 Li Cai1,2†
Li Cai1,2† Yeqing Tong
Yeqing Tong
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Nutr. , 17 May 2022
Sec. Clinical Nutrition
Volume 9 - 2022 | https://doi.org/10.3389/fnut.2022.873890
The progressions of a number of lung diseases, including acute lung injury, cystic fibrosis, asthma, chronic obstructive pulmonary disease, pneumonia and tuberculosis (TB) are found to be highly associated with inflammatory responses. As a signaling nutrient, Vitamin D modulates the activities of dendritic cells, monocytes/macrophages, T and B cells, and tissue epithelial cells in the body to induce inflammatory responses and boost immune functions. Given the high prevalence of vitamin D deficiency among pulmonary insufficiency and inflammation-related cases, researchers indicated vitamin D supplementation could have a potential role in the prevention and treatment of lung disease, especially tuberculosis. In this paper, we reviewed published studies on the role of vitamin D in the prevention and treatment of tuberculosis. The paper identified vitamin D’s potential as an adjunctive therapy and demonstrated its safety so as to provide an impetus for further studies and clinical applications.
Vitamin D (VitD) is a family of vitamins derived from cholesterol. Two major forms of VitD are vitamin D2 (VitD2) and vitamin D3 (VitD3), of which VitD2 is mainly found in plants and VitD3 is only found in animal-sourced food, such as fish oil, liver, egg yolk, butter, and dietary supplements (1). VitD2 differs from VitD3 by its additional methyl group and a double bond. Although different in structure, the two forms of VitD, when activated, exhibit similar responses in the body (2).
VitD3 is synthesized by skin tissue from 7-DHC after a dihydroxylation step. 7-dehydrocholesterol (7-DHC) is a vitamin precursor that is synthesized by cholesterol oxidation and then transferred to skin tissue and stored in keratinocytes and fibroblasts. After binding to a protein, it is transferred to the liver and metabolized to 25-hydroxyVitD by 25-hydroxylase, Vitamin D-binding protein (VDBP) is the major binding protein for VitD metabolites. It mainly plays three important roles in the physiological mechanisms of VitD: enlargement of the biological half-life of VitD (binding protects VitD from bio-degradation), limiting its access to target tissues and maintains plasma VitD levels through reabsorption in the kidneys. To be specific, 85–90% of the total circulating VitD metabolites are bound to VDBP, 10–15% are bound to albumin, and less than 1% remains free in the serum (3, 4). The protein activity in the bound form is affected, so only the unbound protein can exert its activity (4, 5). Thus, the binding of VitD to VDBP impairs its delivery to target cells.
In the form of D2 or D3, Vitamin D is converted to 25-hydroxy-D2 or 25-hydroxy-D3 after intestinal absorption in the form of D2 or D3, respectively. Next, it enters the circulatory system and combines with VDBP. In the renal tubules of the kidney, 25-hydroxyl D is hydroxylated by enzymes 1-a hydroxylase and 24-a hydroxylase to produce the active forms 1,25 dihydroxy-D and 24,25 dihydroxy-D and bind to the nuclear hormone receptor with high affinity under the regulation of phosphate, calcium, fibroblast growth factor, and parathyroid hormone. Finally, 24, 25-dihydroxyVitD is oxidized to form water-soluble metabolites, excreted in vitro by bile and urine (6, 7).
The immune response of the human host to Mycobacterium tuberculosis (MTB) is of special significance from disease onset to have pathophysiological outcomes to observed clinical outcomes (8). Tuberculosis (TB) is an infectious disease caused by MTB. It is mainly transmitted through inhaling tiny droplets from the cough or sneezes of an active infected patient. The bacteria then is activated into alveolar macrophages (9), thus forming early infection foci. The initial process of TB growth within macrophages results in the formation of TB foci with solid caseous necrosis in the center, which limits TB’s further replication. Caseous necrosis presents a cheese-like appearance. During this period, cellular immunity mediated by T cells and delayed hypersensitivity reactions develop, which have a decisive impact on the progression and prognosis of TB (10). Following the symbiotic stage, when bacillus keeps multiplying within the macrophages, macrophages accumulate and divide. In caseous necrosis, TB bacteria are capable of growing but not reproducing. Once liquefied, the necrosis provides an ideal breeding environment for bacteria. Thus, the caseous central site of fibrous necrotic foci is considered to be the main site for bacterial persistence.
