
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Nutr., 14 June 2022
Sec. Clinical Nutrition
Volume 9 - 2022 | https://doi.org/10.3389/fnut.2022.866518
This article is part of the Research TopicInnovative Therapies and Novel Challenges in Pediatric Intestinal FailureView all 9 articles
 Francesca Gigola1
Francesca Gigola1 Maria Chiara Cianci1
Maria Chiara Cianci1 Roberto Cirocchi2
Roberto Cirocchi2 Maria Chiara Ranucci3
Maria Chiara Ranucci3 Marco Del Riccio4
Marco Del Riccio4 Riccardo Coletta1,5*
Riccardo Coletta1,5* Antonino Morabito1,6
Antonino Morabito1,6Background and Objectives: Short-bowel syndrome (SBS) results from the loss of a significant portion of the small intestine leading to a state of malabsorption. After an intestinal loss, there is a process of adaptation involving the Glucagon-Like Peptide-2 (GLP-2), an enteroendocrine peptide also involved in nutrient absorption. Teduglutide is a recombinant analog of GLP-2 approved in 2016 to treat selected SBS pediatric patients who are dependent on parenteral support. The present systematic review aims to evaluate the efficacy of Teduglutide in pediatric patients with SBS in reducing the need for parenteral nutrition (PN).
Materials and Methods: We performed a literature search on MEDLINE and Embase to include articles up to November 2021. We included articles that involved using Teduglutide in the SBS pediatric population to define its efficacy in reducing the need for PN. The key words used were GLP-2, teduglutide, child.
Results: Fourteen studies completely fulfilled the inclusion criteria. Two hundred 23 patients were treated with Teduglutide, and the median duration of treatment was 45 weeks (IQR: 36–52.5 weeks). One-hundred and fifty-two patients were treated with 0.05 mg/Kg/d of subcutaneous Teduglutide, 38 received 0.025 mg/Kg/d and 8 received either 0.125 mg/Kg/d or 0.20 mg/Kg/d. A total of 36 patients achieved enteral autonomy (EA) after a median of 24 weeks of treatment (IQR: 24–48 weeks) and 149 patients showed a reduction in PN needs in terms of volume, calories, or hours per day. Eleven studies reported complications: gastrointestinal were the most common, with 89 cases reported in treated patients and 11 in non-treated patients.
Conclusion: Teduglutide appears safe and effective in reducing PN requirements and improving EA in the pediatric population. However, more studies are needed to understand its efficacy in the long term and after discontinuation and possible complications.
Systematic Review Registration: [https://www.crd.york.ac.uk/prospero/], identifier [CRD42022301593].
Intestinal Failure (IF) is caused by loss of a significant portion of the small intestine following congenital disease, acquired causes or surgical resection. With the inability to maintain protein, electrolyte, and micronutrient balance due to malabsorption the body may fail to sustain growth in affected children.
Short Bowel Syndrome (SBS) is a complex condition that requires specialized care to prevent complications: for these reasons, treatment should be carried out by multidisciplinary intestinal rehabilitation teams. Such a team will help combine medical approaches and surgical techniques to achieve enteral autonomy (EA) and prevent IF-associated complications. SBS patients require PN to get nutrients and fluids that cannot be obtained through enteral nutrition. It is of the utmost importance to find ways to help them achieve EA and weaning from PN since this will improve their overall quality of life and psychological status (1). Moreover, it will reduce the risk of complications related to vascular access and hepatobiliary damage associated with PN dependency. There are different surgical techniques that can be used to treat SBS patients to help them achieve EA, but sometimes surgery is not an available option, and it is important to find other ways to achieve EA in these patients.
After a significant intestinal loss, the remaining intestine will undergo adaptation. Gradually, changes will take place to maximize the absorptive area and provide the body with an adequate quantity of fluids, macro-, and micronutrients. This event is particularly true in pediatric patients, especially under 5 years of age, because bowel length increases in the first 5 years of life (2, 3). In the first months after an intestinal loss patients will suffer diarrhea with significant fluid loss. Crypts will deepen after some time, and villi will become hypertrophic, muscle layers will thicken, granting better fluids and nutrient absorption (2, 4). This process is also known as bowel adaptation (5) and while it takes some time to complete, it is usually associated with bowel dilatation, which worsens intestinal peristalsis because muscle contractions are less effective in a dilated segment (6). In SBS patients some intestinal sections are characterized by reduction of peristaltic movements due to dilatation, creating an ideal environment for bacterial proliferation and overgrowth. This alteration of intestinal microbiota is associated with abdominal pain, inflammation and damage of the mucosa, generation of toxic products such as D-Lactic acid and bacterial translocation with potential risk for sepsis (6).
The adaptation process involves several hormones, such as endothelial growth factor (EGF), growth hormone (GH), and Glucagon-like peptide-2 (GLP-2); among these, GLP-2 is a crucial component. GLP-2 is a 33-amino-acid peptide derived from a proglucagon precursor that also carries the sequence of glucagon and GLP-1. This peptide is secreted by enteroendocrine L cells, which can be found in the basal aspect of the intestinal mucosa in the distal ileum and proximal colon; nutrients induce its secretion in the intestinal lumen and then the peptide acts through second effectors such as IGF-1. GLP-2 improves nutrient absorption and gut-barrier function and slows motility in the short term. Thus, it promotes contact of nutrients with the intestinal mucosa, and it may also act as a regulator of blood supply to the gut (7). GLP-2 acts as a trophic factor for the small bowel mucosa (2, 8, 9), increasing the absorptive capacity of the intestine after intestinal loss and promoting adaptation (9, 10). Unfortunately, human GLP-2 is deactivated by dipeptidyl peptidase-IV, and for this reason, it has a half-life of 7 min if administered subcutaneously to humans (10).
For this reason, researchers studied the formation of an analog recombinant form of this peptide with a longer lifespan, Teduglutide. In 2016 the European Medicines Agency approved the use of Teduglutide in pediatric patients (ages 1–17 years old); Teduglutide is resistant to the action of dipeptidyl peptidase IV, and it has a longer half-life compared to human GLP-2 (11, 12). After its approval, many attempts have been made to use it in the pediatric population; we conducted a systematic review of the articles that assessed the effectiveness of Teduglutide in reducing the need for PN or even achieving EA in children affected by IF.
We conducted a literature search using MEDLINE and Embase to include articles up to November 2021 using the following keywords: glucagon-like peptide, teduglutide, child. We included studies with an English abstract available.
Inclusion criteria for this systematic review were original articles including pediatric patients (aged < 18 years old) affected by SBS and IF and dependent on PN, treated with a recombinant analog of GLP-2 Teduglutide. The primary endpoint was the efficacy of Teduglutide in reducing the dependence of PN. Secondary endpoints included evaluating plasmatic citrulline levels and stool frequency and consistency improvement.
The search strategy was done according to the PRISMA statement, and the present systematic review analysis was registered on the PROSPERO database (registration number: CRD42022301593) (13).
After excluding duplicates, two authors (F.G. and MC.C) reviewed the articles independently and in a blind manner and articles were first screened for inclusion by title and abstract. Any disagreement was resolved by consensus.
