
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Nutr. , 31 March 2022
Sec. Nutritional Epidemiology
Volume 9 - 2022 | https://doi.org/10.3389/fnut.2022.813942
 Ana Zaragoza-Martí1,2
Ana Zaragoza-Martí1,2 Nuria Ruiz-Ródenas1
Nuria Ruiz-Ródenas1 Irene Herranz-Chofre3
Irene Herranz-Chofre3 Miriam Sánchez-SanSegundo4*Verónica de la Cruz Serrano Delgado5
Miriam Sánchez-SanSegundo4*Verónica de la Cruz Serrano Delgado5 Jose Antonio Hurtado-Sánchez1
Jose Antonio Hurtado-Sánchez1
Introduction: Pregnancy is a transcendent period for the mother and the fetus, characterized by an increase on energy requirements. Mediterranean diet (MD) is considered a healthy eating pattern that can provide the nutritional requirements of pregnancy and protect from the development of obstetric pathologies.
Objective: To know the relationship between adherence to the MD and its maternal-fetal benefits.
Methodology: A systematic review was conducted by identifying articles in the PubMed and Cochrane databases. The publication date of the studies was between 2010 and 2020, and the inclusion criteria established were that the articles were written in English and Spanish and were accessible in full text. Studies concerning assisted reproduction, gene modulation, conference abstracts, systematic reviews, and pilot studies were excluded.
Results: Finally, a total of 14 studies were included in the review. The association between the MD and the reduction of some pathologies of pregnancy, such as gestational diabetes, overweight or obesity, sleep quality, complications of childbirth, urinary tract infections (UTIs), and alterations in fetal growth was demonstrated, as well as perinatal problems, including birth weight, prematurity, gastroschisis, and other childhood problems.
Conclusion: The MD is an optimal diet to consume during pregnancy.
Women’s nutritional habits during pregnancy are considered one of the most important aspects for maternal-fetal health (1). During pregnancy, energy and nutrient needs increase to enable fetal growth and development, and major physiological changes occur, including maternal tissue formation, increased uterine size, mammary gland hypertrophy, and accumulation of fat reserves (1).
The physiological changes at the gastrointestinal level experienced by women during pregnancy (a decrease in gastric and intestinal peristalsis together with an increase in the intestinal absorption capacity of water and nutrients) (2), together with weight gain (2) and the lack of essential micronutrients that can lead to anemia (1) are essential aspects of intervention. Therefore, maternal nutritional status before pregnancy and adequate eating habits are very relevant requirements during this period of the life cycle (1). Maternal weight has been shown to have a significant relationship with fetal growth and development, so it is important to control weight gain to maintain it within a healthy range. According to the Centers for Disease Control and Prevention (CDC), women with a normal body mass index (BMI; between 18.5 and 24.9) are recommended to gain between 11 and 15 kg during pregnancy to reduce the risk of obstetric and perinatal complications (3). An increased weight gain during pregnant has been associated with higher risk of instrumented delivery and Cesarean section, gestational diabetes (GD), fetal macrosomia, neural tube defects, postpartum maternal obesity, and even obesity during childhood and diseases in the adult life of the newborn (1). Maternal insufficient weight gain has also been considered as a risk factor for miscarriage, preterm birth, and low birth weight (1). In this sense, it has been found that newborns with low birth weight may have difficulty establishing adequate breastfeeding as well as an increased risk of contracting diseases and developmental delays (3).
The lack of micronutrients during pregnancy has also been linked to the presence of anemia (1). According to data from the World Health Organization (WHO), it is estimated that, in 2011, around 38.2% of pregnant women suffered from anemia, the main cause being iron deficiency (4). Anemia during pregnancy is directly associated with a high risk of preterm birth, low birth weight, maternal mortality (1), and perinatal (5) and neonatal mortality (1).
Given the available evidence of changes affecting women’s health during pregnancy, it is necessary to follow an adequate diet during gestation. The Mediterranean diet (MD) is considered one of the dietary patterns that guarantees a better supply of nutrients. The MD is defined as the traditional dietary pattern found in the early 1960s in Greece, southern Italy, Spain, and other olive-growing countries of the Mediterranean basin (6). The MD use generou amounts of extra virgin olive oil (EVOO) as the main culinary fat and has a high intake of foods of plant origin: fruits, vegetables, legumes, nuts and seeds, and whole unprocessed grains, a moderate intake of fish, poultry, eggs, and dairy products, especially yogurt and cheese, but not butter or cream, and low intake of sweet desserts, red and processed meats (6).
Several previous studies, particularly those reported within the largest MD research project to date, PREDIMED [PREvención con DIeta MEDiterránea (Prevention with MD)] (7), conclude that following an MD is inversely related to overall mortality (8), the incidence of coronary heart disease (9), cardiovascular events (10), and thrombotic stroke (11). It is also inversely related to the incidence of cancer in general (12, 13) (including breast cancer (14) and colorectal cancer (15), as well as to Type 2 diabetes mellitus (in adulthood) (16) or even to hip fractures (17). All these benefits may be favored by the high content of antioxidants of this plant diet, the high fiber content, and the low glycemic load, in addition to the high content of monounsaturated and polyunsaturated fatty acids in relation to saturated ones, as the former reduce cholesterol levels (6).
MD has also positive effects on pregnancy. Numerous studies show that prenatal diet affects maternal-fetal outcomes. Specifically, the St. Carlos Gestational Diabetes Mellitus Prevention Study (18) establishes a direct relationship between high adherence to MD during pregnancy and decreased risk of GD, urinary tract infections (UTIs), prematurity, and low-weight newborns (18). Other research shows more benefits for the mother, as adherence to MD during pregnancy is also associated with better sleep quality throughout pregnancy (19). In addition, MD prevents overweight and obesity during pregnancy, which means that it helps to maintain adequate weight gain (20). Regarding perinatal outcomes, studies conclude that high adherence to MD during pregnancy reduces some cardiovascular risk factors such as high blood pressure and adiposity (21).
Given the available evidence that MD could play a protective role in maternal and fetal health during pregnancy, the aim of this study was to conduct a systematic review of the literature to study the effects of MD during the gestational period.
A systematic review of the literature was carried out, following the PRISMA methodology (22) as a reference. The quality of each of the studies was assessed with the Cochrane Collaboration Risk of Bias (ROB) tool (23), which includes seven items that analyze six domains of bias. This tool classifies the quality of articles into three levels: high, low, or unclear.
The first author (AZ-M) and the second author (NR-R) of the study rated each included article independently, and the discrepancies were resolved through an agreement with the third author (MS-S). Cohen’s kappa statistic was calculated to assess reliability among evaluators for the ROB without elements that assessed the blinding of participants or evaluators, as all studies were rated as high ROB by the two evaluators when all the elements were analyzed. Inter-evaluator reliability was analyzed using Cohen’s kappa statistic, obtaining an intraclass correlation coefficient (ICC) value of 0.8.
To obtain the documents, electronic searches were carried out in the international databases PubMed and Cochrane Library.
