
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Nutr., 16 December 2022
Sec. Nutritional Epidemiology
Volume 9 - 2022 | https://doi.org/10.3389/fnut.2022.1035580
This article is part of the Research TopicUltra-Processed Foods and Human and Planetary HealthView all 12 articles
 Inge Huybrechts1*
Inge Huybrechts1* Fernanda Rauber2,3
Fernanda Rauber2,3 Geneviève Nicolas1Corinne Casagrande1
Geneviève Nicolas1Corinne Casagrande1 Nathalie Kliemann1Roland Wedekind1Carine Biessy1Augustin Scalbert1Mathilde Touvier4
Nathalie Kliemann1Roland Wedekind1Carine Biessy1Augustin Scalbert1Mathilde Touvier4 Krasimira Aleksandrova5,6
Krasimira Aleksandrova5,6 Paula Jakszyn7,8Guri Skeie9
Paula Jakszyn7,8Guri Skeie9 Rashmita Bajracharya10
Rashmita Bajracharya10 Jolanda M. A. Boer11
Jolanda M. A. Boer11 Yan Borné12Veronique Chajes1Christina C. Dahm13Lucia Dansero14Marcela Guevara15,16,17Alicia K. Heath18Daniel B. Ibsen13,19,20,21
Yan Borné12Veronique Chajes1Christina C. Dahm13Lucia Dansero14Marcela Guevara15,16,17Alicia K. Heath18Daniel B. Ibsen13,19,20,21 Keren Papier22Verena Katzke10
Keren Papier22Verena Katzke10 Cecilie Kyrø23
Cecilie Kyrø23 Giovanna Masala24
Giovanna Masala24 Esther Molina-Montes25,26,27,28
Esther Molina-Montes25,26,27,28 Oliver J. K. Robinson29Carmen Santiuste de Pablos26,30
Oliver J. K. Robinson29Carmen Santiuste de Pablos26,30 Matthias B. Schulze31,32
Matthias B. Schulze31,32 Vittorio Simeon33
Vittorio Simeon33 Emily Sonestedt12Anne Tjønneland23
Emily Sonestedt12Anne Tjønneland23 Rosario Tumino34Yvonne T. van der Schouw35W. M. Monique Verschuren11,35Beatrice Vozar1
Rosario Tumino34Yvonne T. van der Schouw35W. M. Monique Verschuren11,35Beatrice Vozar1 Anna Winkvist36,37Marc J. Gunter1
Anna Winkvist36,37Marc J. Gunter1 Carlos A. Monteiro3,38Christopher Millett2,39Renata Bertazzi Levy2,3
Carlos A. Monteiro3,38Christopher Millett2,39Renata Bertazzi Levy2,3Background: Epidemiological studies have demonstrated an association between the degree of food processing in our diet and the risk of various chronic diseases. Much of this evidence is based on the international Nova classification system, which classifies food into four groups based on the type of processing: (1) Unprocessed and minimally processed foods, (2) Processed culinary ingredients, (3) Processed foods, and (4) “Ultra-processed” foods (UPF). The ability of the Nova classification to accurately characterise the degree of food processing across consumption patterns in various European populations has not been investigated so far. Therefore, we applied the Nova coding to data from the European Prospective Investigation into Cancer and Nutrition (EPIC) in order to characterize the degree of food processing in our diet across European populations with diverse cultural and socio-economic backgrounds and to validate this Nova classification through comparison with objective biomarker measurements.
Methods: After grouping foods in the EPIC dataset according to the Nova classification, a total of 476,768 participants in the EPIC cohort (71.5% women; mean age 51 [standard deviation (SD) 9.93]; median age 52 [percentile (p)25–p75: 58–66] years) were included in the cross-sectional analysis that characterised consumption patterns based on the Nova classification. The consumption of food products classified as different Nova categories were compared to relevant circulating biomarkers denoting food processing, measured in various subsamples (N between 417 and 9,460) within the EPIC cohort via (partial) correlation analyses (unadjusted and adjusted by sex, age, BMI and country). These biomarkers included an industrial transfatty acid (ITFA) isomer (elaidic acid; exogenous fatty acid generated during oil hydrogenation and heating) and urinary 4-methyl syringol sulfate (an indicator for the consumption of smoked food and a component of liquid smoke used in UPF).
