
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Nutr. , 22 February 2022
Sec. Clinical Nutrition
Volume 9 - 2022 | https://doi.org/10.3389/fnut.2022.598920
 Mariana Dimitrov Ulian1*†
Mariana Dimitrov Ulian1*† Ana Jéssica Pinto2†
Ana Jéssica Pinto2† Priscila de Morais Sato1
Priscila de Morais Sato1 Fabiana B. Benatti2,3
Fabiana B. Benatti2,3 Patricia Lopes de Campos-Ferraz3Desire Coelho2Odilon J. Roble4
Patricia Lopes de Campos-Ferraz3Desire Coelho2Odilon J. Roble4 Fernanda Sabatini1Isabel Perez1Luiz Aburad1André Vessoni1
Fernanda Sabatini1Isabel Perez1Luiz Aburad1André Vessoni1 Ramiro Fernandez Unsain1
Ramiro Fernandez Unsain1 Marcelo Macedo Rogero1,5
Marcelo Macedo Rogero1,5 Geni Sampaio1
Geni Sampaio1 Bruno Gualano2
Bruno Gualano2 Fernanda B. Scagliusi1
Fernanda B. Scagliusi1We examined whether weight loss following HAES®-based interventions associates with changes in cardiometabolic risk factors and quality of life of women with obesity. This was an exploratory, ancillary analysis of a 7-month, mixed-method, randomized controlled trial. Fifty-five women (age: 33.0 ± 7.2; BMI: 30–39.9 kg/m2) were included in this study. Body weight, cardiovascular risk factors, clustered cardiometabolic risk, and quality of life were assessed before (Pre) and after HAES®-based interventions (Post). Delta scores (Post-Pre) were calculated for each outcome and used in linear regression models. After adjusting by potential confounders, weight loss was associated with improvements in waist circumference (β = 0.83, p <0.001), fasting glycemia (β = 0.45, p = 0.036), total cholesterol (β = 1.48, p = 0.024), LDL (β = 1.33, p = 0.012), clustered cardiometabolic risk (β = 0.18, p = 0.006), and quality of life (β = −1.05, p = 0.007). All participants but one who reduced body weight (n = 11) improved clustered cardiometabolic risk and quality of life. Of relevance, 34% and 73% of the participants who maintained or gained weight improved clustered cardiometabolic risk and quality of life, respectively, although the magnitude of improvements was lower than that among those who lose weight. Improvements in cardiovascular risk factors and quality of life following HAES®-based interventions associated with weight loss as expected. However, most of the participants who maintained or even gained weight experienced benefits to some extent. This suggests that weight-neutral, lifestyle-modification interventions may improve wellness and health-related outcomes, even in the absence of weight loss.
Intentional weight loss remains as the cornerstone treatment of people with obesity (1). However, it has been suggested that the monolithic focus on weight loss as the only determinant of success for strategies that aim to manage obesity may preclude opportunities to focus on lifestyle behaviors. These behaviors are associated with benefits across a wide range of health outcomes, regardless of weight status or weight change (2).
Diet- and exercise-induced weight loss are knowingly associated with reduced cardiometabolic risk (3). However, evidence suggests that people with obesity engaged in non-restrictive diets and exercise interventions may also exhibit improvements in abdominal circumference, insulin resistance, dyslipidemia, systemic inflammation, hypertension, and all-cause mortality with or without weight loss (4). Exercise reduces waist circumference and visceral fat, which is per se associated the improvements in cardiovascular risk factors independently of body weight changes (3, 5, 6).
