
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Nutr. , 08 December 2022
Sec. Clinical Nutrition
Volume 9 - 2022 | https://doi.org/10.3389/fnut.2022.1037842
 Magdalena P. Cardelo1,2
Magdalena P. Cardelo1,2 Andreea Corina1,2Ana Leon-Acuña1,2Gracia M. Quintana-Navarro1,2Juan F. Alcala-Diaz1,2Oriol Alberto Rangel-Zuñiga1,2
Andreea Corina1,2Ana Leon-Acuña1,2Gracia M. Quintana-Navarro1,2Juan F. Alcala-Diaz1,2Oriol Alberto Rangel-Zuñiga1,2 Antonio Camargo1,2
Antonio Camargo1,2 Cristina Conde-Gavilan3Claudia Carmona-Medialdea3Juan A. Vallejo-Casas4Elvira Carmona-Asenjo4Juan J. Ochoa-Sepulveda3
Cristina Conde-Gavilan3Claudia Carmona-Medialdea3Juan A. Vallejo-Casas4Elvira Carmona-Asenjo4Juan J. Ochoa-Sepulveda3 Eduardo Aguera-Morales3
Eduardo Aguera-Morales3 Javier Delgado-Lista1,2
Javier Delgado-Lista1,2 Niki Katsiki5,6José Lopez-Miranda1,2Francisco Perez-Jimenez1,2
Niki Katsiki5,6José Lopez-Miranda1,2Francisco Perez-Jimenez1,2 Elena M. Yubero-Serrano1,2†
Elena M. Yubero-Serrano1,2† Pablo Perez-Martínez1,2*†
Pablo Perez-Martínez1,2*†Introduction: Mild cognitive impairment (MCI) can progress to Alzheimer’s disease (AD). When MCI is not properly controlled, the speed of deterioration can dramatically increase. Reduction of oxidative stress/inflammation and the modulation of the gut-brain axis could be new potential therapeutic targets for the prevention and treatment of AD. Consumption of specific nutrients, diets and probiotic supplementation have been evaluated for neurodegenerative disorders. We focus on a detailed description of the study methods and baseline characteristics of a clinical trial aiming to evaluate the efficacy of a combined nutritional intervention, i.e., a Mediterranean diet with probiotics, on cognitive capacity in a population with MCI.
Methods: In this randomized, latin-square crossover, double-blind, and controlled dietary intervention trial (clinicaltrials.gov NCT05029765), 47 MCI patients were randomized to consume three dietary interventions for 24-weeks each: (1) A Mediterranean diet supplemented with probiotics (109 colony-forming units of Lactobacillus rhamnosus and Bifidobacterium longum); (2) A Mediterranean diet + placebo; and (3) A Healthy diet according to the World Health Organization (WHO) recommendations. Participants will be evaluated before and after each of the three intervention periods (each 24-weeks, with a total of 72-weeks) for adherence to the assigned diet, blood tests, cognitive performance, gut microbiota analysis and functional neuroimaging studies.
Results: Fifty patients, ≥60 years-old and diagnosed with MCI, underwent randomization. A total of 47 patients completed follow-up dietary interventions (57.4% males), with a good glycemic control (HbA1c 5.8 ± 0.1%, fasting glucose and insulin 99.7 ± 3.3 mg/dL and 10.4 ± 0.9 mU/L, respectively), elevated systolic blood pressure (136.9 ± 2.1 mmHg) and increased degree of inflammation (high-sensitivity C-reactive protein, 8.8 ± 0.9 mg/dL). Baseline adherence to the Mediterranean diet was medium (7.5 ± 0.3 points on the score that ranged from 0 to 14 points).
Conclusion: The results of this clinical study would provide more evidence on the need for dietary therapeutic strategies, for clinical and individual practice, in the management of MCI patients to reduce the risk of AD development. Targeting lifestyle modifications in high-risk populations could prevent substantial cases of cognitive decline.
Clinical trial registration: [ClinicalTrials.gov], identifier [NCT05029765].
Mild cognitive impairment (MCI) is usually defined as a transitional state between normal cognition and dementia (1). This prodromic state, which can often go undiagnosed, is characterized by a decline in cognitive function with a relatively intact daily living and social performance (2, 3). When this symptomatology is not properly controlled, the speed of deterioration can dramatically increase, progressing to dementia. The annual MCI progression rate to Alzheimer’s disease (AD), the most common cause of dementia (4), varies from 8.1% in clinical and 6.8% in community settings (5), suggesting that a large proportion of MCI patients do not progress to AD and may revert to normal cognition. Therefore, there is a need to establish preventive and effective strategies that may modulate MCI progression and reduce AD incidence.
The pathophysiological processes of the AD begin a decade or more before the clinical signs of the disease are detectable (6, 7). Accumulation of extracellular β-amyloid A plaques, intra-neuronal neurofibrillary tau tangles, neuronal and synaptic loss, neuro-inflammation and oxidative stress are the major neuropathological hallmarks of this disease (8–10). Moreover, recent evidence supports an interconnection between the gastrointestinal tract and the brain (the gut-brain axis), suggesting that alteration in the composition of the gut microbiota may also contribute to AD development, thus representing a potential therapeutic target for the prevention and treatment of AD (11, 12).
The failure of different clinical trials with candidate drugs to treat AD has refocused attention on the potential of lifestyle interventions in pre-symptomatic but high-risk individuals, such as in the case of MCI patients, to delay or prevent AD progression (13–15). Although several studies evaluated single nutrients and foods (16–18), the study of overall dietary patterns may provide a more powerful tool for assessing dietary habits, as well as the synergistic and cumulative effects of specific nutrients against these diseases. Results from recent clinical studies suggest that the adherence to a Mediterranean diet, characterized by high consumption of vegetables, fruits, legumes, nuts, wholes grains, olive oil (virgin or extra-virgin olive oil –VOO and EVOO, respectively) as the main fat (monounsaturated –MUFA fat) source, could be related to a reduced risk of developing chronic diseases as cognitive impairment and dementia (19–24). On the other hand, efficacy of probiotics administration, such as Bifidobacterium and Lactobacillus strains, have been evaluated for neurodegenerative disorders (25–27).
Considering all the above, the main aim of this trial is to evaluate the efficacy of a combined nutritional intervention, i.e., a Mediterranean diet rich in EVOO, supplemented with probiotics (109 colony-forming units of Lactobacillus rhamnosus and Bifidobacterium longum), on cognitive capacity, measured by Alzheimer’s disease Assessment Scale-Cognitive (ADAs-Cog-11) (28) in a population with MCI, as a therapeutic strategy to prevent AD progression, based on the paradigm that changes in the gut microbiota induce biological mechanisms on the gut-brain-axis. The effect of this combined nutritional intervention will be compared with both the same Mediterranean diet without supplemented probiotics and a World Health Organization (WHO) diet (as a control diet).
In this report, we focus on a detailed description and analysis of the study methodology, including the dietary intervention, study participant selection, recruitment, and adherence strategies, so that these may be applied to future trials.
This clinical study is a randomized, latin-square crossover, double-blind, and controlled dietary intervention trial performed in MCI patients, with an intention-to-treat analysis. The study was conducted at the Maimónides Biomedical Research Institute of Cordoba (IMIBIC, for its initials in Spanish) and the Reina Sofía University Hospital, where the screening, selection and recruitment of the patients who participated in the study were carried out. The study was registered at ClinicalTrials.gov (number NCT05029765). The study protocol was approved by the Human Investigation Review Committee of the Reina Sofía University Hospital, according to institutional and Good Clinical Practice guidelines.
The sample size was calculated based on the following assumptions: for the main outcome variable of the study (i.e., an improvement on the ADAS-Cog-11), a change of 20% from the baseline test was considered as significant (29); alpha risk: 0.05; difference in percentage between comparisons of 20%; power (1-ß):0.90; estimated losses: 10%; two-tailed contrast. Based on these premises, 41 patients were needed. With the aim of minimizing possible losses and increasing the study’s power, a total of 50 participants were included.
The inclusion and exclusion criteria of diagnosed MCI patients are detailed in Table 1. To sum up, patients were eligible if they were ≥60 years-old and had:
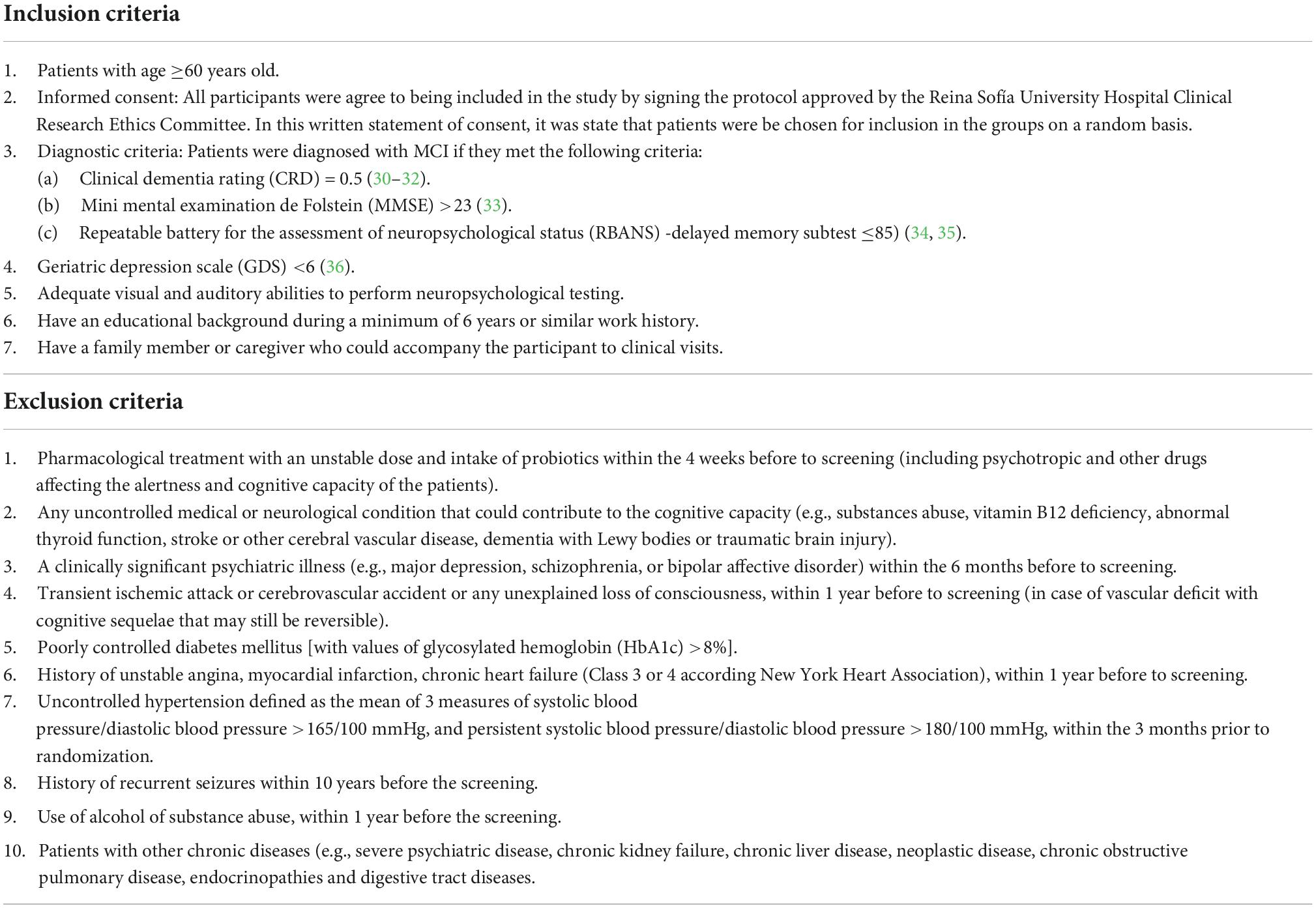
Table 1. Inclusion and exclusion criteria of study patients.
