Corrigendum: Health benefits of probiotics in sport and exercise—Non-existent or a matter of heterogeneity? A systematic review
 Melina Heimer
Melina Heimer Marc Teschler
Marc Teschler Boris Schmitz
Boris Schmitz Frank C. Mooren
Frank C. Mooren- 1Department of Rehabilitation Sciences, Faculty of Health, University of Witten/Herdecke, Witten, Germany
- 2DRV Clinic Königsfeld, Center for Medical Rehabilitation, Ennepetal, Germany
Background: The use of probiotics in sports has been growing in recent years, as up to 50% of athletes suffer from training- and performance-limiting gastrointestinal (GI) problems. Moreover, repeated exhaustive exercise and high training loads may lead to a transiently depressed immune function, associated with an increased risk of upper respiratory tract infection (URTI).
Aim: To provide a qualitative analysis of probiotic effects on URTI, GI symptoms and the immune system in healthy individuals under consideration of performance level as main classifier.
Methods: A systematic review of the literature was conducted (PubMed, SPORTDiscus with Full Text, Web of Science) to analyze the effects of probiotics in athletes and healthy active individuals on GI problems, URTI, and the immune system. A qualitative synthesis with performance level and treatment duration as main classifiers was performed.
Results: Of 41 eligible studies, 24 evaluated the effects of probiotic supplements in athletes, 10 in recreationally active individuals and 7 in healthy untrained adults. Large heterogeneity was observed in terms of probiotic strains, mode of delivery, performance level, treatment duration and outcome assessment. Overall, studies provided inconsistent observations.
Conclusion: The effects of probiotics on immune system, URTI, and GI symptoms in athletes, healthy adults and recreationally active individuals remain inconclusive. Based on the analyzed studies and identified parameters, this article provides suggestions to align future research on the effects of probiotics in exercise.
Systematic Review Registration: PROSPERO, identifier: CRD42021245840.
Introduction
The microbiota (i.e., the communities of commensal, symbiotic and pathogenic microorganisms) is mainly affected by dietary composition and has a significant impact on health (1). Also referred to as commensals, part of the gut microorganisms exert specific beneficial effects on the body including improved micro- and macronutrient uptake (2), increased intestinal barrier function, intestinal epithelial cell regeneration, modulation of the immune system, and improved mucosal barrier (3). Imbalance of the gut microbiota is associated with gastroenteric disorders, respiratory illness as well as metabolic and cardiovascular diseases (4). The Food and Agriculture Organization of the United Nations/World Health Organization (FAO/WHO) defines probiotics as “live microorganisms which when administered in adequate amounts confer a health benefit on the host” (5) with gut and immune health being the predominant applications (6–8). Notably, the term “probiotic” is frequently used for dietary supplements consisting of preparations that contain a multitude of different viable microorganisms. However, probiotic benefits are strain-specific and some strains are more likely to improve health outcomes than others (9). Microorganisms are effectors of the immune system since their characteristic components [nucleic acids, proteins, lipopolysaccharides (LPS) and metabolites] represent potential antigens and toxins. By contrast, microorganisms exerting probiotic potential target immune and body cells and regulate immune responses in a beneficial way (10). Lately, the specific microbial-derived metabolites, such as short-chain fatty acids (SCFAs), tryptophan, and retinoic acid, have been described to play a central regulatory role in the interaction of the host's immune response (11). Moreover, SCFAs may act to improve gut barrier function (12).
Gut microbiota compositions differ in athletes compared to sedentary individuals, as the human gut may be influenced by physical activity levels as well as training intensity and competition level (12). In addition, athlete's diet usually differs from the general population in terms of carbohydrate and protein intake, exerting additional effects on gut microbiota (10, 13). Especially endurance athletes may be exposed to extreme physiological conditions that put high stress on the body and affect normal organ function and homeostasis. Consequently, a high prevalence of upper respiratory tract infections (URTI) (14) and gastrointestinal (GI) problems (15) has been documented, the latter being associated with increased permeability of the gastrointestinal epithelial wall and disruption of mucous thickness and higher rates of bacterial translocation (4). Imbalance in gut microbiota may thus limit athlete's training performance, competitiveness, and overall wellbeing also including fatigue (16), depression and anxiety (17). Of note, 30–50% of athletes experience one or more GI symptoms during competitive events (13) including heartburn, indigestion, bloating or constipation. Serious medical conditions such as ischemic bowel, hemorrhagic gastritis, and hematochezia may also occur (14, 15). Reasons for GI symptoms may involve physiological, mechanical, or nutritional effectors, and reduced mesenteric blood flow, since the blood supply to the GI tract decreases by 60 to 70% already at exercise intensities of 70% of maximum oxygen consumption (VO2max) (14–17). By contrast, moderate exercise increases the number of health-promoting bacteria which produce SCFAs, inducing positive physiological effects (18, 19). Another common condition in athletes are URTIs, which account for 35–65% of disease-associated presentations in sports medicine clinics (20). URTI includes infections of the pharynx, sinuses, the middle ear, or the tonsils and is a mainly caused by various viruses such as respiratory viruses, rhinovirus, influenza, and corona virus interacting with the mucosa of the upper airways (21). Further reasons can be bacterial infections, allergic responses, undiagnosed asthma, and exercise-related trauma (20). The high rate of URTI in athletes has been linked to the observation that exhaustive exercise can lead to systemic immunosuppression (22) and oxidative stress (23), including reduced natural killer (NK) cells and T-lymphocytes (9). Even though acute exercise is known to increase the numbers of neutrophils and monocytes, the immune function can be reduced during recovery, as part of the physiological stress response to exercise (24), a phenomenon known as the “open window” in which athletes may be prone to infections. Further, the anti-inflammatory cytokines interleukin (IL)-10, IL-1Ra, soluble tumor necrosis factor receptor (sTNFR) and inflammation-responsive cytokine IL-6 increase by exhaustive exercise (9). More recently, changes in the gut microbial composition have been linked to local alterations in immune response and development in the respiratory tract (25) in that the lungs production of type-I interferons (IFNs), which prevent virus infections, may be increased (26, 27).
As probiotics have been reported to affect the immune system by inhibition of NK cell activity (28) induction of anti-inflammatory IL-10 (29) and IFN-γ secretion as well as salivary cortisol and gut immunoglobulin (IgA) levels (30) in addition to T and B cell activation (28), they may induce beneficial effects on URTI incidence and severity. In addition, probiotic-induced fermentation of fibers increases the production of SCFAs and may thus strengthen the gut barrier function with beneficial effects on GI problems during endurance exercise. With regard to the potentially improved resistance to illness and immunomodulative effects of probiotics, several studies have investigated probiotic effects in athletes. However, the effectiveness of probiotics in physical exercise on the immune system, URTI and GI problems is still a matter of debate.
Objective
Based on the hypothesis that probiotics may exert differential effects in athletes compared to recreationally active individuals, the aim of this systematic review was to provide a structed summary using a qualitative analysis of studies investigating the effects of probiotics on URTI, GI symptoms and the immune system in healthy individuals under consideration of performance level as main classifier. We propose that this approach would be effective to reveal the specific beneficial potential of probiotics in sport and exercise.
Methods
Study Design and Participants Eligibility Criteria
We performed a systematic review (PROSPERO, CRD42021245840) in accordance with the PRISMA guidelines and following the suggestions for reporting on qualitative summaries (31, 32). Any original article reporting on probiotics in physical exercise was considered for the analysis. Included studies had to report on URTI, GI (as defined by authors; symptoms/severity and duration) or markers of the immune system including IL-6, IL-8, IL-10, granulocyte macrophage-colony stimulating factor (GM-CSF), IFN-γ, TNF-α, and IL-1Ra, serum concentrations of tryptophan, phenylalanine, kynurenine, tyrosine, neopterin, C-reactive protein (CRP), protein carbonyl content (PCC), malondialdehyde (MDA) and total oxidation status of lipids (TOS). Only articles available as full-text (after an attempt to contact the corresponding author) reporting on healthy humans aged 14–65 years were included. This was done since different effects of probiotics and physical activity on the included outcome variables may be observed in children. Articles were not eligible if they (1) reported on probiotic use in patients or animals, (2) did not investigate effects of probiotics only/ included additional interventions, and (3) were not original research [a review or book (chapter)]. Articles were excluded if they (1) focused on performance only, (2) were not written in English (full text), (3) were gray literature or website articles, and (4) did not clearly report on included subjects, interventions, outcome measures and statistical analysis. The combined used of probiotics, prebiotics and synbiotics was not an exclusion criterium. The eligibility criteria were selected also in accordance with the quality assessment (see below).
