 Mônica Araujo Batalha1
Mônica Araujo Batalha1 Paula Normando dos Reis Costa1
Paula Normando dos Reis Costa1 Ana Lorena Lima Ferreira1
Ana Lorena Lima Ferreira1 Nathalia C. Freitas-Costa1
Nathalia C. Freitas-Costa1 Amanda C. Cunha Figueiredo1
Amanda C. Cunha Figueiredo1 Setareh Shahab-Ferdows2
Setareh Shahab-Ferdows2 Daniela Hampel2,3
Daniela Hampel2,3 Lindsay H. Allen2,3
Lindsay H. Allen2,3 Rafael Pérez-Escamilla4
Rafael Pérez-Escamilla4 Gilberto Kac1*
Gilberto Kac1*- 1Nutritional Epidemiology Observatory, Josué de Castro Nutrition Institute, Rio de Janeiro Federal University, Rio de Janeiro, Brazil
- 2United States Department of Agriculture/Agricultural Research Service, Western Human Nutrition Research Center, Davis, CA, United States
- 3Department of Nutrition, University of California, Davis, Davis, CA, United States
- 4Department of Social and Behavioral Sciences, Yale School of Public Health, New Haven, CT, United States
Background: Little is known regarding the association between mental health distress during pregnancy and postpartum maternal serum biomarkers of vitamin B-12 status and milk B-12 concentration.
Objective: To evaluate the association between depressive and anxiety symptoms in the third trimester of pregnancy and changes in postpartum serum B-12, homocysteine, and B-12 milk concentration.
Methods: A total of 101 women (18–40 years) were studied in a prospective cohort with data at the third trimester of pregnancy (baseline) and three postpartum time-points (TPs): 2–8 days (TP1), 28–50 days (TP2), and 88-119 days (TP3) postpartum. B-12 concentrations in milk were measured by competitive chemiluminescent enzyme immunoassay at TP1, TP2, and TP3. Serum B-12 and homocysteine concentrations were evaluated at baseline, TP1, TP2, and TP3 by chemiluminescent immunoassays. Depressive and anxiety symptoms were measured with the Edinburgh Postnatal Depression Scale and the State-Trait Anxiety Inventory at baseline. Spearman's correlation test and multiple linear mixed-effect models were performed.
Results: The prevalence of depressive and anxiety state symptoms was 35.6 and 39.6% at baseline. High prevalence of low milk B-12 concentration (<310 pmol/L) were observed at TP1 (53.2%), TP2 (71.4%), and TP3 (71.1%). Women with anxiety symptoms at baseline presented higher median concentrations of serum homocysteine at TP1 and lower concentrations of serum and milk B-12 at TP2 compared with women without anxiety symptoms [8 (7; 9) vs. 6 (5; 8) and 266 (188; 369) vs. 332 (272; 413)]. Milk B-12 concentrations were positively and significantly correlated with maternal serum B-12 concentrations at different TP. Women with anxiety symptoms at baseline exhibited a decrease in daily postpartum homocysteine concentrations compared to women without anxiety symptoms (β = −0.002, SE = 0.001, p = 0.024).
Conclusion: Anxiety symptoms at the end of pregnancy were associated with longitudinal changes in maternal serum homocysteine concentrations during the first 3 months postpartum.
Introduction
Vitamin B12 (B-12) is an essential nutrient for maternal and child health. It participates as a cofactor in various metabolic processes, including the one-carbon cycle, which is essential for synthesizing DNA and amino acids (1, 2). Women of childbearing age, infants, and young children are included in the group at higher risk for B-12 insufficiency (3, 4). B-12 deficiency during pregnancy has been linked to adverse gestational outcomes (e.g., preterm birth and low birth weight) and could impact the infants' fetal storage of this vitamin (3, 5–7).
There is substantial interest in the relationship between maternal nutrition and maternal mental health in the perinatal period (8). Some studies have linked inadequate intake and low-status biomarkers of folate and B-12, vitamins involved in the one-carbon cycle, in subjects with depressive and anxiety symptoms (9–12). However, these studies were cross-sectional and mixed results were observed (4, 10). B-12 has hematological and neurological functions and is required for S-adenosylmethionine (SAM) synthesis (4), while SAM has anti-depressive properties, as it plays a role in synthesizing neurotransmitters (13). Some studies have demonstrated that B-12 deficiency status could impair SAM synthesis and raise homocysteine levels, thus being related to anxiety and depressive symptoms (14, 15). Homocysteine is a sulfur-containing amino acid formed during the methionine metabolism that also plays a role in neurotransmitter synthesis (16, 17). Hyperhomocysteinemia has been linked to both depression and cardiovascular disease, although results remain inconsistent (17).
Mental health disorders have been linked to micronutrient deficiencies, including B-12 deficiency, as they could contribute to unhealthy lifestyles (18–20), however, this relationship has been less investigated. Thus, this area is of major clinical and public health concern, given the high prevalence of mental health disorders during pregnancy in low- and middle-income countries, in which the prevalence of prenatal depression is around 25.8% (21). In addition, anxiety symptoms seem to increase through pregnancy trimesters, and a prevalence of approximately 24.6% had been self-reported in the third trimester (22).
Perinatal depressive and anxiety are related to several undesirable maternal and child health outcomes, such as poor dietary intake, increased incidence of preterm birth, low Apgar score, and could have a negative impact on breastfeeding practices (19, 23, 24). However, few studies have assessed the association of maternal mental health with human milk composition. Previous studies have focused on mental health disorders during the postpartum period concerning hormones and immunological factors in milk as a physiological response to stress (23, 25). Nevertheless, the relationship between maternal mental health during pregnancy and postpartum B-12 and homocysteine concentration is not well-established, and little is known about their association with milk B-12 concentration. This study tests the primary hypotheses that depressive or anxiety symptoms during the third trimester of pregnancy are associated with changes in maternal serum B-12 and homocysteine concentrations and milk B-12 concentrations during the postpartum period. Additionally, we tested if (1) medians of serum B-12 and homocysteine concentrations and milk B-12 concentrations were different according to maternal mental health status; (2) milk B-12 concentrations are positively correlated with maternal serum B-12 and negatively correlated with maternal homocysteine concentrations.
Materials and Methods
Women and their infants participating in this prospective cohort study received perinatal care at a public health center located in a lower-income community in Rio de Janeiro, Brazil. The study data were collected between January 2017 and January 2020. Eligibility criteria comprised pregnant mothers between 28 and 35 gestational weeks; between 18 and 40 y; with no known infectious or chronic non-communicable diseases (except obesity); singleton pregnancy; and residence in the catchment area of the public health center.
A non-probabilistic sample of 147 pregnant women was enrolled during the study baseline when women were between 28 and 35 weeks of gestation. Subsequently, eight women and their children were excluded due to stillbirth, pre-term birth, or developing a chronic or infectious disease before delivery. As a result, 139 women were followed at five follow-up visits that happened at the following time points (TPs) postpartum: 2–8 days (TP1), 28–50 days (TP2), 88–119 days (TP3), 6 months (TP4), and 12 mo (TP5). The TP postpartum visits were defined considering the routine of maternal and infant health care preconized by the Brazilian Health Ministry. Some refused to answer mental health questionnaires (n = 4) or collect blood/milk biological samples (n = 34). Therefore, we analyzed data from the subsample of 101 women for which we had mental health data and postpartum biological (blood or milk) samples for at least TP1, TP2, and TP3 (Supplementary Figure 1).
Maternal Mental Health
Depressive symptoms were measured at the baseline with the Edinburgh Postnatal Depression Scale (EPDS), the most common screening tool used in the perinatal period (26, 27). EPDS is a 10-item screening questionnaire that assesses depressive symptoms over the preceding 7 days (28, 29). Each item in this scale has four possible answers with qualitative frequency options (e.g., yes, most of the time, or not at all). The options range from 0 to 3, with a maximum score of 30. We classified the participants as with (EPDS ≥11) or without (EPDS <11) depressive symptoms at baseline.
