 Inmaculada Xu Lou
Inmaculada Xu Lou Eugenia Gil-García1
Eugenia Gil-García1 Kamran Ali
Kamran Ali Esther Molina
Esther Molina
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Nutr., 08 August 2022
Sec. Clinical Nutrition
Volume 9 - 2022 | https://doi.org/10.3389/fnut.2022.931090
This article is part of the Research TopicInsights in Clinical NutritionView all 30 articles
Objectives: Chronic pain (CP) is an unpleasant emotional and sensory experience that can be accompanied by tissue damage that persists for more than 3 months. Recent studies show that certain nutritional strategies can help to improve pain, so this study is aimed to systematically review scientific evidence to understand and map the effect of the use of nutritional strategies on the presence or intensity of chronic non-cancer pain (CNCP) and the association of these nutritional aspects with the presence or intensity of CNCP.
Study design: A systematic review.
Methods: Two independent researchers searched for randomized clinical trials (RCTs) and observational studies that explored the relationship between nutrition and CNCP in adults from 2010 to 2020 in PubMed, Web of Science, Scopus, and Cochrane Library databases. A total of 24 studies were included, of which 20 were RCTs and 4 were observational studies. They are classified into the administration of nutritional supplements, dietary modification, and incorporation of food.
Results: Of these studies, those that have a significant effect on pain are dietary modification and the use of nutritional supplements. On the other hand, the main results from the few observational studies included in this review point to the existence of an association relationship between less pain and a ketogenic or hypocaloric diet or adherence to the Mediterranean diet.
Conclusion: Dietary modification seems to be one plausible therapeutic option to improve and relieve CNCP. However, more research is needed in this regard to obtain better conclusions.
Systematic Review Registration: [www.crd.york.ac.uk/prospero], identifier [CRD42021226431].
According to the International Association for the Study of Pain, chronic pain (CP) is defined as an unpleasant emotional and sensory experience that may or may not be accompanied by tissue damage that persists for more than 3 months (1, 2). When pain is not a consequence of an oncological process, it is called chronic non-cancer pain (CNCP) (3).
It is estimated that one in five people in the world suffers from CP and one in three cannot maintain an independent lifestyle due to pain (4).
It produces consequences in the performance of daily activities, in the practice of physical exercise (3), and poor quality sleep (5), and it is difficult to participate in social activities (6) with significant social and health costs (1, 7).
The main intervention for CP relief is the use of antalgic drugs, which gives rise to numerous adverse effects (7). Nevertheless, there are currently other approaches to pain, such as psychosocial strategies, physical activity interventions (2), or nutritional care (8), which seem to show positive results in pain relief.
Recent studies show the potential use of nutritional strategies to decrease pain sensation or reduce the risk of suffering from CP since it is cheaper than analgesic drugs and is less likely to produce adverse effects. That is why some researchers have tried to shed light on the role of nutritional elements in CP. Thus, our objective was to systematically review scientific evidence based on clinical and observational studies to understand and map the effect of the use of different nutrients, foods, or food supplements on the presence or intensity of CNCP, and the association of these nutritional aspects with the presence or intensity of CNCP.
Between March and April 2020, a search was carried out for documents published in the last 10 years in the PubMed, Web of Science, Scopus, and Cochrane Library databases.
The search equation was as follows: (diet OR antioxidants OR micronutrients OR nutrition OR “integrative pain medicine” OR healing OR eating OR “nutritional status” OR “anti-inflammatory diet” OR food OR eating OR appetite OR “food habits” OR “food preferences” OR nutrient OR “diet therapy”) AND (“chronic pain” OR “persistent pain” OR “long term pain” OR pain OR “back pain” OR neuralgia OR “trigeminal neuralgia” OR hyperalgesia OR fibromyalgia OR “phantom limb” OR “complex regional pain syndromes” OR “nociceptive pain” OR headache OR endometriosis OR migraine OR arthritis) NOT (cancer OR tumor OR oncolog*).
The selected documents were (1) original articles or systematic reviews that explored the relationship between nutrition and CNCP; (2) published between 2010 and 2020; (3) in English or Spanish; (4) with experimental (randomized clinical trials; RCTs) or observational epidemiological design; (5) implemented in over 18 years old population, men, and/or women; (6) full text available, and (7) with sufficient methodological quality. Specifically, only those observational studies that had a high or acceptable methodological quality according to the Scottish Intercollegiate Guidelines Network (SIGN) tool (9) and experimental studies with a score greater than 3 on the Jadad scale (10) were included in the present review.
