyström T. Insulin sensitivity and beta-cell function after carbohydrate oral loading in hip replacement surgery: a double-blind, randomised controlled clinical trial. Clin Nutr. (2014) 33:392–8. doi: 10.1016/j.clnu.2013.08.003
65. Hosny H, Ibrahim M, El-Siory W, Abdel-Monem A. Comparative study between conventional fasting versus overnight infusion of lipid or carbohydrate on insulin and free fatty acids in obese patients undergoing elective on-pump coronary artery bypass grafting. A prospective randomized trial. J Cardiothorac Vasc Anesth. (2018) 32:1248–53. doi: 10.1053/j.jvca.2017.11.020
66. Yi HC, Ibrahim Z, Abu Zaid Z, Mat Daud Z, Md Yusop NB, Omar J, et al. Impact of enhanced recovery after surgery with preoperative whey protein-infused carbohydrate loading and postoperative early oral feeding among surgical gynecologic cancer patients: an open-labelled randomized controlled trial. Nutrients. (2020) 12:264. doi: 10.3390/nu12010264
67. Bisgaard T, Kristiansen VB, Hjortsø NC, Jacobsen LS, Rosenberg J, Kehlet H. Randomized clinical trial comparing an oral carbohydrate beverage with placebo before laparoscopic cholecystectomy. Br J Surg. (2004) 91:151–8. doi: 10.1002/bjs.4412
68. Helminen H, Branders H, Ohtonen P, Saarnio J. Effect of pre-operative oral carbohydrate loading on recovery after day-case cholecystectomy: a randomised controlled trial. Eur J Anaesthesiol. (2019) 36:605–11. doi: 10.1097/eja.0000000000001002
69. Lauwick SM, Kaba A, Maweja S, Hamoir EE, Joris JL. Effects of oral preoperative carbohydrate on early postoperative outcome after thyroidectomy. Acta Anaesthesiol Belg. (2009) 60:67–73.
70. Chaudhary NK, Sunuwar DR, Sharma R, Karki M, Timilsena MN, Gurung A, et al. The effect of pre-operative carbohydrate loading in femur fracture: a randomized controlled trial. BMC Musculoskelet Disord. (2022) 23:819. doi: 10.1186/s12891-022-05766-z
71. Sada F, Krasniqi A, Hamza A, Gecaj-Gashi A, Bicaj B, Kavaja F. A randomized trial of preoperative oral carbohydrates in abdominal surgery. BMC Anesthesiol. (2014) 14:93. doi: 10.1186/1471-2253-14-93
72. Harsten A, Hjartarson H, Toksvig-Larsen S. Total hip arthroplasty and perioperative oral carbohydrate treatment: a randomised, double-blind, controlled trial. Eur J Anaesthesiol. (2012) 29:271–4. doi: 10.1097/EJA.0b013e3283525ba9
73. Liu X, Zhang P, Liu MX, Ma JL, Wei XC, Fan D. Preoperative carbohydrate loading and intraoperative goal-directed fluid therapy for elderly patients undergoing open gastrointestinal surgery: a prospective randomized controlled trial. BMC Anesthesiol. (2021) 21:157. doi: 10.1186/s12871-021-01377-8
74. Breuer JP, von Dossow V, von Heymann C, Griesbach M, von Schickfus M, Mackh E, et al. Preoperative oral carbohydrate administration to ASA III-IV patients undergoing elective cardiac surgery. Anesth Analg. (2006) 103:1099–108. doi: 10.1213/01.ane.0000237415.18715.1d
75. Feguri GR, Lima PRL, Franco AC, Cruz FRH, Borges DC, Toledo LR, et al. Benefits of fasting abbreviation with carbohydrates and omega-3 infusion during CABG: a double-blind controlled randomized trial. Braz J Cardiovasc Surg. (2019) 34:125–35. doi: 10.21470/1678-9741-2018-0336
76. Ljunggren S, Nyström T, Hahn RG. Accuracy and precision of commonly used methods for quantifying surgery-induced insulin resistance: prospective observational study. Eur J Anaesthesiol. (2014) 31:110–6. doi: 10.1097/eja.0000000000000017
77. Marsman M, Schönbrodt FD, Morey RD, Yao Y, Gelman A, Wagenmakers EJA. Bayesian bird’s eye view of ‘Replications of important results in social psychology’. R Soc Open Sci. (2017) 4:160426. doi: 10.1098/rsos.160426
78. Zhang Z, Xu X, Ni H. Small studies may overestimate the effect sizes in critical care meta-analyses: a meta-epidemiological study. Crit Care. (2013) 17:R2. doi: 10.1186/cc11919
79. Järvelä K, Maaranen P, Sisto T. Pre-operative oral carbohydrate treatment before coronary artery bypass surgery. Acta Anaesthesiol Scand. (2008) 52:793–7. doi: 10.1111/j.1399-6576.2008.01660.x
80. Lee B, Soh S, Shim JK, Kim HY, Lee H, Kwak YL. Evaluation of preoperative oral carbohydrate administration on insulin resistance in off-pump coronary artery bypass patients: a randomised trial. Eur J Anaesthesiol. (2017) 34:740–7. doi: 10.1097/eja.0000000000000637
81. Ljungqvist O, Thorell A, Gutniak M, Häggmark T, Efendic S. Glucose infusion instead of preoperative fasting reduces postoperative insulin resistance. J Am Coll Surg. (1994) 178:329–36.