Results: Contributions of UPF intake to the overall diet in % grams/day varied across countries from 7% (France) to 23% (Norway) and their contributions to overall % energy intake from 16% (Spain and Italy) to >45% (in the UK and Norway). Differences were also found between sociodemographic groups; participants in the highest fourth of UPF consumption tended to be younger, taller, less educated, current smokers, more physically active, have a higher reported intake of energy and lower reported intake of alcohol. The UPF pattern as defined based on the Nova classification (group 4;% kcal/day) was positively associated with blood levels of industrial elaidic acid (r = 0.54) and 4-methyl syringol sulfate (r = 0.43). Associations for the other 3 Nova groups with these food processing biomarkers were either inverse or non-significant (e.g., for unprocessed and minimally processed foods these correlations were –0.07 and –0.37 for elaidic acid and 4-methyl syringol sulfate, respectively).
Conclusion: These results, based on a large pan-European cohort, demonstrate sociodemographic and geographical differences in the consumption of UPF. Furthermore, these results suggest that the Nova classification can accurately capture consumption of UPF, reflected by stronger correlations with circulating levels of industrial elaidic acid and a syringol metabolite compared to diets high in minimally processed foods.
Worldwide there has been a dramatic increase in the production of industrially processed foods which has coincided with a growing prevalence of obesity, metabolic disorders and multiple chronic diseases (1–16). Global industrialisation, during which diets have been shifting from fresh unprocessed and minimally processed foods toward an increase in the consumption of “ultra-processed” foods (UPF), has been implicated as an important driver of these worrying trends in metabolic disease. UPF that undergo multiple physical, biological, and/or chemical processes, generally contain various processing contaminants, food additives or other industrial substances (17, 18), while they are on average poorer in protective micronutrients (e.g., anti-oxidants) compared to fresh foods (19–33).
The Nova classification system was developed in response to the increased recognition of the importance of classifying foods according to their degree and purpose of processing (i.e., un/minimally processed, processed and ultra-processed foods, as well as culinary ingredients) rather than in terms of nutrients (17, 34, 35). However, recent publications criticized the concepts and definitions used for the Nova classification (36–38), requesting further validation of this food processing classification. While consistent epidemiological evidence linking the consumption of UPF (Nova group 4) to adverse health outcomes such as obesity, type 2 diabetes, cardiovascular diseases, and some cancers is accumulating (3–16), an in depth validation of the Nova classification through comparison with food processing biomarkers is indeed still lacking in population studies.
The European Prospective Investigation into Cancer and Nutrition (EPIC) study offers an appropriate framework to investigate the validity of the Nova classification through comparison with food processing biomarkers already available, namely industrial trans-fatty acids (ITFA) measured in blood (39) and a methylsyringol metabolite measured in urine (40). UPF are the main source of industrially transformed fats, such as partially hydrogenated fats containing industrial trans-fatty acids (ITFA) (11, 41, 42). As such, ITFA profiles in blood may represent a reliable biomarker for UPF consumption. Also, the urinary biomarker 4-methylsyringol sulfate, can be used as an indicator for the consumption of smoked food as it is the human metabolite of 4-methyl syringol, which is formed by the combustion of wood during smoking and deposited on smoked foods (40) and often added as part of liquid smoke to UPF (such as hot dogs) to generate a smoky flavor. A previous intervention study (40) confirmed that syringol markers in urine were detected after intake of ultra-processed hot dogs and to a lower extent after intake of bacon (40). These differences observed after consumption of hot dogs and bacon might be explained by the use of liquid smoke in ultra-processed hot dogs.
The consumption of products from the different Nova categories in relation to relevant biomarkers that are related to food processing such as circulating ITFA has not been evaluated so far (11, 41). To address this gap, we aimed to evaluate UPF consumption patterns in relation to food processing biomarkers available in EPIC as objective indicators of dietary intakes. We hypothesize a positive association of the consumption of UPF with ITFA profiles in blood and syringol markers in urine.
EPIC is a multi-center prospective cohort study, designed to investigate the relationship between nutrition and cancer, among other diseases. A detailed description of the EPIC cohort, including study populations and data collection, has been previously described elsewhere (43). Briefly, it consists of 23 study centers in 10 European countries, including, Denmark, France, Germany, Greece, Italy, Netherlands, Norway, Spain, Sweden, and the United Kingdom. Participants were mostly from the general population and recruited between 1991 and 2000. All participants provided written informed consent and the ethical review boards from the International Agency for Research on Cancer (IARC) and all local centers approved the study. Data from Greece were not available for these analyses.
