
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Nutr., 25 April 2022
Sec. Nutritional Epidemiology
Volume 9 - 2022 | https://doi.org/10.3389/fnut.2022.875607
This article is part of the Research TopicRole of Toxicants, Pollutants, and Trace Elements in Health and NutritionView all 6 articles
 Tommaso Filippini1
Tommaso Filippini1 Thorhallur I. Halldorsson2,3Carolina Capitão4,5Raquel Martins4,5
Thorhallur I. Halldorsson2,3Carolina Capitão4,5Raquel Martins4,5 Konstantinos Giannakou6,7Janneke Hogervorst8
Konstantinos Giannakou6,7Janneke Hogervorst8 Marco Vinceti1,9Agneta Åkesson10
Marco Vinceti1,9Agneta Åkesson10 Karin Leander10
Karin Leander10 Andromachi Katsonouri6Osvaldo Santos4,5,11
Andromachi Katsonouri6Osvaldo Santos4,5,11 Ana Virgolino4,5
Ana Virgolino4,5 Federica Laguzzi10*
Federica Laguzzi10*
Diet is a main source of acrylamide exposure to humans. Existing observational data on the relationship between dietary exposure to acrylamide and risk of cancer are inconsistent. We performed a systematic review and dose-response meta-analysis of epidemiological studies evaluating the association between dietary acrylamide exposure and several site-specific cancer. A systematic literature search was conducted in PubMed, Scopus, and Web of Science databases until March 7, 2022. Studies were eligible if they were carried out in non-occupationally exposed adults, assessed dietary acrylamide exposure (μg/day) and reported risk estimates of cancer incidence (all but gynecological cancers). Using a random-effects model, we performed a meta-analysis of site-specific cancer risk comparing the highest vs. lowest category of dietary acrylamide exposure. We also carried out a one-stage dose-response meta-analysis assessing the shape of the association. Out of 1,994 papers screened, 31 were eligible (total of 16 studies), which included 1,151,189 participants in total, out of whom 48,175 developed cancer during the median follow-up period of 14.9 years (range 7.3–33.9). The mean estimated dose of dietary acrylamide across studies was 23 μg/day. Pooled analysis showed no association between the highest vs. lowest dietary acrylamide exposure and each site-specific cancer investigated, with no evidence of thresholds in the dose-response meta-analysis. There were also no associations between dietary acrylamide exposure and the risk of cancers when stratifying by smoking status, except for increased risk of lung cancer in smokers. In conclusion, high dietary acrylamide exposure was not associated with an increased risk of site-specific non-gynecological cancer.
Acrylamide is a chemical compound mainly used in industry to produce polyacrylamides that are employed for different purposes such as flocculants, dyes, paper, and textiles. Beside the potential exposure of acrylamide in the occupational setting, the main sources of exposure to this substance in the general population is through the intake of certain foods, high in carbohydrates cooked at temperatures >120°C, especially in low moisture conditions (1). Acrylamide may also be formed in foods from acrolein, a compound produced during the degradation of amino acids, carbohydrates, lipids, and organic acids (2). The content of acrylamide in foods varies largely, depending on the food matrix and the food processing method. Thus, dietary exposure to acrylamide differs across countries and global geographical areas, due to distinct traditional diets and its culinary habits (3). Tobacco smoke is also a source of acrylamide, making smokers potentially exposed to higher levels of acrylamide compared to non-smokers (4, 5). Smokers have been shown to have, on average, three to four times higher levels of acrylamide biomarkers (i.e., hemoglobin adducts) compared to non-smokers (6). Additional sources of exposure to acrylamide take place in occupational settings, where an association to neurological alterations has been shown (7).
Acrylamide is classified as probably carcinogenic to humans (class 2A) by the International Agency for Research on Cancer (IARC) (8). However, the underlying mechanisms of the carcinogenicity of acrylamide are far from being understood. Still, experimental evidence has shown that the main metabolite of acrylamide, glycidamide, is genotoxic—highly reactive toward DNA and proteins (9, 10). A study found a glycidamide-related mutational signature in one-third of approximately 1,600 human tumor genomes corresponding to 19 types of cancer (11). Non-genotoxic modes of action of acrylamide involving, for instance, hormonal pathways, are also proposed as underlying mechanisms of carcinogenicity, driving cell transformation or proliferation and apoptosis, independently of acrylamide-induced genotoxicity (9).
Although in vitro and animal studies have consistently shown that acrylamide is genotoxic, mutagenic, and carcinogenic (9, 12), epidemiological studies investigating the relationship between high dietary acrylamide exposure and the risk of several site-specific cancer (e.g., prostate, gastrointestinal and lung) in the general population and in occupational settings have reported inconsistent results, with some studies pointing to an increased risk (13–19) and others to null association (3, 17, 18, 20–41). All of these studies used a dietary assessment method to estimate dietary acrylamide exposure except for one study performed in a Swedish population where acrylamide exposure was assessed through both dietary intake and hemoglobin adducts (20). So far, a few systematic reviews and meta-analyses based on epidemiological studies were performed to synthesize the body of evidence in this field (42–48). In the most recent and comprehensive meta-analysis published in 2015, no association between high dietary acrylamide exposure and the risk of several cancers was noted, except for a modest increased risk of renal cancer (46), which was not observed in another meta-analysis investigating dietary acrylamide exposure and renal cell carcinoma (44). With the exception of a recent study investigating the relationship between dietary acrylamide exposure and female reproductive cancers, observing a relatively linear increased risk for ovarian and endometrial cancer (42), no dose-response meta-analysis exist for other cancer forms.
Hence, we aimed to synthesize the results on the association between dietary acrylamide exposure and risk of site-specific cancer. For this purpose, we performed a systematic literature review and dose-response meta-analysis of epidemiological studies evaluating the association between acrylamide and the risk of several site-specific cancer.
We performed a systematic literature review following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (49) and the Meta-analysis Of Observational Studies in Epidemiology (MOOSE) guidelines (50). Two researchers (C.C. and R.M.) independently searched PubMed, Scopus, and Web of Science databases. A pairwise combination of two sets of terms [medical subject headings (MeSH) terms, whenever possible] were used, being then adapted for each database. One set included terms regarding the exposure to acrylamide and the other to the health outcomes under study. The protocol with the detailed search strategy used for each database, including the PICOS tool can be found in Supplementary Table 1. The literature searches were restricted to English language publications with no time limitation (up till the moment of the search, on March 7, 2022), or any other filter. An additional manual search was performed by screening the references of the included papers of individual studies.
Prospective and retrospective cohort, case-cohort and case-control studies performed in non-occupationally exposed adults (≥18 years) with acrylamide exposure assessed through diet were considered for inclusion. The included papers reported risk estimates [risk ratio (RR), hazard ratio (HR) or odds ratio (OR)] with corresponding 95% confidence intervals (CIs) for any type of cancer in relation to dietary acrylamide exposure, except for the female reproductive cancers (see section “Exclusion Criteria”). Regarding exposure, eligible studies reported acrylamide exposure as continuous and/or categories (i.e., quintiles, quartiles, or tertiles). We considered for inclusion studies reporting number of cases, participants, or person-years per dietary acrylamide category. Studies were included when estimates were adjusted at least for smoking status since smoking has been observed to increase the level of acrylamide, could covary with the consumption of foods high in acrylamide, and is a risk factor for many of the cancer forms under study.
Studies investigating breast, endometrial or ovarian cancers were excluded, as these outcomes were part of a recently published dose-response meta-analysis (42).
All references resulting from the search were downloaded and duplicates were removed. Titles and abstracts retrieved were independently screened for eligibility by two teams of two authors (T.I.H., C.C., R.M., and A.V.). Disagreements were solved by a third author (T.F.). In case of missing information for the meta-analysis, the corresponding author of the paper was contacted for clarification. If no additional information was gathered, the paper was excluded.
