
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Nutr., 14 July 2022
Sec. Nutritional Epidemiology
Volume 9 - 2022 | https://doi.org/10.3389/fnut.2022.897089
This article is part of the Research TopicThe Role of Front-of-Pack Labeling in Making Informed and Healthy Food ChoicesView all 10 articles
 Nadine Khoury1,2†
Nadine Khoury1,2† Clara Gómez-Donoso1,2†María Ángeles Martínez1,2,3
Clara Gómez-Donoso1,2†María Ángeles Martínez1,2,3 Miguel Ángel Martínez-González3,4,5
Miguel Ángel Martínez-González3,4,5 Dolores Corella3,6
Dolores Corella3,6 Montserrat Fitó3,7
Montserrat Fitó3,7 J. Alfredo Martínez3,8,9
J. Alfredo Martínez3,8,9 Ángel M. Alonso-Gómez3,10Julia Wärnberg3,11
Ángel M. Alonso-Gómez3,10Julia Wärnberg3,11 Jesús Vioque12,13Dora Romaguera3,14Ana León-Acuña3,15
Jesús Vioque12,13Dora Romaguera3,14Ana León-Acuña3,15 Francisco J. Tinahones3,16José M. Santos-Lozano3,17Luís Serra-Majem3,18Paloma Massó Guijarro19,20,21
Francisco J. Tinahones3,16José M. Santos-Lozano3,17Luís Serra-Majem3,18Paloma Massó Guijarro19,20,21 Josep A. Tur3,22Vicente Martín Sánchez12,23
Josep A. Tur3,22Vicente Martín Sánchez12,23 Xavier Pintó3,24Miguel Delgado-Rodríguez9,25
Xavier Pintó3,24Miguel Delgado-Rodríguez9,25 Pilar Matía-Martín26Josep Vidal27,28Clotilde Vázquez3,29
Pilar Matía-Martín26Josep Vidal27,28Clotilde Vázquez3,29 Lidia Daimiel30
Lidia Daimiel30 Emili Ros3,31
Emili Ros3,31 Maira Bes-Rastrollo3,4Rocio Barragan3,6
Maira Bes-Rastrollo3,4Rocio Barragan3,6 Olga Castañer3,7
Olga Castañer3,7 Jose D. Torres-Peña3,15
Jose D. Torres-Peña3,15 Leyre Notario-Barandiaran13Carlos Muñoz-Bravo11Itziar Abete3,8,9Lara Prohens3,14
Leyre Notario-Barandiaran13Carlos Muñoz-Bravo11Itziar Abete3,8,9Lara Prohens3,14 Naomi Cano-Ibáñez12,19,21Lucas Tojal Sierra3,10
Naomi Cano-Ibáñez12,19,21Lucas Tojal Sierra3,10 José Carlos Fernández-García3,16Carmen Sayon-Orea3,4Maria Pascual1,2
José Carlos Fernández-García3,16Carmen Sayon-Orea3,4Maria Pascual1,2 Jose V. Sorli3,6Dolores Zomeño3,7,32Patricia J. Peña-Orihuela3,15Antonio J. Signes-Pastor12,13F. Javier Basterra-Gortari4,33Helmut Schröeder3,7
Jose V. Sorli3,6Dolores Zomeño3,7,32Patricia J. Peña-Orihuela3,15Antonio J. Signes-Pastor12,13F. Javier Basterra-Gortari4,33Helmut Schröeder3,7 Jordi Salas Salvadó1,2,3*‡
Jordi Salas Salvadó1,2,3*‡ Nancy Babio1,2,3*‡
Nancy Babio1,2,3*‡Background: Helping consumers to improve the nutritional quality of their diet is a key public health action to prevent cardiovascular diseases (CVDs). The modified version of the Food Standard Agency Nutrient Profiling System Dietary Index (FSAm-NPS DI) underpinning the Nutri-Score front-of-pack label has been used in public health strategies to address the deleterious consequences of poor diets. This study aimed to assess the association between the FSAm-NPS DI and some CVD risk factors including body mass index (BMI), waist circumference, plasma glucose levels, triglyceride levels, high-density lipoprotein (HDL) and low-density lipoprotein (LDL) cholesterol, and diastolic and systolic blood pressure.
Materials and Methods: Dietary intake was assessed at baseline and after 1 year of follow-up using a 143-item validated semi-quantitative food-frequency questionnaire. Dietary indices based on FSAm-NPS applied at an individual level were computed to characterize the diet quality of 5,921 participants aged 55–75 years with overweight/obesity and metabolic syndrome from the PREDIMED-plus cohort. Associations between the FSAm-NPS DI and CVD risk factors were assessed using linear regression models.
Results: Compared to participants with a higher nutritional quality of diet (measured by a lower FSAm-NPS DI at baseline or a decrease in FSAm-NPS DI after 1 year), those participants with a lower nutritional quality of diet (higher FSAm-NPS DI or an increase in score) showed a significant increase in the levels of plasma glucose, triglycerides, diastolic blood pressure, BMI, and waist circumference (β coefficient [95% confidence interval]; P for trend) (1.67 [0.43, 2.90]; <0.001; 6.27 [2.46, 10.09]; <0.001; 0.56 [0.08, 1.05]; 0.001; 0.51 [0.41, 0.60]; <0.001; 1.19 [0.89, 1.50]; <0.001, respectively). No significant associations in relation to changes in HDL and LDL-cholesterol nor with systolic blood pressure were shown.
Conclusion: This prospective cohort study suggests that the consumption of food items with a higher FSAm-NPS DI is associated with increased levels of several major risk factors for CVD including adiposity, fasting plasma glucose, triglycerides, and diastolic blood pressure. However, results must be cautiously interpreted because no significant prospective associations were identified for critical CVD risk factors, such as HDL and LDL-cholesterol, and systolic blood pressure.
Cardiovascular disease (CVD) is the leading cause of mortality and is considered a major global public health problem (1, 2). According to the estimation in 2019, CVD burden was found to be responsible for 17.9 million deaths worldwide, accounting for approximately 32% of all global deaths, representing a huge economic and social cost (3).
A healthy diet is recognized as a lever for public health by using a modifiable determinant of CVD and other chronic diseases that can be addressed through primary prevention interventions (4). In contrast, an unhealthy diet characterized by an excess of energy, added sugar, salt and saturated fats, and a lack of fruits, vegetables, and fibers has been recognized as an important causal CVD risk factor through the modulation of adiposity and other cardiometabolic risk factors (5).
Over the past decade, different strategies have been proposed to increase adherence to a healthy diet and reduce the risk of CVD. One of the recent initiatives in this regard is the adoption of front-of-pack (FOP) nutrition labels (6). Although labels on the back of the pack are already mandatory in all European countries according to RE 1169/2011 (7), there is evidence that this information is not easily understandable by consumers. In contrast, nutrition labels found on the front of pack of products are considered more helpful and efficient for consumers since nutritional information is summarized and available at a glance (8, 9). FOP labeling aims to help consumers make healthier choices at the point of purchase and to incentivize food manufacturers to reduce the content of nutrients that might compromise diet quality (e.g., salt, saturated fatty acids, and sugar) and/or increase the content of beneficial nutrients (e.g., fibers and vitamins) (10, 11).
Front-of-pack nutrition labels reflect the nutritional quality of food using a nutrient profiling system (NPS) (12). Nutrient profiling is widely used to support public health initiatives to promote healthy eating (12). Among the available nutrient profiling systems, the NPS developed by the UK Food Standard Agency (FSA-NPS) has been consistently validated in Europe (13). This system was originally developed to discriminate foods based on their nutritional composition in the context of television commercials targeting children (14). In France, after some modifications of the FSA-NPS by the French High Council for Public Health (Haut Conseil de la Santé Publique, HCSP) and demonstrating its applicability within the French context, the modified FSA-NPS (FSAm-NPS) was established and a dietary index (DI) based on the FSAm-NPS (FSAm-NPS DI) was developed to validate the algorithm underlying the Nutri-Score FOP label (15, 16). The score for a given food or beverage is calculated by allocating points for the content per 100 g or 100 ml. This algorithm considers both positive scoring components (protein, fiber, percentage of fruit, vegetables, legumes, nuts, rapeseed oil, walnut oil, and olive oil) and negative components (energy, sugars, saturated fatty acids, and salt) (17), and has been proved effective to rank products by nutritional quality and improve food purchases in real-life grocery shopping settings (18).