Search Strategy and Data Sources
Electronic searches were performed based on the PICO criteria. Studies in athletes, recreationally active individuals and healthy adults in risk of URTI, GI and transiently depressed immune function [P] in which probiotic foods or supplements [I] were compared to controls not receiving probiotics [C] for establishment of significant effects on URTI, GI or markers of the immune system [O] were included. A systematic search of the literature was conducted (MH) using PubMed, SPORTDiscus with Full Text, and Web of Science for records published until March 2021. Databases were searched using variations and combination of the following keywords: “probiotic,” “exercise,” “gut microbiota,” “respiratory tract infection,” “immune system,” “sport,” “immunology,” “athlete,” “physical activity,” “recreational,” “gastrointestinal disease,” “URTI,” “inflammation.” Additional filters were used if applicable. The search syntax used for the individual data bases is presented in Supplementary Table 1. Manual searches were also performed using reference lists from identified articles and available reviews. The individual steps of report identification, screening and processing are documented in the PRISMA flow chart (Figure 1) (33). Search results and fulfillment of eligibility criteria were discussed if unclear (MH and BS) until consensus was achieved and upon disagreement, a third person was consulted to determine inclusion.
FIGURE 1
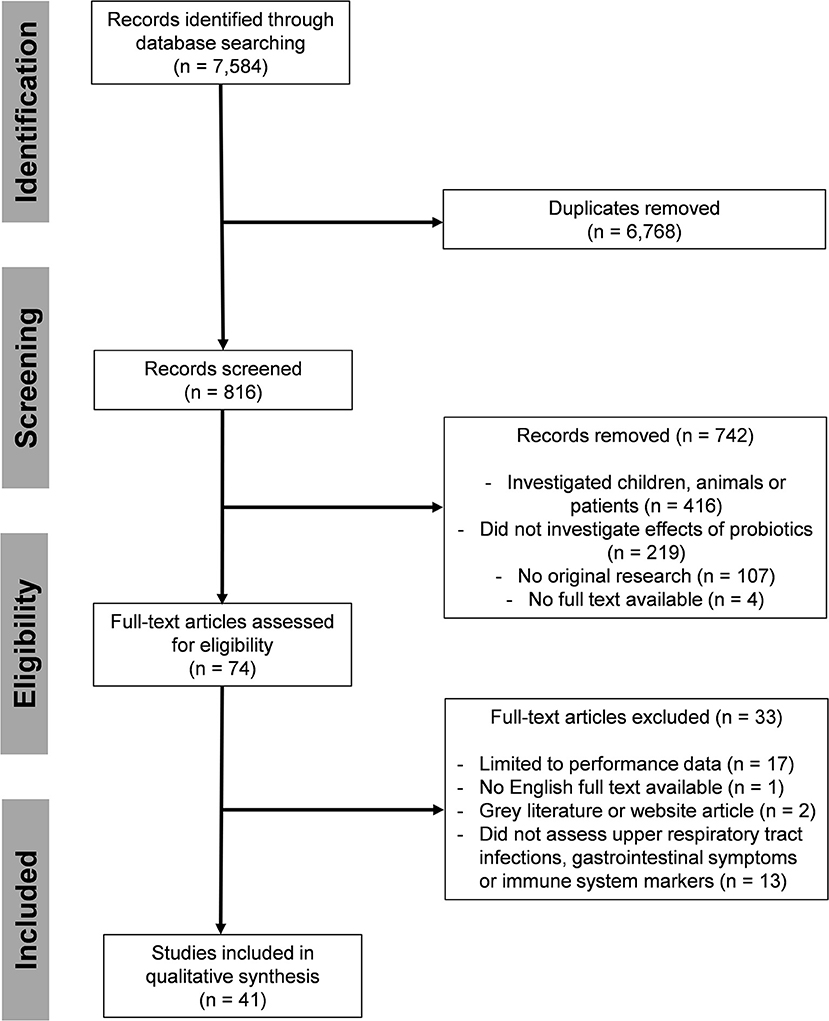
Figure 1. PRISMA flow chart.
Study Selection and Data Extraction
Data were extracted by two reviewers (MH and BS) and tables were created including information on first author, year of publication, probiotic type, strain, dose, and mode of delivery, participants (total number, sex), study type, main outcome, influence on URTI, GI and immune system defined as significant increase, decrease or insignificant effect, type of data assessment, type of sport/ exercise, contextual/ setting factors (acute/ chronic testing), and additional observation.
Grouping of Studies and Synthesis
To provide a structured qualitative summary, studies were grouped by main categories treatment duration and activity/ performance level including (1) professional/ amateur athletes, (2) recreationally active adults, and (3) previously sedentary (healthy) adults. Heterogeneity was investigated using ordering tables including URTI, GI or immune system as main outcome and the above-mentioned categories. Certainty of the evidence was addressed using an evaluation of how directly the included studies addressed the planned question/ applied methodology (measurement validity), the number of studies and participants and the consistency of effects across studies.
Definitions
Individuals were classified as athletes (professional level and non-professional amateurs), recreationally active individuals and healthy adults (previously sedentary), based on the author's descriptions. URTI and GI symptom definitions were accepted as defined by authors. In case of imprecise, uncommon, unclear/ conflicting, or missing descriptions of test participants, full texts were screened by two reviewers (MH and BS) for additional information including club or union associations, training patterns or other information.
Quality Assessment
The methodological quality of the studies was assessed using the 11-item PEDro scale based on the Delphi list developed by Verhagen and colleagues (34). The individual items can be scored as “yes” or “no.” For our analysis, we determined (in accordance with the above mentioned inclusion criteria) that the following items (6 out of 11) had to be scored “yes”: eligibility criteria were specified; the groups were similar at baseline regarding the most important prognostic indicators (in case of non-randomized controlled trial (RCT) study design this item was not applicable); measures of at least one key outcome were obtained from more than 85% of the subjects initially allocated to groups/intervention; all subjects for whom outcome measures were available received the treatment (or control condition) as allocated or, where this was not the case, data for at least one key outcome was analyzed by “intention to treat;” the results of (between-group) statistical comparisons were reported for at least one key outcome; the study provided both point measures and measures of variability for at least one key outcome. Studies were rated by two reviewers (MH and BS). Disagreements were resolved by discussion if necessary. The researchers were not blinded to study authors, results, or publication journal.
Results
A total of 41 articles met the eligibility criteria, involving 2,189 participants. Twenty-four studies evaluated the effects of probiotic supplements in athletes, 10 studies in recreationally active individuals and 7 studies in healthy untrained adults. Included studies had an average score of 9/10 on the PEDro scale indicating low to moderate risk of bias (Supplementary Table 2). Thirty-one studies were conducted as RCT, 7 had a crossover design and three were longitudinal studies with pre-post analysis. Sixteen studies investigated the effects on URTI (8 found significant positive effects), 16 on GI symptoms (5 found significant positive effects) and 31 on the immune system (14 found significant positive effects). An analysis of the intervention period revealed a mean intervention time of ~8 weeks and a maximal intervention time of 21 weeks. Thus, studies were categorized by intervention time <5 weeks (18 studies), 5–12 weeks (14 studies) and >12 weeks (9 studies).
In athletes, 50% of the studies found significant positive effects on URTI, 27% on GI problems, and 50% on the immune system (Figure 2). In recreationally active individuals, 50% of the studies reported significant positive effects on URTI, 33% on GI problems, and 63% on the immune system. In healthy adults, 50% of the studies detected significant positive effects on URTI and 50% on GI problems, while no study out of five in healthy adults reported significant positive effects on the immune system (Figure 2).