The exclusion criteria were (1) documents that studied pharmacological and surgical treatments with no nutritional approach for CNCP, (2) acute pain, and (3) as this systematic review is focused only on nutritional interventions, pain derived from surgical interventions or oncological processes was also excluded.
The search and screening of documents were carried out by two researchers independently and the discrepancies regarding the selected documents were resolved by consensus of the researchers. Registration was made in the International Prospective Register of Systematic Reviews (PROSPERO) with the code CRD42021226431.
A data extraction table was created for the documents included in the review (Table 1), with the following items: first author, year, type of pain, objectives, method, sample, duration, measuring instruments, intervention design, and results.
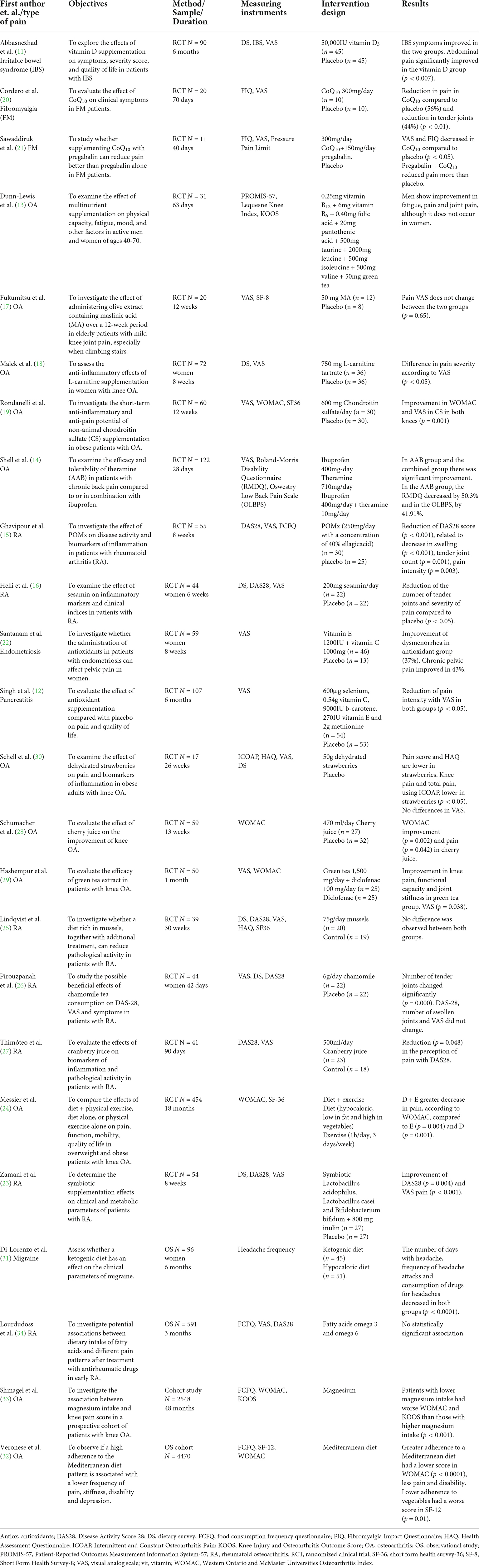
Table 1. Main characteristics of the studies included in this systematic review.
A total of 17,295 documents were found. Of these, 64 articles were selected for full-text reading of which 24 documents were finally included. Figure 1 summarizes the selection process of the studies included in this review.
