
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Nutr., 14 June 2022
Sec. Nutrition and Sustainable Diets
Volume 9 - 2022 | https://doi.org/10.3389/fnut.2022.903216
This article is part of the Research TopicAdvances in Food EnvironmentsView all 8 articles
 Ruixin Chi1,2†
Ruixin Chi1,2† Shijun Lu3†
Shijun Lu3† Na Zhang1,2Man Zhang1,2Kaiwei Guo1,2Songming Du4Jing Guo5Xiaoqi Hu6
Na Zhang1,2Man Zhang1,2Kaiwei Guo1,2Songming Du4Jing Guo5Xiaoqi Hu6 Guansheng Ma1,2*
Guansheng Ma1,2*Objective: Adolescents' alcohol consumption has lifetime adverse physical and mental health effects. Family environment factors have a significant influence in shaping adolescents' beliefs and habits. We conducted the multicenter cross-sectional study aiming to investigate the association between family environment factors and adolescent drinking behavior in China.
Methods: The study investigated 27,762 middle school students from Beijing, Shanghai, Guangzhou, Jinan, Chengdu, and Harbin. A logistic regression model was used to explore the association between family environmental factors and adolescent drinking behavior. Participants were asked to self-report previous experiences of drinking and getting drunk to access their drinking status. Factors of family environment related to alcohol consumption included: parents' educational level, family economic status, family composition, the number of times parents drank alcohol in the past 30 days, and parents' attitudes toward their drinking behavior. The logistic regression model was used to adjust the demographic confounders, including gender, age, city, location, and smoking status, and to explore the association between family environmental factors and adolescent alcohol drinking behaviors.
Results: Compared with students whose parents prohibited drinking, students who were approved drinking were more likely to drink in this year (OR = 16.544, 95%CI:15.265–17.929, P < 0.001; Full adjustment: OR = 13.111, 95% CI: 12.031–14.288, P < 0.001), drink in this month (OR = 7.791, 95% CI: 7.077–8.565, P < 0.001; Full adjustment: OR = 6.010, 95% CI: 5.439–6.641, P < 0.001). In addition, Low family economic status, not living with the mother, parents' ambivalent attitudes toward their children's drinking and parental drinking were risk factors for drinking among middle school students.
Conclusion: The family environment, especially parents' attitudes, is associated with students' drinking and drunken behavior. Mobilizing the power of parents may play a positive role in the effective prevention and control of adolescent drinking.
Alcohol is harmful to people's health. Worldwide, alcohol consumption is responsible for nearly three million deaths in a year. Alcohol is a significant risk factor for premature death and disability in people aged 15–49. Meanwhile, alcohol has toxic effects on the central nervous system, digestive system, and cardiovascular system, and acts as an immunosuppressant to increasethe risk of infectious diseases (1).
For adolescents, alcohol use could lead to long-term health consequences. Adolescents are at an important stage of growth and development; and this stage has an important impact on the development of the brain's structure and function. Alcohol intake can cause changes in the brain, causing impaired neurodevelopment, affecting cognitive and behavioral functions, and resulting in the decline of academic performance and frequent injury events (2). Adolescent alcohol consumption impairs physical and mental health during adolescence and throughout lifetime (3, 4). A global study showed that alcohol (7% of Disability-adjusted life years) was one of the significant risk factors affecting people's (age from 10 to 24) health (5). This findings suggest public health strategies should focus on children and adolescents and prioritize adolescent limiting alcohol consumption (6).
Alcohol is prevalent among teenagers all over the world, including Chinese teenagers. WHO(World Health Organization) reported that 43.0% of people over 15 years old worldwide are drinking, and 12.5% have been drinking before (1). According to a cross-sectional survey conducted in southern China, the current alcohol consumption rate among 9–21 years old is 7.3% (7). A 2005 survey of youth risk behaviors in 18 provinces and cities in China showed that about 51.1% of young people in grades 7 to 12 had used alcohol before (8). A study in the United States showed that 78.2% of teenagers drink alcohol in late adolescence. And the rate of drinking is increasing year by year (9). It is of great importance to pay attention to adolescents' drinking behavior, to understand the factors affecting adolescent drinking, and to control them for improving the health of the adolescent (6).
It has been proved that the food environment can affect adolescents' eating behaviors, such as fruit and vegetable intake, calorie intake, fat intake, and water drinking behavior (10–14). Some studies have also attempted to explore the influence of family environment on adolescent drinking behavior (15, 16). Family composition (17, 18), family economic status (19), parents' educational level (20), drinking behavior (21–24), and parents' attitude (19) toward their children were all mentioned (25). However, the results were inconsistent across different studies. Moreover, variables related to the family environment are not sufficient in studies.
Current research evidence is insufficient to show the relationship between family environment and adolescent drinking behavior in China. This study attempted to investigate the association between family environment and adolescent drinking behavior in China.
