 Iván Antonio García-Montalvo
Iván Antonio García-Montalvo Diana Matías-Pérez
Diana Matías-Pérez- Division of Graduate Studies and Research, National Institute of Technology of Mexico/Technological Institute of Oaxaca, Oaxaca, Mexico
Introduction
Age-related macular degeneration (AMD) is considered the leading cause of irreversible blindness in people between 55 and 65 years of age, and its prevalence is expected to increase in developed and developing countries, in proportion to the existing geriatric population (1–4). Its evolution is due to a complex interaction between demographic, racial, age, genetic, and environmental factors, i.e., AMD is multifactorial. Age is the factor with the highest degree of association with this pathology, followed by smoking as a trigger for the release of free radicals that directly affect the retina. Frequent alcohol consumption leads to a deficient absorption of nutrients, mainly water-soluble vitamins. Other factors involved are poor or no antioxidant intake, obesity, hypertension, prolonged exposure to the sun, ethnicity, and family history (5). These visual disturbances have a great impact on the lifestyle of patients, compromising their daily activities (driving or reading difficulties) (5).
Age-related macular degeneration and carotenoids
AMD is considered a bilateral ocular pathology that damages the central part of the retina, called the macula lutea. It is responsible for photopic vision, which allows visualization of fine details and image resolution. The fovea is in the center of the macula lutea, where the photoreceptor cells are concentrated. Drusens are deposits of cellular debris and are the most common feature of this disease along with the development of choroidal neovascularization (6, 7).
Abnormalities present in photoreceptors, Brunch's membrane, pigment epithelium, and choroid result in neovascularization and geographic atrophy (8). According to the fundoscopic abnormalities observed, they can be classified into two general phenotypes: wet (exudative), and dry (atrophic) (8, 9). The dry phenotype (geographic atrophy) is characterized by progressive obstruction of the drusen, which causes thinning of the pigment epithelium and prevents proper oxygen transport to photoreceptors (10). The wet phenotype can be divided into choroidal neovascularization and polypoidal choroidal vasculopathy, which may involve blood or serum leakage. There are cases in which there is an evolution from dry to wet phenotype (11–13). As mentioned above, dietary habits have been identified as risk factors involved in the origin or development of diseases but can be susceptible to modification. It is important to include foods with antioxidant properties in the regular diet to reduce the constant flow of oxidizing molecules that lead to the development of various maculopathies, including AMD (14). Some risk or pathophysiological aspects to consider in this pathology are stimulation of the complement system, loss of homeostasis between pro-inflammatory and anti-inflammatory factors, activation of microglia and genetic susceptibility (15, 16). It should be considered that the retina has an oxygen rich environment, in addition to prolonged exposure to light, leading to the continuous production of free radicals (17). To reduce this damage to the retinal epithelium, there are enzymatic mechanisms that maintain homeostasis (18). Due to aging, the retina has a weakened antioxidant system, making it susceptible to oxidation, manifesting itself as hard exudates in the periphery, thickening of Brunch's membrane, and thinning of the choriocapillaris (15). Nutritional intervention through the consumption of antioxidants, polyunsaturated fatty acids of plant and animal origin, carotenoids (lutein and zeaxanthin), and minerals has been shown to be effective in preventing or delaying the progression of AMD due to its involvement in decreasing inflammatory and oxidative events (19, 20). Among the main carotenoids that have demonstrated functionality in reducing AMD (see Table 1) are lutein, zeaxanthin, beta-carotene, crocin, and crocetin. Lutein/zeaxanthin supplementation improves visual performance, including glare tolerance, contrast sensitivity, and recovery from photostress (21–25). Crocin and crocetin are used as antiischemic, hypolipidemic, antihypertensive, anxiolytic, antidiabetic, antidepressant, anticancer, and cardioprotective agents (26–35). Antioxidants are used due to their ability to decrease/eliminate anti-inflammatory activity through the release of pro-inflammatory cytokines by glial cells, as well as regulation in inflammatory pathways (28).