At baseline, information on lifestyle, dietary intake and medical information as well as sociodemographic and anthropometric data were collected. Lifestyle and medical history questionnaires were used to obtain information on education, smoking status and intensity, alcohol consumption, diabetes and women’s health (including menopausal status, oral contraceptive use, hormone replacement therapy use, age at menarche and age at first full-term pregnancy). Physical activity levels were estimated using a questionnaire focused on past-year physical activity in occupational, leisure and household domains and classified according to the validated Cambridge physical activity index (44).
Body weight and height were measured in all centers, except for Oxford (UK), France and Norway where these were self-reported. Anthropometric characteristics were measured by trained observers using standardized methods (43, 45). Weight and height were used to calculate body mass index (BMI) defined as weight in kilograms divided by height in meters squared (kg/m2).
Diet was assessed at study baseline using validated country/center-specific methods, including dietary questionnaires (DQs) spanning the previous 12 months (43). In most centers, DQs were self-administered, with the exception of Ragusa (Italy), Naples (Italy) and Spain, where face-to-face interviews were performed. Extensive quantitative DQs were used in northern Italy, and Germany that were structured by meals in Spain, France and Ragusa. Semi-quantitative food-frequency questionnaires (FFQs) were used in Denmark, Netherlands, Norway, Italy, Umeå (Sweden) and the United Kingdom, while a FFQ was combined with a 7-day record on hot meals in Malmö (Sweden). Relying on a common food classification and standard handling of recipes, post-harmonization of all the questionnaire data was done by following standardized procedures (e.g., decomposing local recipes and complex foods into ingredients) to obtain a standardized food list for which the level of detail is more comparable between countries (except for Malmö and Spain where open dietary intake assessment methods were used with a higher level of detail; see Supplementary Table 1 for overview of dietary assessment methods used in the different countries/centers). This standardized food list includes more than 11,000 food items. No brand name information was available in the EPIC dietary questionnaires, although some centers asked for the most frequent brand names or product names, e.g., for breakfast cereals in the UK and for margarines in the Netherlands.
From the initial pool of 521,323 EPIC participants, we excluded subjects with missing dietary and/or lifestyle information (n = 6,837), Greek participants (N = 28,034) due to data access issues, and 9,684 participants in the top or bottom 1% of the ratio of energy intake to energy requirement, leaving a final sample of 476,768 adults.
We classified all recorded food items from the EPIC questionnaires according to the Nova food classification system based on the nature, extent, and purpose of industrial food processing (17, 35). This coding was done in close collaboration with the team of Dr. Carlos Monteiro, University of São Paulo (USP), the founder of the Nova classification system. In summary, the Nova classification includes four processing groups and subgroups were adapted to the EPIC items (see Supplementary Table 2).
(1) Group 1: unprocessed or minimally processed foods, which are natural foods (edible parts of plants or of animals after separation from nature) and natural foods altered by methods such as freezing, pasteurization, fermentation, grinding, and other methods that do not include the addition of substances such as salt, sugar and/or oils or fats (e.g., fresh, dry or frozen fruits or vegetables; grains, flours and pasta; pasteurized/sterilized or powdered plain milk; plain yogurt; fresh or frozen meat);
(2) Group 2: processed culinary ingredients are extractions of fresh foods or elements of nature, including substances obtained directly from group 1 foods or from nature by processes that include pressing, refining, grinding, milling, and drying, and consumed in combination with group 1 foods in freshly prepared dishes (e.g., table sugar; oils; butter; cream and salt);
(3) Group 3: processed foods, which are products manufactured industrially with the addition of culinary ingredients (e.g., salt, sugar, oil or fats) to unprocessed or minimally processed foods. Examples of Nova group 3 include canned vegetables; traditional cheese; traditional bread; smoked fish; plain sweetened yogurt;
(4) Group 4: ultra-processed foods, which are commercial food and drink formulations containing besides salt, sugar or fats other substances derived from foods but not domestically used as culinary ingredients (such as protein isolates, hydrogenated oils, modified starches), flavors or additives designed to make the final product palatable or more appealing, such as colors, sweeteners, and emulsifiers. Examples of Nova group 4 include industrially produced bread, poultry and fish nuggets and sticks and other reconstituted meat products transformed with addition of preservatives other than salt; instant noodles and dehydrated soups; carbonated diet and regular sodas; chocolate with emulsifiers, chewing gums and candies with dyes (confectionery); margarine; instant desserts; most breakfast “cereals,” “energy” bars; “energy” drinks; flavored milk drinks/yogurts; sweet desserts made from fruit with added sugars, artificial flavors and texturizing agents; cooked seasoned vegetables with ready-made sauces; vegetable patties (meat substitutes) containing food additives; “health” and “slimming” products such as powdered or “fortified” meal and dish substitutes (see Supplementary Table 2).