• Clinical Dementia Rating (CDR) scale score = 0.5 (30–32).
• Mini Mental Examination de Folstein (MMSE) >23 (33).
• Repeatable Battery for the Assessment of Neuropsychological Status (RBANS)-delayed memory subtest ≤85 (34, 35).
• Geriatric Depression Scale score of <6 (confirming lack of mild or major depression) (36).
• Adequate visual and auditory abilities to carry out neuropsychological tests, a minimum educational background and a family member or caregiver who could accompany the participant to clinical visits.
The screening, selection and recruitment processes were carried out by internists and neuropsychologists between January 2017 and September 2018 (Figure 1). Initially, out of 189 potentially eligible candidates, 166 were screened. From these patients, 116 were excluded (76 did not meet inclusion criteria and 40 declined participation). Finally, 50 patients, ≥60 years-old and diagnosed with MCI, underwent randomization. A total of 47 patients completed follow-up dietary intervention (three abandoned the dietary intervention and denied their permission to be followed up by electronic health record or phone calls, and therefore were censored at that point). All the patients gave their written informed consent to participate in the study.
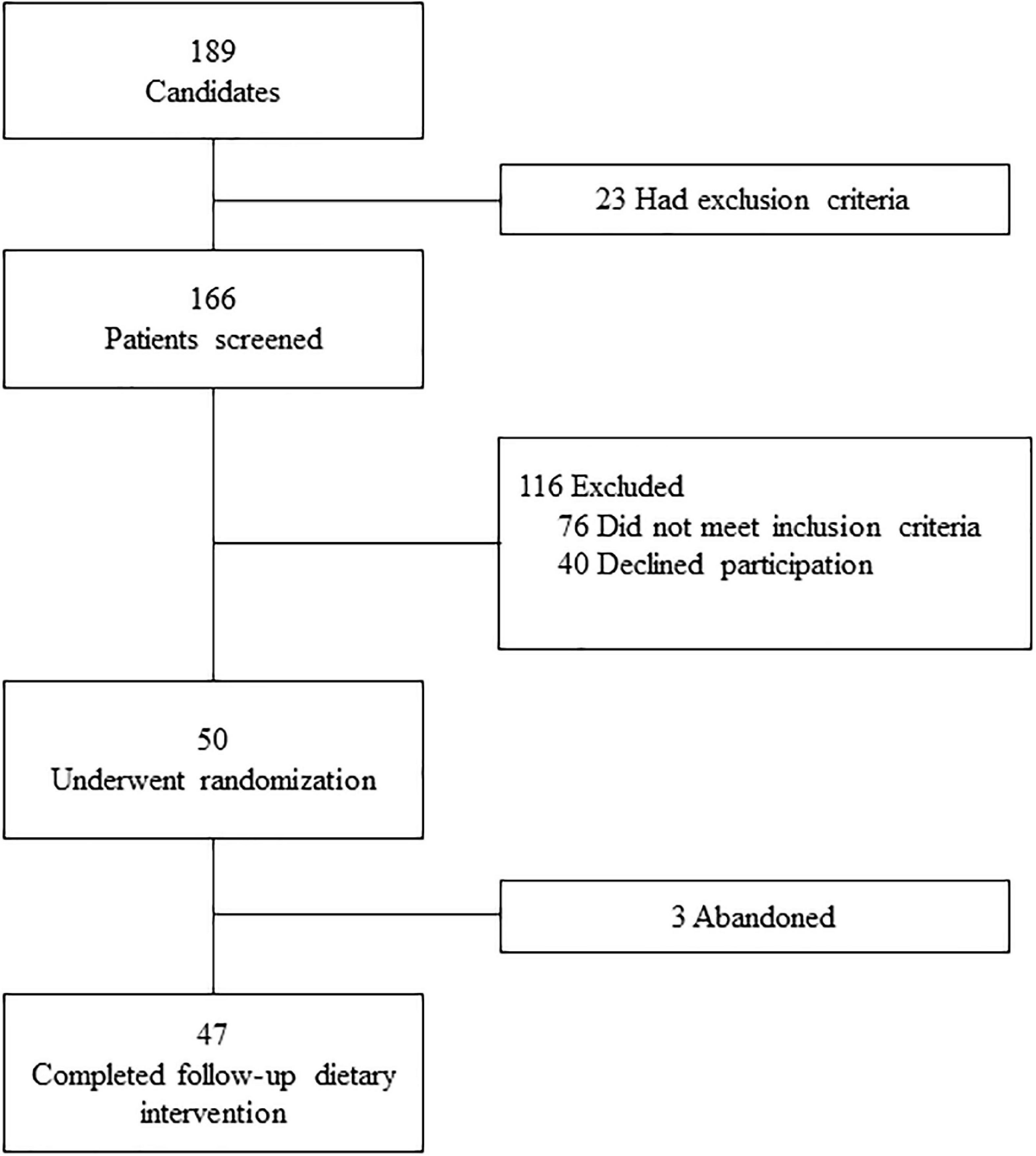
Figure 1. Screening, selection and recruitment flow-chart of patients for the study.
Participants enrolled in the study were randomly assigned, by a computerized random sequence generator, to consume three dietary interventions, for 24-weeks each, with a dietary follow-up period of 72-weeks as a total (Figure 2): (1) A Mediterranean diet supplemented with probiotics [109 colony-forming units of Lactobacillus rhamnosus CECT8361 and Bifidobacterium longum CECT737 -Biopolis-MIX42 (ADM Biopolis, Paterna, Valencia, Spain)]; (2) A Mediterranean diet + placebo; and (3) A Healthy diet according to WHO recommendations.
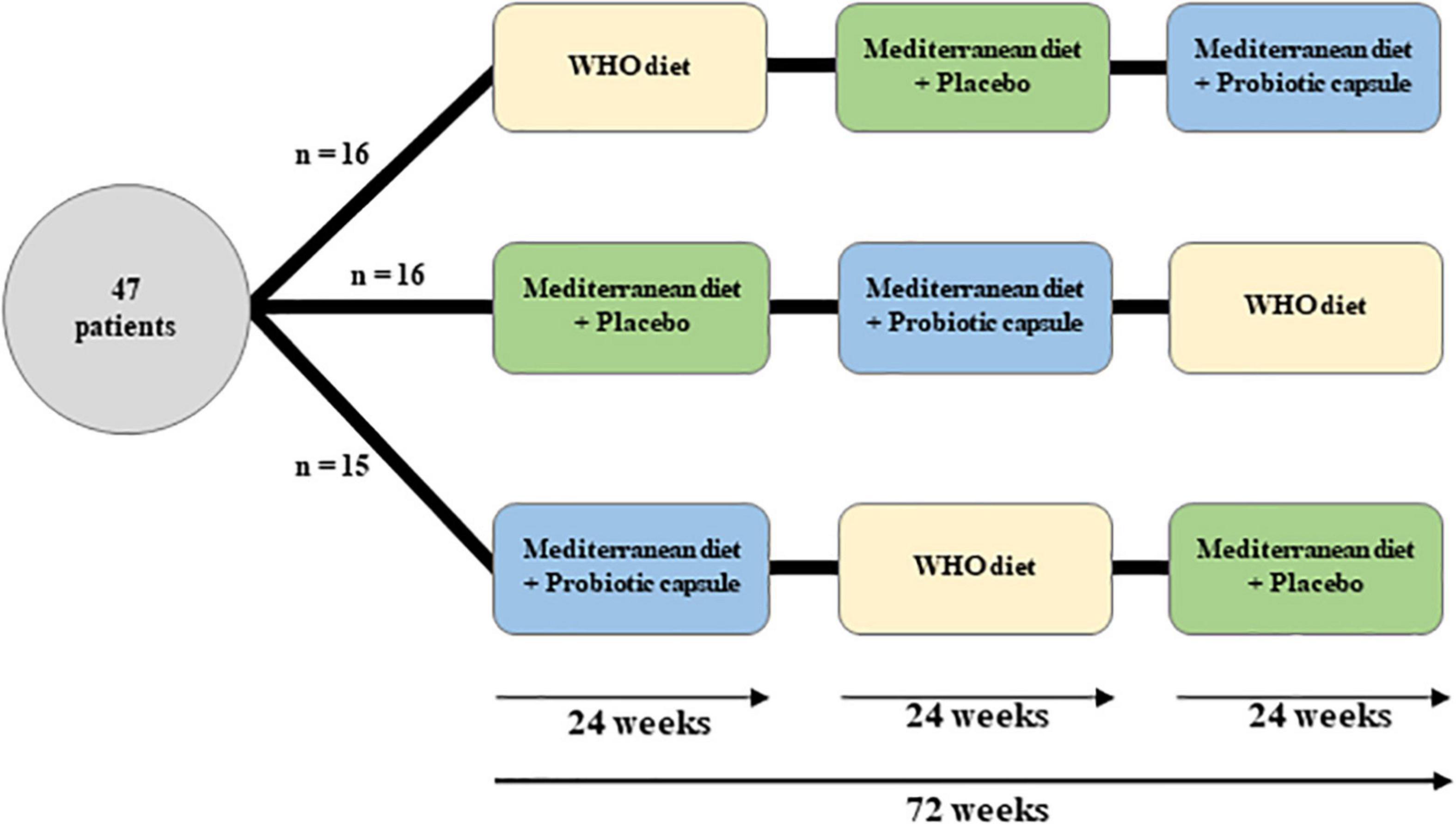
Figure 2. Study design.
Safety studies as well as preclinical and/or clinical trials for each of the strains have been carried out following WHO criteria (37–39).
Dietary interventions were performed by a team of registered dietitians (RDs) who were previously trained to ensure uniformity and the quality of the intervention. The primary goal was to change the eating habits of the patients toward the randomized healthy diet (Mediterranean or WHO diet), focusing on the overall quality of the diet, rather than on specific nutrients, and to evaluate the additive effect of Mediterranean diet supplemented with probiotics. No intervention to increase physical activity or lose weight was included. Since the study patients were MCI-diagnosed, dietary recommendations were particularly focused on the family member or person responsible for cooking at home.