Anxiety symptoms were measured at the baseline with the Spielberger State-Trait Anxiety Inventory (STAI) which evaluates anxiety traits and a state, two different anxiety types (30). The anxiety trait refers to stable and relatively permanent personality characteristics. The anxiety state refers to a transitory emotional state concerning a specific period. The STAI consists of 40 items separated into two distinct subscales of 20 items each, with Likert-type response options ranging from 1 to 4. The total STAI score for each subscale (state-anxiety and trait-anxiety) ranges from 20 to 80 (30). In the present study, we used an anxiety state to evaluate the anxiety related to the specific moment of pregnancy (in the third trimester). We classified the participants as with (STAI ≥40) or without (STAI <40) anxiety symptoms.
The EPDS and STAI instruments were validated for use in the pregnancy and postnatal periods (29, 31). The cross-cultural adaptation of STAI comprised four steps previously described (32), and then, the instrument was translated and adapted for use in Brazil (33). The Portuguese version of EPDS was validated in a study conducted by Santos et al. (34).
Maternal Serum B-12 and Homocysteine
After an 8-12 h overnight fast, maternal blood samples were collected at baseline, TP1, TP2, and TP3. The samples were collected in tubes with separator gel and centrifuged within 1 h of blood collection. Serum was separated into aliquots of 1 ml and stored at −80°C until analysis. Serum B-12 concentrations were analyzed by chemiluminescent immunoassays in an automated system (UniCel DxI 800, Beckman Coulter, Brea, USA), and homocysteine concentrations were analyzed by chemiluminescent immunoassays in an Abbott Alinity i (Abbott Diagnostics, Chicago, USA). B-12 deficient status was defined as serum level <148 pmol/L (35) and serum homocysteine >15 μmol/L was defined as hyperhomocysteinemia (36). These cut points were only used to characterize the participants' status in the postpartum period, as they overestimate the actual prevalence of B-12 deficiency in pregnancy (4). In our models, serum B-12 and homocysteine were used as continuous variables.
Human Milk Collection and Milk B-12 Concentration Analysis
Following procedures established by the Brazilian Network of Human Milk Banks protocol (37), we instructed women breastfeeding on-demand to collect milk samples at TP1, TP2, and TP3, as previously described (38). The participants collected milk, preferably in the morning after breakfast (until ~10:00 am), considering that the concentrations of B vitamins in milk exhibit little or no diurnal variation (39). The milk samples were collected from the same breast through hand expression because a pump could be a potential risk of contamination. Before starting the collection, the participants were asked to wash their hands and put on masks to protect their face and head coverings to avoid possible sample contamination during the process. The trained interviewer also used the same hygiene procedures because, if necessary, they helped the participant with the milk sample extraction using nitrile gloves.
In total, 5 ml of milk was collected from each participant at TP1 and 17 ml at TP2 and TP3. The samples were expressed directly into 50 ml sterile, ribonuclease (RNase)-free, deoxyribonuclease (DNase)-free, and non-pyrogenic tubes. Although the breast was not fully emptied, previous studies have shown that the concentrations of water-soluble vitamins in milk remain relatively stable during the feeding episode (hind or foremilk) (39). The samples were homogenized and aliquoted immediately after collection. One aliquot of 1 ml at each visit was used for B-12 analyses. The samples were frozen at −20°C and then transported in a temperature-controlled box (−1 to −5°C) to Rio de Janeiro Federal University and stored at −80°C. For analysis, the frozen samples were shipped on dry ice to the USDA/ARS-Western Human Nutrition Research Center, Davis, CA, USA. Milk B-12 was analyzed using the Siemens IMMULITE 1000 competitive chemiluminescent enzyme immunoassay (coefficient of variation: 8.5%) as previously described (40). To evaluate the prevalence of low B-12 milk concentration, we consider a cutoff of <310 pmol/L proposed by Williams et al. (41). In our models, milk B-12 was used as a continuous variable.
Covariates
A structured questionnaire was administered at baseline to collect socio-economic and demographic data, such as maternal age (years), education (schooling years), marital status (with and without a partner), and parity (primiparous/multiparous). Breastfeeding status was defined as exclusive and predominant (42). Exclusive breastfeeding means no other food or drink, not even water, except human milk for the first 6 months of life, except for rehydration solution, drops, and syrups (vitamins, minerals, and medicines). Predominant breastfeeding means that the infant's primary source of nourishment is human milk; however, the infant may also have received liquids (including water or water-based drinks and fruit juice), ritual fluids, and medicines (42).
Serum folate concentrations (ng/ml) were analyzed by chemiluminescent immunoassay in an automated system UniCel DxI 800 (Beckman Coulter, Brea, USA).
The interviewers were trained to measure height in duplicate using a stadiometer (Altura Exata, Belo Horizonte, Brazil) at TP2. When the measurements of height differed by >0.5 cm, a third measurement was performed, and the mean of the two more similar measurements was used. The self-reported pre-pregnancy weight was used to calculate the pre-pregnancy BMI (kg/m2); women were classified according to the WHO cutoffs (43) as underweight (<18.5 kg/m2), normal (≥18.5 and <25.0 kg/m2), overweight (≥25.0 and <30.0 kg/m2), or obese (≥30 kg/m2).
Statistical Analyses
The distribution of continuous variables was assessed using histograms, kurtosis, and skewness measurements. We used absolute (n) and relative frequencies (%) for categorical variables and median and interquartile range (IQR) for continuous variables to describe maternal characteristics, blood biomarkers, and milk B-12 concentrations. We compared the characteristics of women with and without biological samples using the Mann–Whitney, Chi-square, and Fisher's exact tests.
The Mann–Whitney test was performed to compare maternal serum B-12, homocysteine, and milk B-12 median concentrations, at each visit, between women with or without anxiety and depressive symptoms. The Spearman's rank correlation test was performed to investigate correlations between maternal B-12 and serum homocysteine concentrations during pregnancy and lactation and milk B-12 at TP1, TP2, and TP3. The correlations were interpreted as weak (0.00 to 0.39), moderate (0.40 to 0.69), strong (0.70 to 0.89), and very strong (0.90 to 1.00) (44).
Unadjusted and adjusted longitudinal linear mixed-effects models were performed using baseline anxiety or depressive symptom scores as interaction terms. These models were performed to evaluate whether maternal mental health (exposures) were associated with daily postpartum changes in serum B-12 and homocysteine and milk B-12 concentrations (outcomes). Considering that our outcomes were skewed, the regression models used log-transformed variables. We performed diagnostic plots to check for violations of the model's assumptions; residual plots were used to assess the linearity and homoscedasticity. Quantile-quantile plots were used to check the normality of the residuals and random effects.
All the models were adjusted for specific confounders selected from previously published studies. The models in which postpartum serum B-12 and homocysteine were the outcomes were adjusted for maternal age, education, pre-pregnancy BMI, B-vitamin supplement intake during pregnancy (including folate), and serum folate concentration in the third trimester of pregnancy. The model in which postpartum milk B-12 was the outcome was adjusted for pre-pregnancy BMI, B-vitamin supplement intake during pregnancy (including folate), and serum B-12 concentration in the third trimester of pregnancy. The associations were considered statistically significant when p-values were <0.05. Statistical analyses were performed using Stata version 15 (StataCorp) and R version 4.0.3.
Results
The median maternal age was 26 (IQR: 22–31) years, and 44.7% of the participants were classified as pre-pregnancy overweight or obese. The prevalence of depressive and anxiety state symptoms was 35.6 and 39.6% at baseline, respectively. The prevalence of B-12 deficient status (<148 pmol/L) at TP1 was 27.3% and 3.9% at TP2, and no case of hyperhomocysteinemia (>15 μmol/L) was observed during the postpartum period. The prevalence of low milk B-12 concentrations (<310 pmol/L) was 53.2% at TP1, 71.4% at TP2, and 71.1% at TP3, respectively (Table 1). The participants with and without biological (milk and blood) samples were not statistically different when comparing socio-economic, demographic, and biomedical characteristics at baseline (Supplementary Table 1).