In addition, several large European prospective studies have shown associations between a higher FSAm-NPS (lower nutritional quality) and an increased risk of cancer (19), CVD (20), cancer mortality (21), CVD mortality (22), and all-cause mortality (23). In contrast, a lower FSAm-NPS (better nutritional quality) has been associated with a lower risk of long-term weight gain and metabolic syndrome incidence in the SU.VI.MAX French cohort study (24, 25). However, there is less information available about the association between the FSAm-NPS DI and CVD risk factors. The aim of this study was to evaluate the association between the FSAm-NPS DI and different CVD risk factors including body mass index (BMI), waist circumference, glucose, triglycerides, HDL- and LDL-cholesterol levels, as well as diastolic and systolic blood pressure in elderly adults with overweight/obesity and metabolic syndrome.
A prospective analysis was conducted using the data of the PREDIMED-Plus (PREvención con DIeta MEDiterránea) cohort. The PREDIMED-Plus trial is an ongoing randomized, controlled trial conducted in 23 Spanish centers that aims to compare the effect of an intensive weight loss intervention (based on an energy-reduced Mediterranean diet, physical activity promotion, and behavioral support) on the incidence of CVD events, to a control group that receives usual care advice and non-caloric reduced Mediterranean diet recommendations. A detailed description of the PREDIMED-Plus study is available at https://www.predimedplus.com. Between October 2013 and December 2016, 6,874 participants were recruited in Spain and were randomly assigned to either an intensive lifestyle intervention or standard medical care in a 1:1 ratio. Eligible participants were overweight or obese (BMI 27–40 kg/m2) men and women aged 55–75 years who met at least three metabolic syndrome criteria as follows: waist circumference > 102 cm in men and >88 cm in women; serum triglycerides ≥ 150 mg/dl or drug treatment for elevated triglycerides; HDL-c < 40 mg/dl in men and <50 mg/dl in women or drug treatment for low HDL-cholesterol; blood pressure ≥ 130/85 mmHg or antihypertensive drug treatment; and fasting plasma glucose level ≥ 100 mg/dl or hypoglycemic treatment and without documented history of CVD. Extensive descriptions of inclusion and exclusion criteria can be found elsewhere (26). All subjects gave written informed consent, and the final protocol and methods were approved by the institutional review boards of each participating center. A total of 953 participants who did not complete a food frequency questionnaire (FFQ) at baseline and after 1 year of follow-up or with total calorie intake outside the pre-specified energy limits (women < 500 and >3,500 kcal/day, and men < 800 and >4,000 kcal/day) were excluded from the analyses (27) Figure 1.
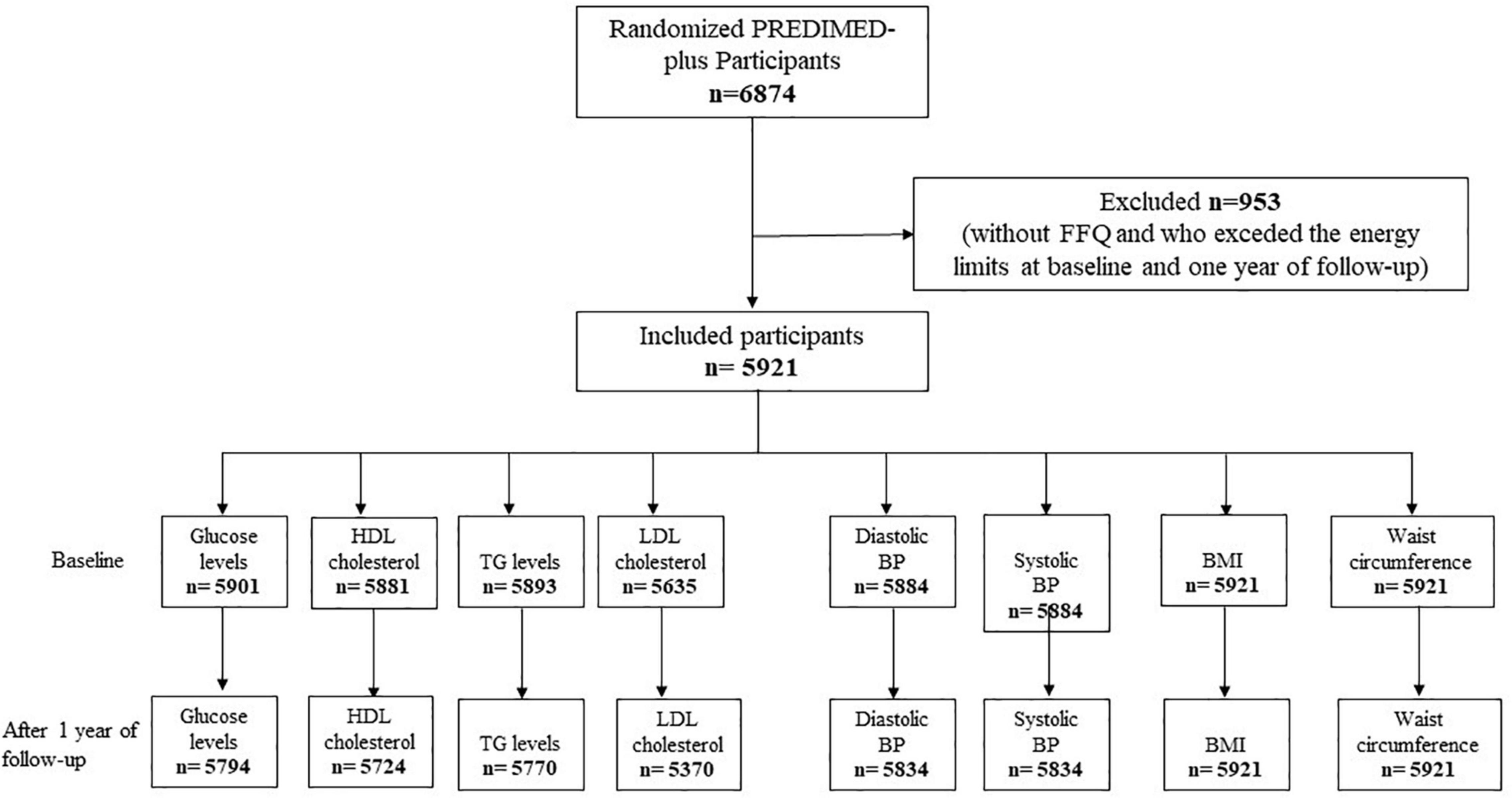
Figure 1. Flow chart of participant’s inclusion.
Dietary intake was assessed at baseline and after 1 year of follow-up using a validated FFQ administered face-to-face by trained dietitians (27). The participants reported their average consumption in terms of frequency and quantity for 143 food and beverage items during the previous year. The frequency of consumption was shown through nine categories ranging from never or almost never to more than six times a day, and a commonly used portion size was specified (e.g., slices, glass, and teaspoons) to indicate serving sizes for each of the items.
The nutrient intake was calculated as the sum of the frequency of daily consumption of each item multiplied by the nutrient composition of the specified serving size according to the Spanish food composition database (28). The total energy intake was also estimated from the quantity and frequency of food and beverage consumption.