FIGURE 2
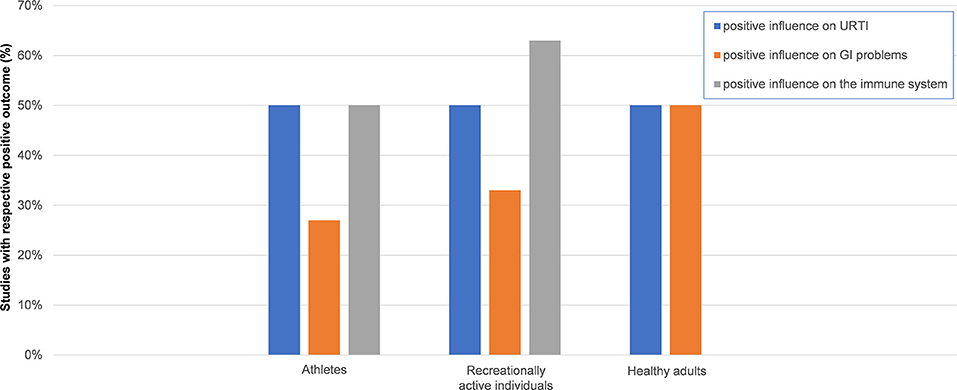
Figure 2. Effect of probiotic supplementation on URTI, GI problems and the immune system by performance level. Columns illustrate the ratio of studies reporting positive effects on upper respiratory tract infections (URTI), gastrointestinal (GI) problems and the immune system. Results were based on the following number of studies. URTI in athletes, 5/10 studies; GI problems in athletes, 3/11 studies; immune system in athletes, 9/18 studies; URTI in recreationally active individuals, 2/4 studies; GI problems in recreationally active individuals, 1/3 studies; immune system in recreationally active individuals, 5/8 studies; URTI in healthy adults, 1/2 studies; GI problems in healthy adults, 1/2 studies; immune system in healthy adults, 0/5 studies. No influence was defined as non-significant change in outcome variables of URTI, GI problems or the immune system. GI problems were defined as incidence of symptoms and severity of nausea, vomiting, diarrhea, abdominal pain, abdominal bloating, flatulence, stomach “rumbles,” loss of appetite, and markers for GI barrier function (e.g., zonulin); URTI was defined as symptoms and severity of throat soreness, sneezing, fever, ear pain, blocked or runny nose, cough, duration, number of episodes based on author's descriptions.
In terms of probiotics applied, different combinations of Lactobacilli and/ or Bifidobacteria in form of single or multi strains, sometimes combined with S. thermophilus or E. faecium were used (Table 1). Seventeen studies used Lactobacillus strains (10 detected positive effects), 4 studies used Bifidobacterium (one found positive effects), and 20 studies used a combination with or without excipients (12 reported significant positive effects) (Figure 3). Twenty-four studies used single strain probiotics (12 detected positive effects) and 17 used multi strain probiotics (11 reported positive effects). In addition, different modes of delivery were applied. Sixteen studies provided (enterically-coated) capsules and 25 used a different mode of delivery without protection from dissolution or disintegration in the gastric environment (mainly solutions in water/ milk or yogurt). Of these, 9 (56%) and 12 (48%) reported positive effects, respectively (Table 2).
TABLE 1
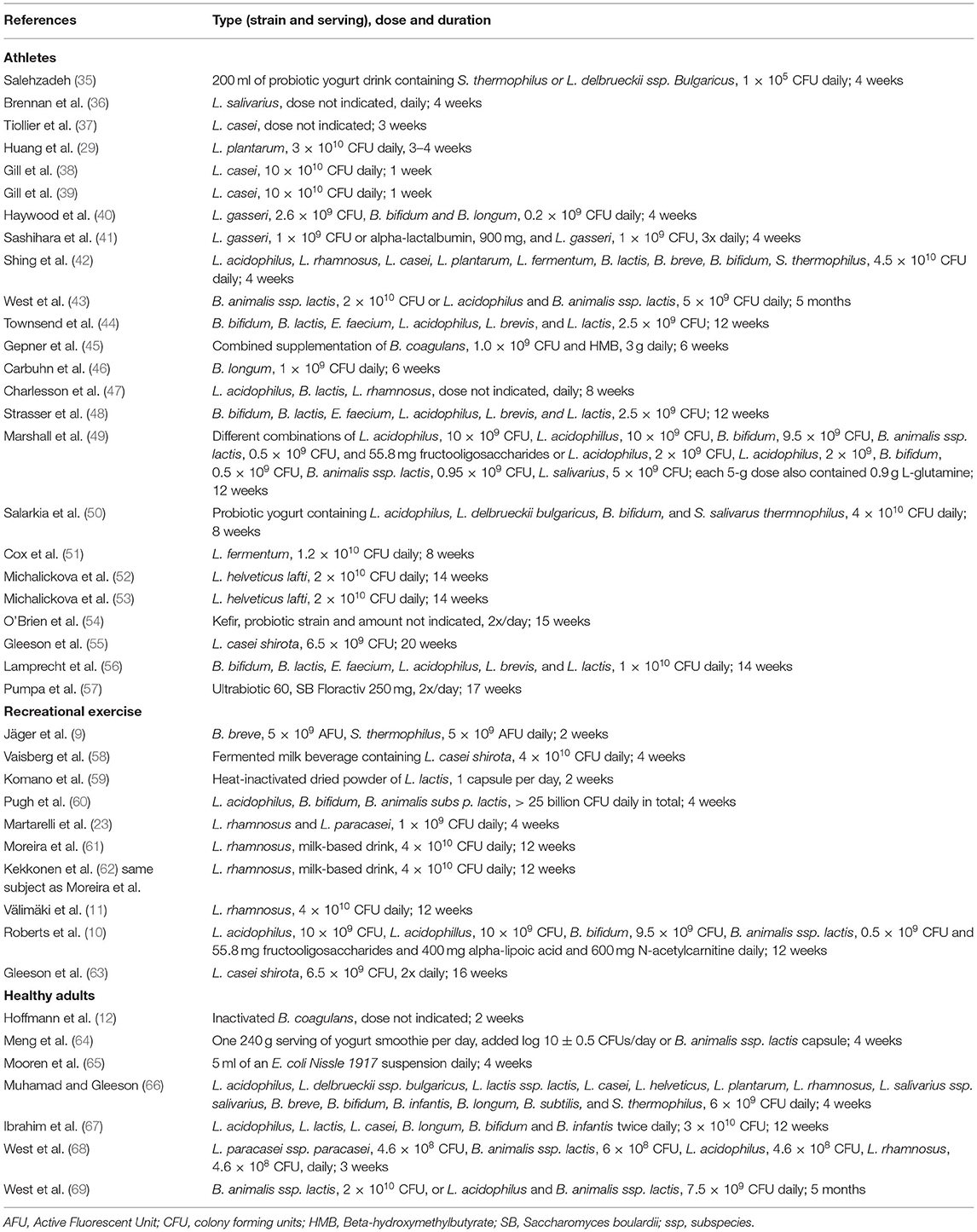
Table 1. Type, dose, and duration of probiotic use of included studies.
FIGURE 3
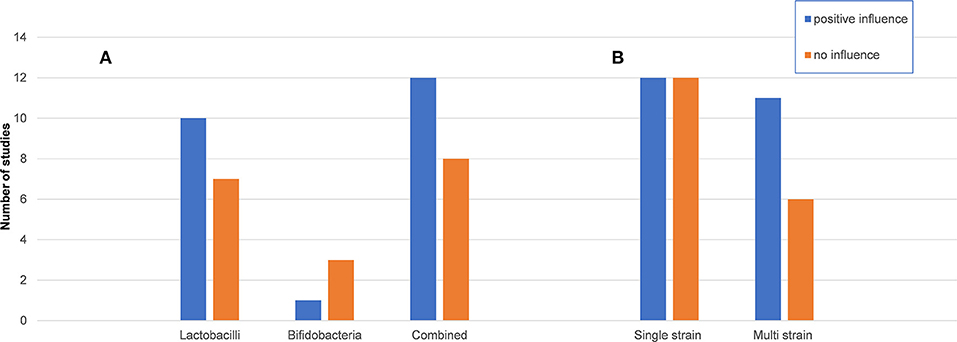
Figure 3. Effect of probiotic supplementation on URTI, GI problems and the immune system by probiotic strain. Columns illustrate the number of studies reporting positive effects on upper respiratory tract infections (URTI), gastrointestinal (GI) problems or the immune system for the different probiotic (A) genera and their combination and (B) single or multi strain preparations. Lactobacilli, preparations only including Lactobacillus strains; Bifidobacteria, preparations only including Bifidobacterium strains; combined, including different Lactobacillus and Bifidobacteria strains with or without different other genera; single strain, only one strain of Lactobacillus or Bifidobacteria was given; multi strains, any combination of different Lactobacillus and/ or Bifidobacteria was given. Positive influence was defined as any significant positive effect on URTI, GI and the immune system based on author's descriptions.
TABLE 2

Table 2. Effects of probiotics by performance level and duration of intervention.
Probiotic Supplementation in Athletes
Sixty percent of the identified studies (24 of 41 studies) investigated the impact of probiotics on URTI (10 studies), GI symptoms (10 studies), and/or immune system (18 studies) in athletes. Outcomes were evaluated after supplementation for <5 weeks (N = 9), 5–12 weeks (N = 8) and > 12 weeks (N = 7). Five studies found significant positive effects of probiotics on URTI, 3 on GI symptoms and 10 on the immune system and inflammatory response.