The three dietary interventions included foods from all major food groups, but not total calorie restriction was advised. The Mediterranean diet (supplemented or not with probiotics) comprised a minimum of 35% of total calories from fat [22% MUFAs, 6% polyunsaturated fatty acids (PUFAs), <10% saturated fatty acids (SFAs)], ≤50% from carbohydrates and 15% from protein. The WHO diet included a minimum of 30% of total calories from fat (mainly from MUFAs and PUFAs), emphasizing on the reduction of SFAs (<10%), trans-fat (<1%) and salt consumption (<5 g), and an increase in vegetables and fruits (400 g/day) (Figure 3).
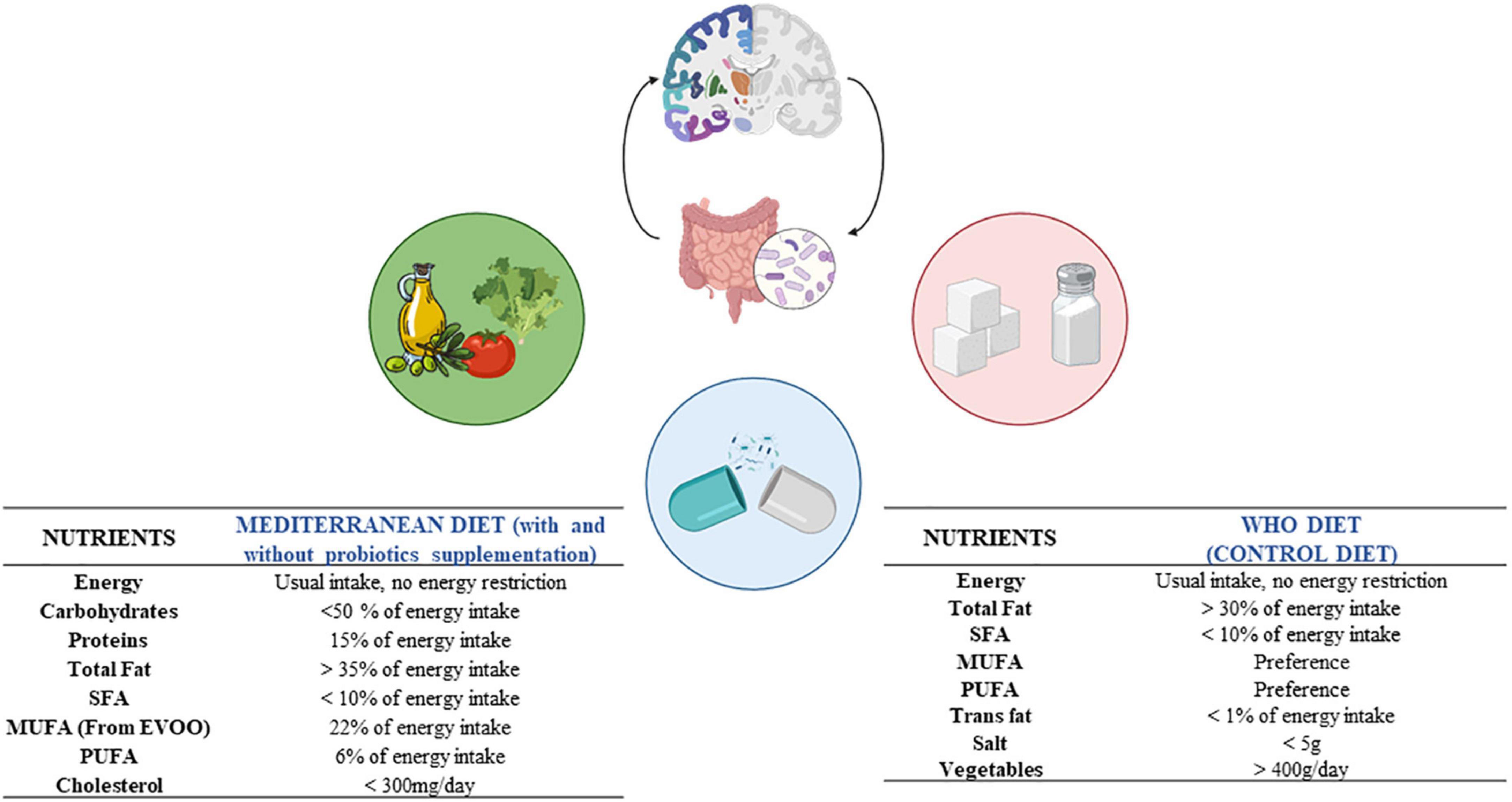
Figure 3. Nutrient composition of the dietary interventions analyzed in the study. WHO, world health organization; SFA, saturated fatty acids; MUFA, monounsaturated fatty acids; PUFA, polyunsaturated fatty acids.
In the three dietary groups, RDs gave personalized counseling to achieve the goals for each diet progressively as follows:
– In both Mediterranean diet groups (with and without probiotics supplementation), patients were recommended to consume, as we previously described (40): (1) abundant use of EVOO for cooking and dressing (≥4 tablespoons/day; 10–15 g/tablespoon), (2) daily consumption of at least two servings of vegetables (200 g/serving; at least one serving raw or as salad) and three or more units of fresh fruit (125–150 g/unit), (3) weekly consumption of at least three servings of legumes (150 g cooked weight/serving), three or more servings of fish or seafood (especially oily fish; 100–150 g/serving) and fresh nuts and seeds (three or more handfuls per week), (4) cooking dishes seasoned with “sofrito” (a slow-cooked homemade sauce with tomato, garlic, onion, aromatic herbs, and olive oil) at least twice a week, (5) a reduction in meat consumption, choosing (skinless) white meat instead of red meat or processed meat (<1 serving/day), (6) avoidance of additional fats (butter, margarine, seed oils, creams, etc.) and foods rich in sugar and unhealthy fats (commercial bakery products, chips, precooked food, sugared beverages, etc.), and (7) in alcohol drinkers, a moderate consumption of red wine.
– In the WHO diet group, patients were recommended to: (1) consume unsaturated fats, as primary source of fat (found in fish, avocado, nuts, and vegetables oils) instead of saturated fats (found in fatty meat, butter, palm and coconut oil, cream, cheese) and industrially produced trans-fats (41, 42), (2) consume vegetable products as fruits, vegetables, legumes, nuts and whole grains (e.g., unprocessed maize, millet, oats, wheat, and brown rice) (42), (3) consume five portions (400 g) of fruit and vegetables daily, excluding potatoes, sweet potatoes, and other starchy roots, (4) reduce the intake of free sugars (<10% of total energy intake) found in foods or drinks by the manufacturer, cook or consumer, as well as sugars naturally present in honey, syrups, fruit juices and fruit juice concentrates (43), and (5) consume <5 g of salt (equivalent to about one teaspoon) per day (44). Salt should be iodized.
The RDs conducted each dietary intervention with the same intensity. Table 2 summarizes the frequency and type of visits performed during the intervention period. At baseline and every 12-weeks, patients had an individual face-to-face visit with the RDs which included assessment of dietary intake and adherence, feedback, and reinforcement, as well as future directions. At each visit, RDs and patients worked together to identify dietary habits that needed to be changed, to set short-term goals and to work out how to implement modifications. Between each face-to-face visit, telephone interviews were performed by the RDs to monitor compliance with the assigned diet, negotiate nutrition goals, and reinforce the dietary recommendations.
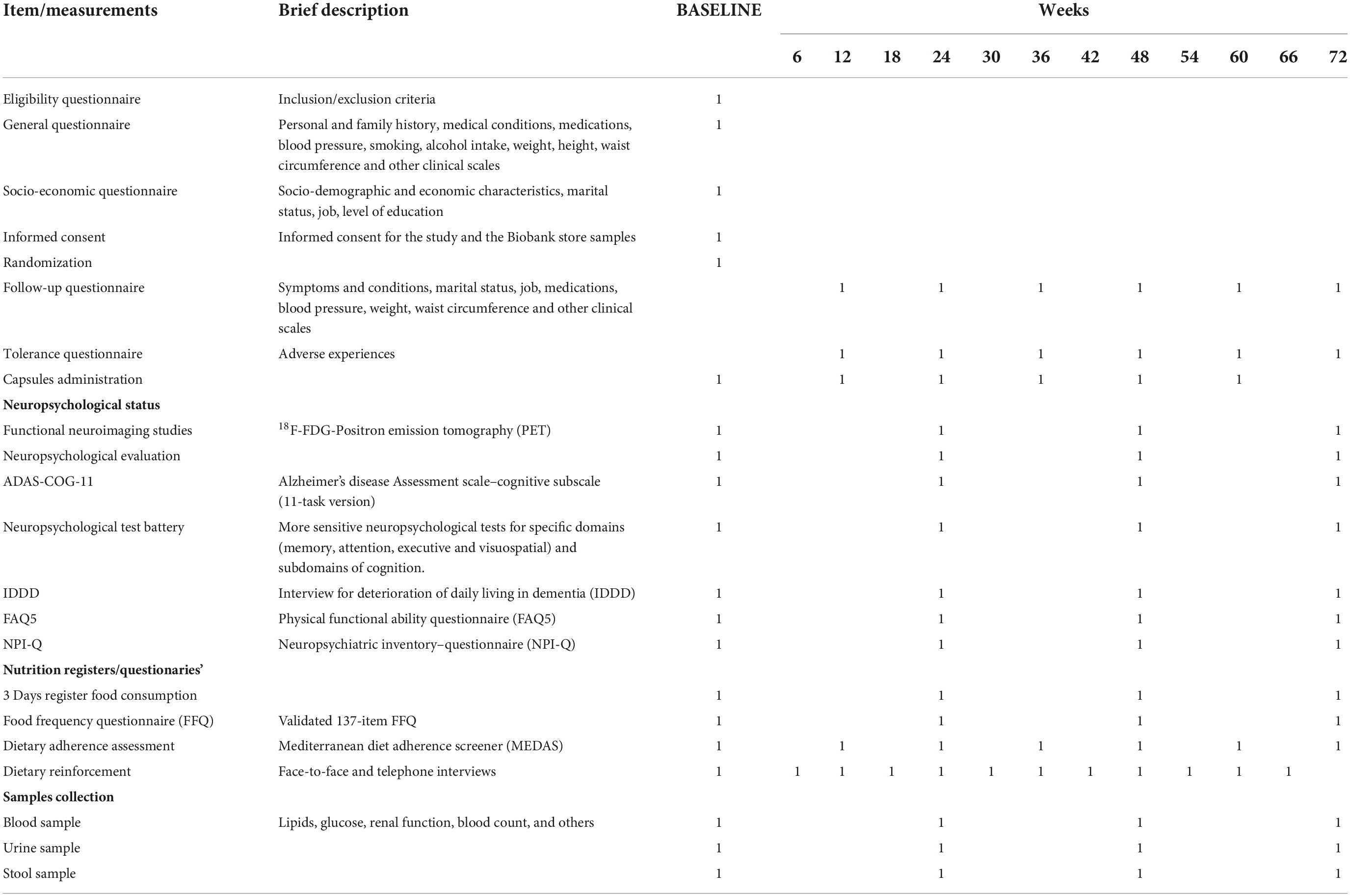
Table 2. Interventions, subsequent care and follow up visits.