Macrophage decreased while using a VitD-mediated immune response against TB bacteria and further reduced with the addition of cytokines IFN-g and CYP27B1 (macrophage promoter). In 2006, an increased expression of both vitamin D receptor (VDR) and CYP27B1 was detected by TLR2/1 by Liu et al. (11). This is due to the VDR transactivation of an antimicrobial peptide (cathelicidin, LL37) that can successively activate the intracellular PRR and NOD2 and ultimately activate the NF-KB. The VitD receptors have macrophages on the surface. The interaction between macrophages and Mycobacterium tuberculosis, through activation of receptors I and II, enhanced 1α-hydroxylase (CYP27B1), VDR and Catherine Xitin (VDR target organ) expression. Meanwhile, VitD induces the production of methyl glycol and β-Fenin 2 (antimicrobial peptide) to introduce monocytes, neutrophils, and T cells to the site of infection, playing an immunomodulatory role in the treatment of TB (12).
Determinants of VitD status included age, race, skin color, and living habits. VitD deficiency is prevalent across countries. Such deficiency is widely found in latent and active tuberculosis patients. Researchers have made the below argument to illustrate the association between VitD and tuberculosis: VitD deficiency could aggravate the susceptibility and accelerate the progression of the disease (13, 14). Thereby, it is assumed that VitD supplements could play a role in the prevention and treatment of tuberculosis.
Studies demonstrated that VitD level is highly associated with the susceptibility of hosts to mycobacterium tuberculosis. Researchers enumerated three observations that could illustrate its association: first, cold winter with reduced VitD from sun exposure is the season of high tuberculosis incidence; second, people with specific demographic characteristics (e.g., children, the elderly, uremic patients, and Asian immigrants in the United Kingdom) are prone to have higher tuberculosis incidence rate and lower serum VitD level than the left groups (14–16). Hewison explained that VitD level is closely related to innate and adaptive immunity, which made those people susceptible to tuberculosis (17).