The Health at Every Size® (HAES®) approach promotes a shift from a weight-centered to a weight-neutral approach by encouraging people with different body sizes to engage in healthier behaviors, with no primary focus on losing weight (7). Its principles include the promotion of a pleasurable and sustainable physical activity practice, and flexible, individualized eating based on hunger, satiety, nutritional needs, and pleasure. We recently showed that an intensive HAES®-based intervention was capable of improving participants' eating attitudes and practices, perception of body image, cardiorespiratory fitness, physical function, and health-related quality of life (8, 9). The central aim of our physical activity program was to increase enjoyment and autonomy in daily physical activities; thus, the participants were encouraged to exercise at a self-selected intensity. The nutritional intervention was based on nutritional counseling and diets were not prescribed. Instead, participants were encouraged to eat based on the principles of the HAES® approach. To date, it remains unclear whether HAES® interventions with the above-mentioned features can yield health-related benefits irrespective of changes in body weight. In this ancillary, exploratory study, we examined whether weight loss following a HAES®-based intervention is a determinant of changes in cardiometabolic risk factors and quality of life in women with obesity. Our working hypothesis was that weigh loss would relate to improvements in cardiometabolic health and wellness as expected, but even those participants who did not lose weight would experience some beneficial effects from the interventions.
The ancillary analysis is derived from a 7-month, mixed-method, randomized controlled trial. This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving human subjects were approved by the Ethics Committee of the School of Public Health, University of São Paulo (protocol 1.738.855). Written informed consent was obtained from all participants. This study is registered at clinicaltrials.gov (NCT02102061). Details regarding the experimental design, intervention, measures and outcomes, and main results can be found elsewhere (8, 10). In brief, the trial was designed to test the efficacy of two HAES®-based interventions of different intensities on health- and wellness-related variables in obese women. The intensive HAES® group underwent a program comprising three-times-a-week physical activity sessions, bimonthly individual nutritional sessions, and five philosophical workshops. The traditional HAES® group (control) only attended bimonthly educational lectures based on the HAES® principles. In this ancillary analysis, data from 55 participants who had complete body weight data were analyzed. We opted for combining data from both groups (intensive HAES® n = 36; traditional HAES® n = 19) to increase the power of our analysis, after considering that the assessment of separate groups would not significantly add to the current research question. Changes in anthropometric measures, cardiovascular risk factors, clustered cardiometabolic risk, and quality of life (delta score) were calculated and associated with weight loss.
Weight was measured by a digital scale. Weight loss was defined as a decrease in body weight ≥3%, in accordance with the definition of weight maintenance proposed by Stevens et al. (11). Waist circumference was measured using a plastic tape measure placed in the smallest circumference between the lowest margin of the ribs and the upper margin of the iliac crest with subjects standing.
Cardiovascular risk factors included blood pressure, fasting plasma glucose, insulin, glycated hemoglobin, and lipid profile. Homeostatic Model Assessment (HOMA-IR) was also calculated. Glucose was assessed using a colorimetric enzymatic assay (Bioclin, Brazil). Insulin was assessed using a radioimmunoassay technique (Diagnostic Products Corporation, Inc). Lipid profile was assessed using enzymatic colorimetric assays (CELM, São Paulo, Brazil).
Continuous clustered cardiometabolic risk was computed using waist circumference, mean blood pressure (average of systolic and diastolic pressure), fasting plasma triglycerides, high-density cholesterol (HDL), and glucose (12). Reference values were 88 cm, 115 mmHg, 150, 50, and 100 mg/dL, respectively. All variables were standardized [z = (value – reference) / SD]; for HDL (protective for cardiometabolic risk), z-score was inverted. The risk score was the sum of all standardized scores, with higher z-scores indicating higher cardiometabolic disease risk.
Quality of life was assessed by means of the total score of the World Health Organization Quality of Life—BREF questionnaire (WHOQOL-BREF), which has been translated to Portuguese and validated for the Brazilian population (13, 14). Higher scores represent higher quality of life, and the calculations were made following the syntax proposal by The WHOQOL Group (15). A total score of the WHOQOL-BREF was calculated. Such score consists of calculating the arithmetic mean of the scores of the 26 questions of the instrument for each participant (15).