Data from each selected paper were extracted by one of the research team members and independently checked by a second one (T.F., C.C., R.M., A.V., and F.L.). The following data were extracted: author, year of publication, type of study design, country including the geographical area, year of the baseline assessment, follow-up time, age, sex, smoking status, doses of acrylamide exposure (mean and/or median; according to what was available), number of cases, number of participants, person-years, risk estimates, and list of the confounders which were adjusted for. The risk estimates with their 95% confidence intervals were extracted from the model adjusted for smoking and the greatest number of other covariables.
The median or mean diet acrylamide exposure in each exposure category was assigned to the corresponding relative risk (RR), hazard ratio (HR), or odds ratio (OR). If the average intake in each category of exposure was not reported, the midpoint of the upper and lower boundaries of the category was assigned as the average intake. If the upper bound of the highest category or the lowest bound of the lowest category were not reported, they have been estimated using minus/plus 20% of the lower or higher open boundaries, respectively. For the RR reported for each quintile but with no respective intakes reported, the values were calculated under the assumption of a normal distribution using the mean, standard deviation, and zeta for each quintile considered (X-SD*Z quintile).
Any site-specific cancer (except for female reproductive cancers) previously investigated in relation to dietary acrylamide exposure was included in the analysis.
The risk of bias was assessed by C.C., R.M., and A.V. using the Cochrane Collaboration tool for assessing risk of bias in non-randomized studies of interventions (ROBINS-I) (51). Risk of bias for each of the six ROBINS-I domains was classified as low, moderate, serious, critical or with lack of information (“no information”). The assessment within each of the six domains was used to determine an overall risk of bias for the outcome under assessment.
We employed a restricted maximum likelihood random-effects meta-analysis to assess summary RR along with 95% confidence interval (CI) for high dietary acrylamide exposure in comparison to low dietary exposure for each site-specific cancer, when at least two risk estimates were available on the same outcome.
A dose-response meta-analysis of the association between dietary acrylamide exposure and site-specific cancer was performed using the one-stage approach recently employed in other research fields (52, 53). Potential non-linear associations were evaluated using cubic splines with knots at 3 fixed points (10th, 50th, and 90th percentiles) of the exposure through a multivariate random-effects meta-analysis using the restricted maximum likelihood method (54). The reference value for the dose-response meta-analysis was set at the mean value of all the included studies, i.e., 23 μg/day. We also fitted a linear regression model reporting its slope alongside the non-linear relationship yielded by the spline analysis.
Additional analyses were conducted stratifying by geographical area (West and East) due to potential differences in the dietary exposure to acrylamide across countries (3), and smoking status since smokers have been shown to have higher levels of acrylamide than never smokers (55).
We assessed the possible presence of publication bias and small-study bias using funnel plots and Egger’s regression asymmetry test for studies reporting highest vs. lowest exposure when at least five studies evaluated the same outcome (56, 57). We also assessed heterogeneity using the I2 statistic, and through the evaluation of the effect of variation across studies using a graphical overlay of study-specific predicted curves (58). All statistical analyses were conducted with STATA, version 17.0 (Stata Corp., College Station, TX, United States, 2021).
Out of 1,994 papers retrieved through the literature and manual search, we identified 31 papers that met the inclusion criteria, corresponding to a total of 16 studies. Detailed information on the selection of the studies included is presented in Figure 1. Descriptive characteristics of the studies included are presented in Table 1. Most studies were performed in Europe (n = 21), primarily in the Netherlands (n = 8) and Sweden (n = 7), followed by Japan (n = 6) and the United States (n = 3). A total of 1,151,189 participants were included in these case-control, case-cohort, and cohort studies. Participants’ age ranged from 50 to 70 years (mean: 60 years). During a median follow-up period of 14.9 years (range: 7.3–33.9 years), 48,175 participants developed cancer. The following site-specific cancer were investigated in the papers in relation to dietary acrylamide exposure: oral cavity, esophageal, stomach, colorectal (including colon and rectal), pancreatic, laryngeal, lung, lymphoma, multiple myeloma, renal, bladder/urothelial, prostate, melanoma, and brain. Dietary acrylamide was assessed through food frequency questionnaires in all the analyzed studies. The mean and median estimated dose of dietary acrylamide across studies was 23 μg/day.
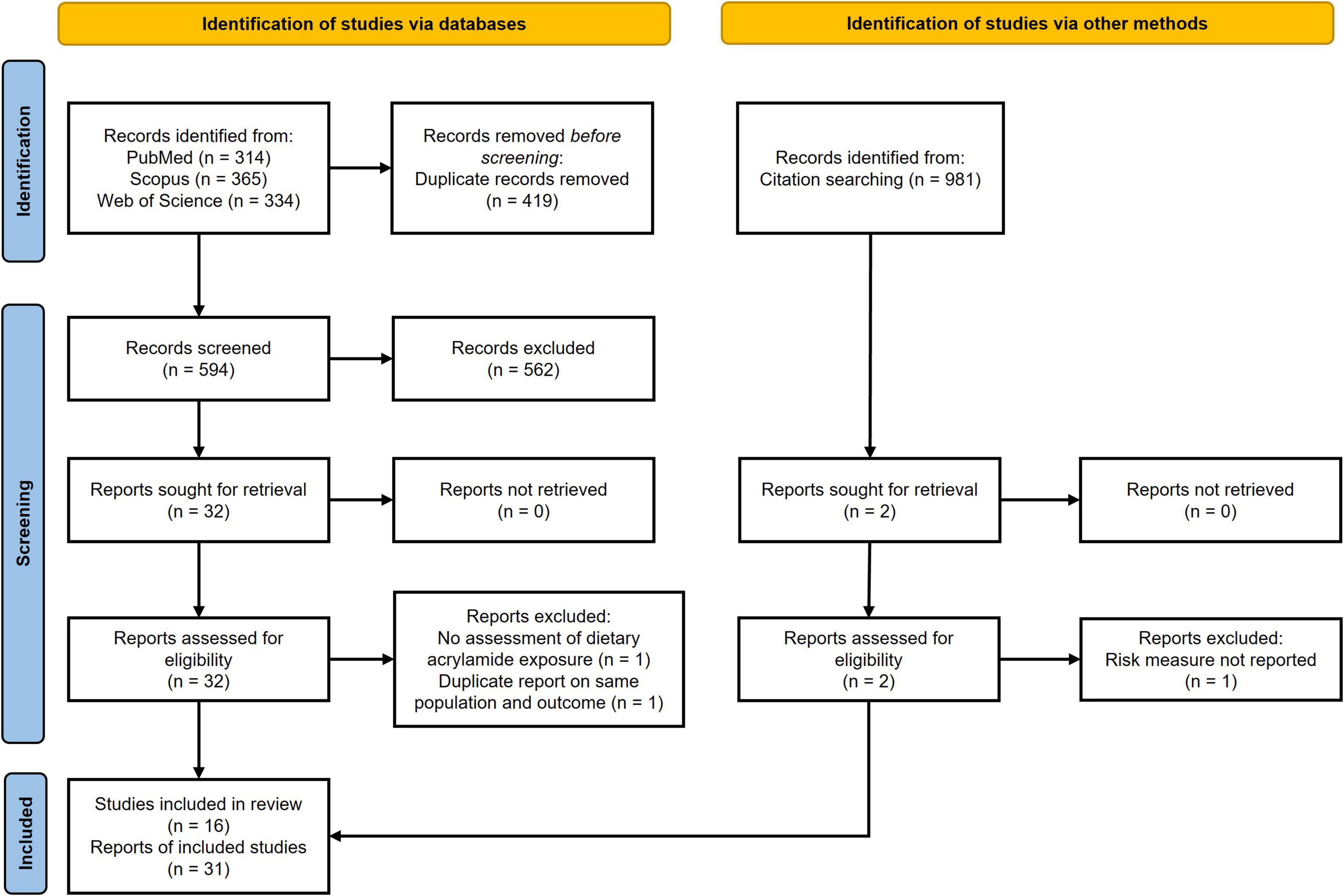
Figure 1. Flow chart of the included study following PRISMA guidelines.