VitD can also be an adjuvant treatment for tuberculosis. The study by Zhang and Li found that VitD supplementation is beneficial to the conversion of TB and can significantly reduce the positive rate of sputum culture in patients and shorten the negative transfer time of sputum culture (15). Researchers also found that adequate VitD supplementation shortened the conversion time of sputum smear and sputum culture in patients (18, 19). Moreover, related investigations also demonstrated that VitD is capable of being an adjuvant treatment for multidrug-resistant tuberculosis (MDR-TB). Therefore, VitD deficiency may lead to the prolonged negative conversion time of sputum smear in patients with MDR-TB (20). Regarding the mechanism by which VitD supplementation works, Hewison (17) noted that VitD could facilitate the clearance of TB bacteria in the body.
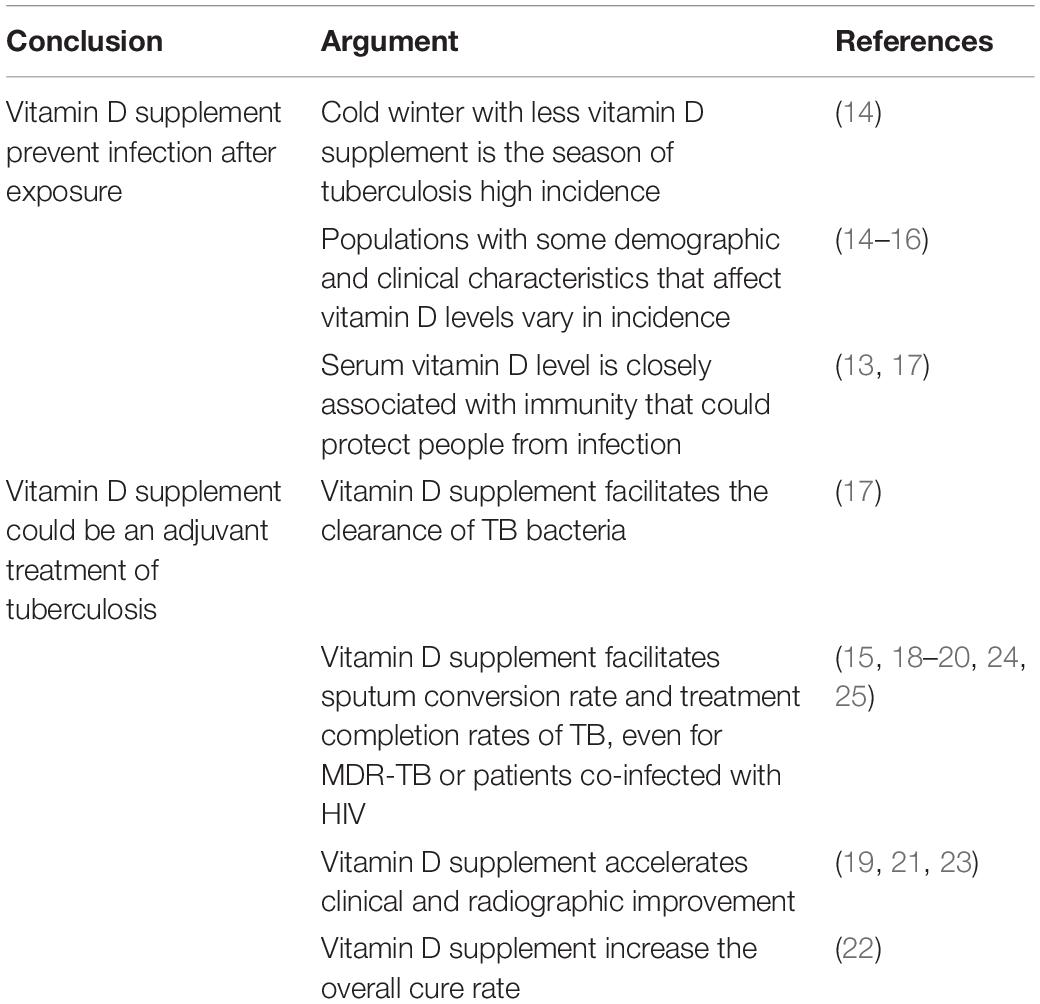
Table 1. Main findings of vitamin D for tuberculosis prevention and treatment.
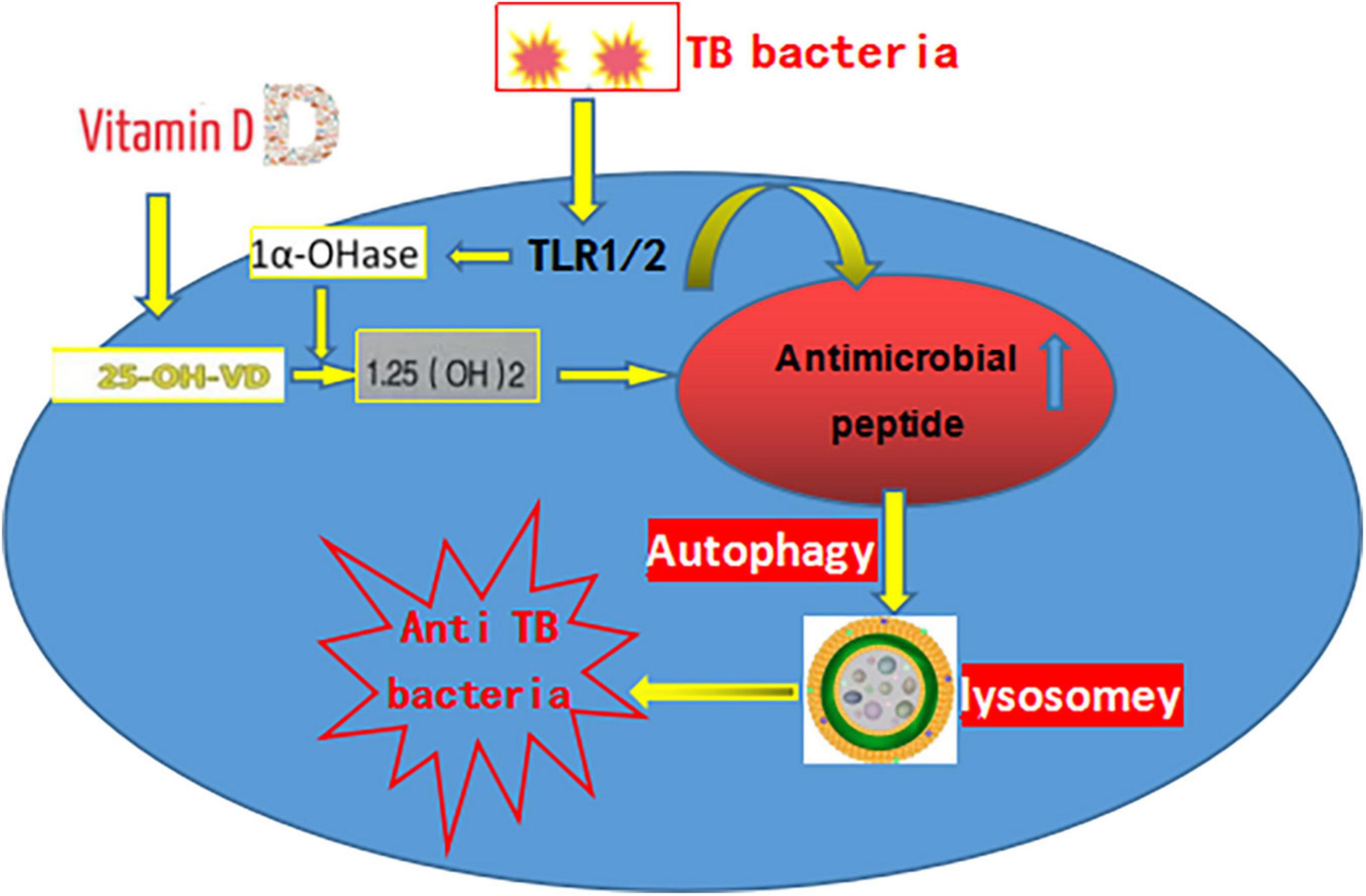
Figure 1. The pathogenesis of tuberculosis.
In addition to its contribution to shortening conversion time, VitD supplementation can also accelerate clinical and radiographic improvement for active TB patients. Through case-control studies, researchers found patients in the VitD supplementation group had greater clinical improvement. Significantly fewer patients had fever in the control group (19, 21). The study of Dai found that the patient’s serum 25-hydroxyvitamin D level was slightly related to the outcome of tuberculosis treatment (22). The higher the 25-hydroxyvitamin D concentration detected in the patient, the greater the cure rate. Sutaria et al. conducted a systematic review pertaining to case-control studies in this area to examine the potential of VitD. The study concluded that supplementation with VitD to tuberculosis patients can improve clinical outcomes (23). Jahnavi and Sudha conducted a case-control study for 100 patients undergoing anti-tubercular therapy in Anganwadi Centres of India. Researchers provided food supplements that can meet the daily intake target of vitamins and minerals for the experimental group. Patients who were randomly assigned to the control plan did not