Written materials were designed and given to the patients at face-to-face sessions (every 12 weeks) to enhance oral recommendations: leaflets summarizing the main food components, their frequency of consumption, and cooking recipes focused on increasing skills for preparing meals complied with the assigned diet and meal plans. Telephone interviews between each face-to-face session were performed to enhance dietary adherence and solve possible doubts about given recommendations. To encourage dietary adherence, patients also received free EVOO during the 24-weeks period of both interventions with Mediterranean diets (with and without supplemented with probiotics) (approximately 1 L per week).
Information on habitual dietary intake was collected at baseline and at the end of each dietary intervention (i.e., 24, 48, and 72-weeks) using a 137-item semi-quantitative food-frequency questionnaire (FFQ), previously validated in the Spanish population (45, 46). Participants were asked to report their average intake of different food and beverage items over the previous 12 months, as we previously described (40). For each item, typical portion size was included, and consumption frequencies were registered in nine categories ranging from “never or hardly ever” to “≥six times/day.” Energy and nutrient intakes were calculated from Spanish food composition tables (47, 48).
A prospective 3 day-food record of 3 consecutive days [covering 2 weekdays and 1 weekend day (49, 50)] was also assessed at baseline and at the end of each dietary intervention (i.e., 24, 48, and 72-weeks) to enrich the information about dietary consumption and cooking methods.
The 14-item MEditerranean Diet Adherence Screener (MEDAS) was used to measure adherence to the Mediterranean diet (40) in each dietary intervention (in both the Mediterranean dietary groups-with and without probiotics supplementation- and in the WHO dietary group-control diet). This score is an extension of a 9-point score developed by Martinez-Gonzalez et al. (51) and consists of two questions about eating habits, eight questions about the frequency of consumption of typical foods of the Mediterranean diet, and four questions on the consumption of foods not recommended in this diet. Each question was scored with 0 (non-compliant) or 1 (compliant), and the total score (from a total of 14 questions), can range from 0 to 14. Therefore, a score of 14 points depicts maximum adherence.
Primary and secondary outcomes of the study are summarized in Table 3. As part of the main objective, the following outcomes were assessed upon inclusion in the study (baseline), and at the end of each dietary intervention period (i.e., 24, 48, and 72-weeks) (Table 2).
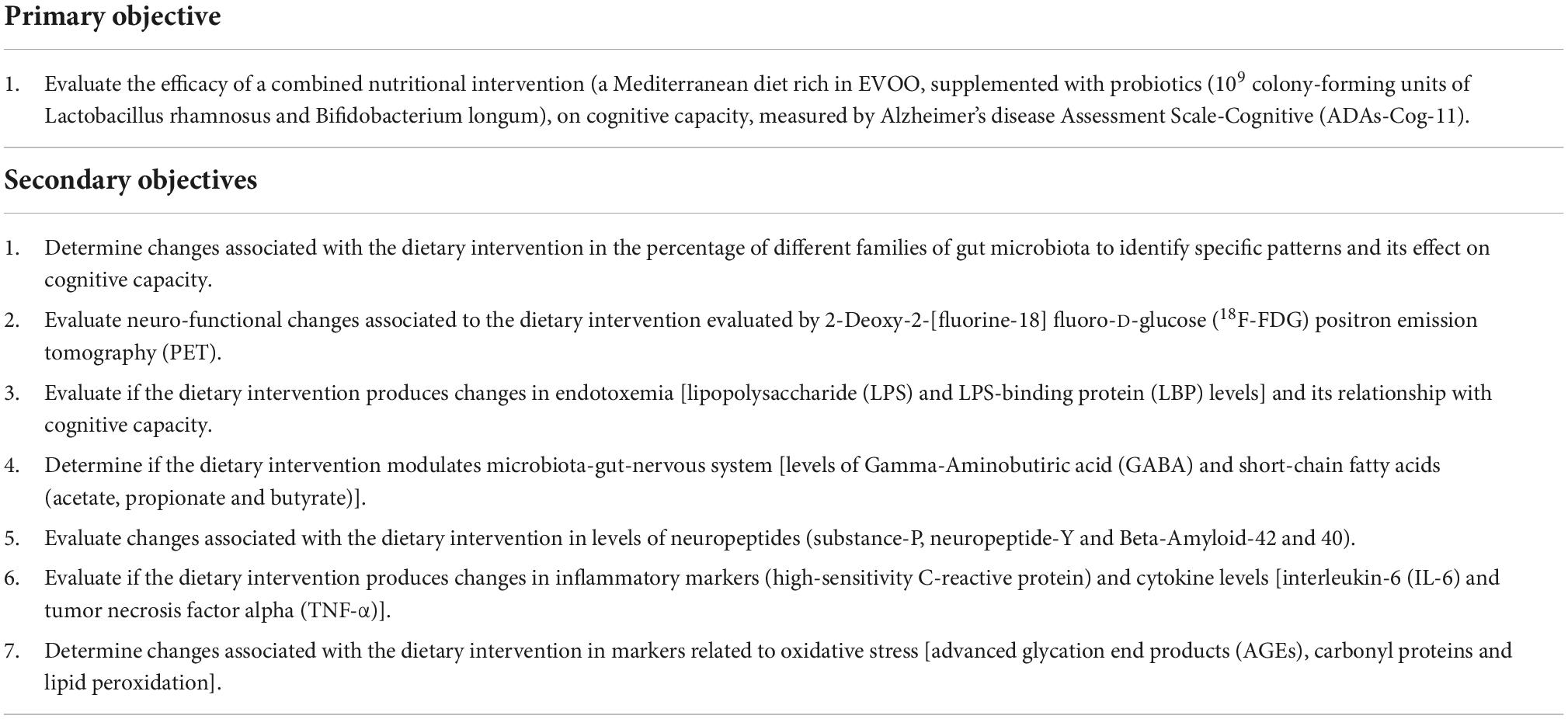
Table 3. Description of the main and secondary objectives of the study.
Although allocation to the diet intervention was randomly assigned, the participant and the RD could not be blinded to diet. All other staff members involved in the measurement of any outcome were blind to the assignments, including the neuropsychologists, magnetic resonance imaging (MRI) technicians, and the lab technician where the blood tests were analyzed. Data entry was performed by a research assistant who was also blinded to group assignments.
Fasting blood samples were drawn and analyzed locally for fasting glucose, fasting insulin, glycated hemoglobin (HbA1c), high-sensitivity C-reactive protein (hsCRP), lipid profile, creatinine, homocysteine, folate, and cobalamin (B12). In addition, blood tubes were centrifuged, and plasma and serum were separated into tubes stored at −80°C for future analysis. Urine and feces samples were also obtained and stored at −80°C.
Anthropometric parameters were measured by trained dietitians using calibrated scales (BF511 body composition analyzer/scale, OMROM, Japan) and a wall-mounted stadiometer (Seca 242, HealthCheck Systems, Brooklyn, NY, USA). Waist circumference was measured midway between the lowest rib and the iliac crest. Body mass index (BMI) was calculated as weight per square meter (kg/m2). Fat-free mass, fat mass and visceral fat were measured by bioelectrical impedance analysis technique (BF511 body composition analyzer/scale, OMROM, Japan). Each measurement was made three times and the average value was calculated. Blood pressure (BP) was determined after a resting period of 10 min in the supine position using an automatic and calibrated sphygmomanometer (OMRON M3, OMRON Healthcare Europe, Spain). As indicated for the anthropometrical measures, BP was measured three times with a 1-min gap between each measurement and an average value was calculated. Smoking habits, Interview for Deterioration of Daily Living in Dementia (IDDD), Physical Functional Ability Questionnaire (FAQ5) and Neuropsychiatric Inventory–Questionnaire (NPI-Q) were assessed.
Regular medical visits to ascertain the existence of any changes in clinical characteristics or drug therapy were carried out (Table 2). Additional (“on demand”) visits were performed, when the patients attending the dietary visits reported any modification in their health status or treatment.
A neuropsychological assessment was performed by an experienced neuropsychologist specializing in the cognitive assessment of older adults. A paper-and-pencil battery, administered in face-to-face sessions, included commonly used cognitive tests presenting a range of cognitive domains, such as attention, executive functions, language, visuospatial, and memory (Supplementary Table 1).
Changes in the Alzheimer’s disease Assessment Scale–Cognitive Subscale (ADAs-Cog-11) (11-task version) was the main outcome of our study (28) (Supplementary Table 1). ADAs-Cog-11 is a rating scale to assess the severity of cognitive dysfunction from mild to severe that includes 11 tasks, subject-completed tests and observer-based assessments. Memory, language, and praxis cognitive domains were assessed by this test (28).
Alzheimer’s disease assessment scale-cognitive scores generally appear able to detect differences in cognitive ability in groups defined by an exposure that is expected to be associated with cognitive ability, although the magnitude of the differences detected tends to be small (28, 52). Responsiveness of the ADAs-Cog-11 to diverse treatment effects appears low compared with other global outcome measures designed to assess subdomains of cognition or other aspects of dementia and MCI syndromes (28). For this reason, other neuropsychological tests were also assessed to detect more subtle differences in MCI evolution in specific domains (i.e., memory, attention, executive, and visuospatial) and subdomains of cognition. A more detailed summary of the different neuropsychological tests performed is presented in Supplementary Table 2. With the aim to evaluate changes in both global neuropsychological condition and at each specific domain, different scores were calculated, using the information from these neuropsychological tests, grouping them by a total sum of values and dividing them by the number of tests used for each case (i.e., Σ Neuropsychological tests/number of Neuropsychological tests).
At baseline and at the end of each dietary intervention (i.e., at 24, 48, and 72-weeks), functional neuroimaging studies by 2-Deoxy-2-[fluorine-18] fluoro-D-glucose (FDG) positron emission tomography–computed tomography (PET/CT) were performed. The CT-based attenuation correction was carried out using the Siemens CAREDose 4D AEC system [Biograph mCT S (20) 3R system, Siemens Medical Solutions USA, Inc.].
All statistical analyses were performed with SPSS version 19.0 for Windows (SPSS Inc., Chicago, IL, USA). Data are presented as the mean ± standard error of the mean (SEM) for continuous variables and as proportions for the categorical variables.