We identified homemade and artisanal food preparations, based on FFQ food names and/or local habits. Those identified as homemade recipes were decomposed using local recipes, and the Nova classification was applied to their ingredients. This disaggregation in ingredients was essential to correctly assess the consumption of culinary ingredients (Nova group 2). For breads, data from the Low Energy Ovens Project (46) were used at the country level and a visual check was performed at the DQ item level (e.g., usual Italian and French breads were considered artisanal, while UK bread was classified as ultra-processed). The very detailed EPIC 24-h recalls calibration data (47) and the website Open Food Facts1 were also considered as sources of information on the degree of processing in the different EPIC countries (48).
Changes in the practice of food processing over the past decades require the use of different scenarios when classifying foods according to the Nova classification in a long-term follow-up cohort like EPIC. Dietary intakes were collected at baseline, while the food environment has changed in the intervening years, exposing the EPIC participants to potentially different degrees of food processing over the course of their follow-up (e.g., certain products that were still prepared at home during the 1990s have been replaced by industrial products). As such, a particular food item can potentially be classified in different Nova groups depending on the time period. Therefore, we created three possible scenarios. The “most likely scenario,” in food safety terminology often called the middle bound scenario (MB), which is the scenario considering the most common food processing environment around the baseline period, was used as the main scenario (as agreed upon between the USP team and the IARC team). However, as we were unsure about the level of processing for some of the food items (e.g., when insufficient level of detail was available) for the period 1990–2020, we decided to introduce two alternative scenarios, namely a lower bound (LB) scenario reflecting the lowest degree of processing, and a more processed or upper bound (UB) scenario. For the lower bound scenario, some foods were classified in a less processed Nova group compared to the middle bound scenario when the food item may also have been prepared at home or in an artisanal setting instead of being industrially produced. For the upper bound scenario, some food items were classified in a more processed Nova group compared to the middle bound scenario when it was possible that the food item could be more processed than the most likely option assigned in the middle bound scenario. An example of these three scenarios used for the Nova classification is given in Supplementary Table 3.
The coding of the Nova classification has been evaluated and checked via different quality controls (e.g., comparing the Nova coding proposed by independent food coders, systematic and logic quality controls, checking if the sum of Nova subgroups is equal to the attached Nova group, etc.). One of the quality controls was the comparison with an independent coding performed by the Spanish team in Barcelona on their food list from the Spanish EPIC cohort. The Nova coding performed by the international team was compared with the coding applied in Spain for the Spanish food list. Differences between these two classifications have been discussed between the two teams and few corrections to the three scenarios were made based upon this quality control.
To evaluate the validity of the Nova classification in EPIC, we investigated correlations between the different Nova categories and food processing biomarkers available in subsets of EPIC participants (calibration study and nested case-control studies) analysed in biospecimens collected around the time that the baseline questionnaires were collected. ITFA (elaidic acid levels) measured in plasma phospholipids (49) have been used as biomarkers of dietary intake of industrial trans-fat which is mainly found in UPFs (according to Nova, the presence in the list of ingredients of partially hydrogenated oils, which provide industrial trans fats, makes the product be classified as ultra-processed). Fatty acid profiling was performed using a method previously described (49). ITFA was quantified using an Agilent 7890 gas chromatograph instrument (Agilent Technologies, Santa Clara, CA, USA), and concentrations were expressed as the percentage of total fatty acids (n = 9,460). Elaidic acid was the only ITFA measured in EPIC and as such used as a biomarker for industrially produced foods in these validation analyses.
4-Methyl syringol sulfate which has recently been proposed as a biomarker of smoked meat intake (40) was measured in 24 h urine samples (n = 417) from the EPIC calibration study that included samples from Italy, France and Germany. Sample preparation, laboratory measurement and data processing is described elsewhere (40).