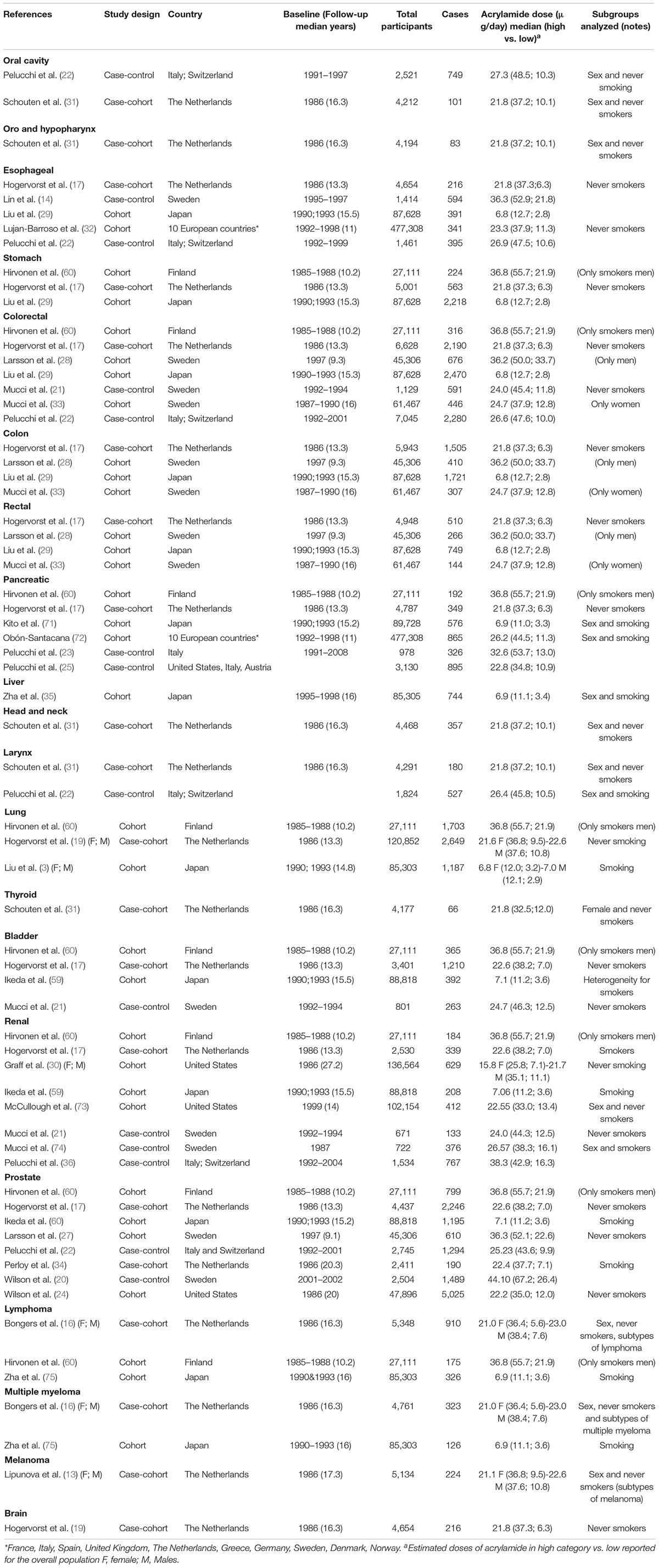
Table 1. Descriptive characteristics of the included studies by site-specific cancer.
Summary estimates for the association between highest vs. lowest dietary acrylamide exposure and the risk of various types of cancer in smokers and never smokers combined, and by smoking status, are shown in Table 2 and in forest plots (Supplementary Figures 1–15). Regardless smoking status, summary estimates showed no association between higher dietary acrylamide and any of the site-specific cancer investigated.
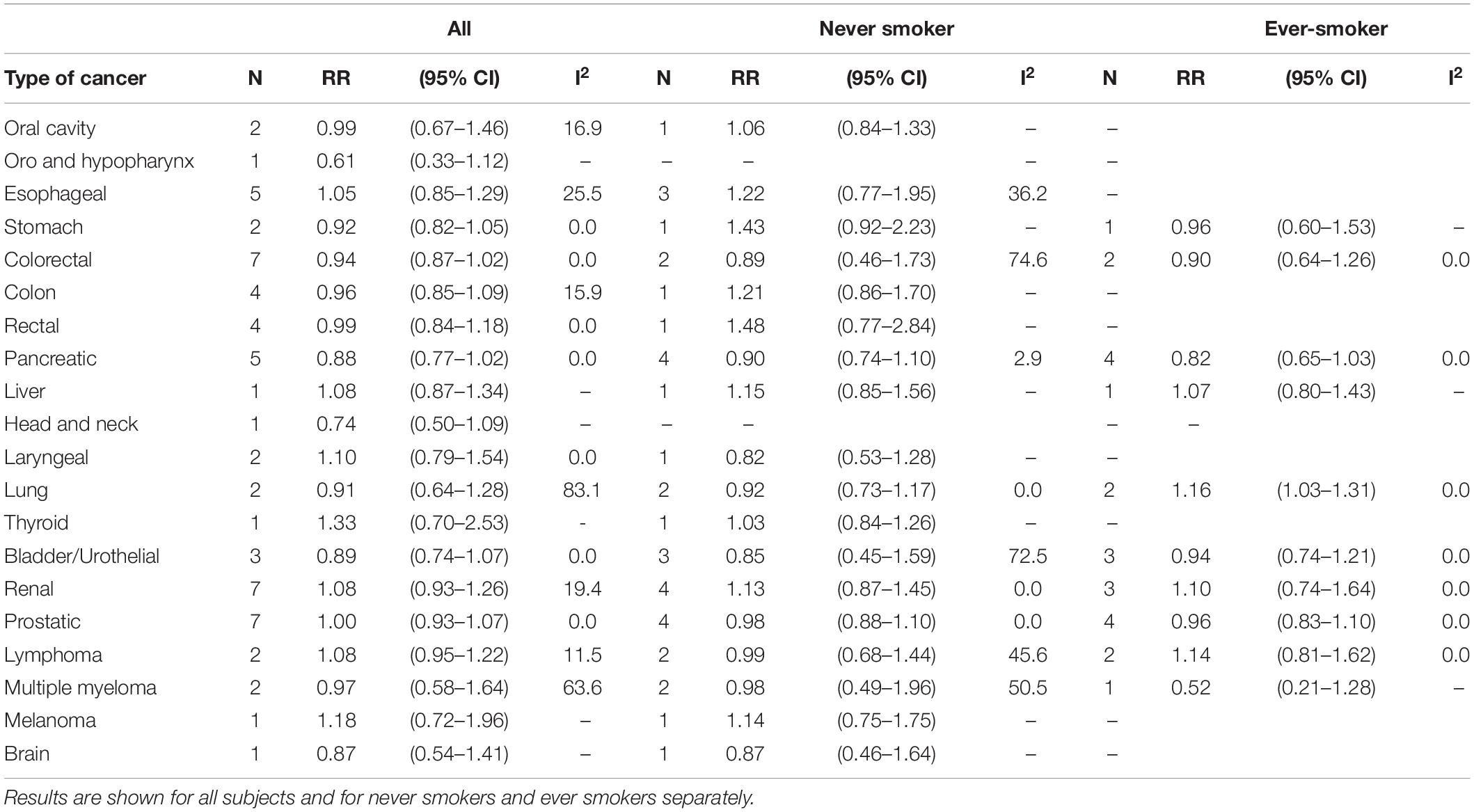
Table 2. Summary relative risk (RR) with 95% confidence interval (CI) of the association between high dietary acrylamide exposure and site-specific cancer.
Results from the dose-response analysis showed a null association with no thresholds for all site-specific cancer considered in relation to increasing levels of dietary acrylamide (Figures 2, 3).
