
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Nutr. , 06 January 2023
Sec. Clinical Nutrition
Volume 9 - 2022 | https://doi.org/10.3389/fnut.2022.1085037
This article is part of the Research Topic Nutritional Assessment Tools for Identification and Monitoring of Malnutrition in Patients with Chronic Disease, Volume II View all 14 articles
 Tianyu Jiang1,2†
Tianyu Jiang1,2† Yongmei Jiang3†
Yongmei Jiang3† Qianwen Jin3†
Qianwen Jin3† Shining Xu1,2
Shining Xu1,2 Abraham Fingerhut1,2,4
Abraham Fingerhut1,2,4 Yongmei Shi3*
Yongmei Shi3* Minhua Zheng1,2*
Minhua Zheng1,2* Zirui He1,2*
Zirui He1,2*Background: Perioperative immune-nutritional status is correlated with post-operative outcomes. This study aimed to evaluate whether pre-operative nutritional status could predict post-operative complications in patients with Crohn’s disease (CD) and whether pre-operative enteral nutrition (EN) can prevent post-operative complications.
Methods: This retrospective cohort study analyzed the electronic health records of 173 patients diagnosed with CD in Ruijin Hospital, Shanghai, China, between August 2015 and May 2021: 122 patients had pre-operative nutritional support while 51 patients underwent surgery without pre-operative nutritional support. The pre-operative nutritional status, disease activity index, disease-related data, frequency of multiple surgery, operative data, and post-operative characters in each group were compared to determine whether the nutritional support and status could significantly affect post-operative outcome. One-to-one propensity score matching (PSM) was performed to limit demographic inequalities between the two groups.
Results: After PSM, no statistically significant differences were found in pre-operative patient basic characteristics between the two groups of 47 patients (98 patients in all) included in this study. Overall, 21 patients developed 26 post-operative complications. In terms of pre-operative nutritional status, the level of serum albumin (ALB), pre-albumin (pre-ALB), and hemoglobin (Hb) in the nutrition group were statistically higher than that in the control group. We also observed a statistically significant decrease in post-operative complications, need for emergency surgery, and staged operations, while the rate of laparoscopic surgery was higher in the nutrition group compared to the non-nutritional group. Post-operative complications were related to pre-operative nutritional condition, which indicated that EN may improve the nutritional status and reduced the rate of post-operative complications.
Conclusion: Pre-operative nutritional status is correlated with post-operative outcomes while EN plays a positive role in preventing the post-operative complications. EN is useful for improving the pre-operative nutritional status and reducing the post-operative adverse events for CD patients undergoing surgery.
Crohn’s disease (CD) is a chronic inflammatory disease of the intestinal mucosa which can occur discontinuously throughout the entire digestive tract. Its pathogenesis is still poorly understood (1, 2). In China, the morbidity and prevalence of CD are increasing constantly, which leads to a heavy economic and social burden (3). Although the innovation and application of series of new drugs has greatly improved the therapeutic effect (4), complications such as intestinal bleeding, obstruction, fistula, perforation, abscess still occur (5, 6), these patients as well as those who respond poorly to conservative treatment may require surgery (7, 8).
During the natural course of CD, the nutritional condition and the diet are important in the etiology of CD, particularly in regions where the rising prevalence rate has paralleled changes in eating habits and food industrialization (9, 10). High prevalence of malnutrition and micronutrient deficiencies were observed in patients with CD and constitutes a challenging issue for patients who require surgery (9). While malnutrition was confirmed to be an independent prognostic factor for increased risk of post-operative complications after abdominal surgery, which contributes to approximate 20–40% of surgical complication rates (11, 12). In this regards, early diagnosis of malnutrition is extremely important since pre-operative nutritional intervention may contribute to lower post-surgical complication and mortality rates (13–15). However, until now, there is few evidence directly linking nutritional status to post-operative complications in CD patients. Evidence that supports the effectiveness of nutritional support for patients with CD during peri-operative period, and whether it can contribute to lower post-operative complication incidence rate is scant (11, 16). Thus, we selected scored Patient-Generated Subjective Global Assessment (PG-SGA score) as a validated tool to screen patients’ immune-nutritional status (17, 18), and we selected the comprehensive complication index (CCI) to quantify the post-operative complications within 30 days.
Furthermore, several strategies were adopted to establish a standard clinical protocol of pre-operative enteral nutrition (EN): including patient nutrition education programs, dietary instruction, partial enteral nutrition (PEN), exclusive enteral nutrition (EEN), and total parenteral nutrition (TPN), which can significantly reduce the effects of catabolism (19). Our primary hypothesis was that pre-operative EN would increase pre-operative immune-nutritional status and reduce 30-day post-operative complications, as measured using the CCI. The objective of this study is to evaluate whether the nutritional status could predict post-operative complications in CD patients and the benefit of EN on the nutritional status and preventing post-operative complications of CD patients.
This retrospective study included all patients undergoing surgery for CD at Ruijin Hospital from 12 August 2015 to 19 May 2021. Included were patients with post-operative histological diagnosis of CD according to the European Crohn’s and Colitis Organization (ECCO) guidelines (7, 8) and Consensus Opinion on Diagnosis and Treatment of inflammatory bowel disease (2018, Beijing) of the Chinese Inflammatory Bowel Disease Group (20), who underwent surgical resection due to failure of medical therapy or developed complications with the following inclusion criteria: (1) age ≥18 years, male or non-pregnant female; (2) American Society of Anesthesiologists (ASA) Grades I–III; and (3) complete follow-up data. All indications were discussed in the multidisciplinary team (MDT) conference including gastrointestinal surgeons, gastroenterologists, nutritionists, pathologists, radiologists, and nurses. Patients with incomplete clinical data or electronic health record were excluded. Patients were divided into two groups according to whether they had received pre-operative nutritional support or not.
This study was approved by the hospital’s Ethics Committee and all patients provided informed consent.
All patients receiving nutritional support were assessed by the PG-SGA score and activity of CD with Crohn’s Disease Activity Index (CDAI) before surgical procedure. The index was assessed by nutritionists and surgeons at the time of admission for surgery and were stored in patients’ clinical database and electronic health record. Patients with CDAI scored 0 to 149 points were identified as remission, while patients with CDAI scored no less than 150 points were identified with active disease, according to the ECCO and Beijing guidelines (7, 8, 20). During the course of nutritional support, nutritional deficiency was screened by blood tests routinely, once every 3 months for patients with mild to severe active disease and once every 6 months in patients in asymptomatic remission. Laboratory data refer to the nutritional condition were collected from electronic health record.
Protein requirements for patients in remission was 1 g⋅kg–1⋅day–1 in adults, similar to that recommended for the general population, while protein requirement was 1.2–1.5 g⋅kg–1⋅day–1 in adults with active disease (21). All patients were asked to adhere to nutrition education programs. The nutritionist provided individual dietetic recommendation for each patient (22).