When two articles were published by the same research group or in case of potential patients’ overlap, we considered the study that included a higher number of patients to avoid duplication of data.
Data were extracted using an internal spreadsheet, and the following information was extracted: (1) Study characteristics; title, first author, year of publication, country of the hospital in which the study was conducted, study design, number of patients enrolled, and number of patients treated; (2) characteristics of participants and treatment; (3) outcome of treatment; (4) complications.
Given the paucity of available studies and patients identified with our selection criteria, data are reported as a narrative review.
Quality assessment of studies was performed independently and in a blind manner by two authors, according to The Risk of Bias in Non-randomized Studies-of-Intervention (ROBINS-I) tool available at https://methods.cochrane.org/methods-cochrane/robins-i-tool (14). Any disagreement was resolved by consensus.
The literature search identified 313 studies (184 from MEDLINE, 129 from EMBASE). After removing 39 duplicates, 274 studies were screened for inclusion based on title and abstract review. Given the lack of records and the condition’s rarity, we considered eligible abstracts and posters when they included relevant information regarding treatment efficacy and fulfilled inclusion criteria. The abstract or the complete text, when available, were then examined in detail. Fourteen studies fulfilled the inclusion criteria and were finally included in our review (9, 12, 15–26). Principal reasons for exclusion were overlapped with published studies (n = 8), study design (n = 2) and inclusion of non-pediatric patients (n = 1). The complete screening process is detailed in Figure 1.
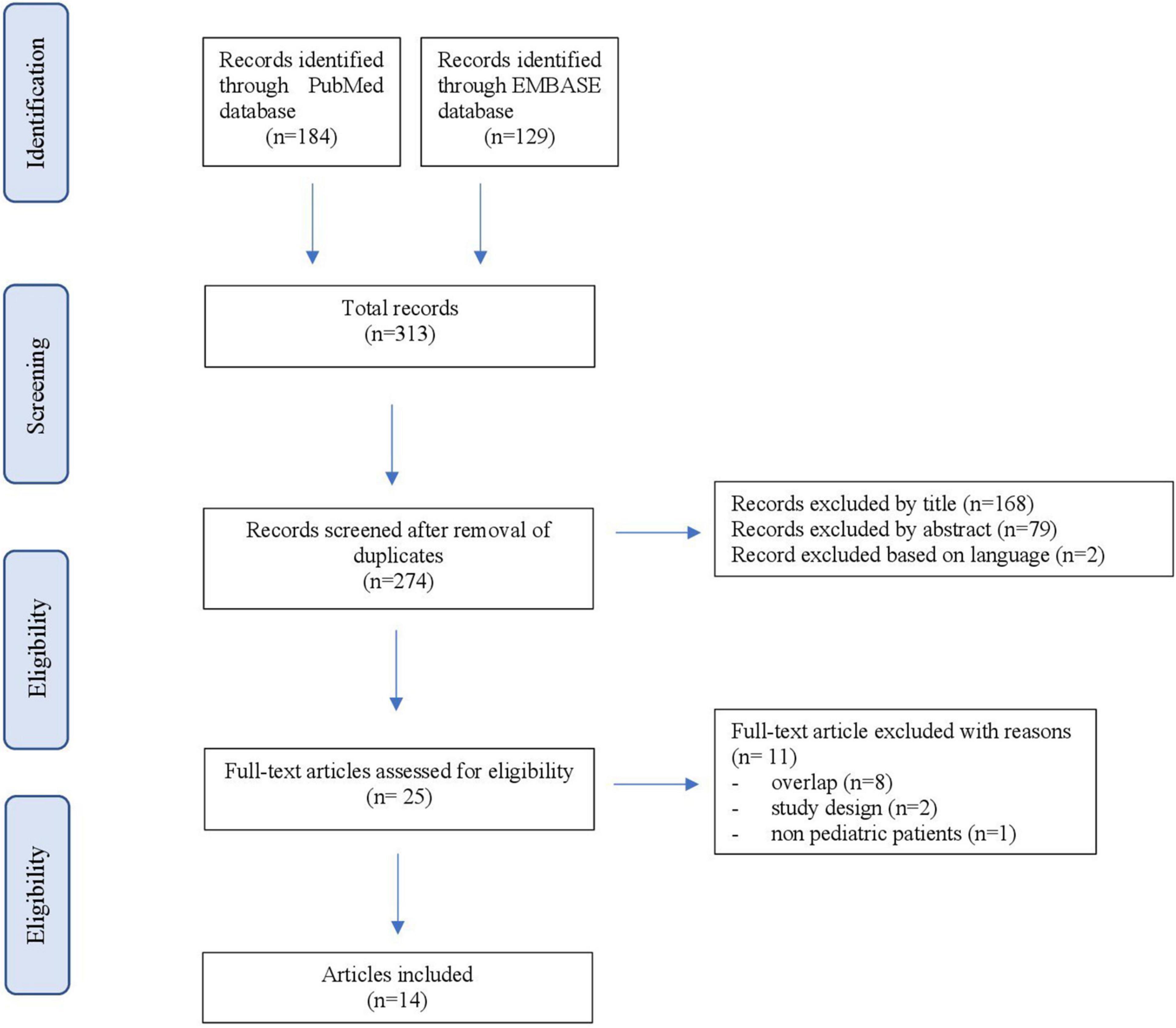
Figure 1. PRISMA flowchart.
The main characteristics of those studies are summarized in Table 1.