The FSAm-NPS is a modified version of the original FSA-NPS (29). Modifications made by the French National Nutrition and Health Program and the French High Council for Public Health impacted the score standards for cheese, added fats, and beverages. For all foods and beverages in the PREDIMED-plus FFQ, the FSAm-NPS was computed per 100 g of the product as follows: 0–40 points was given for the content of critical nutrients that should be limited (0–10 points for each: sugars, saturated fats, sodium, and energy), and 0–15 points was given for the content of beneficial nutrients that should be encouraged (0–5 points for each: fibers, proteins, and the percentage of fruits, vegetables, legumes, nuts, rapeseeds, walnuts, and olive oil that make up the total product). The total score was calculated by subtracting the “negative” (nutrients to avoid) scores from the “positive” (nutrients to promote) scores. As a result, the final FSAm-NPS for each food/beverage was calculated using a discrete continuous scale with a theoretical range of −15 (healthiest) to 40 (least healthy). To generate a dietary index at the individual level, the FSAm-NPS DI was calculated for each participant accounting for their whole diet through energy-weighted means of the FSAm-NPS of all foods and beverages consumed with the following equation:
where “i” signifies a food or beverage consumed by the participant, “FSi” the food (or beverage) score, “Ei”, the mean daily energy intake from this food (or beverage), and “n” the number of different foods.
Therefore, a higher FSAm-NPS-DI reflects lower nutritional quality of the individual’s overall diet.
Qualified PREDIMED-Plus staff followed the study protocol to measure anthropometric variables and blood pressure. CVD risk factors such as glucose levels, triglyceride levels, HDL-cholesterol, LDL-cholesterol, diastolic and systolic blood pressure, BMI, and waist circumference were assessed at baseline and after 1 year of follow-up.
It was measured midway between the lowest rib and the iliac crest using an anthropometric tape, and body weight was measured twice using high-quality electronic calibrated scales and height was measured twice using a wall-mounted stadiometer.
It was computed by dividing the weight in kilograms by the square of height in meters.
They were measured three times using a validated semiautomatic oscillometer (Omron HEM-705CP, Kyoto, Japan) and the mean of repeated measures was used.
They were measured using standard enzymatic methods. LDL-cholesterol was calculated using the Friedewald formula (whenever triglycerides were less than 300 mg/dl and whenever triglycerides were more than 300 mg/dl, LDL-cholesterol was calculated with the standard method).
Covariates were assessed by trained staff in a face-to face interview using self-reported general questionnaires that collect information on socio-demographics (sex, age, marital status, and level of education), lifestyle (smoking habits and physical activity), and medication use. Leisure time physical activity was estimated using the validated Minnesota-REGICOR Short Physical Activity questionnaire (30).
For our analyses, we used the PREDIMED-Plus database updated in December 2020. Analysis of descriptive baseline characteristics of sociodemographic, dietary, and biomedical variables was carried out and reported as means ± SD or median [P25–P75] and percentages (number) for continuous and categorical variables, respectively.
Participants were categorized by tertiles of the FSAm-NPS DI, ranging from tertile 1 (T1) for the best nutritional quality to tertile 3 (T3) for the lowest nutritional quality. The Chi-square test for categorical variables and one-way ANOVA for continuous variables were used to compare the baseline characteristics between the tertiles.
Linear regression models were fitted to assess the associations [β-coefficient (95% confidence interval (CI)] between FSAm-NPS DI (in tertiles and as continuous variables) and CVD risk factors at baseline. We also used linear regression models to explore the prospective associations between changes in the FSAm-NPS DI (in tertiles and as continuous variable) and changes in CVD risk factors after 1 year of follow-up. Changes in the FSAm-NPS-DI were calculated by subtracting 1 year from the baseline values. Missing data after 1 year of follow-up for BMI (four participants) and diastolic BP (one participant) were imputed using the mean value method.
Three models were fitted as follows: crude model, model 1, and the fully adjusted model. Model 1 was adjusted for age (years), sex, BMI (kg/m2), educational level (primary or lower, secondary or academic, or graduate), smoking habit (never, former, or current), total energy consumption (kcal/day), physical activity (METs. min/week), and marital status (married, widowed, single or divorced or separated, or religious). The fully adjusted model was further adjusted for medication for the treatment of hypercholesterolemia, hypertension and diabetes, size of the recruitment centers (<250, 250 to <300, 300 to <400, ≥400), and intervention group. In the prospective analysis, each CVD risk factor was adjusted for its baseline level (in model 1 and fully adjusted).
To indirectly assess the effect of olive oil on the associations with cardiovascular risk factors, we conducted a sensitivity analysis where olive oil was valued −8 (the healthiest value in the score, such as for fruits, vegetables, or legumes) in the computation of the FSAm-NPS-DI.
The statistical significance threshold for the results was set at p < 0.05. All analyses were conducted with robust estimates of the variance to correct for intra-cluster correlation and using the Stata 14 software program (StataCorp).
A total of 5,921 participants (52% men and 48% women, with the mean age of 65 years) were included in this study. Baseline characteristics of the participants overall and according to the tertiles of the FSAm-NPS are shown in Table 1. Participants with a higher FSAm-NPS DI were more likely to be men of younger age, to have a higher level of education, to smoke, to be less physically active, and to have a higher alcohol intake. As expected, participants with a lower FSAm-NPS DI, reflecting a higher nutritional quality (Tertile 1), consumed higher amounts of vegetables, fruits, legumes, unrefined cereals, dairy products, white meat, fish and shellfish, nuts, and fiber. In contrast, participants with a higher FSAm-NPS DI (Tertile 2 and 3), reflecting a lower nutritional quality, consumed higher amounts of refined cereals, biscuits, red meat and processed meat, olive oil, alcohol, and sugar, and showed higher intakes of total energy and saturated fat. In relation to biochemical parameters, the participants in the higher tertile of the FSAm-NPS DI showed higher serum concentrations of triglycerides and LDL-cholesterol and lower levels of HDL-cholesterol (Table 1).
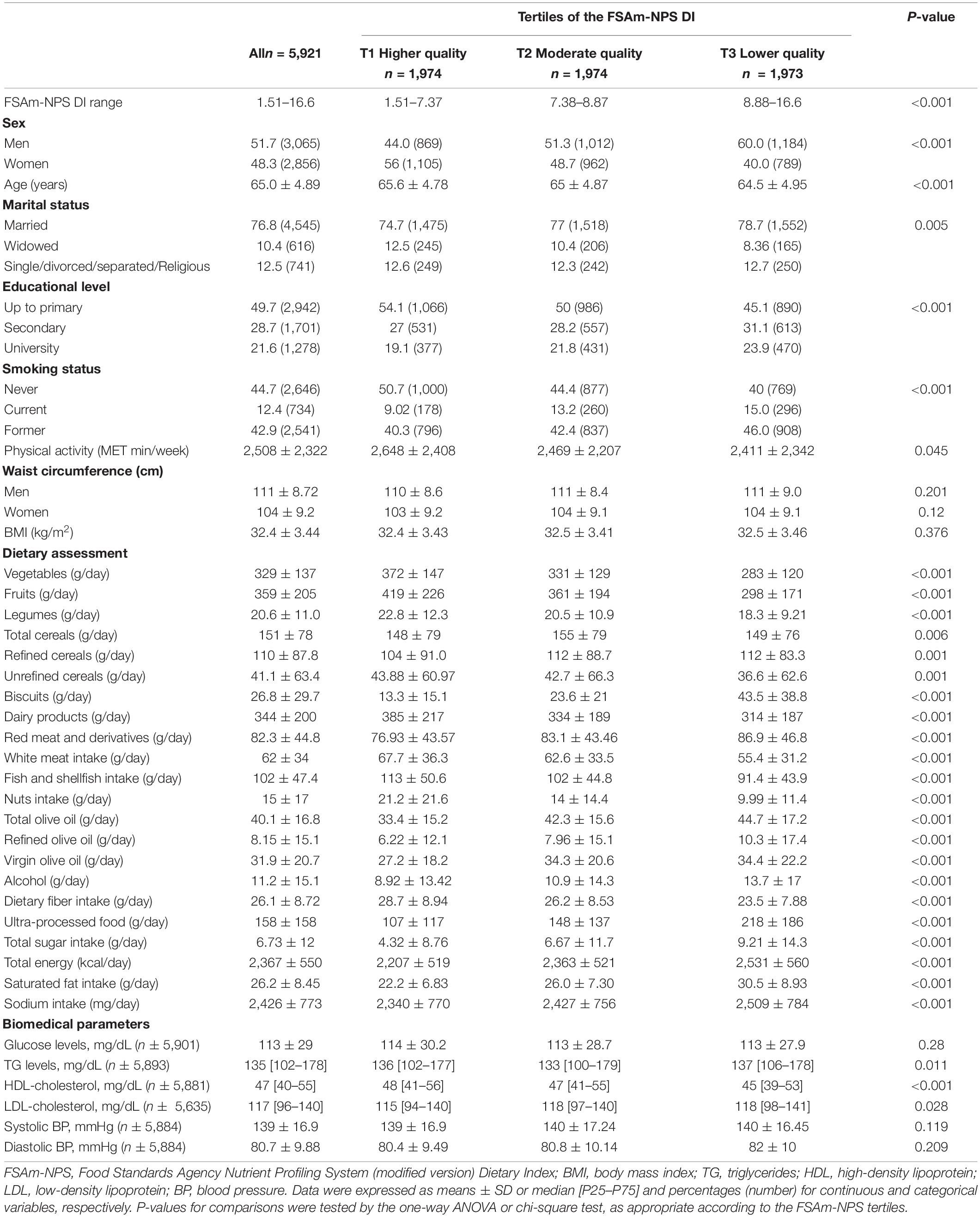
Table 1. Baseline characteristics of participants overall and by tertiles of FSAm-NPS DI score, PREDIMED-plus study.