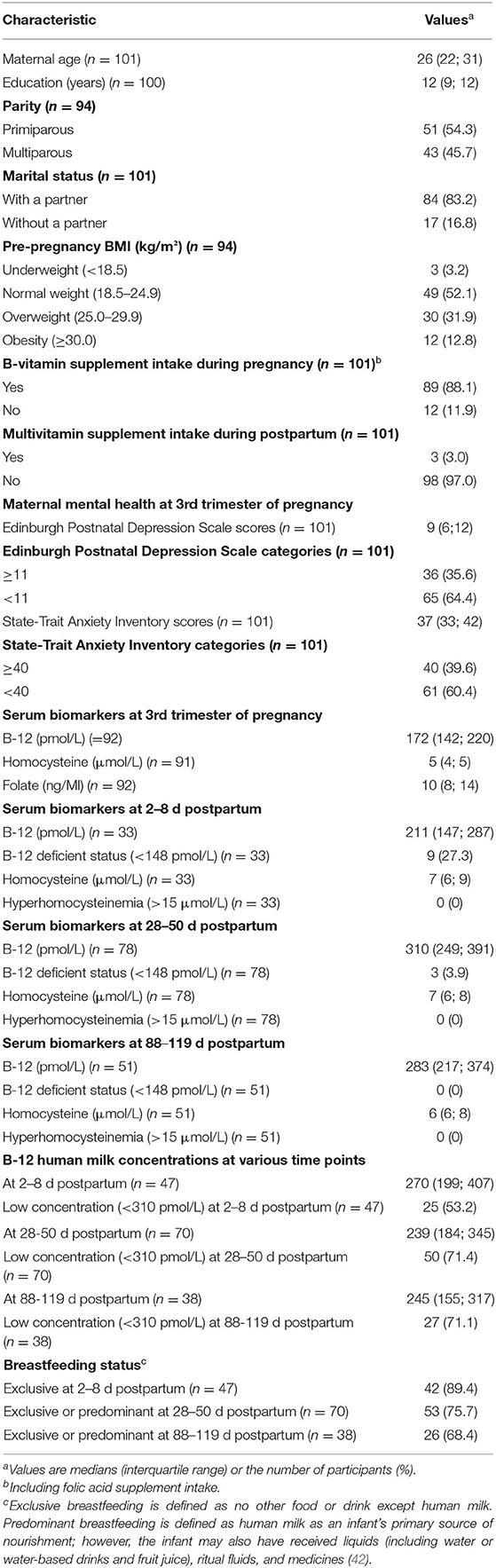
Table 1. Characteristics, biomarkers, and human milk concentrations of participants followed in the cohort in Rio de Janeiro, Brazil.
Women with anxiety symptoms in the third trimester of pregnancy presented higher median serum homocysteine concentrations at 2–8 days postpartum and lower median concentration of maternal serum and milk B-12 at 28-45 days postpartum compared with women without anxiety symptoms [8 (7; 9) vs. 6 (5; 8), p = 0.03 and 266 (188; 369) vs. 332 (272; 413), p = 0.02]. No difference was observed in serum B-12, homocysteine, and B-12 milk concentration between women with and without depressive symptoms at baseline (Figure 1).
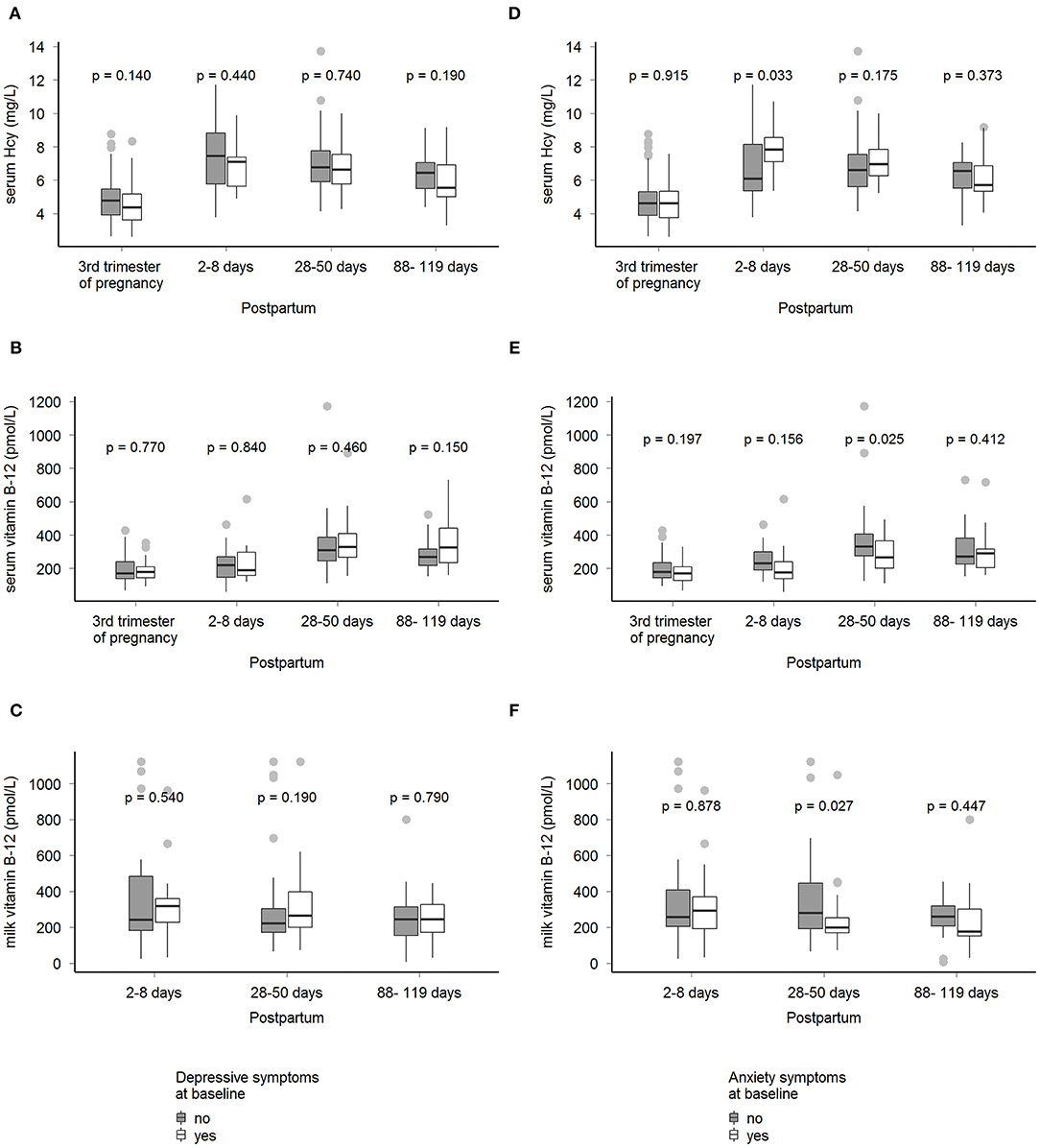
Figure 1. Median concentrations of serum B-12, serum homocysteine, and milk B-12 by maternal mental health status in Rio de Janeiro, Brazil. Mann–Whitney's test was performed to compare medians (IQR) of biological samples (serum vitamin B-12, serum homocysteine, and milk vitamin B-12) at the 3rd trimester of pregnancy, 2-8 d, 28-50 d, and 88-119 d postpartum between women with and without depressive or anxiety symptoms at 3rd trimester of pregnancy (baseline), p < 0.05. Depressive symptoms were assessed by the Edinburgh Postnatal Depression Scale (EPDS), yes (EPDS ≥11, n = 36) and no (EPDS <11, n = 65) (A–C). Anxiety state was assessed by the State-Trait Anxiety Inventory (STAI), yes (STAI ≥40, n = 40), and no (STAI <40, n = 61) (D–F). Hcy, homocysteine.