Effects on URTI
As URTI are common in athletes, 10 studies investigated the effect of probiotic supplementation on URTI with 5 studies reporting significant positive effects (Table 2, Figure 2). All studies documented URTI via self-reported symptoms using questionnaires or daily diaries, recording the number, duration and severity of symptoms including throat soreness, sneezing, fever, ear pain, a blocked or runny nose and cough. One study defined two or more symptoms on at least two consecutive days as an episode of illness (43). No study involved medical diagnosis of URTI. Mucosal immunity was assessed by lactoferrin, lysozyme, secretory immunoglobulin (sIgA) and albumin concentrations.
Studies reporting reduced number, duration, and severity of infections included rugby players (n = 30, multi strain probiotic, 4 weeks) (40) and athletes in general (13 males and 16 females, no type of sport indicated, multi strain probiotics, 12 weeks) (48). A reduction in respiratory and ear infections has been documented in female endurance swimmers (n = 46, multi strain probiotic, 8 weeks) (50). Elite distance runners (n = 20, single strain probiotic, 16 weeks) showed a reduction in respiratory episodes and severity (51). A reduction in URTI duration and symptoms but not in severity and incidence was recorded in elite athletes involved in different sports (n = 39, single strain probiotic, 14 weeks) (53).
No effects were observed in endurance runners (n = 8, single strain probiotic, 7 days) (38), in commando cadets (n = 47, single strain probiotic, 3 weeks) (37), in university athletes and game players (n = 243, single strain probiotic, 20 weeks) (55) and elite rugby union athletes (n = 19, multi strain probiotic, 17 weeks) (57). One study reported sex-dependent differences in that no reduction of URTI has been found in female (n = 35) compared to male (n = 64) competitive cyclists (single strain probiotic, 11 weeks) (43).
Effects on GI Symptoms
Ten studies investigated the effects of probiotic supplementation on GI symptoms in athletes, 3 of which found significant positive effects. GI illness was measured by self-reported symptoms including nausea, vomiting, diarrhea, abdominal pain, abdominal bloating, flatulence, stomach “rumbles” and loss of appetite using scores for severity. Only one study (60) used the structured Gastrointestinal Symptom Rating Scale (70). Some studies involved fecal microbiology to determine abundance of Bacteroides, short chain fatty acids (SCFA) concentrations, α1-antitrypsin and zonulin levels (marker of GI barrier integrity/ intestinal permeability). One study (36) assessed GI permeability as sugar recovered in urine. Another study (47) used a daily log to record symptoms of diarrhea, classified using the World Health Organization (WHO) definition of ≥ 3 loose or watery stools in a 24-h period.
Significant changes in 60 bacterial species, an increased microbial diversity and an attenuated exercise-induced intestinal hyperpermeability indicated by urine sucrose concentration were found in endurance athletes (n = 7, single strain probiotics, 4 weeks) (36). Reduced episodes of GI illness were reported in rugby players (n = 30, multi strain probiotic, 4 weeks) (40). In a study involving 23 endurance-trained men (triathletes, runners, and cyclists; multi strain probiotic, 14 weeks) serum zonulin levels were decreased (56).
No effects on gut inflammation markers were found in division one collegiate female swimmers (n = 17, single strain probiotic, 6 weeks) (46). No effect on GI was observed in athletes (n = 33, multi strain probiotic, 12 weeks) (48), runners in the heat (n = 10, multi strain probiotic, 4 weeks) (42), division one baseball players (n = 25, single strain probiotic, 12 weeks) (44), athletes (no type of sport specified, n = 8, multi strain probiotic, 8 weeks) (47), elite rugby union athletes (n = 19, multi strain probiotic, 17 weeks) (57) and female endurance swimmers (n = 46, multi strain probiotic, 8 weeks) (50). Interestingly, number and duration of GI symptoms increased in 64 male competitive cyclists supplemented with probiotics (single strain, 11 weeks), which was interpreted as a response of the GI tract to alteration in the composition of microflora (43).
Effects on the Immune System
Eighteen studies investigated effects on the immune system and inflammatory response, 10 of which found significant positive effects. Frequently assessed markers included anti- and pro-inflammatory cytokines (IL-6, IL-8, IL-10, GM-CSF, IFN-γ, TNF-α, and IL-1RA), serum concentrations of tryptophan, phenylalanine, kynurenine, tyrosine, neopterin (immune activation marker), CRP and PCC, as well as MDA and TOS.
Positive effects were reported in endurance athletes (n = 30, single strain probiotic, 4 weeks) in terms of reduced CRP and increased high-density lipoprotein levels (35). In triathletes (n = 34, single strain probiotic, 3–4 weeks) reduced post-race inflammatory cytokine levels (TNF-α, IL-6, IL-8) and oxidative stress (thioredoxin and myeloperoxidase indices), reduction in the extend of muscle injury (creatine kinase level), and increased IL-10 and amino acid levels were reported (29). Athletes from a university football club (n = 44, multi strain probiotic, 4 weeks), showed no reduction in NK cell activity (41). In division one baseball players (n = 25, single strain probiotic, 12 weeks), reduced TNF-α levels were reported (44). In elite athletes from several different sports (n = 39, single strain probiotic, 14 weeks) increased self-rated sense of vigor and improved CD4+/CD8+ ratio (ratio of T helper cells) was demonstrated (53). In runners (n = 65, single strain probiotic, 15 weeks) an attenuated increase in serum CRP was found (54). University athletes and game players (n = 243, single strain probiotic, 20 weeks) showed a reduced cytomegalovirus and Epstein-Barr virus load (55). In soldiers of an elite combat unit (n = 26, single strain probiotic, 6 weeks), IL-6 but also IL-10 levels were attenuated (45). Elite distance runners (n = 20, single strain probiotic, 16 weeks) showed increased IFN-γ levels but no significant differences in salivary IgA/ IgA1 and serum IL-4 and IL-12 levels (51). Elite rugby union athletes (n = 19, multi strain probiotic, 17 weeks) showed increased salivary alpha-amylase (host defense peptide) levels (57).
No effects of probiotics on markers of the immune system were found in division one collegiate female swimmers (n = 17, single strain probiotic, 6 weeks) (46), elite athletes (badminton, triathlon, bicycling, athletics, karate, kayaking, and judo, n = 30, single strain probiotic, 14 weeks) (52), commando cadets (n = 47, single strain probiotic, 3 weeks) (37), runners in the heat (n = 8, single strain probiotic, 1 week; n = 10, multi strain probiotic, 4 weeks) (38, 42), ultra-marathon runners (n = 32, multi strain probiotic, 12 weeks) (49), endurance runners in the heat (n = 8, single strain probiotic, 1 week) (39) and endurance-trained men (triathletes, runners, and cyclists, n = 23, multi strain probiotics, 14 weeks) (56). However, a tendency for supplementation over a period longer than 12 weeks in athletes may potentially produce stronger effects on the immune system compared to shorter intervention times.
Probiotic Supplementation in Recreational Exercise
Ten of the included studies investigated the effects of probiotics on URTI (4 studies), GI symptoms (3 studies), and/or immune system (8 studies) in recreationally active individuals. Outcomes have been evaluated after supplementation for <5 weeks (N = 5), 5–12 weeks (N = 4) and >12 weeks (N = 1). Two studies found significant positive effects of probiotics on URTI, one on GI symptoms and 5 on the immune system and inflammatory response (Figure 2).
Effects on URTI
Four of the 10 studies investigated the effects of probiotic supplementation on URTI, two of which showed significant positive effects (Table 2). In students at a university sports club (n = 51, single strain probiotic, 13 days), significant lower days of URTI were reported (59). Participants involved in endurance activities (n = 84, single strain probiotic, 16 weeks) reported a significant reduction of URTI episodes (63). No effects were reported in amateur marathon runners (n = 42, single strain probiotic, 4 weeks) (58) and in individuals training for a marathon (n = 141, single strain probiotic, 12 weeks) (62).
Effects on GI Symptoms
Three of 10 studies investigated the effect of probiotic supplementation on GI markers and symptoms, one of which showed significant positive effects. Recreational marathon runners (n = 24, multi strain probiotic, 4 weeks) reported lower incidence and severity of GI symptoms (60). No effects were reported in individuals training for a marathon (n = 141, single strain probiotic, 12 weeks) (62) and recreational triathletes (n = 30, multi strain probiotic, 12 weeks) (10).
Effects on the Immune System
Eight of 10 studies investigated the effect of probiotic supplementation on the immune system, 5 of which showed significant positive effects. Supplementing amateur marathon runners (n = 42, single strain probiotic, 4 weeks) improved airway and systemic immune system/inflammatory response in that IL-10 levels were increased, TNF-α levels were decreased, and lower neutrophil infiltration was found post-marathon (58). Amateur cyclists (n = 42, multi strain probiotic, 4 weeks) showed reduced oxidative stress, as plasma antioxidant levels increased (23). In recreational triathletes (n = 30, multi strain pro/prebiotic/antioxidant, 12 weeks) reduced endotoxin levels were reported (10). In students at a university sports club (n = 51, single strain probiotic, 2 weeks), CD86, a maturation marker on plasmacytoid dendritic cells (pDC), was significantly increased (59). Recreational endurance-trained individuals (n = 84, single strain probiotic, 16 weeks) showed higher saliva IgA concentrations (63).
