 Dorsa Ghazvineh
Dorsa Ghazvineh Mojtaba Daneshvar2
Mojtaba Daneshvar2 Elnaz Daneshzad
Elnaz Daneshzad
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Nutr. , 14 July 2022
Sec. Sport and Exercise Nutrition
Volume 9 - 2022 | https://doi.org/10.3389/fnut.2022.942702
Objectives: Yoga is a mind-body stress-relieving exercise that increases mental and physical health, which may have a role in the improvement of metabolic disorders. The present study has reviewed the effect of yoga on lipid profiles as a systematic review and meta-analysis.
Methods: We evaluated the available randomized controlled trials on the effects of yoga-based programs, and lipid profiles by searching PubMed/Medline, Scopus, Web of Science, and the Cochrane central register of control trials up to January 2022. Both fixed and random effect analyses were used to find the relationships. Subgroup analysis was performed based on the continent, duration of the included studies, gender, and health condition of participants to discover the sources of heterogeneity.
Result: Fifty-three studies were included in the current systematic review and meta-analysis with a total sample size of 13,191. There was a striking association between yoga and total cholesterol (−10.31 mg/dl; 95% CI: −14.16, −6.45; I2 = 82.5%, P < 0.001), low-density lipoprotein cholesterol (−8.64 mg/dl; 95% CI: −12.03, −5.25; I2 = 75.0%, P < 0.001), high-density lipoprotein cholesterol (1.98 mg/dl; 95% CI: 0.81, 3.14; I2 = 91.6%, P < 0.001), triglycerides (−13.50 mg/dl; 95% CI: −20.09, −6.92; I2 = 90.7%, P < 0.001) and very low-density lipoprotein (−3.94 mg/dl; 95%CI: −6.31, −1.56; I2 = 72.2%, P < 0.001).
Conclusion: It seems yoga interventions had a substantial effect on lipid profiles, however, more qualified trials or cohort studies are needed to conclude exactly.
Modernization has brought increased comforts and limited mobility in our lives at the cost of an increased prevalence of hypertension, diabetes mellitus, dyslipidemia, and obesity, which are predecessors of major cardiovascular diseases (CVD) (1). Evidence suggests most of these diseases were rare before the present century and their prevalence has increased over the past 50 years (1). Also, metabolic syndrome (MetS) has been described as a pandemic, with a rapidly increasing prevalence worldwide (2). While dyslipidemia is a contributing risk factor for various macrovascular complications, MetS and CVD, which is characterized by high levels of triglyceride (TG ≥ 150 mg/dl), high low-density lipoprotein (LDL-C ≥ 130 mg/dl), low high-density lipoprotein (HDL-C < 40 mg/dl for men; < 50 mg/dl for women), and high levels of total cholesterol (TC ≥ 200 mg/dl) (3). Both prevention and control of coronary heart disease and its associated diseases are essential and can be achieved by modifying the lipid profile (4). Given the increasing prevalence and the associated premature mortality, disability, and health and social-economic costs of chronic diseases which are related to serum lipid levels, its management is of importance to public health (5). Not only healthy dietary patterns and a healthy lifestyle are effective on serum lipid levels but also physical activity and management of mental stress play an integral role in this area.
One of the best exercises that could help with physical and mental health is yoga. It was born in India thousands of years ago and has gradually expanded throughout the world. Yoga is a range of effective alternatives to traditional aerobic and strength training programs, which require little space, no equipment, and have limited side effects. Components of yoga that are commonly applied for health benefits are asanas (physical postures), pranayama (regulated breathing), meditation, relaxation, and various physical postures. Yoga calms and relaxes the mind, strengthens, and tunes the body, and brings them into harmony with one another (1). Deep relaxation, a unique part of a yoga program, relaxes the sympathetic nervous system and helps with physiological stress reduction. Physiological stress itself is related to metabolic disease (6). It seems yoga by improving physiological stress, will help cure cardiometabolic risk factors such as blood pressure, lipid, and glucose levels, as well as body weight (6). Even more, a study reported a better lipid profile in long and medium-term meditators when compared to non-meditators (7). Despite these claims, there is some evidence that shows that high-intensity yoga has no significant effects on cardiovascular outcomes or any of the blood parameters (8). Therefore, this review aims to systematically assess the effects of yoga on blood lipid levels, including through randomized clinical trials (RCTs).
This study was conducted and reported according to PRISMA guidelines (preferred reporting items for systematic reviews and meta-analyses) (9).
A comprehensive literature search was conducted using PubMed, Scopus, Web of Science, Google Scholar, and Cochrane databases. The query was based on a combination of text words and terms from the Medical Subject Headings (MeSH): [Yoga(tiab) OR Yoga(MeSH) OR yogic OR yog* OR “yogasana” OR “surya namaskar” OR “vinyasa” OR “Thai yoga” OR “asana” OR “hatha” OR “pranayama” OR Pranayam* OR “dhyana” OR “Laughter therapy”(tiab) OR “Laughter therapy”(MeSH) OR “mind-body” OR “mind-body therapies”(tiab) OR “Mind-Body Therapies”(MeSH) OR “Mindfulness-based interventions” OR “Mindful exercise” OR “Exercise therapy”(tiab) OR “Traditional Chinese exercise” OR “Mindfulness interventions”(tiab) OR “complementary therapies”(tiab) OR meditation OR mindfulness OR “mindfulness-based stress reduction”] AND [“lipid profile” OR “serum lipids” OR “blood lipids” OR lipoproteins OR lipoprotein OR lipids OR Hypercholesterolemia(MeSH) OR Hyperlipidemias(MeSH) OR Hypercholesterolemia OR Hyperlipidemias OR “serum lipid markers” OR hypertriglyceridemia OR dyslipid* OR HDL OR HDL-C OR “Lipoproteins, HDL”(MeSH) OR “Cholesterol, HDL”(MeSH) OR “HDL Cholesterol” OR “high density lipoprotein” OR “high-density LDL-C OR “Lipoproteins, LDL”(MeSH) OR “Cholesterol, LDL”(MeSH) OR “LDL Cholesterol” OR “Low density lipoprotein” OR “low-density lipoprotein” OR “LDL-cholesterol” OR “Low Density Lipoprotein Cholesterol” OR TAG OR TG OR Triglyceride OR Triglycerides(MeSH) OR triacylglycer* OR TC OR Cholesterol OR “total cholesterol” OR Cholesterol(MeSH)].
All articles published before January 2022 were searched and examined by two authors to determine whether they were eligible for the present systematic review and meta-analysis. First, the titles and abstracts of the studies were reviewed to find articles related to our research question. If it was not certain whether or not the study met the inclusion criteria, the full text was reviewed to clarify this issue. Bibliographies of eligible studies and relevant reviews were also checked to reduce the possibility that a publication had been overlooked. All of the above steps were performed independently by two authors. Any discrepancies, from study selection to data extraction, were resolved in consultation with the lead author.
RCTs that investigated the effect of yoga on lipid profiles were included in this review. Eligibility criteria for inclusion in this study were defined as follows: if the study design was RCT (parallel/crossover), conducted in adult subjects (> 18 years), reporting mean and standard deviation (SD) outcomes at baseline and the end of the study or mean changes between the intervention and control groups. Only articles published in English were included in the present study. In addition, the following exclusion criteria were defined, namely, observational studies, non-interventional studies, studies without a placebo group, studies in children, lactating or pregnant women, animal studies, gray literature (books, letters, commentaries, and conferences), as well as dissertations and reviews were excluded.
Two reviewers (DG and MD) independently scanned the articles for titles and abstracts. Any discrepancies between these two authors were clarified by a third researcher (ED) as the principal investigator. In this study, the effect of yoga was considered as an intervention. Moreover, the mean and SD of HDL-C, LDL-C, very-low-density lipoprotein (VLDL), TG, and TC were the outcomes. Data were extracted from each included study, including the first author of the study, date of publication, type of study, population, number of participants in intervention and control groups, gender of participants, age of participants at baseline, study location, duration of intervention, and body mass index (BMI) as well as mean and SDs of lipid criteria before and after the intervention.
Based on the Cochrane guideline (10), we evaluated the quality of the studies by the following criteria: random sequence generation, allocation concealment, blinding, incomplete outcome data, selective outcome reporting, and other possible sources of bias. According to this guideline, studies were categorized as low risk or high risk of bias or unclear regarding each domain (Supplementary Table 1).