get any dietary plan or food supplements. After 3 months, patients in the experimental group reached significant higher sputum conversion rates and treatment completion rates (24). Moreover, by conducting a two-by-two factorial trial in Tanzania, Range et al. argued that vitamin and mineral supplementation could significantly increase the survival rate of sputum-positive patients co-infected with HIV (25).
In 1969, Brincourt proposed to use 15 mg (600,000IU) VitD to treat TB (26). In 1981, Gwinup et al. proposed to treat TB with 125 μg VitD2 for TB (27). During the same period, the study by Stern et al. (28) and Tjellesen et al. (29) used a high dose of VitD to treat TB, but there were still no adverse effects. In 2006, A study found that 250 μg of VitD per day for 6 weeks after the start of anti-TB treatment in Indonesia could clear TB bacteria more quickly from sputum. The imagings of patients with TB were also significantly improved (21). A cohort study of multiethnic patients with TB in the United Kingdom showed that a single oral dose of 2.5 mg of vitamin D2 in the treatment of TB has no adverse reactions such as hypercalcemia (30). In 2012, a randomized controlled trial showed that oral dose of 2.5 mg of vitamin D as an adjuvant treatment could shorten the sputum smear-negative rotation time in 95 treated patients with TB (31). Currently, that dose of vitamin D has not been reported to be applied to elderly patients with TB.
Although it has been confirmed by many researchers that VitD can be used as adjuvant therapy for tuberculosis, there are still limitations in the existing research. For clarity, so far, there is no consensus on the reference values that define VitD sufficiency and deficiency. Studies cited by this paper mostly take the reference value as the mean serum 25-hydroxyvitamin D concentration in the population of the research regions. Besides, whether vitamin concentration could be considered to be sufficient also varies for its different functions, such as for bone health or for immunity. In this regard, the optimal amount of VitD supplements for the prevention and treatment of TB remain unknown. Research breakthrough on the reference value is needed (32).