No effects were seen in recreational resistance-trained men (n = 15, single strain probiotic, 2 weeks) (71), non-elite marathon runners (n = 141, single strain probiotic, 12 weeks) (61), and recreational marathon runners (n = 119, single strain probiotic, 12 weeks) (11).
Probiotic Supplementation in Healthy Humans
Seven of the included studies investigated the effects of probiotics on URTI (2 studies), GI symptoms (3 studies), and/or the immune system (5 studies) in recreationally active individuals. Outcomes were evaluated after supplementation for <5 weeks (N = 4), 5–12 weeks (N = 2) and >12 weeks (N = 1). One study found significant positive effects of probiotics on URTI, one on GI symptoms and none on the immune system and inflammatory response (Figure 2).
Effects on URTI
Two of the 7 studies investigated the effect of probiotic supplementation on URTI markers and symptoms. One showed significant positive effects (Table 2). Supplementing active individuals (n = 465, multi strain probiotic, 5 months) led to a significant reduction of URTI episodes (69). No effects on URTI severity were reported in healthy adults (n = 30, single strain probiotic, 4 weeks) (64).
Effects on GI Symptoms
Three of the 7 studies investigated the effect of probiotic supplementation on GI markers and symptoms with one study reporting significant positive effects. In untrained subjects (n = 19, single strain probiotics, 4 weeks), a lower increase in intestinal fatty acid-binding protein (I-FABP), indicating improved intestinal barrier function, and thiobarbituric acid reactive substances (TBARS), indicating reduced lipid peroxidation was detected after exercise (65).
No significant effects on GI markers or symptoms were found in active individuals (n = 22, multi strain probiotics, 3 weeks) (68). Another study with healthy physically active individuals (n = 465, multi strain probiotic, 5 months), reported an insufficient number of GI illness episodes for analysis (69).
Effects on the Immune System
Five studies investigated the effect of probiotic supplementation on the immune system, none of which showed significant positive effects. No effects were reported in soldiers (n = 16, single strain probiotic, 2 weeks) (12), in healthy adults (n = 30, single strain probiotic, 4 weeks) (64), active students (n = 11, multi strain probiotic, 4 weeks) (66), active individuals (n = 22, multi strain probiotic, 3 weeks) (68) and healthy sedentary young males (n = 48, multi strain probiotic, 12 weeks) (67).
Discussion
The aim of this systematic review was to provide a structured summary of probiotic effects in athletes, recreationally active individuals, and healthy adults on URTI, GI symptoms and the immune system. To account for the potential effects of performance level and training intensity, studies were grouped by activity/ performance level of participants, intervention duration and investigated outcome. Strain type, mode of delivery and study type were also noted as potential effectors. The main findings of our investigation were, that the identified studies differed largely in terms of selected probiotics and probiotic strains, mode of delivery, intervention duration, selected outcome variables and measurement as well as included subjects. In athletes, the type of sport performed added to the observed heterogeneity. Further, our approach revealed that studies provided inconsistent observations without significant differences between the analyzed performance levels.
The analysis of 41 studies in the field revealed that some interventions induced positive effects in terms of URTI and GI symptom reduction, but almost half of the analyzed studies did not detect improvements independent of performance levels. In addition, longer duration of application did not show stronger effects on any analyzed outcome. Considering that protection of probiotics from dissolution or disintegration in the gastric environment may improve efficiency of the treatment (72–74), we also investigated the mode of delivery as potential confounding factor. However, comparison of encapsulated probiotics to probiotic beverages etc. did not reveal differences between the different modes of delivery, as on average only 50% of studies reported positive outcomes. With respect to the combined use of different genera and application of single vs. multi strain probiotics, an overall tendency toward a higher number of studies reporting beneficial effects with multi strain applications was seen. While this could simply be explained by the general assumption that the combination of a diverse selection of microorganisms with different properties would likely induce positive effects in a larger number of different individuals, none of the identified studies directly compared the use of single and multi strain probiotics. Thus, future RCTs should investigate if multi strain probiotics induce significantly greater effects on URTI, GI problems or the immune system in sport and exercise. In addition, the fact that probiotic benefits are strain-specific and some strains are more likely to improve gut or immune health in athletes than others (9), adds largely to the limited comparability between studies and complicates the interpretation of studies administering multi strain probiotics.
Considerable heterogeneity between studies was detected also in terms of the outcome variables used and their methodical assessment. However, even in studies that included identical outcome variables, no distinct effect of probiotics emerged. For example, no effects on S-IgA concentrations were detected after 3 weeks (37) or 4 weeks (51) of probiotic supplementation. Since another study reported increased S-IgA concentration after 16 weeks of probiotic supplementation (63) it could be speculated that a short-term supplementation was ineffective to induce significant effects on S-IgA levels. However, a 14-week probiotic supplementation also did not result in an elevation of S-IgA levels (52).
In terms of URTI, a number of well-designed RCTs that investigated the effects of probiotics in athletes, provided evidence that supplementation may lead to fewer days and reduced severity of URTI (40, 51, 53). These reports are opposed to studies in athletes, which reported no effects on respiratory infection incidence or symptom duration (37–39, 42, 46, 49). Of note, all identified studies which assessed the effects of probiotics on URTI, used self-assessment and self-reporting by diary or unvalidated questionnaires. Self-assessment and self-reporting were also the standard for the assessment of probiotic effects on GI symptoms, potentially contributing to opposing results even in individuals at comparable performance levels. For example, no effect on GI incidence and severity was reported after 6-week probiotic supplementation in elite rugby union players (57), while supplementing runners for 4 weeks prior to a marathon race with probiotics was suggested to reduce resting GI symptoms and severity (60). In addition, the time point (resting vs. post-exercise) or individual characteristics may have affected the observed results. To this respect, it has been speculated that GI symptoms may be more pronounced in runners who are unable to maintain their race pace, which elicits negative emotions potentially affecting the GI system (75).
In general, a significant level of heterogeneity in the field resides in the selection of analyzed subjects and their respective performance and training status. While athletes may be more susceptible to GI problems than healthy moderately-trained or sedentary adults not exposed to intense training conditions, athletes might benefit considerably from the use of probiotics (76). However, our analysis provides evidence that also in athletes, the effects of probiotics on GI symptoms are unclear and the percentage of studies reporting positive effects tended to be identical or even lower compared to individuals at lower performance levels. Of note, studies that involved objective markers of gastrointestinal barrier function such as zonulin and I-FABP did not detect significant effects of probiotics. However, a 4-week probiotic supplementation in healthy individuals was reported to lead to a reduced increase in acute I-FABP and TBARS after exercise, suggesting that results may differ also depending on the time point of assessment (65).
In terms of probiotic supplementation on immune system function, some studies found significant acute effects of probiotics such as reduced acute NK cell activity post-exercise (41) as well as chronic effects including an increase in microbial diversity (36) or reduced resting TNF-α, IL-6 and IL-8 levels (29). Of note, even within study types (RCT vs. longitudinal studies) no consistent effect was observed. In addition, no type of sport or exercise with specific stressors in which probiotics could have been particularly effective was identified, even if studies on endurance-trained athletes or resistance-trained athletes were compared. Of note, out of five studies investigating the effects of probiotics on the immune system in healthy individuals, no study detected significant improvements, indicating that performance level could be a relevant classifier in this aspect.
Limitations
Some limitations for the presented analysis may exist. Reporting and publication bias may have affected the present review since some data/ studies may have remained unreported or were not published because of unexpected/ contradictory, negative or not significant test results. Furthermore, the record search was limited to studies published in English and inclusion of data reported in other languages may have altered the results preliminary in subgroups with smaller sample sizes.