Deltas score (Post-Pre) was calculated for the dependent variables to assess changes following the interventions. Linear regression models were used to test possible associations between changes in body weight (independent variable) and changes in waist circumference, cardiovascular risk factors, clustered cardiometabolic risk, and quality of life (dependent variables). Regression models were unadjusted or adjusted by potential confounding factors (i.e., age, body mass index, and baseline value of the dependent variable). Cohen's d effect sizes (ES) were calculated for changes in clustered cardiometabolic risk and quality of life for participants who lost (n = 11), maintained or gained body weight (n = 44), and for participants who maintained or gained body weight and improved clustered cardiometabolic risk (n = 15) and quality of life (n = 32). Data analysis was performed using the SAS (9.3) for Windows. The level of significance was set at p ≤ 0.050. Data are presented as mean ± SD and β or ES (95% confidence interval [95%CI]), except when stated otherwise.
Participants' age and BMI were 33.0 ± 7.2 years and 33.6 ± 2.8 kg/m2, respectively. Table 1 shows baseline data and delta scores for body weight, waist circumference, cardiovascular risk factors, clustered cardiometabolic risk, and quality of life.
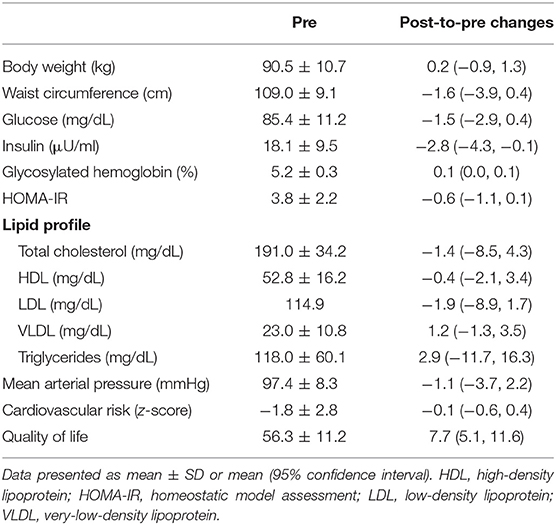
Table 1. Baseline values and delta changes for anthropometric measures, cardiovascular risk factors, clustered cardiometabolic risk, and quality of life.
Weight loss was associated with reductions in waist circumference (β = 0.79, p = 0.002), fasting glucose (β = 0.45, p = 0.036), L DL (β = 1.54, p = 0.018), clustered cardiometabolic risk (β = 0.20, p = 0.003), and quality of life (β = −0.82, p = 0.039) (Table 2). After adjusting by potential confounders, all associations were maintained; in addition, weight loss was associated with improvements in total cholesterol (β = 1.48, p = 0.024) (Table 2). No associations were found between weight loss and other risk factors (all p ≥ 0.050).
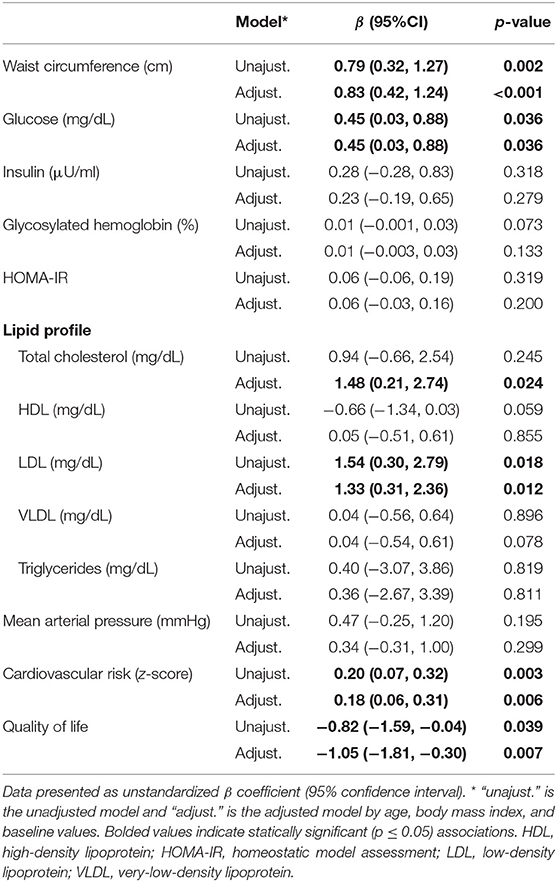
Table 2. Associations between changes in body weight (predictor variable) and waist circumference, cardiovascular risk factors, clustered cardiometabolic risk, and quality of life.