Patients who could not meet the expected energy requirements underwent EN depending on the disease activity, duration of feeding, patient compliance, and gastrointestinal function. For the patients with asymptomatic remission, energy supply was 25–30 kcal⋅kg–1⋅day–1. PEN was recommended for these patients while 400–1800 kcal⋅d–1 through method of EN, the rest of energy requirement was taken by dietary. For patients with active disease, energy supply was 8–10% higher than the remission phase, which was 30–35 kcal⋅kg–1⋅day–1. For patients whose dietic intake did not meet the standard nutritional requirements, we selected EEN as the method of nutritional support. Patients who could not tolerate EN because of severe obstruction or fistule, TPN was recommended.
The supplement of microelements was applied according to the result of laboratory blood test at the discretion of treating physician. Vitamin D and calcium supplements were recommended depending on the assessment of osteoporosis and level of serum calcium when 25-OH-Vit D was inferior to 75 nmol/L. Hypoferric anemia was corrected by iron therapy: oral supplement for the patients of mild iron deficiency anemia (100 g⋅L–1 ≤ hb<120 g⋅L–1), intravenous iron supplementation for the patients of moderate anemia (hb < 100 g⋅L–1). For the loss of vitamin B12, folic acid, potassium, magnesium, calcium, and phosphorus caused by diarrhea in CD patients, oral supplement was applicated according to the results of blood test.
Laboratory data including white blood count (WBC), total lymphocyte count (TLC), red blood count (RBC), hemoglobin (Hb), albumin (ALB), pre-albumin (pre-ALB), C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), and parameter such as vitamin D, vitamin K, folic acid, 25-OH-Vit D, serum iron, serum calcium, serum phosphorus, serum magnesium. The prognostic nutritional index (PNI) was calculated from the serum ALB and TLC level, and the formula was PNI = 10 × ALB (g/dL) + 0.005 TLC (per mL).
Intraoperative data including surgical approach (open vs. laparoscopy), surgical option (resection or ostomy), surgical type, staged surgery or not, operation time, estimated blood loss (EBL) and intraoperative mortality or complication.
Post-operative data including post-operative complications recorded up to 30 days after surgery (graded according to the Clavien-Dindo classification), treatment of complications, time to bowel movements, post-operative fluid intake time, and length of stay (LOS) were obtained from electronic medical records. Time to bowel movements, post-operative fluid intake time, total LOS, post-operative LOS, and hospitalization expenses were recorded. CCI integrates all complications with their respective severities on a continuous scale ranging from 0 (no burden due to complications) to 100 (death as a result of complications). The CCI was scored by the CCI calculator available online.1
Baseline characteristics data including age, sex, ASA score, body mass index (BMI), comorbidity, smoking and alcohol history, medication history. perioperative data, and laboratory data were collected from the clinical database and electronic health record. CD-related data included CDAI, PG-SGA score, Montreal classification, duration of disease, recurrence rate, and pre-operative drug therapy: either infliximab (documented dose of infliximab for more than 4 weeks before surgery) or corticosteroids (daily dose of 5 mg prednisolone or 4 mg methylprednisolone and within 4 weeks before surgical intervention). Missing data were treated with multiple imputations.
All statistical analyses were performed using SPSS 26.0 (Armonk, NY, USA: IBM Corp). PSM analysis was conducted using a logistic regression model with the selected co-variates. We used a caliper width of 0.05 for the pooled standard deviation of the logit for PSM. Demographic and clinical characteristics were summarized and descriptively analyzed, and all quantitative values were presented as means and standard deviations. The Student’s t-test or the Mann–Whitney U-test and Pearson’s χ2 (or Fisher’s exact test) were used to compare continuous and categorical variables, respectively. All values were two tailed, and p-values < 0.05 were considered to be significant.
The study flow chart was summarized in Figure 1. We identified 183 consecutive cases of CD that underwent surgery from August 2015 to May 2021. We excluded 10 cases due to missing important records: missing nutritional support data (n = 3), missing nutritional assessment data (n = 3), and missing CCI report (n = 4). Hence, 122 cases in the nutrition group and 51 cases in the non-nutrition group were adjusted by PSM. Table 1 shows the baseline characteristics of the 173 patients. Compared with patients in the non-nutrition group, patients in nutrition group had younger ages (p = 0.031), higher ASA score (p = 0.002). The PSM analysis was conducted using a logistic regression model with the following co-variates: age, sex, ASA Score, and drug therapy (Table 1).
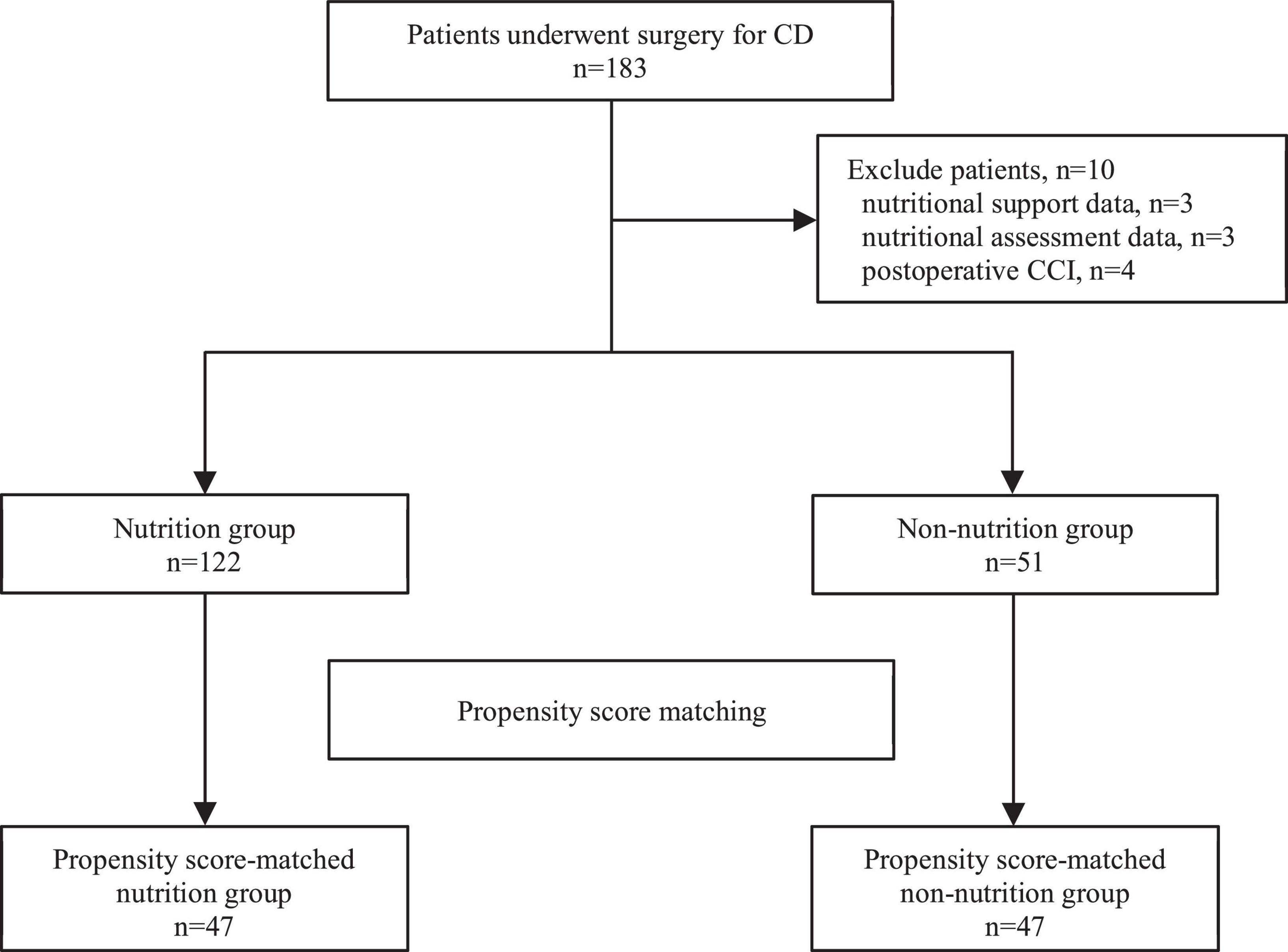
Figure 1. Study flow chat.