The study was performed in middle school students in China. We carried out a cross-sectional survey in Beijing, Shanghai, and Guangzhou in 2013 and completed the survey in Jinan, Chengdu, and Harbin with the same process in 2014. This study used a multi-stage stratified cluster sampling method to select 4–6 urban districts in each city based on administrative division, geographical location, and class size. Middle and high schools (including ordinary high schools and vocational schools) were selected from the selected urban districts. There were three grades in both middle and high schools in China. If it were impossible to investigate the third-grade class due to the college entrance examination or internship, we would select one more second-grade class from the school for investigation. Participants completed a voluntary and anonymous self-management questionnaire during class. Subjects were informed of the purpose of the study and will have the right to refuse to participate. Students who complete the questionnaire will be rewarded with gifts.
The Ethics Committee of the National Institute for Nutrition and Food Safety, Chinese Center for Disease Control and Prevention, approved the study. The ethical approval number is 2013–19. All investigations were conducted with the informed consent of all participating students, guardians, and school units.
Demographic characteristics were measured with a questionnaire. Participants reported their gender, age, cities, and location. The general information questionnaire was used to collect basic demographic information, including gender, age, city, location, and whether the study subjects smoked. Locations were divided into urban and suburban areas.
According to the Youth Risk Behavior Survey (YRBS) questionnaire and Global School-based Student Health Survey (GSHS) of WHO, the questionnaire of Drinking Behavior of Middle School Students used in this survey was determined through the discussion of experts of the project team. The subjects were asked to fill in the questionnaire according to their actual situation. A detailed analysis of drinking behavior will be carried out separately. In this study, only the following indicators were included: “whether you ever consumed alcohol,” “whether you consumed alcohol within a year,” “whether you consumed alcohol within a month,” and “whether you were ever drunk.” The outcome variables were all binary variables, divided into “yes and no. The questionaires used in this survey was determined through the discussion of experts of the project team. The subjects were asked to fill in the questionnaire according to their actual situation. A detailed analysis of drinking behavior will be carried out separately. In this study, only the following indicators were included: “have you ever consumed alcohol,” “have you consumed alcohol within a year,” “have you consumed alcohol within a month,” and “have you ever being drunk.” The outcome variables were all binary variables, divided into “yes” and “no.”
In this study, family environment variables associated with alcohol consumption included: family economic status, father's education level, mother's education level, and cohabitants. In addition, the times of parents' drinking behaviors and attitudes toward student alcohol consumption were also taken into consideration. We used the family affluence scale (FAS) to measure family economic status described in our previous study (26). Cohabitants fall into four categories: living with both parents, living only with their father, living only with their mother, and living with others. Parents' education level was divided into three categories, high school and lower, college, and graduate school. The number of times parents drank alcohol was defined as never, 1–4 times a month, or more than 4 times a month. The scale measuring parental attitudes favorable toward drinking includes three options, including “forbid” (0), “agree” (1) and “not sure” (2).
We used SAS 9.4 and SPSS 25 for data cleaning and analysis. For questions with logical errors, according to the cleaning principle of CDC in the YRBSS survey, only the questions with logical errors were set as missing, but the whole record of the investigator was not deleted, and the result analysis of other questions was not affected. Logistic regression analysis was used to analyze the relationship between family environment and adolescent drinking behavior. We set drinking behavior as a dependent variable. We included variables related to family environment, including family economic status, father's education level, mother's education level, cohabitant, parents' alcohol behaviors, and attitudes. Confounders were determined by literature review and expert discussion, including demographic characteristics and smoking status (27). In Model 2, we adjusted common counfounders of alcohol drinking, including age, gender and smoking. The study included data from 6 different cities. The drinking habits themselves from these regions can be profoundly different, so we also adjusted city and location in this model. The adjusted model was named Model 2. The difference was statistically significant at P < 0.05.
Before the survey, all investigators were provided with a standard training manual and a workshop to explain the survey. The investigators were made up of medical workers with experience in epidemiological investigations, educators, and staff from local Disease Control and Prevention centers. The questionnaire results were filled in by students using an answer sheet that could be scanned by an automatic laser card reader. After scanning, two people check the data and finally save the data in excel form.
The total number of participants was 27,762, including 13,417 males (48.3%) and 14,345 females (51.7%). The age distribution of subjects ranged from 12 to 20 years [M (IQR) = 15.00 (3)]. The subjects from Beijing, Shanghai, Guangzhou, Jinan, and Chengdu were 3,782, 3,142, 5,241, 4,889, 5,363, and 5,345. Accounting for 13.6%, 11.3%, 18.9%, 17.6%, 19.3% and 19.3%, respectively. 14,375 (51.8%) of the subjects came from urban areas and 13,387 (48.2%) from suburban areas. The general characters of this study participants are shown in Table 1.