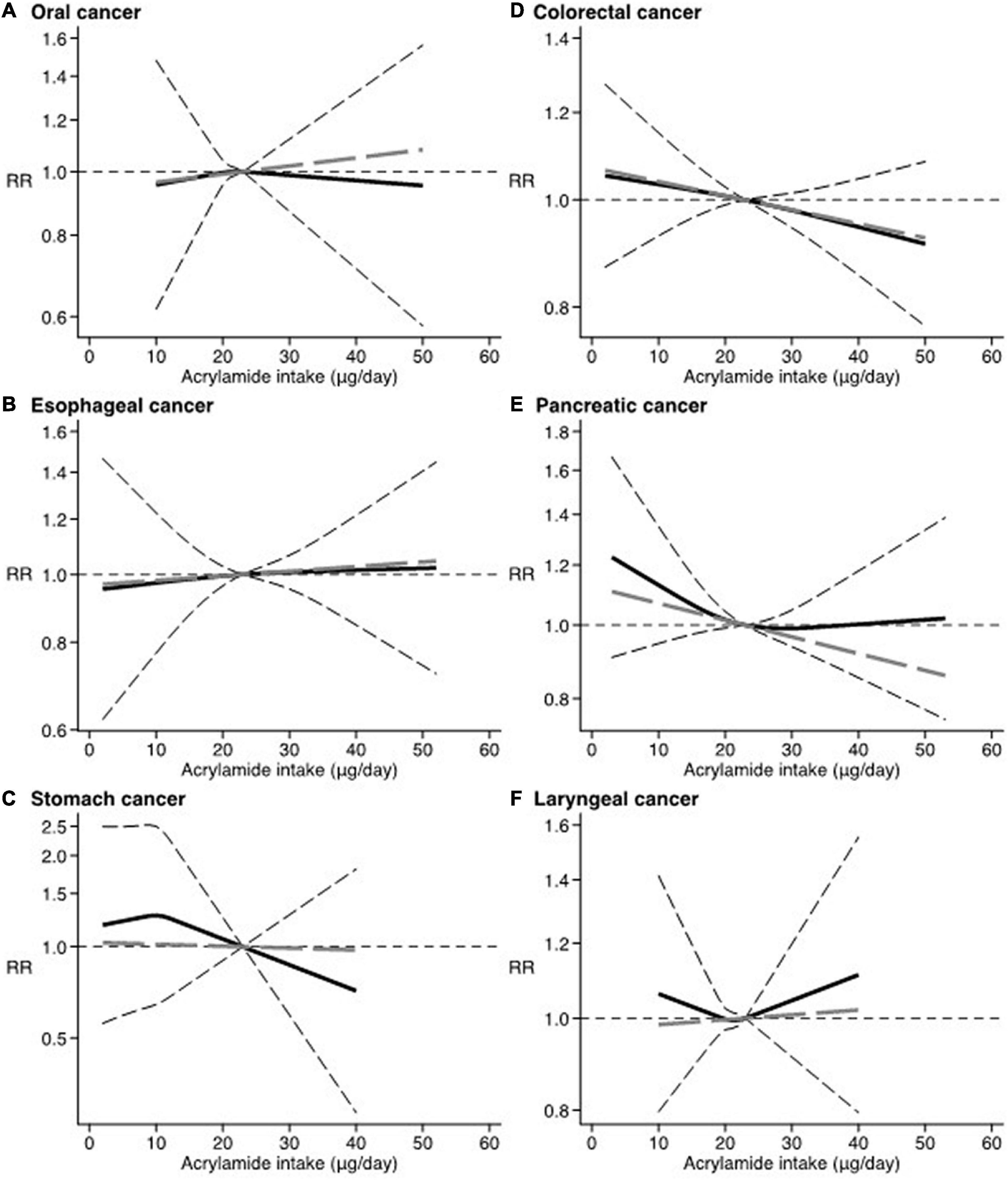
Figure 2. Dose-response. Spline curve (black solid line) with 95% confidence limits (black dashed lines). Linear trend (gray long-dashed line). RR, relative risk. Reference value of dietary acrylamide exposure: 23 μg/day. (A) Oral cancer (22, 31). (B) Esophageal cancer (14, 17, 22, 29, 32). (C) Stomach cancer (17, 29). (D) Colorectal cancer (17, 21, 22, 28, 29, 33). (E) Pancreatic cancer (17, 23, 71, 72). (F) Laryngeal cancer (22, 31).
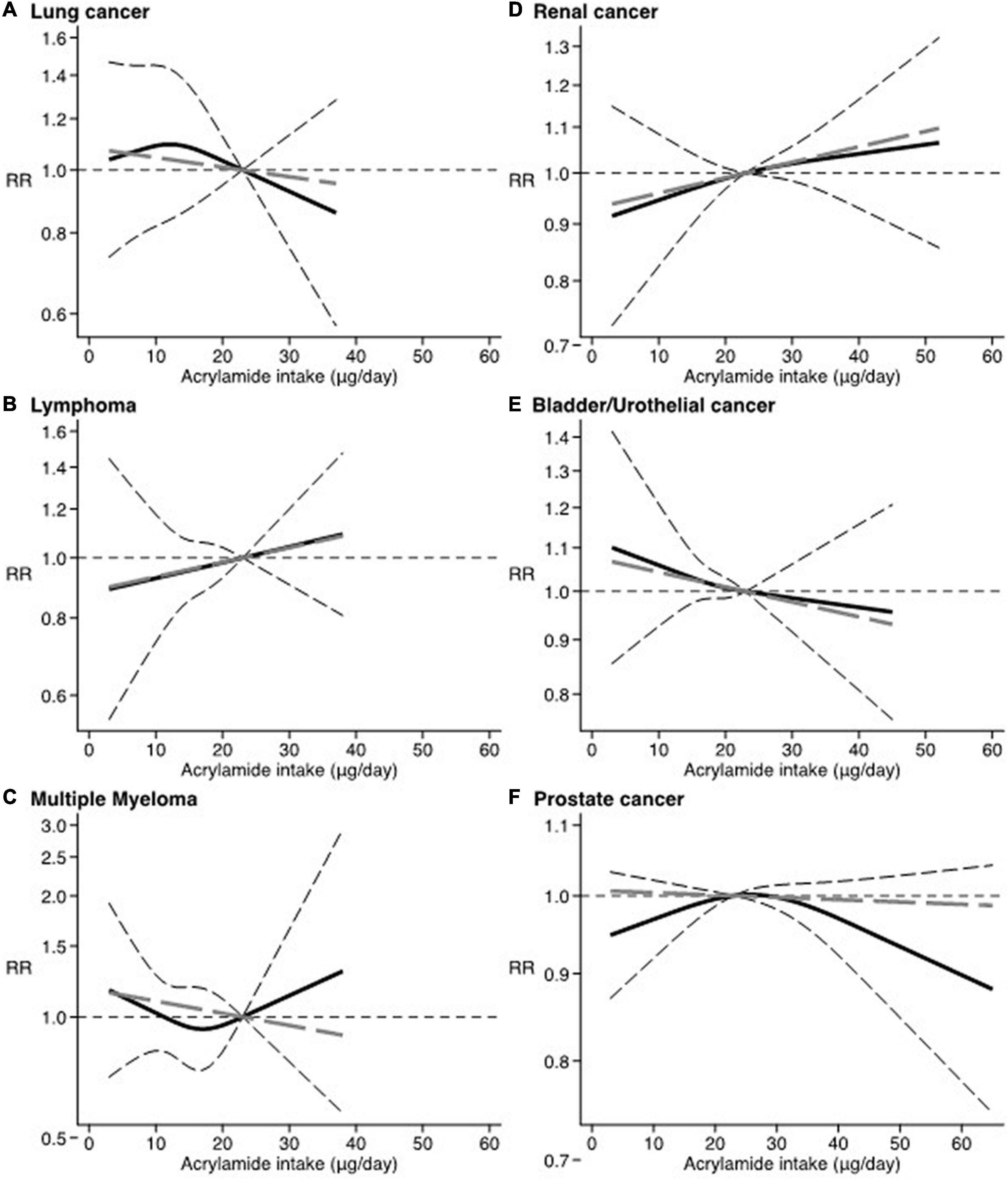
Figure 3. Dose-response. Spline curve (black solid line) with 95% confidence limits (black dashed lines). Linear trend (gray long-dashed line). RR: relative risk. Reference value of dietary acrylamide exposure: 23 μg/day. (A) Lung cancer (3, 19). (B) Lymphoma (16, 75). (C) Multiple myeloma (16, 75). (D) Renal cancer (17, 21, 30, 36, 59, 73, 74). (E) Bladder/Urothelial cancer (17, 21, 59). (F) Prostate cancer (17, 20, 22, 24, 27, 34, 59).