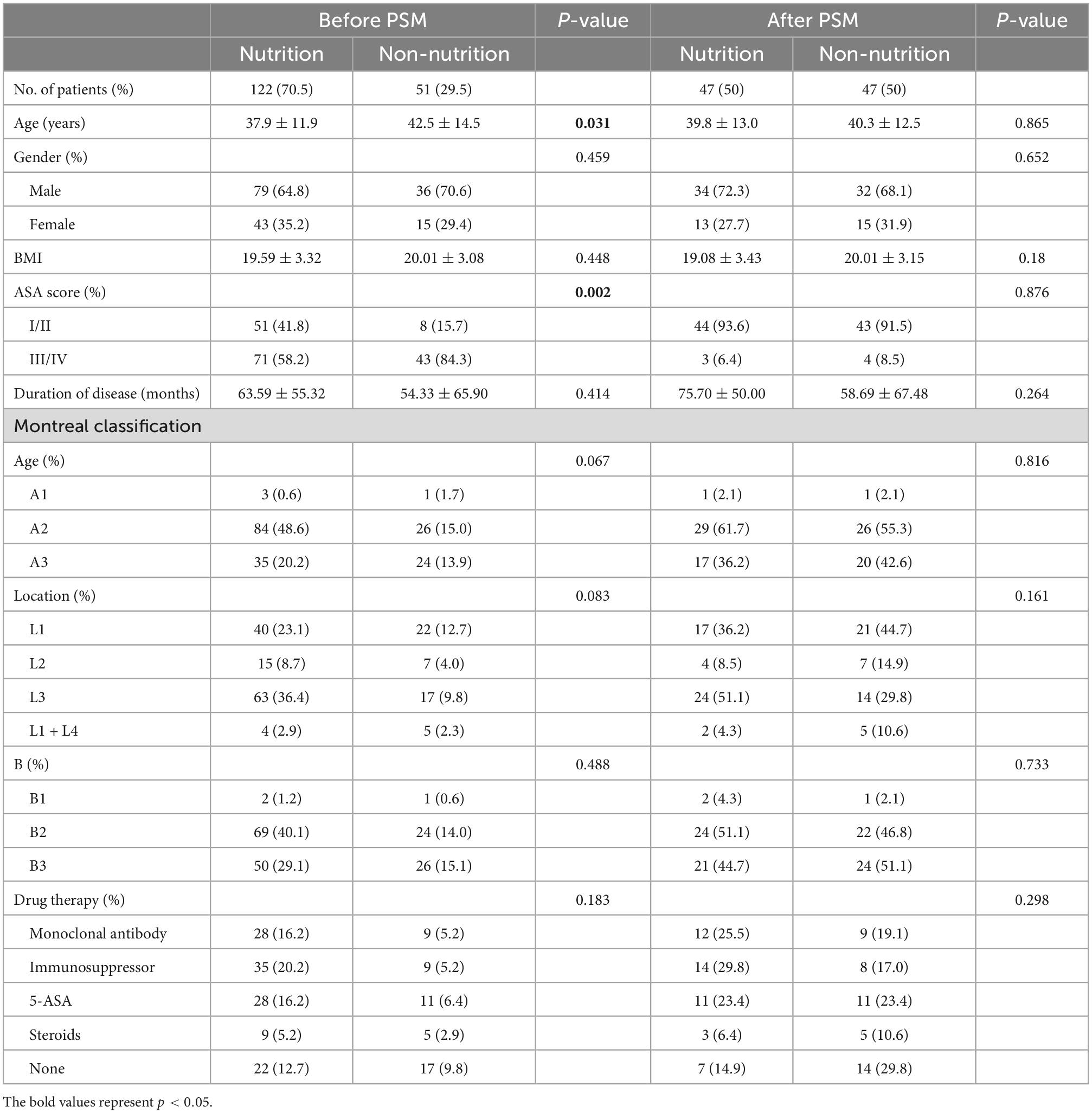
Table 1. Patient demographics characteristics.
After 1:1 PSM, there were 47 patients in each treatment strategy. No statistically significant difference was found in mean duration before surgery between the two groups (p = 0.264) (overall 65.35 ± 7.4 months). Ileal and ileocolonic involvement were the most common disease patterns, 34.0 and 33.0%, respectively. The overall recurrence rate was 24.5%, without any statistically significant difference between the two groups [10/47 (21.3%) vs. 13/47 (27.7%), p = 0.472]. Likewise, there were no statistically significant differences in age, gender, BMI, ASA score, duration from CD diagnosis to surgery, Montreal classification, and pre-operative medical history (Table 1).
The overall mean duration of nutritional treatment was 124 ± 22 days. All patients completed at least 3 months of nutritional support (range 93–475 days). Among all 47 patients who received nutritional support, 32 patients (68.1%) received PEN, 8 patients (17.0%) received EEN, 1 patient (2.1%) received EEN + PN, 6 patients (12.8%) received only dietary recommendation with micronutrient supplement. All 47 patients in the nutritional group demonstrated significant laboratory improvement of nutritional indices. Changes in inflammation and nutritional parameters are presented in Table 2. Mean-while, the nutritional group had a higher PG-SGA score, PG-SGA classification, CDAI index, and PNI (p < 0.0001). No statistically significant difference in BMI was observed (Table 3).