All analyses were performed using the three scenarios for the Nova classification (the lower, middle and upper bound scenarios, representing changes in the food environment over time). Baseline characteristics were examined for the total population and by sex-specific quartiles of each Nova food group. The potential differences between participants were assessed using analysis of variance or χ2 tests when appropriate. Descriptive analyses were performed for each Nova food group considering their daily actual and relative intake in grams and kcal.
Pearson correlations were used to evaluate the association between the Energy % from UPF obtained via the Nova coding performed by the Spanish team (considered as the middle bound scenario) versus those obtained via the three codings performed by the international team for the Spanish food list. In addition, weighted kappa statistics were used to investigate agreement between these two independent codings of the Spanish food list.
Pearson and Spearman correlations were used to investigate associations of levels of biomarkers with % grams and % energy derived from the four Nova groups. Sensitivity analyses were run using partial correlations adjusted for sex, age, BMI and country.
In addition, we also ran sensitivity analyses for the Nova 3 and Nova 4 groups while excluding the alcoholic beverages from these two Nova groups in order to investigate associations between the Nova group intakes and the food processing biomarkers while eliminating the effect of alcohol.
EPIC data and biospecimens are available for investigators who seek to answer important questions on health and disease in the context of research projects that are consistent with the legal and ethical standard practices of IARC/WHO and the EPIC centres. The primary responsibility for accessing the data, including the Nova categories obtained in the frame of the present publication, belongs to the EPIC centres that provided them. The use of a random sample of anonymised data from the EPIC study can be requested by contacting ZXBpY0BpYXJjLmZy. The request will then be passed to members of the EPIC Steering Committee for deliberation.
A total of 476,768 participants were included in the analysis (71.5% women) investigating characteristics of the degree of food processing in EPIC. The mean and median age of participants at recruitment were 51 (SD 9.93) years and 52 (p25–75: 58–66) years, respectively (Table 1). Supplementary Table 4 presents the distributions of the different Nova groups for the total EPIC cohort using the three different scenarios and expressed in both grams and kcal (absolute and relative values) per day. A visual presentation is given in Figure 1. When looking at intakes expressed as grams per day, most of the intakes are from Nova group 1 (Nova group 1 intake is more than 6 times the amount of the processed and UPF groups), while the contributions from the processed and ultra-processed foods (Nova groups 3 and 4) are rather comparable, and Nova group 2 contributing less. The intakes expressed as kcal are rather comparable between the Nova groups 1, 3 and 4, while far lower for Nova group 2 (culinary ingredients). UPF intake contributed to 14% of the total diet in grams/day and to 32% of total daily energy intake. Differences in the consumption of ultra-processed foods were found between socio-demographic groups (Table 1). Although there was a higher proportion of women in this cohort, the contribution of UPF to the overall diet was very similar between men and women. Compared with the lowest fourth of UPF consumption, participants in the highest fourth of UPF consumption tended to be younger, taller, more often current smokers, more physically active, have a lower level of attained education, higher intakes of energy, fat and carbohydrates and lower intake of alcohol (see Table 1). In addition, the FSAm-NPS Dietary Index (DI) score (50), for which a higher score reflects an overall lower nutritional quality of consumed foods, increased with increasing fourth of UPF intake. Supplementary Tables 6A–C present the characteristics of the study population by sex-specific quartiles of relative intake for Nova groups 1 to 3. Subjects in the higher quartiles for diets rich in fresh and minimally processed foods (Nova group 1;% kcal/day) had higher Mediterranean diet scores (51) (Supplementary Table 6A).