The means and corresponding SDs of all variables of all included studies in both intervention and control groups were used to calculate the weighted mean difference (WMD) as effect size in the meta-analysis. For studies that did not report mean changes, we computed this variable using mining pre-and post-intervention data. Also, the SD of the mean difference was calculated by the following formula: SD = [(SDbaseline2 + SDfinal2) – (2 × R × SDbaseline2 × SDfinal2)], (R-value = 0.5) (11). In cases where SD was not reported, we calculated SD using SE and sample size (SD = SE × √sample size). The reported rate of lipid profile in all studies was converted into the usual unit (mg/dl). The analysis was performed using the fixed-effect model. Also, the random effect model was used for variables with high heterogeneity. Subgroup analyses by continent, duration, gender, and condition were performed using Cochran’s Q test and the I2 statistic to assess the possible sources of heterogeneity. In addition, publication bias was assessed using funnel plots and Egger’s regression test. A sensitivity analysis was performed to determine the extent to which summary estimates might be related to a particular study or group of studies and also meta-regression test was used to determine the effect of age confounded. Data analyses were performed using Stata Software, version 14. P-values were reported as statistically significant at the < 0.05 level.
After screening the titles and abstracts of 6,238 articles, about 233 studies were adopted to be assessed for full-text. After excluding unrelated and review studies, 53 studies were kept and included in this systematic review (Figure 1). All studies employed a parallel design. Characteristics of the included studies, which were published from 1991 to 2021 are illustrated in Table 1. The sample size of these studies varied from 8 to 8,116 (3) and overall 13,191 participants, divided into 6,700 individuals in the control group and 6,517 in the intervention group. The age range was between 18 and 70 years old. Of the 53 included studies, 36 were conducted in India (3, 7, 12–44), but two effect sizes were extracted from Rani et al. (13), four effect sizes from Murthy et al. (25), and two effect sizes from P. A et al. (27), as well as six in the United States (6, 45–49), and three in China (2, 5, 50). Seven studies were conducted on women (2, 19, 37, 49, 51–53), six on men (6, 16, 18, 22, 31, 34), and the remaining studies were conducted on both genders (3, 5, 7, 12–15, 17–21, 23, 25–30, 32, 33, 35, 37–48, 50, 54–59). Included 37 studies had assessed BMI (2, 5–7, 12, 13, 15–19, 21, 22, 24, 27–31, 33, 34, 36–38, 40–43, 46–49, 52, 53, 56–58), 48 studies had measured TC (2, 3, 6, 7, 12–43, 45–47, 49, 52–59),4 6 studies had determined LDL-C (2, 3, 6, 7, 12–42, 45–47, 49, 52–58), 51 studies had measured HDL-C (2, 3, 5–7, 12–21, 23–54, 56, 58, 59), 53 studies had determined TG (2, 3, 5–7, 12–59), and 19 studies had assessed VLDL-C (14, 16, 18, 19, 24, 26, 28, 29, 31, 32, 34–40, 42, 55). These outcomes were reported as mean ± SD, also a meta-analysis as reported below was conducted. RCTs were performed on 11 studies with healthy situations (2, 21, 34, 39, 41, 45, 47, 49, 52, 56, 58), and 19 studies with type 2 diabetes mellitus (3, 6, 7, 12, 13, 16–20, 22–24, 27, 33, 35, 37, 38, 55), 10 studies with MetS (5, 26, 36, 42–44, 46, 48, 50, 51), 5 studies with heart diseases (MI, CAD, CVD) (29–31, 33, 54), 4 studies with hypertension (14, 25, 53, 57), 3 studies with chronic kidney disease (CKD) (15, 28, 59), 1 study with human immunodeficiency virus (HIV) (54) and 1 with obesity (40).
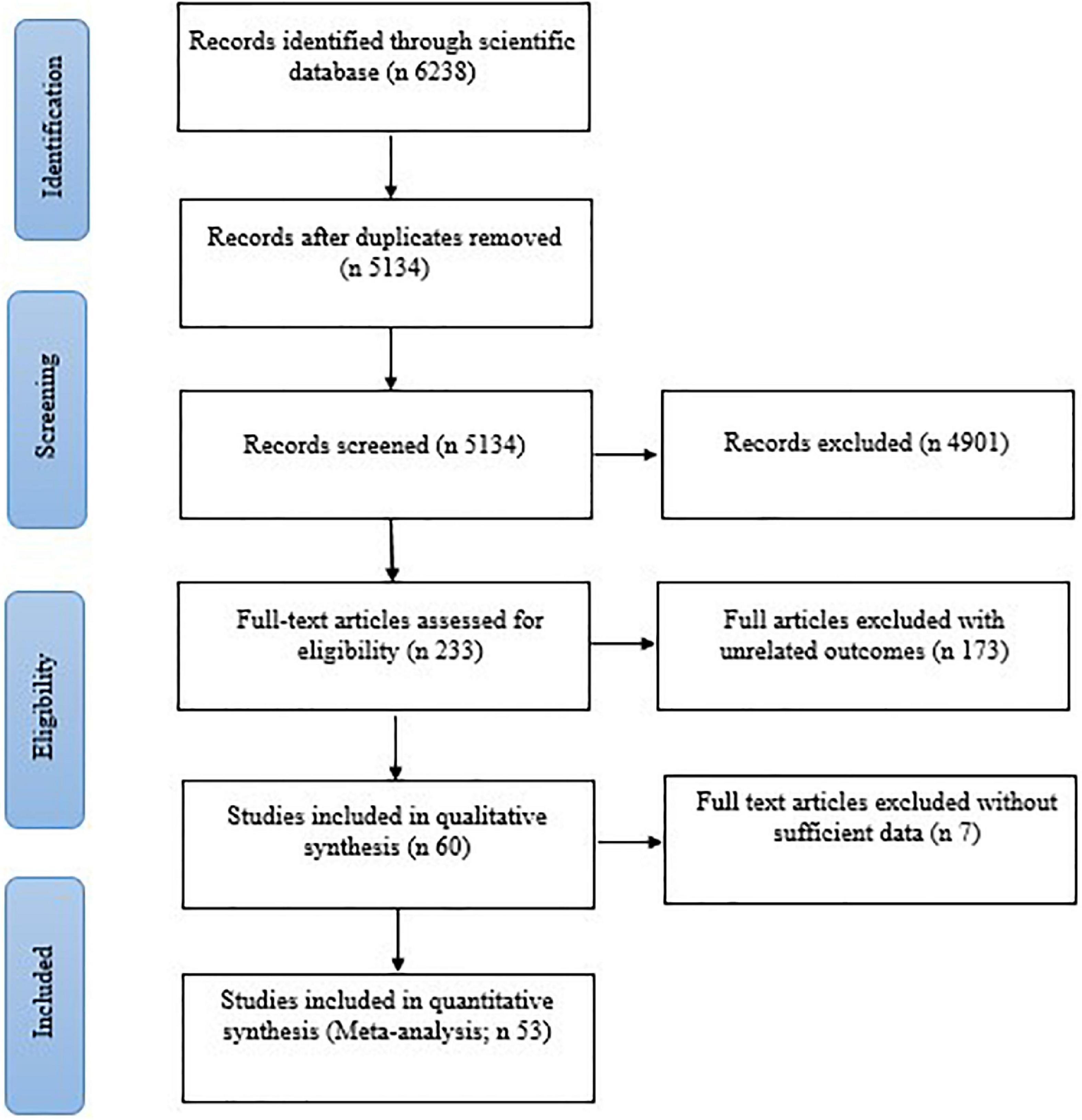
Figure 1. Flow diagram showing the selection of RCT studies for the current systematic review and meta-analysis of the effect of yoga exercise on lipid profile.

Table 1. Characteristics of included studies in the current systematic review and meta-analysis on lipid.
Findings from 55 effect sizes have shown an inverse effect of yoga on TC with high heterogeneity by pooling amounts (−10.31 mg/dl; 95% CI: −14.16, −6.45; P < 0.001; I2 = 82.5%, Pheterogeneity < 0.001) (Figure 2).