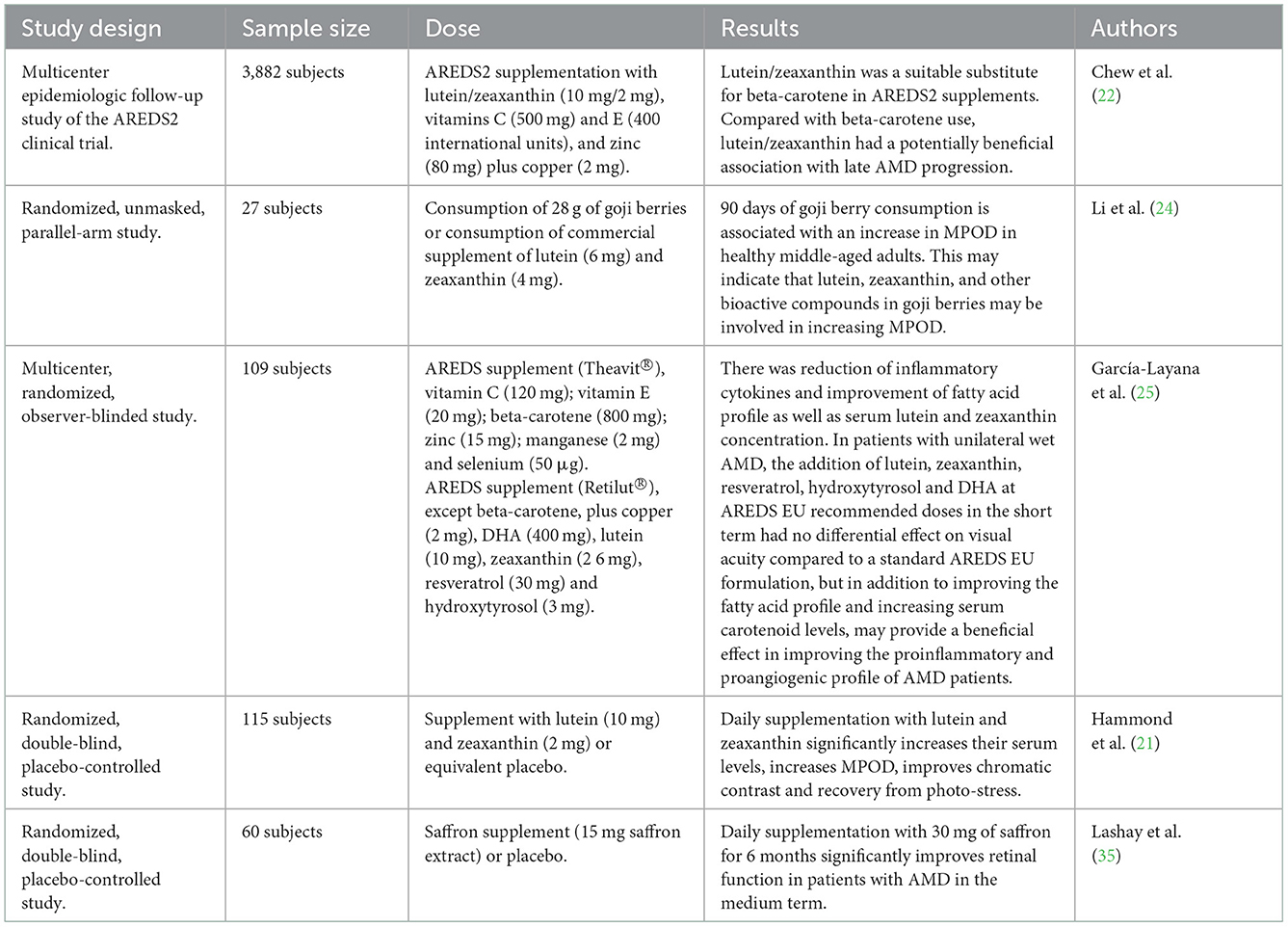
Table 1. Clinical trials on the treatment of AMD and carotenoid consumption.
Discussion
The lutein and zeaxanthin present in the retina is more abundant than in any other type of human tissue, however, their distribution is not uniform. In the fovea, the concentration of lutein is lower than that of zeaxanthin (1:2 ratio) (36–38) and decrease as they approach the ocular periphery. The generated production of reactive oxygen species (ROS) through extramitochondrial oxidative phosphorylation in the outer segment of rods (39, 40) leads to the release of compounds such as cytochrome c, which results in the mechanism of photoreceptor apoptosis (activation of caspase 9). The main function of lutein in the retina is to scavenge free radicals, due to its chemical structure in which there are two hydroxyl groups that are mainly responsible for trapping ROS (41–43). Xanthophylls and carotenes are the most effective oxygen regulators of the carotenoid family due to the double bonds present in their structures that facilitate the reduction of their energy state (36). Oxidative stress is caused by an imbalance between the two reactive species (ROS and RNS). These reactive species are a fundamental part of innate immunity that protects cells from infections and, unfortunately, contribute to the pathogenesis of degenerative diseases such as AMD. Under physiological conditions, the eye is sensitive to this type of stress due to the rich content of polyunsaturated lipids present in cell membranes and exposure to pro-oxidant agents.