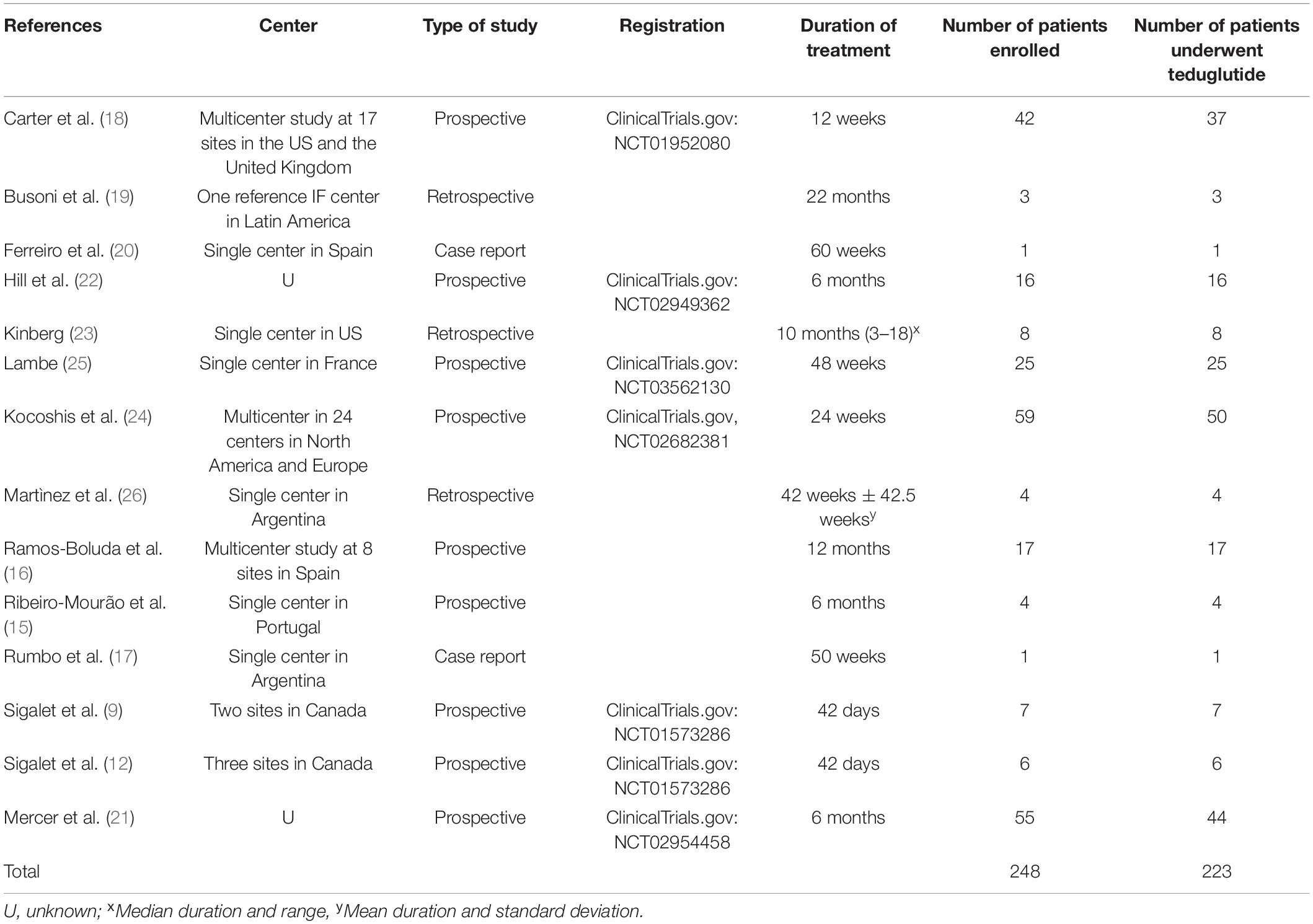
Table 1. Characteristics of included studies.
The 14 selected studies included 248 patients, of which 223 were treated with Teduglutide. Duration of treatment went from 42 days to 60 weeks with a median of 45 weeks (IQR: 36–52.5 weeks). Seven studies were single center studies, while five were multicentric. Two papers did not report the country or the center of the study. Nine were prospective, three were retrospective analyses, and two were case reports in the included studies.
All but one study included patients aged 1–17; one study included children < 1 year of age (9). The age range went from 1.5 months to 17 years. Three studies did not specify the age range. All patients were affected by SBS-IF; specific inclusion criteria of each study are reported in Table 2.
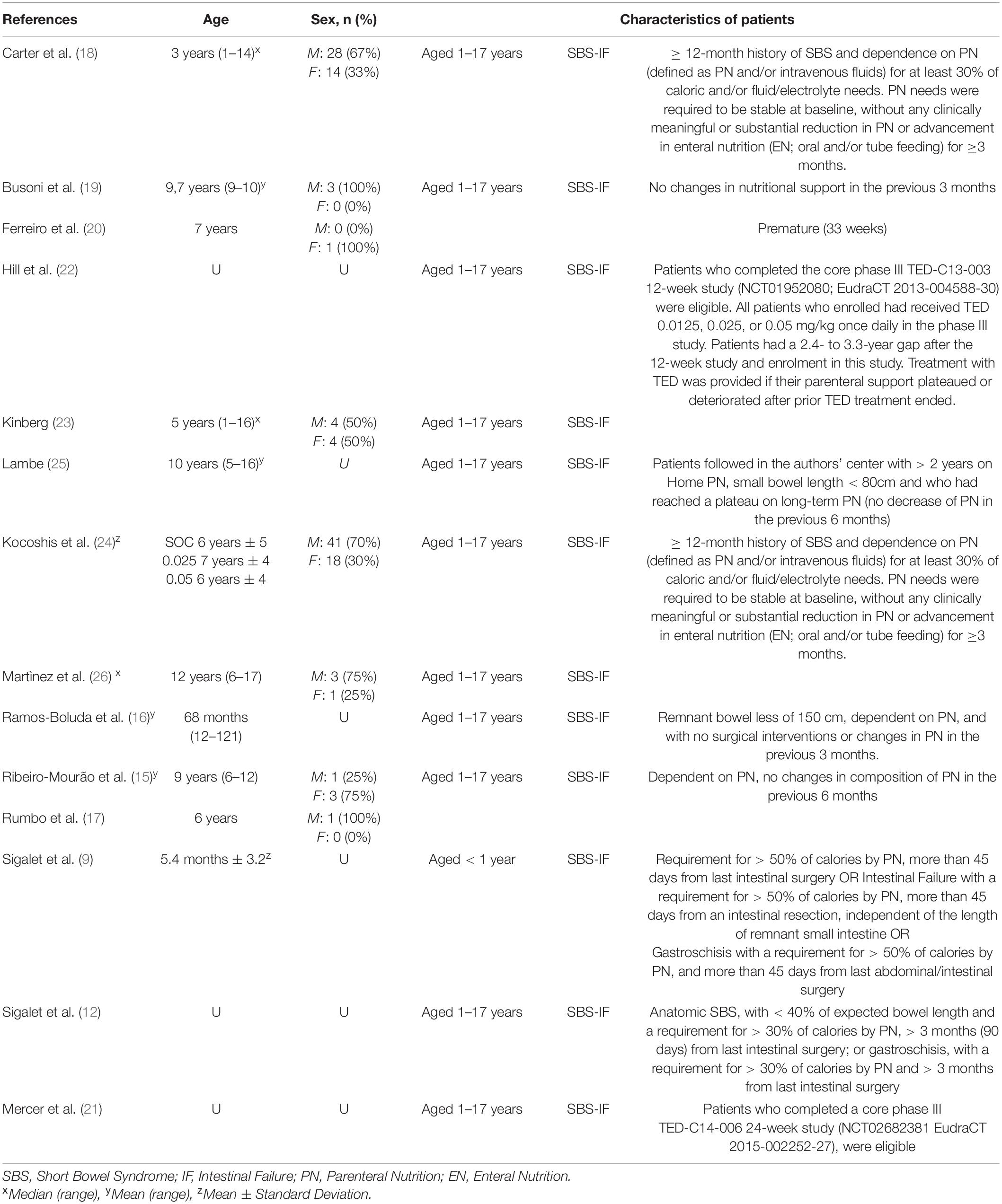
Table 2. Characteristics of patients.
Gender was specified in 8 studies, out of 122 patients for which it was known 81 (67%) were male, and 41 (33%) were female.
Ten studies specified the underlying diagnosis that led to SBS-IF, with a total number of 144 patients, while four studies did not mention the primary diagnosis. The most common diagnosis was gastroschisis (n = 44, 31%), followed by volvulus (n = 41, 28%), necrotizing enterocolitis (n = 36, 25%) and intestinal atresia (n = 23, 16%). The causes of resection are summarized in Table 3.