The cross-sectional association between the FSAm-NPS DI and CVD risk factors at baseline is shown in Table 2. Compared to those participants with a lower FSAm-NPS DI (T1) reflecting a healthier diet, those with a higher FSAm-NPS DI (T3) showed lower HDL-cholesterol levels (β: −0.77 [95% CI = −1.47, −0.06]; P for trend = 0.027). This association was consistent for the HDL-cholesterol and FSAm-NPS DI as a continuous variable (β: −0.21 [95% CI = −0.37, −0.05]). A direct association was observed between the FSAm-NPS DI as continuous and baseline BMI and waist circumference (β: 0.08 [95% CI = 0.03, 0.13] and β: 0.22 [95% CI = 0.09, 0.35], respectively).
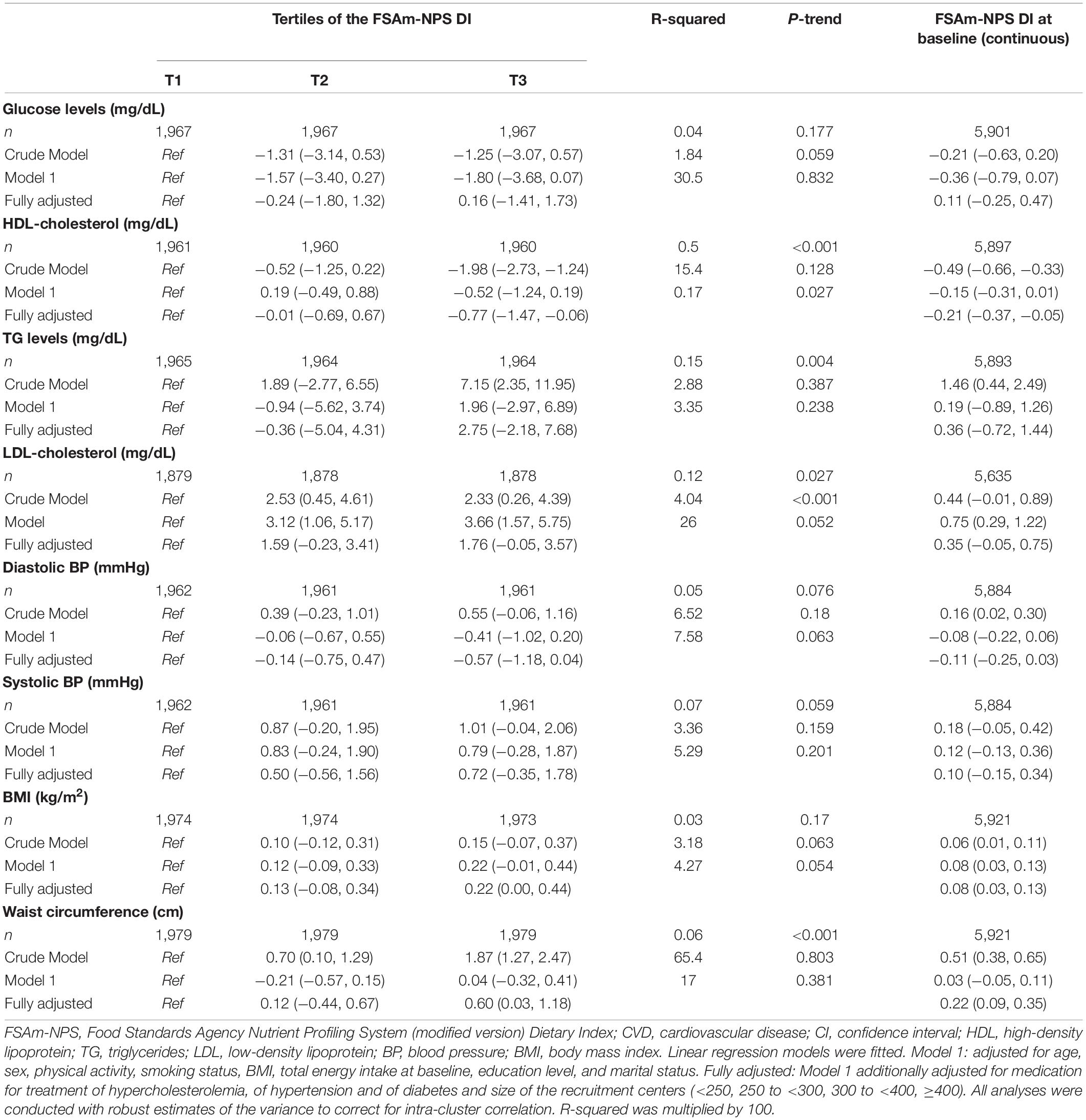
Table 2. Association between FSAm-NPS DI and CVD risk factors at baseline, and β coefficient (95% CI).
Associations between 1 year changes in the FSAm-NPS DI and changes in the CVD risk factors are shown in Table 3. Compared to participants with a score change resulting in a lower FSAm-NPS DI (T1), those participants with a higher FSAm-NPS DI (T3) after 1 year of follow-up showed a significant increase in the levels of plasma glucose, triglycerides, diastolic blood pressure, BMI, and waist circumference (β: 1.67 [95% CI = 0.43, 2.90]; P for trend < 0.001; β: 6.27 [95% CI = 2.46, 10.09]; P for trend < 0.001; β: 0.56 [95% CI = 0.08, 1.05]; P for trend = 0.001; β: 0.51 [95% CI = 0.41, 0.60]; P for trend < 0.001; β: 1.19 [CI = 0.89, 1.50]; P for trend < 0.001, respectively).

Table 3. Association between 1-year change of FSAm-NPS and changes of the CVD risk factors levels after 1 year of follow-up, and β coefficient (95% CI).