To obtain the documents, electronic searches were carried out during the months of October, November, and December 2020. We used the following keywords transformed into terms MeSH (Medical Subject Heading): “diet, Mediterranean,” “pregnancy,” “treatment adherence and compliance” combined with the Boolean operators AND and OR. Table 1 shows the search strategy used in the databases.
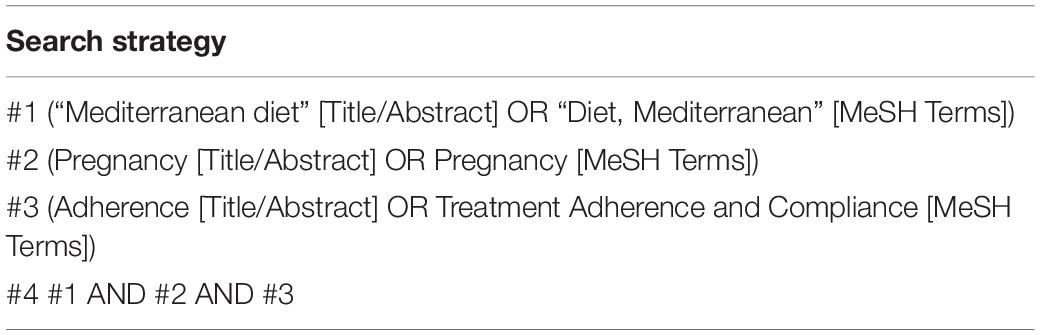
Table 1. Database search strategy.
The inclusion criteria were: (1) articles accessible in full text, open access, and available abstract; (2) articles written in English or Spanish; (3) articles published within a range of 10 years: between 2010 and 2020; (4) articles that included at least one sample of pregnant women, and (5) that included MD as an outcome.
We excluded articles that analyzed (1) sterility or assisted reproduction techniques; (2) gene modulation studies; (3) duplicate studies; (4) conference abstracts; (5) systematic reviews or meta-analyses; (6) pilot studies.
The selection of articles was made by reading the title and abstract of all articles resulting from the search in PubMed, and Cochrane. The quality of each study was independently evaluated by two authors, using the Crombie criteria adapted by Petticrew and Roberts. Disagreements were resolved by a third author.
The AXIS (24) critical evaluation tool was used to assess the quality and ROB in cross-sectional studies (Table 2). Randomized clinical trials were assessed using the PEDro tool (25) (Table 3). Finally, both the quality of the cohort studies (Table 4) and the quality of cases and controls were assessed with the Newcastle-Ottawa scale (26) (Table 4). For all scales, agreements were above kappa values of 0.75. The third and last authors (MS-S and AZ-M) rated each included article independently, and discrepancies were resolved by agreement with the second author (JH-S). We also calculated the Cohen’s Kappa statistic to assess interrater realibility. The Cohen’s Kappa provides a level of agreement between two or more raters than is higher than chance. It is considered as moderate or substantial when values are above 0.6 (moderate) or 0.8–1 as substantial agreement (27).

Table 2. First ten questions of the AXIS tool.
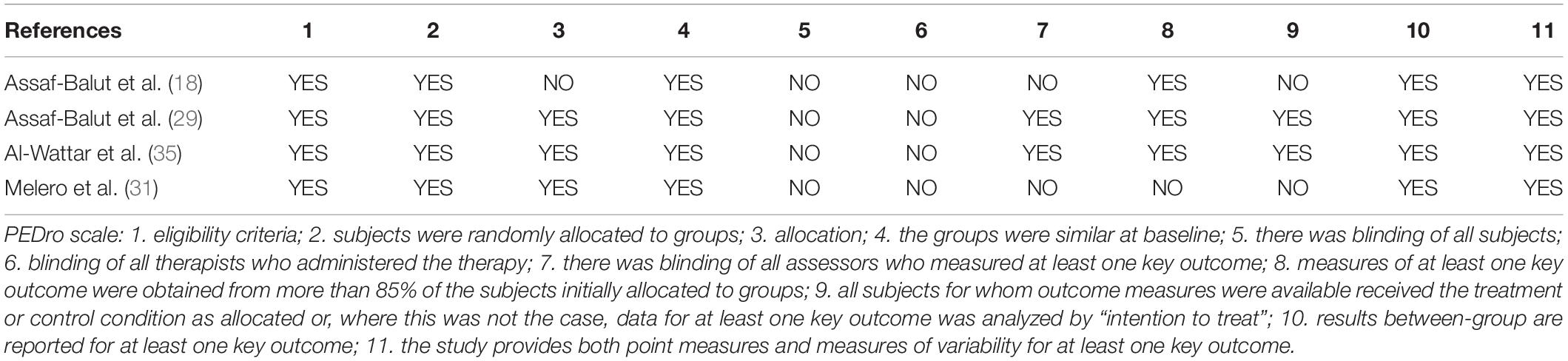
Table 3. PEDro tool questions.
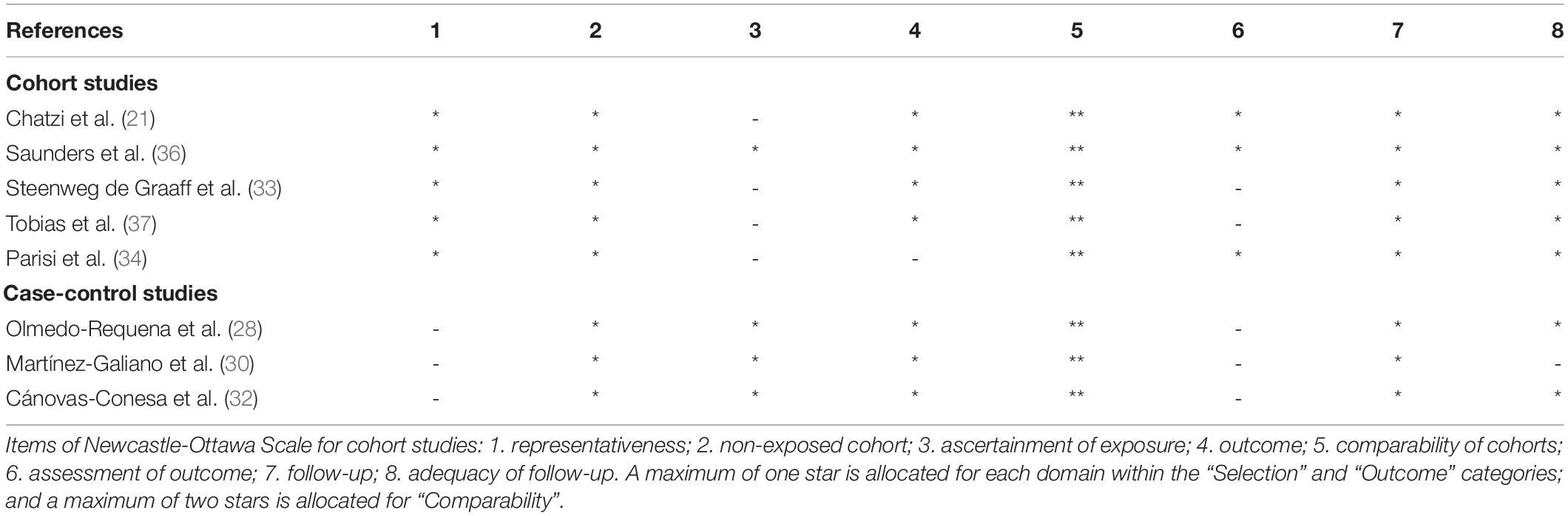
Table 4. Tool questions Newcastle-Ottawa.