Table 3. Causes of intestinal resection.
Figure 2 shows the quality assessment results conducted using the ROBINS-I tool for non-Randomized studies of Intervention (14). All studies turned out to be at low risk regarding bias in classification of interventions, selection of reported results and discrimination due to missing data. Two reports (18, 24) were at moderate risk regarding the selection bias due to the allocation of open-label treatment and the resulting remote-control cohort. This caused patients selection to be influenced by post-intervention variables; furthermore, the sample size was based on the available patient population rather than a statistical power calculation. Moreover, Kocoshis et al. (24) excluded patients who were considered incapable of advancing in enteral nutrition, and the authors did not define how patients were considered as such. Carter et al.’s (18) analysis presented a small control cohort of a younger population that may be more capable of endogenous intestinal adaptation. Bias due to deviations from intended interventions was assessed as low for all the studies except for Sigalet et al. (9) (moderate): two patients did not adhere to intervention due to adverse events (which were non-Teduglutide related) and because the trial was discontinued early after a drop in potency.
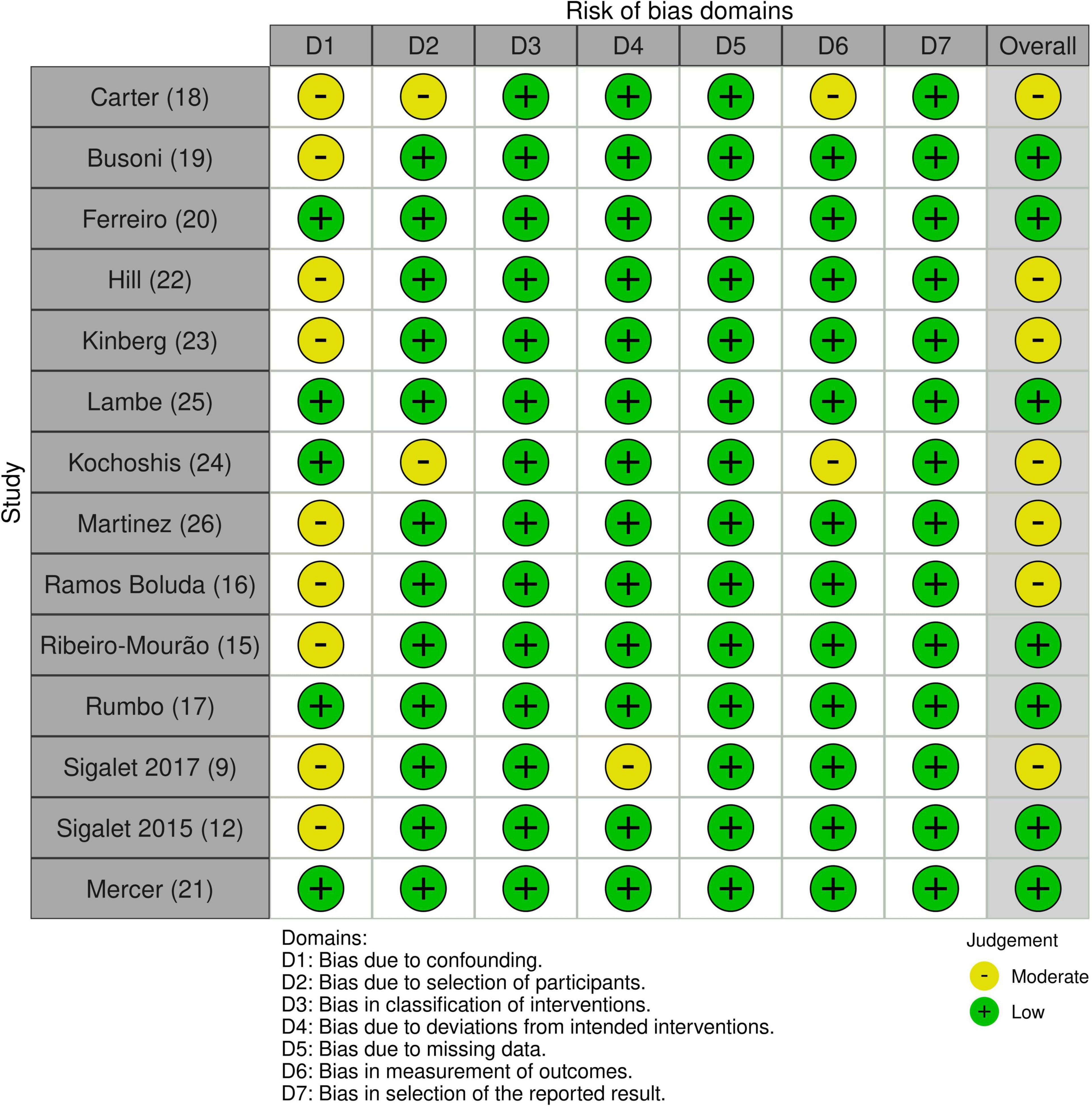
Figure 2. Quality assessment results according to ROBINS-I.
Regarding bias in measuring outcomes, all but two studies were considered at low risk, while Carter et al.’s and Kocoshis et al. studies turned out at moderate risk (18, 24). In these two studies, assessment methods are comparable across groups. Still, outcome measures could have been influenced by knowledge of the intervention: a non-blinded control sample coupled with expected clinical benefit from teduglutide may have biased parenteral support adjustments.
Bias due to confounding is low for five studies out of 14 (17, 20, 21, 24, 25). At the same time, the remainders present a moderate risk of bias due to small sample size and short follow up (9, 12, 15, 18, 19, 26), different periods of treatment with teduglutide (26) and absence of stratification of results based on age bowel length (16, 23) and teduglutide dose (22).
In conclusion, the overall risk of bias is considered low for seven out of fourteen studies (12, 15, 17, 19–21, 25), while it is classified as moderate for seven surveys (9, 16, 18, 22–24, 26).
Intestinal length varied from a minimum of 0 cm to a maximum of 175 cm (18, 20). Three papers did not specify the intestinal length at the beginning of treatment; the intestinal length mainly was determined by surgery with a total of 43 cases, even though only five papers stated the method used to determine the length of the remaining intestine in patients.
Eight studies evaluated the presence of the ileocecal valve. In 38 patients the Ileocecal valve was preserved (28%), while in 98 patients it was absent (72%) (12, 15–18, 23, 24, 26). In addition, in 6 studies, patients had been submitted to prior lengthening surgery (9, 15, 17–20) as the STEP procedure (serial transverse enteroplasty) in 82.4% of cases (15, 17, 18, 20).
Length of the colon was reported in 8 papers, mainly as a percentage of the remaining colon, ranging from 8% of total length to the presence of the whole colon.