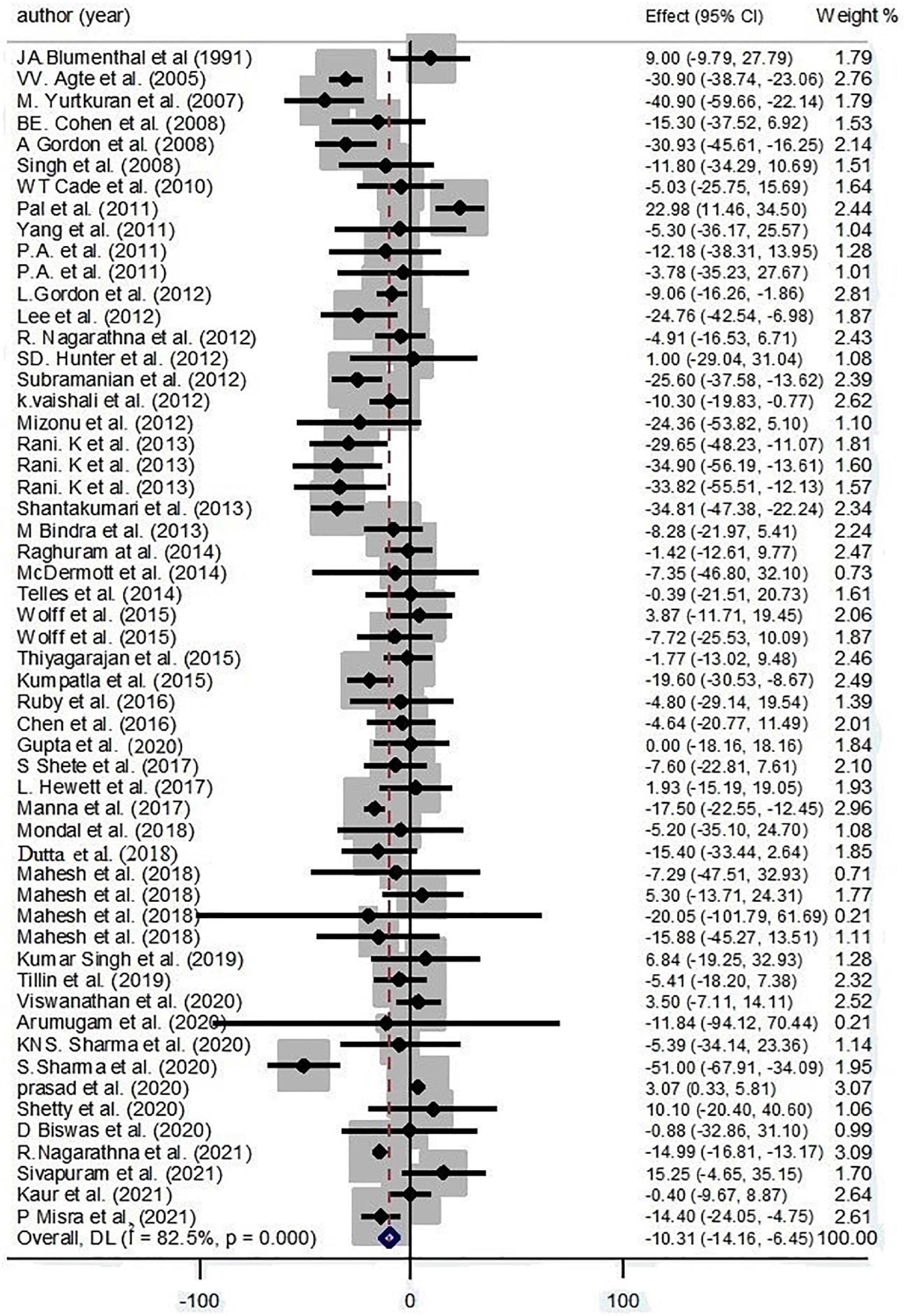
Figure 2. Forest plot for the association between yoga exercise and total cholesterol (Random-effect model).
Because of high heterogeneity, groups were subdivided according to different factors. Based on subgroup analysis, continent, condition, and gender were considered as the main sources of heterogeneity for TC. Results revealed that yoga significantly decreased TC levels among American (−13.6 mg/dl; 95% CI: −21.39, −4.77; P = 0.002; I2 = 54.3%; Pheterogeneity = 0.41) and Asian (−10.51 mg/dl; 95% CI: −11.74, −9.28; P < 0.001; I2 = 85.5%; Pheterogeneity < 0.001) yoga workers. In addition, yoga had a negative effect on TC levels in healthy practitioners (−11.61 mg/dl; 95% CI: −16.13, −9.09; P < 0.001; I2 = 60.1%; Pheterogeneity = 0.005) and patients with MetS (−14.68 mg/dl; 95% CI: −19.94, −9.41; P < 0.001; I2 = 87.9%; Pheterogeneity < 0.001) and CKD (−13.43 mg/dl; 95% CI: −19.73, −7.13; P < 0.001; I2 = 79.4%; Pheterogeneity = 0.008) (Supplementary Table 2).
Based on the result of meta-regression, no effect was found for age on the effect size (regression coefficient = −0.05; 95%CI: −0.65, 0.53; P = 0.839) (Supplementary Figure 1).
According to the result of Egger’s test and funnel plot of 55 studies, no evidence of publication bias was found (P = 0.918) (Supplementary Figure 2). Moreover, the sensitivity analysis of included trials did not affect the final pooled amounts.
An inverse effect of yoga on LDL-C has been detected by collecting 53 effect sizes (−8.64 mg/dl; 95% CI: −12.03, −5.25; P < 0.001; I2 = 75.0%, Pheterogeneity < 0.001) (Figure 3).
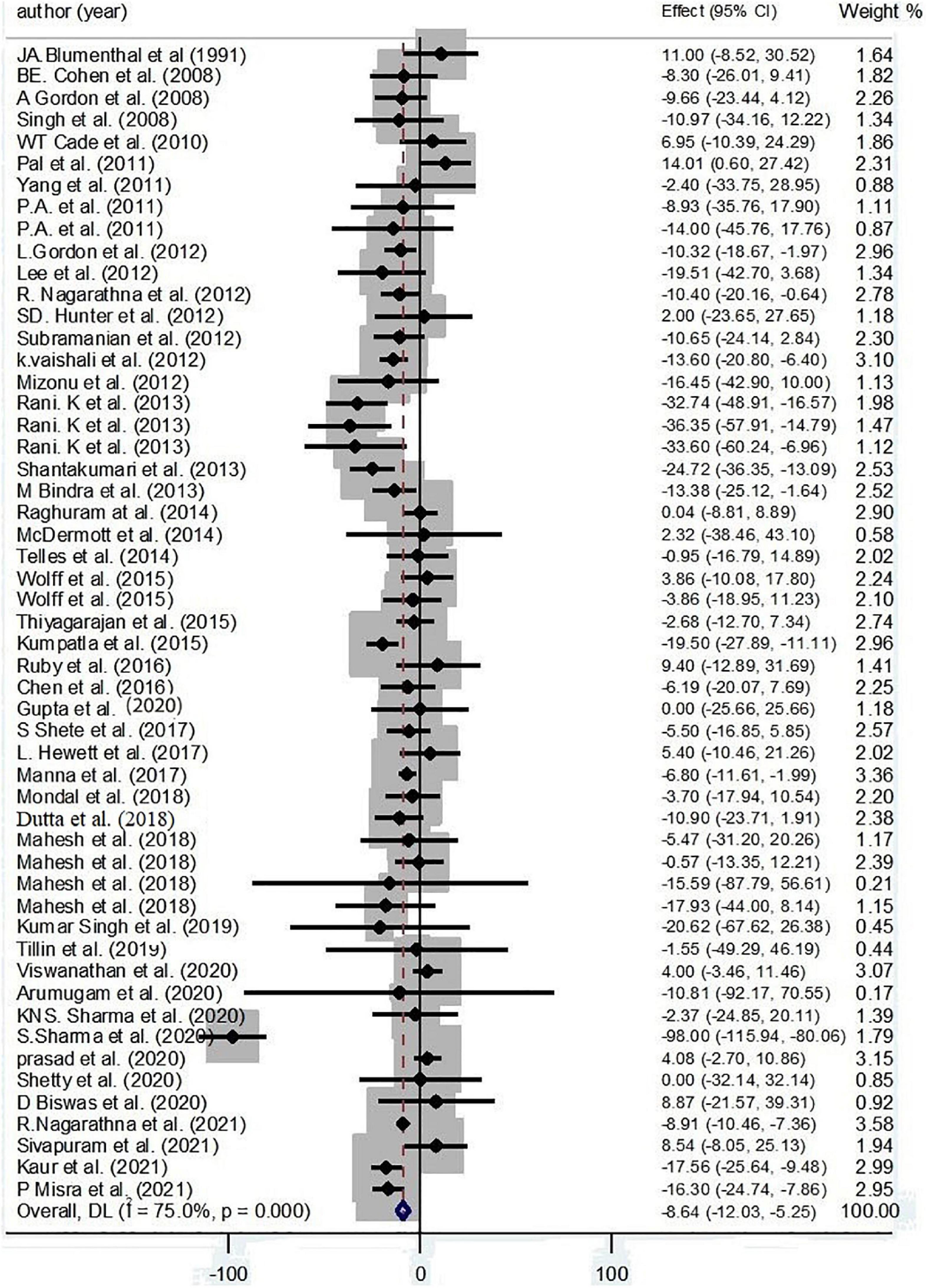
Figure 3. Forest plot for the association between yoga exercise and LDL-C (Random-effect model).