There was also no association between dietary acrylamide and the risk of site-specific cancer in the subgroups of smokers and never smokers, except for lung cancer, where we observed an increased risk in smokers (RR 1.16; 95% CI 1.03–1.31). Compared to smokers, the summary estimates for never smokers were observed to be higher, albeit very imprecise, for stomach, pancreatic, liver, renal, prostate, and multiple myeloma (Supplementary Figures 3, 7, 11, 12, 14).
Additional analysis by geographical regions (West and East) could be performed only excluding Asian population (i.e., Japan studies) since most of the studies were performed in the West area (Europe and United States). We observed a slightly, though imprecise, increased risk of lymphoma in relation to high dietary acrylamide when we consider only study from the West (n = 1) (RR 1.12; 95% CI 0.99–1.22) (Supplementary Figure 13).
There was no evidence of between-study heterogeneity except for lung and multiple myeloma cancers (Supplementary Figures 9, 14, respectively) (I2 > 50%). The graphical overlay of single study effects in the dose-response meta-analysis did not show substantial variation (data not shown). No evidence of publication bias, visualized by funnel plots, was observed (Supplementary Figures 2, 4, 7, 11, 12). The results of the risk of bias assessment, using the ROBINS-I are shown in Supplementary Figures 16, 17. Within the six dimensions analyzed, all studies had a low risk of bias regarding the measurement of outcomes and the reported result, and 75% of the studies showed a low risk of bias on the dimensions selection of participants and classification of interventions. All studies had a moderate risk of bias for confounding. There was missing information (classified as “no information”) regarding the dimensions’ deviations from intended interventions and missing data for more than 75% of the analyzed studies.
In this up-to-date systematic review and meta-analysis, based on 31 papers, we observed no association between high dietary acrylamide exposure and increased risk of any of the investigated cancers, including those of oral cavity, esophageal, gastric, colon-rectal, pancreatic, prostate, bladder, lung, renal, lymphoma, myeloma, thyroid, brain, larynx, and melanoma. As a novel finding, we found no thresholds between different levels of dietary acrylamide and the risk of any of the site-specific cancers considered. Considering studies performed in Western geographical areas alone, a slightly increased risk of lymphoma was observed in relation to high dietary acrylamide exposure. In general, findings did not differ by smoking status, except for increased risk of lung cancer in smokers.
Overall, our results of no association between high dietary acrylamide exposure and different site-specific cancers in the general population confirm the findings of previous meta-analyses that did not perform dose-response meta-analysis (22, 44, 46, 48). On the other hand, Pelucchi et al. (46) found a slight increased risk of renal cell carcinoma by 20% in relation to high dietary acrylamide (RR 1.20; 95% CI 1.00–1.45). This difference may be explained by the fact that we included three recent cohort studies with American (18, 30) and Japanese (59) participants. Results from these additional studies were to some extent heterogenous, with either a tendency of increased (18, 30) or decreased risk (30, 59) of renal cell carcinoma. The studies with American participants (18, 30) also contributed largely to the analysis (around 10% weight), possibly affecting our overall results. Moreover, we did not include the Finnish Alpha-Tocopherol, Beta-Carotene Cancer (ATBC) prevention study (60), a cohort study of 27,111 smoking men, in our main analysis which was based on both smokers and never smokers.
To the best of our knowledge, our meta-analysis is the first one investigating the shape of the dose-response relationships between dietary acrylamide exposure and the risk of site-specific cancer. Our results suggest that these associations, if present, may generally be without thresholds. These results are in line with those reported in a previous meta-analysis investigating the association between dietary acrylamide exposure and female reproductive cancers, which were not considered for inclusion in our meta-analysis (42).
Our aforementioned results may be explained by the relatively low dietary acrylamide exposure in the general population (intake ranged from 6.8 to 44.1 μg/day in the included studies—corresponding up to about 0.7 μg/kg body weight/day) when compared to the levels of acrylamide observed to be toxic in animal studies (50 mg/kg body weight/day) (9). There is also evidence showing that acrylamide does not generate any toxicologically detrimental effects when male rats were administrated three low oral doses of acrylamide (20, 40, and 90 μg/kg body weight/day, respectively) (61). Also, it is relevant to take into account that the EFSA CONTAM Panel selected BMDL10 value of 0.17 mg/kg body weight/day for neoplastic effects in mice (12), i.e., much higher level compared with those generally experienced by humans. Most of the included epidemiological studies investigating the relationship between dietary acrylamide and cancer risk were performed in North European regions, where dietary exposure to acrylamide is higher than in the Eastern geographical regions (i.e., Japanese populations), which reported the lowest mean dietary exposure below 10 μg/day. Additionally, the no association found in this study may be explained by the lack of assessment of co-exposure to other compounds in food matrixes, including other foodborne carcinogens (62) or substances that can confer protection to carcinogenic compounds (63, 64).
The findings related to the slightly increased risk of lymphomas in relation to high dietary acrylamide exposure restricted to the Western geographical region needs to be interpreted with caution as they are based on one single study (16) and combining the subtypes of lymphoma, characterized by very different clinical features, as well as genetic profile (65). These findings disagree to some extent with those reported by Pelucchi et al. (46). However, the latter did not investigate lymphomas and multiple myeloma separately and considered the ATBC study that we excluded from the main analysis because based on smokers alone. The biological mechanisms underlying the potentially increased risk of lymphoma in relation to high dietary acrylamide exposure in Western regions are unclear, but explanations may be speculated. Firstly, the hydrophilic nature of acrylamide leads to systemic exposure and so all human tissues, including the hemopoietic and lymphoid tissues, are potential targets for acrylamide-induced carcinogenesis. Also, acrylamide has been shown to induce carcinogenicity through dysregulation of the endocrine system, including hormones (66) and this has been suggested to play a role in the pathophysiology of lymphomas (16). The restriction of these findings to the Western geographical areas may be attributed to possible interactions between genetic and environmental exposures determinants, such as different sources of dietary acrylamide (67, 68).
In general, the similar results found in smokers and never smokers in our meta-analysis are in line with a previous meta-analysis (46). The results of increased risk of lung cancer in smokers and melanoma in non-smokers need be carefully interpreted since they are based on few and heterogenous studies. Also, for some of the cancers considered, the summary estimates suggested that never smokers could experience a slightly positive association between dietary acrylamide and cancer risk, which was not detectable in smokers. These results are in line with previous studies investigating this relationship by smoking status (16, 60). A possible explanation is that for the same level of exposure, less dietary acrylamide is converted to the genotoxic and carcinogenic metabolite of acrylamide, glycidamide, because smoking affects the metabolism of acrylamide by e.g., saturating enzymes involved in its conversion to glycidamide (55).
Firstly, we have performed an updated meta-analysis of the relationship between dietary acrylamide and the risk of several site-specific cancer. Compared to the previous meta-analyses, we were able to add some studies for several site-specific cancers, resulting in summary estimates with higher precision and accuracy.