Correlation Between Serum B-12 and Homocysteine Concentrations and Milk B-12 Concentration
The correlations varied between low and moderate. Milk B-12 concentrations at TP1 were positively and significantly correlated with serum B-12 concentrations at baseline (ρ = 0.39, p < 0.01) and at TP1 (ρ = 0.64, p < 0.01). Milk B-12 concentrations at TP2 were positively and significantly correlated with serum B-12 concentrations at TP1 (ρ = 0.44, p = 0.03). Milk B-12 concentrations at TP2 were positively and significantly correlated with serum B-12 levels at TP1 (ρ = 0.44, p =0.03) and were negatively and significantly correlated with homocysteine at TP2 (ρ = −0.34, p =0.01). Milk B-12 concentrations at TP3 were positively and significantly correlated with serum B-12 levels at TP1 (ρ = 0.64, p = 0.02), at TP2 (ρ= 0.48, p =0.01), and at TP3 (ρ = 0.39, p = 0.02) (data not shown).
Maternal Mental Health and Changes in the Serum B-12 and Homocysteine, and Milk B-12 Concentrations
The presence of depressive symptoms in the third trimester of pregnancy was not associated with daily postpartum changes in maternal serum B-12, homocysteine, and milk B-12 concentrations (Figure 2 and Table 2). However, women with anxiety symptoms in the third trimester exhibited a decrease in daily postpartum homocysteine concentrations compared to women without anxiety symptoms (β = −0.002 (SE = 0.001), p = 0.035), even after adjusting for maternal age, education, pre-pregnancy BMI, B-vitamin supplement intake during pregnancy, and serum folate concentration at the third trimester of pregnancy (β = −0.002 (SE = 0.001), p = 0.024) (Figure 3 and Table 3).
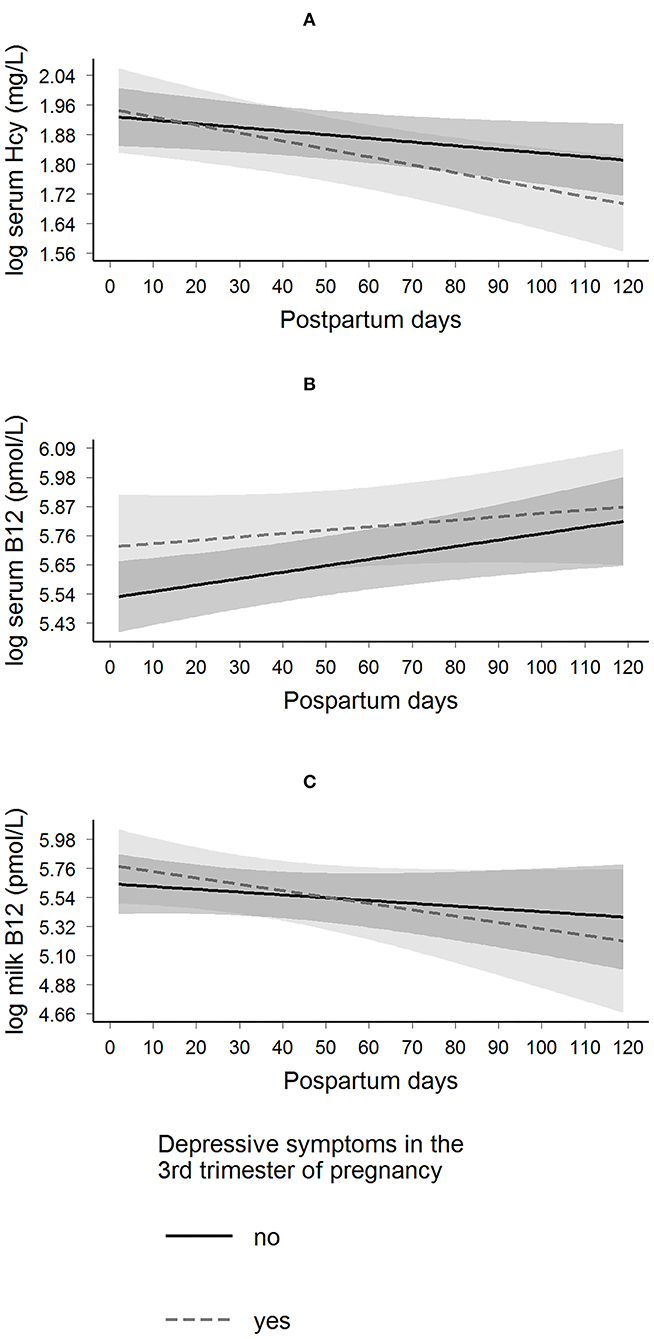
Figure 2. Longitudinal predictions of maternal serum homocysteine, serum B-12, and milk B-12 concentrations according to the presence of depressive symptoms in the 3rd trimester of pregnancy in Rio de Janeiro, Brazil. β Coefficient interactions (βinteraction) and standard error (SE) were estimated. These parameters were used to evaluate the changes of having depressive symptoms on the trajectory of each biological sample. Depressive symptoms were assessed by the Edinburgh Postnatal Depression Scale (EPDS), yes (EPDS ≥11, n = 36) and no (EPDS <11, n = 65). (A) Log serum homocysteine: βinteraction = −0.001 (0.001); p = 0.194, and the model was adjusted for maternal age, education, pre-pregnancy BMI, B-vitamin (including folate) supplement intake during pregnancy, and serum folate concentration at the 3rd trimester of pregnancy. (B) Log serum B-12: βinteraction = −0.001 (0.002); p = 0.445, and the model was adjusted for maternal age, education, pre-pregnancy BMI, B-vitamin (including folate) supplement intake during pregnancy, and serum folate concentration at the 3rd trimester of pregnancy (C) Log milk-B-12: βinteraction = −0.003 (0.004); p = 0.455, and the model was adjusted for pre-pregnancy BMI, B-vitamin (including folate) supplement intake during pregnancy, and serum B-12 concentration at the 3rd trimester of pregnancy. Hcy, homocysteine.
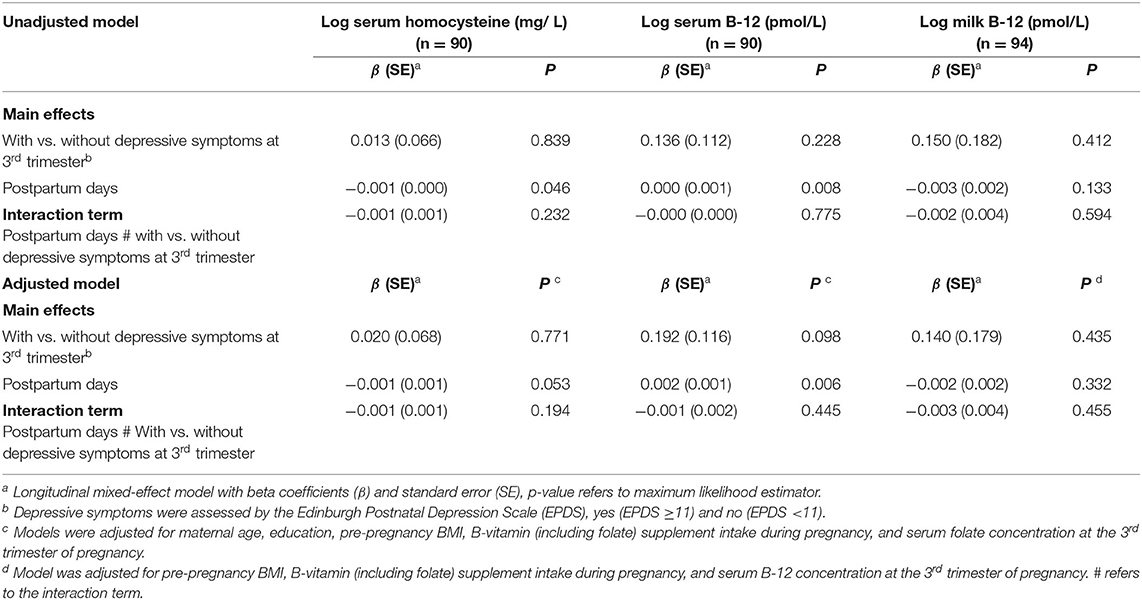
Table 2. Models of longitudinal prediction of serum homocysteine and vitamin B-12 and milk B-12 trajectories based on the presence of depressive symptoms at the 3rd trimester of pregnancy, Rio de Janeiro, Brazil.