Conclusion and Perspective
While athletes may be more susceptible to GI problems and URTI due to the immunosuppressive effects of repeated intensive exercise (76, 77), recreational exercise does not induce immunosuppressive effects in healthy adults and the beneficial effects of probiotics may thus be less obvious in this group. Since the number of available studies in healthy adults is currently rather limited, this aspect requires further investigation. Currently, due to overall inconsistent observations, the use of probiotics in sport and exercise remains inconclusive. In addition, further studies investigating the effect of probiotics on acute exercise-induced changes of immune function markers are mandatory to identify the potential effects of probiotics in physically active individuals at different performance levels. Moreover, the effects of probiotics in women need further examination, since available studies predominantly included male subjects and one study indicated sex-specific differences, reporting a significant reduction in duration and severity of respiratory illness in males, but not in females (68). In general, the heterogeneity in the documentation of GI illness and URTI incidence, duration, severity, and symptoms by self-reporting adds further uncertainty to the evaluation of potential beneficial probiotic effects. A concerted approach to definition, diagnosis, and documentation, as well as to assessed variables would help to obtain comparable results. This should include the use of validated questionnaires such as the Gastrointestinal Symptom Rating Scale (GSRS) (70) for GI problems and the Wisconsin Upper Respiratory Symptom Survey (WURSS) (78) for URTI. In addition, it might be necessary to include serological diagnosis of URTI instead of using symptomatic monitoring as recently suggested (48). Since a correlation between an increase in the number of respiratory illnesses and a decrease in s-IgA during training has been observed (79), s-IgA may be a useful marker with some potential to investigate the connection of immune system function and URTI. Since GI permeability has been shown to be increased following strenuous exercise also without apparent self-reported GI symptoms (80) serum markers of GI barrier integrity/ intestinal permeability including zonulin should be included in future studies on probiotic supplementation in exercise.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Materials, further inquiries can be directed to the corresponding author.
Author Contributions
MH and FM contributed to the conception and design of the study. MH performed the systematic literature search. MH, BS, and MT screened records and extracted data. MH, FM, and BS interpreted the data. MH and BS wrote the manuscript. All authors contributed to the drafting, revision of the manuscript, and approved the final version of the manuscript.
Funding
FM and BS are supported by the European Commission within the Horizon 2020 framework program (grant number: 101017424).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnut.2022.804046/full#supplementary-material
References
1. David LA, Maurice CF, Carmody RN, Gootenberg DB, Button JE, Wolfe BE, et al. Diet rapidly and reproducibly alters the human gut microbiome. Nature. (2014) 505:559–63. doi: 10.1038/nature12820
2. Yang Q, Liang Q, Balakrishnan B, Belobrajdic DP, Feng QJ, Zhang W. Role of dietary nutrients in the modulation of gut microbiota: a narrative review. Nutrients. (2020) 12:381. doi: 10.3390/nu12020381
3. Mohr AE, Jager R, Carpenter KC, Kerksick CM, Purpura M, Townsend JR, et al. The athletic gut microbiota. J Int Soc Sports Nutr. (2020) 17:24. doi: 10.1186/s12970-020-00353-w
4. McQuade JL, Daniel CR, Helmink BA, Wargo JA. Modulating the microbiome to improve therapeutic response in cancer. Lancet Oncol. (2019) 20:e77–91. doi: 10.1016/S1470-2045(18)30952-5
5. Hill C, Guarner F, Reid G, Gibson GR, Merenstein DJ, Pot B, et al. The International Scientific Association for Probiotics and Prebiotics consensus statement on the scope and appropriate use of the term probiotic. Nat Rev Gastroenterol Hepatol. (2014) 11:506–14. doi: 10.1038/nrgastro.2014.66
6. Gibson GR, Hutkins R, Sanders ME, Prescott SL, Reimer RA, Salminen SJ, et al. Expert consensus document: the international scientific association for probiotics and prebiotics (ISAPP) consensus statement on the definition and scope of prebiotics. Nat Rev Gastroenterol Hepatol. (2017) 14:491–502. doi: 10.1038/nrgastro.2017.75
7. Rowland I, Capurso L, Collins K, Cummings J, Delzenne N, Goulet O, et al. Current level of consensus on probiotic science–report of an expert meeting–London, 23 November 2009. Gut Microbes. (2010) 1:436–9. doi: 10.4161/gmic.1.6.13610
8. Swanson KS, Gibson GR, Hutkins R, Reimer RA, Reid G, Verbeke K, et al. The international scientific association for probiotics and prebiotics (ISAPP) consensus statement on the definition and scope of synbiotics. Nat Rev Gastroenterol Hepatol. (2020) 17:687–701. doi: 10.1038/s41575-020-0344-2
9. Jäger R, Mohr AE, Carpenter KC, Kersick CM, Purpura M, Moussa A, et al. International Society of Sports Nutrition Position Stand: Probiotics. J Int Soc Sports Nutr. (2019) 16:62. doi: 10.1186/s12970-019-0329-0
10. Roberts JD, Suckling CA, Peedle GY, Murphy JA, Dawkins TG, Roberts MG. An exploratory investigation of endotoxin levels in novice long distance triathletes, and the effects of a multi-strain probiotic/prebiotic, antioxidant intervention. Nutrients. (2016) 8:733. doi: 10.3390/nu8110733
11. Valimaki IA, Vuorimaa T, Ahotupa M, Kekkonen R, Korpela R, Vasankari T. Decreased training volume and increased carbohydrate intake increases oxidized LDL levels. Int J Sports Med. (2012) 33:291–6. doi: 10.1055/s-0031-1291223
12. Hoffman JR, Hoffman MW, Zelicha H, Gepner Y, Willoughby DS, Feinstein U, et al. The effect of 2 weeks of inactivated probiotic bacillus coagulans on endocrine, inflammatory, and performance responses during self-defense training in soldiers. J Strength Cond Res. (2019) 33:2330–7. doi: 10.1519/JSC.0000000000003265
13. Brouns F, Beckers E. Is the gut an athletic organ? digestion, absorption and exercise. Sports Med. (1993) 15:242–57. doi: 10.2165/00007256-199315040-00003
14. de Oliveira EP, Burini RC, Jeukendrup A. Gastrointestinal complaints during exercise: prevalence, etiology, and nutritional recommendations. Sports Med. (2014) 44:S79–85. doi: 10.1007/s40279-014-0153-2
15. Camilleri M. Leaky gut: mechanisms, measurement and clinical implications in humans. Gut. (2019) 68:1516–26. doi: 10.1136/gutjnl-2019-318427
16. Peters HP, De Vries WR, Vanberge-Henegouwen GP, Akkermans LM. Potential benefits and hazards of physical activity and exercise on the gastrointestinal tract. Gut. (2001) 48:435–9. doi: 10.1136/gut.48.3.435
17. Deibert P, MH-M, Rathman S, Berg A. Der Gastrointestinaltrakt – ein wichtiges Zielorgan für Gesundheit und Leistungsfähigkeit von SportlernDer Gastrointestinaltrakt – ein wichtiges Zielorgan für Gesundheit und Leistungsfähigkeit von Sportlern. Österreichisches J für Sportmedizin. (2000) 2:6–15.