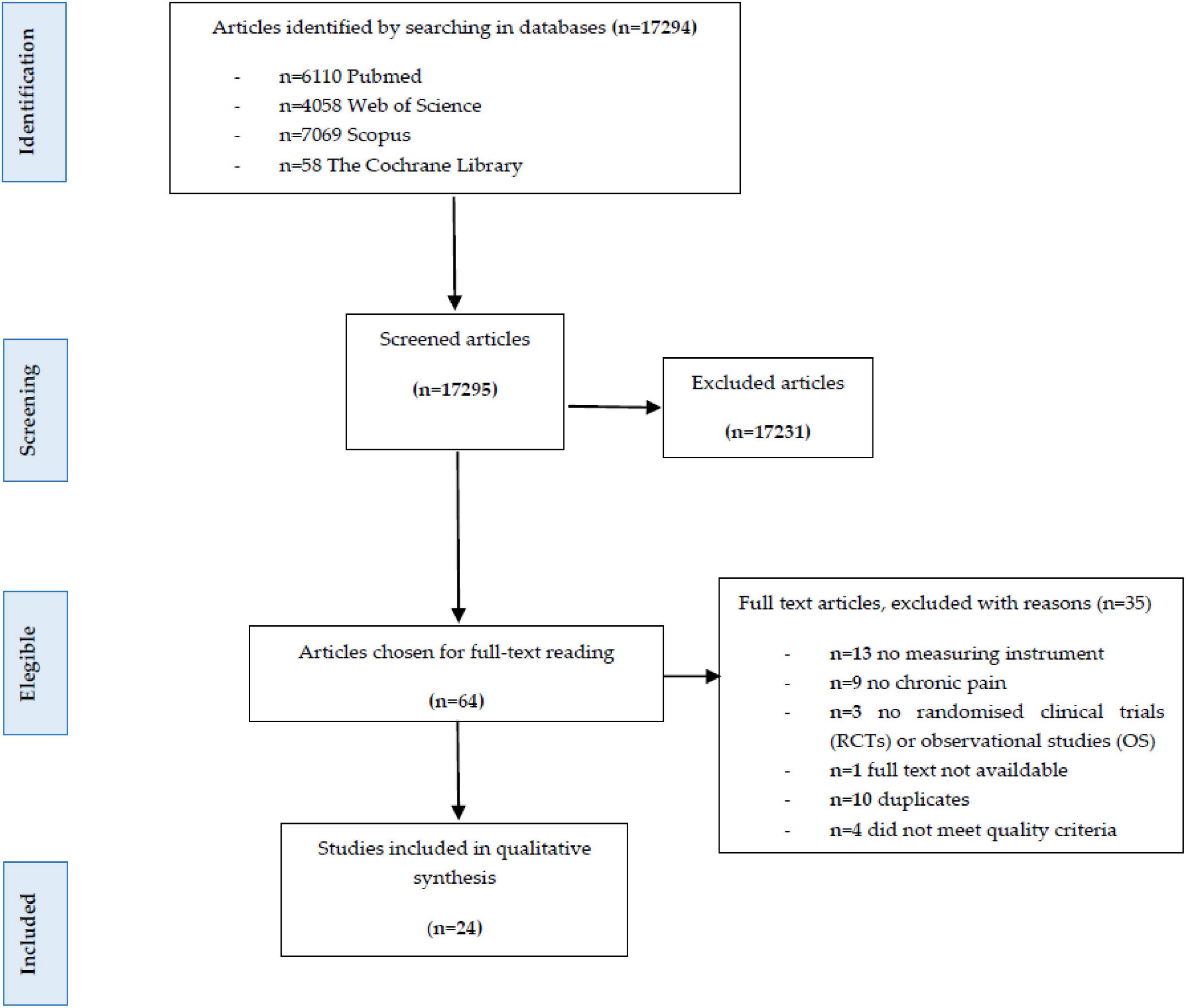
Figure 1. Preferred reporting items for systematic reviews (PRISMA) flow diagram.
Regarding the epidemiological design of the studies included, 20 studies were experimental (RCTs), 2 studies were prospective cohort observational studies, 1 was the retrospective cohort, and 1 was case-control. The most common etiology of pain in the studies was osteoarthritis (n = 10), followed by rheumatoid arthritis (n = 7). Table 1 describes the main characteristics of the studies included in this systematic review.
The nutritional interventions evaluated for CNCP in the studies included the administration of nutritional supplements, dietary modification, and incorporation of food.
Regarding the studies carried out on pain caused by chronic pancreatitis, Abbasnezhad et al. (11) reported a significant improvement in pain during 6 months with the administration of 50,000 IU of vitamin D (p < 0.007). In addition, Singh et al. (12) described a significant reduction in the number of days with pain caused by chronic pancreatitis (p < 0.05) and a significant decrease in the intensity of the pain (p = 0.001) evaluated with the visual analog scale (VAS) after 3 months under treatment with an antioxidant compound of 600 μg of selenium, 0.54 g of vitamin C, 9,000 IU of beta carotene, 270 IU of vitamin E, and 2 g of methionine.