Based on subgroup analysis, continent, condition, duration, and gender were considered as the main sources of heterogeneity. The subgroup analysis based on continent has cleared an inverse effect of yoga on LDL-C among Asian participants (−8.92 mg/dl; 95% CI: −10.11, −7.72; P < 0.001; I2 = 79.1%, Pheterogeneity < 0.001). Moreover, pooling effect sizes have revealed that more than 12 weeks of yoga interventions decreased LDL-C levels (−8.57 mg/dl; 95% CI: −9.75, −7.38; P < 0.001; I2 = 78.2%, Pheterogeneity < 0.001). Also, an inverse effect of yoga on LDL-C levels was found among healthy practitioners (−4.98 mg/dl; 95% CI: −8.43, −1.53; P = 0.005; I2 = 60.1%, Pheterogeneity = 0.005) and patients with CKD (−10.49 mg/dl; 95% CI: −17.49, −3.50; P = 0.003; I2 = 0.0%, Pheterogeneity = 0.941) and type 2 diabetes (−10.76 mg/dl; 95% CI: −12.14, −9.38; P < 0.001; I2 = 84.4%, Pheterogeneity < 0.001) (Supplementary Table 3).
Based on the result of meta-regression, no effect was found for age on the effect sizes (regression coefficient = −0.15; 95%CI: −0.63, 0.31; P = 0.508) (Supplementary Figure 3).
According to the result of Egger’s test and funnel plot of 53 studies, no evidence of publication bias was found (P = 0.981) (Supplementary Figure 4). Moreover, the sensitivity analysis of included trials did not affect the final pooled amounts.
A positive effect of yoga on HDL-C has illustrated by collecting 58 effect sizes (1.98 mg/dl; 95% CI: 0.81, 3.14; P < 0.001; I2 = 91.6%, Pheterogeneity < 0.001) (Figure 4).
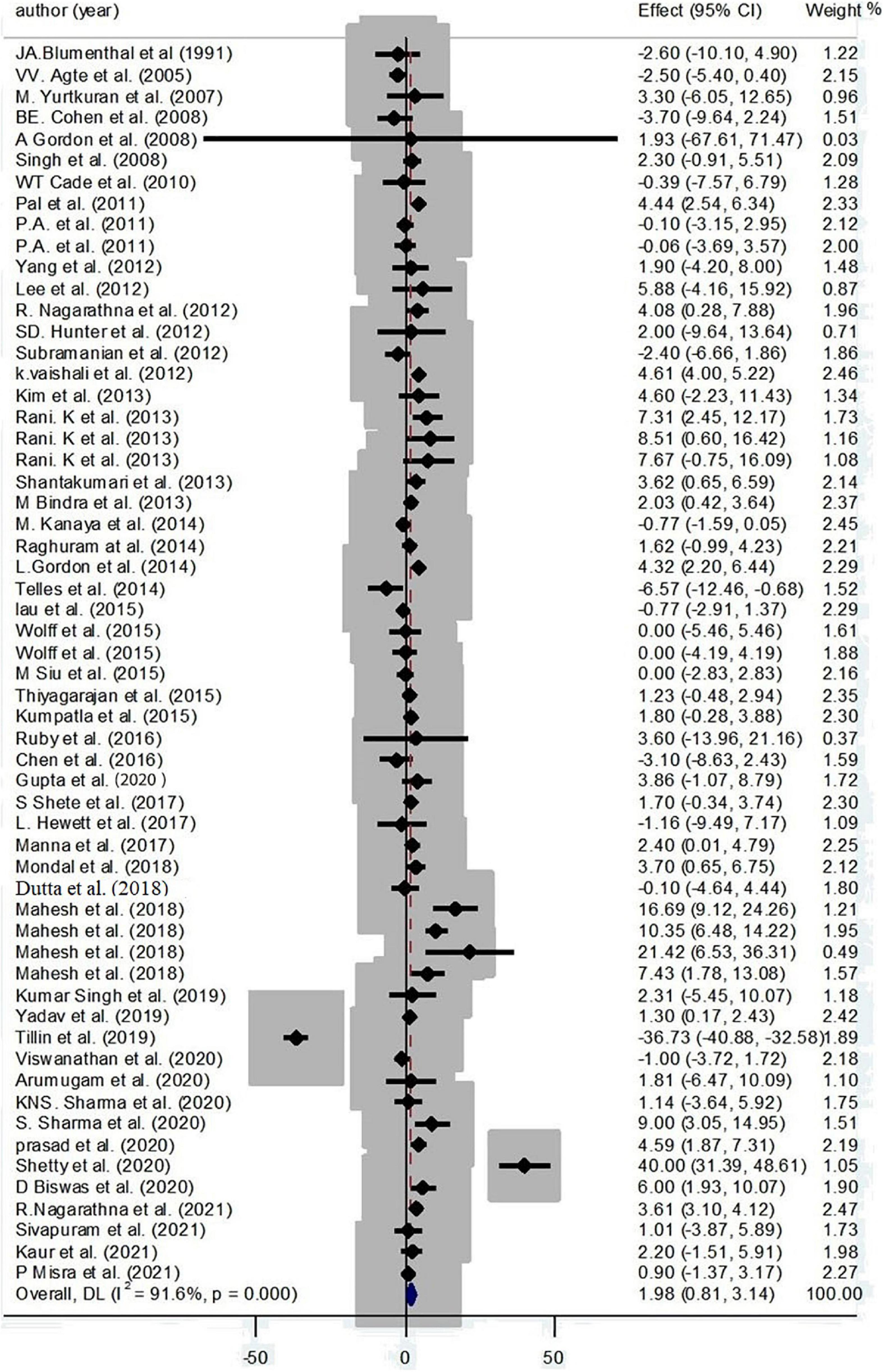
Figure 4. Forest plot for the association between yoga exercise and HDL-C (Random-effect model).
Based on subgroup analysis, continent, condition, and gender were considered as the main sources of heterogeneity. The subgroup analysis based on continent has cleared a positive effect of yoga on HDL-C among Asian participants (3.19 mg/dl; 95% CI: 2.89, 3.48; P < 0.001; I2 = 81.3%, Pheterogeneity < 0.001). Also, a positive effect of yoga on HDL-C levels was found among patients with type 2 diabetes (3.75 mg/dl; 95% CI: 3.41, 4.10; P < 0.001; I2 = 81.9%; Pheterogeneity < 0.001) and hypertension (6.18 mg/dl; 95% CI: 4.25, 8.10; P < 0.001; I2 = 79.6%; Pheterogeneity < 0.001) (Supplementary Table 4).
Based on the result of meta-regression, no effect was found for age on the effect sizes (regression coefficient = 0.03; 95%CI: −0.23, 0.30; P = 0.780) (Supplementary Figure 5).
According to the result of Egger’s test and funnel plot of 58 studies, no evidence of publication bias was found (P = 0.396) (Supplementary Figure 6). Moreover, the sensitivity analysis indicated that the final estimates did not change by the omission of any included studies.
By collecting 58 effect sizes, we found an inverse effect of yoga on TG (−13.50 mg/dl; 95% CI: −20.09, −6.92; P < 0.001; I2 = 90.7%, Pheterogeneity < 0.001) (Figure 5).