Figure 1 illustrates individual data for changes in body weight, clustered cardiometabolic risk, and quality of life. All participants but one who reduced body weight (n = 11) consistently reduced clustered cardiometabolic risk (ES: −1.2, 95%CI: −1.9, −0.6) and improved quality of life (ES: 1.2, 95%CI: 0.5, 2.0). The magnitude of the changes in clustered cardiometabolic risk (ES: 0.1, 95%CI: 0.0, 0.3) and quality of life (ES: 0.5, 95%CI: 0.2, 0.8) was lower in participants who maintained or increased body weight. Interestingly, however, 34% and 73% of these participants who did not lose weight experienced improvements in clustered cardiometabolic risk (ES: −0.5, 95%CI: −0.7, −0.2) and quality of life (ES: 0.9, 95%CI: 0.6, 1.3), respectively (Figure 2).
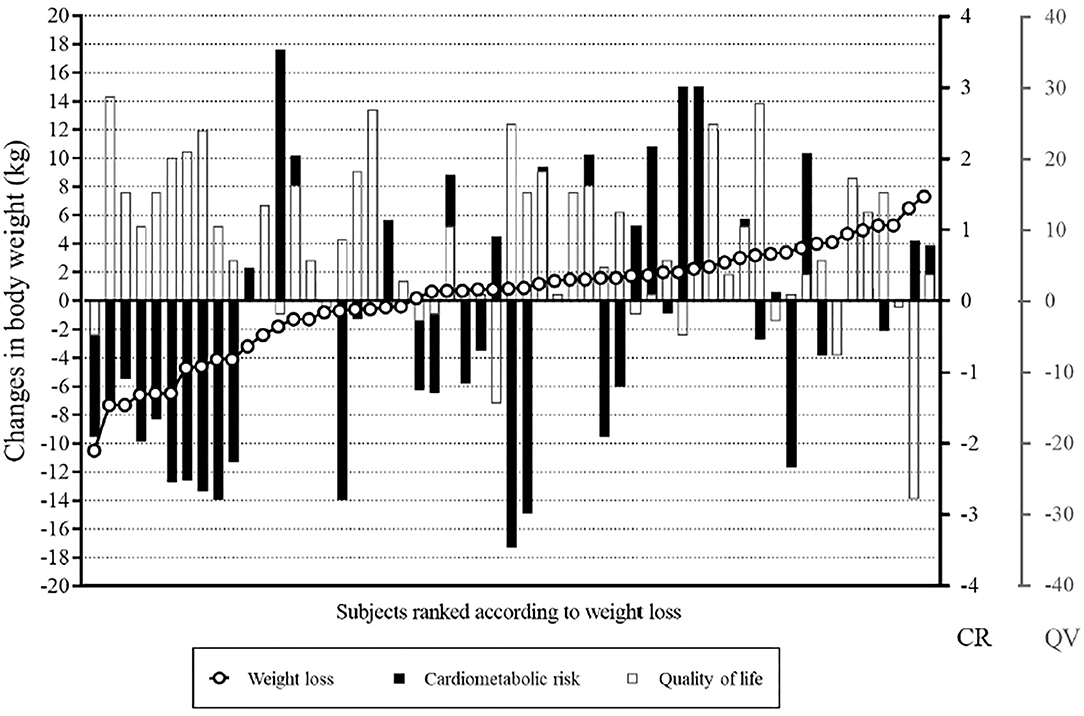
Figure 1. Individual data for changes in body weight, clustered cardiometabolic risk, and quality of life. Although the participants who lost more weight showed greater health improvements (those on the left side), benefits in cardiometabolic risk and quality of life can be seen all across the spectrum of changes in body weight. CR, cardiovascular risk: negative values mean improvement; QL, quality of life: positive values mean improvement.