Regarding chronic back pain, Dunn-Lewis et al. (13) found a significant decrease (p < 0.05) in the intensity of back pain measured with the Patient-Reported Outcomes Measurement Information System–57 (PROMIS-57) and Knee Injury and Osteoarthritis Outcome Score (KOOS) instruments in men after supplementing the diet for 63 days with a multi-nutrient complex containing 0.25 mg of vitamin B12, 6 mg of vitamin B6, 0.40 mg of folic acid, 20 mg of pantothenic acid, 500 mg of taurine, 2,000 mg of leucine, 500 mg of isoleucine, 500 mg of valine, and 50 mg of green tea per supplement unit. However, no change in the intensity of pain was detected in women. Shell et al. (14) found a decrease in back pain intensity measured with the Roland Morris and Oswestry Disability Scales after 28 days of intervention with the combined administration of theramine (710 mg/day) and ibuprofen (p < 0.05).
Concerning patients with CP due to rheumatoid arthritis, Ghavipour et al. (15) supplemented the diet of the participants with two daily capsules of POMx (250 mg/day with a concentration of 40% ellagic acid) for 8 weeks and observed a significant reduction in rheumatoid arthritis pain perception measured with disease activity score-28 (DAS28; p < 0.001) and a decrease in the number of tender joints (p = 0.001) that also reduced pain intensity (p = 0.003). Helli et al. (16) observed that when 200 mg/day of sesamin was administered for 6 weeks, the number of tender joints and the intensity of pain evaluated with DAS28 and VAS were significantly reduced (p < 0.05 for both of them).
In the case of pain caused by osteoarthritis, Fukumitsu et al. (17) performed an intervention with maslinic acid with a dose of 50 mg/day for 12 weeks and found no significant difference in pain intensity measured with VAS when compared with the placebo group. However, Malek et al. (18), after using L-carnitine with a dose of 750 mg/day for 8 weeks, did find significantly lower pain intensity levels assessed by the VAS in the intervention group as compared to the control group (p = 0.019). Analogously, Rondanelli et al. (19) found that the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) score in the group that had consumed chondroitin sulfate for 12 weeks at a dose of 600 mg/day had decreased significantly by 8.70 points, compared to the placebo group (p = 0.001).
On the other hand, Cordero et al. (20) evaluated pain in patients with fibromyalgia using Fibromyalgia Impact Questionnaire (FIQ). After the administration of 300 mg/day of CoQ10 for 70 days, they found a significant reduction in pain intensity (p < 0.01) and a significantly lower number of tender joints (p < 0.01) in comparison with the placebo. Furthermore, Sawaddiruk et al. (21) studied the effect of CoQ10 at a dose of 300 mg/day for 40 days in fibromyalgia and observed that the VAS and FIQ values decreased significantly in the CoQ10 group as compared to the placebo (p < 0.05).
Regarding dysmenorrhea, Santanam et al. (22) found a significant decrease in the number of painful days of the menstrual cycle in the group of participants who had ingested 1,200 IU of vitamin E and 1,000 mg of vitamin C for 8 weeks (p < 0.05). After the antioxidant intervention, chronic pelvic pain was decreased in 43% of the patients, and dysmenorrhea was descended in 37%.
For their part, Zamani et al. (23) carried out a clinical trial administering symbiotic supplements (Symbiotic Lactobacillus acidophilus, Lactobacillus casei, Bifidobacterium bifidum, and 800 mg inulin) for 8 weeks to patients with rheumatoid arthritis. A significant improvement was observed in scores measured with the DAS28 and VAS scales in this group (p = 0.004 and p < 0.001, respectively).
In other research studies, diet intervention is accompanied by physical exercise. Messier et al. (24) carried out an intervention with a hypocaloric diet (low in fat and high in vegetables) combined with 1 h per day of physical training for 3 days a week, alternating aerobic and strength exercises in patients with osteoarthritis. The results showed that the compressive strength in the knee was decreased by 5% in the group that only did physical exercise (E), 10% in the group where only the diet was modified (D), and 9% in the diet group accompanied by physical exercise (D + E) at 18 months. However, in the D + E group, a greater decrease in pain was found, according to WOMAC, at 18 months when compared to E (p = 0.004) and D (p = 0.001).
The addition of foods, such as mussels, chamomile tea, blueberry or cherry juice, green tea, and strawberries, has been studied to evaluate the reduction of osteoarticular pain.