18. Munukka E, Ahtiainen JP, Puigbo P, Jalkanen S, Pahkala K, Keskitalo A, et al. Six-week endurance exercise alters gut metagenome that is not reflected in systemic metabolism in over-weight women. Front Microbiol. (2018) 9:2323. doi: 10.3389/fmicb.2018.02323
19. Larun L, Brurberg KG, Odgaard-Jensen J, Price JR. Exercise therapy for chronic fatigue syndrome. Cochrane Database Syst Rev. (2017) 4:CD003200. doi: 10.1002/14651858.CD003200.pub7
20. Gleeson M, Pyne DB. Respiratory inflammation and infections in high-performance athletes. Immunol Cell Biol. (2016) 94:124–31. doi: 10.1038/icb.2015.100
21. Furushima D, Nishimura T, Takuma N, Iketani R, Mizuno T, Matsui Y, et al. Prevention of acute upper respiratory infections by consumption of catechins in healthcare workers: a randomized, placebo-controlled trial. Nutrients. (2019) 12:4. doi: 10.3390/nu12010004
22. Clancy RL, Gleeson M, Cox A, Callister R, Dorrington M, D'Este C, et al. Reversal in fatigued athletes of a defect in interferon gamma secretion after administration of Lactobacillus acidophilus. Br J Sports Med. (2006) 40:351–4. doi: 10.1136/bjsm.2005.024364
23. Martarelli D, Verdenelli MC, Scuri S, Cocchioni M, Silvi S, Cecchini C, et al. Effect of a probiotic intake on oxidant and antioxidant parameters in plasma of athletes during intense exercise training. Curr Microbiol. (2011) 62:1689–96. doi: 10.1007/s00284-011-9915-3
24. Peake JM, Neubauer O, Walsh NP, Simpson RJ. Recovery of the immune system after exercise. J Appl Physiol (1985). (2017) 122:1077–87. doi: 10.1152/japplphysiol.00622.2016
25. Budden KF, Gellatly SL, Wood DL, Cooper MA, Morrison M, Hugenholtz P, et al. Emerging pathogenic links between microbiota and the gut-lung axis. Nat Rev Microbiol. (2017) 15:55–63. doi: 10.1038/nrmicro.2016.142
26. Antunes KH, Fachi JL, de Paula R, da Silva EF, Pral LP, Dos Santos AA, et al. Microbiota-derived acetate protects against respiratory syncytial virus infection through a GPR43-type 1 interferon response. Nat Commun. (2019) 10:3273. doi: 10.1038/s41467-019-11152-6
27. Bradley KC, Finsterbusch K, Schnepf D, Crotta S, Llorian M, Davidson S, et al. Microbiota-driven tonic interferon signals in lung stromal cells protect from influenza virus infection. Cell Rep. (2019) 28:245–56 e4. doi: 10.1016/j.celrep.2019.05.105
28. Shida K, Sato T, Iizuka R, Hoshi R, Watanabe O, Igarashi T, et al. Daily intake of fermented milk with Lactobacillus casei strain Shirota reduces the incidence and duration of upper respiratory tract infections in healthy middle-aged office workers. Eur J Nutr. (2017) 56:45–53. doi: 10.1007/s00394-015-1056-1
29. Huang WC, Wei CC, Huang CC, Chen WL, Huang HY. The beneficial effects of lactobacillus plantarum PS128 on high-intensity, exercise-induced oxidative stress, inflammation, and performance in triathletes. Nutrients. (2019) 11:353. doi: 10.3390/nu11020353
30. Zhang H, Yeh C, Jin Z, Ding L, Liu BY, Zhang L, et al. Prospective study of probiotic supplementation results in immune stimulation and improvement of upper respiratory infection rate. Synth Syst Biotechnol. (2018) 3:113–20. doi: 10.1016/j.synbio.2018.03.001
31. Lucas PJ, Baird J, Arai L, Law C, Roberts HM. Worked examples of alternative methods for the synthesis of qualitative and quantitative research in systematic reviews. BMC Med Res Methodol. (2007) 7:4. doi: 10.1186/1471-2288-7-4
32. Campbell M, McKenzie JE, Sowden A, Katikireddi SV, Brennan SE, Ellis S, et al. Synthesis without meta-analysis (SWiM) in systematic reviews: reporting guideline. BMJ. (2020) 368:l6890. doi: 10.1136/bmj.l6890
33. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
34. Verhagen AP, de Vet HC, de Bie RA, Kessels AG, Boers M, Bouter LM, et al. The delphi list: a criteria list for quality assessment of randomized clinical trials for conducting systematic reviews developed by delphi consensus. J Clin Epidemiol. (1998) 51:1235–41. doi: 10.1016/S0895-4356(98)00131-0
35. Salehzadeh K. The effects of probiotic yogurt drink on lipid profile, CRP, and record changes in aerobic athletes. Life Sci. (2015) 9:32–7. doi: 10.3126/ijls.v9i4.12672
36. Brennan CJ Christopher A, Paul D, Hull M, Kirwan JP. Effects of a novel probiotic on exercise-induced gut permeability and microbiota in endurance athletes. Med Sci Sports Exerc. (2018) 50:840. doi: 10.1249/01.mss.0000538764.55259.9c
37. Tiollier E, Chennaoui M, Gomez-Merino D, Drogou C, Filaire E, Guezennec CY. Effect of a probiotics supplementation on respiratory infections and immune and hormonal parameters during intense military training. Mil Med. (2007) 172:1006–11. doi: 10.7205/MILMED.172.9.1006
38. Gill SK, Teixeira AM, Rosado F, Cox M, Costa RJ. High-dose probiotic supplementation containing lactobacillus casei for 7 days does not enhance salivary antimicrobial protein responses to exertional heat stress compared with placebo. Int J Sport Nutr Exerc Metab. (2016) 26:150–60. doi: 10.1123/ijsnem.2015-0171
39. Gill SK, Allerton DM, Ansley-Robson P, Hemmings K, Cox M, Costa RJ. Does short-term high dose probiotic supplementation containing lactobacillus casei attenuate exertional-heat stress induced endotoxaemia and cytokinaemia? Int J Sport Nutr Exerc Metab. (2016) 26:268–75. doi: 10.1123/ijsnem.2015-0186
40. Haywood BA, Black KE, Baker D, McGarvey J, Healey P, Brown RC. Probiotic supplementation reduces the duration and incidence of infections but not severity in elite rugby union players. J Sci Med Sport. (2014) 17:356–60. doi: 10.1016/j.jsams.2013.08.004
41. Sashihara T, Nagata M, Mori T, Ikegami S, Gotoh M, Okubo K, et al. Effects of Lactobacillus gasseri OLL2809 and alpha-lactalbumin on university-student athletes: a randomized, double-blind, placebo-controlled clinical trial. Appl Physiol Nutr Metab. (2013) 38:1228–35. doi: 10.1139/apnm-2012-0490
42. Shing CM, Peake JM, Lim CL, Briskey D, Walsh NP, Fortes MB, et al. Effects of probiotics supplementation on gastrointestinal permeability, inflammation and exercise performance in the heat. Eur J Appl Physiol. (2014) 114:93–103. doi: 10.1007/s00421-013-2748-y
43. West NP, Pyne DB, Cripps AW, Hopkins WG, Eskesen DC, Jairath A, et al. Lactobacillus fermentum (PCC(R)) supplementation and gastrointestinal and respiratory-tract illness symptoms: a randomised control trial in athletes. Nutr J. (2011) 10:30. doi: 10.1186/1475-2891-10-30
44. Townsend JR, Bender D, Vantrease WC, Sapp PA, Toy AM, Woods CA, et al. Effects of probiotic (bacillus subtilis DE111) supplementation on immune function, hormonal status, and physical performance in division i baseball players. Sports. (2018) 6:70. doi: 10.3390/sports6030070
45. Gepner Y, Hoffman J, Shemesh E, Stout J, Church D, Varanoske A, et al. The effect of bacillus coagulans and HMB on muscle integrity and inflammation during military training: 336 Board #157. Med Sci Sports Exerc. (2017) 49:81. doi: 10.1249/01.mss.0000517046.74329.2e
46. Carbuhn AF, Reynolds SM, Campbell CW, Bradford LA, Deckert JA, Kreutzer A, et al. Effects of probiotic (bifidobacterium longum 35624) supplementation on exercise performance, immune modulation, and cognitive outlook in division I female swimmers. Sports. (2018) 6:116. doi: 10.3390/sports6040116
47. Charlesson B, Ingram S, Deaville C, McNeilly A. The effect of short-term probiotic supplementation on gut flora of elite athletes. In: International Sport and Exercise Nutrition Conference. Human Kinetics Publishers Inc. (2013). p. 13.
48. Strasser B, Geiger D, Schauer M, Gostner JM, Gatterer H, Burtscher M, et al. Probiotic supplements beneficially affect tryptophan-kynurenine metabolism and reduce the incidence of upper respiratory tract infections in trained athletes: a randomized, double-blinded, placebo-controlled trial. Nutrients. (2016) 8:752. doi: 10.3390/nu8110752
49. Marshall H, Chrismas BCR, Suckling CA, Roberts JD, Foster J, Taylor L. Chronic probiotic supplementation with or without glutamine does not influence the eHsp72 response to a multi-day ultra-endurance exercise event. Appl Physiol Nutr Metab. (2017) 42:876–83. doi: 10.1139/apnm-2017-0131
50. Salarkia N, Ghadamli L, Zaeri F, Sabaghian Rad L. Effects of probiotic yogurt on performance, respiratory and digestive systems of young adult female endurance swimmers: a randomized controlled trial. Med J Islam Repub Iran. (2013) 27:141–6.