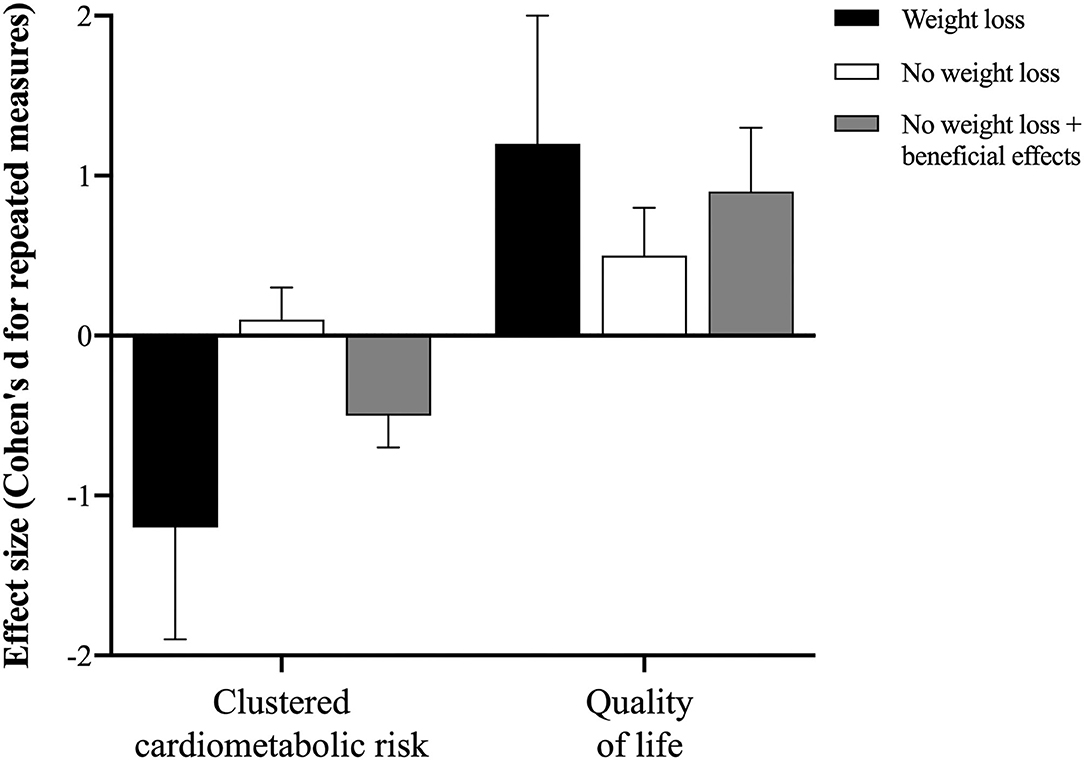
Figure 2. Effect size (Cohen's d for repeated measures) for clustered cardiometabolic risk, and quality of life in participants who lost weight (“weight loss”; n = 11), those who maintained or gained body weight (“no weight loss”, n = 44), and those who maintained or gained body weight and showed some improvement in cardiometabolic profile or quality of life (“no weight loss + beneficial effect”, n = 15 and 32, respectively). This overview picture supports the conclusion that intervention-induced weight loss induces greater improvements in cardiometabolic health; however, improvements in health and wellness may take place in the absence of weight loss or even weight gain, although the magnitude of the benefits is clearly lower, as compared to that of the first scenario.