Data extraction was performed by the lead review author, taking into account the year of publication (2010–2020), the design and objective of the study, the year in which the study was conducted, the sample size, the mean age of the participants, the country of origin, the outcomes of the interventions, and the conclusions of the studies.
The results were grouped into two large blocks: (1) maternal outcomes and (2) perinatal outcomes, which were classified according to the description of the concrete benefits of consuming MD during pregnancy. The maternal outcomes were divided into five sub-blocks: (I) Gestational diabetes (GD), (II) Healthy lifestyle, (III) Complications in childbirth, (IV) UTIs, and (V) Fetal growth; whereas the benefits found in newborns, were grouped into four subgroups: (I) Birth weight, (II) Prematurity, (III) Gastroschisis, and (IV) Problems in childhood.
A total of 121 articles were identified. After removing the duplicates there were 108 articles. After applying the “2010–2020,” “English” and “Spanish” filters, and all duplicate articles were discarded: 43 articles were deleted. Subsequently, the titles and abstracts were read, and another 51 articles were discarded, according to the inclusion and exclusion criteria set out above. Finally, a total of 14 articles were included in the review (Figure 1).
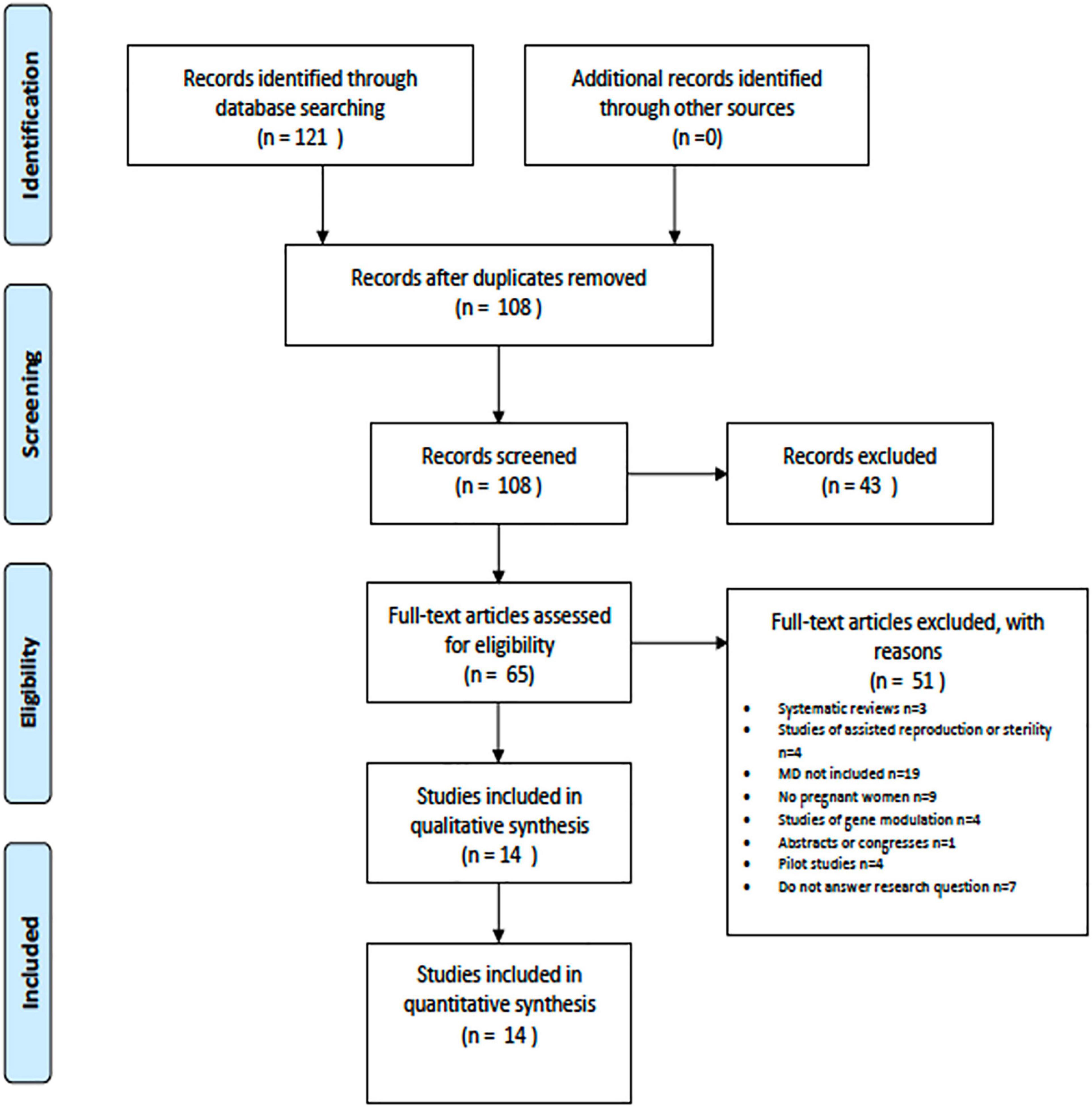
Figure 1. Selection of studies.
Table 5 shows the characteristics of the articles included. Due to the nature of this review, all participants in these studies were pregnant women whose mean age was 31 ± 2.36 years.