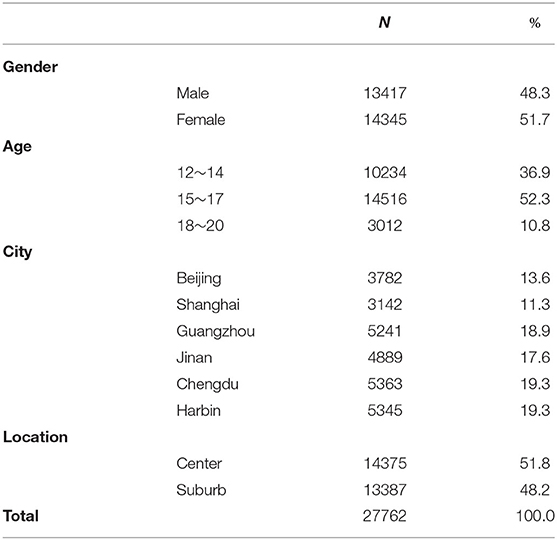
Table 1. The demographic information of participants.
The results show that 15,723 students (56.6%) had drunk alcohol before; 10,925 students had drunk alcohol in the past year, accounting for 44.8%; 6107 students had drunk alcohol in the past month, accounting for 23.3%. Four thousand nine hundered fivety students had been drunk, accounting for 19.3%. Among the respondents, 61.4% of male and 52.2% of female ever drank alcohol. Over the past year, 51.8% of men and 38.1% of women ever drank alcohol. 29.0% of men and 18.1% of women ever drank alcohol over the past month. And 23.6% of men and 15.3% of women ever been drunk. There were statistically significant differences in alcohol-related behaviors among subjects of different genders (P < 0.05). Among the subjects aged 12 to 14, 15 to 17, and 18 to 20, the drinking rates were 32.8%, 62.9%, and 73.2%, respectively. The proportion of those who had drunk in the past year was 30.6%, 51.5%, and 61.6%, respectively. The proportion of people used alcohol in past month was 16.0%, 26.8%, and 31.8%. The rates of previous drunkenness were 9.6%, 23.3%, and 33.7%, respectively. There were statistically significant differences in alcohol-related behaviors among subjects of different ages (P < 0.05). In Beijing, Chengdu, Guangzhou, Harbin, Jinan, and Shanghai, those who drank alcohol were 50.8%, 64.2%, 66.6%, 49.6%, 52.9%, and 51.9%, respectively. The proportion of people who had drunk alcohol in the past year was 37.3%, 50.2%, 54.1%, 39.8%, 41.8%, and 42.2%, respectively. The proportion of people who had drunk alcohol in the past month was 24.8%, 23.9%, 26.5%, 19.7%, 23.4%, and 21.2% and the proportion of people who had been drunk was 19.1%, 23.4%, 21.1%, 18.8%, 16.2%, and 15.1%, respectively. There was a significant difference in the rate of alcohol drinking-related behaviors among the subjects in different cities (P < 0.05). In urban and suburban areas, the proportion of people who had drunk alcohol ever was 57.7% and 55.4%, the proportion of people who had drunk alcohol in the past year was 46.0% and 43.5%, the proportion of people who had drunk alcohol in the past month was 24.7% and 21.8%, and the proportion of people who had drunk alcohol in the past month was 18.4% and 20.2%, respectively. There were statistically significant differences in alcohol-related behaviors between urban and suburban subjects (P < 0.05). Participates' alcohol drinking behaviors are shown in Table 2.

Table 2. Participates' alcohol drinking behaviors.
Table 3 shows the family environment related to drinking among the subjects. Most of the subjects' parents had a secondary school education or below. Most of the subjects lived with their parents. 77.1% of the study subjects reported that their fathers did not drink alcohol, and 78.9% reported that their mothers did not drink alcohol. Parents who forbid, support, and unsure about their children's drinking accounted for 39.9%, 47.3%, and 12.7%, respectively.
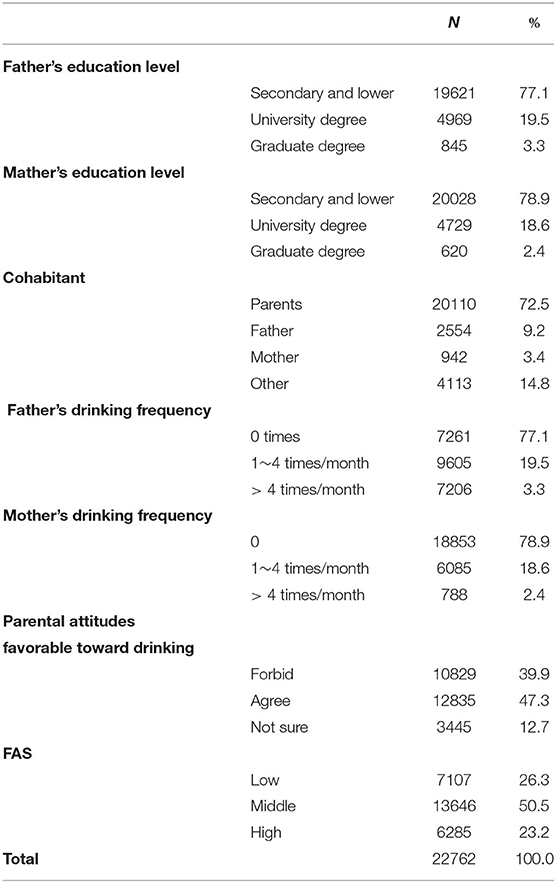
Table 3. Family environment about alcohol drinking.