Of the 223 treated patients 152 (61%) were treated with 0.05 mg/Kg/d of subcutaneous Teduglutide, 38 (16%) received 0.025 mg/Kg/d, 8 (3%) received 0.125 mg/Kg/d and 8 (3%) were treated with 0.20 mg/Kg/d. In 17 patients (7%) the dose was not specified. Twenty-five patients (10%) were in the Standard of Care (SOC) arm and did not receive Teduglutide. Characteristics of Teduglutide administration are summarized in Table 4.
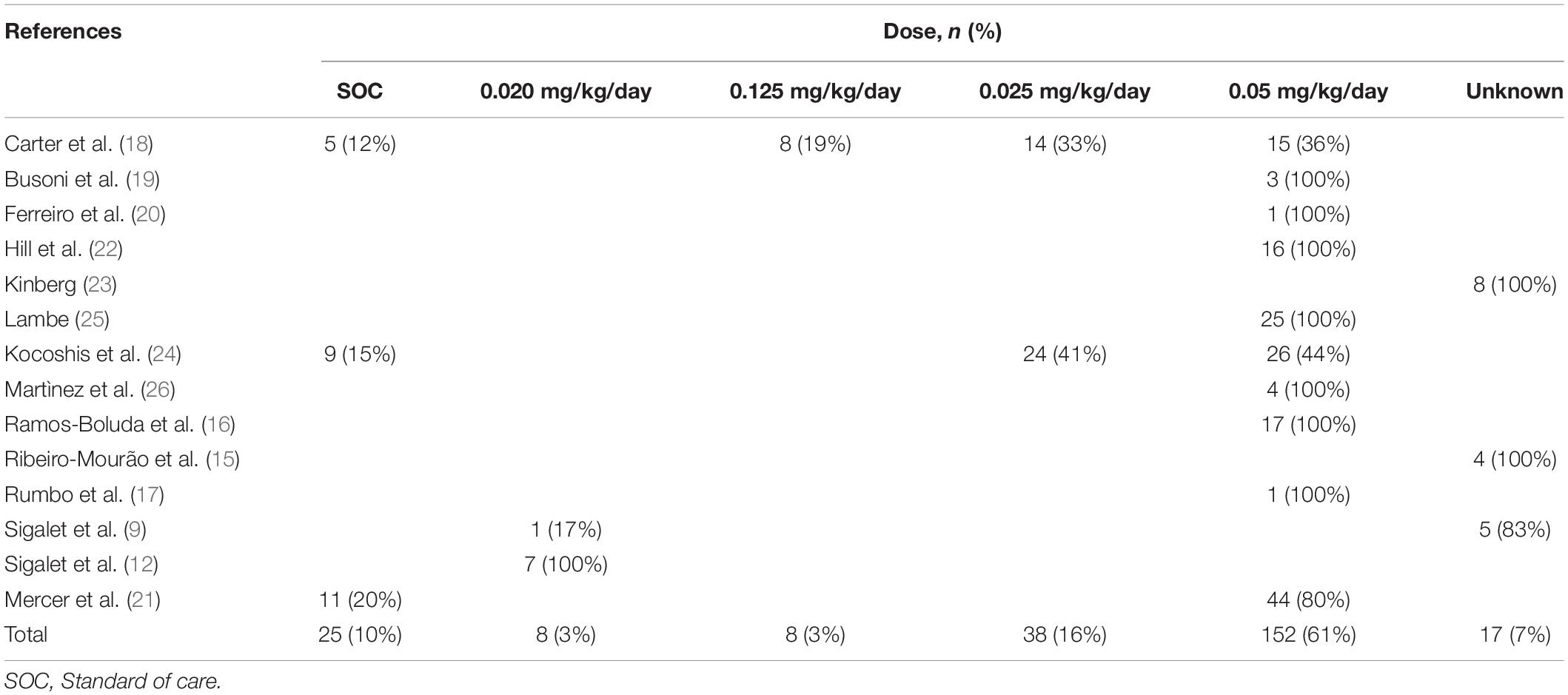
Table 4. Characteristics of teduglutide administration.
After treatment, a total of 36 patients (16%) achieved EA after a median of 24 weeks of treatment (IQR: 24–48 weeks), and 149 patients (67%) showed a reduction in PN needs in terms of volume, calories, or hours per day. Thirty-eight patients who reduced PN requirements were in the 0.025 mg/kg/day group, 105 were in the 0,05 mg/kg/day group, one patient was in the 0.02 mg/kg/day group, and five patients the dose was not known. Study results are reported in Table 5.
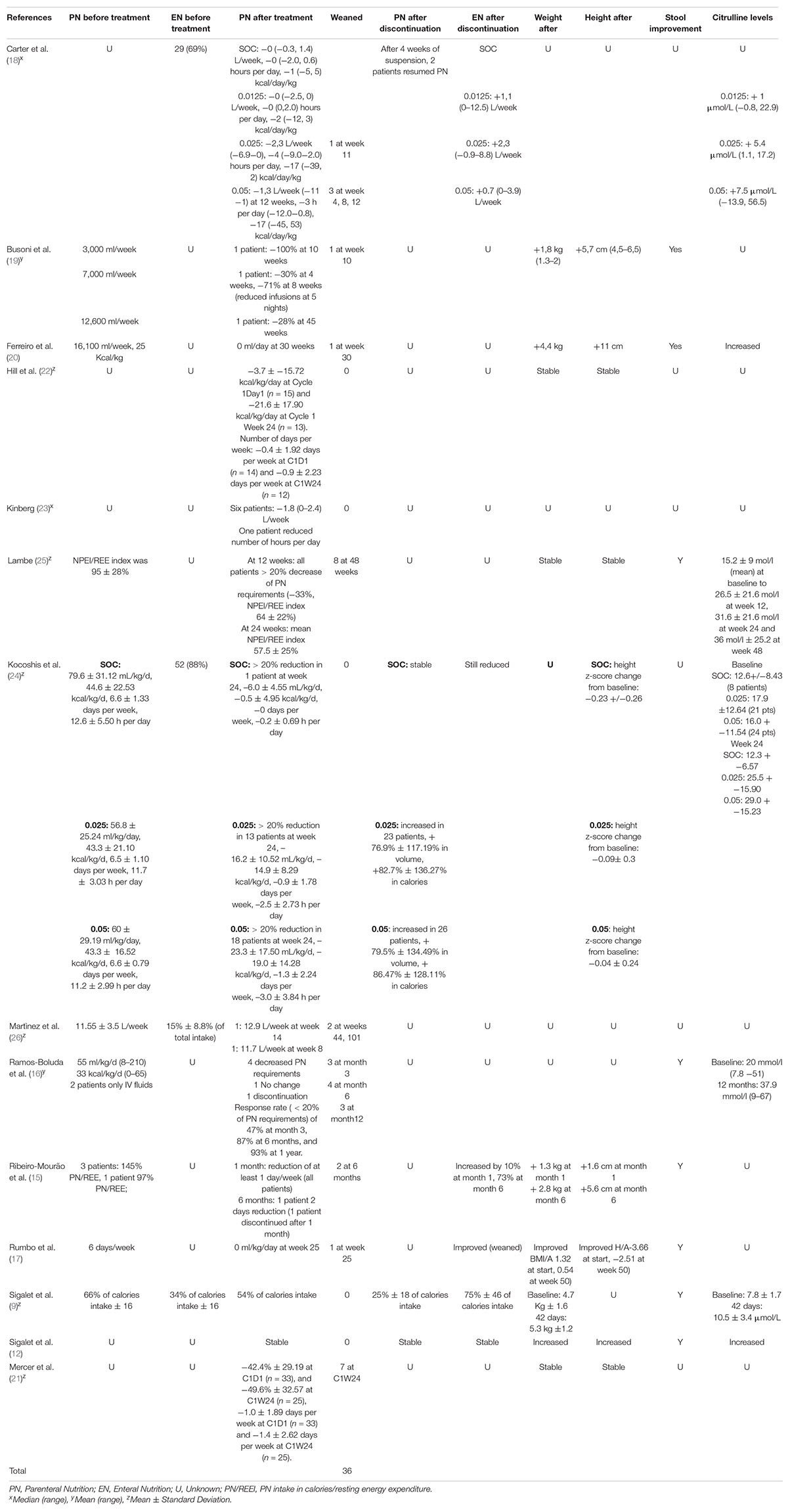
Table 5. Results.