With respect to rheumatoid arthritis, Lindqvist et al. (25) observed that the group that consumed 75 g/day of mussels showed a lower intensity of perceived pain measured with DAS28 (p = 0.017). However, this difference was not observed when compared with the group that consumed meat (p = 0.200). Likewise, no statistically significant difference was obtained when comparing the number of tender joints and the assessment of pain intensity using the VAS tool when comparing the intervention group with the control group (p = 0.48). For their part, Pirouzpanah et al. (26) analyzed the effect of chamomile tea (6 g/day) on rheumatoid arthritis. The number of tender joints was decreased significantly (p < 0.001), although this change was not observed in the score measured by DAS28, the number of swollen joints, or the perception of pain. Regarding the consumption of blueberry juice (500 ml/day) at 90 days, Thimóteo et al. (27) stated that there was a significant reduction (p = 0.048) in the perception of pain when compared with the control group measured with the DAS28 instrument.
For osteoarthritis, Schumacher et al. (28) observed a significant improvement in the WOMAC score at 13 weeks in the group that consumed 470 ml/day of cherry juice (p = 0.002) when compared with the placebo group. The same relationship was observed by Hashempur et al. (29) in all the variables analyzed (knee pain, functional capacity, and joint stiffness) that included the VAS score (p = 0.038) in the group that consumed green tea (1,500 ml/day) during 30 days. In the control group, pain intensity only significantly descended when measured with WOMAC but not when measured with VAS.
Regarding knee pain, Schell et al. (30) described that in the group that consumed 50 g/day of strawberries, the intensity of pain was significantly lower at 12 weeks (p < 0.05) for both constant pain and intermittent pain, measured with the Intermittent and Constant Osteoarthritis Pain (ICOAP), although there were no differences in VAS for pain at the end of the 26 weeks of intervention.
Nutritional aspects, such as the type of diet or some supplements, have been evaluated from observational studies for their plausible relation to pain. Concerning diet modification studies, Di Lorenzo et al. (31) observed that the number of days with headache was decreased in the two groups that followed hypocaloric or ketogenic diet (p < 0.0001). However, this improvement had occurred earlier in the group with a hypocaloric diet, from the second month, while in the group with a ketogenic diet, it had occurred from the sixth month. On the other hand, other clinical variables, such as frequency of headache attacks or consumption of drugs for headaches, were decreased equally in the two groups from the sixth month (p < 0.0001). Furthermore, Veronese et al. (32) found that patients who had greater adherence to the Mediterranean diet had better scores in WOMAC (p < 0.0001) and less general pain evaluated by WOMAC (p < 0.05).
Regarding the observational studies about nutritional supplements, Shmagel et al. (33) focused on knee pain in patients with osteoarthritis and observed that a lower intake of magnesium in the diet was associated with worse scores on WOMAC and KOOS than those with higher magnesium intake (p < 0.001). Likewise, they found a relationship between people who had low magnesium intakes in their diet and greater intensity of knee pain due to osteoarthritis at 48 months of follow-up. However, Lourdudoss et al. (34) did not find a statistically significant association between the consumption of omega 3 fatty acids within the diet and pain due to rheumatoid arthritis nor did they found an association between supplementation with omega 3, omega 6, and the omega 6:omega 3 ratios with DAS28 scores.
The aim of this study was to review the scientific literature on the impact of the use of nutritional strategies among people with CNCP. We found that most of the interventions with nutritional supplements collected in our study show improvement and relief in CP (11, 13, 20, 21). This is also the case when it is modified to a hypocaloric, Mediterranean, or with a healthier profile diet (24, 31, 32). However, the use of stand-alone foods, such as fruit juices, yields few hopeful results (26, 30).
We found a few studies whose intervention was the modification of the diet, and it was easier to find studies whose intervention was by using a capsule or pill. This could be due to the ease of applicability of the second one, while the modification in diet requires more effort both in patients and researchers. That is why we understand the nutritional education of special relevance in these patients, highlighting above all the main difficulties they may go through, such as lack of knowledge, lack of interest, or rigidity in the face of change (35).
The use of nutritional interventions to relieve pain in clinical practice has numerous benefits, such as fewer adverse effects than drugs, being more economical methods, or increasing patient autonomy (7, 8, 36).
We observe that the intervention that offers the best results is diet modification. This is also confirmed by Brain et al. (8), Clinton et al. (37), and Kaartinen et al. (38). However, this modification has to be easy to wear, durable, and adapted to the patient to obtain the best results (35).