In Figure 2, we present the β coefficient (95% CI) for the prospective associations between changes in the FSAm/NPS DI (continuous) and changes in the CVD risk factors after 1 year of follow-up. Consistent with the results described above, positive associations were found between changes in the FSAm-NPS DI and changes in the glucose and triglyceride levels, diastolic blood pressure, BMI, and waist circumference after 1 year of follow-up. Non-significant association was observed in the case of HDL-cholesterol, LDL-cholesterol, and systolic blood pressure changes. Nevertheless, after 1 year of follow-up, 79.36 and 19.4% of the population remained in the recommended levels of HDL and LDL-cholesterol, 12.82 and 8.9% of the participants showed increased levels, and only 7.82 and 10.9% of the participants showed a decrease in HDL-cholesterol or LDL-cholesterol, respectively (data not shown).
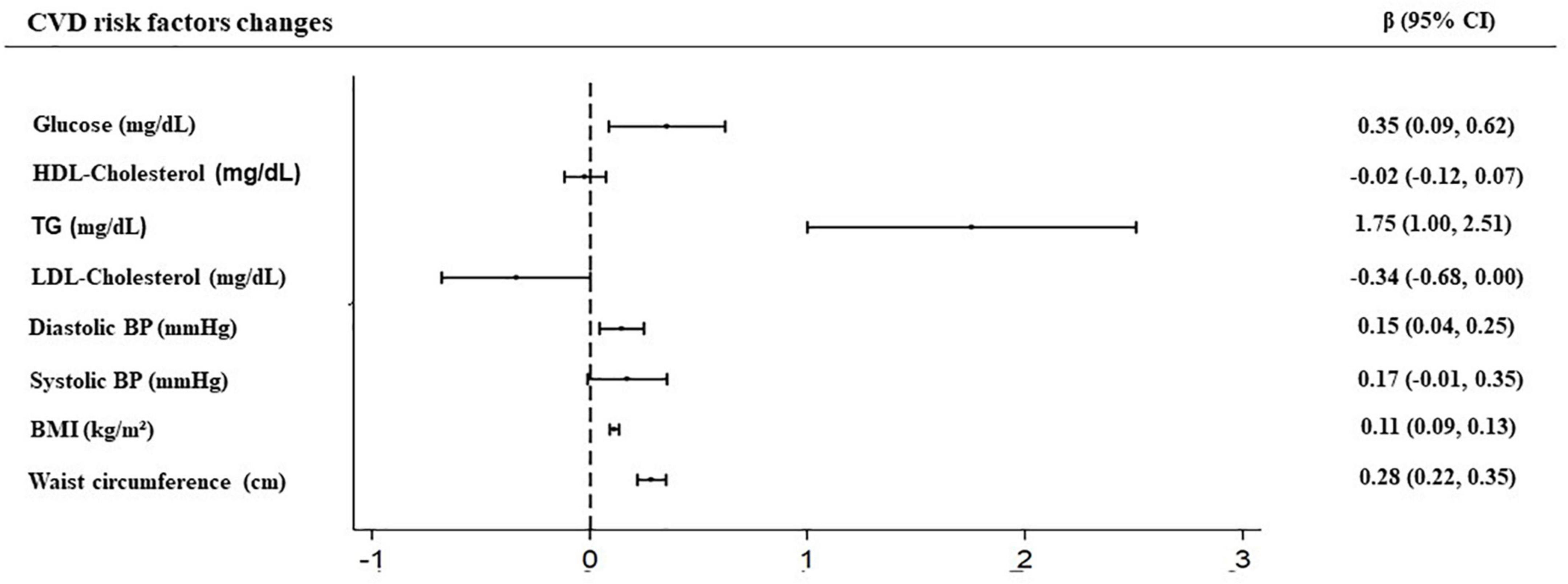
Figure 2. Prospective associations between dietary index based on the French context, the modified FSA-NPS (FSAm-NPS DI) and cardiovascular diseases (CVD) risk factors changes after 1 year of follow-up.
The cross-sectional and longitudinal associations remained significant when olive oil was considered the healthiest food option in the computation of the FSAm-NPS DI (data not shown).
To the best of our knowledge, this study is one of the first to evaluate the prospective associations between the nutritional quality of diet assessed using the FSAm-NPS DI (algorithm underpinning the Nutri-Score FOP label) and different CVD risk factors. Findings of this study showed that the consumption of foods with higher scores of FSAm NPS (foods with less favorable rating in the Nutri-Score scale) was associated with unfavorable changes in CVD risk factors after 1 year of follow-up, specifically with an increase in adiposity (BMI and waist circumference) and the levels of plasma glucose, triglycerides, and diastolic blood pressure.
Our results are partially in line with the SU.VI.MAX study where the authors assessed the prospective association between the FSAm-NPS DI and metabolic syndrome and its components (24). Even though, these authors found significant and positive association between the FSAm-NPS DI and the incidence of metabolic syndrome, when the components were assessed individually, only systolic and diastolic blood pressure showed a significant association. In our study, we also found significant and positive association with diastolic blood pressure, but not for systolic. These results may be explained because the FSAm-NPS DI considers the salt content of food that has been proved to be related to hypertension (31). However, we cannot discard that other factors of the score, as well as their synergistic effect, may also explain these results on blood pressure. In contrast to the SU.VI.MAX study, we have demonstrated significant prospective associations with triglycerides and fasting glucose. These results in relation to triglycerides and glucose may be explained because the participants in our study were elderly Mediterranean individuals (aged between 55 and 75 years) with overweight/obesity and metabolic syndrome. Therefore, as they were already at the risk of CVD, the results of our study could be influenced by their pre-existing risk and conditions. In contrast, in the SU.VI.MAX study, the participants were younger and healthier (women aged between 35 and 60 years and men aged between 45 and 60 years).
In our study, no prospective associations were observed between changes in the FSAm-NPS DI and changes in HDL-cholesterol or LDL-cholesterol concentrations. Even though, in the cross-sectional analysis, we found an association between HDL-cholesterol and FSAm-NPS DI at the baseline, the lack of association in the prospective analysis might be explained because most of the population did not show changes in the levels of HDL-cholesterol after 1 year of follow-up. In a previous study, analysis conducted in the SU.VI.MAX cohort reported a negative association between the FSAm-NPS DI and LDL-cholesterol concentration (16). According to the authors, the absence of association or the negative association observed in the case of the LDL-cholesterol could be partly explained by the fact that, even when saturated fat is considered in the score, the FSAm-NPS DI does not distinguish between fatty acid subtypes (monounsaturated or polyunsaturated fatty acids) (25).
In our study, a higher 1-year increase in the FSAm-NPS, reflecting a decrease in the nutritional quality of diet, was also positively associated with increases in adiposity measured by BMI and waist circumference. These findings are in line with other studies using other nutritional quality indexes (32, 33), and with other two studies analyzing the FSAm-NPS. In the SU.VI.MAX French cohort, a positive association between the FSAm-NPS DI and body weight and BMI gain (24) was found in both men and women. In addition, an increased risk of obesity was observed only in men after 13 years of follow-up. A study using data from the French NutriNet-Santé cohort has recently analyzed the prospective associations between different nutrient profiling systems (the original Food Standards Agency nutrient profiling system and three variants, Food Standards Australia New Zealand Nutrient Profiling Scoring Criterion (NPSC), Health Star Rating NPS and the French NPS (HCSP-NPS), and adiposity markers and overweight/obesity risk. The results showed that participants with a dietary index reflecting lower diet nutritional quality (irrespective of the nutrient profiling used) were more likely to increase the BMI over time and had an increased risk to develop overweight/obesity (34). It is important to remark that whilst differences were small, the French FSAm-NPS one appeared to show a significantly greater association with the risk of overweight compared to other nutrient profile scores. It is important to highlight that the reclassification of olive oil in the FSAm-NPS computation only induced small effects in our study, whereas previous evidence from the SUN cohort found that the reclassification of olive oil strengthened the associations between the FSAm-NPS and total mortality (23).