This study will be analyzed under the principle of intention-to-treat (ITT). The ITT analysis will include all randomized participants, regardless of any protocol deviation including non-adherence. Statistical comparisons will be performed using 2-sided significance tests. The primary statistical comparison will be analysis of variance (ANOVA) for repeated measures test with Bonferroni’s adjustment. To adjust for heterogeneity among the subjects, several baseline covariates, including age, sex, basal glucose levels, systolic and diastolic blood pressure, body mass index, diet consumed and drug therapy will be used. The level of significance for all the analyses will be a two-sided p < 0.05.
Categorical variables will be analyzed by chi squared test, whereas continuous variables by ANOVA. Linear and logistic regression analyses will be performed to determine which variables studied were associated with changes in the progression of MCI through time. In order to detect more subtle differences in MCI evolution in specific domains and subdomains of cognition a neuropsychological test battery was assessed, and different scores were calculated grouping them by a total sum of values and dividing them by the number of tests used for each case (i.e., Σ Neuropsychological tests/number of Neuropsychological tests).
Analysis of variance for repeated measures test with Bonferroni’s adjustment and linear mixed effect models will be also used by biochemical characteristics, anthropometric measures, clinical scales and food intake (FFQ, 3 Days Register Food Consumption and MEDAS).
Based on the heterogeneity of the secondary outcomes, statistical tests will be selected individually for each outcome. For example, the processing and analysis of the series images will be performed using the free software SPM and the statistical package R (SPM12 (Statistical Parametric Mapping, Welcome Trust Center for Neuroimaging, London, UK)1 (53). PETs from each subject will be separately analyzed using SPM12. Single subject analysis and two multi subject analysis will be performed for testing for the main effects of subject and diet and testing for the main effects of subject and time, respectively. In addition, the gut microbiota changes, induced by the different dietary interventions, will be analyzed in term of the structure and composition. 16S metagenomic row data sequences will be analyzed using the Quantitative Insights into Microbial Ecology (QIIME2) program.2 These analyses, which include the relative abundance at different levels (phylum, class, order, etc.) and alpha and beta diversity metrics. Further, data modeling (Lasso, Random Forest, General lineal models, etc.) will allow us to evaluate any relationship between gut microbiota and cognitive changes and their influence in cognitive capacity. The level of significance for all the analyses will be a two-sided p < 0.05. Heterogeneity among the subjects will be adjusted for several baseline covariates, including age, and sex.
Participants’ baseline characteristics are presented in Tables 4, 5. The mean age was 73.1 ± 0.9, 57.4% of patients were males and 40.4% have ever smoked (10.6% being current smokers). Furthermore, mean HbA1c was 5.9 ± 0.1% (in a prediabetic range), whereas fasting glucose and insulin levels were 99.7 ± 3.3 mg/dL and 10.4 ± 0.9 mU/L (both within a normal range), respectively. With regards to the lipid profile, mean total cholesterol levels were 180 ± 5.1 mg/dL, triglycerides 99.8 ± 4.3 mg/dL, LDL-cholesterol 80.7 ± 5.0 mg/dL and HDL-cholesterol 57.1 ± 2.0 mg/dL. Mean systolic BP was 136 ± 2.1 mmHg and mean hsCRP levels were 8.8 ± 0.9 mg/dL (Table 4). Patients were overweight with a mean BMI of 27.9 ± 0.5 kg/m2 and mean waist circumference of 99.6 ± 1.6 cm.
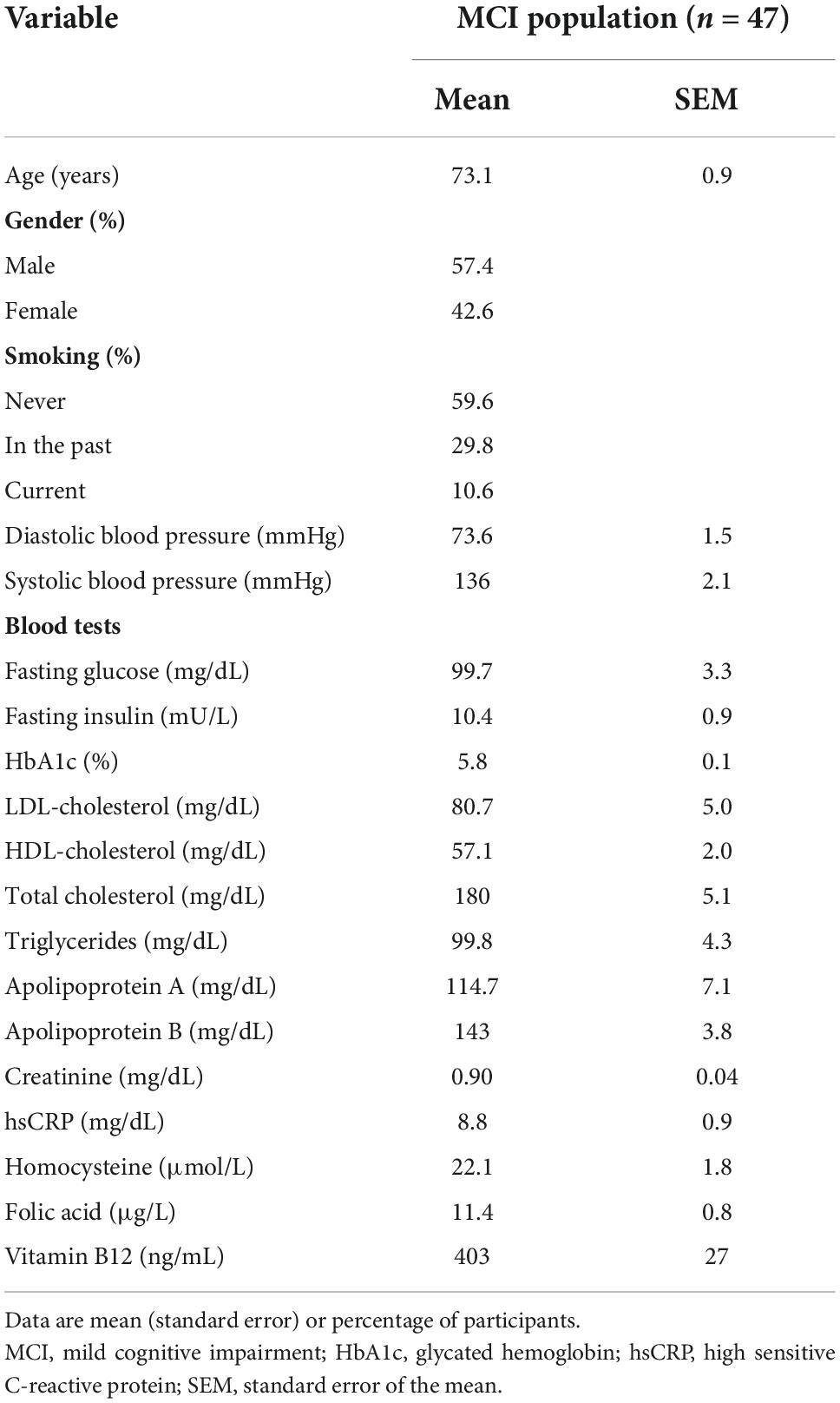
Table 4. Baseline demographic, clinical and biochemical characteristics of the MCI patients.
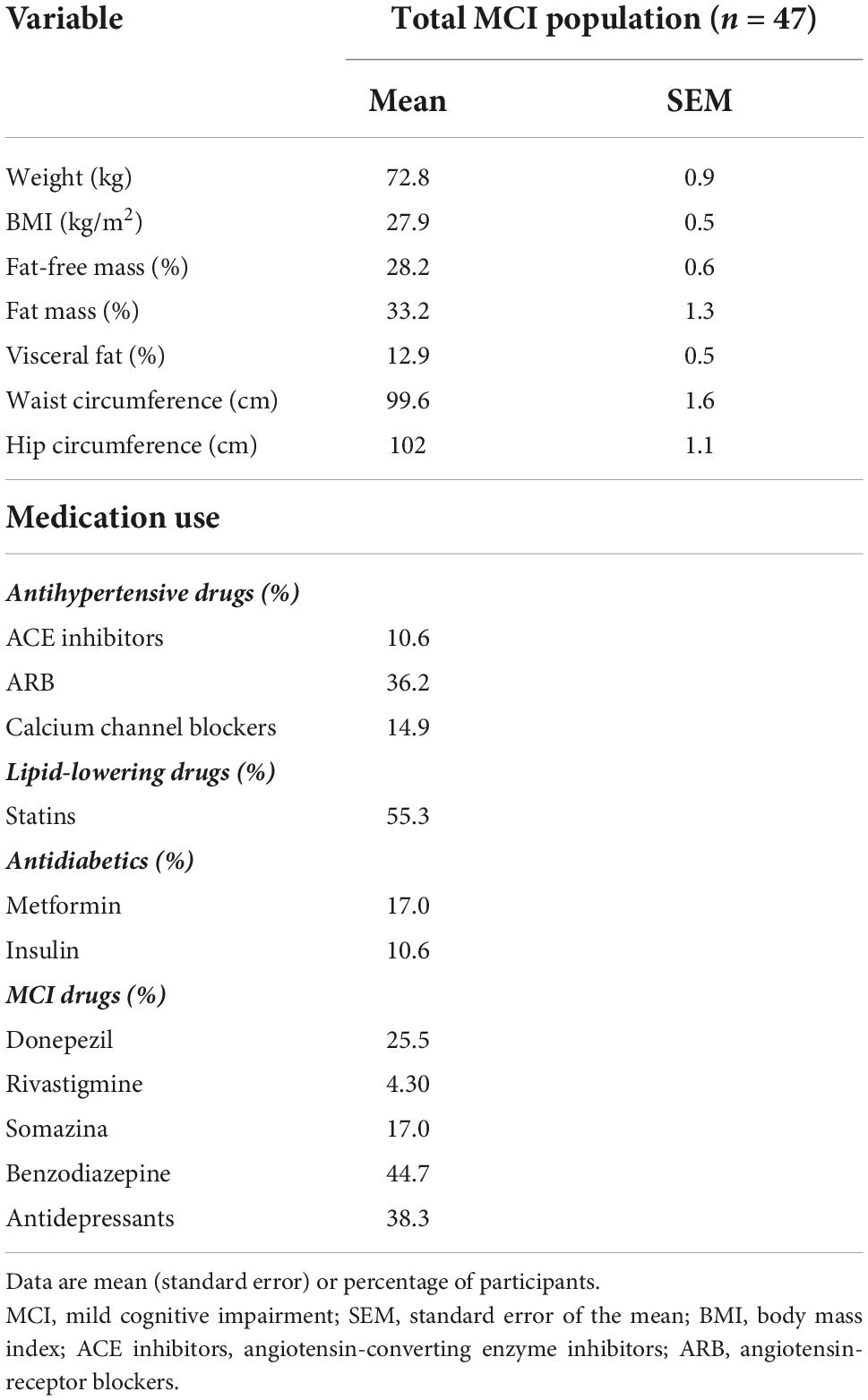
Table 5. Baseline anthropometric characteristics and treatment regimens of the MCI patients.