We believe that the consumption of carotenoids provides benefits in the progressive improvement of AMD due to the antioxidant power they possess. Lutein and zeaxanthin can absorb specific wavelengths of light (490–495 nm) which helps in protecting the eyes. In addition to the fact that carotenoids may provide protection against certain types of cancer by limiting abnormal cell growth and improving communication between functional spaces, carotenoids may prevent heart disease by blocking the formation and oxidation of low-density lipoproteins. Ocular carotenoids (mesozeaxanthin, zeaxanthin and lutein isomers) are concentrated in the macula and fovea. Increasing their daily intake would provide benefits to ocular health, as carotenoids have several functions in the retina, such as protection against photochemical injury, ROS neutralizing capacity and protection against UV-induced peroxidation and reduction of lipofuscin formation. Despite the dosage trials that have been carried out and the results obtained, there are still gaps to be filled, considering the results of the trials consulted we can indicate that the intake of supplements with lutein/zeaxanthin content (10 mg/2 mg per day) is recommended over those supplements with beta-carotene, since the excessive use of beta-carotene is associated with the risk of lung cancer. Such is the case of the establishment of reference values by gender, age, and ethnicity worldwide, as well as the reclassification of these carotenoids, which should be considered as conditionally essential nutrients. This is the case of resveratrol present in grape seed oil and alpha-lipoic acid, which have been shown to be effective in reducing the loss of retinal ganglion cells and inhibiting the destructive processes that accompany them, with the aim of delaying degenerative eye diseases. We hope that the advancement and development of future research in this area can be considered as a contribution to global public health as we face a continuously increasing geriatric population.
Author contributions
IG-M, DM-P, EH-B, and EP-C participated in the design, structuring, and revision of the manuscript. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Di Carlo E, Augustin AJ. Prevention of the onset of age-related macular degeneration. J Clin Med. (2021) 10:3297. doi: 10.3390/jcm10153297
2. Jager RD, Mieler WF, Miller JW. Age-related macular degeneration. N Engl J Med. (2008) 358:2606–17. doi: 10.1056/NEJMra0801537
3. Edo A, Pertiwi YD, Hirooka K, Masuda S, Kamaruddin MI, Yanagi M, et al. Association of dietary nutrient intake with early age-related macular degeneration in Japanese-Americans. Metabolites. (2021) 11:673. doi: 10.3390/metabo11100673
4. Ke KM. The direct, indirect and intangible costs of visual impairment caused by neovascular age-related macular degeneration. Eur J Health Econ. (2010) 11:525–31. doi: 10.1007/s10198-009-0207-9
5. Lim LS, Mitchell P, Seddon JM, Holz FG, Wong TY. Age-related macular degeneration. Lancet. (2012) 379:1728–38. doi: 10.1016/S0140-6736(12)60282-7
6. Mullins RF, Russell SR, Anderson DH, Hageman GS. Drusen associated with aging and age-related macular degeneration contain proteins common to extracellular deposits associated with atherosclerosis, elastosis, amyloidosis, and dense deposit disease. FASEB J. (2000) 14:835–46. doi: 10.1096/fasebj.14.7.835
7. Stahl A. The diagnosis and treatment of age-related macular degeneration. Dtsch Arztebl Int. (2020) 117:513–20. doi: 10.3238/arztebl.2020.0513
8. Thomas CJ, Mirza RG, Gill MK. Age-related macular degeneration. Med Clin North Am. (2021) 105:473–91. doi: 10.1016/j.mcna.2021.01.003
10. Fritsche LG, Fariss RN, Stambolian D, Abecasis GR, Curcio CA, Swaroop A. Age-related macular degeneration: genetics and biology coming together. Annu Rev Genomics Hum Genet. (2014) 15:151–71. doi: 10.1146/annurev-genom-090413-025610
11. Klein R, Klein BE, Tomany SC, Meuer SM, Huang GH. Ten-year incidence and progression of age-related maculopathy: The Beaver Dam eye study. Ophthalmology. (2002) 109:1767–79. doi: 10.1016/S0161-6420(02)01146-6