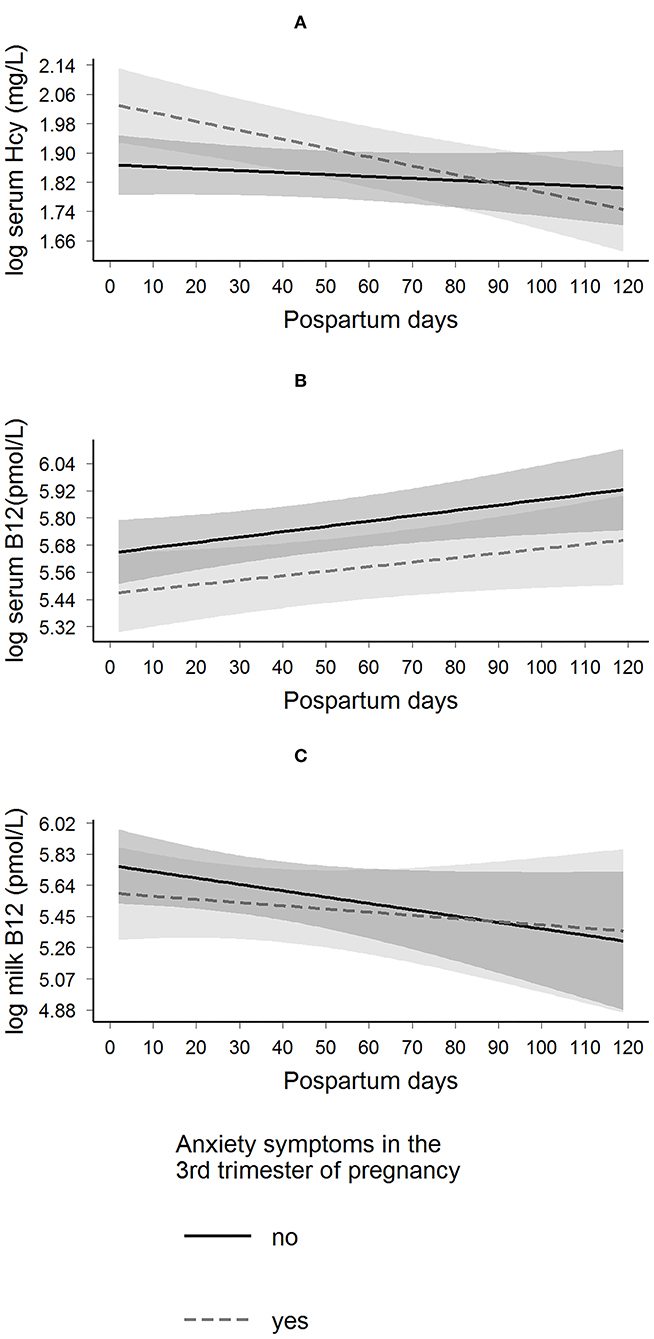
Figure 3. Longitudinal predictions of maternal serum homocysteine, serum B-12, and milk B-12 concentrations according to the presence of anxiety symptoms in the 3rd trimester of pregnancy in Rio de Janeiro, Brazil. β Coefficient interactions (βinteraction) and standard error (SE) were estimated. These parameters were used to evaluate the changes of having anxiety symptoms on the trajectory of each biological sample. Anxiety state was assessed by the State-Trait Anxiety Inventory (STAI), yes (STAI ≥40, n = 40) and no (STAI <40, n = 61). (A) Log serum homocysteine: βinteraction = −0.002 (0.001); p = 0.024, and the model was adjusted for maternal age, education, pre-pregnancy BMI, B-vitamin (including folate) supplement intake during pregnancy, and serum folate concentration at the 3rd trimester of pregnancy. (B) Log serum B-12: βinteraction = −0.000 (0.001); p = 0.797, and the model was adjusted for maternal age, education, pre-pregnancy BMI, B-vitamin (including folate) supplement intake during pregnancy, and serum folate concentration at the 3rd trimester of pregnancy (C) Log milk-B-12: βinteraction = 0.002 (0.004); p = 0.585, and the model was adjusted for pre-pregnancy BMI, B-vitamin (including folate) supplement intake during pregnancy, and serum B-12 concentration at the 3rd trimester of pregnancy. Hcy, homocysteine.
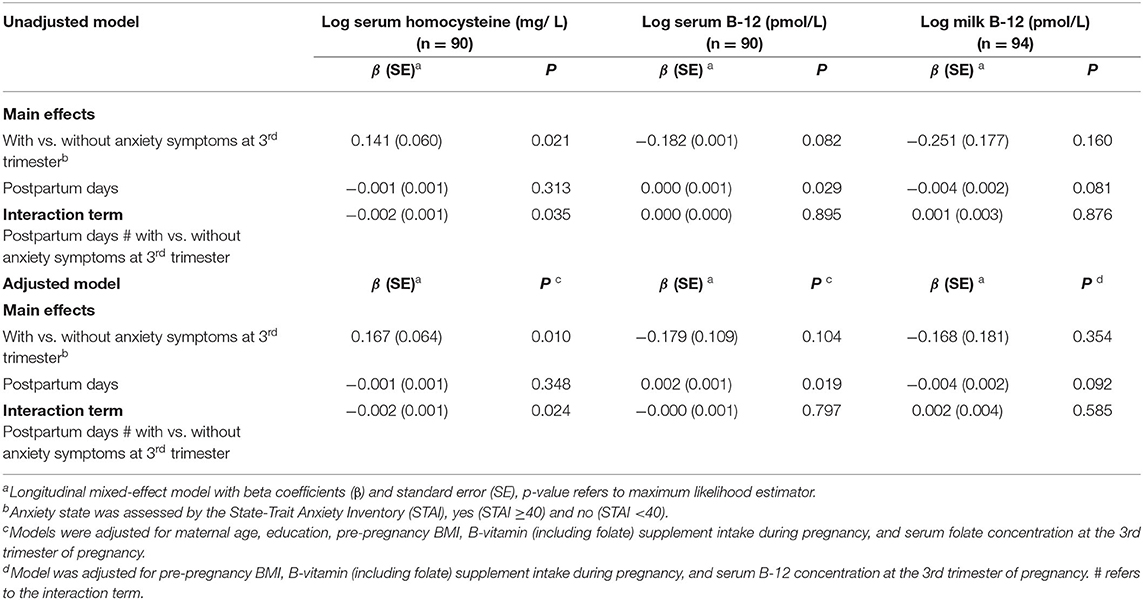
Table 3. Models of longitudinal prediction of maternal serum homocysteine and vitamin B-12 and milk B-12 trajectories based on the presence of anxiety symptoms at the 3rd trimester of pregnancy, Rio de Janeiro, Brazil.