In 7 studies (9, 12, 15, 17, 19, 20, 25), patients were evaluated for changes in weight or height with an increase in weight in 6 cases and height in 5. However, in one study (25), patients did not improve weight or height after treatment.
Eight studies out of 14 evaluated changes in stool’s quality and all of them showed an improvement in patients’ stool either in reducing the number of evacuations per day or in better quality of stool (9, 12, 15–17, 19, 20, 25).
Seven studies evaluated plasmatic levels of citrulline, showing higher plasmatic levels if compared to baseline (9, 12, 16, 18, 20, 24, 25).
Eleven studies reported complications on treatment: gastrointestinal complications were the most common event, with 87 cases reported in treated patients and 10 in non-treated patients. Other complications (more than two events) were upper respiratory tract infections, CVC related complications, pyrexia, hepatobiliary or pancreatic disorder, dehydration, or electrolyte dysfunctions or injections site bruises. One study reported insurgence of abdominal distensions, loss of appetite, and worsening diarrhea in one patient after 2 weeks of treatment discontinuation due to unexpected drug supply issues (15). The most common complications are listed in Table 6.
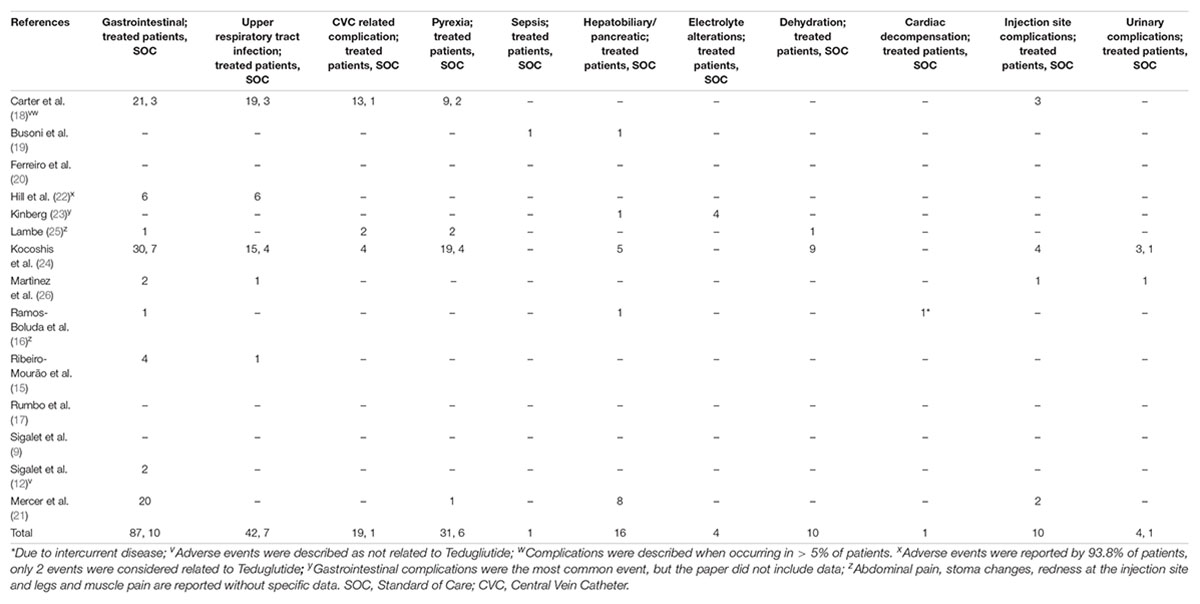
Table 6. Adverse events emerged during treatment period; different complications may have developed in the same patient.
SBS is a complex condition that affects around 24.5 children every 100,000 live births (2, 18). Achieving EA is the crucial goal in treating these patients to improve their quality of life, reduce complications and prolong their life expectancy.
In the last 40 years, treatment of SBS has changed dramatically since the introduction of Autologous Gastrointestinal Reconstruction procedures (AGIR) pioneered by Adrian Bianchi in the ‘80s (27). Non-transplant surgery establishes itself as therapy when dealing with SBS (28). Furthermore, AGIR procedures, when performed as part of multidisciplinary treatment, help reduce the need for PN and achieve EA (29). Therefore, it is crucial to find a holistic approach (medical and surgical) to treat this rare and complex condition.
Teduglutide was approved in 2016 to treat patients older than 1 year of age affected by IF. It has proven to be safe in this population and adults, and the studies included in our review confirm the safety of the treatment. Side effects and possible adverse reactions reported in the drug leaflet are respiratory tract infections, anxiety and insomnia, headache, gastrointestinal disorders, congestive heart failure, hepatobiliary, and pancreatic disorders, injections site reactions and stoma complications. The findings in our study are primarily consistent with what was already known of adverse effects based on adults’ studies. At the same time, anxiety and insomnia were not reported as typical (more than two events) in any of the studies included.
This study aimed to evaluate the efficacy of Teduglutide in reducing the need for PN in children affected by SBS-IF. Six studies among inclusion criteria specified that patients should be stable at baseline with no changes in PN support in the last 3 months at least (15, 16, 18, 19, 24, 25). Two studies only included patients at least 45 days apart from previous intestinal surgery (9, 12). It is essential to understand that weaning patients from PN could mean reducing their risk of Catheter-Associated Bloodstream Infections (CABSI) dramatically, preventing IF Associated Liver Disease (IFALD) and thrombosis, without mentioning the quality-of-life improvement and reduction of costs for the national health system (30, 31). Among included studies 16% of patients achieved EA, and 67% showed a decrease in PN needs in terms of volume, calories, or hours per day after the trial period of treatment. All studies included showed at least a partial reduction in PN requirements and demonstrated the safety of Teduglutide in the pediatric population. One study included infants treated with doses of 0.005–0.02 mg/kg/day in divided doses with no adverse events correlated to GLP-2 treatment (9).