In the FSAm-NPS, total energy, salt, saturated fat, and sugar are considered negative components whereas fiber, protein, fruits and vegetables, legumes, and some vegetable oils are considered positive. The FSAm-NPS DI resumes the FSAm-NPS scores of all food items mostly consumed by an individual, by assigning points based on the consumption of foods, food groups, or nutrients relevant to the risk of chronic diseases. All these nutrients or food groups have been demonstrated to be related to CVD risk factors in numerous studies (5, 35, 36). Particularly, added sugar and saturated fat have been previously associated with higher levels of fasting blood glucose and triglycerides (37, 38). Therefore, the observed associations are consistent with the nature of the FSAm-NPS and with previous findings regarding diet and CVD.
Furthermore, there is also increasing evidence that ultra-processed foods (UPF) have detrimental effects on CVD risk (39), In this sense, we should bear in mind that the FSAm-NPS DI and the NOVA classification (based on degree of food processing) are two different complementary approaches to assess nutritional quality and healthiness (40). Indeed, in our study, those participants allocated in the highest FSAm-NPS DI tertiles had higher UPF consumption. It is acknowledged that the FSAm-NPS DI does not cover all the health dimensions of food (e.g., food processing, additives, and presence of pesticides). It considers neither the added sugar included in food nor the monounsaturated or polyunsaturated fat because this score has been based on those nutrients that, in Europe, are mandatory to be disclosed in the list of nutrients in the food labeling. However, at the moment, there is no classification system including all these nutrients and dimensions of food in a single indicator. Therefore, FSAm-NPS focuses on the nutritional dimension and serves as the underlying system of some front-of-pack labels to allow consumers to easily compare foods belonging to the same category. Importantly, FSAm-NPS has the advantage of considering a large number of elements from a nutritional point of view, in particular the content, per 100 g of food of fruits and vegetables (proxy of the amount of antioxidants, vitamins, and minerals), legumes, nuts, proteins (e.g., proxy of the amount of calcium and iron), olive oil, rapeseed oil, and walnut oils.
Overall, our results support the suitability of the FSAm-NPS as a nutritional quality indicator aimed at improving diets and preventing the development of chronic diseases. Further prospective studies analyzing the effect of modifying the nutritional quality of diet through changes in this dietary index are warranted in the future to confirm our results.
Our study has several limitations that deserve to be discussed. First, the results cannot be generalized to other populations since participants included in the analysis were elderly Mediterranean individuals with overweight/obesity and metabolic syndrome. Therefore, as they were already at the risk of CVD, the results of this study could be influenced by this condition. Second, the assessment of food intake through a FFQ is prone to possible measurement errors. However, despite this limitation, food-based FFQs have been widely used as a tool in epidemiological studies since the 1990s (41). Third, we cannot rule out bias due to unmeasured potential confounders related to the risk of CVD.
This study also has some strengths such as its prospective design, which reduces the possibility of reverse causation bias, the control for several potential confounding factors, the large sample size, and the extensive data collected by trained staff.
In conclusion, the results of this prospective cohort study suggest that the consumption of foods with higher FSAm-NPS (reflecting a lower nutritional quality) is associated with an increase in some CVD risk factors (adiposity, fasting plasma glucose, triglycerides, and diastolic blood pressure). However, no significant associations were identified for critical CVD risk factors such as HDL-cholesterol, LDL-cholesterol, and systolic blood pressure.
The datasets presented in this article are not readily available because the datasets generated and analyzed during the current study are not publicly available due to data regulations and for ethical reasons, considering that this information might compromise research participants’ consent because our participants only gave their consent for the use of their data by the original team of investigators. However, collaboration for data analyses can be requested by sending a letter to the PREDIMED-Plus Steering Committee (cHJlZGltZWRfcGx1c19zY29tbWl0dGVlQGdvb2dsZWdyb3Vwcy5jb20=). The request will then be passed to all the members of the PREDIMED-Plus Steering Committee for deliberation. Requests to access the datasets should be directed to cHJlZGltZWRfcGx1c19zY29tbWl0dGVlQGdvb2dsZWdyb3Vwcy5jb20=.
The studies involving human participants were reviewed and approved by JW: CEI Provincial de Málaga-Servicio Andaluz de Salud (O01_feb_PR2), José Lapetra: CEI de los Hospitales Universitarios Virgen Macarena y Virgen del Rocío-Servicio Andaluz de Salud (PI13/00673), JAM: CEIC Universidad de Navarra (053/2013), DR: CEI de las Illes Balears – Conselleria de Salut Direcció General de Salut Publica i Consum (IB 2242/14 PI), MF: CEIC Parc de Salut Mar y IDIAP Jordi Gol (PI13/120), JSS: CEIC del Hospital Universitari Sant Joan de Reus y IDIAB Jordi Gol (13-07-25/7proj2), Aurora Bueno: CEI de la Provincia de Granada- Servicio Andaluz de Salud (MAB/BGP/pg), CV: CEIC de la Fundacion Jiménez Díaz (EC 26-14/IIS-FJD), MM-G: CEIC Universidad de Navarra (053/2013), Fernando Aros: CEIC Euskadi (PI2014044), DC: CEIC Corporativo de Atención Primaria de la Comunitat Valenciana (2011-005398-22), LS-M: CEI Humana de la Universidad de las Palmas de Gran Canaria (CEIH-2013-07), XP: CEIC del Hospital de Bellvitge (PR240/13), José López Miranda: CEI de Cordoba-Junta de Salud (3078), José María Ordovás: CEI de la Fundación IMDEA Alimentación (PI-012), PM-M: CEIC Hospital Clínico San Carlos de Madrid-Piloto-CEIC Servicio Madrileño de salud-General (30/15), FT: CEI Provincial de Málaga-Servicio Andaluz de Salud, JT: CEI de las Illes Balears – Conselleria de Salut Direcció General de Salut Publica i Consum (IB 2251/14 PI), JoV: CEIC del Hospital Clínic de Barcelona (HCB/2017/0351), JeV: CEIC del Hospital General Universitario de Alicante (CEIC PI2017/02), M-DR: CEIC de la Investigación Biomédica de Andalucía (CCEIBA), VM: CEI de la Universidad de León (TICA-ULE-014-2015), and Ramon Estruch: CEIC del Hospital Clínic de Barcelona (HCB/2016/0287). The patients/participants provided their written informed consent to participate in this study.
NK, CG-D, MM, JSS, and NB conceived and designed the study. MM, DC, MF, JAM, ÁA-G, JW, JV, DR, FT, JS-L, LS-M, JT, VM, XP, MD-R, PM-M, JVi, CV, LD, and ER conducted data acquisition. NK, CG-D, and NB performed statistical analyses. NK, CG-D, MM, JSS, and NB carried out interpretation of the data for the study. All authors were involved in draft redaction, revision for important intellectual content, read, and approved the final manuscript.
This study was supported by the official Spanish Institutions for Funding Scientific Biomedical Research, CIBER Fisiopatología de la Obesidad y Nutrición (CIBEROBN) and Instituto de Salud Carlos III (ISCIII), through the Fondo de Investigación para la Salud (FIS), which is co-funded by the European Regional Development Fund (six coordinated FIS projects led by JSS and JVi, including the following projects: PI13/00673, PI13/00492, PI13/00272, PI13/01123, PI13/00462, PI13/00233, PI13/02184, PI13/00728, PI13/01090, PI13/01056, PI14/01722, PI14/00636, PI14/00618, PI14/00696, PI14/01206, PI14/01919, PI14/00853, PI14/01374, PI14/00972, PI14/00728, PI14/01471, PI16/00473, PI16/00662, PI16/01873, PI16/01094, PI16/00501, PI16/00533, PI16/00381, PI16/00366, PI16/01522, PI16/01120, PI17/00764, PI17/01183, PI17/00855, PI17/01347, PI17/00525, PI17/01827, PI17/00532, PI17/00215, PI17/01441, PI17/00508, PI17/01732, PI17/00926, PI19/00957, PI19/00386, PI19/00309, PI19/01032, PI19/00576, PI19/00017, PI19/01226, PI19/00781, PI19/01560, PI19/01332, PI20/01802, PI20/00138, PI20/01532, PI20/00456, PI20/00339, PI20/00557, PI20/00886, and PI20/01158); the Especial Action Project entitled: Implementación y evaluación de una intervención intensiva sobre la actividad física Cohorte PREDIMED-Plus grant to JSS; the European Research Council (Advanced Research Grant 2014–2019; agreement #340918) granted to MM-G; the Recercaixa (number 2013ACUP00194) grant to JSS; grants from the Consejería de Salud de la Junta de Andalucía (PI0458/2013, PS0358/2016, and PI0137/2018); the PROMETEO/21/2021 grant from the Generalitat Valenciana; the SEMERGEN grant; None of the funding sources took part in the design, collection, analysis, interpretation of the data, or writing the report, or in the decision to submit the manuscript for publication. JSS senior author, gratefully acknowledges the financial support by ICREA under the ICREA Academia program. NK was funded by a research grant from the Agència de Gestió d’Ajuts Universitaris de Recerca (AGAUR FI, record number: 2021FI_B 00145). MM was funded by Sara Borrell (CD21/00045).