To our knowledge, this was the first study to investigate whether weight loss following HAES®-based interventions is associated with changes in waist circumference, cardiovascular risk factors, clustered cardiometabolic risk, and quality of life in women with obesity. Our main finding was that weight loss was associated with improvements in selected cardiovascular risk factors, clustered cardiometabolic risk, and quality of life as expected; however, the majority of participants who maintained or even gained weight also benefited from the intervention to some extent.
Intentional weight loss is associated with reduction of all-cause mortality (16). In our study, weight loss associated with improvements in glucose, LDL, clustered cardiometabolic risk, and quality of life. Participants who lost weight were the ones who most benefited from the intervention, which is in line with the evidence that improvements in cardiovascular risk factors are proportional to the degree of weight loss (17). Indeed, weight loss is considered the most common target for success in obesity management. However, health-related benefits associated with weight loss may be better explained by concomitant reductions in total body and visceral fat, which are more strongly associated with cardiovascular risk than BMI itself (18).
The result showing that weight loss correlates with improvements in overall health following a lifestyle intervention is not novel. Nonetheless, our most striking finding was that some participants who maintained weight or even gained weight also improved waist circumference, clustered metabolic risk, and quality of life, with ES varying between moderate to high (although at values below those found for the participant who lost weight; see Figure 2 for an overview). These results corroborate the potential of eating and exercise interventions in improving health- and wellness-related markers to some level despite weight loss (4), and extend this notion to HAES®-based interventions, which refrain from targeting weight loss as a primary focus. In the majority of HAES®-based interventions (19, 20), physical activity is not an effective component of the intervention; despite participants are generally encouraged to practice physical activity, this is not formally included in the programs or even assessed as an outcome. Conversely, in our study, we developed a specific physical activity program based on HAES® approach, which is thoroughly described elsewhere (8). Indeed, the applicability of our program in different contexts (e.g., distinct sociocultural status, ages, body sizes, men groups, etc.) requires validation.
It has been argued that HAES® approach may lead to poor nutritional choices and to a state of passivity, resulting in weight gain (21). Our data challenge this notion by showing that 80% of our participants who underwent a weight-neutral intervention reduced or maintained weight. Notably, the participants also improved eating attitudes, body image, physical capacity, and quality of life (8, 9). The excessive focus on weight loss may deviate the focus on overall health gains potentially attained with lifestyle-modification programs characterized by an increase in physical activity and healthy eating (2, 4). Moreover, interventions highly centered in weight loss have been shown to lead to frustration due to weight loss failures (2), and reinforcement of fat stigma, according to which certain types of body are simply “inadequate”, potentially leading to body image and eating disorders (22). Our findings support the notion that interventions aimed at preventing obesity should be primarily focused on lifestyle-based behavior changes rather than weight loss, which should not be sole indicator of success in the management of obesity (4). Long-term studies should confirm the feasibility and efficacy of this sort of intervention, since obesity is a complex condition whose successful management relies in numerous biological, social and environmental factors.
In conclusion, improvements in cardiovascular risk factors and quality of life following an HAES®-based intervention were associated with weight loss. Indeed, beneficial effects were more pronounced in those who reduced body weight; however, participants who maintained or even gained weight also experienced benefits to some extent regarding cardiovascular health and quality of life. These findings suggest that weight loss enhances, but not determine, the beneficial effects of a weight-neutral, lifestyle-modification intervention, which can be an efficient strategy in the management of obesity.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
The studies involving human participants were reviewed and approved by Ethics Committee of the School of Public Health, University of São Paulo (protocol 1.738.855). The patients/participants provided their written informed consent to participate in this study.
MD, AP, FS, and BG conceived the presented idea. PM, FB, PL, DC, OR, FS, IP, LA, AV, and RF contributed to the design and implementation of the research. GS and MR contributed to the data analysis. All authors contributed to the analysis of the results and to the writing of the manuscript.