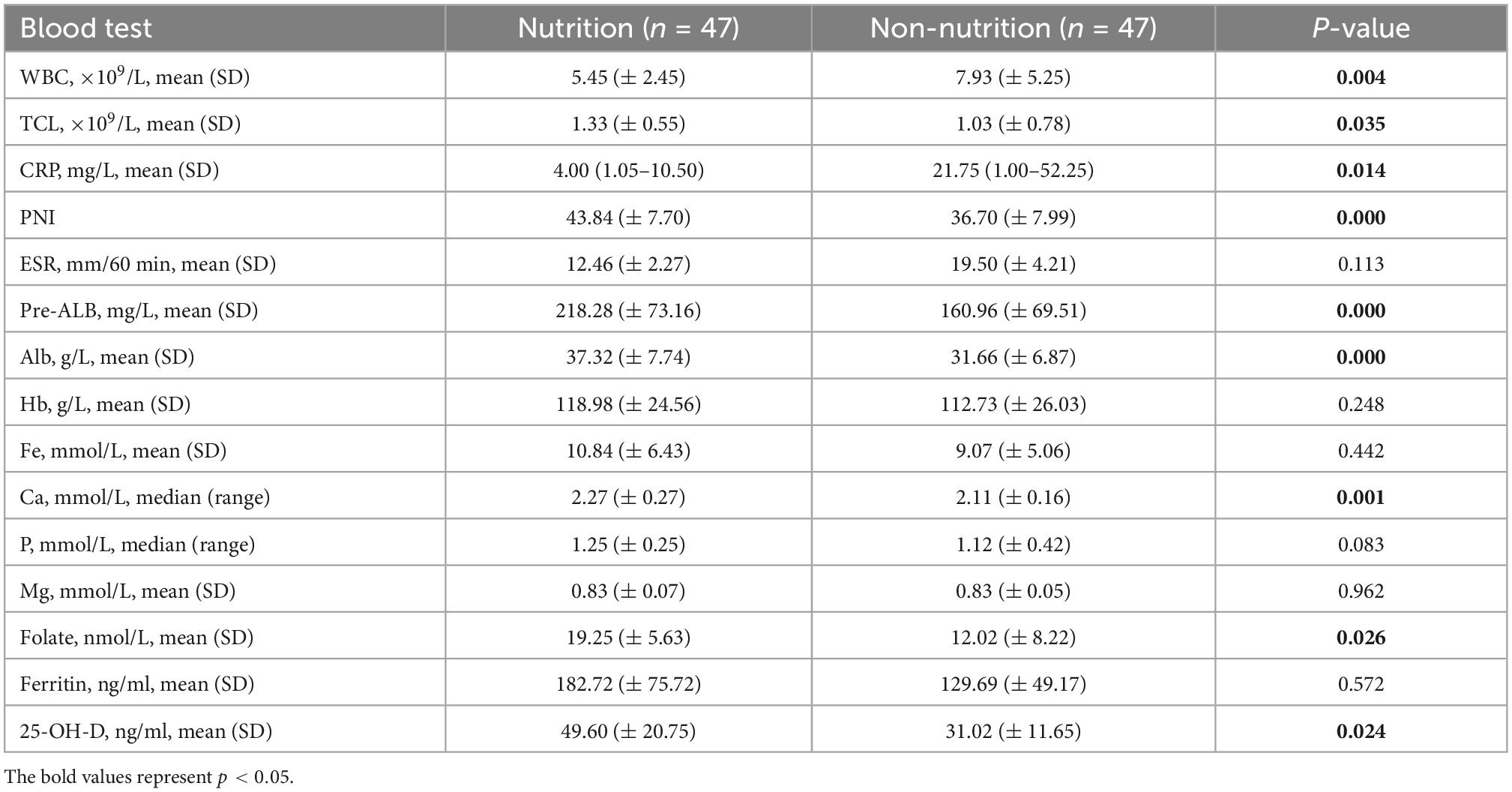
Table 2. Laboratorial inflammation and nutritional parameters.
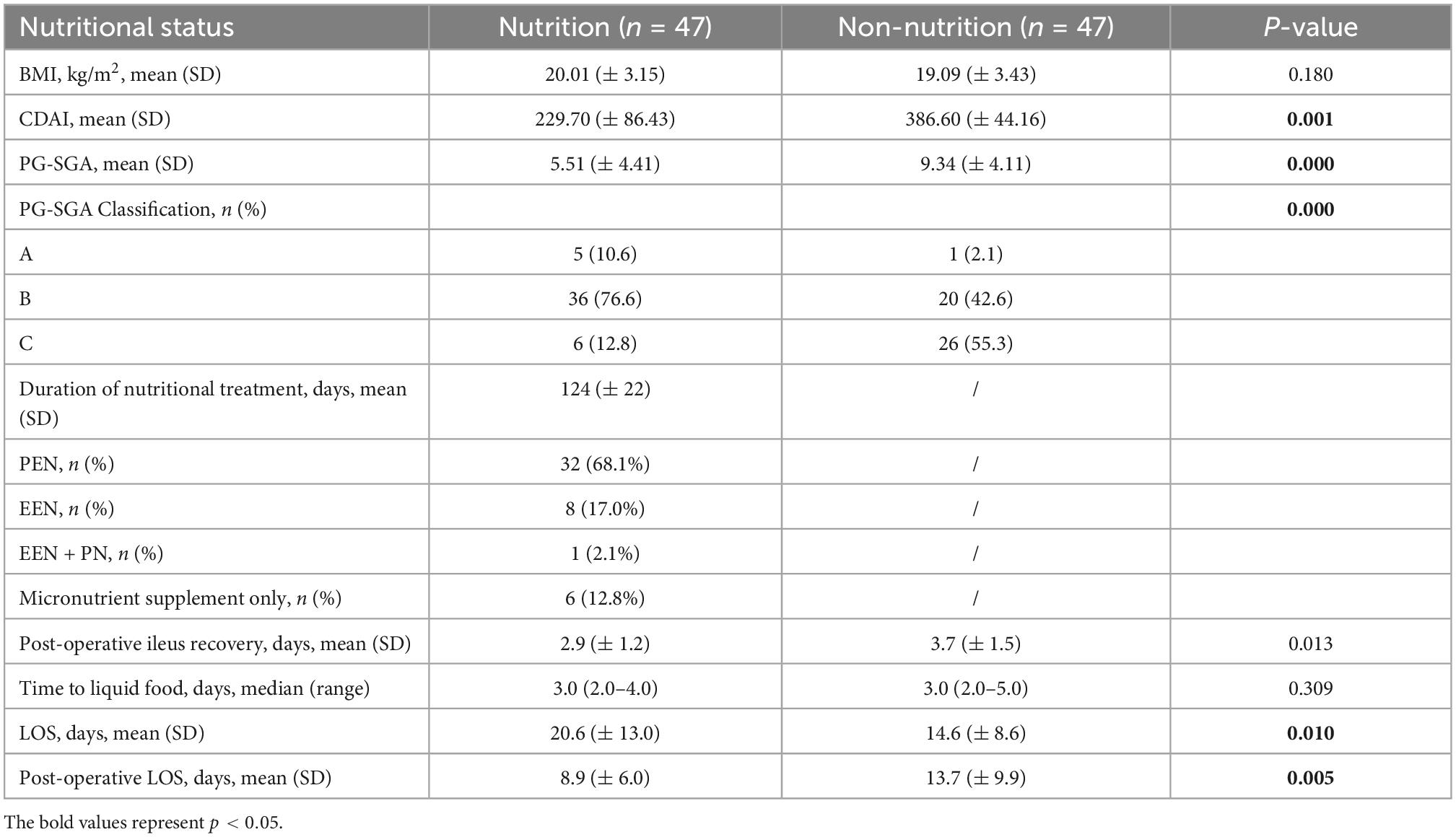
Table 3. Nutritional condition.