Discussion
Women with anxiety symptoms in the third trimester of pregnancy presented higher median serum homocysteine concentrations at 2–8 postpartum days and lower serum and milk B-12 at 28–45 days compared with women without anxiety symptoms. Women with anxiety symptoms exhibited a decrease in homocysteine concentrations in the first 3 months postpartum compared to women without anxiety symptoms. However, depressive symptoms did not change the postpartum trajectories of the maternal serum B12, homocysteine, and milk B-12 concentrations. Maternal serum B-12 concentration was positively correlated to milk B-12 concentration.
Pregnancy and lactation are characterized by increased nutrient requirements for women; thus, these are considered stages at which women are at higher risk of B-12 insufficiency (4). In addition, serum B-12 concentrations by themselves may not be sufficiently accurate to confirm or refute this assumption; hence other biomarkers have been suggested (4, 45). For example, homocysteine levels have been used as a sensitive marker of folate and B-12 deficiency (46). In countries with mandatory flour fortification with folic acid (such as Brazil), homocysteine is likely to be an accepted biomarker for B-12 deficiency (47). Our study observed lower median concentrations of serum B-12 and homocysteine at the end of pregnancy compared to the postpartum period, which is in line with the literature. A decrease in the B-12 (~25–30%) is expected through pregnancy, which has been assumed to be a normal physiological response (48–50). In addition, previous studies also showed that the homocysteine concentrations could increase during pregnancy; however, pregnant women have lower serum concentrations compared to non-pregnant women (48).
The studies conducted prior to ours' had yielded conflicting conclusions about the relationship between depression and B-12 or homocysteine concentrations (15). Some studies, with adults and elderly individuals, have indicated hyperhomocysteinemia in patients with depression (51, 52), while others did not find any association (53). Data from NHANES 2005–2006 showed that depressive symptoms among participants aged 20–85 years were not associated with homocysteine concentration; nevertheless, they found a positive association when they restricted the analysis to participants older than 50 years. Therefore, age could be a possible path to modifying this relationship (54). In this context, it is also important to highlight that our study sample was comprised of young (18–40 years old) women, without any case of hyperhomocysteinemia, perhaps because most of the women in our sample have taken folic acid supplements during pregnancy.
Even without any case of hyperhomocysteinemia, we observed higher median homocysteine concentrations in the first 2–8 days and lower B-12 concentrations at approximately the 1st month postpartum, respectively, in women with anxiety compared to those without anxiety. The association between B-12 or homocysteine concentration and anxiety is less investigated than this relationship with depression, and few studies were performed during pregnancy or postpartum. Regarding this result, an experimental study observed that the increased homocysteine concentration in rats might be the result of stress-induced depression rather than a cause of depression (55). However, in our study, women with anxiety presented a daily decrease in postpartum homocysteine concentration compared to women without. It is also possible that the strength of the association of maternal mental health at the end of pregnancy over B-12 and homocysteine may be stronger in the 1st days and up to the 1st month postpartum, thereafter mental health could be influenced more strongly by other environmental factors, which could explain the decrease in postpartum homocysteine concentration of women with anxiety symptoms.
There is a paucity of studies evaluating maternal mental health and milk composition. To our knowledge, only one study has previously evaluated the association with vitamin concentrations in human milk (25). That cross-sectional study focused only on vitamin B-6 and postpartum depressive symptoms, used a different instrument, and did not find any association (56). Even though maternal mental health was not associated with changes in the trajectories of postpartum serum and milk B-12 concentrations, we observed lower concentrations of serum and milk B-12 at 28–50 days postpartum in women with anxiety symptoms than women without these symptoms at the end of pregnancy. The manifestation of anxiety at the end of pregnancy may promote unhealthy lifestyles (18–20), and, therefore, it could result in poor B-12 maternal status and, thus, it may contribute to lower B-12 milk concentration.
Our finding regarding the correlation of maternal serum B-12 with milk B-12 concentrations aligns with previous studies that had already reported this relationship; i.e., B-12 status during both pregnancy and lactation is associated with the milk B-12 concentration (57). Similar to our results, Bae et al. (48) reported, based on data from a feeding trial study with 28 lactating women in the US, that milk B-12 concentration was moderately positively correlated with maternal serum B-12 concentration and also tended to be inversely correlated with maternal serum homocysteine at 5 weeks postpartum.
The strengths of this study include its prospective design and the use of blood status biomarker concentrations, which are more accurate and free of the self-reported bias related to the conventional methods of dietary assessments that could under-or overestimate maternal nutritional status. As homocysteine concentration could be impacted by other vitamin deficiencies and pathological conditions, we adjusted our models for serum folate concentration, which could impact homocysteine and B-12 concentrations and maternal mental health, and only included healthy women (without any chronic or infectious diseases) in the study. Besides, none of the participants was taking antidepressants or any medication for anxiety or depression upon enrollment.
We acknowledge that our study has some limitations. Although we adjusted our models for important confounders, we cannot rule out residual confounders by other factors, such as genetic makeup, that may be linked to both maternal mental health distress and B-12 and homocysteine concentrations. Second, although limited empirical evidence has shown that milk vitamin B-12 seems not to vary during the feeding episode, this requires further research as existing data is still conflicting. Thus, we acknowledge that B-12 milk concentration in our study could have been affected as the breast was not fully emptied, and not every child was exclusively breastfed. Finally, our study had a limited sample size and was conducted in only one public health center, limiting the generalization of our findings.
Considering that there is a high prevalence of mental health disorders during pregnancy, particularly in low- and middle-income countries (21), our study contributes evidence on the association of this condition with postpartum blood and milk vitamin B12 concentration, which are important determinants of a child's nutritional status. Vitamin B12 deficiency can start in early infancy due to low fetal storage at birth if the mother is deficient during pregnancy. Deficits can continue or be exacerbated by poor maternal vitamin B12 status during lactation with consequent low amounts of the vitamin in the human milk, increasing the risk of infant short- and long-term outcomes, such as growth and developmental delays (3, 4).
In conclusion, we observed differences in concentrations of serum B-12, homocysteine, and milk B-12 between women with and without anxiety symptoms. Our results support previous studies that showed a positive correlation between maternal serum B-12 and milk B-12 concentration. Additionally, anxiety in the third trimester of pregnancy was associated with changes in postpartum trajectories of serum homocysteine concentration. Thus, our findings suggest that monitoring maternal mental health and the biomarkers of vitamin B12 status could be an essential strategy for better maternal and child nutritional status. However, large randomized clinical trials in populations with a high prevalence of B-12 deficiency are needed to explain better the mechanisms by which maternal mental health disorders could be related to maternal serum and human milk vitamin composition.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Materials, further inquiries can be directed to the corresponding author/s.
Ethics Statement
The studies involving human participants were reviewed and approved by The Research Ethics Committee of the Municipal Health Secretary and Civil Defense of the State of Rio de Janeiro (Protocol number: 49218115.0.0000.5275) and the Maternity School of Rio de Janeiro Federal University (Protocol number: 49218115.0.0000.5275) approved the present study. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
MB, AFe, NF-C, and GK designed and conducted the research. MB analyzed data and performed statistical analysis. MB, PR, AFe, NF-C, AFi, and GK wrote the manuscript's first draft. DH performed analysis of vitamin B-12 in human milk samples. DH, SS-F, LA, and RP-E contributed to interpretation of findings and provided critical evaluation and input into the manuscript. All authors edited the manuscript and read and approved the final manuscript.