51. Cox AJ, Pyne DB, Saunders PU, Fricker PA. Oral administration of the probiotic Lactobacillus fermentum VRI-003 and mucosal immunity in endurance athletes. Br J Sports Med. (2010) 44:222–6. doi: 10.1136/bjsm.2007.044628
52. Michalickova DM, Kostic-Vucicevic MM, Vukasinovic-Vesic MD, Stojmenovic TB, Dikic NV, Andjelkovic MS, et al. Lactobacillus helveticus lafti L10 supplementation modulates mucosal and humoral immunity in elite athletes: a randomized, double-blind, placebo-controlled trial. J Strength Cond Res. (2017) 31:62–70. doi: 10.1519/JSC.0000000000001456
53. Michalickova D, Minic R, Dikic N, Andjelkovic M, Kostic-Vucicevic M, Stojmenovic T, et al. Lactobacillus helveticus lafti L10 supplementation reduces respiratory infection duration in a cohort of elite athletes: a randomized, double-blind, placebo-controlled trial. Appl Physiol Nutr Metab. (2016) 41:782–9. doi: 10.1139/apnm-2015-0541
54. O'Brien KV, Stewart LK, Forney LA, Aryana KJ, Prinyawiwatkul W, Boeneke CA. The effects of postexercise consumption of a kefir beverage on performance and recovery during intensive endurance training. J Dairy Sci. (2015) 98:7446–9. doi: 10.3168/jds.2015-9392
55. Gleeson M, Bishop NC, Struszczak L. Effects of Lactobacillus casei shirota ingestion on common cold infection and herpes virus antibodies in endurance athletes: a placebo-controlled, randomized trial. Eur J Appl Physiol. (2016) 116:1555–63. doi: 10.1007/s00421-016-3415-x
56. Lamprecht M, Bogner S, Schippinger G, Steinbauer K, Fankhauser F, Hallstroem S, et al. Probiotic supplementation affects markers of intestinal barrier, oxidation, and inflammation in trained men; a randomized, double-blinded, placebo-controlled trial. J Int Soc Sports Nutr. (2012) 9:45. doi: 10.1186/1550-2783-9-45
57. Pumpa KL, McKune AJ, Harnett J. A novel role of probiotics in improving host defence of elite rugby union athlete: a double blind randomised controlled trial. J Sci Med Sport. (2019) 22:876–81. doi: 10.1016/j.jsams.2019.03.013
58. Vaisberg M, Paixao V, Almeida EB, Santos JMB, Foster R, Rossi M, et al. Daily intake of fermented milk containing lactobacillus casei shirota (Lcs) modulates systemic and upper airways immune/inflammatory responses in marathon runners. Nutrients. (2019) 11:1678. doi: 10.3390/nu11071678
59. Komano Y, Shimada K, Naito H, Fukao K, Ishihara Y, Fujii T, et al. Efficacy of heat-killed Lactococcus lactis JCM 5805 on immunity and fatigue during consecutive high intensity exercise in male athletes: a randomized, placebo-controlled, double-blinded trial. J Int Soc Sports Nutr. (2018) 15:39. doi: 10.1186/s12970-018-0244-9
60. Pugh JN, Sparks AS, Doran DA, Fleming SC, Langan-Evans C, Kirk B, et al. Four weeks of probiotic supplementation reduces GI symptoms during a marathon race. Eur J Appl Physiol. (2019) 119:1491–501. doi: 10.1007/s00421-019-04136-3
61. Moreira A, Kekkonen R, Korpela R, Delgado L, Haahtela T. Allergy in marathon runners and effect of Lactobacillus GG supplementation on allergic inflammatory markers. Respir Med. (2007) 101:1123–31. doi: 10.1016/j.rmed.2006.11.015
62. Kekkonen RA, Vasankari TJ, Vuorimaa T, Haahtela T, Julkunen I, Korpela R. The effect of probiotics on respiratory infections and gastrointestinal symptoms during training in marathon runners. Int J Sport Nutr Exerc Metab. (2007) 17:352–63. doi: 10.1123/ijsnem.17.4.352
63. Gleeson M, Bishop NC, Oliveira M, Tauler P. Daily probiotic's (lactobacillus casei Shirota) reduction of infection incidence in athletes. Int J Sport Nutr Exerc Metab. (2011) 21:55–64. doi: 10.1123/ijsnem.21.1.55
64. Meng H, Lee Y, Ba Z, Peng J, Lin J, Boyer AS, et al. Consumption of Bifidobacterium animalis subsp. lactis BB-12 impacts upper respiratory tract infection and the function of NK and T cells in healthy adults. Mol Nutr Food Res. (2016) 60:1161–71. doi: 10.1002/mnfr.201500665
65. Mooren FC, Maleki BH, Pilat C, Ringseis R, Eder K, Teschler M, et al. Effects of escherichia coli strain nissle 1917 on exercise-induced disruption of gastrointestinal integrity. Eur J Appl Physiol. (2020) 120:1591–9. doi: 10.1007/s00421-020-04382-w
66. Muhamad A GM. Effects of a 14-strain probiotics supplement on salivary antimicrobial proteins at rest and in reponse to an acute bout of prolonged exercise. Int J Sports Sci. (2014) 4:60–6. doi: 10.5923/j.sports.20140402.04
67. Ibrahim NS, Muhamad AS, Ooi FK, Meor-Osman J, Chen CK. The effects of combined probiotic ingestion and circuit training on muscular strength and power and cytokine responses in young males. Appl Physiol Nutr Metab. (2018) 43:180–6. doi: 10.1139/apnm-2017-0464
68. West NP, Pyne DB, Cripps AW, Christophersen CT, Conlon MA, Fricker PA. Gut Balance, a synbiotic supplement, increases fecal lactobacillus paracasei but has little effect on immunity in healthy physically active individuals. Gut Microbes. (2012) 3:221–7. doi: 10.4161/gmic.19579
69. West NP, Horn PL, Pyne DB, Gebski VJ, Lahtinen SJ, Fricker PA, et al. Probiotic supplementation for respiratory and gastrointestinal illness symptoms in healthy physically active individuals. Clin Nutr. (2014) 33:581–7. doi: 10.1016/j.clnu.2013.10.002
70. Svedlund J, Sjodin I, Dotevall G. GSRS–a clinical rating scale for gastrointestinal symptoms in patients with irritable bowel syndrome and peptic ulcer disease. Dig Dis Sci. (1988) 33:129–34. doi: 10.1007/BF01535722
71. Jager R, Purpura M, Stone JD, Turner SM, Anzalone AJ, Eimerbrink MJ, et al. Probiotic streptococcus thermophilus FP4 and bifidobacterium breve BR03 supplementation attenuates performance and range-of-motion decrements following muscle damaging exercise. Nutrients. (2016) 8:642. doi: 10.3390/nu8100642
72. Mahmoud M, Abdallah NA, El-Shafei K, Tawfik NF, El-Sayed HS. Survivability of alginate-microencapsulated lactobacillus plantarum during storage, simulated food processing and gastrointestinal conditions. Heliyon. (2020) 6:e03541. doi: 10.1016/j.heliyon.2020.e03541
73. Martoni C, Bhathena J, Jones ML, Urbanska AM, Chen H, Prakash S. Investigation of microencapsulated BSH active lactobacillus in the simulated human GI tract. J Biomed Biotechnol. (2007) 2007:13684. doi: 10.1155/2007/13684
74. Pourjafar H, Noori N, Gandomi H, Basti AA, Ansari F. Viability of microencapsulated and non-microencapsulated lactobacilli in a commercial beverage. Biotechnol Rep. (2020) 25:e00432. doi: 10.1016/j.btre.2020.e00432
75. Buman MP OJ, Giacobbi PR, Brewer BW. Experiences and coping responses of “hitting the wall” for recreational marathon runners. J Appl Sport Psychol. (2008) 20:282–300. doi: 10.1080/10413200802078267
76. ter Steege RW, Van der Palen J, Kolkman JJ. Prevalence of gastrointestinal complaints in runners competing in a long-distance run: an internet-based observational study in 1281 subjects. Scand J Gastroenterol. (2008) 43:1477–82. doi: 10.1080/00365520802321170
77. Nieman DC, Johanssen LM, Lee JW, Arabatzis K. Infectious episodes in runners before and after the Los Angeles marathon. J Sports Med Phys Fitness. (1990) 30:316–28.
78. Barrett B, Brown RL, Mundt MP, Thomas GR, Barlow SK, Highstrom AD, et al. Validation of a short form wisconsin upper respiratory symptom survey (WURSS-21). Health Qual Life Outcomes. (2009) 7:76. doi: 10.1186/1477-7525-7-76
79. Gleeson M, Pyne DB. Special feature for the olympics: effects of exercise on the immune system: exercise effects on mucosal immunity. Immunol Cell Biol. (2000) 78:536–44. doi: 10.1111/j.1440-1711.2000.t01-8-.x
Keywords: exercise, gut microbiota, respiratory infection, immune system, nutrition, immunology, probiotic, gastrointestinal
Citation: Heimer M, Teschler M, Schmitz B and Mooren FC (2022) Health Benefits of Probiotics in Sport and Exercise - Non-existent or a Matter of Heterogeneity? A Systematic Review. Front. Nutr. 9:804046. doi: 10.3389/fnut.2022.804046
Received: 28 October 2021; Accepted: 28 January 2022;
Published: 23 February 2022.
Edited by:
Laurel M. Wentz, Appalachian State University, United StatesReviewed by:
Michael D. Roberts, Auburn University, United StatesMark Elisabeth Willems, University of Chichester, United Kingdom
Alex E. Mohr, Arizona State University, United States
Copyright © 2022 Heimer, Teschler, Schmitz and Mooren. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Frank C. Mooren, frank.mooren@uni-wh.de