Brain et al. (8) included four types of interventions in their review, which were dietary modifications, nutrient intake modifications, use of nutritional supplements, and use of fasting. Comparing our systematic review with that carried out by Brain et al. (8), we found that their team did not include observational studies and interventions that were to add a specific food. In addition, they included non-RCTs, so we could find some bias. On the other hand, if we compare it with Ahmed Ali et al. (39), they conducted a systematic review that specifically focused on clinical trials on chronic pancreatitis, while our team has addressed a broader field.
The main limitation that we found in our study was that there are still a few studies on the relationship between nutrition and pain, maybe because it is a new topic (36). When comparing the 24 documents included in this review, the heterogeneity between them was revealed, which particularly affects the methodology and design of the intervention. It is for this reason that we could not do a meta-analysis. An effort is needed to carry out future research on this topic using validated instruments to assess non-cancer CP and the nutritional variables, with deep described homogeneous interventions on large and well-characterized patient samples.
The results obtained show that there are nutritional interventions, especially diet modification, that can improve and alleviate CNCP. Furthermore, there is a need for future research to study CP as an independent entity and not as a symptom of the disease. If the evidence is strong, interventions could be applied in a clinical setting to improve the quality of life of patients suffering from this problem.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
IX obtained the data, performed the analysis, and contributed to writing the draft. EM performed the literature review, supervised all aspects of its implementation, contributed to the review of the manuscript, and contributed ideas and approved the final version. EG-G and RC-M supervised all aspects of its implementation, contributed to the revision of the manuscript, and contributed ideas and approved the final version. KA edited and corrected the article. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Herrera AS, Rolle PA, Babul KM, Maldonado MA, Zamora HM, Nazar JC. Pain management: Prescription opioid use disorder and its relationship with clinical practice. Chil J Anesth. (2017) 45:35–41.
2. World Health Organization [WHO]. WHO Guideline for the management of chronic pain in children. Geneva: World Health Organization (2020). p. 1–11.
3. Cáceres-Matos R, Gil-García E, Barrientos-Trigo S, Porcel-Gálvez AM, Cabrera-León A. Consequences of non-oncological chronic pain in adulthood. Scoping review. Rev Saude Publica. (2020) 54:39.
4. De Barutell C. Pain units in Spain. SED survey pain day 2007. Mag Spanish Soc Pain. (2009) 16:421–8.
5. Reid MC, Williams CS, Gill TM. The relationship between psychological factors and disabling musculoskeletal pain in community-dwelling older persons. J Am Geriatr Soc. (2003) 51:1092–8.
6. World Health Organization [WHO]. WHO world health organization supports global effort to relieve chronic pain. Geneva: World Health Organization (2004).
7. Piegang BN, Tigoufack IBN, Ngnokam D, Achounna AS, Watcho P, Greffrath W, et al. Cycloartanes from Oxyanthus pallidus and derivatives with analgesic activities. BMC Complement Altern Med. (2016) 16:97. doi: 10.1186/s12906-016-1075-3
8. Brain K, Burrows TL, Rollo ME, Chai LK, Clarke ED, Hayes C, et al. A systematic review and meta-analysis of nutrition interventions for chronic noncancer pain. J Hum Nutr Diet. (2018) 32:198–225. doi: 10.1111/jhn.12601
9. (SIGN) SIGN. Scottish intercollegiate guidelines network (sign) [internet]. Scottish intercollegiate guidelines network SIGN. (2020). Available from: https://www.sign.ac.uk/what-we-do/methodology/checklists/ [cited 2020 Jul 11] *
10. Jadad Bechara A. Jadad scale [Internet]. Journal of controlled clinical trials. San Francisco, CA: Scribd Inc (1996).