82. Awad S, Constantin-Teodosiu D, Constantin D, Rowlands BJ, Fearon KC, Macdonald IA, et al. Cellular mechanisms underlying the protective effects of preoperative feeding: a randomized study investigating muscle and liver glycogen content, mitochondrial function, gene and protein expression. Ann Surg. (2010) 252:247–53. doi: 10.1097/SLA.0b013e3181e8fbe6
83. Soop M, Nygren J, Thorell A, Weidenhielm L, Lundberg M, Hammarqvist F, et al. Preoperative oral carbohydrate treatment attenuates endogenous glucose release 3 days after surgery. Clin Nutr. (2004) 23:733–41. doi: 10.1016/j.clnu.2003.12.007
84. van Stijn MFM, Soeters MR, van Leeuwen PAM, Schreurs WH, Schoorl MG, Twisk JWR, et al. Effects of a carbohydrate-, glutamine-, and antioxidant-enriched oral nutrition supplement on major surgery-induced insulin resistance: a randomized pilot study. JPEN J Parenter Enteral Nutr. (2018) 42:719–29. doi: 10.1177/0148607117711691
85. Suh S, Hetzel E, Alter-Troilo K, Lak K, Gould JC, Kindel TL, et al. The influence of preoperative carbohydrate loading on postoperative outcomes in bariatric surgery patients: a randomized, controlled trial. Surg Obes Relat Dis. (2021) 17:1480–8. doi: 10.1016/j.soard.2021.04.014
86. Tewari N, Awad S, Duška F, Williams JP, Bennett A, Macdonald IA, et al. Postoperative inflammation and insulin resistance in relation to body composition, adiposity and carbohydrate treatment: a randomised controlled study. Clin Nutr. (2019) 38:204–12. doi: 10.1016/j.clnu.2018.01.032
Keywords: preoperative carbohydrate loading, insulin resistance, postoperative comfort and safety, elective surgery, adults, Bayesian network meta-analysis
Citation: Tong E, Chen Y, Ren Y, Zhou Y, Di C, Zhou Y, Shao S, Qiu S, Hong Y, Yang L and Tan X (2022) Effects of preoperative carbohydrate loading on recovery after elective surgery: A systematic review and Bayesian network meta-analysis of randomized controlled trials. Front. Nutr. 9:951676. doi: 10.3389/fnut.2022.951676
Received: 24 May 2022; Accepted: 31 October 2022;
Published: 23 November 2022.
Edited by:
Maurizio Muscaritoli, Department of Translational and Precision Medicine, Faculty of Medicine and Dentistry, Sapienza University of Rome, ItalyReviewed by:
Robert Hahn, Karolinska Institutet (KI), SwedenAnthony Senagore, AJS Innovative Solutions, LLC, United States
Copyright © 2022 Tong, Chen, Ren, Zhou, Di, Zhou, Shao, Qiu, Hong, Yang and Tan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xiaohua Tan, eGlhb2h1YXRhbkBoem51LmVkdS5jbg==
†These authors have contributed equally to this work