Secondly, we also investigated the shape of the relationship between acrylamide and site-specific cancer and we evaluated heterogeneity among some groups (types of cancer, smoking status, and geographical regions). However, for some outcomes, the results were still based on a very limited number of available studies.
Our systematic review and meta-analysis have some limitations. They are based on epidemiological studies that assessed dietary acrylamide exposure through self-reported questionnaires. Hence, we cannot exclude that the summary estimates may be affected by misclassification of exposure related to the self-reported dietary intake (2, 69). Moreover, the acrylamide food database used in the separate studies, will not fully capture the variations in acrylamide levels between brands of a given food and in different food categories, as well as the different cooking methods used at home by the participants. However, results from a validation study showed a significant correlation between dietary acrylamide exposure and the acrylamide hemoglobin adducts (70). Furthermore, results from the only study investigating the exposure to acrylamide measured by acrylamide hemoglobin adducts in relation to cancer (i.e., prostate) showed no association in a Swedish population (20). In addition, the low number of available studies for each the site-specific cancer was not compatible with subgroup analyses and, so, we could not conduct a sensitivity analysis stratified by type of study design (case-control and cohort studies), which may have led to different summary estimates and, consequently, different conclusions. However, since there is little evidence for the occurrence of reverse causation or other biases in the studies with case-control design, the potential source of bias is very limited.
Additionally, for several of the studies included in the analysis stratified by smoking, doses of acrylamide by smoking status were not available and we used the doses indicated for the general population. Hence, the results on possible differences between smokers and non-smokers need to be carefully interpreted.
Based on the results of this dose-response meta-analysis of epidemiological studies, higher dietary acrylamide exposure (vs. lower) was not associated with an increased risk of several site-specific cancers. If associations between dietary acrylamide and the risk of several site-specific cancers were present, the shape of the dose-response relationships would be with no thresholds. Smoking status might modify the relation between dietary acrylamide and some site-specific cancers, but findings need to be furtherly investigated.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
TF, TH, AV, and FL conceptualized the study and drafted the manuscript. TF performed the statistical analyses. All authors contributed substantively to this work, involved in the interpretation of results, editing of the manuscript, and approved manuscript submission.
This work was supported by the European Union Horizon-2020 Research and Innovation Programme under grant agreement No. 733032 HBM4EU.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We thank all the partners of the HBM4EU project.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnut.2022.875607/full#supplementary-material
ATBC, Alpha-Tocopherol, Beta-Carotene Cancer; CI, Confidence Interval; DNA, Deoxyribonucleic acid; HR, Hazard Ratio; IARC, International Agency for Research on Cancer; MeSH, Medical Subject Headings; MOOSE, Meta-analysis Of Observational Studies in Epidemiology; OR, Odds Ratio; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; ROBINS-I, Risk of Bias In Non-randomized Studies of Interventions; RR, Relative Risk.
1. Tareke E, Rydberg P, Karlsson P, Eriksson S, Tornqvist M. Analysis of acrylamide, a carcinogen formed in heated foodstuffs. J Agric Food Chem. (2002) 50:4998–5006. doi: 10.1021/jf020302f
2. Yaylayan VA, Stadler RH. Acrylamide formation in food: a mechanistic perspective. J AOAC Int. (2005) 88:262–7. doi: 10.1093/jaoac/88.1.262
3. Liu R, Zha L, Sobue T, Kitamura T, Ishihara J, Kotemori A, et al. Dietary acrylamide intake and risk of lung cancer: the Japan public health center based prospective study. Nutrients. (2020) 12:2417. doi: 10.3390/nu12082417
4. Cecil TL, Brewer TM, Young M, Holman MR. Acrolein yields in mainstream smoke from commercial cigarette and little cigar tobacco products. Nicotine Tob Res. (2017) 19:865–70. doi: 10.1093/ntr/ntx003
5. Mojska H, Gielecinska I, Cendrowski A. Acrylamide content in cigarette mainstream smoke and estimation of exposure to acrylamide from tobacco smoke in Poland. Ann Agric Environ Med. (2016) 23:456–61. doi: 10.5604/12321966.1219187
6. Vesper HW, Slimani N, Hallmans G, Tjonneland A, Agudo A, Benetou V, et al. Cross-sectional study on acrylamide hemoglobin adducts in subpopulations from the European prospective investigation into cancer and nutrition (EPIC) Study. J Agric Food Chem. (2008) 56:6046–53. doi: 10.1021/jf703750t
7. Hagmar L, Tornqvist M, Nordander C, Rosen I, Bruze M, Kautiainen A, et al. Health effects of occupational exposure to acrylamide using hemoglobin adducts as biomarkers of internal dose. Scand J Work Environ Health. (2001) 27:219–26. doi: 10.5271/sjweh.608
8. World Health Organization, International Agency for Research on Cancer. IARC monographs on the evaluation of carcinogenic risks to humans. IARC working group on the evaluation of carcinogenic risks to humans: some industrial chemicals. Lyon, 15–22 February 1994. IARC Monogr Eval Carcinog Risks Hum. (1994) 60:1–560.
9. Besaratinia A, Pfeifer GP. A review of mechanisms of acrylamide carcinogenicity. Carcinogenesis. (2007) 28:519–28. doi: 10.1093/carcin/bgm006
10. Beland FA, Olson GR, Mendoza MC, Marques MM, Doerge DR. Carcinogenicity of glycidamide in B6C3F1 mice and F344/N rats from a two-year drinking water exposure. Food Chem Toxicol. (2015) 86:104–15. doi: 10.1016/j.fct.2015.09.017
11. Zhivagui M, Ng AWT, Ardin M, Churchwell MI, Pandey M, Renard C, et al. Experimental and pan-cancer genome analyses reveal widespread contribution of acrylamide exposure to carcinogenesis in humans. Genome Res. (2019) 29:521–31. doi: 10.1101/gr.242453.118
12. EFSA Panel on Contaminants in the Food Chain (CONTAM). Scientific Opinion on acrylamide in food. EFSA Journal. (2015) 13:4104. doi: 10.2903/j.efsa.2015.4104
13. Lipunova N, Schouten LJ, van den Brandt PA, Hogervorst JGF. A prospective cohort study on dietary acrylamide intake and the risk for cutaneous malignant melanoma. Eur J Cancer Prev. (2017) 26:528–31. doi: 10.1097/CEJ.0000000000000268
14. Lin Y, Lagergren J, Lu Y. Dietary acrylamide intake and risk of esophageal cancer in a population-based case-control study in Sweden. Int J Cancer. (2011) 128:676–81. doi: 10.1002/ijc.25608