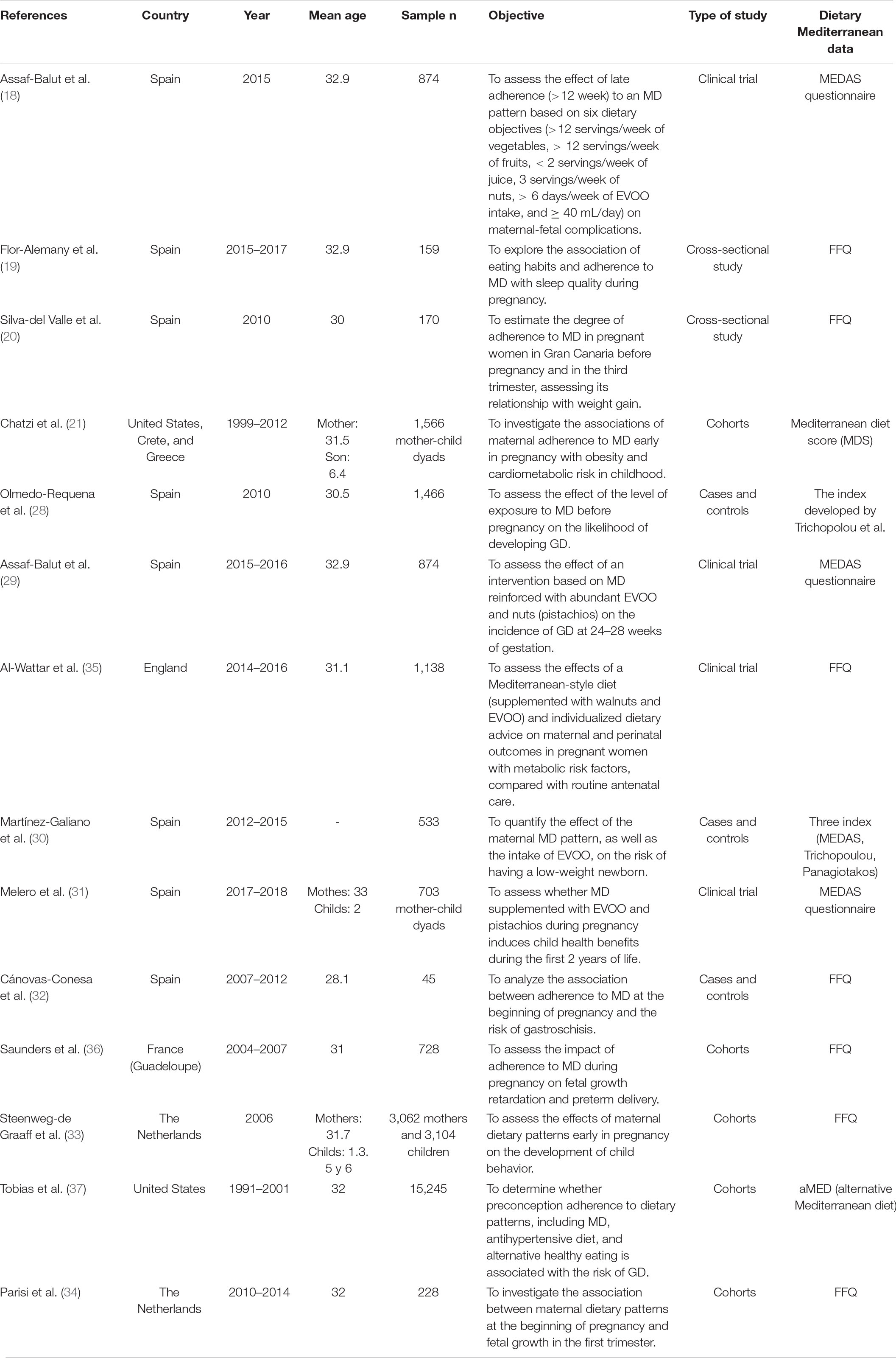
Table 5. Description of the studies.
As for the country of origin, 57.14% (n = 8) (18–20, 28–32) of the articles were carried out in Spain, two studies were carried out in the Netherlands (14.29%) (33, 34), one in England (7.14%) (35), one in France (more specifically on the island of Guadeloupe) (7.14%) (36), one in the United States (7.14%) (37), and, finally, one that included participants from the United States, Greece, and Crete (7.14%) (21). In terms of design, of the 14 studies included, five were cohorts (35.71%) (21, 33, 34, 36, 37), four clinical trials (28.57%) (18, 29, 31, 35), three cases and controls (21.43%) (24, 30, 32), and two were cross-sectional studies (14.29%) (19, 20).
Finally, adherence to the Mediterranean diet was measured through the MEDAS (Mediterranean Diet Adherence Screener) in 3 studies (18, 29, 31), through a FFQ (Food frequency questionnarire) in 7 studies (19, 20, 31–35), one study through the Mediterranean diet score (MDS) (21), another study through the index created by Trichopoulou (28) and another study with the aMED (alternative Mediterranean diet) (37). In addition there was a study that evaluated the Mediterranean diet with three indices, the MEDAS, the one created by Trichopoulou and the one created by Panagiotakos (30).
Table 6 shows the results of the studies included in the review regarding maternal benefits.
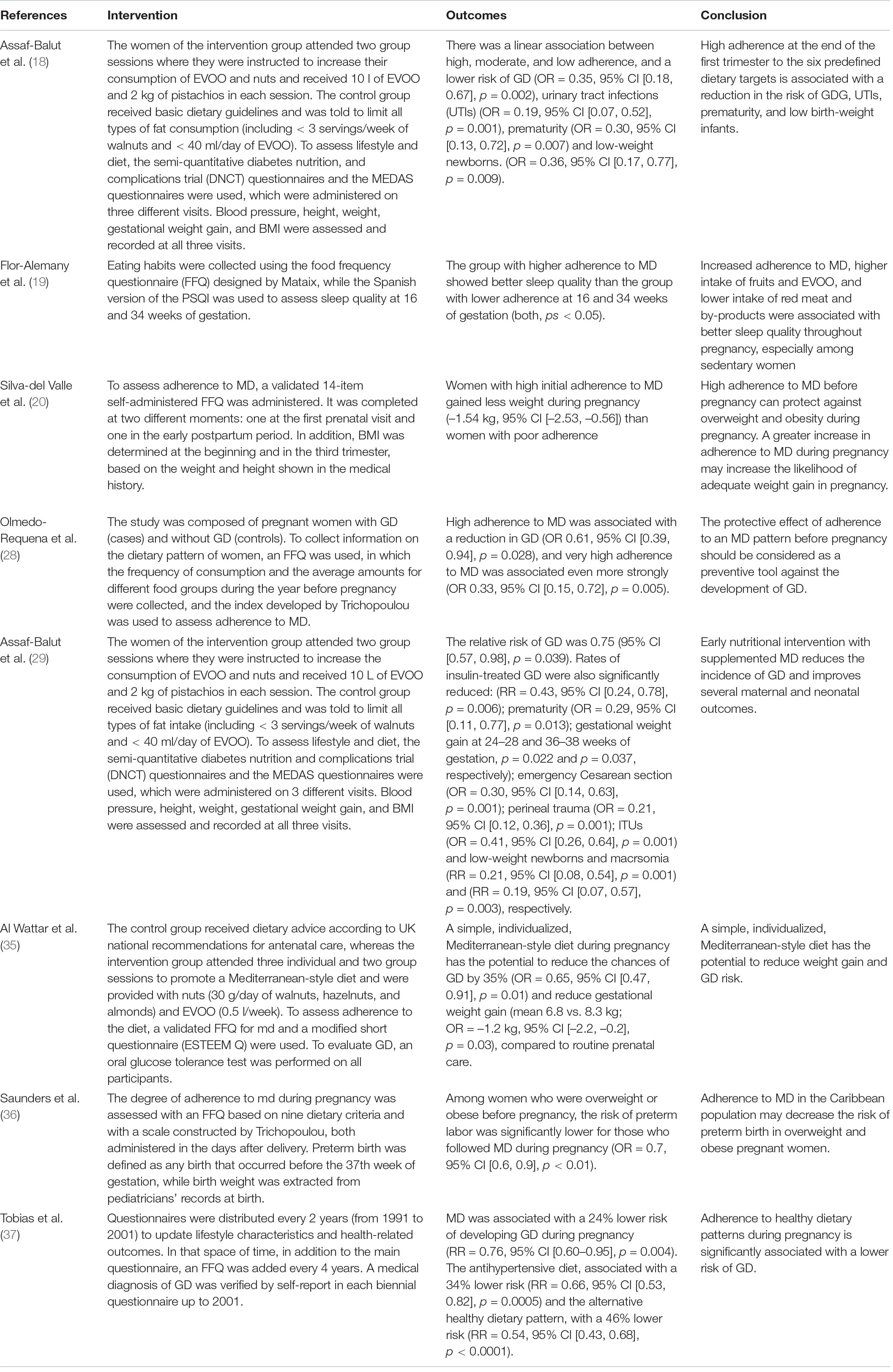
Table 6. Maternal outcomes.