The results demonstrate that family environment was closely related to adolescent drinking behavior. The association between family environment and adolescent drinking behavior is shown in Table 4. Subjects whose parents supported their drinking were more likely to drink alcohol (ever consumed alcohol (OR, odds ratio= 15.069, 95% CI, confidence interval:13.998–16.222, P < 0.001; Full adjustment: OR = 12.741, 95% CI: 11.772–13.789, P < 0.001), consumed alcohol in this year (OR = 16.544, 95% CI:15.265–17.929, P < 0.001; Full adjustment: OR = 13.111, 95% CI: 12.031–14.288, P < 0.001), consumed alcohol in this month [OR = 7.791, 95%CI: 7.077–8.565, P < 0.001; Full adjustment: Odds Ratio (OR) = 6.010, 95% CI: 5.439–6.641, P < 0.001) than those whose parents prohibited it. Low family economic status, not living with the mother, parents' unclear attitude to their children's drinking, and parental drinking were also the risk factors for adolescent drinking.
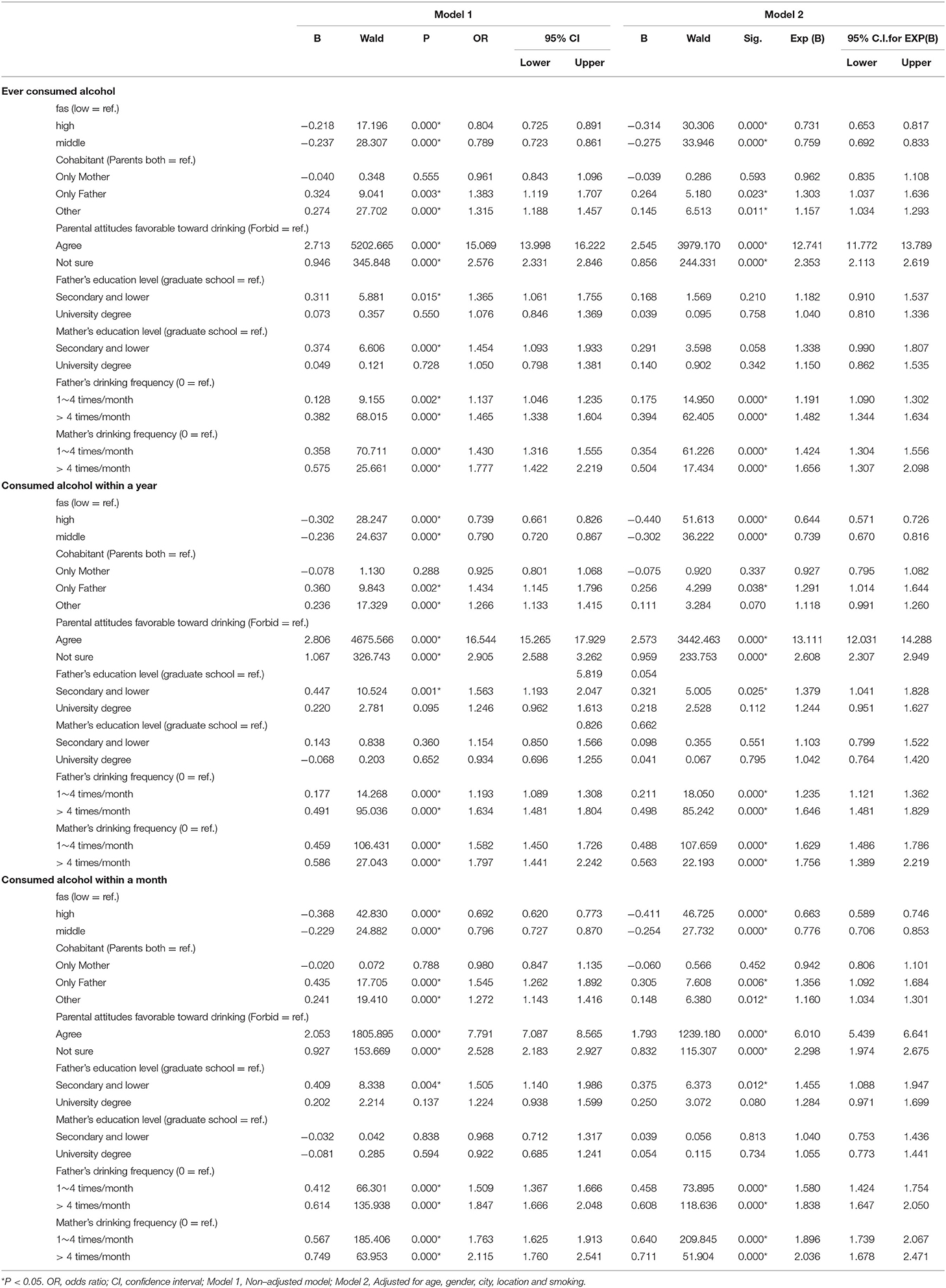
Table 4. Unadjusted and adjusted logistic regression analyses of family environment factors and alcohol drinking.