More than 50% of the patients were on antihypertensive and lipid-lowering (particularly, statins) drug therapy, whereas 27.6% of them were receiving antidiabetic treatment (Table 5).
Table 6 shows the baseline values of energy and nutrient intake. Mean energy intake was 2067 ± 74 kcal, while the percentage of total energy by carbohydrates, protein, and fat energy were 42.9 ± 1.1, 14.8 ± 0.4, 39.7 ± 1.1, respectively. Adherence to the Mediterranean diet as defined with the MEDAS was 7.51 ± 0.29 points (the score ranged from 0 to 14 points) at the baseline for the whole patient population (i.e., regardless of the randomization group to which they were assigned).
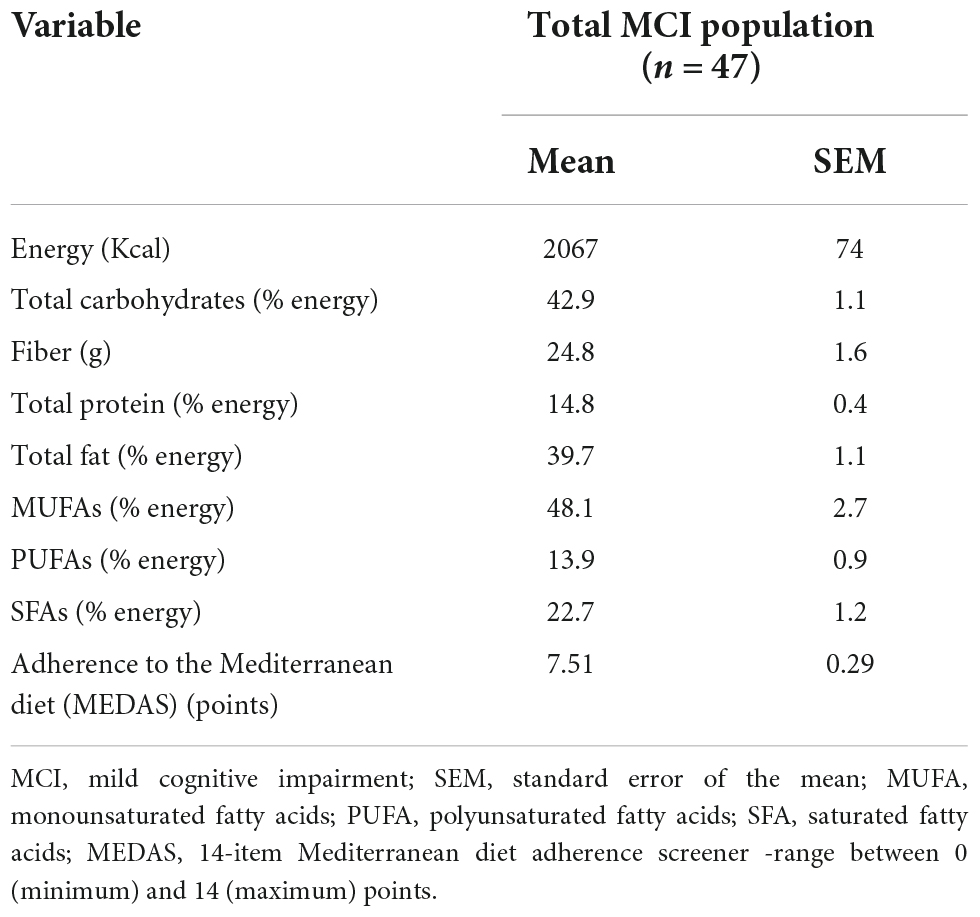
Table 6. Baseline values in energy and nutrient intake.
The present manuscript describes the methodology, study participant selection, recruitment, adherence strategies and baseline characteristics of a randomized clinical study assessing the efficacy of a combined nutritional intervention (i.e., a Mediterranean diet rich in EVOO supplemented with probiotics (Lactobacillus rhamnosus and Bifidobacterium longum)], on cognitive capacity in patients with MCI.
Considering the fact that there are currently no effective pharmacological treatments for MCI (54), lifestyle modifications (such as physical activity and an improvement of diet quality) have shown promising results in slowing the progression of MCI (55). Previous studies focused on single nutrients and foods (ginko biloba), vitamins (vitamin E, C, and B12) or supplements (multivitamins) have reported inconsistent results (56–58). However, strong evidence exists for a beneficial effect of the Mediterranean diet [a dietary pattern rich in plant-based foods such as vegetables, whole grains, nuts, and olive oil [mainly VOO and EVOO) as the main source of fat (in particular MUFA)] in reducing the risk of developing cognitive impairment and dementia (19–22). Different pathways and underlying biological mechanisms have been proposed to explain the effects of the Mediterranean diet on cognitive impairment. In this context, adherence to a Mediterranean diet was associated with less AD biomarkers abnormalities (such as lower Pittsburgh compound B -PET deposition and higher brain glucose metabolism) in middle-aged adults (59, 60). Moreover, the Mediterranean diet reduces cardiovascular risk factors, which are themselves risk factors for the development of cognitive impairment (61, 62). This dietary pattern may also decrease oxidative stress and inflammation, thus potentially exerting neuroprotective properties (63–66). In particular, polyphenols and other minor components of VOO and EVOO showed a beneficial effect on β-aggregation, neurofibrillary tangles, autophagy and mitochondrial function, as well as in cerebral insulin resistance (67). Finally, it has been suggested that the Mediterranean diet could act as a modulator of the gut microbiota (68); the latter being also implicated in aging (69). Recent evidence supports a strong relationship between cognitive impairment disorders and gut microbiota alterations (67, 70). This association is based on the role of the gut-brain axis as a bidirectional communication pathway between the brain and the gastrointestinal tract (11, 12).
In this regard, oral probiotic consumption may modulate the capacity of the gut microbiota, by increasing the diversity and number of beneficial microbes, thus potentially leading to changes in the integrity of the intestinal barrier and the production of microbiota-derived metabolites, as well as to reduction of inflammation and oxidative stress (71) and alterations in the hypothalamic–pituitary–adrenal axis (72, 73). Therefore, some probiotics have been suggested as strategies for modulation of the central nervous system that could prevent cognitive decline, as well as attenuate or improve cognitive impairment related to dementia (74). However, there are certain limitations that do not permit the extraction of safe conclusions in relation to the effects of probiotics on cognitive function. First, clinical studies are mostly performed in patients with AD, with only a few of them conducted in patients with MCI. Secondly, although there are randomized controlled trials, a large number of them were double-blind (75). Moreover, some studies did not provide the exact probiotic strain(s) or the dose administered. Additionally, other studies lack of clarity regarding any form of power calculation to determine sample size or providing basic information such as age range and gender distribution (75, 76).
In this context, further well-designed, randomized controlled trials, with a primary focus on cognitive performance and potential mechanisms of action, are required to elucidate how effective probiotic interventions can be for improving cognitive function. To the best of our knowledge, the present clinical study (a randomized, double-blind, and controlled dietary intervention trial with probiotic supplementation), would be the first to evaluate the synergistic action of two different dietary strategies with potential effects on cognitive capacity in patients with MCI, i.e., a Mediterranean diet (well-known for its cardioprotective, anti-inflammatory and antioxidant properties) with probiotic supplementation (with Lactobacillus rhamnosus and Bifidobacterium longum).
The main limitations of the present study are those inherent to all long-term intervention studies. In this context, although several layers of internal controls have been established to ascertain adherence to the diet, the nature of the study contributes to potential deviations from a strict dietary adherence. On the other hand, the cost of acquiring certain foods (such as fish or nuts) that are determinant for following a Mediterranean diet could be a limitation for an adequate adherence to this type of diet. In conclusions, we described the methods, study participant selection and recruitment, adherence strategies and baseline characteristics of a randomized, latin-square crossover, double-blind, and controlled dietary intervention trial, performed in MCI patients, assessing the efficacy of a combined nutritional intervention on cognitive capacity through the modulation of pathways and mechanisms related to the gut-brain axis. This clinical study will also emphasize the need to evaluate MCI participants and provide dietary therapeutic strategies, for clinical and individual practice, focusing on reducing their risk to develop AD.
Data is available upon request to the corresponding author.
The studies involving human participants were reviewed and approved by the Ethics Committee of Reina Sofía University Hospital (trial protocol 1496/27/03/2009). The patients/participants provided their written informed consent to participate in this study.
PP-M and FP-J contributed to the study concept. PP-M, JL-M, NK, JD-L, and EY-S critically reviewed the manuscript. MC and EY-S contributed to the design of the manuscript, figure preparation, edition, and manuscript drafting. MC, ACo, AL-A, GQ-N, JA-D, OR-Z, ACa, CC-G, CC-M, JV-C, EC-A, JO-S, and EA-M contributed to the acquisition and analysis of data. All authors gave final approval for all aspects of the work, agreed to be fully accountable for ensuring the integrity and accuracy of the work, and read and approved the final manuscript.
This clinical trial has received research grants from the Institute of Health Carlos III (ISCIII), Ministry of Science, Innovation and Universities of Spain (PI16/01777 to PP-M). The CIBEROBN is an initiative of the Instituto de Salud Carlos III, Madrid. EY-S was also the recipient of the Nicolas Monardes Programme from the “Servicio Andaluz de Salud, Junta de Andalucía”, Spain (C1-0005-2019). The funding bodies had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript, data analysis or interpretation, or writing of the manuscript.
We would like to thank ADM Biopolis (Paterna, Valencia, Spain) for providing Biopolis-MIX42 capsules to this study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnut.2022.1037842/full#supplementary-material
AD, Alzheimer’s disease; ADAs-Cog-11, Alzheimer’s disease assessment scale-cognitive; BMI, body mass index; CDR, clinical dementia rating; EVOO, extra virgin olive oil; FFQ, food-frequency questionnaire; HbA1c, glycated hemoglobin; hsCRP, high sensitive C-reactive protein; ITT, intention-to-treat; IDDD, index of deterioration of daily living in dementia; MRI, magnetic resonance imaging; MEDAS, Mediterranean diet adherence screener; MCI, mild cognitive impairment; MMSE, mini mental examination de Folstein; MUFA, monounsaturated fatty acids; NPI-Q, neuropsychiatric inventory–questionnaire; FAQ5, physical functional ability questionnaire; PUFA, polyunsaturated fatty acids; RCT, randomized controlled trial; RDs, registered dietitians; RBANS, repeatable battery for the assessment of neuropsychological status; SFA, saturated fatty acids; SEM, standard error of the mean; VOO, virgin olive oil; WHO, world health organization.