The proportion of laparoscopic surgery and emergency surgery was statistically significantly higher in the nutritional support group: 91.5 vs. 40.4% (p = 0.001), 7.4 vs. 31.9% (p < 0.0001), respectively. Fewer patients received staged surgery in the nutritional group [5 (10.7%) vs. 18 (38.3%) (p = 0.002)]. The proportion of patients who had resections and/or protective diversion are indicated in Table 4.
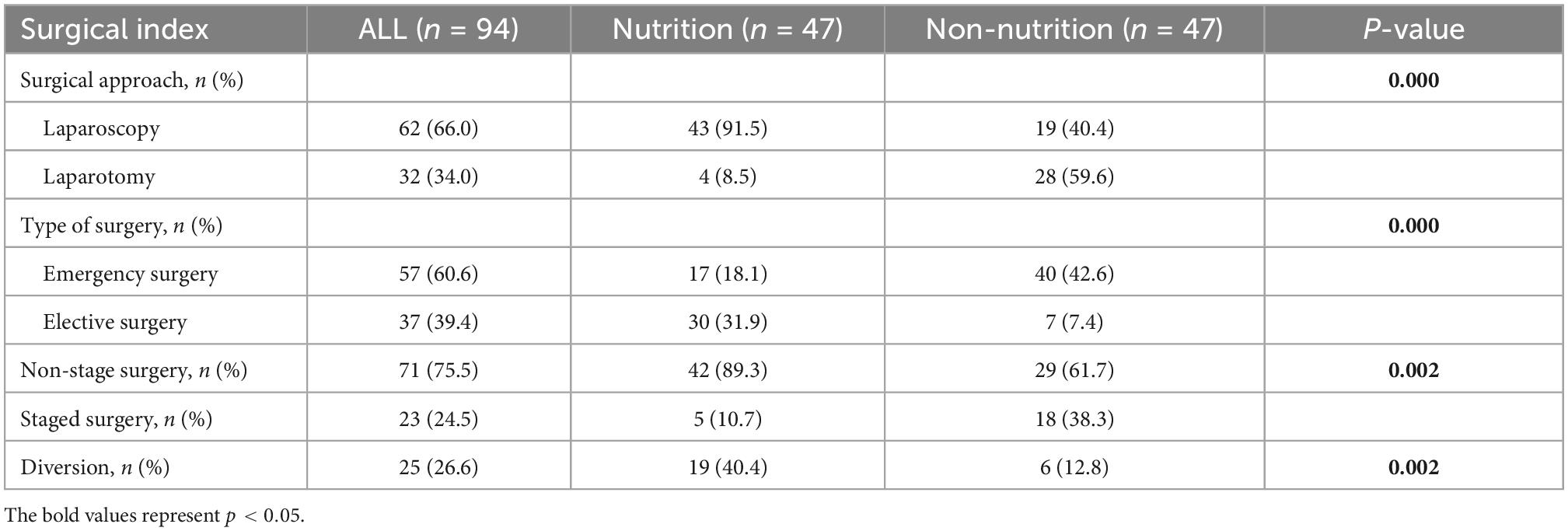
Table 4. Operative data.
No data were missing for the primary endpoint (CCI), complications, LOS, or rate of re-operation. Data regarding post-operative outcomes are presented in Table 4. A lower 30-day CCI score of nutritional group was found in the primary outcome measure (2.86 vs. 9.89, P = 0.015). Post-operative complications developed in 21 (22.3%) patients, 6 (12.8%) in the nutritional group and 15 (31.9%) in the non-nutritional group (p = 0.026). A total of 26 complication events were observed while 5 (19.2%) events of Clavien-Dindo I complications, 3 (11.5%) events of Clavien-Dindo II complications, 12 (46.2%) events of Clavien-Dindo IIIa complications, 2 (7.7%) events of Clavien-Dindo IIIb complications, and 4 (15.4%) events of Clavien-Dindo IVa complications. The common complications in our hospital were wound infection (19.2%), early post-operative bowel obstruction (19.2%), intra-abdominal abscess (19.2%), anastomotic leakage (11.5%), and excessive fluid losses of stoma (11.5%). Among all these post-operative complications, a lower incidence rate of intra-abdominal abscess (0 vs. 10.6%, P = 0.022) and excessive fluid losses of stoma (0 vs. 10.6%, P = 0.022) in nutritional group were mentioned. While no difference was observed between two groups of wound infection, early post-operative bowel obstruction, or anastomosis related complications (8.5 vs. 2.1%, P = 0.168, 6.4 vs. 8.5%, P = 0.694, 4.3 vs. 2.1%, P = 0.557, and 0.0 vs. 2.1%, P = 0.315, respectively) (Table 5). The number of multiple complication events for one patient in nutritional and non-nutritional group was 5 (10.6%) and 0 (0.0%), respectively (Table 5). Mean time of return of bowel movement, of total LOS, and of post-operative LOS were significantly fewer in the nutritional group with 2.94 ± 1.24 days, 14.62 ± 8.57 days, and 8.85 ± 6.04 days, vs. 3.67 ± 1.52 days, 20.62 ± 12.98 days, and 13.70 ± 9.90 days in the non-nutritional group (p = 0.013, 0.010, and 0.005, respectively) (Table 3).