Seven studies included showed augmentation of plasmatic Citrulline levels along with Teduglutide treatment. Citrulline can be used as a marker of intestinal function in situations where there is a significant loss of enterocytes’ mass and function, its levels appear to be strongly correlated with small bowel length and intestinal absorption in patients affected by SBS (32, 33). The correlation between citrulline levels and enteral absorption appears to be moderate, but it is strongly correlated with intestinal length and state. Citrulline levels appear higher in patients treated with Teduglutide, and this finding is consistent with our analysis (33).
Patients suffering from IF still have a high mortality rate that ranges from 30 to 50% (28). Survival of these patients also depends on comorbidities and complications due to their condition as they are exposed to Catheter Induced Bloodstream Infections, IF Associated Liver Disease, thrombosis, electrolyte dysfunction, and malnutrition. In the last years, survival has improved after the introduction of multidisciplinary intestinal rehabilitation programs, autologous bowel-lengthening procedures, and the use of new and improved formulas in PN (34). To improve their chances of survival and intestinal function, we should promptly refer these patients to highly specialized centers to get a multidisciplinary treatment that involves different professional medical and surgical treatment. Treatment in SBS-IF should not be considered a single process, and patients should be included in a personalized program that involves both medical and surgical approaches. AGIR is a fundamental part of SBS-IF treatment as it allows to gain intestinal lengths and maximize its function by improving transit and reducing intestinal dilation. AGIR procedures consist of a systematic and personalized approach to SBS, and it should be planned as part of an IRP program. Among available medical treatments in the pediatric population, Teduglutide appears safe and effective. It should be considered part of the tools in the hand of professionals to help these patients.
This review has different limitations that should be recognized. Data are extracted from both prospective and retrospective studies, and we included clinical trials and case reports. Only a limited number of studies was available at this systematic review, and only 14 studies completely fulfilled the inclusion criteria. Given the paucity of records, we decided to include abstracts without a full article available: this could impact the overall quality of included studies. Limitations concerning the availability of data and information were previously reported in the quality assessment in the results section: small sample size and short follow up (9, 12, 15, 18, 19, 26), different periods of treatment with teduglutide (26) and absence of stratification of results based on age bowel length (16, 23) and teduglutide dose (22).
In many studies, we did not find the intestinal size, previous surgery or height and weight before and after treatment. In some cases, PN and EN regimens before or after treatment were not described. Another limiting factor is the different doses at which Teduglutide was administered; the exact amount was also not specified in three papers (9, 15, 23). Finally, we must acknowledge the diversity in included studies regarding measurements of primary and secondary outcomes; data were not expressed uniformly in different papers: some used median, and range and others used mean and range or standard deviation, PN requirements were defined in ml/kg/day as well as the percentage of total intake, weight and height were reported in Kg and cm as well as Z-score. A standard definition of primary outcome across all the Intestinal Rehabilitation Units would be beneficial to measure across different units how GLP-2 can effectively help SBS patients.
Despite limiting factors, our work could contribute to the scientific community: this is the first systematic review ever conducted on the use of Teduglutide in the pediatric population. SBS is a rare disease that has a high impact on the lives of affected patients and their families. It is fundamental to give these children more options for treatment possibilities. Teduglutide seems to be a promising opportunity in selected SBS patients that must be considered when thinking of a multidisciplinary approach to this complex condition. It should be proposed for treatment in patients over 1 year of age affected by SBS who are stable following a period of intestinal adaptation after surgery. The recommended dose is 0.05 mg/kg body weight once daily.
Since its approval in 2016, different studies have been conducted on the pediatric population, but more data on the long-term efficacy of Teduglutide and complications related to treatment are needed. Moreover, it still must be studied and understood if the improvement in achieving EA and reducing PN requirements persists in the long-term, especially after treatment discontinuation. Only four studies out of the 14 included in this systematic review analyzed the PN requirement after treatment discontinuation (9, 12, 18, 24). Two studies showed an increase in PN requirements, one showed no change, and one showed a decrease in the percentage of calories taken enterally at 1 month after discontinuation (without going back to pre-treatment needs) and an increase in EA at 6 and 12 months after treatment.
This study represents the first systematic review on the efficacy of Teduglutide in the pediatric population. Our work shows that teduglutide appears safe in treating patients under 18 years of age and effectively reduces PN requirements and improves EA in pediatric patients affected by SBS. Teduglutide is a valuable tool in the hands of professionals who treat these patients, and it should be considered when creating a multidisciplinary treatment plan for these children. However, more studies are needed to fully understand the complications related to long term treatment and the efficacy of Teduglutide, especially after discontinuation of treatment.
The original contributions presented in this study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
FG, RCi, RCo, and AM contributed to conception and design of the study. FG and RCi organized the database. FG, RCi, and MDR performed data extraction. MCC and MCR performed the quality assessment. FG wrote the first draft of the manuscript. MCR, RCo, RCi, MCC, MDR, and AM wrote sections of the manuscript. All authors contributed to manuscript revision, read, and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Nagelkerke SCJ, van Oers HA, Haverman L, Vlug LE, de Koning BAE, Benninga MA, et al. Longitudinal development of health-related quality of life and fatigue in children on home parenteral nutrition. J Pediatr Gastroenterol Nutr. (2022) 74:116–22. doi: 10.1097/MPG.0000000000003329
2. Muto M, Kaji T, Onishi S, Yano K, Yamada W, Ieiri S. An overview of the current management of short-bowel syndrome in pediatric patients. Surg Today. (2022) 52:12–21. doi: 10.1007/s00595-020-02207-z
3. Struijs M-C, Diamond IR, de Silva N, Wales PW. Establishing norms for intestinal length in children. J Pediatr Surg. (2009) 44:933–8. doi: 10.1016/j.jpedsurg.2009.01.031
4. Coletta R, Aldeiri B, Morabito A. Institutional experience with spiral intestinal lengthening and tailoring. Eur J Pediatr Surg. (2018) 29:412–6. doi: 10.1055/s-0038-1660850
5. Quirós-Tejeira RE, Ament ME, Reyen L, Herzog F, Merjanian M, Olivares-Serrano N, et al. Long-term parenteral nutritional support and intestinal adaptation in children with short bowel syndrome: a 25-year experience. J Pediatr. (2004) 145:157–63. doi: 10.1016/j.jpeds.2004.02.030
6. Bianchi A, Morabito A. The dilated bowel: a liability and an asset. Semin Pediatr Surg. (2009) 18:249–57. doi: 10.1053/j.sempedsurg.2009.07.010
7. Bremholm L, Hornum M, Henriksen BM, Larsen S, Holst JJ. Glucagon-like peptide-2 increases mesenteric blood flow in humans. Scand J Gastroenterol. (2009) 44:314–9. doi: 10.1080/00365520802538195
8. Brubaker PL, Anini Y. Direct and indirect mechanisms regulating secretion of glucagon-like peptide-1 and glucagon-like peptide-2. Can J Physiol Pharmacol. (2003) 81:1005–12. doi: 10.1139/y03-107
9. Sigalet DL, Brindle ME, Boctor D, Dicken B, Lam V, Lu LS, et al. A safety and pharmacokinetic dosing study of glucagon-like peptide 2 in infants with intestinal failure. J Pediatr Surg. (2017) 52:749–54. doi: 10.1016/j.jpedsurg.2017.01.034
10. Thulesen J. Glucagon-like peptide 2 (GLP-2), an intestinotrophic mediator. Curr Protein Pept Sci. (2004) 5:51–65. doi: 10.2174/1389203043486946
11. Jeppesen PB. Teduglutide (ALX-0600), a dipeptidyl peptidase IV resistant glucagon-like peptide 2 analogue, improves intestinal function in short bowel syndrome patients. Gut. (2005) 54:1224–31. doi: 10.1136/gut.2004.061440
12. Sigalet DL, Brindle M, Boctor D, Casey L, Dicken B, Butterworth S, et al. Safety and dosing study of glucagon-like peptide 2 in children with intestinal failure. J Parenter Enteral Nutr. (2015) 41:844–52. doi: 10.1177/0148607115609566
13. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
14. Sterne JA, Hernán MA, Reeves BC, Savović J, Berkman ND, Viswanathan M, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. (2016) 355:i4919. doi: 10.1136/bmj.i4919
15. Ribeiro-Mourão F, de Braganca RL, Nogueira M, Guerra P, Espinheira C, Trindade E, et al. Short-term results of teduglutide therapy in children with short bowel syndrome. J Pediatr Gastroenterol Nutr. (2021) 72:1300. doi: 10.1016/j.jpeds.2016.10.027
16. Ramos Boluda E, Redecillas Ferreiro S, Manrique Moral O, García Romero R, Irastorza Terradillos I, Nuñez Ramos R, et al. Experience with teduglutide in pediatric short bowel syndrome: first real-life data. J Pediatr Gastroenterol Nutr. (2020) 71:734–9. doi: 10.1097/MPG.0000000000002899
17. Rumbo C, Martinez MI, Gondolesi GE, Fernandez A. Intestinal rehabilitation in Latin-America, report of the first paediatric case treated with Teduglutide, fifty weeks of follow up. J Pediatr Gastroenterol Nutr. (2018) 66:391–2.