1. Langa K, Levine D. The diagnosis and management of mild cognitive impairment: a clinical review. JAMA. (2014) 312:2551–61. doi: 10.1001/jama.2014.13806
2. Sanford A. Mild cognitive impairment. Clin Geriatr Med. (2017) 33:325–37. doi: 10.1016/j.cger.2017.02.005
3. Lee H, Kim D, Lee W, Kim H, Kim Y. Preventive approach for overcoming dementia. Arch Pharm Res. (2019) 42:647–57. doi: 10.1007/s12272-019-01168-3
4. Alzheimer’s Association. 2015 Alzheimer’s disease facts and figures. Alzheimers Dement. (2015) 11:332–84. doi: 10.1016/j.jalz.2015.02.003
5. Pandya S, Clem M, Silva L, Woon F. Does mild cognitive impairment always lead to dementia? A review. J Neurol Sci. (2016) 369:57–62. doi: 10.1016/j.jns.2016.07.055
6. Hampel H, Hardy J, Blennow K, Chen C, Perry G, Kim S, et al. The Amyloid-beta pathway in Alzheimer’s disease. Mol Psychiatry. (2021) 26:5481–503. doi: 10.1038/s41380-021-01249-0
7. Villemagne V, Burnham S, Bourgeat P, Brown B, Ellis K, Salvado O, et al. Amyloid beta deposition, neurodegeneration, and cognitive decline in sporadic Alzheimer’s disease: a prospective cohort study. Lancet Neurol. (2013) 12:357–67. doi: 10.1016/S1474-4422(13)70044-9
8. Venigalla M, Sonego S, Gyengesi E, Sharman M, Munch G. Novel promising therapeutics against chronic neuroinflammation and neurodegeneration in Alzheimer’s disease. Neurochem Int. (2016) 95:63–74. doi: 10.1016/j.neuint.2015.10.011
9. Tiwari S, Atluri V, Kaushik A, Yndart A, Nair M. Alzheimer’s disease: pathogenesis, diagnostics, and therapeutics. Int J Nanomedicine. (2019) 14:5541–54. doi: 10.2147/IJN.S200490
10. Lowe V, Wiste H, Senjem M, Weigand S, Therneau T, Boeve B, et al. Widespread brain tau and its association with ageing, Braak stage and Alzheimer’s dementia. Brain. (2018) 141:271–87. doi: 10.1093/brain/awx320
11. Clark A, Mach N. The crosstalk between the gut microbiota and mitochondria during exercise. Front Physiol. (2017) 8:319. doi: 10.3389/fphys.2017.00319
12. Cryan J, O’Riordan K, Cowan C, Sandhu K, Bastiaanssen T, Boehme M, et al. The microbiota-gut-brain axis. Physiol Rev. (2019) 99:1877–2013.
13. Zhao X, Yuan L, Feng L, Xi Y, Yu H, Ma W, et al. Association of dietary intake and lifestyle pattern with mild cognitive impairment in the elderly. J Nutr Health Aging. (2015) 19:164–8. doi: 10.1007/s12603-014-0524-2
14. An R, Liu G, Khan N, Yan H, Wang Y. Dietary habits and cognitive impairment risk among oldest-old chinese. J Gerontol B Psychol Sci Soc Sci. (2019) 74:474–83. doi: 10.1093/geronb/gbw170
15. Wang Z, Pang Y, Liu J, Wang J, Xie Z, Huang T. Association of healthy lifestyle with cognitive function among Chinese older adults. Eur J Clin Nutr. (2021) 75:325–34. doi: 10.1038/s41430-020-00785-2
16. Ajith TA. A recent update on the effects of omega-3 fatty acids in Alzheimer’s disease. Curr Clin Pharmacol. (2018) 13:252–60. doi: 10.2174/1574884713666180807145648
17. Williams D, Hagg S, Pedersen N. Circulating antioxidants and Alzheimer disease prevention: a mendelian randomization study. Am J Clin Nutr. (2019) 109:90–8. doi: 10.1093/ajcn/nqy225
18. Dhakal S, Kushairi N, Phan C, Adhikari B, Sabaratnam V, Macreadie I. Dietary polyphenols: a multifactorial strategy to target Alzheimer’s disease. Int J Mol Sci. (2019) 20:5090. doi: 10.3390/ijms20205090
19. Singh B, Parsaik A, Mielke M, Erwin P, Knopman D, Petersen R, et al. Association of mediterranean diet with mild cognitive impairment and Alzheimer’s disease: a systematic review and meta-analysis. J Alzheimers Dis. (2014) 39:271–82. doi: 10.3233/JAD-130830
20. Santoro A, Pini E, Scurti M, Palmas G, Berendsen A, Brzozowska A, et al. Combating inflammaging through a Mediterranean whole diet approach: the NU-AGE project’s conceptual framework and design. Mech Ageing Dev. (2014) 136-137:3–13. doi: 10.1016/j.freeradbiomed.2013.08.109
21. Coelho-Junior H, Trichopoulou A, Panza F. Cross-sectional and longitudinal associations between adherence to Mediterranean diet with physical performance and cognitive function in older adults: a systematic review and meta-analysis. Ageing Res Rev. (2021) 70:101395. doi: 10.1016/j.arr.2021.101395
22. Garcia-Casares N, Gallego Fuentes P, Barbancho M, Lopez-Gigosos R, Garcia-Rodriguez A, Gutierrez-Bedmar M. Alzheimer’s disease, mild cognitive impairment and mediterranean diet. A systematic review and dose-response meta-analysis. J Clin Med. (2021) 10:4642. doi: 10.3390/jcm10204642
23. Perez-Martinez P, Huelgas R, Perez-Jimenez F. Healthy planetary diet: do we have to rethink the recommendations based on the Mediterranean diet? Clin Investig Arterioscler. (2019) 31:218–21. doi: 10.1016/j.artere.2019.10.002
24. Romero-Cabrera J, Yubero-Serrano E, Diaz-Caceres A, Serran-Jimenez A, Arenas-Montes J, Alcala-Diaz J, et al. Educational strategy to improve cardiovascular health and mitigate food insecurity: rationale for the E-DUCASS program. Span J Med. (2022) 2:1–8. doi: 10.24875/SJMED.21000025
25. Abraham D, Feher J, Scuderi G, Szabo D, Dobolyi A, Cservenak M, et al. Exercise and probiotics attenuate the development of Alzheimer’s disease in transgenic mice: role of microbiome. Exp Gerontol. (2019) 115:122–31. doi: 10.1016/j.exger.2018.12.005
26. Rezaeiasl Z, Sepehri G, Salami M. Probiotic treatment improves the impaired spatial cognitive performance and restores synaptic plasticity in an animal model of Alzheimer’s disease. Behav Brain Res. (2019) 376:112183. doi: 10.1016/j.bbr.2019.112183
27. Rezaeiasl Z, Salami M, Sepehri G. The effects of probiotic lactobacillus and bifidobacterium strains on memory and learning behavior, long-term potentiation (LTP), and some biochemical parameters in beta-amyloid-induced rat’s model of Alzheimer’s disease. Prev Nutr Food Sci. (2019) 24:265–73. doi: 10.3746/pnf.2019.24.3.265
28. Kueper J, Speechley M, Montero-Odasso M. The Alzheimer’s disease assessment scale-cognitive subscale (ADAS-COG): modifications and responsiveness in pre-dementia populations. A narrative review. J Alzheimers Dis. (2018) 63:423–44. doi: 10.3233/JAD-170991
29. Skinner J, Carvalho J, Potter G, Thames A, Zelinski E, Crane P, et al. The Alzheimer’s disease assessment scale-cognitive-plus (ADAS-Cog-Plus): an expansion of the ADAS-Cog to improve responsiveness in MCI. Brain Imaging Behav. (2012) 6:489–501. doi: 10.1007/s11682-012-9166-3
30. Morris J. The clinical dementia rating (CDR): current version and scoring rules. Neurology. (1993) 43:2412–4. doi: 10.1212/WNL.43.11.2412-a
31. Morris J. Clinical dementia rating: a reliable and valid diagnostic and staging measure for dementia of the Alzheimer type. Int Psychogeriatr. (1997) 9(Suppl. 1):173–6. doi: 10.1017/S1041610297004870
33. Blesa R, Pujol M, Aguilar M, Santacruz P, Bertran-Serra I, Hernandez G, et al. Clinical validity of the ‘mini-mental state’ for Spanish speaking communities. Neuropsychologia. (2001) 39:1150–7. doi: 10.1016/S0028-3932(01)00055-0
34. Hobson V, Hall J, Humphreys-Clark J, Schrimsher G, O’Bryant S. Identifying functional impairment with scores from the repeatable battery for the assessment of neuropsychological status (RBANS). Int J Geriatr Psychiatry. (2010) 25:525–30. doi: 10.1002/gps.2382
35. Randolph C, Tierney M, Mohr E, Chase T. The repeatable battery for the assessment of neuropsychological status (RBANS): preliminary clinical validity. J Clin Exp Neuropsychol. (1998) 20:310–9. doi: 10.1076/jcen.20.3.310.823
36. Koenig H, Meador K, Cohen H, Blazer D. Self-rated depression scales and screening for major depression in the older hospitalized patient with medical illness. J Am Geriatr Soc. (1988) 36:699–706. doi: 10.1111/j.1532-5415.1988.tb07171.x
37. Navarro-Lopez V, Martinez-Andres A, Ramirez-Bosca A, Ruzafa-Costas B, Nunez-Delegido E, Carrion-Gutierrez M, et al. Efficacy and safety of oral administration of a mixture of probiotic strains in patients with psoriasis: a randomized controlled clinical trial. Acta Derm Venereol. (2019) 99:1078–84.
38. Sanchez Macarro M, Avila-Gandia V, Perez-Pinero S, Canovas F, Garcia-Munoz A, Abellan-Ruiz M, et al. Antioxidant effect of a probiotic product on a model of oxidative stress induced by high-intensity and duration physical exercise. Antioxidants. (2021) 10:323. doi: 10.3390/antiox10020323
39. Caviglia G, Tucci A, Pellicano R, Fagoonee S, Rosso C, Abate M, et al. Clinical response and changes of cytokines and zonulin levels in patients with diarrhoea-predominant irritable bowel syndrome treated with bifidobacterium longum es1 for 8 or 12 weeks: a preliminary report. J Clin Med. (2020) 9:2353. doi: 10.3390/jcm9082353
40. Quintana-Navarro G, Alcala-Diaz J, Lopez-Moreno J, Perez-Corral I, Leon-Acuna A, Torres-Pena J, et al. Long-term dietary adherence and changes in dietary intake in coronary patients after intervention with a Mediterranean diet or a low-fat diet: the CORDIOPREV randomized trial. Eur J Nutr. (2020) 59:2099–110. doi: 10.1007/s00394-019-02059-5
41. Astrup A, Bertram H, Bonjour J, de Groot L, de Oliveira Otto M, Feeney E, et al. WHO draft guidelines on dietary saturated and trans fatty acids: time for a new approach? BMJ. (2019) 366:l4137. doi: 10.1136/bmj.l4137
42. World Health Organization [WHO]. Diet, nutrition and the prevention of chronic diseases. World health organization technical report series. (Vol. 916). Geneva: World Health Organization (WHO) (2003). p. 1–149.