12. Algvere PV, Seregard S. Drusen maculopathy: a risk factor for AMD Can we prevent visual loss? Acta Ophthalmol Scand. (2003) 81:427–9. doi: 10.1034/j.1600-0420.2003.00157.x
13. Friberg TR, Bilonick RA, Brennen PM. Risk factors for conversion to neovascular age-related macular degeneration based on longitudinal morphologic and visual acuity data. Ophthalmology. (2012) 119:1432–37. doi: 10.1016/j.ophtha.2012.02.048
14. Sin HP, Liu DT, Lam DS. Lifestyle modification, nutritional and vitamins supplements for age-related macular degeneration. Acta Ophthalmol. (2013) 91:6–11. doi: 10.1111/j.1755-3768.2011.02357.x
15. Jarrett SG, Boulton ME. Consequences of oxidative stress in age-related macular degeneration. Mol Aspects Med. (2012) 33:399–417. doi: 10.1016/j.mam.2012.03.009
16. Ardeljan D, Chan CC. Aging is not a disease: distinguishing age-related macular degeneration from aging. Prog Retin Eye Res. (2013) 37:68–89. doi: 10.1016/j.preteyeres.2013.07.003
17. Álvarez-Barrios A, Álvarez L, García M, Artime E, Pereiro R, González-Iglesias H. Antioxidant defenses in the human eye: a focus on metallothioneins. Antioxidants (Basel). (2021) 10:89. doi: 10.3390/antiox10010089
18. Taurone S, Ralli M, Artico M, Madia VN, Scarpa S, Nottola SA, et al. Oxidative stress and visual system: a review. EXCLI J. (2022) 21:544–53. doi: 10.17179/excli2022-4663
19. Zampatti S, Ricci F, Cusumano A, Marsella LT, Novelli G, Giardina E. Review of nutrient actions on age-related macular degeneration. Nutr Res. (2014) 34:95–105. doi: 10.1016/j.nutres.2013.10.011
20. Köpcke W, Krutmann J. Protection from sunburn with beta-Carotene—a meta-analysis. Photochem Photobiol. (2008) 84:284–8. doi: 10.1111/j.1751-1097.2007.00253.x
21. Hammond BR, Fletcher LM, Roos F, Wittwer J, Schalch W, A. double-blind, placebo-controlled study on the effects of lutein and zeaxanthin on photostress recovery, glare disability, and chromatic contrast. Invest Ophthalmol Vis Sci. (2014) 55:8583–9. doi: 10.1167/iovs.14-15573
22. Chew EY, Clemons TE, Agrón E, Domalpally A, Keenan TDL, Vitale S, et al. AREDS2 Research Group. Long-term Outcomes of Adding Lutein/Zeaxanthin and ω-3 Fatty Acids to the AREDS Supplements on Age-Related Macular Degeneration Progression: AREDS2 Report 28. JAMA Ophthalmol. (2022) 140:692–8. doi: 10.1001/jamaophthalmol.2022.1640
23. Agrón E, Mares J, Clemons TE, Swaroop A, Chew EY, Keenan TDL. AREDS and AREDS2 Research Groups. Dietary nutrient intake and progression to late age-related macular degeneration in the age-related eye disease studies 1 and 2. Ophthalmology. (2021) 128:425–42. doi: 10.1016/j.ophtha.2020.08.018
24. Li X, Holt RR, Keen CL, Morse LS, Yiu G, Hackman RM. Goji berry intake increases macular pigment optical density in healthy adults: a randomized pilot trial. Nutrients. (2021) 13:4409. doi: 10.3390/nu13124409
25. García-Layana A, Recalde S, Hernandez M, Abraldes MJ, Nascimento J, Hernández-Galilea E, et al. Randomized study of nutritional supplementation in patients with unilateral wet age-related macular degeneration. Nutrients. (2021) 13:1253. doi: 10.3390/nu13041253
26. Xi L, Qian Z, Du P, Fu J. Pharmacokinetic properties of crocin (crocetin digentiobiose ester) following oral administration in rats. Phytomedicine. (2007) 14:633–6. doi: 10.1016/j.phymed.2006.11.028
27. Hosseini A, Razavi BM, Hosseinzadeh H. Pharmacokinetic properties of saffron and its active components. Eur J Drug Metab Pharmacokinet. (2018) 43:383–90. doi: 10.1007/s13318-017-0449-3
28. Ghaffari S, Roshanravan N. Saffron; An updated review on biological properties with special focus on cardiovascular effects. Biomed Pharmacother. (2019) 109:21–7. doi: 10.1016/j.biopha.2018.10.031
29. Fernández-Albarral JA, de Hoz R, Ramírez AI, López-Cuenca I, Salobrar-García E, Pinazo-Durán MD, et al. Beneficial effects of saffron (Crocus sativus L.) in ocular pathologies, particularly neurodegenerative retinal diseases. Neural Regen Res. (2020) 15:1408–16. doi: 10.4103/1673-5374.274325