Nine studies (18–20, 28, 29, 34–37), found positive maternal effects related to adherence to MD during pregnancy.
A total of five studies (18, 28, 29, 35, 37) obtained found that MD acts as a protective factor against the development of GD.
In three studies (18, 29, 37), MD was supplemented with EVOO and nuts. Two articles found that high adherence to MD was associated with a 65% lower risk of GD (p = 0.002) (18) and (p = 0.039) (18, 29). MD supplemented with EVOO and nuts in pregnant women with metabolic risk (obesity, arterial hypertension, or hypertriglyceridemia) was also found to lead to a 35% lower likelihood of developing GD if their adherence to MD was high (p = 0.01) (35).
Two studies analyzed the effect of MD consumption before pregnancy. One of the studies showed a decrease of 24% in the risk of developing GD (p = 0.004) when women followed an MD nutritional pattern before pregnancy (33). In addition, one study (28) found a protective effect of MD and low consumption of meat and derivatives on the development of GD (p = 0.028 for high adherence to MD and p = 0.005 for very high adherence) (28).
Four studies (19, 20, 29, 35) analyzed the relationship between MD consumption during pregnancy and the healthy lifestyles during pregnancy. Results suggested that mothers with adherence to MD gained less gestational weight (29, 35). Also, women with a strong preconception adherence to MD gained less weight during pregnancy (20). A cross-sectional study conducted by Flor-Alemany et al. (19) showed that greater adherence to MD was associated with better sleep quality during weeks 16–34 of gestation, especially among sedentary pregnant women (p < 0.05).
Two studies (29, 36) associated MD consumption with reduced complications during childbirth.
First, in the cohort study conducted by Saunders et al. (36), it was hypothesized that adherence to MD decreases the risk of preterm birth but they only found relevant results in overweight or obese women (p < 0.01).
In addition, in the second study (29), it was found that women who had followed an MD pattern were less likely to give birth by emergency Cesarean section as well as a lower probability of perineal trauma during childbirth (both, ps = 0.001). This reduction could be due to improvements in the evolution of childbirth or also to the reduction in the number of newborns with macrosomia (29).
In two studies, high adherence to MD was found to reduce the risk of UTIs during pregnancy. This relationship (p = 0.001) was found in the research of Assaf-Balut et al. (18, 29), and this result may be due to the relationship between MD, inflammation, and immunomodulation. This effect is possibly due to the presence of some food components, such as phenolic compounds and oleic acid (29).
Finally, one study (37) found a significant association between maternal adherence at the beginning of pregnancy to a high content of fish and EVOO and a dietary pattern low in meat (characteristic food of the Mediterranean diet), with increased fetal growth. An increase in embryonic volume was also found, with percentages of 20.4% at 7 weeks and 14.4% at 11 weeks (34).
Table 7 shows the results of the studies analyzed regarding perinatal benefits. A total of seven studies (18, 21, 29–33), showed a statistically significant relationship between adequate maternal adherence to MD and improvements in perinatal health.
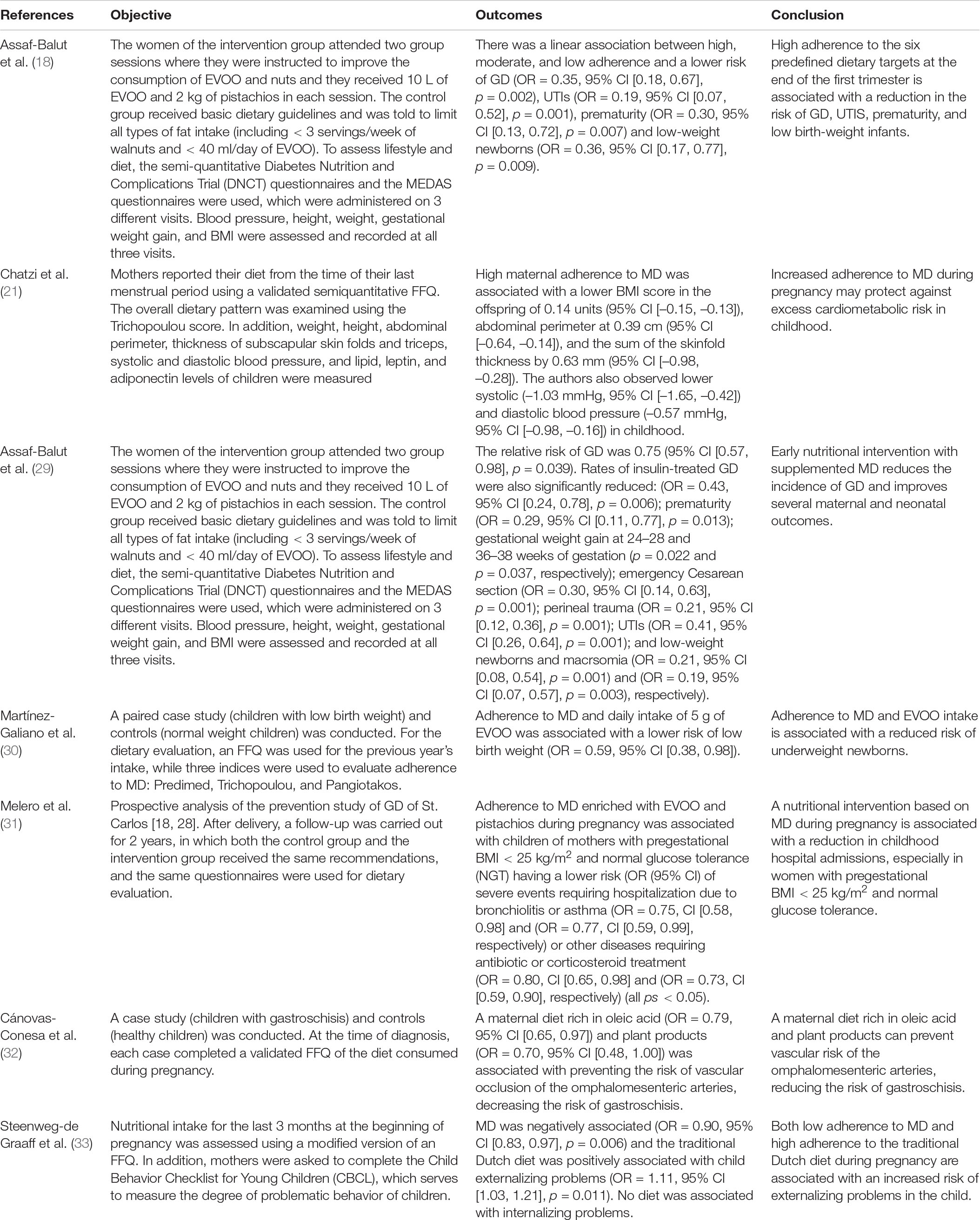
Table 7. Perinatal outcomes.