43. World Health Organization [WHO]. WHO guidelines approved by the guidelines review committee. Guideline: sugars intake for adults and children. Geneva: World Health Organization (2015).
44. World Health Organization [WHO]. W guidelines approved by the guidelines review committee. Guideline: sodium intake for adults and children. Geneva: World Health Organization (2012).
45. Fernandez-Ballart J, Pinol J, Zazpe I, Corella D, Carrasco P, Toledo E, et al. Relative validity of a semi-quantitative food-frequency questionnaire in an elderly Mediterranean population of Spain. Br J Nutr. (2010) 103:1808–16. doi: 10.1017/S0007114509993837
46. Martin-Moreno J, Boyle P, Gorgojo L, Maisonneuve P, Fernandez-Rodriguez J, Salvini S, et al. Development and validation of a food frequency questionnaire in Spain. Int J Epidemiol. (1993) 22:512–9. doi: 10.1093/ije/22.3.512
47. Moreiras OCA, Cabrera L, Cuadrado C. Tablas de composición de alimentos y guía de prácticas. Madrid: Ediciones Pirámide (2013).
48. Mataix JGL, Mañas M, Martinez de Victoria E, Llopis J. Tabla de composición de alimentos españoles. Granada: Universidad de Granada (2003).
49. Taggart N. Diet, activity and body-weight. A study of variations in a woman. Br J Nutr. (1962) 16:223–35. doi: 10.1079/BJN19620024
50. Castro D. [Psychological aspects of treatment compliance in the insulin- dependent diabetic child]. Ann Pediatr. (1991) 38:455–8.
51. Schroder H, Fito M, Estruch R, Martinez-Gonzalez M, Corella D, Salas-Salvado J, et al. A short screener is valid for assessing Mediterranean diet adherence among older Spanish men and women. J Nutr. (2011) 141:1140–5. doi: 10.3945/jn.110.135566
52. Karin A, Hannesdottir K, Jaeger J, Annas P, Segerdahl M, Karlsson P, et al. Psychometric evaluation of ADAS-COG and NTB for measuring drug response. Acta Neurol Scand. (2014) 129:114–22. doi: 10.1111/ane.12153
53. Friston KJ, Holmes A, Worsley K, Poline J, Frith C, Frackowiak RS. Statistical parametric maps in functional imaging: a general linear approach. Human Brain Mapping. (1994) 2:189–210. doi: 10.1002/hbm.460020402
54. Cooper C, Ketley D, Livingston G. Systematic review and meta-analysis to estimate potential recruitment to dementia intervention studies. Int J Geriatr Psychiatry. (2014) 29:515–25. doi: 10.1002/gps.4034
55. Sofi F, Valecchi D, Bacci D, Abbate R, Gensini G, Casini A, et al. Physical activity and risk of cognitive decline: a meta-analysis of prospective studies. J Intern Med. (2011) 269:107–17. doi: 10.1111/j.1365-2796.2010.02281.x
56. Krause D, Roupas P. Effect of vitamin intake on cognitive decline in older adults: evaluation of the evidence. J Nutr Health Aging. (2015) 19:745–53. doi: 10.1007/s12603-015-0539-3
57. Snitz B, O’Meara E, Carlson M, Arnold A, Ives D, Rapp S, et al. Ginkgo biloba for preventing cognitive decline in older adults: a randomized trial. JAMA. (2009) 302:2663–70. doi: 10.1001/jama.2009.1913
58. Naeini A, Elmadfa I, Djazayery A, Barekatain M, Ghazvini M, Djalali M, et al. The effect of antioxidant vitamins E and C on cognitive performance of the elderly with mild cognitive impairment in Isfahan, Iran: a double-blind, randomized, placebo-controlled trial. Eur J Nutr. (2014) 53:1255–62. doi: 10.1007/s00394-013-0628-1
59. Berti V, Walters M, Sterling J, Quinn C, Logue M, Andrews R, et al. Mediterranean diet and 3-year Alzheimer brain biomarker changes in middle-aged adults. Neurology. (2018) 90:e1789–98. doi: 10.1212/WNL.0000000000005527
60. Walters M, Sterling J, Quinn C, Ganzer C, Osorio R, Andrews R, et al. Associations of lifestyle and vascular risk factors with Alzheimer’s brain biomarker changes during middle age: a 3-year longitudinal study in the broader New York City area. BMJ Open. (2018) 8:e023664. doi: 10.1136/bmjopen-2018-023664
61. Yubero-Serrano E, Lopez-Moreno J, Gomez-Delgado F, Lopez-Miranda J. Extra virgin olive oil: more than a healthy fat. Eur J Clin Nutr. (2019) 72(Suppl. 1):8–17. doi: 10.1038/s41430-018-0304-x
62. Torres-Pena J, Rangel-Zuniga O, Alcala-Diaz J, Lopez-Miranda J, Delgado-Lista J. Mediterranean diet and endothelial function: a review of its effects at different vascular bed levels. Nutrients. (2020) 12:2212. doi: 10.3390/nu12082212
63. Iadecola C, Duering M, Hachinski V, Joutel A, Pendlebury S, Schneider J, et al. Vascular cognitive impairment and dementia: JACC scientific expert panel. J Am Coll Cardiol. (2019) 73:3326–44. doi: 10.1016/j.jacc.2019.04.034
64. Yubero-Serrano E, Garcia-Rios A, Delgado-Lista J, Delgado-Casado N, Perez-Martinez P, Rodriguez-Cantalejo F, et al. Postprandial effects of the Mediterranean diet on oxidant and antioxidant status in elderly men and women. J Am Geriatr Soc. (2011) 59:938–40. doi: 10.1111/j.1532-5415.2011.03381.x
65. Lopez-Moreno J, Quintana-Navarro G, Delgado-Lista J, Garcia-Rios A, Delgado-Casado N, Camargo A, et al. Mediterranean diet reduces serum advanced glycation end products and increases antioxidant defenses in elderly adults: a randomized controlled trial. J Am Geriatr Soc. (2016) 64:901–4. doi: 10.1111/jgs.14062
66. Delgado-Lista J, Alcala-Diaz J, Torres-Pena J, Quintana-Navarro G, Fuentes F, Garcia-Rios A, et al. Long-term secondary prevention of cardiovascular disease with a Mediterranean diet and a low-fat diet (CORDIOPREV): a randomised controlled trial. Lancet. (2022) 399:1876–85.
67. Silva P, Rodriguez-Perez M, Gomez-Torres O, Burgos-Ramos E. Olive oil and wine as source of multi-target agents in the prevention of Alzheimer disease. Nutr Res Rev. (2021). [Epub head of print]. doi: 10.1017/S095442242100041X
68. Rejeski J, Wilson F, Nagpal R, Yadav H, Weinberg R. The impact of a mediterranean diet on the gut microbiome in healthy human subjects: a pilot study. Digestion. (2021) 103:133–40. doi: 10.1159/000519445
69. Ctoi A, Corina A, Katsiki N, Vodnar D, Andreicut A, Stoian A, et al. Gut microbiota and aging-A focus on centenarians. Biochim Biophys Acta Mol Basis Dis. (2020) 1866:165765. doi: 10.1016/j.bbadis.2020.165765
70. Jiang C, Li G, Huang P, Liu Z, Zhao B. The gut microbiota and Alzheimer’s disease. J Alzheimers Dis. (2017) 58:1–15. doi: 10.3233/JAD-161141
71. Den H, Dong X, Chen M, Zou Z. Efficacy of probiotics on cognition, and biomarkers of inflammation and oxidative stress in adults with Alzheimer’s disease or mild cognitive impairment - a meta-analysis of randomized controlled trials. Aging. (2020) 12:4010–39. doi: 10.18632/aging.102810
72. Smith C, Emge J, Berzins K, Lung L, Khamishon R, Shah P, et al. Probiotics normalize the gut-brain-microbiota axis in immunodeficient mice. Am J Physiol Gastrointest Liver Physiol. (2014) 307:G793–802. doi: 10.1152/ajpgi.00238.2014
73. Farzi A, Frohlich E, Holzer P. Gut microbiota and the neuroendocrine system. Neurotherapeutics. (2018) 15:5–22. doi: 10.1007/s13311-017-0600-5
74. Xiao J, Katsumata N, Bernier F, Ohno K, Yamauchi Y, Odamaki T, et al. Probiotic bifidobacterium breve in improving cognitive functions of older adults with suspected mild cognitive impairment: a randomized, double-blind, placebo-controlled trial. J Alzheimers Dis. (2020) 77:139–47. doi: 10.3233/JAD-200488
75. Ruiz-Gonzalez C, Roman P, Rueda-Ruzafa L, Rodriguez-Arrastia M, Cardona D. Effects of probiotics supplementation on dementia and cognitive impairment: a systematic review and meta-analysis of preclinical and clinical studies. Prog Neuropsychopharmacol Biol Psychiatry. (2021) 108:110189. doi: 10.1016/j.pnpbp.2020.110189
Keywords: mild cognitive impairment, Mediterranean diet, dietary strategies, probiotics, gut-brain axis
Citation: Cardelo MP, Corina A, Leon-Acuña A, Quintana-Navarro GM, Alcala-Diaz JF, Rangel-Zuñiga OA, Camargo A, Conde-Gavilan C, Carmona-Medialdea C, Vallejo-Casas JA, Carmona-Asenjo E, Ochoa-Sepulveda JJ, Aguera-Morales E, Delgado-Lista J, Katsiki N, Lopez-Miranda J, Perez-Jimenez F, Yubero-Serrano EM and Perez-Martínez P (2022) Effect of the Mediterranean diet and probiotic supplementation in the management of mild cognitive impairment: Rationale, methods, and baseline characteristics. Front. Nutr. 9:1037842. doi: 10.3389/fnut.2022.1037842
Received: 06 September 2022; Accepted: 22 November 2022;
Published: 08 December 2022.
Edited by:
Xiaojie Zhang, Department of Psychiatry, Second Xiangya Hospital, Central South University, ChinaReviewed by:
Manja Zec, The University of Arizona, United StatesCopyright © 2022 Cardelo, Corina, Leon-Acuña, Quintana-Navarro, Alcala-Diaz, Rangel-Zuñiga, Camargo, Conde-Gavilan, Carmona-Medialdea, Vallejo-Casas, Carmona-Asenjo, Ochoa-Sepulveda, Aguera-Morales, Delgado-Lista, Katsiki, Lopez-Miranda, Perez-Jimenez, Yubero-Serrano and Perez-Martínez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Pablo Perez-Martínez, cGFibG9wZXJlekB1Y28uZXM=
†These authors have contributed equally to this work and share senior authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.