This work was supported by the Research Support Foundation of the State of São Paulo (FAPESP), Grant Number 2015/03878-2. Finally, each author received a fellowship grant. FS was supported by CNPq (Grant Numbers 311357/2015-6 and 309514/2018-5) and FAPESP (Grant Number 2017/17424-9); AP, PM, and RF by FAPESP (Grant Numbers 2015/26937-4, 2017/05651-0, and 2015/12235-8, respectively); BG has a productivity grant by CNPq and is also supported by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior—Brasil (CAPES), and MD by CAPES—Finance code 001. The funding sources had no involvement in study design and in the collection, analysis and interpretation of data.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Jensen MD, Ryan DH, Apovian CM, Ard JD, Comuzzie AG, Donato KA, et al. 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and The Obesity Society. J Am Coll Cardiol. (2014) 63:2985–3023. doi: 10.1016/j.jacc.2013.11.004
2. Ross R, Blair S, de Lannoy L, Després JP, Lavie CJ. Changing the endpoints for determining effective obesity management. Prog Cardiovasc Dis. (2015) 57:330–6. doi: 10.1016/j.pcad.2014.10.002
3. Ross R, Dagnone D, Jones PJ, Smith H, Paddags A, Hudson R, et al. Reduction in obesity and related comorbid conditions after diet-induced weight loss or exercise-induced weight loss in men: a randomized, controlled trial. Ann Intern Med. (2000) 133:92–103. doi: 10.7326/0003-4819-133-2-200007180-00008
4. Hyde PN, Sapper TN, Crabtree CD, LaFountain RA, Bowling ML, Buga A, et al. Dietary carbohydrate restriction improves metabolic syndrome independent of weight loss. JCI Insight. (2019) 4:12. doi: 10.1172/jci.insight.128308
5. Lee S, Kuk JL, Davidson LE, Hudson R, Kilpatrick K, Graham TE, et al. Exercise without weight loss is an effective strategy for obesity reduction in obese individuals with and without Type 2 diabetes. J Appl Physiol. (2005) 99:1220–5. doi: 10.1152/japplphysiol.00053.2005
6. Ross R, Janssen I, Dawson J, Kungl AM, Kuk JL, Wong SL, et al. Exercise-induced reduction in obesity and insulin resistance in women: A randomized controlled trial. Obes Res. (2004) 12:789–98. doi: 10.1038/oby.2004.95
7. ASDAH. Association for Size Diversity and Health. (2003). Available online at: https://www.sizediversityandhealth.org/ (accessed December 6, 2021).
8. Ulian MD, Pinto AJ, Sato PM, Benatti FB, de Campos-Ferraz P, Coelho D, et al. Effects of a new intervention based on the Health at Every Size approach for the management of obesity: The “Health and Wellness in Obesity” study. PLoS ONE. (2018) 13:e0198401. doi: 10.1371/journal.pone.0198401
9. Sabatini F, Ulian MD, Perez I, Pinto AJ, Vessoni A, Aburad L, et al. Eating pleasure in a sample of obese Brazilian women: a qualitative report of an interdisciplinary intervention based on the Health at Every Size Approach. J Acad Nutr Diet. (2019) 119:1470–82. doi: 10.1016/j.jand.2019.01.006
10. Ulian M, Gualano B, Benatti F, de Campos-Ferraz P, Coelho D, Roble O, et al. The design and rationale of an interdisciplinary, non-prescriptive, and Health at Every Size®-based clinical trial: The “Health and Wellness in Obesity” study. J Nutr Health. (2017) 23:261–70. doi: 10.1177/0260106017731260
11. Stevens J, Truesdale KP, McClain JE, Cai J. The definition of weight maintenance. Int J Obes. (Lond.). (2006) 30:391–9. doi: 10.1038/sj.ijo.0803175