Three studies (18, 29, 30) found a relationship between maternal adherence to MD and birth weight. In particular, it was found that MD reduced the probability of low birth weight (18, 29) and that the EVOO component and the presence of macrosomia was essential to control the low birth weight (35) because the risk of macrosomia is inversely associated with diets of low glycemic index, a characteristic of MD. The risk of newborns with low weight is a consequence of placental insufficiency. In this sense, MD supplemented with EVOO and nuts could play a fundamental role in improving placental flow and, therefore, decreased intrauterine growth retardation (29).
Maternal adherence to MD was associated with a significant reduction in the rates of preterm infants (18, 29).
In a study by Cánovas-Conesa et al. (32), it was observed that adherence to MD, rich in EVOO and vegetables, helped to prevent the risk of vascular occlusion and risk of gastroschisis.
The relationship between maternal adherence to MD and health in children’s development was analyzed in three studies (21, 31, 33). First, the cohort study of Chatzi et al. (21) revealed that increased adherence to MD at early gestation was associated with lower adiposity levels (BMI 0.14 units lower, arm crease thickness 0.63 mm lower, and abdominal circumference 0.39 mm lower), leptin (reflecting lower fat and lower triglyceride levels in childhood) and lower systolic and diastolic blood pressure in children. According to the authors, this may be due to the effect of MD’s low glycemic index and its high antioxidant content, which can lead to better fetal glucose metabolism and better metabolic function and, finally, influence the individual’s susceptibility to weight gain in childhood (21).
In addition, in the research conducted by Steenweg-de Graaff et al. (33), an association was found between the consumption of MD during pregnancy and a lower risk of developing behavioral problems in childhood, specifically, externalizing problems (attention problems and aggressive behavior) (p = 0.006), whereas the traditional Dutch diet favored the development of these problems (p = 0.011) by Steenweg-de Graaff et al. (33).
Finally, the study of Melero et al. (31) found a relationship between maternal intake of MD and reduced risk of hospitalization in children up to 2 years of age. However, this relationship was stronger in women with a pregestational BMI < 25 kg/m2 and normal glucose tolerance (p < 0.05) (31).
The objective of this study was to conduct a systematic review of the literature to study the effects of the MD during the gestational period both on the mother and the fetus. A total of 14 studies were analyzed. The results showed that the MD was associated with the reduction of some pathologies of pregnancy, such as GD, overweight or obesity, complications of childbirth, UTIs, alterations of fetal growth, and sleep quality; as well as perinatal problems, including birth weight, prematurity, gastroschisis, and other childhood problems. These results may be due to the relationship between MD, inflammation, and immunomodulation. This effect is possibly a consequence of the presence of some food components, such as phenolic compounds and oleic acid (29). Some previous studies have suggested that some foods such as nuts or olive oil may facilitate weight loss and may have potential effects on insulin sensitivity and inflammation (38). Also, the MD has potential antioxidant effect given their high levels of lutein, β-carotene, and γ-tocopherol (39) improving the inflammatory cytokine profiles.
Likewise, the results of this study show that MD favors a decrease in complications during pregnancy, as it is related to a lower risk of preterm delivery (32), emergency Cesarean sections, and perineal trauma (29). Also, adherence to MD promotes adequate fetal growth (34) because this type of diet provides the nutrients necessary for the correct development of the fetus (34). As for the newborn, MD intake during pregnancy has been shown to be a protective factor linked to a decrease in the number of hospitalizations (31), a lower risk of gastroschisis (32), a decrease in attention problems and aggressiveness (33), as well as a lower risk of developing cardiometabolic complications, such as hypertension or obesity (21), a lower risk of prematurity (18, 29), and adequate birth weight (18, 29, 30).
These results are similar to those obtained in other systematic reviews. For example, Biagi et al. (40) and Amati et al. (41) found a positive effect between adherence to MD during pregnancy and children’s health. Hassani Zadeh et al. showed that following an MD pattern during pregnancy is beneficial both for the mother and the offspring, and also showed that the MD can potentially decrease the risk of suffering from atopia in the offspring and GD in the mother (42), results that are highly consistent with our study. In particular, MD is associated with a lower incidence of asthma/allergic diseases in childhood, although further studies would be needed to clarify this relationship (38). The beneficial effects of MD had also been associated with health parameters, including improved glycemic control, a reduction in insulin use during pregnancy, a decreased risk of newborns with macrosomia (43), and better control of blood pressure. Eating patterns before and during pregnancy characterized by a high intake of fruits, vegetables, legumes, whole grains, nuts, olive oil, and a low intake of red meat and processed meats have been associated with an increased risk of hypertension during pregnancy. Although the biological mechanisms by which MD plays a protective role are not precisely known, these findings could indicate that the consumption of unsaturated fatty acids and micronutrients as well as some bioactive compounds make this diet help prevent complications during pregnancy (44).
Due to the beneficial effects of the MD, some authors highlight the need to recover the MD pattern in the general population and, in particular, in pregnant women, to avoid overweight and obesity, problems during pregnancy, as well as to achieve an adequate weight gain, as all this is related to overweight and the increase in adiposity in the offspring (40, 41, 44, 45).
The present work presents several limitations that require future areas of research. First, the wide variety in the design of the included studies, the variability of the strength of association in different health outcomes, and the presence of studies that used a small sample size limit the conclusions. In addition, the search only included publications in English and Spanish; therefore, not all current evidence to date may be represented. Thirdly, the data sources used for this review were PubMed, Medline, and the Cochrane Library. Fourthly, the intervention was performed at different times of gestation, which may affect the robustness of the results and conclusions. Also, there is a bias of quality and selection of articles that, despite having been reduced to the maximum, is still inherent in this type of study. And finally, there is high variability in the type of intervention performed, in the method of collecting data, and in the foods that constitute MD in each region, which can make it difficult to compare their effectiveness. However, this study has strengths; for example, it is one of the few reviews existing in the literature, where the relationship of the MD is analyzed in an applied way not only in pregnancy, but also in the offspring. This study provides also evidence about the beneficial effect of the MD in the reduction of some pathologies of pregnancy including: sleep problem, gastroschiis, alteration in fetal growth and prematurity. In addition, we examined the quality of studies using three independent tool. We found that most studies (80%) described main areas of bias in controlled clinical studies including: eligibility criteria, allocation, randomization, measurement of drop outs, measures of at least one key outcome, results between group. However, few studies were described as double-blind or the blinding method was inappropiated. Future studies should be carried out controlling the ROB of studies. Finally, future longitudinal studies should be carried out with a large sample to obtain strongly conclusive data evidencing the need to promote adherence to the MD in this population, working not only with pregnant women but with the family as a whole. In this regard, more studies on health promotion and prevention are needed to improve the health of pregnant women and their families.
The MD is optimal to ensure an adequate supply of nutrients during pregnancy. It provides all the energy and nutrients required to allow fetal growth and development, protecting from the development of obstetric pathologies including complications of childbirth, infections and alteration in fetal growth. The MD diet also can prevent some maternal complications such as diabetes, sleep quality and overweight or obesity. Given the available evidence of changes affecting women’s health during pregnancy, it is necessary to follow an adequate diet during gestation. Therefore, strategies to promote adherence to MD can be of considerable importance for public health given that MD may play a protective role in maternal and fetal health during the gestational period.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding authors.