JSS served on the board of the International Nut and Dried Fruit Council and receives grant support through this institution. He also served in the Executive Committee of the Instituto Danone, Spain, and on the Scientific Committee of the Danone International Institute. He received research support from the Patrimonio Comunal Olivarero, Spain, and Borges S.A., Spain. He received consulting fees or travel expenses from Eroski Foundation, the Instituto Danone, Spain, Mundipharma and Abbot Laboratories. ER reports grants, personal fees, non-financial support, and others from California Walnut Commission and Alexion, personal fees, non-financial support, and others from Ferrer International and Danone, and personal fees from Amarin, other than the submitted study.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We would like to thank the PREDIMED-Plus participants for their enthusiastic collaboration, the PREDIMED-Plus personnel for their outstanding support, and staff of all associated primary care centers for their exceptional study. CIBEROBN, CIBERESP, and CIBERDEM are initiatives of the Carlos III Health Institute, Spain. We would also like to thank the PREDIMED-Plus Biobank Network, which is part of the National Biobank Platform of the Carlos III Health Institute for storing and managing the biological samples.
1. Nichols M, Townsend N, Scarborough P, Rayner M. Cardiovascular disease in Europe: epidemiological update. Eur Heart J. (2013) 34:3028–34. doi: 10.1093/EURHEARTJ/EHT356
2. Townsend N, Nichols M, Scarborough P, Rayner M. Cardiovascular disease in Europe–epidemiological update 2015. Eur Heart J. (2015) 36:2696–705. doi: 10.1093/EURHEARTJ/EHV428
3. WHO. Cardiovascular Diseases (CVDs). (2022). Available online at: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds) (accessed February 9, 2022).
4. Willett WC, Koplan JP, Nugent R, Dusenbury C, Puska P, Gaziano TA. Prevention of Chronic Disease by Means of Diet and Lifestyle Changes. Dis Control Priorities Dev Ctries. (2006). Available online at: https://www.ncbi.nlm.nih.gov/books/NBK11795/ (accessed February 9, 2022).
5. Joint WHO/FAO Expert Consultation. Diet, Nutrition and the Prevention of Chronic Diseases. Geneva: WHO (2003).
6. Jones A, Neal B, Reeve B, Ni Mhurchu C, Thow AM. Front-of-pack nutrition labelling to promote healthier diets: current practice and opportunities to strengthen regulation worldwide. BMJ Glob Health. (2019) 4:1–16. doi: 10.1136/bmjgh-2019-001882
7. FAO. FAOLEX Database. (2022). Available online at: https://www.fao.org/faolex/results/details/en/c/LEX-FAOC128444/ (accessed February 9, 2022).
8. Egnell M, Talati Z, Gombaud M, Galan P, Hercberg S, Pettigrew S, et al. Consumers’ responses to front-of-pack nutrition labelling: results from a sample from the Netherlands. Nutrients. (2019) 11:1817. doi: 10.3390/NU11081817
9. Martini D, Menozzi D. Food labeling: analysis, understanding, and perception. Nutrients. (2021) 13:268. doi: 10.3390/NU13010268
10. Kristal AR, Levy L, Patterson RE, Li SS, White E. Trends in food label use associated with new nutrition labeling regulations. Am J Public Health. (1998) 88:1212–5. doi: 10.2105/AJPH.88.8.1212
11. Roodenburg AJC, Popkin BM, Seidell JC. Development of international criteria for a front of package food labelling system: the international choices programme. Eur J Clin Nutr. (2011) 65:1190–200. doi: 10.1038/ejcn.2011.101
12. Alrige MA, Chatterjee S, Medina E, Nuval J. Applying the concept of nutrient-profiling to promote healthy eating and raise individuals’ awareness of the nutritional quality of their food. AMIA Annu Symp Proc. (2017) 2017:393–402.
13. Arambepola C, Scarborough P, Rayner M. Validating a nutrient profile model. Public Health Nutr. (2008) 11:371–8. doi: 10.1017/S1368980007000377
14. Rayner M, Scarborough P, Heart B, Health F. The UK Ofcom Nutrient Profiling Model Defining “Healthy” and “Unhealthy” Foods and Drinks for TV Advertising to Children. London: International Obesity Task Force (2009).
15. Julia C, Touvier M, Méjean C, Ducrot P, Péneau S, Hercberg S, et al. Development and validation of an individual dietary index based on the British food standard agency nutrient profiling system in a French context. J Nutr. (2014) 144:2009–17. doi: 10.3945/jn.114.199679
16. Julia C, Méjean C, Touvier M, Péneau S, Lassale C, Ducrot P, et al. Validation of the FSA nutrient profiling system dietary index in French adults-findings from SUVIMAX study. Eur J Nutr. (2016) 55:1901–10. doi: 10.1007/S00394-015-1006-Y
17. Szabo De Edelenyi F, Egnell M, Galan P, Druesne-Pecollo N, Hercberg S, Julia C. Ability of the Nutri-Score front-of-pack nutrition label to discriminate the nutritional quality of foods in the German food market and consistency with nutritional recommendations. Arch Public Health. (2019) 77:1–9. doi: 10.1186/S13690-019-0357-X/FIGURES/6
18. Dubois P, Albuquerque P, Allais O, Bonnet C, Bertail P, Combris P, et al. Effects of front-of-pack labels on the nutritional quality of supermarket food purchases: evidence from a large-scale randomized controlled trial. J Acad Mark Sci. (2021) 49:119–38. doi: 10.1007/S11747-020-00723-5
19. Deschasaux M, Huybrechts I, Murphy N, Julia C, Hercberg S, Srour B, et al. Nutritional quality of food as represented by the FSAm-NPS nutrient profiling system underlying the Nutri-Score label and cancer risk in Europe: results from the EPIC prospective cohort study. PLoS Med. (2018) 15:e1002651. doi: 10.1371/JOURNAL.PMED.1002651
20. Adriouch S, Julia C, Kesse-Guyot E, Ducrot P, Péneau S, Méjean C, et al. Association between a dietary quality index based on the food standard agency nutrient profiling system and cardiovascular disease risk among French adults. Int J Cardiol. (2017) 234:22–7. doi: 10.1016/J.IJCARD.2017.02.092
21. Deschasaux M, Huybrechts I, Julia C, Hercberg S, Egnell M, Srour B, et al. Association between nutritional profiles of foods underlying Nutri-Score front-of-pack labels and mortality: EPIC cohort study in 10 European countries. BMJ. (2020) 370:3173. doi: 10.1136/BMJ.M3173
22. Donat-Vargas C, Sandoval-Insausti H, Rey-García J, Ramón Banegas J, Rodríguez-Artalejo F, Guallar-Castillón P. Five-color Nutri-Score labeling and mortality risk in a nationwide, population-based cohort in Spain: the study on nutrition and cardiovascular risk in Spain (ENRICA). Am J Clin Nutr. (2021) 113:1301–11. doi: 10.1093/AJCN/NQAA389
23. Gómez-Donoso C, Martínez-González MÁ, Perez-Cornago A, Sayón-Orea C, Martínez JA, Bes-Rastrollo M. Association between the nutrient profile system underpinning the Nutri-Score front-of-pack nutrition label and mortality in the SUN project: a prospective cohort study. Clin Nutr. (2021) 40:1085–94. doi: 10.1016/j.clnu.2020.07.008
24. Julia C, Ducrot P, Lassale C, Fézeu L, Méjean C, Péneau S, et al. Prospective associations between a dietary index based on the British food standard agency nutrient profiling system and 13-year weight gain in the SU.VI.MAX cohort. Prev Med (Baltim). (2015) 81:189–94. doi: 10.1016/j.ypmed.2015.08.022
25. Julia C, Fézeu LK, Ducrot P, Méjean C, Peneau S, Touvier M, et al. The nutrient profile of foods consumed using the British food standards agency nutrient profiling system is associated with metabolic syndrome in the SU.VI.MAX cohort1-3. J Nutr. (2015) 145:2355–61. doi: 10.3945/jn.115.213629
26. Martínez-González MA, Buil-Cosiales P, Corella D, Bulló M, Fitó M, Vioque J, et al. Cohort profile: design and methods of the PREDIMED-Plus randomized trial. Int J Epidemiol. (2019) 48:387–8o. doi: 10.1093/ije/dyy225
27. De La Fuente-Arrillaga C, Vzquez Ruiz Z, Bes-Rastrollo M, Sampson L, Martinez-González MA. Reproducibility of an FFQ validated in Spain. Public Health Nutr. (2010) 13:1364–72. doi: 10.1017/S1368980009993065
28. Moreiras O, Carbajal A, Cabrera L, Cuadrado C. Tablas de Composicion de Alimentos (Ciencia Y Tecnica). 16th ed. Madrid: Ediciones Pirámide (2013).