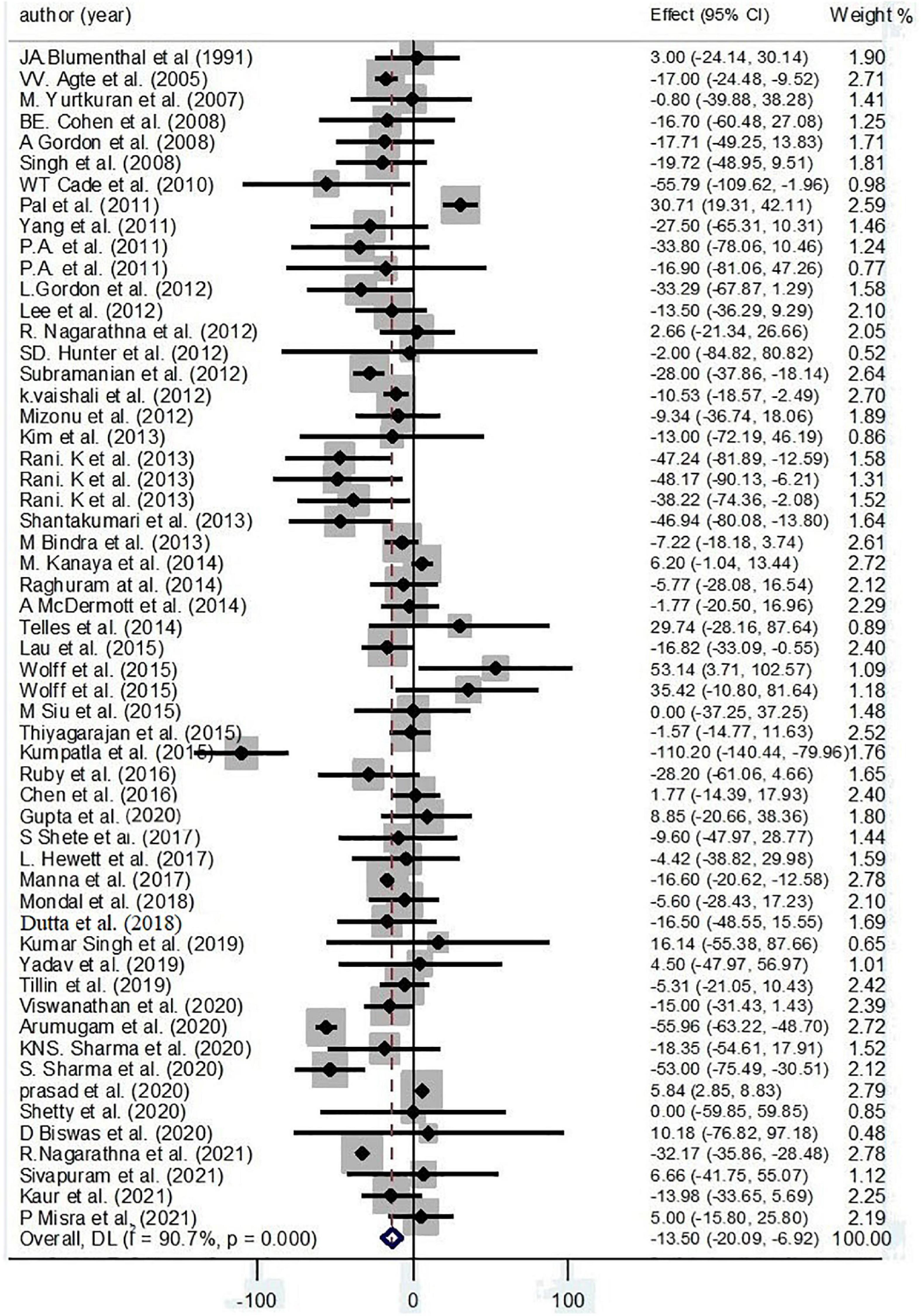
Figure 5. Forest plot for the association between yoga exercise and TG (Random-effect model).
Based on subgroup analysis, continent, condition, and gender were considered the main sources of heterogeneity. The subgroup analysis based on continent has illustrated an inverse effect of yoga on TG among Asian participants (−13.45 mg/dl; 95% CI: −15.08, −11.81; P < 0.001; I2 = 92.3%, Pheterogeneity < 0.001). Also, an inverse effect of yoga on TG levels was found among healthy practitioners (−15.25 mg/dl; 95% CI: −18.55, −11.95; P < 0.001; I2 = 49.2%, Pheterogeneity = 0.032) and patients with CKD (−18.03 mg/dl; 95% CI: −38.17, 2.11; P = 0.079; I2 = 0.0%, Pheterogeneity = 0.471) and type 2 diabetes (−29.96 mg/dl; 95% CI: −32.66, −27.27; P < 0.001; I2 = 87.0%, Pheterogeneity < 0.001) (Supplementary Table 5).
Based on the result of meta-regression, no effect was found for age on the effect sizes (regression coefficient = 0.68; 95%CI: −0.26, 1.64; P = 0.153) (Supplementary Figure 7).
According to the result of Egger’s test and funnel plot of 56 studies, no evidence of publication bias was found (P = 0.781) (Supplementary Figure 8). Moreover, the sensitivity analysis of included trials did not affect the final pooled amounts.
Findings from 21 effect sizes have detected an inverse effect of yoga on VLDL-C (−3.94 mg/dl; 95%CI: −6.31, −1.56; P < 0.001; I2 = 72.2%, Pheterogeneity < 0.001) (Figure 6).
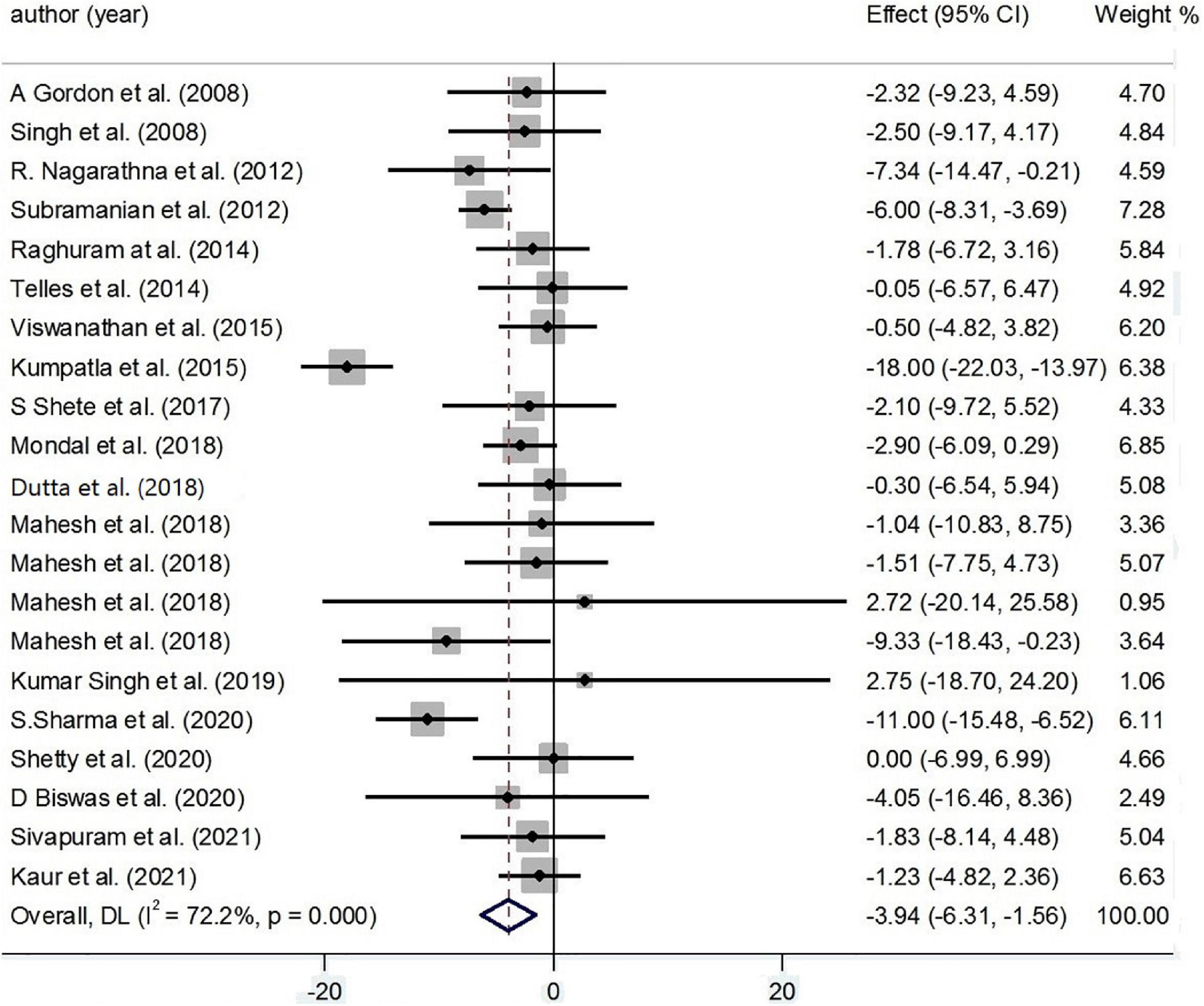
Figure 6. Forest plot for the association between yoga exercise and VLDL-C (Random-effect model).
Based on subgroup analysis, condition, duration, and gender were considered the main sources of heterogeneity. The subgroup analysis based on condition has shown an inverse effect of yoga on VLDL-C levels among healthy practitioners (−5.67 mg/dl; 95% CI: −7.88, −3.46; P < 0.001; I2 = 0.0%, Pheterogeneity = 0.337) and patients with type 2 diabetes (−5.81 mg/dl; 95% CI: −7.44, −4.18; P < 0.001; I2 = 87.5%, Pheterogeneity < 0.001) (Supplementary Table 6).
Based on the result of meta-regression, no effect was found for age on the effect sizes (regression coefficient = 0.20; 95%CI: −0.24, 0.65; P = 0.331) (Supplementary Figure 9).