NR-R and AZ-M: conceptualization. NR-R, AZ-M, and MS-S: methodology. VS, IH-C, MS-S, and JH-S: validation. NR-R: formal analysis and writing—original draft preparation. NR-R, AZ-M, MS-S, JH-S, VS, and IH-C: investigation. AZ-M: data curation and supervision. NR-R, AZ-M, MS-S, and VS: writing—review and editing. NR-R, AZ-M, MS-S, JH-S, and VS: visualization. All authors have read and agreed to the published version of the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Puszko B, Sánchez S, Vilas N, Pérez M, Barretto L, López L. El impacto de la educación alimentaria nutricional en el embarazo: una revisión de las experiencias de intervención. Rev Chil Nutr. (2017) 44:79–88. doi: 10.4067/S0717-75182017000100011
2. Cereceda Bujaico MP, Quintana Salinas MR. Consideraciones para una adecuada alimentación durante el embarazo. Rev Per Gin Obs. (2014) 60:153–60.
3. Weight gain during pregnancy.Centers for Disease Control and Prevention: Reproductive Health 2000. (2021). Available online at: https://www.cdc.gov/reproductivehealth/maternalinfanthealth/pregnancy-weight-gain.htm#recommendations (Accessed March 20, 2021)
4. World Health Organization.The Global Prevalence Of Anaemia in 2011. Geneva: World Health Organization (2015).
5. García Odio A, Izaguirre Mayor DR, Álvarez Bolivar D. Impacto de la anemia para una embarazada e importancia del riesgo preconcepcional. Rev Cuba Med Gen Integral. (2017) 33:146–53.
6. Trichopoulou A, Martínez-González MA, Tong TY, Forouhi NG, Khandelwal S, Prabhakaran D, et al. Definitions and potential health benefits of the mediterranean diet: views from experts around the world. BMC Med. (2014) 12:112. doi: 10.1186/1741-7015-12-112
7. Predimed.Prevención Con Dieta Mediterránea. (2021). Available online at: http://www.predimed.es/ (Accessed March 20, 2021)
8. Trichopoulou A, Orfanos P, Norat T, Bueno-de-Mesquita B, Ocké MC, Peeters PH, et al. Modified Mediterranean diet and survival: EPIC-elderly prospective cohort study. BMJ. (2005) 330:991. doi: 10.1136/bmj.38415.644155.8F
9. Mente A, de Koning L, Shannon HS, Anand SS. A systematic review of the evidence supporting a causal link between dietary factors and coronary heart disease. Arch Intern Med. (2009) 169:659–69. doi: 10.1001/archinternmed.2009.38
10. Estruch R, Ros E, Salas-Salvadó J, Covas M, Corella D, Arós F, et al. Primary prevention of cardiovascular disease with a mediterranean diet. N Engl J Med. (2013) 368:1279–90. doi: 10.1056/NEJMoa1200303
11. Misirli G, Benetou V, Lagiou P, Bamia C, Trichopoulos D, Trichopoulou A. Relation of the traditional mediterranean diet to cerebrovascular disease in a mediterranean population. Am J Epidemiol. (2012) 176:1185–92. doi: 10.1093/aje/kws205
12. Benetou V, Trichopoulou A, Orfanos P, Naska A, Lagiou P, Boffetta P, et al. Conformity to traditional mediterranean diet and cancer incidence: the Greek EPIC cohort. Br J Cancer. (2008) 99:191–5. doi: 10.1038/sj.bjc.6604418
13. Couto E, Boffetta P, Lagiou P, Ferrari P, Buckland G, Overvad K, et al. Mediterranean dietary pattern and cancer risk in the EPIC cohort. Br J Cancer. (2011) 104:1493–9. doi: 10.1038/bjc.2011.106
14. Trichopoulou A, Bamia C, Lagiou P, Trichopoulos D. Conformity to traditional mediterranean diet and breast cancer risk in the Greek EPIC (European Prospective Investigation into Cancer and Nutrition) cohort. Am J Clin Nutr. (2010) 92:620–5. doi: 10.3945/ajcn.2010.29619
15. Bamia C, Lagiou P, Buckland G, Grioni S, Agnoli C, Taylor AJ, et al. Mediterranean diet and colorectal cancer risk: results from a European cohort. Eur J Epidemiol. (2013) 28:317–28. doi: 10.1007/s10654-013-9795-x
16. Rossi M, Turati F, Lagiou P, Trichopoulos D, Augustin LS, La Vecchia C, et al. Mediterranean diet and glycaemic load in relation to incidence of type 2 diabetes: results from the Greek cohort of the population-based European prospective investigation into cancer and nutrition (EPIC). Diabetologia. (2013) 56:2405–13. doi: 10.1007/s00125-013-3013-y
17. Benetou V, Orfanos P, Pettersson-Kymmer U, Bergström U, Svensson O, Johansson I, et al. Mediterranean diet and incidence of hip fractures in a European cohort. Osteoporosis Int. (2013) 24:1587–98. doi: 10.1007/s00198-012-2187-3
18. Assaf-Balut C, García de la Torre N, Fuentes M, Durán A, Bordiú E, Del Valle L, et al. A high adherence to six food targets of the mediterranean diet in the late first trimester is associated with a reduction in the risk of materno-foetal outcomes: the St. Carlos gestational diabetes mellitus prevention study. Nutrients. (2019) 11:66. doi: 10.3390/nu11010066
19. Flor-Alemany M, Nestares T, Alemany-Arrebola I, Marín-Jiménez N, Borges-Cosic M, Aparicio VA. Influence of dietary habits and mediterranean diet adherence on sleep quality during pregnancy. The GESTAFIT Project. Nutrients. (2020) 12:3569. doi: 10.3390/nu12113569
20. Silva-del Valle MA, Sánchez-Villegas A, Serra-Majem L. Association between the adherence to the mediterranean diet and overweight and obesity in pregnant women in Gran Canaria. Nutr Hosp. (2013) 28:654–9. doi: 10.3305/nh.2013.28.3.6377
21. Chatzi L, Rifas-Shiman SL, Georgiou V, Joung KE, Koinaki S, Chalkiadaki G, et al. Adherence to the mediterranean diet during pregnancy and offspring adiposity and cardiometabolic traits in childhood. Pediatr Obes. (2017) 12:47–56. doi: 10.1111/ijpo.12191
22. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. Updating guidance for reporting systematic reviews: development of the PRISMA 2020 statement. J Clin Epidemiol. (2021) 34:103–12. doi: 10.1016/j.jclinepi.2021.02.003
23. Higgins JP, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, et al. The cochrane collaboration’s tool for assessing risk of bias in randomised trials. BMJ. (2011) 343:d5928. doi: 10.1136/bmj.d5928
24. Downes MJ, Brennan ML, Williams HC. Dean, RS. development of a critical appraisal tool to assess the quality of cross-sectional studies (AXIS). BMJ Open. (2016) 6:e011458. doi: 10.1136/bmjopen-2016-011458