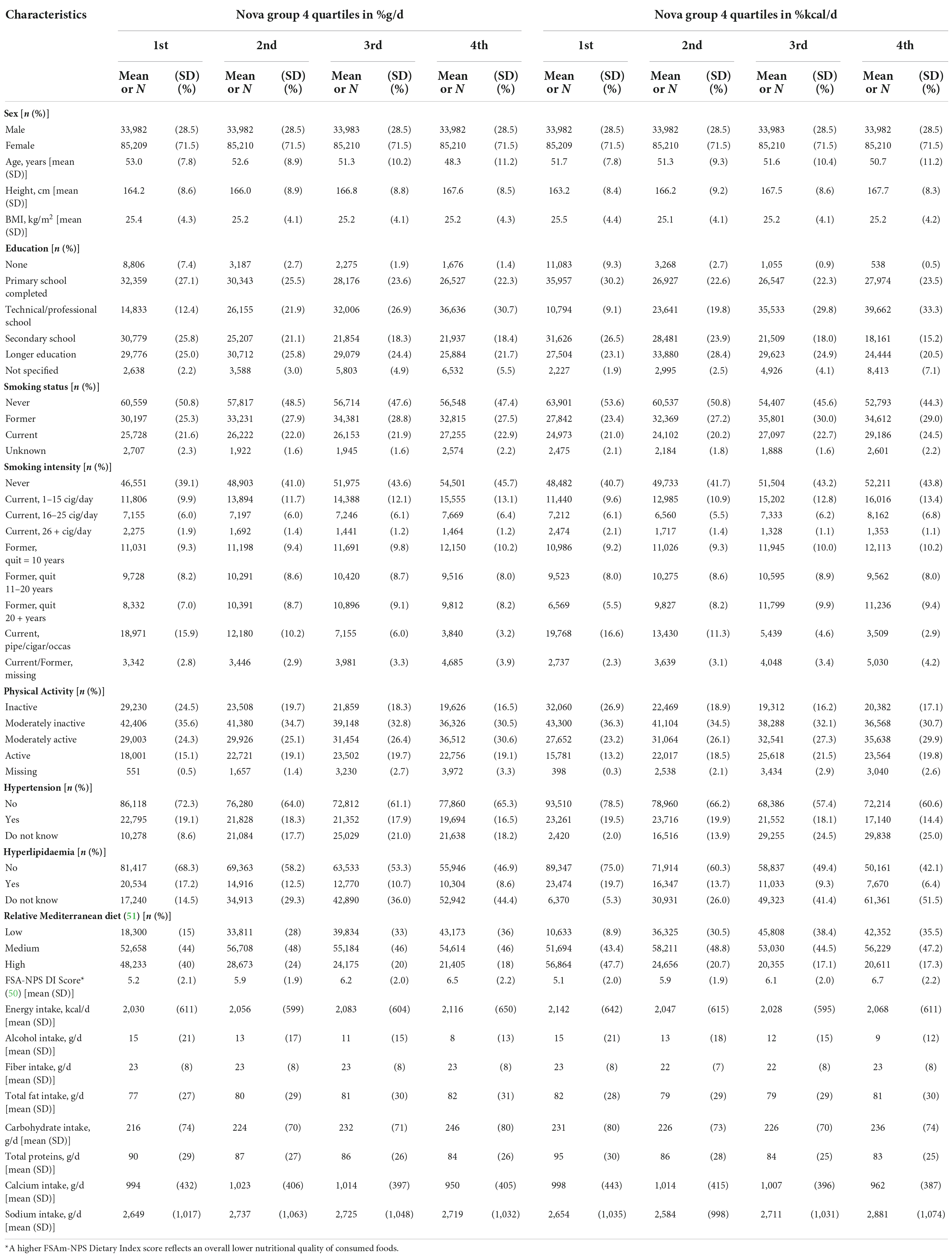
Table 1. Baseline characteristics by sex-specific quartiles of relative intakes of Nova group 4 – ultra-processed foods (% g/day and % kcal/day including alcohol).
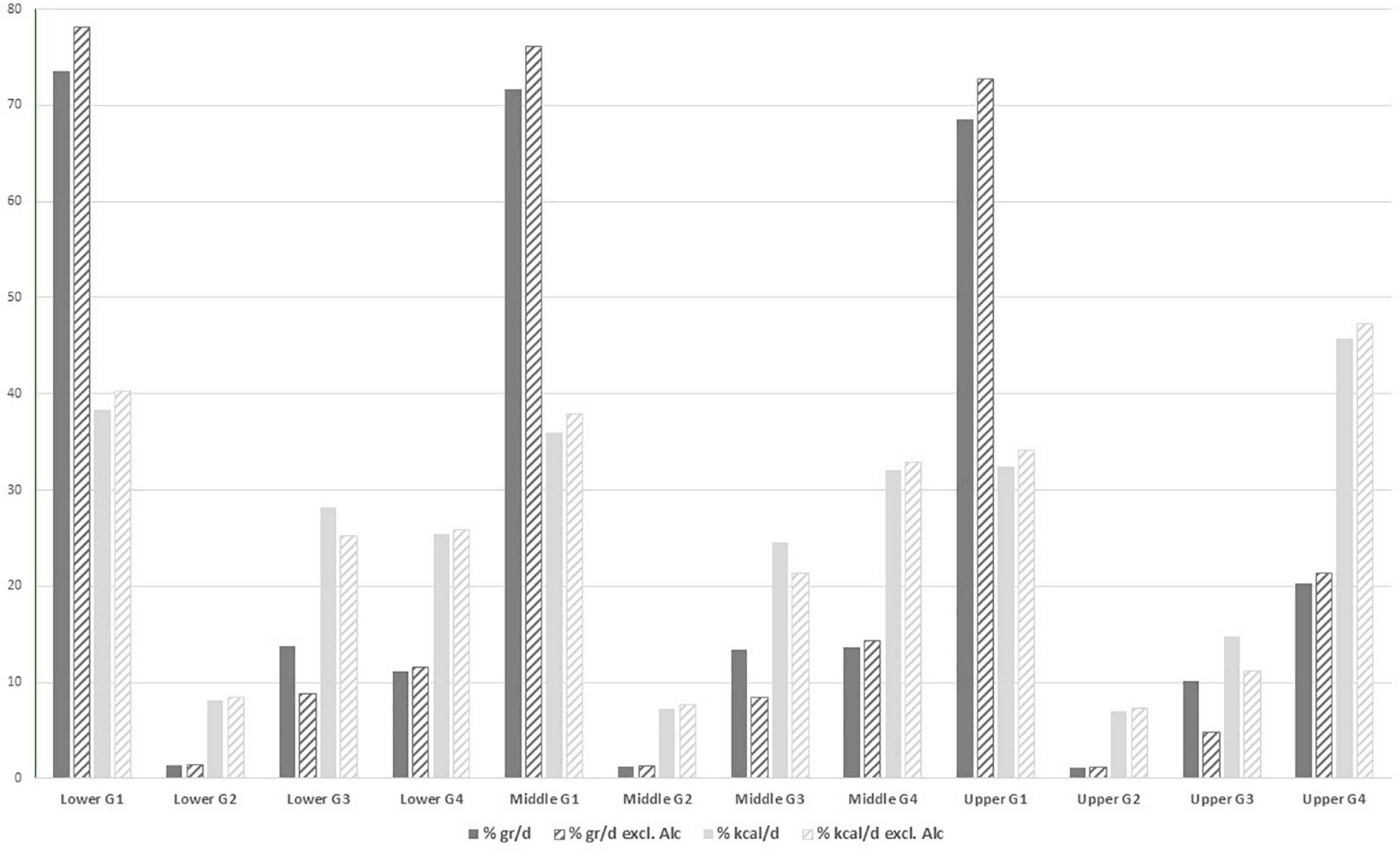
Figure 1. Distributions of the different Nova categories, group G1 to G4, using the three different scenarios (lower, middle and upper bound) for the total EPIC cohort (N = 476,768; distributions per country are provided as Supplementary Tables and Figures). Results derived from the Nova classification in which alcoholic drinks were excluded have been shaded in lighter color font.
The contribution of UPF intake to overall diet varied substantially within the different countries (Supplementary Table 5 and Supplementary Figures 1A,B). The contribution of UPF intake to overall diet in grams/day varied from 7% (France) to 23% (Norway) and their contribution to overall daily energy intake varied from 16% (Spain and Italy) to 46% (for the Norway).
Supplementary Tables 7A,B present the contributions of the different EPIC food groups to the four Nova categories expressed in g/day and kcal/day using the middle bound scenario. “Tea and coffee” were the highest contributors for Nova group 1 while “Beer and cider” were the main contributors to Nova group 3 and “carbonated/soft/isotonic drinks and diluted syrups” were the highest contributors to Nova group 4 when using the absolute values in g/day. When considering the contributions in kcal/day, “fruits” were the main contributors to Nova group 1, while “Bread, crispbread and rusks” were the main contributors for both Nova groups 3 and 4.
The 3 Nova scenarios (lower bound = lowest degree of processing; middle bound = most likely scenario and upper bound = more processed scenario) performed by the international team (USP and IARC) for the Spanish food list were compared with the coding (most likely scenario) applied in Spain to the Spanish food list as one of the quality controls. This demonstrated good comparability (Spearman correlation for % energy derived from UPF = 0.78) between the codes independently assigned by the two teams for the middle bound/most likely scenario (Table 2). The lower and middle bound scenarios gave very similar results while the associations in the upper bound scenario were lower. The weighted kappa statistics also demonstrated good agreement (kappa ranged between 0.48 and 0.68 depending on sex and region) between the two independently assigned Nova classifications for the Spanish EPIC cohort (Supplementary Table 8).