The significance of the association between VitD status and tuberculosis still left the direction of the causation relationship quite uncertain. On the one hand, TB patients with already low VitD levels may have lower VitD since the commencement of treatment (33, 34). On the other hand, VitD deficiency might be an important determinant for patients with latent tuberculosis to become active. Therefore, further studies that could explicate the mechanism of VitD in preventing and treating tuberculosis should be done.
The analysis from Huang et al. found that vitamin D level is positively associated with the CD4 + and CD8 + expression in the patient (35) and negatively associated with the patient’s condition, which may be related to the low epidemic ability and unbalanced immune regulation in T cell rabbits, and the susceptibility to TB may even aggravate the patient’s progress. The study shows that the number of reported TB in the elderly, aged 65 years old accounted for about 1/5 of total TB whether the diagnosis and medication compliance, or the prevention and treatment of elderly TB patients are relatively difficult (36). Age growth can lead to VitD metabolism disorders, coupled with less light time and eating, physiological decline of renal function, and reduced endogenous VitD synthesis, can result in a low concentration of blood 25-hydroxyvitamin D. At present, many elderly people with osteoporosis add calcium and vitamin D, indirectly enhance the physical fitness, has a positive effect to the prevention and treatment of TB for themselves.
A longitudinal study of patients with TB in Lahore, Pakistan, found that TB patients have severe vitamin D deficiency (37), but the Lahore region has an annual ultraviolet radiation intensity enough to induce VitD synthesis in the skin. The mean serum VitD concentration (27.3 nmol/L) was lower than the reported concentration (40.5 nmol/L) elsewhere, presenting many lung lesions and mostly bilateral lesions. Among the patients with presumed active TB, VitD deficiency preceded active TB. However, the effects of reverse causality or potential confounders cannot be excluded. Maintaining sufficient VitD levels in patients with TB may help to control the infection and activation of TB. Individuals can adjust their lifestyle and take appropriate vitamin D supplementation as a means of preventing and treating TB.
Taken together, according to the results of preceding studies, Vit D plays an important role in the prevention and treatment of tuberculosis. For TB patients, it is recommended that clinicians should strengthen nutrition monitoring to improve the VitD level in the body of patients. This review is mainly to advise decision-makers to supply VitD as a preventive and adjuvant treatment for tuberculosis susceptible populations and patients. It is suggested to add VitD supplements to TB standard regimen, especially that of the elderly, as an important progress in the personalized treatment of TB.
YT, LC, and PZ: conceptualization. XH and GW: methodology. HZ and FW: resources. YT and XH: writing—original draft preparation. LC: writing—review and editing. HZ: visualization. XH: supervision. FW: project administration. YT: funding acquisition. All authors contributed to the article and approved the submitted version.
This study was supported by the National Natural Science Foundation of China (92169117), the Hubei Youth Talent program (2021), the Hubei Public Health Youth Talent program (2021), the Hubei Medical Youth Reserve Talent program (2019), and the Hubei Young Talent Plan (2017) as well as Hubei Outstanding Young Funding Program (2020CFA075).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We thank to all participants of this study and Katherine A. Mason for her help in the language of the manuscript.
1. Reijven PLM, Soeters PB. Vitamin D: a magic bullet or a myth? Clin Nutr. (2020) 39:2663–74. doi: 10.1016/j.clnu.2019.12.028
2. Khammissa RAG, Fourie J, Motswaledi MH, Ballyram R, Lemmer J, Feller L. The biological activities of vitamin D and its receptor in relation to calcium and bone homeostasis, cancer, immune and cardiovascular systems, skin biology, and oral health. Biomed Res Int. (2018) 2018:9276380. doi: 10.1155/2018/9276380
3. Bikle DD. Vitamin D metabolism, mechanism of action, and clinical applications. Chem Biol. (2014) 21:319–29. doi: 10.1016/j.chembiol.2013.12.016
4. Yousefzadeh P, Shapses SA, Wang X. Vitamin D binding protein impact on 25-hydroxyvitamin D levels under different physiologic and pathologic conditions. Int J Endocrinol. (2014) 2014:981581. doi: 10.1155/2014/981581
5. Chun RF, Peercy BE, Orwoll ES, Nielson CM, Adams JS, Hewison M. Vitamin D and DBP: the free hormone hypothesis revisited. J Steroid Biochem Mol Biol. (2014) 144:132–7. doi: 10.1016/j.jsbmb.2013.09.012
6. Kalousova M, Dusilova-Sulkova S, Zakiyanov O, Kostirova M, Safranek R, Tesar V, et al. Vitamin D binding protein is not involved in vitamin D deficiency in patients with chronic kidney disease. Biomed Res Int. (2015) 2015:492365. doi: 10.1155/2015/492365
7. Pilz S, März W, Cashman KD, Kiely ME, Whiting SJ, Holick MF, et al. Rationale and plan for vitamin D food fortification: a review and guidance paper. Front Endocrinol. (2018) 9:373. doi: 10.3389/fendo.2018.00373
8. Wang H, Luo L, Rao G, Yang F. Research progress of tuberculosis pathogenesis and its significance for current tuberculosis prevention and control. Inf Infect Dis. (2021) 34:361–4.