12. Wijndaele K, Beunen G, Duvigneaud N, Matton L, Duquet W, Thomis M, et al. A continuous metabolic syndrome risk score: utility for epidemiological analyses. Diabetes Care. (2006) 29:2329. doi: 10.2337/dc06-1341
13. WHOQOL Group. (The). Development of the World Health Organization WHOQOL-BREF Quality of Life Assessment. Psychol Med. (1998) 28:551–8. doi: 10.1017/S0033291798006667
14. Fleck MPA. O instrumento de avaliação de qualidade de vida da Organização Mundial da Saúde(WHOQOL-100): características e perspectivas. Cien Saude Colet. (2000) 5:33–8. doi: 10.1590/S1413-81232000000100004
15. Pedroso B, Pilatti LA, Gutierrez GL, Picinin CT. Calculation of scores and descriptive statistics of WHOQOL-bref through Microsoft Excel. Revista Brasileira de Qualidade de Vida. (2010) 1:31–6. doi: 10.3895/S2175-08582010000100004
16. Kritchevsky SB, Beavers KM, Miller ME, Shea MK, Houston DK, Kitzman DW, et al. Intentional weight loss and all-cause mortality: a meta-analysis of randomized clinical trials. PLoS ONE. (2015) 10:e0121993. doi: 10.1371/journal.pone.0121993
17. Wing RR, Lang W, Wadden TA, Safford M, Knowler WC, Bertoni AG, et al. Benefits of modest weight loss in improving cardiovascular risk factors in overweight and obese individuals with type 2 diabetes. Diabetes Care. (2011) 34:1481–6. doi: 10.2337/dc10-2415
18. Despres J-P. Abdominal obesity: The most prevalent cause of the metabolic syndrome and related cardiometabolic risk. Eur Heart J Suppl. (2006) 8:B4–12. doi: 10.1093/eurheartj/sul002
19. Bacon L, Stern J, Van Loan M, Keim N. Size acceptance and intuitive eating improve health for obese, female chronic dieters. J Am Diet Assoc. (2005) 105:929–36. doi: 10.1016/j.jada.2005.03.011
20. Provencher V, Bégin C, Tremblay A, Mongeau L, Boivin S, Lemieux S. Short-term effects of a “Health-At-Every-Size” approach on eating behaviors and appetite ratings. Obesity. (2007) 15:957–66. doi: 10.1038/oby.2007.638
21. Sainsbury A. Call for an urgent rethink of the Health at Every Size concept. J Eat Disord. (2014) 2:8. doi: 10.1186/2050-2974-2-8
Keywords: obesity, lifestyle intervention, cardiovascular risk, physical activity, weight-neutral approach
Citation: Dimitrov Ulian M, Pinto AJ, Morais Sato Pd, Benatti FB, Lopes de Campos-Ferraz P, Coelho D, Roble OJ, Sabatini F, Perez I, Aburad L, Vessoni A, Fernandez Unsain R, Rogero MM, Sampaio G, Gualano B and Scagliusi FB (2022) Health at Every Size®-Based Interventions May Improve Cardiometabolic Risk and Quality of Life Even in the Absence of Weight Loss: An Ancillary, Exploratory Analysis of the Health and Wellness in Obesity Study. Front. Nutr. 9:598920. doi: 10.3389/fnut.2022.598920
Received: 25 August 2020; Accepted: 27 January 2022;
Published: 22 February 2022.
Edited by:
Nada Rotovnik Kozjek, Institute of Oncology Ljubljana, SloveniaReviewed by:
Milena Blaz Kovac, Community Health Centre Ljubljana, SloveniaCopyright © 2022 Dimitrov Ulian, Pinto, Morais Sato, Benatti, Lopes de Campos-Ferraz, Coelho, Roble, Sabatini, Perez, Aburad, Vessoni, Fernandez Unsain, Rogero, Sampaio, Gualano and Scagliusi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mariana Dimitrov Ulian, bS5kaW1pdHJvdkB1c3AuYnI=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.