11. Abbasnezhad A, Amani R, Hajiani E, Alavinejad P, Cheraghian B, Ghadiri A. Effect of vitamin D on gastrointestinal symptoms and health-related quality of life in irritable bowel syndrome patients: A randomized double-blind clinical trial. Neurogastroenterol Motil. (2016) 28:1533–44. doi: 10.1111/nmo.12851
12. Singh N, Ahuja V, Sachdev V, Upadhyay AD, Goswami R, Ramakrishnan L, et al. Antioxidants for pancreatic functions in chronic pancreatitis: A double-blind randomized placebo-controlled pilot study. J Clin Gastroenterol. (2020) 54:284–93. doi: 10.1097/MCG.0000000000001178
13. Dunn-Lewis C, Kraemer WJ, Kupchak BR, Kelly NA, Creighton BA, Luk HY, et al. A multi-nutrient supplement reduced markers of inflammation and improved physical performance in active individuals of middle to older age: A randomized, double-blind, placebo-controlled study. Nutr J. (2011) 10:90. doi: 10.1186/1475-2891-10-90
14. Shell WE, Pavlik S, Roth B, Silver M, Breitstein ML, May L, et al. Reduction in pain and inflammation associated with chronic low back pain with the use of the medical food theramine. Am J Ther. (2016) 23:e1353–62. doi: 10.1097/MJT.0000000000000068
15. Ghavipour M, Sotoudeh G, Tavakoli E, Mowla K, Hasanzadeh J, Mazloom Z. Pomegranate extract alleviates disease activity and some blood biomarkers of inflammation and oxidative stress in rheumatoid arthritis patients. Eur J Clin Nutr. (2017) 71:92–6. doi: 10.1038/ejcn.2016.151
16. Helli B, Shahi MM, Mowla K, Jalali MT, Haghighian HK. A randomized, triple-blind, placebo-controlled clinical trial, evaluating the sesamin supplement effects on proteolytic enzymes, inflammatory markers, and clinical indices in women with rheumatoid arthritis. Phytother Res. (2019) 33:2421–8. doi: 10.1002/ptr.6433
17. Fukumitsu S, Villareal MO, Aida K, Hino A, Hori N, Isoda H, et al. Maslinic acid in olive fruit alleviates mild knee joint pain and improves quality of life by promoting weight loss in the elderly. J Clin Biochem Nutr. (2016) 59:220–5. doi: 10.3164/jcbn.16-40
18. Malek Mahdavi A, Mahdavi R, Kolahi S. Effects of l-carnitine supplementation on serum inflammatory factors and matrix metalloproteinase enzymes in females with knee osteoarthritis: A randomized, double-blind, placebo-controlled pilot study. J Am Coll Nutr. (2016) 35:597–603. doi: 10.1080/07315724.2015.1068139
19. Rondanelli M, Braschi V, Gasparri C, Nichetti M, Faliva MA, Peroni G, et al. Effectiveness of non-animal chondroitin sulfate supplementation in the treatment of moderate knee osteoarthritis in a group of overweight subjects: A randomized, double-blind, placebo-controlled pilot study. Nutrients. (2019) 11:2027. doi: 10.3390/nu11092027
20. Cordero MD, Alcocer-Gómez E, De Miguel M, Culic O, Carrión AM, Alvarez-Suarez JM, et al. Can coenzyme Q10 improve clinical and molecular parameters in fibromyalgia? Antioxid Redox Signal. (2013) 19:1356–61. doi: 10.1089/ars.2013.5260
21. Sawaddiruk P, Apaijai N, Paiboonworachat S, Kaewchur T, Kasitanon N, Jaiwongkam T, et al. Coenzyme Q10 supplementation alleviates pain in pregabalin-treated fibromyalgia patients via reducing brain activity and mitochondrial dysfunction. Free Radic Res. (2019) 53:901–9. doi: 10.1080/10715762.2019.1645955
22. Santanam N, Kavtaradze N, Murphy A, Dominguez C, Parthasarathy S. Antioxidant supplementation reduces endometriosis-related pelvic pain in humans. Transl Res. (2013) 161:189–95. doi: 10.1016/j.trsl.2012.05.001
23. Zamani B, Farshbaf S, Golkar HR, Bahmani F, Asemi Z. Synbiotic supplementation and the effects on clinical and metabolic responses in patients with rheumatoid arthritis: A randomised, double-blind, placebo-controlled trial. Br J Nutr. (2017) 117:1095–102.
24. Messier SP, Mihalko SL, Legault C, Miller GD, Nicklas BJ, DeVita P, et al. Effects of intensive diet and exercise on knee joint loads, inflammation, and clinical outcomes among overweight and obese adults with knee osteoarthritis: The IDEA randomized clinical trial. JAMA J Am Med Assoc. (2013) 310:1263–73. doi: 10.1001/jama.2013.277669
25. Lindqvist HM, Gjertsson I, Eneljung T, Winkvist A. Influence of blue mussel (Mytilus edulis) intake on disease activity in female patients with rheumatoid arthritis: The MIRA randomized cross-over dietary intervention. Nutrients. (2018) 10:481. doi: 10.3390/nu10040481
26. Pirouzpanah S, Mahboob S, Sanayei M, Hajaliloo M, Safaeiyan A. The effect ofchamomile tea consumption on inflammation among rheumatoid arthritis patients: Randomized clinical trial. Prog Nutr. (2017) 19:27–33.