The relationship between different dimensions of family environment and getting drunk is shown in Table 5, low educational level, and parental alcohol consumption are the risk factors for adolescent drunkenness. Parents' positive attitudes toward children's drinking were also associated with higher risk of getting drunk (OR = 5.201, 95% CI:4.734–5.714, P < 0.001; Full adjustment, OR =3.433, 95% CI: 3.103–3.797, P < 0.001). Low family economic status, not living with the mother, unclear parents' attitude to their children's alcohol consumption were also had association with drunk behavior significantly.
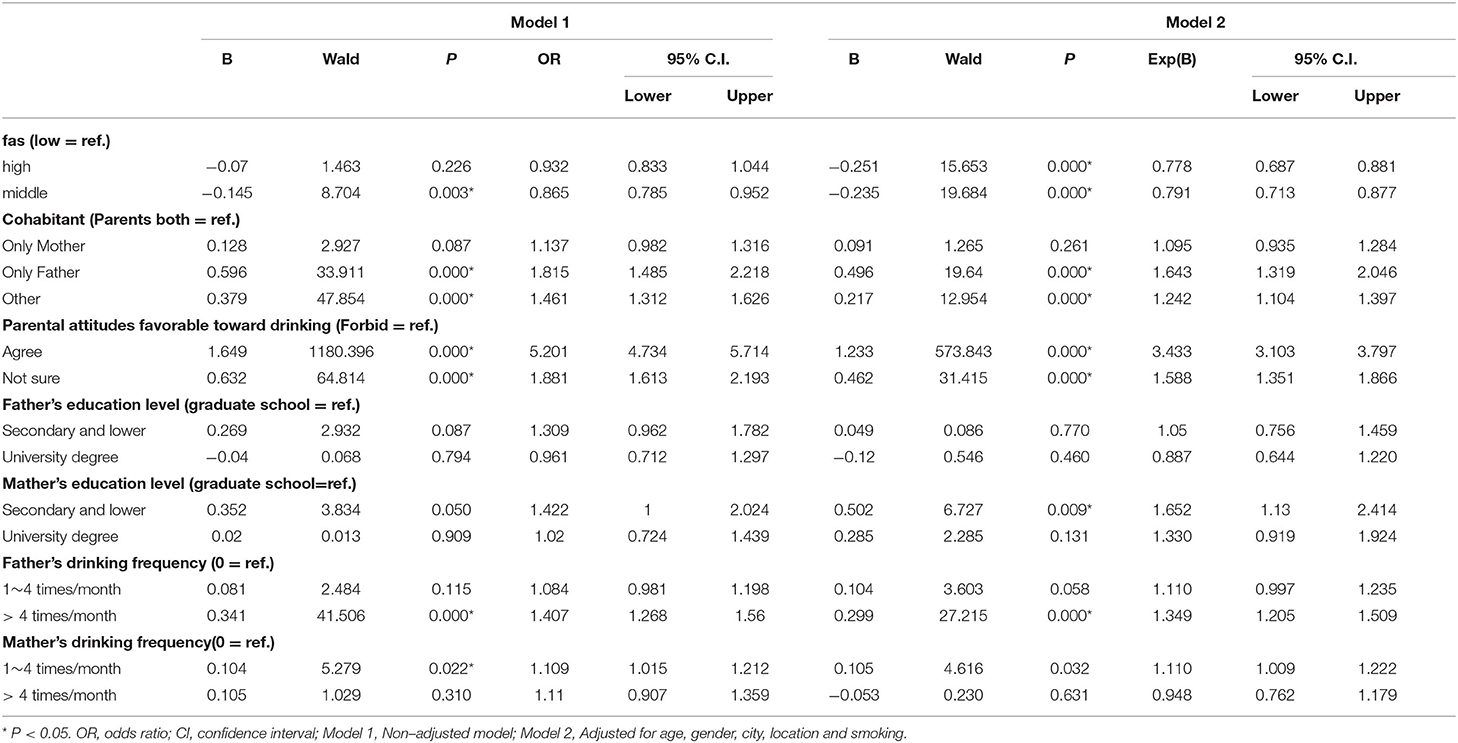
Table 5. Unadjusted and adjusted logistic regression analyses of family environment factors and getting drunk.