15. Hogervorst JG, de Bruijn-Geraets D, Schouten LJ, van Engeland M, de Kok TM, Goldbohm RA, et al. Dietary acrylamide intake and the risk of colorectal cancer with specific mutations in KRAS and APC. Carcinogenesis. (2014) 35:1032–8. doi: 10.1093/carcin/bgu002
16. Bongers ML, Hogervorst JG, Schouten LJ, Goldbohm RA, Schouten HC, van den Brandt PA. Dietary acrylamide intake and the risk of lymphatic malignancies: the Netherlands Cohort Study on diet and cancer. PLoS One. (2012) 7:e38016. doi: 10.1371/journal.pone.0038016
17. Hogervorst JG, Schouten LJ, Konings EJ, Goldbohm RA, van den Brandt PA. Dietary acrylamide intake and the risk of renal cell, bladder, and prostate cancer. Am J Clin Nutr. (2008) 87:1428–38. doi: 10.1093/ajcn/87.5.1428
18. McCullough ML, Hodge RA, Um CY, Gapstur SM. Dietary acrylamide is not associated with renal cell cancer risk in the CPS-II nutrition cohort. Cancer Epidemiol Biomarkers Prev. (2019) 28:616–9. doi: 10.1158/1055-9965.EPI-18-0909
19. Hogervorst JG, Schouten LJ, Konings EJ, Goldbohm RA, van den Brandt PA. Lung cancer risk in relation to dietary acrylamide intake. J Natl Cancer Inst. (2009) 101:651–62. doi: 10.1093/jnci/djp077
20. Wilson KM, Balter K, Adami HO, Gronberg H, Vikstrom AC, Paulsson B, et al. Acrylamide exposure measured by food frequency questionnaire and hemoglobin adduct levels and prostate cancer risk in the cancer of the Prostate in Sweden Study. Int J Cancer. (2009) 124:2384–90. doi: 10.1002/ijc.24175
21. Mucci LA, Dickman PW, Steineck G, Adami HO, Augustsson K. Dietary acrylamide and cancer of the large bowel, kidney, and bladder: absence of an association in a population-based study in Sweden. Br J Cancer. (2003) 88:84–9. doi: 10.1038/sj.bjc.6600726
22. Pelucchi C, Galeone C, Levi F, Negri E, Franceschi S, Talamini R, et al. Dietary acrylamide and human cancer. Int J Cancer. (2006) 118:467–71. doi: 10.1002/ijc.21336
23. Pelucchi C, Galeone C, Talamini R, Negri E, Polesel J, Serraino D, et al. Dietary acrylamide and pancreatic cancer risk in an Italian case–control study. Ann Oncol. (2011) 22:1910–5. doi: 10.1093/annonc/mdq672
24. Wilson KM, Giovannucci E, Stampfer MJ, Mucci LA. Dietary acrylamide and risk of prostate cancer. Int J Cancer. (2012) 131:479–87. doi: 10.1002/ijc.26383
25. Pelucchi C, Rosato V, Bracci PM, Li D, Neale RE, Lucenteforte E, et al. Dietary acrylamide and the risk of pancreatic cancer in the international pancreatic cancer case-control consortium (PanC4). Ann Oncol. (2017) 28:408–14. doi: 10.1093/annonc/mdw618
26. Hogervorst JG, Schouten LJ, Konings EJ, Goldbohm RA, van den Brandt PA. Dietary acrylamide intake and brain cancer risk. Cancer Epidemiol Biomarkers Prev. (2009) 18:1663–6. doi: 10.1158/1055-9965.EPI-08-1133
27. Larsson SC, Akesson A, Wolk A. Dietary acrylamide intake and prostate cancer risk in a prospective cohort of Swedish men. Cancer Epidemiol Biomarkers Prev. (2009) 18:1939–41. doi: 10.1158/1055-9965.EPI-09-0280
28. Larsson SC, Akesson A, Bergkvist L, Wolk A. Dietary acrylamide intake and risk of colorectal cancer in a prospective cohort of men. Eur J Cancer. (2009) 45:513–6. doi: 10.1016/j.ejca.2008.12.001
29. Liu R, Sobue T, Kitamura T, Kitamura Y, Ishihara J, Kotemori A, et al. Dietary acrylamide intake and risk of esophageal, gastric, and colorectal cancer: the Japan public health center-based prospective study. Cancer Epidemiol Biomarkers Prev. (2019) 28:1461–8. doi: 10.1158/1055-9965.EPI-18-1259
30. Graff RE, Cho E, Preston MA, Sanchez A, Mucci LA, Wilson KM. Dietary acrylamide intake and risk of renal cell carcinoma in two large prospective cohorts. Cancer Epidemiol Biomarkers Prev. (2018) 27:979–82. doi: 10.1158/1055-9965.EPI-18-0320
31. Schouten LJ, Hogervorst JG, Konings EJ, Goldbohm RA, van den Brandt PA. Dietary acrylamide intake and the risk of head-neck and thyroid cancers: results from the Netherlands cohort study. Am J Epidemiol. (2009) 170:873–84. doi: 10.1093/aje/kwp213
32. Lujan-Barroso L, Gonzalez CA, Slimani N, Obon-Santacana M, Ferrari P, Freisling H, et al. Dietary intake of acrylamide and esophageal cancer risk in the European prospective investigation into cancer and nutrition cohort. Cancer Causes Control. (2014) 25:639–46. doi: 10.1007/s10552-014-0359-5
33. Mucci LA, Adami HO, Wolk A. Prospective study of dietary acrylamide and risk of colorectal cancer among women. Int J Cancer. (2006) 118:169–73. doi: 10.1002/ijc.21309
34. Perloy A, Schouten LJ, van den Brandt PA, Godschalk R, van Schooten FJ, Hogervorst JGF. The role of genetic variants in the association between dietary acrylamide and advanced prostate cancer in the Netherlands cohort study on diet and cancer. Nutr Cancer. (2018) 70:620–31. doi: 10.1080/01635581.2018.1460682
35. Zha L, Sobue T, Kitamura T, Kitamura Y, Ishihara J, Kotemori A, et al. Dietary acrylamide intake and the risk of liver cancer: the Japan public health center-based prospective study. Nutrients. (2020) 12:2503. doi: 10.3390/nu12092503
36. Pelucchi C, Galeone C, Dal Maso L, Talamini R, Montella M, Ramazzotti V, et al. Dietary acrylamide and renal cell cancer. Int J Cancer. (2007) 120:1376–7. doi: 10.1002/ijc.22457
37. Collins JJ, Swaen GM, Marsh GM, Utidjian HM, Caporossi JC, Lucas LJ. Mortality patterns among workers exposed to acrylamide. J Occup Med. (1989) 31:614–7. doi: 10.1097/00043764-198907000-00013
38. Marsh GM, Lucas LJ, Youk AO, Schall LC. Mortality patterns among workers exposed to acrylamide: 1994 follow up. Occup Environ Med. (1999) 56:181–90. doi: 10.1136/oem.56.3.181
39. Marsh GM, Youk AO, Buchanich JM, Kant IJ, Swaen G. Mortality patterns among workers exposed to acrylamide: updated follow up. J Occup Environ Med. (2007) 49:82–95. doi: 10.1097/JOM.0b013e31802db536
40. Sobel W, Bond GG, Parsons TW, Brenner FE. Acrylamide cohort mortality study. Br J Ind Med. (1986) 43:785–8. doi: 10.1136/oem.43.11.785
41. Swaen GM, Haidar S, Burns CJ, Bodner K, Parsons T, Collins JJ, et al. Mortality study update of acrylamide workers. Occup Environ Med. (2007) 64:396–401. doi: 10.1136/oem.2006.030130
42. Adani G, Filippini T, Wise LA, Halldorsson TI, Blaha L, Vinceti M. Dietary intake of acrylamide and risk of breast, endometrial, and ovarian cancers: a systematic review and dose-response meta-analysis. Cancer Epidemiol Biomarkers Prev. (2020) 29:1095–106. doi: 10.1158/1055-9965.EPI-19-1628
43. Je Y. Dietary acrylamide intake and risk of endometrial cancer in prospective cohort studies. Arch Gynecol Obstet. (2015) 291:1395–401. doi: 10.1007/s00404-014-3595-8
44. Jiang F, Teng M, Zhu YX, Li YJ. No association between dietary acrylamide and renal cell carcinoma: an updated meta-analysis. J Sci Food Agric. (2020) 100:3071–7. doi: 10.1002/jsfa.10339
45. Benisi-Kohansal S, Salari-Moghaddam A, Seyed Rohani Z, Esmaillzadeh A. Dietary acrylamide intake and risk of women’s cancers: a systematic review and meta-analysis of prospective cohort studies. Br J Nutr. (2021) 126:1355–63. doi: 10.1017/S0007114520005255
46. Pelucchi C, Bosetti C, Galeone C, La Vecchia C. Dietary acrylamide and cancer risk: an updated meta-analysis. Int J Cancer. (2015) 136:2912–22. doi: 10.1002/ijc.29339