27. Thimóteo NSB, Iryioda TMV, Alfieri DF, Rego BEF, Scavuzzi BM, Fatel E, et al. Cranberry juice decreases disease activity in women with rheumatoid arthritis. Nutrition. (2019) 60:112–7. doi: 10.1016/j.nut.2018.10.010
28. Schumacher HR, Pullman-Mooar S, Gupta SR, Dinnella JE, Kim R, McHugh MP. Randomized double-blind crossover study of the efficacy of a tart cherry juice blend in treatment of osteoarthritis (OA) of the knee. Osteoarthr Cartil. (2013) 21:1035–41. doi: 10.1016/j.joca.2013.05.009
29. Hashempur MH, Sadrneshin S, Mosavat SH, Ashraf A. Green tea (Camellia sinensis) for patients with knee osteoarthritis: A randomized open-label active-controlled clinical trial. Clin Nutr. (2018) 37:85–90. doi: 10.1016/j.clnu.2016.12.004
30. Schell J, Hal Scofield R, Barrett JR, Kurien BT, Betts N, Lyons TJ, et al. Strawberries improve pain and inflammation in obese adults with radiographic evidence of knee osteoarthritis. Nutrients. (2017) 9:949. doi: 10.3390/nu9090949
31. Di Lorenzo C, Coppola G, Sirianni G, Di Lorenzo G, Bracaglia M, Di Lenola D, et al. Migraine improvement during short lasting ketogenesis: A proof-of-concept study. Eur J Neurol. (2015) 22:170–7. doi: 10.1111/ene.12550
32. Veronese N, Stubbs B, Noale M, Solmi M, Luchini C, Maggi S. Adherence to the mediterranean diet is associated with better quality of life: Data from the osteoarthritis initiative. Am J Clin Nutr. (2016) 104:1403–9. doi: 10.3945/ajcn.116.136390
33. Shmagel A, Onizuka N, Langsetmo L, Vo T, Foley R, Ensrud K, et al. Low magnesium intake is associated with increased knee pain in subjects with radiographic knee osteoarthritis: Data from the osteoarthritis initiative. Osteoarthr Cartil. (2018) 26:651–8. doi: 10.1016/j.joca.2018.02.002
34. Lourdudoss C, Di Giuseppe D, Wolk A, Westerlind H, Klareskog L, Alfredsson L, et al. Dietary intake of polyunsaturated fatty acids and pain in spite of inflammatory control among methotrexate-treated early rheumatoid arthritis patients. Arthritis Care Res. (2018) 70:205–12. doi: 10.1002/acr.23245
35. Bimbela Pedrola JL, Gorrotxategi Larrea M. Tools to improve patient adherence. Granada: Andalusian School of Public Health (2006).
36. Brain K, Burrows TL, Bruggink L, Malfliet A, Hayes C, Hodson FJ, et al. Diet and chronic non-cancer pain: The state of the art and future directions. J Clin Med. (2021) 10:5023. doi: 10.3390/jcm10215203
37. Clinton CM, O’Brien S, Law J, Renier CM, Wendt MR. Whole-foods, plant-based diet alleviates the symptoms of osteoarthritis. Arthritis. (2015) 2015:708152. doi: 10.1155/2015/708152
38. Kaartinen K, Lammi K, Hypen M, Nenonen M, Hänninen O. Vegan diet alleviates fibromyalgia symptoms. Scand J Rheumatol. (2000) 29:308–13. doi: 10.1080/030097400447697
Keywords: chronic pain, diet, feeding, nutrients, nutrition, supplements
Citation: Xu Lou I, Gil-García E, Cáceres-Matos R, Ali K and Molina E (2022) Nutritional aspects in chronic non-cancer pain: A systematic review. Front. Nutr. 9:931090. doi: 10.3389/fnut.2022.931090
Received: 28 April 2022; Accepted: 18 July 2022;
Published: 08 August 2022.
Edited by:
Maurizio Muscaritoli, Sapienza University of Rome, ItalyReviewed by:
Joeri Pen, UZ Brussel, BelgiumCopyright © 2022 Xu Lou, Gil-García, Cáceres-Matos, Ali and Molina. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rocío Cáceres-Matos, cmNhY2VyZXMzQHVzLmVz
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.