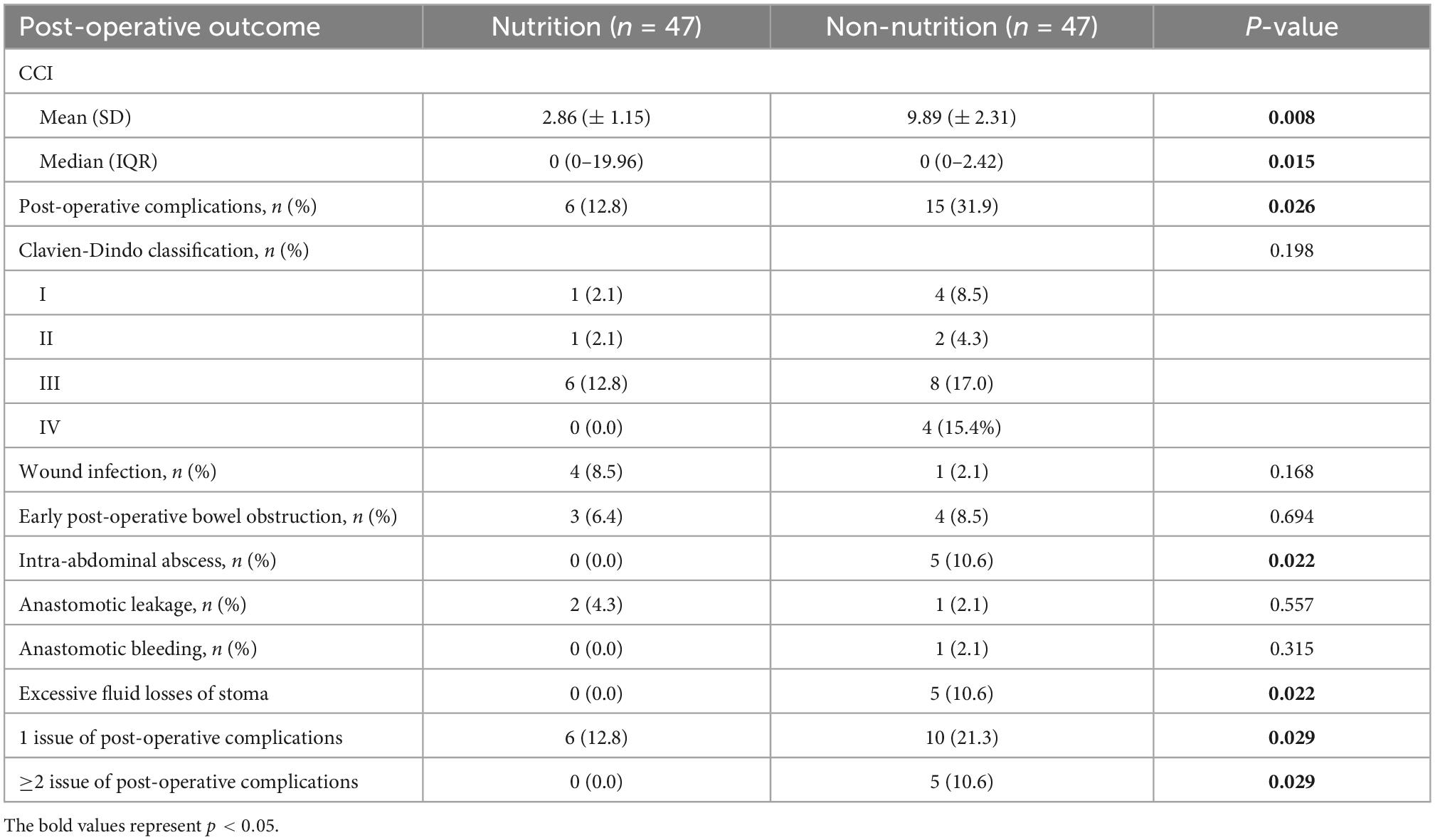
Table 5. Post-operative complications and perioperative characters.
Despite the advent of medicine, a huge step forward for patients with CD, leading to a rapid response and huge remission of disease. However, complications such as intestinal bleeding, intestinal obstruction, fistula, perforation, abscess still exist (5–7). In such kind of occasion, surgery is still the recommended treatment (7). Therefore, it is crucial to enhance the outcome by optimizing perioperative management. Pre-operative malnutrition has been shown to be associated with increased risk of post-operative complications and increased LOS after abdominal surgery (12, 23, 24). Factors such as nausea, vomiting, abdominal pain, and diarrhea reducing oral food intake contribute to malnutrition in CD patients (25, 26). Furthermore, medications such as glucocorticoids often reduce phosphorus, zinc, and calcium absorption and may lead to osteoporosis (17). Although several studies demonstrated improved disease activity and prolonged time to relapse following nutritional support (27, 28), the efficacy and protocol of nutritional support has not been fully clarified.
Consistent with previous findings, pre-operative nutritional optimization was recommended in CD patients with poor nutritional status to minimize post-operative complications (23, 29). In our study, patients with lower nutritional status and higher inflammatory level are related with post-operative complications in quantity and severity. Furthermore, the pre-operative nutritional status may also have impact on post-operative recovery of gastrointestinal function. Prolonged post-operative ileus and delay in recovery of the gastrointestinal function were commonly observed in non-nutritional group, leading to a longer LOS directly. Meanwhile, malnutrition will also increase the rate of emergency surgery, staged surgery, and diversion. The difference of surgical strategy was done for the reason leading to the surgical difficulty such as severe intra-abdominal adhesions, tissue edema, complete intestinal obstruction, or severe fistula, which indicates that successful pre-operative nutritional support could decrease the occurrence of complications during the course CD and reduce intra-abdominal inflammation.
In recent studies, diet appears to play an important role in disease pathogenesis (23, 24, 30, 31). Recent studies have shown that EEN can induce remission and mucosal healing (32, 33). So far, nutritional support, including dietary and EN is likely to play an important role during the treatment of CD. But few evidence support the effectiveness of EN. Furthermore, the evidence to support the interplay between nutritional status and post-operative complications is still lacking. Based on our results, a specific nutritional strategy may be able to play a pivotal role in improving immune-nutritional status and preventing post-operative complications of CD patients. The pre-operative EN was found to significantly improve the nutritional status scored by PG-SGA assessment and reduce the inflammatory response according to CDAI score. Meanwhile, improvements in level of serum albumin concentration, pre-albumin concentration, and TLC were also mentioned. The TLC indicates the immunological status of patient, which is also one of the important components of PNI score. Various studies have indicated that T lymphocytes affected by the systemic inflammatory response play an important role in the depression of innate cellular immunity of intestinal inflammation in cancer patients and found PNI an independent prognostic indicator in predicting post-operative complication (34, 35). Accompany with the significant decrease of inflammatory indicators such as WBC and CRP, our results indicated the beneficial effect of this new kind of comprehensive nutritional strategy in alleviating nutritional status and intestinal inflammation in CD patients.
Micronutrient status is also impacted by inflammatory severity and disease location, which may reduce surface area for absorption (36). The level of serum microelement may also be affected by some medicines (36). Weisshof et al. indicated that these micronutrients lead to deleterious downstream effects such as impaired immune response within the gut, and inflammation because of increased production of reactive oxygen species (37). In this study, we monitored important nutrients such as folate, 25-OH-vit D, calcium, potassium, magnesium, and phosphorus which were determined to be frequently suboptimal in patient with CD (38, 39). The statistic between two groups indicated that micronutrients supplementary play an important role in treatment of CD patients whose micronutrient intake from dietary was suboptimal.