This study shows that family environment factors, including parents' attitudes, behavior, and companionship are related to children's drinking behavior. The study supports that family supervision is negatively correlated with adolescent drinking, which is consistent with the results of other foreign studies (19, 28). And this study proved evidence to support this conclusion in the China. Consistent with some research, not living with their mother is a risk factor for adolescent alcohol use, (17, 18). Just as the results of other countries and Taiwan (Province of the People's Republic of China), parental drinking is a predictor of adolescent drinking in this study (21–24). In addition to parents' attitudes, behavior, and companionship, other factors in the family environment also influenced teenagers' drinking behavior in this study. Differ from the research results in some western countries, teenagers from families with low economic status are more likely to drink than those with high economic status (19). The difference may be related to the consumption tendency and culture between different countries.
This study supports the conclusion that family environmental factors are associated with adolescent alcohol consumption. One possible reason is that adolescents connect closely to their parents and internalize their parents' values and norms (29). According to social learning theory, teenagers spend much time with their families, which means teenagers are willing to learn the behavior from the people around them. Social control theory points that parental control can protect children (30, 31).
Previous studies have looked more closely at environmental factors associated with fruit and vegetable intake, calorie intake, fat intake, and water drinking behavior (10). There are few studies on the influence of school/family environment on drinking behavior. Exploring the relationship between family environment and drinking behavior is helpful in finding out which family environment factors are closely related to adolescent drinking behavior. As with other research into the food environment, this is critical for the successfully designing, implementing, and adopting appropriate interventions and policies (32). Teenagers are susceptible to social influences. They are less influenced by their families and become more independent decision-makers. However, at the same time, they tend to have lower levels of self-control, higher levels of impulsivity (33), and higher rates of alcohol use and related harmful behaviors at this stage of life (1, 2, 7–9). Moreover, health behaviors during adolescence impact on lifelong physical and mental health (3, 4). In conclusion, it is vital to carry out this study to explore the relationship between family environmental factors and adolescent drinking behavior.
Although some past studies have explored the relationship between family environment and adolescent alcohol consumption, only a few factors have been identified. Various family environmental factors are considered in this study at the same time. Family structures, economic income levels, and parents' attitudes and behaviors are included in the model simultaneously, which is more detailed than other studies. Moreover, the adjusted model has fully considered the influence of different cities, age, gender, urban area, and other factors. With a relatively large sample size, the results of this study represent the actual situation of a considerable number of Chinese teenagers, which is highly convincing.
There are some limitations to this study. Firstly, due to the limitation of data collection, some spatial environmental factors were not included in this study (34, 35). Moreover, the survey was conducted through the self-report questionnaire, which was not accurate in evaluating variables (36, 37). In addition, our research was conducted in six Chinese cities and is not fully representative of the situation in China. Although this study confirmed the correlation between family environmental factors and adolescents' drinking behavior in six Chinese cities, it could not estabilish the causal relationship as a cross-sectional survey. Further studies are needed to verify the results of this study and explore the causal relationship. If causality is established, more targeted interventions can be implemented. Besides, future research can explore suitable food environment assessment tools for drinking in China. Then appropriate interventions and policies can be designed and implemented according to health-related environmental indicators to impact adolescent drinking behavior positively.
Fairness and ethical principles should be considered in intervene programme and policy making. In particular, authorities should pay more attention to low-income groups and left-behind children. In education and health intervention, health educators should pay attention to adolescents' mental health, emphasizing encouragement rather than punishment.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by the Ethics Committee for Research in Human Subjects of the National Institute for Nutrition and Food Safety, Chinese Center for Disease Control and Prevention. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
RC conducted statistical analysis and completed the first draft of the paper, while SL was responsible for the implementation of the project, data cleaning and participated in the writing of the paper. GM was involved in the survey and gave guidance on writing and revising the article. NZ, MZ, and KG participated in the writing, discussion and revision of the article. SD was responsible for the on-site quality control of the project and participated in the research design. JG participated in the implementation of the project and the revision of the article. XH directed the on-site work of the project and participated in the research design. All authors contributed to the article and approved the submitted version.
This study was received by Pernod Ricard (China) Trading Co. Ltd. Financial support, Pernod Ricard (China) Trading Co. Ltd. The company did not intervene in implementing the project, data analysis, and results reporting.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Thank to Pernod Ricard (China) Trading Co. Ltd. Financial support. We thank CDC in Beijing, Shanghai, Guangzhou, Jinan, Chengdu, and Harbin for their support. Thanks to all the on-site staff for their dedication to the project.