Funding
The National Council for Scientific and Technological Development (CNPq in the Portuguese acronym; grant number: 409676/2016), the Carlos Chagas Filho Foundation for Research Support of Rio de Janeiro State (FAPERJ, grant number: E-26/210.190/2014), and intramural USDA-Agricultural Research Service project 5306-51000-004-00D funded the study. GK received a research productivity scholarship from CNPq. This study was also funded in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brasil (CAPES in the Portuguese acronym) - Finance Code 001.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We are grateful to all the women who participated in this study.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnut.2022.923569/full#supplementary-material
References
1. Rush EC, Katre P, Yajnik CS. Vitamin B12: one carbon metabolism, fetal growth and programming for chronic disease. Eur J Clin Nutr. (2014) 68:2–7. doi: 10.1038/ejcn.2013.232
2. Finkelstein JL, Layden AJ, Stover PJ. Vitamin B-12 and perinatal health. Adv Nutr. (2015) 6:552–63. doi: 10.3945/an.115.008201
3. Allen LH. Vitamin B 12 metabolism and status during pregnancy, lactation and infancy. Nutrient regulation during pregnancy, lactation, and infant growth. Adv Exp Med Biol. (1994) 352:173–86. doi: 10.1007/978-1-4899-2575-6_14
4. Allen LH, Miller JW, De Groot L, Rosenberg IH, Smith AD, Refsum H, Raiten DJ. Biomarkers of Nutrition for Development (BOND): vitamin B-12 review. J Nutr. (2018) 148:1995S−2027S. doi: 10.1093/jn/nxy201
5. Allen L. Maternal micronutrient malnutrition: effects on breast milk and infant nutrition, and priorities for intervention. SCN news. (1994) 11:21–4.
6. Rogne T, Tielemans MJ, Chong MF-F, Yajnik CS, Krishnaveni GV, Poston L, et al. Maternal vitamin B12 in pregnancy and risk of preterm birth and low birth weight: a systematic review and individual participant data meta-analysis. Am J Epidemiol. (2017) 185:212–23. doi: 10.1093/aje/kww212
7. Behere RV, Deshmukh AS, Otiv S, Gupte MD, Yajnik CS. Maternal Vitamin B12 status during pregnancy and its association with outcomes of pregnancy and health of the offspring: a systematic review and implications for policy in India. Front Endocrinol (Lausanne). (2021) 12:619176. doi: 10.3389/fendo.2021.619176
8. Khan R, Waqas A, Bilal A, Mustehsan ZH, Omar J, Rahman A. Association of maternal depression with diet: a systematic review. Asian J Psychiatr. (2020) 52:102098. doi: 10.1016/j.ajp.2020.102098
9. Chong MF, Wong JX, Colega M, Chen L-W, van Dam RM, Tan CS, et al. Relationships of maternal folate and vitamin B12 status during pregnancy with perinatal depression: the GUSTO study. J Psychiatr Res. (2014) 55:110–6. doi: 10.1016/j.jpsychires.2014.04.006
10. Sparling TM, Nesbitt RC, Henschke N, Gabrysch S. Nutrients and perinatal depression: a systematic review. J Nutr Sci. (2017) 6:e61. doi: 10.1017/jns.2017.58
11. Peppard L, Oh KM, Gallo S, Milligan R. Risk of depression in pregnant women with low-normal serum Vitamin B12. Res Nurs Health. (2019) 42:264–72. doi: 10.1002/nur.21951
12. Dhiman P, Pillai RR, Wilson AB, Premkumar N, Bharadwaj B, Ranjan VP, et al. Cross-sectional association between vitamin B12 status and probable postpartum depression in Indian women. BMC Pregnancy Childbirth. (2021) 21:146. doi: 10.1186/s12884-021-03622-x
13. Mischoulon D, Fava M. Role of S-adenosyl-L-methionine in the treatment of depression: a review of the evidence. Am J Clin Nutr. (2002) 76:1158S-61S. doi: 10.1093/ajcn/76.5.1158S
14. Folstein M, Liu T, Peter I, Buel J, Arsenault L, Scott T, et al. The homocysteine hypothesis of depression. Am J Psychiatry. (2007) 164:861–7. doi: 10.1176/ajp.2007.164.6.861
15. Moradi F, Lotfi K, Armin M, Clark CC, Askari G, Rouhani MH. The association between serum homocysteine and depression: a systematic review and meta-analysis of observational studies. Eur J Clin Invest. (2021) 51:e13486. doi: 10.1111/eci.13486
16. Moretti R, Caruso P. The controversial role of homocysteine in neurology: from labs to clinical practice. Int J Mol Sci. (2019) 20:231. doi: 10.3390/ijms20010231
17. Zaric BL, Obradovic M, Bajic V, Haidara MA, Jovanovic M, Isenovic ER. Homocysteine and hyperhomocysteinaemia. Curr Med Chem. (2019) 26:2948-61. doi: 10.2174/0929867325666180313105949
18. Barker ED, Kirkham N, Ng J, Jensen SK. Prenatal maternal depression symptoms and nutrition, and child cognitive function. Br J Psychiatry. (2013) 203:417–21. doi: 10.1192/bjp.bp.113.129486
19. Saeed A, Raana T, Saeed AM, Humayun A. Effect of antenatal depression on maternal dietary intake and neonatal outcome: a prospective cohort. J Nutr. (2015) 15:1–9. doi: 10.1186/s12937-016-0184-7
20. Boutté AK, Turner-McGrievy GM, Wilcox S, Liu J, Eberth JM, Kaczynski AT. Associations of maternal stress and/or depressive symptoms with diet quality during pregnancy: a narrative review. Nutr Rev. (2021) 79:495–517. doi: 10.1093/nutrit/nuaa019
21. Gelaye B, Rondon MB, Araya R, Williams MA. Epidemiology of maternal depression, risk factors, and child outcomes in low-income and middle-income countries. Lancet Psychiatry. (2016) 3:973–82. doi: 10.1016/S2215-0366(16)30284-X
22. Dennis CL, Falah-Hassani K, Shiri R. Prevalence of antenatal and postnatal anxiety: Systematic review and meta-analysis. Br J Psychiatry. (2017) 210:315–23. doi: 10.1192/bjp.bp.116.187179
23. Fallon V, Groves R, Halford JCG, Bennett KM, Harrold JA. Postpartum anxiety and infant-feeding outcomes: a systematic review. J Hum Lact. (2016) 32:740–58. doi: 10.1177/0890334416662241
24. Coo S, García MI, Mira A, Valdés V. The role of perinatal anxiety and depression in breastfeeding practices. Breastfeeding Med. (2020) 15:495–500. doi: 10.1089/bfm.2020.0091
25. Di Benedetto MG, Bottanelli C, Cattaneo A, Pariante CM, Borsini A. Nutritional and immunological factors in breast milk: a role in the intergenerational transmission from maternal psychopathology to child development. Brain Behav Immun. (2020) 85:57–6. doi: 10.1016/j.bbi.2019.05.032
26. Hewitt CE, Gilbody SM, Mann R, Brealey S. Instruments to identify post-natal depression: which methods have been the most extensively validated, in what setting and in which language? Int J Psychiatry Clin Pract. (2010) 14:72–6. doi: 10.3109/13651500903198020
27. O'Connor E, Rossom RC, Henninger M, Groom HC, Burda BU. Primary care screening for and treatment of depression in pregnant and postpartum women: evidence report and systematic review for the US preventive services task force. JAMA. (2016) 315:388–406. doi: 10.1001/jama.2015.18948
28. Cox JL, Holden JM, Sagovsky R. Detection of postnatal depression: development of the 10-item Edinburgh postnatal depression scale. Br J Psychiatry. (1987) 150:782–6. doi: 10.1192/bjp.150.6.782
29. Murray D, Cox JL. Screening for depression during pregnancy with the Edinburgh depression scale (EDDS). J Reprod Infant Psychol. (1990) 8:99–107. doi: 10.1080/02646839008403615
30. Spielberger CD, Gorsuch R, Lushene R, Vagg P, Jacobs G. State-Trait Anxiety Inventory. Palo Alto CA: Mind Garden (1983).