29. Haut Conseil de la Santé Publique. On Information Regarding the Nutritional Quality of Foodstuffs. (2022). Available online at: https://www.hcsp.fr/explore.cgi/avisrapportsdomaine?clefr=524 (accessed February 10, 2022).
30. Molina L, Sarmiento M, Peñafiel J, Donaire D, Garcia-Aymerich J, Gomez M, et al. Validation of the regicor short physical activity questionnaire for the adult population. PLoS One. (2017) 12:e0168148.
31. Law MR, Frost CD, Wald NJ. By how much does dietary salt reduction lower blood pressure? III–analysis of data from trials of salt reduction. BMJ. (1991) 302:819–24. doi: 10.1136/BMJ.302.6780.819
32. Carruba MO, Caretto A, De Lorenzo A, Fatati G, Ghiselli A, Lucchin L, et al. Front-of-pack (FOP) labelling systems to improve the quality of nutrition information to prevent obesity: NutrInform battery vs Nutri-Score. Eat Weight Disord. (2021). 27(5):1575–1584. doi: 10.1007/S40519-021-01316-Z
33. Egnell M, Seconda L, Neal B, Mhurchu CN, Rayner M, Jones A, et al. Prospective associations of the original food standards agency nutrient profiling system and three variants with weight gain, overweight and obesity risk: results from the French NutriNet-Santé cohort. Br J Nutr. (2021) 125:902–14. doi: 10.1017/S0007114520003384
34. Rimm EB, Ascherio A, Giovannucci E, Spiegelman D, Stampfer MJ, Willett WC, et al. Vegetable, fruit, and cereal fiber intake and risk of coronary heart disease among men however, Trowell and Burkitt5 sug-from the departments of epidemiology Drs. JAMA. (1996) 275:447–51.
35. Rank F, Eir M, Tampfer JS, Nn JOA, Anson EM, Imm RR, et al. Dietary fat intake and the risk of coronary heart disease in women. N Engl J Med. (1997) 337:1491–9.
36. Truswell AS. Cereal grains and coronary heart disease. Eur J Clin Nutr. (2002) 56:1–14. doi: 10.1038/SJ.EJCN.1601283
37. Mensink RP, Katan MB. Effect of dietary fatty acids on serum lipids and lipoproteins. A meta-analysis of 27 trials. Arterioscler Thromb J Vasc Biol. (1992) 12:911–9. doi: 10.1161/01.ATV.12.8.911
38. Zimmet P. Epidemiology of diabetes mellitus and associated cardiovascular risk factors: focus on human immunodeficiency virus and psychiatric disorders. Am J Med. (2005) 118(Suppl. 2):3S–8S. doi: 10.1016/J.AMJMED.2005.01.044
39. Lane MM, Davis JA, Beattie S, Gómez-Donoso C, Loughman A, O’Neil A, et al. Ultraprocessed food and chronic noncommunicable diseases: a systematic review and meta-analysis of 43 observational studies. Obes Rev. (2021) 22:1–19. doi: 10.1111/obr.13146
40. Romero Ferreiro C, Lora Pablos D, Gómez de la Cámara A. Two dimensions of nutritional value: Nutri-Score and Nova. Nutrients. (2021) 13:2783. doi: 10.3390/nu13082783
Keywords: front of pack food labeling, cardiovascular risk factor, body weight, FSAm-NPS dietary index, PREDIMED-Plus study
Citation: Khoury N, Gómez-Donoso C, Martínez MÁ, Martínez-González MÁ, Corella D, Fitó M, Martínez JA, Alonso-Gómez ÁM, Wärnberg J, Vioque J, Romaguera D, León-Acuña A, Tinahones FJ, Santos-Lozano JM, Serra-Majem L, Massó Guijarro P, Tur JA, Martín Sánchez V, Pintó X, Delgado-Rodríguez M, Matía-Martín P, Vidal J, Vázquez C, Daimiel L, Ros E, Bes-Rastrollo M, Barragan R, Castañer O, Torres-Peña JD, Notario-Barandiaran L, Muñoz-Bravo C, Abete I, Prohens L, Cano-Ibáñez N, Tojal Sierra L, Fernández-García JC, Sayon-Orea C, Pascual M, Sorli JV, Zomeño D, Peña-Orihuela PJ, Signes-Pastor AJ, Basterra-Gortari FJ, Schröeder H, Salas Salvadó J and Babio N (2022) Associations Between the Modified Food Standard Agency Nutrient Profiling System Dietary Index and Cardiovascular Risk Factors in an Elderly Population. Front. Nutr. 9:897089. doi: 10.3389/fnut.2022.897089
Received: 15 March 2022; Accepted: 22 June 2022;
Published: 14 July 2022.
Edited by:
Xiongfei Pan, Sichuan University, ChinaReviewed by:
Amanda Grech, The University of Sydney, AustraliaCopyright © 2022 Khoury, Gómez-Donoso, Martínez, Martínez-González, Corella, Fitó, Martínez, Alonso-Gómez, Wärnberg, Vioque, Romaguera, León-Acuña, Tinahones, Santos-Lozano, Serra-Majem, Massó Guijarro, Tur, Martín Sánchez, Pintó, Delgado-Rodríguez, Matía-Martín, Vidal, Vázquez, Daimiel, Ros, Bes-Rastrollo, Barragan, Castañer, Torres-Peña, Notario-Barandiaran, Muñoz-Bravo, Abete, Prohens, Cano-Ibáñez, Tojal Sierra, Fernández-García, Sayon-Orea, Pascual, Sorli, Zomeño, Peña-Orihuela, Signes-Pastor, Basterra-Gortari, Schröeder, Salas Salvadó and Babio. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Nancy Babio, bmFuY3kuYmFiaW9AdXJ2LmNhdA==; Jordi Salas Salvadó, am9yZGkuc2FsYXNAdXJ2LmNhdA==
†These authors have contributed equally to this work
‡These authors share senior authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.