9. Hunter RL. The pathogenesis of tuberculosis: the early infiltrate of post-primary (adult pulmonary) tuberculosis: a distinct disease entity. Front Immunol. (2018) 9:2108. doi: 10.3389/fimmu.2018.02108
10. Dheda K, Gumbo T, Maartens G, Dooley KE, Murray M, Furin J, et al. The lancet respiratory medicine commission: 2019 update: epidemiology, pathogenesis, transmission, diagnosis, and management of multidrug-resistant and incurable tuberculosis. Lancet Respir Med. (2019) 7:820–6. doi: 10.1016/S2213-2600(19)30263-2
11. Liu PT, Stenger S, Tang DH, Modlin RL. Cutting edge: vitamin D-mediated human antimicrobial activity against Mycobacterium tuberculosis is dependent on the induction of cathelicidin. J Immunol. (2007) 179:2060–3. doi: 10.4049/jimmunol.179.4.2060
12. Rivas-Santiago B, Serrano CJ, Enciso-Moreno JA. Susceptibility to infectious diseases based on antimicrobial peptide production. Infect Immunity. (2009) 77:4690–5. doi: 10.1128/IAI.01515-08
13. Talat N, Perry S, Parsonnet J, Dawood G, Hussain R. Vitamin D deficiency and tuberculosis progression. Emerg Infect Dis. (2010) 16:853. doi: 10.3201/eid1605.091693
14. Chan TYK. Vitamin D deficiency and susceptibility to tuberculosis. Calcified Tissue Int. (2000) 66:476–8. doi: 10.1007/s002230010095
15. Zhang M, Li Q. Advances in studying vitamin D and clinically related diseases. J Shenyang Med Coll. (2017) 19:451–4.
16. Zhang X, Yang J, Zeng Y, Shu M, Cai Y. Study on the incidence of tuberculosis and vitamin D level in Aba Tibetan children in Sichuan Province. Grassroots Med Forum. (2020) 24:3562–4.
17. Hewison M. Vitamin D and immune function: an overview. Proc Nutr Soc. (2012) 71:50–61. doi: 10.1017/S0029665111001650
18. Sato S, Tanino Y, Saito J, Nikaido T, Inokoshi Y, Fukuhara A, et al. The relationship between 25-hydroxyvitamin D levels and treatment course of pulmonary tuberculosis. Respir Investig. (2012) 50:40–5. doi: 10.1016/j.resinv.2012.05.002
19. Salahuddin N, Ali F, Hasan Z, Rao N, Aqeel M, Mahmood F. Vitamin D accelerates clinical recovery from tuberculosis: results of the SUCCINCT study [supplementary cholecalciferol in recovery from tuberculosis]. A randomized, placebo-controlled, clinical trial of vitamin D supplementation in patients with pulmonary tuberculosis’. BMC Infect Dis. (2013) 13:22. doi: 10.1186/1471-2334-13-22
20. Rathored J, Sharma SK, Singh B, Banavaliker JN, Sreenivas V, Srivastava AK, et al. Risk and outcome of multidrug-resistant tuberculosis: vitamin D receptor polymorphisms and serum 25 (OH) D. Int J Tuberc Lung Dis. (2012) 16:1522–8. doi: 10.5588/ijtld.12.0122
21. Nursyam EW, Amin Z, Rumende CM. The effect of vitamin D as supplementary treatment in patients with moderately advanced pulmonary tuberculous lesion. Acta Med Indones. (2006) 38:3–5.
22. Dai Y. Study of the Association Between Genetic Polymorphisms in Vitamin D and its Metabolic Pathways and the Risk and Prognosis of TB Onset. Nanjing: Nanjing Medical University (2013).