This study is, to the best of our knowledge, the first study focusing on the application of EN on post-operative outcomes of CD patients. We used PSM for potential imbalances between groups, which confirmed the robustness of our conclusions. On account of CCI, we can quantify the post-operative complication more precisely with the application of such a comprehensive and sensitive measure. Regular follow-up consultation no longer than 3 or 6 months and weekly self-reporting was executed in our program since compliance is often limited for the strategy of dietary, EEN, PEN. In light of these design considerations, we believe that our results contribute new evidence for the role of nutritional support in CD patients who are candidates for surgical treatment.
Our result should be considered with some limitations. Groups were not balanced at baseline for age and ASA scores at first, however, our analyses were adjusted for these potential confounders. There was a considerable rate of missing data for PG-SGA score, CDAI index as a result of missing follow-up consultations. These missing data were handled with multiple imputation to reduce the risk of attrition bias. And the self-reporting database such as dietary compliance might be subject to reporting bias. Last but not least, this is a retrospective observational study which outcomes might be influenced by our local experience, a multi-center prospective study is excepted.
In conclusion, pre-operative nutritional status is correlated with post-operative outcomes while EN plays a positive role in preventing the post-operative complications. EN is a useful method for improving the pre-operative nutritional status and reducing the post-operative adverse events for CD patients undergoing surgery.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by the Ethics Committee of Shanghai Ruijin Hospital. The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
ZH, TJ, YJ, and QJ: conceptualization. TJ, YJ, and QJ: writing—original draft. ZH, MZ, AF, and YS: review and editing. SX: supervision. All authors read and agreed to the published version of the manuscript.
This research was supported by funding from the Shanghai Municipal Key Clinical Specially Fund (SHSLCZDZK102).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Torres J, Mehandru S, Colombel J-F, Peyrin-Biroulet L. Crohn’s disease. Lancet. (2017) 389:1741–55. doi: 10.1016/S0140-6736(16)31711-1
2. Dong X, Tang S, Liu W, Qi W, Ye L, Yang X, et al. Prognostic significance of the controlling nutritional status (Conut) score in predicting postoperative complications in patients with Crohn’s disease. Sci Rep. (2020) 10:19040. doi: 10.1038/s41598-020-76115-0
3. Mak WY, Zhao M, Ng SC, Burisch J. The epidemiology of inflammatory bowel disease: east meets west. J Gastroenterol Hepatol. (2020) 35:380–9. doi: 10.1111/jgh.14872
4. Regueiro M, Velayos F, Greer JB, Bougatsos C, Chou R, Sultan S, et al. American gastroenterological association institute technical review on the management of Crohn’s disease after surgical resection. Gastroenterology. (2017) 152:277–95.e3. doi: 10.1053/j.gastro.2016.10.039
5. Yamamoto T. Surgery for luminal Crohn’s disease. World J Gastroenterol. (2014) 20:78. doi: 10.3748/wjg.v20.i1.78
6. Alós R, Hinojosa J. Timing of surgery in Crohn’s disease: a key issue in the management. World J Gastroenterol. (2008) 14:5532. doi: 10.3748/wjg.14.5532
7. Adamina M, Bonovas S, Raine T, Spinelli A, Warusavitarne J, Armuzzi A, et al. ECCO guidelines on therapeutics in Crohn’s disease: surgical treatment. J Crohns Colitis. (2020) 14:155–68. doi: 10.1093/ecco-jcc/jjz187
8. Torres J, Bonovas S, Doherty G, Kucharzik T, Gisbert JP, Raine T, et al. ECCO guidelines on therapeutics in Crohn’s disease: medical treatment. J Crohns Colitis. (2020) 14:4–22. doi: 10.1093/ecco-jcc/jjz180
9. Svolos V, Hansen R, Nichols B, Quince C, Ijaz UZ, Papadopoulou RT, et al. Treatment of active Crohn’s disease with an ordinary food-based diet that replicates exclusive enteral nutrition. Gastroenterology. (2019) 156:1354–67.e6. doi: 10.1053/j.gastro.2018.12.002
10. Lee SH, Kwon JE, Cho M-L. Immunological pathogenesis of inflammatory bowel disease. Intest Res. (2018) 16:26–42. doi: 10.5217/ir.2018.16.1.26
11. Gold SL, Kohler D, Philippou A, Rabinowitz L, Manning L, Keefer L, et al. High prevalence of malnutrition and micronutrient deficiencies in patients with inflammatory bowel disease early in disease course. Inflamm Bowel Dis. (2022) doi: 10.1093/ibd/izac102 [Ebup ahead of print].
12. Maurício SF, Xiao J, Prado CM, Gonzalez MC, Correia MITD. Different nutritional assessment tools as predictors of postoperative complications in patients undergoing colorectal cancer resection. Clin Nutr. (2018) 37:1505–11. doi: 10.1016/j.clnu.2017.08.026
13. Paccagnella A, Morassutti I, Rosti G. Nutritional intervention for improving treatment tolerance in cancer patients. Curr Opin Oncol. (2011) 23:322–30. doi: 10.1097/CCO.0b013e3283479c66
14. Di Fiore A, Lecleire S, Gangloff A, Rigal O, Benyoucef A, Blondin V, et al. Impact of nutritional parameter variations during definitive chemoradiotherapy in locally advanced oesophageal cancer. Dig Liver Dis. (2014) 46:270–5. doi: 10.1016/j.dld.2013.10.016
15. Schwegler I, von Holzen A, Gutzwiller J-, Schlumpf R, Mühlebach S, Stanga Z. Nutritional risk is a clinical predictor of postoperative mortality and morbidity in surgery for colorectal cancer. Br J Surg. (2009) 97:92–7. doi: 10.1002/bjs.6805
16. Jouvin I, Lefevre JH, Creavin B, Pitel S, Chafai N, Tiret E, et al. Postoperative morbidity risks following ileocolic resection for Crohn’s disease treated with Anti-TNF alpha therapy: a retrospective study of 360 patients. Inflamm Bowel Dis. (2018) 24:422–32. doi: 10.1093/ibd/izx036
17. Balestrieri M, Ribolsi M, Guarino L, Emerenziani S, Altomare A, Cicala M. Nutritional aspects in inflammatory bowel diseases. Nutrients. (2020) 12:372. doi: 10.3390/nu12020372