31. Tendais I, Costa R, Conde A, Figueiredo B. Screening for depression and anxiety disorders from pregnancy to postpartum with the EPDS and STAI. Span J Psychol. (2014) 17:E7. doi: 10.1017/sjp.2014.7
32. Biaggio AMB, Natalício L, Spielberger CD. Desenvolvimento e validação de uma forma experimental em português do Inventário de Ansiedade Traço-Estado (IDATE) de Spielberger. Arquivos brasileiros de psicologia aplicada. (1977) 29:31–44.
33. Biaggio A, Natalicio L. Manual para o Inventario de Ansiedade Traço-Estado (IDATE)[State-Trait Anxiety Inventory Manual]. Rio De Janeiro: Centro de Psicologia Aplicada (1979).
34. Santos IS, Matijasevich A, Tavares BF, Barros AJ, Botelho IP, Lapolli C, Magalhães PVdS, Barbosa APPN, Barros FC. Validation of the Edinburgh postnatal depression scale (EPDS) in a sample of mothers from the 2004 Pelotas birth cohort study. Cad Saude Publica. (2007) 23:2577–88. doi: 10.1186/s12888-014-0284-x
35. Institute of Medicine. Dietary Reference Intakes for Thiamin, Riboflavin, Niacin, Vitamin B6, Folate, Vitamin B12, Pantothenic Acid, Biotin, and Choline. Washington (DC): National Academy Press (1998).
36. Veeranna V, Zalawadiya SK, Niraj A, Pradhan J, Ference B, Burack RC, et al. Homocysteine and reclassification of cardiovascular disease risk. J Am Coll Cardiol. (2011) 58:1025–33. doi: 10.1016/j.jacc.2011.05.028
37. Agência Nacional de. Vigilância Sanitária (ANVISA). Banco de Leite Humano: funcionamento, prevenção e controle de riscos Brasilia. Brazil: ANVISA (2008).
38. Batalha MA, Ferreira AL, Freitas-Costa NC, Figueiredo AC, Carrilho TR, Shahab-Ferdows S, et al. Factors associated with longitudinal changes in B-vitamin and choline concentrations of human milk. Am J Clin Nutr. (2021) 114:1560–73. doi: 10.1093/ajcn/nqab191
39. Allen LH, Hampel D. Water-soluble vitamins in human milk factors affecting their concentration and their physiological significance. Human milk: composition, clinical benefits and future opportunities. Nestle Nutr Inst Workshop Ser. (2019) 90:69–81. doi: 10.1159/000490296
40. Hampel D, Shahab-Ferdows S, Domek JM, Siddiqua T, Raqib R, Allen LH. Competitive chemiluminescent enzyme immunoassay for vitamin B12 analysis in human milk. Food Chem. (2014) 153:60–5. doi: 10.1016/j.foodchem.2013.12.033
41. Williams AM, Chantry CJ, Young SL, Achando BS, Allen LH, Arnold BF, et al. Vitamin B-12 concentrations in breast milk are low and are not associated with reported household hunger, recent animal-source food, or vitamin B-12 intake in women in rural Kenya. J Nutr. (2016) 146:1125–31. doi: 10.3945/jn.115.228189
42. World Health Organization. Indicators for Assessing Infant and Young Child Feeding Practices: Definitions and Measurement Methods. Geneva, Switzerland: WHO (2008).
43. World Health Organization. Maternal Anthropometry and Pregnancy Outcomes: A WHO Collaborative Study. Geneva, Switzerland: WHO (1995).
44. Overholser BR, Sowinski KM. Biostatistics primer: part 2. Nutr Clin Prac. (2008) 23:76–84. doi: 10.1177/011542650802300176
45. Carmel R. Diagnosis and management of clinical and subclinical cobalamin deficiencies: why controversies persist in the age of sensitive metabolic testing. Biochimie. (2013) 95:1047–55. doi: 10.1016/j.biochi.2013.02.008
46. Bottiglieri T. Homocysteine and folate metabolism in depression. Prog Neuro Psychopharmacol Biol Psychiatry. (2005) 29:1103–12. doi: 10.1016/j.pnpbp.2005.06.021
47. Green R, Miller JW. Vitamin B12 deficiency is the dominant nutritional cause of hyperhomocysteinemia in a folic acid-fortified population. Clin Chem Lab Med. (2005) 43:1048–51. doi: 10.1515/CCLM.2005.183
48. Bae S, West AA, Yan J, Jiang X, Perry CA, Malysheva O, et al. Vitamin B-12 status differs among pregnant, lactating, and control women with equivalent nutrient intakes. J Nutr. (2015) 145:1507–14. doi: 10.3945/jn.115.210757
49. Visentin CE, Masih SP, Plumptre L, Schroder TH, Sohn K-J, Ly A, et al. Low serum vitamin B-12 concentrations are prevalent in a cohort of pregnant Canadian women. J Nutr. (2016) 146:1035–42. doi: 10.3945/jn.115.226845
50. Hure AJ, Collins CE, Smith R, A. longitudinal study of maternal folate and vitamin B12 status in pregnancy and postpartum, with the same infant markers at 6 months of age. Matern Child Health J. (2012) 16:792–801. doi: 10.1007/s10995-011-0782-0
51. Nabi H, Bochud M, Glaus J, Lasserre AM, Waeber G, Vollenweider P, et al. Association of serum homocysteine with major depressive disorder: results from a large population-based study. Psychoneuroendocrinology. (2013) 38:2309–18. doi: 10.1016/j.psyneuen.2013.04.018
52. Permoda-Osip A, Dorszewska J, Skibinska M, Chlopocka-Wozniak M, Rybakowski JK. Hyperhomocysteinemia in bipolar depression: clinical and biochemical correlates. Neuropsychobiology. (2013) 68:193–6. doi: 10.1159/000355292
53. Elstgeest L, Brouwer I, Penninx BW, Van Schoor N, Visser M. Vitamin B12, homocysteine and depressive symptoms: a longitudinal study among older adults. Eur J Clin Nutr. (2017) 71:468–75. doi: 10.1038/ejcn.2016.224
54. Beydoun MA, Shroff MR, Beydoun HA, Zonderman AB. Serum folate, vitamin B-12 and homocysteine and their association with depressive symptoms among US adults. Psychosom Med. (2010) 72:862. doi: 10.1097/PSY.0b013e3181f61863
55. Chengfeng S, Wei L, Xinxing W, Lei W, Rui Z, Lingjia Q. Hyperhomocysteinemia is a result, rather than a cause, of depression under chronic stress. PLoS ONE. (2014) 9:e106625. doi: 10.1371/journal.pone.0106625
56. Boylan LM, Hart S, Porter KB, Driskell JA. Vitamin B-6 content of breast milk and neonatal behavioral functioning. J Am Diet Assoc. (2002) 102:1433–8. doi: 10.1016/S0002-8223(02)90317-2
Keywords: pregnancy, lactation, human milk, vitamin B12, homocysteine, anxiety, depression
Citation: Batalha MA, dos Reis Costa PN, Ferreira ALL, Freitas-Costa NC, Figueiredo ACC, Shahab-Ferdows S, Hampel D, Allen LH, Pérez-Escamilla R and Kac G (2022) Maternal Mental Health in Late Pregnancy and Longitudinal Changes in Postpartum Serum Vitamin B-12, Homocysteine, and Milk B-12 Concentration Among Brazilian Women. Front. Nutr. 9:923569. doi: 10.3389/fnut.2022.923569
Received: 03 May 2022; Accepted: 09 June 2022;
Published: 11 July 2022.
Edited by:
Daniel Joseph Lamport, University of Reading, United KingdomReviewed by:
Guiju Sun, Southeast University, ChinaFrancisco Felix Caballero, Autonomous University of Madrid, Spain
Copyright © 2022 Batalha, dos Reis Costa, Ferreira, Freitas-Costa, Figueiredo, Shahab-Ferdows, Hampel, Allen, Pérez-Escamilla and Kac. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gilberto Kac, Z2lsYmVydG8ua2FjQGdtYWlsLmNvbQ==