1. Organization WH. Global Status Report On Alcohol And Health (2018). World Health Organization (2019).
2. Wetherill R, Tapert SF. Adolescent brain development, substance use, and psychotherapeutic change. Psychol Addict Behav. (2013) 27:393–402. doi: 10.1037/a0029111
3. Andersen A, Due P, Holstein BE, Iversen L. Tracking drinking behaviour from age 15-19 years. Addiction. (2003) 98:1505–11. doi: 10.1046/j.1360-0443.2003.00496.x
4. Pisinger VSC, Hoffmann SH, Palsson L, Dalum P, Grønbæk MK, Tolstrup JS, et al. “High schools High on life”: development of an intervention to reduce excessive drinking in danish high schools. Front Public Health. (2020) 8:435. doi: 10.3389/fpubh.2020.00435
5. Gore FM, Bloem PJ, Patton GC, Ferguson J, Joseph V, Coffey C, et al. Global burden of disease in young people aged 10–24 years: a systematic analysis. Lancet. (2011) 377:2093–102. doi: 10.1016/S0140-6736(11)60512-6
6. Marshall EJ. Adolescent alcohol use: risks and consequences. Alcohol alcoholism. (2014) 49:160–4. doi: 10.1093/alcalc/agt180
7. Guo L, Deng J, He Y, Deng X, Huang J, Huang G, et al. Alcohol use and alcohol-related problems among adolescents in China: a large-scale cross-sectional study. Medicine. (2016) 95:e4533. doi: 10.1097/MD.0000000000004533
8. Xing Y, Ji C, Zhang L. Relationship of binge drinking and other health-compromising behaviors among urban adolescents in China. J Adolesc Health. (2006) 39:495–500. doi: 10.1016/j.jadohealth.2006.03.014
9. Swendsen J, Burstein M, Case B, Conway KP, Dierker L, He J, et al. Use and abuse of alcohol and illicit drugs in US adolescents: results of the national comorbidity survey–adolescent supplement. Arch Gen Psychiat. (2012) 69:390–8. doi: 10.1001/archgenpsychiatry.2011.1503
10. Micha R, Karageorgou D, Bakogianni I, Trichia E, Whitsel LP, Story M, et al. Effectiveness of school food environment policies on children's dietary behaviors: a systematic review and meta-analysis. Plos ONE. (2018) 13:0194555. doi: 10.1371/journal.pone.0194555
11. Pineda E, Swinburn B, Sassi F. Effective school food environment interventions for the prevention of childhood obesity: systematic review and meta-analysis. Lancet. (2019) 394:S77. doi: 10.1016/S0140-6736(19)32874-0
12. Watts AW, Barr SI, Hanning RM, Lovato CY, Mâsse LC. The home food environment and associations with dietary intake among adolescents presenting for a lifestyle modification intervention. BMC Nutrition. (2018) 4:1–9. doi: 10.1186/s40795-018-0210-6
13. Schnettler B, Grunert KG, Lobos G, Miranda-Zapata E, Denegri M, Hueche C. Exploring relationships between family food behaviour and well-being in single-headed and dual-headed households with adolescent children. Curr Psychol. (2021) 40:585–600. doi: 10.1007/s12144-018-9974-8
14. Vaivada T, Lassi ZS, Irfan O, Salam RA, Das JK, Oh C, et al. Nourishing our future: the Lancet Series on adolescent nutrition. Lancet. (2022) 399:123–5. doi: 10.1016/S0140-6736(21)02140-1
15. Nash SG, McQueen A, Bray JH. Pathways to adolescent alcohol use: family environment, peer influence, and parental expectations. J Adolescent Health. (2005) 37:19–28. doi: 10.1016/j.jadohealth.2004.06.004
16. Iacopetti C, Londi I, Patussi V, Cosci F. Family climate in children living with parents who harmfully consume alcohol. Clin Psychol Psychot. (2021) 28:1128–34. doi: 10.1002/cpp.2562
17. Oman RF, Vesely SK, Tolma E, Aspy CB, Rodine S, Marshall L. Does family structure matter in the relationships between youth assets and youth alcohol, drug and tobacco use? J Res Adolescence. (2007) 17:743–65. doi: 10.1111/j.1532-7795.2007.00545.x
18. Elgar FJ, Roberts C, Parry-Langdon N, Boyce W. Income inequality and alcohol use: a multilevel analysis of drinking and drunkenness in adolescents in 34 countries. Eur J Public Health. (2005) 15:245–50. doi: 10.1093/eurpub/cki093
19. Kask K, Markina A, Podana Z. The effect of family factors on intense alcohol use among european adolescents: a multilevel analysis. Psychiatry J. (2013) 2013:250215. doi: 10.1155/2013/250215
20. Wells L, Östberg V. Parental education differentially predicts young adults' frequency and quantity of alcohol use in a longitudinal Swedish sample. SSM-Population Health. (2018) 6:91–7. doi: 10.1016/j.ssmph.2018.09.001