47. Pelucchi C, La Vecchia C, Bosetti C, Boyle P, Boffetta P. Exposure to acrylamide and human cancer–a review and meta-analysis of epidemiologic studies. Ann Oncol. (2011) 22:1487–99. doi: 10.1093/annonc/mdq610
48. Virk-Baker MK, Nagy TR, Barnes S, Groopman J. Dietary acrylamide and human cancer: a systematic review of literature. Nutr Cancer. (2014) 66:774–90. doi: 10.1080/01635581.2014.916323
49. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Syst Rev. (2021) 10:89. doi: 10.1186/s13643-021-01626-4
50. Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson GD, Rennie D, et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis of observational studies in epidemiology (MOOSE) group. JAMA. (2000) 283:2008–12. doi: 10.1001/jama.283.15.2008
51. Sterne JA, Hernan MA, Reeves BC, Savovic J, Berkman ND, Viswanathan M, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. (2016) 355:i4919. doi: 10.1136/bmj.i4919
52. Filippini T, Torres D, Lopes C, Carvalho C, Moreira P, Naska A, et al. Cadmium exposure and risk of breast cancer: a dose-response meta-analysis of cohort studies. Environ Int. (2020) 142:105879. doi: 10.1016/j.envint.2020.105879
53. Filippini T, Malavolti M, Whelton PK, Naska A, Orsini N, Vinceti M. Blood pressure effects of sodium reduction: dose-response meta-analysis of experimental studies. Circulation. (2021) 143:1542–67. doi: 10.1161/circulationaha.120.050371
54. Orsini N. Weighted mixed-effects dose–response models for tables of correlated contrasts. Stata J. (2021) 21:320–47. doi: 10.1177/1536867x211025798
55. Schettgen T, Rossbach B, Kutting B, Letzel S, Drexler H, Angerer J. Determination of haemoglobin adducts of acrylamide and glycidamide in smoking and non-smoking persons of the general population. Int J Hyg Environ Health. (2004) 207:531–9. doi: 10.1078/1438-4639-00324
56. Egger M, Smith GD, Phillips AN. Meta-analysis: principles and procedures. BMJ. (1997) 315:1533–7. doi: 10.1136/bmj.315.7121.1533
57. Lin L, Shi L, Chu H, Murad MH. The magnitude of small-study effects in the Cochrane database of systematic reviews: an empirical study of nearly 30 000 meta-analyses. BMJ Evid Based Med. (2020) 25:27–32. doi: 10.1136/bmjebm-2019-111191
58. Crippa A, Discacciati A, Bottai M, Spiegelman D, Orsini N. One-stage dose-response meta-analysis for aggregated data. Stat Methods Med Res. (2019) 28:1579–96. doi: 10.1177/0962280218773122
59. Ikeda S, Sobue T, Kitamura T, Ishihara J, Kotemori A, Zha L, et al. Dietary acrylamide intake and the risks of renal cell, prostate, and bladder cancers: a Japan public health center-based prospective study. Nutrients. (2021) 13:780. doi: 10.3390/nu13030780
60. Hirvonen T, Kontto J, Jestoi M, Valsta L, Peltonen K, Pietinen P, et al. Dietary acrylamide intake and the risk of cancer among Finnish male smokers. Cancer Causes Control. (2010) 21:2223–9. doi: 10.1007/s10552-010-9642-2
61. Raju J, Kocmarek A, Roberts J, Taylor M, Patry D, Chomyshyn E, et al. Lack of adverse health effects following 30-weeks of dietary exposure to acrylamide at low doses in male F344 rats. Toxicol Rep. (2016) 3:673–8. doi: 10.1016/j.toxrep.2016.08.010
62. Parzefall W. Minireview on the toxicity of dietary acrylamide. Food Chem Toxicol. (2008) 46:1360–4. doi: 10.1016/j.fct.2007.08.027
63. Nehlig A, Cunha RA. The coffee-acrylamide apparent paradox: an example of why the health impact of a specific compound in a complex mixture should not be evaluated in isolation. Nutrients. (2020) 12:3141. doi: 10.3390/nu12103141
64. Eisenbrand G. Revisiting the evidence for genotoxicity of acrylamide (AA), key to risk assessment of dietary AA exposure. Arch Toxicol. (2020) 94:2939–50. doi: 10.1007/s00204-020-02794-3
65. de Leval L, Jaffe ES. Lymphoma classification. Cancer J. (2020) 26:176–85. doi: 10.1097/PPO.0000000000000451
66. Bandarra S, Fernandes AS, Magro I, Guerreiro PS, Pingarilho M, Churchwell MI, et al. Mechanistic insights into the cytotoxicity and genotoxicity induced by glycidamide in human mammary cells. Mutagenesis. (2013) 28:721–9. doi: 10.1093/mutage/get052
67. Chihara D, Ito H, Matsuda T, Shibata A, Katsumi A, Nakamura S, et al. Differences in incidence and trends of haematological malignancies in Japan and the United States. Br J Haematol. (2014) 164:536–45. doi: 10.1111/bjh.12659
68. Miranda-Filho A, Pineros M, Ferlay J, Soerjomataram I, Monnereau A, Bray F. Epidemiological patterns of leukaemia in 184 countries: a population-based study. Lancet Haematol. (2018) 5:e14–24. doi: 10.1016/S2352-3026(17)30232-6
69. Perez Rodrigo C, Aranceta J, Salvador G, Varela-Moreiras G. Food frequency questionnaires. Nutr Hosp. (2015) 31 (Suppl. 3):49–56. doi: 10.3305/nh.2015.31.sup3.8751
70. Wirfalt E, Paulsson B, Tornqvist M, Axmon A, Hagmar L. Associations between estimated acrylamide intakes, and hemoglobin AA adducts in a sample from the Malmo diet and cancer cohort. Eur J Clin Nutr. (2008) 62:314–23. doi: 10.1038/sj.ejcn.1602704
71. Kito K, Ishihara J, Kotemori A, Zha L, Liu R, Sawada N, et al. Dietary acrylamide intake and the risk of pancreatic cancer: the Japan Public Health Center-based prospective study. Nutrients. (2020) 12:3584. doi: 10.3390/nu12113584
72. Obón-Santacana M, Slimani N, Lujan-Barroso L, Travier N, Hallmans G, Freisling H, et al. Dietary intake of acrylamide and pancreatic cancer risk in the European Prospective Investigation into Cancer and Nutrition (EPIC) cohort. Ann Oncol. (2013) 24:2645–51. doi: 10.1093/annonc/mdt255
73. McCullough ML, Hodge RA, Um CY, Gapstur SM. Dietary acrylamide is not associated with renal cell cancer risk in the CPS-II Nutrition Cohort. Cancer Epidemiol Biomarkers Prev. (2019) 28:616–9. doi: 10.1158/1055-9965.EPI-18-0909
74. Mucci LA, Lindblad P, Steineck G, Adami HO. Dietary acrylamide and risk of renal cell cancer. Int J Cancer. (2004) 109:774–6. doi: 10.1002/ijc.20011
Keywords: acrylamide, dietary exposure, neoplasms, carcinoma, systematic review, meta-analysis, epidemiological studies
Citation: Filippini T, Halldorsson TI, Capitão C, Martins R, Giannakou K, Hogervorst J, Vinceti M, Åkesson A, Leander K, Katsonouri A, Santos O, Virgolino A and Laguzzi F (2022) Dietary Acrylamide Exposure and Risk of Site-Specific Cancer: A Systematic Review and Dose-Response Meta-Analysis of Epidemiological Studies. Front. Nutr. 9:875607. doi: 10.3389/fnut.2022.875607
Received: 14 February 2022; Accepted: 18 March 2022;
Published: 25 April 2022.
Edited by:
Abu Mohammed Naser Titu, University of Memphis, United StatesReviewed by:
José María Huerta, Instituto de Salud Carlos III (ISCIII), SpainCopyright © 2022 Filippini, Halldorsson, Capitão, Martins, Giannakou, Hogervorst, Vinceti, Åkesson, Leander, Katsonouri, Santos, Virgolino and Laguzzi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Federica Laguzzi, ZmVkZXJpY2EubGFndXp6aUBraS5zZQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.