30. Assimopoulou AN, Sinakos Z, Papageorgiou VP. Radical scavenging activity of Crocus sativus L. extract and its bioactive constituents. Phytother Res. (2005) 19:997–1000. doi: 10.1002/ptr.1749
31. Zeinali M, Zirak MR, Rezaee SA, Karimi G, Hosseinzadeh H. Immunoregulatory and anti-inflammatory properties of Crocus sativus (Saffron) and its main active constituents: a review. Iran J Basic Med Sci. (2019) 22:334–44. doi: 10.22038/ijbms.2019.34365.8158
32. Falsini B, Piccardi M, Minnella A, Savastano C, Capoluongo E, Fadda A, et al. Influence of saffron supplementation on retinal flicker sensitivity in early age-related macular degeneration. Invest Ophthalmol Vis Sci. (2010) 51:6118–24. doi: 10.1167/iovs.09-4995
33. Piccardi M, Marangoni D, Minnella AM, Savastano MC, Valentini P, Ambrosio L, et al. longitudinal follow-up study of saffron supplementation in early age-related macular degeneration: sustained benefits to central retinal function. Evid Based Complement Alternat Med. (2012) 2012:429124. doi: 10.1155/2012/429124
34. Marangoni D, Falsini B, Piccardi M, Ambrosio L, Minnella AM, Savastano MC, et al. Functional effect of Saffron supplementation and risk genotypes in early age-related macular degeneration: a preliminary report. J Transl Med. (2013) 11:228. doi: 10.1186/1479-5876-11-228
35. Lashay A, Sadough G, Ashrafi E, Lashay M, Movassat M, Akhondzadeh S. Short-term outcomes of saffron supplementation in patients with age-related macular degeneration: a double-blind, placebo-controlled, randomized trial. Med Hypothesis Discov Innov Ophthalmol. (2016) 5:32–8.
36. Koushan K, Rusovici R, Li W, Ferguson LR, Chalam KV. The role of lutein in eye-related disease. Nutrients. (2013) 5:1823–39. doi: 10.3390/nu5051823
37. Trieschmann M, Spital G, Lommatzsch A, van Kuijk E, Fitzke F, Bird AC, et al. Macular pigment: quantitative analysis on autofluorescence images. Graefes Arch Clin Exp Ophthalmol. (2003) 241:1006–12. doi: 10.1007/s00417-003-0796-4
38. Nolan JM, Kenny R, O'Regan C, Cronin H, Loughman J, Connolly EE, et al. Macular pigment optical density in an ageing Irish population: the Irish longitudinal study on ageing. Ophthalmic Res. (2010) 44:131–9. doi: 10.1159/000315531
39. Panfoli I, Calzia D, Ravera S, Morelli AM, Traverso CE. Extra-mitochondrial aerobic metabolism in retinal rod outer segments: new perspectives in retinopathies. Med Hypotheses. (2012) 78:423–7. doi: 10.1016/j.mehy.2011.12.012
40. Panfoli I, Calzia D, Ravera S, Bruschi M, Tacchetti C, Candiani S, et al. Extramitochondrial tricarboxylic acid cycle in retinal rod outer segments. Biochimie. (2011) 93:1565–75. doi: 10.1016/j.biochi.2011.05.020
41. Bone RA, Landrum JT. Macular pigment in Henle fiber membranes: a model for Haidinger's brushes. Vision Res. (1984) 24:103–8. doi: 10.1016/0042-6989(84)90094-4
42. Landrum J, Bone R, Mendez V, Valenciaga A, Babino D. Comparison of dietary supplementation with lutein diacetate and lutein: a pilot study of the effects on serum and macular pigment. Acta Biochim Pol. (2012) 59:167–9. doi: 10.18388/abp.2012_2198
Keywords: carotenoids, age-related macular degeneration (AMD), dietary habits, stress oxidative, lifestyle
Citation: García-Montalvo IA, Matías-Pérez D, Hernández-Bautista E and Pérez-Campos E (2023) Inclusion of carotenoids in dietary habits as an alternative to prevent age-related macular degeneration. Front. Nutr. 9:1063517. doi: 10.3389/fnut.2022.1063517
Received: 07 October 2022; Accepted: 14 December 2022;
Published: 09 January 2023.
Edited by:
Hock Eng Khoo, Guilin University of Technology, ChinaReviewed by:
Shi-Hui Cheng, University of Nottingham Malaysia Campus, MalaysiaCeren Gezer, Eastern Mediterranean University, Turkey
Copyright © 2023 García-Montalvo, Matías-Pérez, Hernández-Bautista and Pérez-Campos. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Iván Antonio García-Montalvo,  aXZhbi5nYXJjaWEmI3gwMDA0MDtpdG9heGFjYS5lZHUubXg=
aXZhbi5nYXJjaWEmI3gwMDA0MDtpdG9heGFjYS5lZHUubXg=