According to the result of Egger’s test and funnel plot of 53 studies, no evidence of publication bias was found (P = 0.304) (Supplementary Figure 10). Moreover, the sensitivity analysis of included trials did not affect the final pooled amounts.
In the present meta-analysis, we found out from several articles published in 1991 and since then that yoga had decreased TC, LDL-C, TG, and VLDL-C and increased HDL-C among yoga practitioners.
Along with our findings, some articles have shown improvement in lipid profiles. Many researchers have noted that the practice of yoga and yoga-based programs may have a positive influence on body composition and blood lipid profiles (60, 61), mindfulness may help improve chronic diseases by increasing the individual’s ability to encounter challenges with more efficient coping strategies (62, 63), also it has been reported that modification and stress management educational programs lead to significant improvement in the subjective wellbeing scores and can therefore make an appreciable contribution to primary prevention as well as management of diseases (64). For instance, yoga has decreased TC and LDL-C among Asian athletes through its strong potential as a lifestyle management skill in the Indian population (5). Since yoga stimulates metabolism, it had significant effects on improving TC levels in patients with MetS and type 2 diabetes (5). Not only does practicing yoga regularly improve the flexibility but it also has an effective influence on the function of both endocrine and exocrine glands of the body (64), increased B-cells sensitivity of the pancreas to glucose signals (65), and improved insulin sensitivity as well as a decline in insulin resistance (66), which leads to a reduction in both fasting blood glucose (FBG) and postprandial glucose (PPBG) levels and better glycemic control (64, 67).
It has been shown that HDL-C levels have improved among patients with MetS. The potential mechanism behind this has shown yoga improves several MetS components, suggesting that yoga may prevent or improve atherosclerosis (51). The improvement in lipid profile by practicing yoga could be due to increased hepatic lipase and lipoprotein lipase, which can increase the uptake of TGs by adipose tissue and affect lipoprotein metabolism (7). On the other hand, yoga improves LDL-C receptor sensitivity, receptor-mediated endocytosis, and receptor recycling (3). Also, the regulatory effect of yoga on HDL-C is mediated through a reverse cholesterol transport mechanism that includes macrophage cholesterol efflux in arteries (3). In addition, Indian traditional yoga practices are known as an antioxidant or anti-inflammatory against such diseases by replacing inflammatory markers and metabolic risk factors (68, 69). Overall, the possible reason for the reduction in TG, TC, and LDL-C; as well as elevation in HDL-C is that yoga interventions, especially deep breathing, stretching, and flexibility exercises, increased metabolism and utilization of blood lipids and lipoprotein for energy production (33). For instance, in a study, one participant reported that her medication reduced and improved her clinical status after doing yoga every day (64). Studies presented that TG levels were improved by yoga among patients with CKD and type 2 diabetes (12, 15, 32, 35). Also, by following a regular exercise program, VLDL-C was reduced among type 2 diabetes yoga workers (19, 55). Yoga could also assist in the redistribution of body fat and the reduction of abdominal obesity (7). Also, Thind et al. and Cramer et al. concluded yoga improved lipid status in all participants who had T2DM and MetS (70, 71).
Whereas some studies that accessed the effect of yoga interventions on lipid profiles found contradictory results. Koertge et al. demonstrated that yoga had no improvement effect on HDL-C and TG levels in coronary artery disease (CAD) participants (72). Also, Dutta et al. stated that yoga did not lower HbA1c significantly among people who had done yoga as compared to those who had not done yoga (73). Contrary results are probably due to the lack of high-quality data and also due to the fact that lipids profile in most of the studies were not evaluated as a primary outcome (73). In addition, the different number of participants at the end of the study who completed the intervention and dropout samples could influence the exact results (72).
This is the first study that concentrates on the effect of yoga on lipid profiles with a wide searching process, also performed by PRISMA guidelines (74). Another strength is that we included a large number of well-designed RCTs with relatively large sample sizes and performed subgroup analyses that focused on this effectiveness in different diseases and situations. In most of the studies both gender participated, also RCTs with more than 12 weeks have shown better results on lipid profiles (24). However, some limitations must be considered in the current study, for instance; BMI was not reported in many studies and they had not measured the intensity of yoga, besides most of the RCTs were not blinded and all participants were aware of why they did yoga. Many of the included studies were conducted in India, therefore the results may not be generalizable to all countries. Moreover, we did not study this effect on heart rate, body composition, or sleep quality.
To conclude, the results of our meta-analysis expand the evidence that yoga had a striking effect on balancing lipid profiles. However, heterogeneity among studies was notable. Further studies are needed to clarify our findings.
The original contributions presented in this study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
ED and DG designed the article and wrote syntaxes for primary and advanced searchings from PubMed/Medline, Scopus, Web of Science, and the Cochrane and performed first and second screenings for exclusion and inclusion, eventually, 53 articles were included to our article after the final screening. ED, DG, and VB wrote the body of the article and grammatically checked the possible mistakes for all part of the passages. DG and MD extracted the emergency data from all 53 included articles carefully, evaluated addition quality of the studies based on the Cochrane guideline by the following criteria: random sequence generation, allocation concealment, blinding, incomplete outcome data, selective outcome reporting, and other possible sources of bias. ED performed data analyses using Stata software, version 14 from the data extracted information and tables. All authors contributed to the article and approved the submitted version.
This study was supported by Alborz University of Medical Sciences (103-4530).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnut.2022.942702/full#supplementary-material
1. Divya TS, Vijayalakshmi MT, Mini K, Asish K, Pushpalatha M, Suresh V. Cardiopulmonary and metabolic effects of yoga in healthy volunteers. Int J Yoga. (2017) 10:115–20. doi: 10.4103/0973-6131.186162
2. Chen N, Xia X, Qin L, Luo L, Han S, Wang G, et al. Effects of 8-week hatha yoga training on metabolic and inflammatory markers in healthy, female Chinese subjects: a randomized clinical trial. Bio Med Res Int. (2016) 2016:5387258. doi: 10.1155/2016/5387258
3. Nagarathna R, Kumar S, Anand A, Acharya IN, Singh AK, Patil SS, et al. Effectiveness of yoga lifestyle on lipid metabolism in a vulnerable population-a community based multicenter randomized controlled trial. Medicines. (2021) 8:37. doi: 10.3390/medicines8070037
4. Arati M, Arpita P, Arati M. Effect of yoga (asana and pranayama) on serum lipid profile in normal healthy volunteers. Medicine. (2015). Available online at: https://www.semanticscholar.org/paper/Effect-of-Yoga-(Asana-and-Pranayama)-on-Serum-Lipid-Arati-Arpita/024c04c6f70a7b7ab3da0fda6728ef93f15e8d24#citing-papers
5. Lau C, Yu R, Woo J. Effects of a 12-week hatha yoga intervention on metabolic risk and quality of life in Hong Kong Chinese adults with and without metabolic syndrome. PLoS One. (2015) 10:e0130731. doi: 10.1371/journal.pone.0130731
6. Yang K, Bernardo LM, Sereika SM, Conroy MB, Balk J, Burke LE. Utilization of 3-month yoga program for adults at high risk for type 2 diabetes: a pilot study. Evid Based Complement Alternat Med. (2011) 2011:257891. doi: 10.1093/ecam/nep117
7. Shantakumari N, Sequeira S., El deeb R. Effects of a yoga intervention on lipid profiles of diabetes patients with dyslipidemia. Indian Heart J. (2013) 65:127–31. doi: 10.1016/j.ihj.2013.02.010
8. Papp ME, Lindfors P, Nygren-Bonnier M, Gullstrand L, Wändell PE. Effects of high-intensity hatha yoga on cardiovascular fitness, adipocytokines, and apolipoproteins in healthy students: a randomized controlled study. J Alternat Complement Med. (2016) 22:81–7. doi: 10.1089/acm.2015.0082
9. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. (2009) 6:e1000097. doi: 10.1371/journal.pmed.1000097
10. Higgins JP, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, et al. The cochrane collaboration’s tool for assessing risk of bias in randomised trials. BMJ. (2011) 343:d5928. doi: 10.1136/bmj.d5928
11. Kohler CG, Walker JB, Martin EA, Healey KM, Moberg PJ. Facial emotion perception in schizophrenia: a meta-analytic review. Schizophr Bull. (2010) 36:1009–19. doi: 10.1093/schbul/sbn192
12. Arumugam G, Nagarathna R, Majumdar V, Singh M, Srinivasalu R, Sanjival R, et al. Yoga-based lifestyle treatment and composite treatment goals in Type 2 diabetes in a rural South Indian setup- a retrospective study. Sci Rep. (2020) 10:6402. doi: 10.1038/s41598-020-63133-1
13. Rani KB, Sreekumaran E. Yogic practice and diabetes mellitus in geriatric patients. Int J Yoga. (2013) 6:47–54. doi: 10.4103/0973-6131.105946
14. Biswas D. Effect of relaxation technique on lipid profile in cases of essential hypertension. Int J Recent Adv Multidiscip Res. (2020) 7:6225–9.