21. Jackson C. Initial and experimental stages of tobacco and alcohol use during late childhood: Relation to peer, parent, and personal risk factors. Addict Behav. (1997) 22:685–98. doi: 10.1016/S0306-4603(97)00005-1
22. Garmiene A, Zemaitiene N, Zaborskis A. Family time, parental behaviour model and the initiation of smoking and alcohol use by ten-year-old children: an epidemiological study in Kaunas, Lithuania. BMC Public Health. (2006) 6:1–9. doi: 10.1186/1471-2458-6-287
23. Li CY, Pentz MA, Chou CP. Parental substance use as a modifier of adolescent substance use risk. Addiction. (2002) 97:1537–50. doi: 10.1046/j.1360-0443.2002.00238.x
24. Hung CC, Yen LL, Wu WC. Association of parents' alcohol use and family interaction with the initiation of alcohol use by sixth graders: a preliminary study in Taiwan. BMC Public Health. (2009) 9:1–9. doi: 10.1186/1471-2458-9-172
25. Welch KA, Carson A, Lawrie SM. Brain structure in adolescents and young adults with alcohol problems: systematic review of imaging studies. Alcohol Alcoholism. (2013) 48:433–44. doi: 10.1093/alcalc/agt037
26. Lu S, Du S, Hu X, Zou S, Liu W, Ba L, et al. Drinking patterns and the association between socio-demographic factors and adolescents' alcohol use in three metropolises in China. Int J Env Res Pub He. (2015) 12:2037–53. doi: 10.3390/ijerph120202037
27. Reed MB, Wang R, Shillington AM, Clapp JD, Lange JE. The relationship between alcohol use and cigarette smoking in a sample of undergraduate college students. Addict Behav. (2007) 32:449–64. doi: 10.1016/j.addbeh.2006.05.016
28. Tael-Öeren M, Naughton F, Sutton S. The relationship between parental attitudes and children's alcohol use: a systematic review and meta-analysis. Addiction. (2019) 114:1527–46. doi: 10.1111/add.14615
29. Luthar SS, Cicchetti D, Becker B. The construct of resilience: a critical evaluation and guidelines for future work. Child Dev. (2000) 71:543–62. doi: 10.1111/1467-8624.00164
30. Hawkins JD, Weis JG. The social development model: An integrated approach to delinquency prevention. J Prim Prev. (1985) 6:73–97. doi: 10.1007/BF01325432
31. Bufford RK. Social foundations of thought and action - a social cognitive theory - bandura,A. J Psychol Theol. (1986) 14:341–2. doi: 10.1017/S0813483900008238
32. Turner C, Aggarwal A, Walls H, Herforth A., Drewnowski A, Coates J, et al. Concepts and critical perspectives for food environment research: a global framework with implications for action in low- and middle-income countries. Glob Food Secur-Agr. (2018) 18:93–101. doi: 10.1016/j.gfs.2018.08.003
33. Van Dam S, Van Reijmersdal E. Insights in adolescents' advertising literacy, perceptions and responses regarding sponsored influencer videos and disclosures. Cyberpsychology: J Psychosocial Res Cyberspace. (2019) 13:1–19. doi: 10.5817/CP2019-2-2
34. Mackenbach JD, Nelissen KGM, Dijkstra SC, Poelman MP, Daams JG, et al. A systematic review on socioeconomic differences in the association between the food environment and dietary behaviors. Nutrients. (2019) 11:2215. doi: 10.3390/nu11092215
35. Lima LR, Okamura AB, Carvalho KMB, Dutra ES, Gonçalves VSS. The food environment in schools and their immediate vicinities associated with excess weight in adolescence: a systematic review and meta-analysis. Health Place. (2021) 71:102664. doi: 10.1016/j.healthplace.2021.102664
36. Paulhus DL, Vazire S. The self-report method. Handbook Research Methods Persona Psychology. (2007) 1:224–39.
Keywords: family environment, alcohol drinking (MeSH), family, adolescent, underage drinking
Citation: Chi R, Lu S, Zhang N, Zhang M, Guo K, Du S, Guo J, Hu X and Ma G (2022) The Association Between Family Environment and Adolescent Alcohol Drinking Behavior: A Cross-Sectional Study of Six Chinese Cities. Front. Nutr. 9:903216. doi: 10.3389/fnut.2022.903216
Received: 24 March 2022; Accepted: 19 May 2022;
Published: 14 June 2022.
Edited by:
Xinli Li, Nanjing Medical University, ChinaReviewed by:
Iokfai Cheang, The First Affiliated Hospital of Nanjing Medical University, ChinaCopyright © 2022 Chi, Lu, Zhang, Zhang, Guo, Du, Guo, Hu and Ma. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Guansheng Ma, bWFnc0Biam11LmVkdS5jbg==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.