23. Sutaria N, Liu CT, Chen TC. Vitamin D status, receptor gene polymorphisms, and supplementation on tuberculosis: a systematic review of case-control studies and randomized controlled trials. J Clin Transl Endocrinol. (2014) 1:151–60. doi: 10.1016/j.jcte.2014.08.001
24. Jahnavi G, Sudha CH. Randomised controlled trial of food supplements in patients with newly diagnosed tuberculosis and wasting. Singapore Med J. (2010) 51:957.
25. Range N, Changalucha J, Krarup H, Magnussen P, Andersen AB, Friis H. The effect of multi-vitamin/mineral supplementation on mortality during treatment of pulmonary tuberculosis: a randomised two-by-two factorial trial in Mwanza, Tanzania. Br J Nutr. (2006) 95:762–70. doi: 10.1079/bjn20051684
26. Brincourt J. Liquefying effect on suppurations of an oral dose of calciferol. Presse Med. (1969) 77:467–70.
27. Gwinup G, Randazzo G, Elias A. The influence of vitamin D intake on serum calcium in tuberculosis. Eur J Endocrinol. (1981) 97:114–7. doi: 10.1530/acta.0.0970114
28. Stern PH, Taylor AB, Bell NH, Epstein S. Demonstration that circulating 1 alpha, 25-dihydroxyvitamin D is loosely regulated in normal children. J Clin Investig. (1981) 68:1374–7. doi: 10.1172/jci110386
29. Tjellesen L, Hummer L, Christiansen C, Rødbro P. Serum concentration of vitamin D metabolites during treatment with vitamin D2 and D3 in normal premenopausal women. Bone Miner. (1986) 1:407–13.
30. Martineau AR, Nanzer AM, Satkunam KR, Packe GE, Rainbow SJ, Maunsell ZJ, et al. Influence of a single oral dose of vitamin D2 on serum 25-hydroxyvitamin D concentrations in tuberculosis patients. Int J Tuberc Lung Dis. (2009) 13:119–25.
31. Coussens AK, Wilkinson RJ, Hanifa Y, Nikolayevskyy V, Elkington PT, Islam K, et al. Vitamin D accelerates resolution of inflammatory responses during tuberculosis treatment. Proc Natl Acad Sci USA. (2012) 109:15449–54. doi: 10.1073/pnas.1200072109
32. Ross AC, Abrams SA, Aloia JF, Brannon PM, Clinton SK, Durazo-Arvizu RA, et al. Dietary Reference Intakes for Vitamin D and Calcium. Washington, DC: National Academies Press (2011). doi: 10.17226/13050
33. Nnoaham KE, Clarke A. Low serum vitamin D levels and tuberculosis: a systematic review and meta-analysis. Int J Epidemiol. (2008) 37:113–9. doi: 10.1093/ije/dym247
34. Wejse C, Gomes VF, Rabna P, Gustafson P, Aaby P, Lisse IM, et al. Vitamin D as supplementary treatment for tuberculosis: a double-blind, randomized, placebo-controlled trial. Am J Respir Critic Care Med. (2009) 179:843–50. doi: 10.1164/rccm.200804-567OC
35. Huang T, Tang X, Chen Q, Luo M, He W, Luo D, et al. Analysis of serum vitamin D levels and clinical characteristics in elderly tuberculosis patients. Chin J Geriatr Med. (2020) 39:618–21.
36. Li G, Yang W. Detection and treatment management analysis of elderly tuberculosis in Pinggu District, Beijing, 2010–2016. China Health Care Nutr. (2019) 29:274–5.
Keywords: tuberculosis, prevention, treatment, vitamin D, association
Citation: Cai L, Wang G, Zhang P, Hu X, Zhang H, Wang F and Tong Y (2022) The Progress of the Prevention and Treatment of Vitamin D to Tuberculosis. Front. Nutr. 9:873890. doi: 10.3389/fnut.2022.873890
Received: 16 February 2022; Accepted: 05 April 2022;
Published: 17 May 2022.
Edited by:
Laurel M. Wentz, Appalachian State University, United StatesReviewed by:
Pradeep Kumar Dabla, G B Pant Institute of Postgraduate Medical Education and Research (GIPMER), IndiaCopyright © 2022 Cai, Wang, Zhang, Hu, Zhang, Wang and Tong. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yeqing Tong, dF95ZXFpbmdAMTYzLmNvbQ==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.