18. Carter BA, Cohran VC, Cole CR, Corkins MR, Dimmitt RA, Duggan C, et al. Outcomes from a 12-week, open-label, multicenter clinical trial of teduglutide in pediatric short bowel syndrome. J Pediatr. (2017) 181:102–11.e5.
19. Busoni V, Izquierdo C, Frangi F, Lobos P, Orsi M. Initial experience with teduglutide in pediatric intestinal failure. J Pediatr Gastroenterol Nutr. (2021) 72:1284.
20. Ferreiro SR, Ruiz VC, Martínez LG, Ramos RN, Recio JB, Canton S. Teduglutide?: The New Weapon in Pediatric Short Bowel Syndrome Pediatric Gastroenterology, Hepatology and Nutrition Unit. Barcelona: Hospital Vall d’ Hebrón. (2019).
21. Mercer D, Carter B, Hill S, Horslen S, Kaufman S, Kocoshis S, et al. A prospective, open-label, long-term safety and efficacy study of teduglutide in pediatric patients with short bowel syndrome-associated intestinal failure: 6-month interim analysis. J Pediatr Gastroenterol Nutr. (2019) 69:11–4.
22. Hill S, Carter B, Horslen S, Kocoshis S, Yoon MJ, Grimm A. A prospective, open-label, long-term safety and efficacy study of teduglutide in pediatric patients with short bowel syndrome-associated intestinal failure: 6-month interim analysis (SHP633-303). J Pediatr Gastroenterol Nutr. (2019) 69:2019–22.
23. Kinberg S. Single-center experience with teduglutide in pediatric patients with short bowel syndrome associated intestinal failure. Transplantation. (2021) 105:S67–67. doi: 10.1097/01.tp.0000757952.00163.8c
24. Kocoshis S, Carter BA, Hill S, Horslen S, Li B, Goyal S, et al. Intestinal adaptation in children with short bowel syndrome during treatment with teduglutide. J Parente Enteral Nutr. (2016) 40:132–3.
25. Lambe CA. Monocentric single-arm study on long-term safety and efficacy of teduglutide in SBS pediatric patients on long-term home-parenteral nutrition. Transplantation. (2021) 105:S2–2. doi: 10.1097/01.tp.0000757480.19792.d7
26. Martinez MI, Rumbo C, Fernández A, Ramisch D, Gondolesi GE. Teduglutide: intestinal rehabilitation in children, our initial experience. Transplantation. (2019) 103:PS162.
27. Bianchi A. Intestinal loop lengthening—a technique for increasing small intestinal length. J Pediatr Surg. (1980) 15:145–51. doi: 10.1016/S0022-3468(80)80005-4
28. Massironi S, Cavalcoli F, Rausa E, Invernizzi P, Braga M, Vecchi M. Understanding short bowel syndrome: current status and future perspectives. Dig Liver Dis. (2020) 52:253–61. doi: 10.1016/j.dld.2019.11.013
29. Coletta R, Morabito A. Non-transplant surgical management of short bowel syndrome in children: an overview. Curr Pediatr Rev. (2019) 15:106–10. doi: 10.2174/1573396315666181129164112
30. Spencer AU, Kovacevich D, McKinney-Barnett M, Hair D, Canham J, Maksym C, et al. Pediatric short-bowel syndrome: the cost of comprehensive care. Am J Clin Nutr. (2008) 88:1552–9. doi: 10.3945/ajcn.2008.26007
31. Fonseca G, Burgermaster M, Larson E, Seres DS. The relationship between parenteral nutrition and central line-associated bloodstream infections: 2009-2014. J Parenter Enteral Nutr. (2018) 42:171–5. doi: 10.1177/0148607116688437
32. Crenn P, Messing B, Cynober L. Citrulline as a biomarker of intestinal failure due to enterocyte mass reduction. Clin Nutr. (2008) 27:328–39. doi: 10.1016/j.clnu.2008.02.005
33. Fragkos KC, Forbes A. Citrulline as a marker of intestinal function and absorption in clinical settings: a systematic review and meta-analysis. United Eur Gastroenterol J. (2018) 6:181–91. doi: 10.1177/2050640617737632
Keywords: glucagon-like peptide 2, rare disease, parenteral nutrition, short bowel syndrome, malabsorption, intestinal adaptation
Citation: Gigola F, Cianci MC, Cirocchi R, Ranucci MC, Del Riccio M, Coletta R and Morabito A (2022) Use of Teduglutide in Children With Intestinal Failure: A Systematic Review. Front. Nutr. 9:866518. doi: 10.3389/fnut.2022.866518
Received: 31 January 2022; Accepted: 11 May 2022;
Published: 14 June 2022.
Edited by:
Barbara De Koning, Erasmus MC-Sophia Children’s Hospital, NetherlandsReviewed by:
Georg Singer, Medical University of Graz, AustriaCopyright © 2022 Gigola, Cianci, Cirocchi, Ranucci, Del Riccio, Coletta and Morabito. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Riccardo Coletta, cmljY2FyZG8uY29sZXR0YUBtZXllci5pdA==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.