15. Gordon L, McGrowder DA, Pena YT, Cabrera E, Lawrence-Wright M. Effect of exercise therapy on lipid parameters in patients with end-stage renal disease on hemodialysis. J Lab Phys. (2012) 4:17–23. doi: 10.4103/0974-2727.98665
16. Gupta U, Gupta Y, Jose D, Mani K, Jyotsna VP, Sharma G, et al. Effectiveness of yoga-based exercise program compared to usual care, in improving HbA1c in individuals with type 2 diabetes: a randomized control trial. Int J Yoga. (2020) 13:233–8. doi: 10.4103/ijoy.IJOY_33_20
17. Vaishali K. Effects of yoga-based program on glycosylated hemoglobin level serum lipid profile in community dwelling elderly subjects with chronic type 2 diabetes mellitus–a randomized controlled trial. Phys Occup Ther Geriatr. (2012) 30:22–30. doi: 10.3109/02703181.2012.656835
18. Kaur N, Majumdar V, Nagarathna R, Malik N, Anand A, Nagendra HR. Diabetic yoga protocol improves glycemic, anthropometric and lipid levels in high risk individuals for diabetes: a randomized controlled trial from Northern India. Diabetol Metab Syndr. (2021) 13:149. doi: 10.1186/s13098-021-00761-1
19. Kumpatla S, Michael C, Viswanathan V. Effect of yogasanas on glycaemic, haemodynamic and lipid profile in newly diagnosed subjects with type 2 diabetes. Int J Diabetes. (2015) 35:181–8. doi: 10.1007/s13410-014-0255-2
20. Bindra M, Seema D, Shema N. Influence of pranayamas and yoga-asanas on blood glucose, lipid profile and hba1c in type 2 diabetes 2013. Int J Pharma Bio Sci. (2013) 23:365–8.
21. Manna I. Effects of yoga training on body composition, cardiovascular and biochemical parameters in healthy adult male volunteers. Int J Yoga. (2017) 11:105–10. doi: 10.4103/ijoy.IJOY_31_17
22. McDermott KA, Rao MR, Nagarathna R, Murphy EJ, Burke A, Nagendra RH, et al. A yoga intervention for type 2 diabetes risk reduction: a pilot randomized controlled trial. BMC Complement Alternat Med. (2014) 14:212. doi: 10.1186/1472-6882-14-212
23. Misra P, Sharma G, Tandon N, Kant S, Sangral M, Rai SK, et al. Effect of community-based structured yoga program on Hba1c level among type 2 diabetes mellitus patients: an interventional study. Int J Yoga. (2021) 14:222–8. doi: 10.4103/ijoy.ijoy_150_21
24. Mondal S, Kundu B, Saha S. Yoga as a therapeutic intervention for the management of type 2 diabetes mellitus. Int J Yoga. (2018) 11:129–38. doi: 10.4103/ijoy.IJOY_74_16
25. Murthy SN, Rao NS, Nandkumar B, Kadam A. Role of naturopathy and yoga treatment in the management of hypertension. Complement Ther Clin Pract. (2011) 17:9–12. doi: 10.1016/j.ctcp.2010.08.005
26. Nagarathna R. Efficacy of yoga based life style modification program on medication score and lipid profile in type 2 diabetes-a randomized control study. Int J Diabetes Dev Ctries. (2012) 32:122–30. doi: 10.1007/s13410-012-0078-y
27. Balaji PA, Varne SR, Sadat-Ali S. Effects of yoga pranayama practices on metabolic parameters and anthropometry in type 2 diabetes. Int Multi Discip Res J. (2011) 1:1–4.
28. Dutta A, Green SR, Balayogi AB, Hemachandar R, Dhivya P, Mathew KT. Effect of yoga therapy on fasting lipid profile in chronic kidney disease: a comparative study. Int J Adv Med. (2018):2349–3925. doi: 10.18203/2349-3933.ijam20180955
29. Pal A, Srivastava N, Tiwari S, Verma NS, Narain VS, Agrawal GG, et al. Effect of yogic practices on lipid profile and body fat composition in patients of coronary artery disease. Complement Ther Med. (2011) 19:122–7. doi: 10.1016/j.ctim.2011.05.001
30. Prasad A, Bhardwaj S, Dwivedi S, Arora YK, Sharma V. Effect of yoga in post-myocardial infarction cases. J Sci Innov Res. (2020) 9:63–8.
31. Raghuram N, Parachuri VR, Swarnagowri MV, Babu S, Chaku R, Kulkarni R, et al. Yoga based cardiac rehabilitation after coronary artery bypass surgery: one-year results on LVEF, lipid profile and psychological states–a randomized controlled study. Indian Heart J. (2014) 66:490–502. doi: 10.1016/j.ihj.2014.08.007
32. Sharma S. Influence of yoga on status of lipid indices in type 2 diabetes mellitus subjects. Int J Diabetes Dev Ctries. (2020) 40:410–15. doi: 10.1007/s13410-020-00813-8
33. Sharma KNS, Pailoor S, Choudhary NR, Bhat P, Shrestha S. Integrated yoga practice in cardiac rehabilitation program: a randomized control trial. J Altern Complement Med. (2020) 26:918–27. doi: 10.1089/acm.2019.0250
34. Shete SU, Verma A, Kulkarni DD, Bhogal RS. Effect of yoga training on inflammatory cytokines and C-reactive protein in employees of small-scale industries. J Educ Health Promot. (2017) 6:76. doi: 10.4103/jehp.jehp_65_17
35. Shetty KG. Combined effect of yoga and naturopathy treatments on lipid profile among type 2 diabetes mellitus -a randomised trail. Eur J Biomed Pharm Sci. (2020) 7:368–72.
36. Singh AK, Kaur N, Kaushal S, Tyagi R, Mathur D, Sivapuram MS, et al. Partitioning of radiological, stress and biochemical changes in pre-diabetic women subjected to diabetic yoga protocol. Diabetes Metab Synd. (2019) 13:2705–13. doi: 10.1016/j.dsx.2019.07.007
37. Singh S, Kyizom T, Singh KP, Tandon OP, Madhu SV. Influence of pranayamas and yoga-asanas on serum insulin, blood glucose and lipid profile in type 2 diabetes. Indian J Clin Biochem. (2008) 23:365–8. doi: 10.1007/s12291-008-0080-9
38. Sivapuram MS, Srivastava V, Kaur N, Anand A, Nagarathna R, Patil S, et al. Ayurveda body-mind constitutional types and role of yoga intervention among type 2 diabetes mellitus population of Chandigarh and Panchkula regions. Ann Neurosci. (2020) 27:214–23. doi: 10.1177/09727531211000040
39. Subramanian S, Elango T, Malligarjunan H, Kochupillai V, Dayalan H. Role of sudarshan kriya and pranayam on lipid profile and blood cell parameters during exam stress: a randomized controlled trial. Int J Yoga. (2012) 5:21–7. doi: 10.4103/0973-6131.91702
40. Telles S, Sharma SK, Yadav A, Singh N, Balkrishna A. A comparative controlled trial comparing the effects of yoga and walking for overweight and obese adults. Med Sci Monit. (2014) 20:894–904. doi: 10.12659/MSM.889805
41. Thiyagarajan R, Pal P, Pal GK, Subramanian SK, Trakroo M, Bobby Z, et al. Additional benefit of yoga to standard lifestyle modification on blood pressure in prehypertensive subjects: a randomized controlled study. Hypertens Res. (2015) 38:48–55. doi: 10.1038/hr.2014.126
42. Viswanathan V, Sivakumar S, Sai Prathiba A, Devarajan A, George L, Kumpatla S. Effect of yoga intervention on biochemical, oxidative stress markers, inflammatory markers and sleep quality among subjects with type 2 diabetes in South India: results from the SATYAM project. Diabetes Res Clin Pract. (2021) 172:108644. doi: 10.1016/j.diabres.2020.108644
43. Agte VV. Sudarshan kriya yoga for treating type 2 diabetes. Alternat Complement Ther. (2005) 10:220–2. doi: 10.1089/1076280041580323
44. Yadav R, Yadav RK, Khadgawat R, Pandey RM, Upadhyay AD, Mehta N. Randomized controlled trial of a 12-week yoga-based (including diet) lifestyle vs. dietary intervention on cardio-metabolic risk factors and continuous risk score in indian adults with metabolic syndrome. Behav Med. (2020) 46:9–20. doi: 10.1080/08964289.2018.1538098
45. Blumenthal JA, Emery CF, Madden DJ, Coleman RE, Riddle MW, Schniebolk S, et al. Effects of exercise training on cardiorespiratory function in men and women older than 60 years of age. Am J Cardiol. (1991) 67:633–9. doi: 10.1016/0002-9149(91)90904-y