18. Zittan E, Gralnek MI, Hatoum OA, Sakran N, Kolonimos N. Preoperative exclusive total parental nutrition is associated with clinical and laboratory remission in severe active Crohn’s disease—a pilot study. Nutrients. (2020) 12:1244. doi: 10.3390/nu12051244
19. Pan Y, Liu Y, Guo H, Jabir MS, Liu X, Cui W, et al. Associations between folate and vitamin B12 levels and inflammatory bowel disease: a meta-analysis. Nutrients. (2017) 9:382. doi: 10.3390/nu9040382
20. Inflammatory Bowel Disease Group, Chinese Society of Gastroenterology, Chinese Medical Association. Chinese consensus on diagnosis and treatment in inflammatory bowel disease (2018, Beijing). J Dig Dis. (2021) 22:298–317. doi: 10.1111/1751-2980.12994
21. Bischoff SC, Escher J, Hébuterne X, Kłęk S, Krznaric Z, Schneider S, et al. ESPEN practical guideline: clinical nutrition in inflammatory bowel disease. Clin Nutr. (2020) 39:632–53. doi: 10.1016/j.clnu.2019.11.002
22. Lambert K, Pappas D, Miglioretto C, Javadpour A, Reveley H, Frank L, et al. Systematic review with meta-analysis: dietary intake in adults with inflammatory bowel disease. Aliment Pharmacol Ther. (2021) 54:742–54. doi: 10.1111/apt.16549
23. Santarpia L, Alfonsi L, Castiglione F, Pagano MC, Cioffi I, Rispo A, et al. Nutritional rehabilitation in patients with malnutrition due to Crohn’s disease. Nutrients. (2019) 11:2947. doi: 10.3390/nu11122947
24. Carli F, Bousquet-Dion G, Awasthi R, Elsherbini N, Liberman S, Boutros M, et al. Effect of multimodal prehabilitation vs postoperative rehabilitation on 30-day postoperative complications for frail patients undergoing resection of colorectal cancer. JAMA Surg. (2020) 155:233. doi: 10.1001/jamasurg.2019.5474
25. Stein J, Connor S, Virgin G, Ong DEH, Pereyra L. Anemia and iron deficiency in gastrointestinal and liver conditions. World J. Gastroenterol. (2016) 22:7908. doi: 10.3748/wjg.v22.i35.7908
26. Cioffi I, Imperatore N, Di Vincenzo O, Santarpia L, Rispo A, Marra M, et al. Association between health-related quality of life and nutritional status in adult patients with Crohn’s disease. Nutrients. (2020) 12:746. doi: 10.3390/nu12030746
27. Knowles SR, Graff LA, Wilding H, Hewitt C, Keefer L, Mikocka-Walus A. Quality of life in inflammatory bowel disease: a systematic review and meta-analyses—part I. Inflamm Bowel Dis. (2018) 24:742–51. doi: 10.1093/ibd/izx100
28. Castiglione F, Imperatore N, Testa A, De Palma GD, Nardone OM, Pellegrini L, et al. One-year clinical outcomes with biologics in Crohn’s disease: transmural healing compared with mucosal or no healing. Aliment Pharmacol Ther. (2019) 49:1026–39. doi: 10.1111/apt.15190
29. Cioffi I, Imperatore N, Di Vincenzo O, Pagano MC, Santarpia L, Pellegrini L, et al. Evaluation of nutritional adequacy in adult patients with Crohn’s disease: a cross-sectional study. Eur J Nutr. (2020) 59:3647–58. doi: 10.1007/s00394-020-02198-0
30. Durchschein F, Petritsch W, Hammer HF. Diet therapy for inflammatory bowel diseases: the established and the new. World J Gastroenterol. (2016) 22:2179–94. doi: 10.3748/wjg.v22.i7.2179
31. Ferreira TMR, Albuquerque A, Cancela Penna FG, Macedo Rosa R, Correia MITD, Barbosa AJA, et al. Effect of oral nutrition supplements and TGF−β2 on nutrition and inflammatory patterns in patients with active Crohn’s disease. Nutr Clin Pract. (2020) 35:885–93. doi: 10.1002/ncp.10448
32. Li YC, Chen Y, Du J. Critical roles of intestinal epithelial vitamin D receptor signaling in controlling gut mucosal inflammation. J Steroid Biochem Mol Biol. (2015) 148:179–83. doi: 10.1016/j.jsbmb.2015.01.011
33. Yue B, Lu X, Yu Z, Mani S, Wang Z, Dou W. Inflammatory bowel disease: a potential result from the collusion between gut microbiota and mucosal immune system. Microorganisms. (2019) 7:440. doi: 10.3390/microorganisms7100440
34. Zhou W, Cao Q, Qi W, Xu Y, Liu W, Xiang J, et al. Prognostic nutritional index predicts short-term postoperative outcomes after bowel resection for Crohn’s disease. Nutr Clin Pract. (2017) 32:92–7. doi: 10.1177/0884533616661844
35. Ge X, Dai X, Ding C, Tian H, Yang J, Gong J, et al. Early postoperative decrease of serum albumin predicts surgical outcome in patients undergoing colorectal resection. Dis Colon Rectum. (2017) 60:326–34. doi: 10.1097/DCR.0000000000000750
36. Castro Aguilar-Tablada T, Navarro-Alarcón M, Quesada Granados J, Samaniego Sánchez C, Rufián-Henares J, Nogueras-Lopez F. Ulcerative colitis and Crohn’s disease are associated with decreased serum selenium concentrations and increased cardiovascular risk. Nutrients. (2016) 8:780. doi: 10.3390/nu8120780
37. Weisshof R, Chermesh I. Micronutrient deficiencies in inflammatory bowel disease. Curr Opin Clin Nutr Metab Care. (2015) 18:576–81. doi: 10.1097/MCO.0000000000000226
38. O’Sullivan M. Is vitamin D supplementation a viable treatment for Crohn’s disease? Expert Rev Gastroenterol Hepatol. (2016) 10:1–4. doi: 10.1586/17474124.2016.1120157
Keywords: Crohn’s disease, nutritional assessment, oral supplement, enteral nutrition, post-operative complications
Citation: Jiang T, Jiang Y, Jin Q, Xu S, Fingerhut A, Shi Y, Zheng M and He Z (2023) Role of perioperative nutritional status and enteral nutrition in predicting and preventing post-operative complications in patients with Crohn’s disease. Front. Nutr. 9:1085037. doi: 10.3389/fnut.2022.1085037
Received: 31 October 2022; Accepted: 15 December 2022;
Published: 06 January 2023.
Edited by:
Lilia Castillo-Martinez, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán (INCMNSZ), MexicoReviewed by:
José L. Villanueva-Juárez, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán (INCMNSZ), MexicoCopyright © 2023 Jiang, Jiang, Jin, Xu, Fingerhut, Shi, Zheng and He. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zirui He,  aGV6aXJ1aUBhbGl5dW4uY29t; Minhua Zheng, em1odGlnZXJAeWVhaC5uZXQ=; Yongmei Shi, c3ltMTA2NTlAcmpoLmNvbS5jbg==
aGV6aXJ1aUBhbGl5dW4uY29t; Minhua Zheng, em1odGlnZXJAeWVhaC5uZXQ=; Yongmei Shi, c3ltMTA2NTlAcmpoLmNvbS5jbg==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.