25. Sherrington C, Herbert RD, Maher CG, Moseley AM. PEDro. A database of randomized trials and systematic reviews in physiotherapy. Man Ther. (2000) 5:223–6. doi: 10.1054/math.2000.0372
26. Wells G, Shea B, O’ Connell D, Peterson J, Welch V, Losos M, et al. The Newcastle-Ottawa Scale (NOS) for Assessing The Quality Of Nonrandomised Studies In Meta-Analyses (2013). Available online at: http://www.ohri.ca/programs/clinical_epidemiology/oxford.htm (accessed October 19, 2009)
28. Olmedo-Requena R, Gómez-Fernández J, Amezcua-Prieto C, Mozas-Moreno J, Khan KS, Jiménez-Moleón JJ. Pre-pregnancy adherence to the mediterranean diet and gestational diabetes mellitus: a case-control study. Nutrients. (2019) 11:1003. doi: 10.3390/nu11051003
29. Assaf-Balut C, García de la Torre N, Durán A, Fuentes M, Bordiú E, Del Valle L, et al. A Mediterranean diet with additional extra virgin olive oil and pistachios reduces the incidence of gestational diabetes mellitus (GDM): a randomized controlled trial: The St. Carlos GDM prevention study. PLoS One. (2017) 12:e0185873. doi: 10.1371/journal.pone.0185873
30. Martínez-Galiano JM, Olmedo-Requena R, Barrios-Rodríguez R, Amezcua-Prieto C, Bueno-Cavanillas A, Salcedo-Bellido I, et al. Effect of adherence to a mediterranean diet and olive oil intake during pregnancy on risk of small for gestational age infants. Nutrients. (2018) 10:1234. doi: 10.3390/nu10091234
31. Melero V, Assaf-Balut C, Torre NG, Jiménez I, Bordiú E, Valle LD, et al. Benefits of adhering to a mediterranean diet supplemented with extra virgin olive oil and pistachios in pregnancy on the health of offspring at 2 years of age. results of the San Carlos gestational diabetes mellitus prevention study. J Clin Med. (2020) 9:1454. doi: 10.3390/jcm9051454
32. Cánovas-Conesa A, Gomariz-Peñalver V, Sánchez-Sauco MF, Vega DJ, Ortega-García JA, García MA, et al. Asociación de la adherencia a la dieta mediterránea al inicio del embarazo y riesgo de gastrosquisis en la descendencia: un estudio de casos-controles. Cir Pediatr. (2013) 26:37.
33. Steenweg-de Graaff J, Tiemeier H, Steegers-Theunissen RP, Hofman A, Jaddoe VW, Verhulst FC, et al. Maternal dietary patterns during pregnancy and child internalising and externalising problems. the generation R study. Clin Nutr. (2014) 33:115–21. doi: 10.1016/j.clnu.2013.03.002
34. Parisi F, Rousian M, Huijgen NA, Koning AH, Willemsen SP, de Vries JH, et al. Periconceptional maternal ‘high fish and olive oil, low meat’ dietary pattern is associated with increased embryonic growth: the rotterdam periconceptional cohort (Predict) study. Ultrasound Obstet Gynecol. (2017) 50:709–16. doi: 10.1002/uog.17408
35. Al-Wattar B, dds J, Placzek A, Beresford L, Spyreli E, Moore A, et al. Mediterranean-style diet in pregnant women with metabolic risk factors (ESTEEM): a pragmatic multicentre randomised trial. PLoS Med. (2019) 16:e1002857. doi: 10.1371/journal.pmed.1002857
36. Saunders L, Guldner L, Costet N, Kadhel P, Rouget F, Monfort C, et al. Effect of a Mediterranean diet during pregnancy on fetal growth and preterm delivery: results from a French caribbean mother–child cohort study (TIMOUN). Paediatr Perinat Epidemiol. (2014) 28:235–44. doi: 10.1111/ppe.12113
37. Tobias DK, Zhang C, Chavarro J, Bowers K, Rich-Edwards J, Rosner B, et al. Prepregnancy adherence to dietary patterns and lower risk of gestational diabetes mellitus. Am J Clin Nutr. (2012) 96:289–95. doi: 10.3945/ajcn.111.028266
38. Hernández-Alonso P, Salas-Salvadó J, Baldrich-Mora M, Juanola-Falgarona M, Bulló M. Beneficial Effect of Pistachio Consumption on Glucose Metabolism, Insulin Resistance, Inflammation, and Related Metabolic Risk Markers: A Randomized Clinical Trial. Diabetes Care. (2014) 37:3098–105. doi: 10.2337/dc14-1431.
39. Hernández-Alonso P, Bulló M, Salas-Salvadó J. Pistachios for health: what do we know about this multifaceted nut? Nutr Today. (2016) 51:133–8. doi: 10.1097/NT.0000000000000160
40. Biagi C, Nunzio MD, Bordoni A, Gori D, Lanari M. Effect of adherence to mediterranean diet during pregnancy on children’s health: a systematic review. Nutrients. (2019) 11:997. doi: 10.3390/nu11050997
41. Amati F, Hassounah S, Swaka A. The impact of mediterranean dietary patterns during pregnancy on maternal and offspring health. Nutrients. (2019) 11:1098. doi: 10.3390/nu11051098
42. Hassani Zadeh S, Boffetta P, Hosseinzadeh M. Dietary patterns and risk of gestational diabetes mellitus: a systematic review and meta-analysis of cohort studies. Clin Nutr ESPEN. (2020) 36:1–9. doi: 10.1016/j.clnesp
43. Mahajan A, Donovan LE, Vallee R, Yamamoto JM. Evidenced-based nutrition for gestational diabetes mellitus. Curr Diab Rep. (2019) 19:94–94. doi: 10.1007/s11892-019-1208-4
44. Li M, Grewal J, Hinkle SN, Yisahak SF, Grobman WA, Newman RB, et al. Healthy dietary patterns and common pregnancy complications: a prospective and longitudinal study. Am J Clin Nutr. (2021) 114:1229–37. doi: 10.1093/ajcn/nqab145
Keywords: Mediterranean diet, pregnancy, adherence, benefits, offspring
Citation: Zaragoza-Martí A, Ruiz-Ródenas N, Herranz-Chofre I, Sánchez-SanSegundo M, Serrano Delgado VdlC and Hurtado-Sánchez JA (2022) Adherence to the Mediterranean Diet in Pregnancy and Its Benefits on Maternal-Fetal Health: A Systematic Review of the Literature. Front. Nutr. 9:813942. doi: 10.3389/fnut.2022.813942
Received: 12 November 2021; Accepted: 08 March 2022;
Published: 31 March 2022.
Edited by:
Raquel Aparicio-Ugarriza, Polytechnic University of Madrid, SpainReviewed by:
Stefania Triunfo, University of Milan, ItalyCopyright © 2022 Zaragoza-Martí, Ruiz-Ródenas, Herranz-Chofre, Sánchez-SanSegundo, Serrano Delgado and Hurtado-Sánchez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Miriam Sánchez-SanSegundo, bWlyaWFtLnNhbmNoZXpAdWEuZXM=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.