46. Cohen BE, Chang AA, Grady D, Kanaya AM. Restorative yoga in adults with metabolic syndrome: a randomized, controlled pilot trial. Metab Syndr Relat Disord. (2008) 6:223–9. doi: 10.1089/met.2008.0016
47. Hunter SD, Laosiripisan J, Elmenshawy A, Tanaka H. Effects of yoga interventions practised in heated and thermoneutral conditions on endothelium-dependent vasodilatation: the Bikram yoga heart study. Exp physiol. (2018) 103:391–6. doi: 10.1113/EP086725
48. Kanaya AM, Araneta MR, Pawlowsky SB, Barrett-Connor E, Grady D, Vittinghoff E, et al. Restorative yoga and metabolic risk factors: the practicing restorative yoga vs.stretching for the metabolic syndrome (PRYSMS) randomized trial. J Diabetes Complicat. (2014) 28:406–12. doi: 10.1016/j.jdiacomp.2013.12.001
49. Ruby M, Repka CP, Arciero PJ. Comparison of protein-pacing alone or with yoga/stretching and resistance training on glycemia, total and regional body composition, and aerobic fitness in overweight women. J Phys Act Health. (2016) 13:754–64. doi: 10.1123/jpah.2015-0493
50. Siu PM, Yu AP, Benzie IF, Woo J. Effects of 1-year yoga on cardiovascular risk factors in middle-aged and older adults with metabolic syndrome: a randomized trial. Diabetol Metab Syndr. (2015) 7:40. doi: 10.1186/s13098-015-0034-3
51. Kim HN, Ryu J, Kim KS, Song SW. Effects of yoga on sexual function in women with metabolic syndrome: a randomized controlled trial. J Sex Med. (2013) 10:2741–51. doi: 10.1111/jsm.12283
52. Lee JA, Kim JW, Kim DY. Effects of yoga exercise on serum adiponectin and metabolic syndrome factors in obese postmenopausal women. Menopause. (2012) 19:296–301. doi: 10.1097/gme.0b013e31822d59a2
53. Wolff M, Memon AA, Chalmers JP, Sundquist K, Midlöv P. Yoga’s effect on inflammatory biomarkers and metabolic risk factors in a high risk population - a controlled trial in primary care. BMC Cardiovasc Disord. (2015) 15:91. doi: 10.1186/s12872-015-0086-1
54. Cade WT, Reeds DN, Mondy KE, Overton ET, Grassino J, Tucker S, et al. Yoga lifestyle intervention reduces blood pressure in HIV-infected adults with cardiovascular disease risk factors. HIV Med. (2010) 11:379–88. doi: 10.1111/j.1468-1293.2009.00801.x
55. Gordon LA, Morrison EY, McGrowder DA, Young R, Fraser YT, Zamora EM, et al. Effect of exercise therapy on lipid profile and oxidative stress indicators in patients with type 2 diabetes. BMC Complement Alternat Med. (2008) 8:21.
56. Hewett ZL, Pumpa KL, Smith CA, Fahey PP, Cheema BS. Effect of a 16-week Bikram yoga program on heart rate variability and associated cardiovascular disease risk factors in stressed and sedentary adults: a randomized controlled trial. BMC Complement Alternat Med. (2017) 17:226. doi: 10.1186/s12906-017-1740-1
57. Mizuno J, Monteiro HL. An assessment of a sequence of yoga exercises to patients with arterial hypertension. J Bodyw Mov Ther. (2013) 17:35–41. doi: 10.1016/j.jbmt.2012.10.007
58. Tillin T, Tuson C, Sowa B, Chattopadhyay K, Sattar N, Welsh P, et al. Yoga and cardiovascular health trial (YACHT): a UK-based randomised mechanistic study of a yoga intervention plus usual care versus usual care alone following an acute coronary event. BMJ Open. (2019) 9:e030119. doi: 10.1136/bmjopen-2019-030119
59. Yurtkuran M, Alp A, Yurtkuran M, Dilek K. A modified yoga-based exercise program in hemodialysis patients: a randomized controlled study. Complement Ther Med. (2007) 15:164–71. doi: 10.1016/j.ctim.2006.06.008
60. Isayeva AS, Vovchenko MM, Galchynska VY. Blood lipids and anthropometric parameters in healthy subjects practicing yoga or resistance training in leisure time. What matters: type or intensity of physical activity? Pol Merkur Lekarski. (2021) 49:203–8.
61. Sadhasivam S, Alankar S, Maturi R, Williams A, Vishnubhotla RV, Hariri S, et al. Isha yoga practices and participation in samyama program are associated with reduced HbA1C and systemic inflammation. Improved lipid profile, and short-term and sustained improvement in mental health: a prospective observational study of meditators. Front Psychol. (2021) 12:659667. doi: 10.3389/fpsyg.2021.659667
62. Shapiro SL, Carlson LE, Astin JA, Freedman B. Mechanisms of mindfulness. J Clin Psychol. (2006) 62:373–86. doi: 10.1002/jclp.20237
63. Vago DR, Silbersweig DA. Self-awareness, self-regulation, and self-transcendence (S-ART): a framework for understanding the neurobiological mechanisms of mindfulness. Front Hum Neurosci. (2012) 6:296. doi: 10.3389/fnhum.2012.00296
64. Madanmohan, Bhavanani AB, Dayanidy G, Sanjay Z, Basavaraddi IV. Effect of yoga therapy on reaction time, biochemical parameters and wellness score of peri and post-menopausal diabetic patients. Int J Yoga. (2012) 5:10–5. doi: 10.4103/0973-6131.91696
65. Manjunatha S, Vempati RP, Ghosh D, Bijlani RL. An investigation into the acute and long-term effects of selected yogic postures on fasting and postprandial glycemia and insulinemia in healthy young subjects. Indian J Physiol Pharmacol. (2005) 49:319–24.
67. Singh S, Malhotra V, Singh KP, Madhu SV, Tandon OP. Role of yoga in modifying certain cardiovascular functions in type 2 diabetic patients. J Assoc Physicians India. (2004) 52:203–6.
68. Sarvottam K, Yadav RK. Obesity-related inflammation & cardiovascular disease: efficacy of a yoga-based lifestyle intervention. Indian J Med Res. (2014) 139:822–34.
69. Vijayaraghava A, Doreswamy V, Narasipur OS, Kunnavil R, Srinivasamurthy N. Effect of yoga practice on levels of inflammatory markers after moderate and strenuous exercise. J Clin Diagn Res. (2015) 9:CC08–12. doi: 10.7860/JCDR/2015/12851.6021
70. Cramer H, Langhorst J, Dobos G, Lauche R. Yoga for metabolic syndrome: a systematic review and meta-analysis. Eur J Prev Cardiol. (2016) 23:1982–93. doi: 10.1177/2047487316665729
71. Thind H, Lantini R, Balletto BL, Donahue ML, Salmoirago-Blotcher E, Bock BC, et al. The effects of yoga among adults with type 2 diabetes: a systematic review and meta-analysis. Prev Med. (2017) 105:116–26. doi: 10.1016/j.ypmed.2017.08.017
72. Koertge J, Weidner G, Elliott-Eller M, Scherwitz L, Merritt-Worden TA, Marlin R, et al. Improvement in medical risk factors and quality of life in women and men with coronary artery disease in the multicenter lifestyle demonstration project. Am J Cardiol. (2003) 91:1316–22. doi: 10.1016/s0002-9149(03)00320-5
73. Dutta D, Bhattacharya S, Sharma M, Khandelwal D, Surana V, Kalra S. Effect of yoga on glycemia and lipid parameters in type-2 diabetes: a meta-analysis. J Diabetes Metab Disord. (2021) 20:349–67. doi: 10.1007/s40200-021-00751-0
Keywords: yoga, exercise, lipid profile, systematic review, meta-analysis
Citation: Ghazvineh D, Daneshvar M, Basirat V and Daneshzad E (2022) The Effect of Yoga on the Lipid Profile: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Front. Nutr. 9:942702. doi: 10.3389/fnut.2022.942702
Received: 12 May 2022; Accepted: 16 June 2022;
Published: 14 July 2022.
Edited by:
Vassilis Mougios, Aristotle University of Thessaloniki, GreeceReviewed by:
Raj Kumar Yadav, All India Institute of Medical Sciences, IndiaCopyright © 2022 Ghazvineh, Daneshvar, Basirat and Daneshzad. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Elnaz Daneshzad, ZGFuZXNoemFkQGdtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.