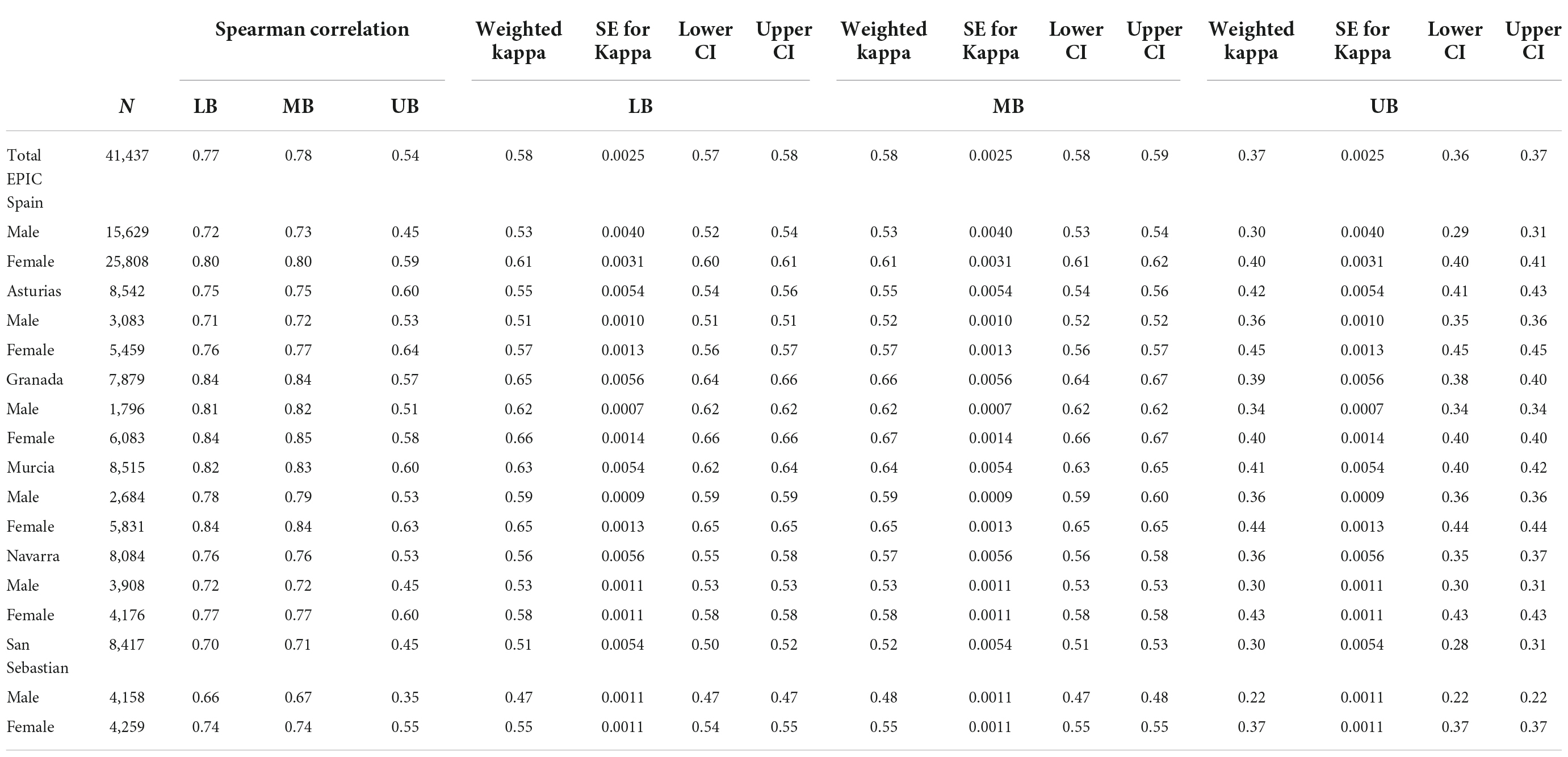
Table 2. Correlations between the % of Energy from Ultra-Processed Food (UPF) obtained from the Nova coding performed by the Spanish team versus those obtained via the coding performed by the international team for the Spanish food list using the three different scenarios: lower bound (LB), middle bound (MB) and upper bound (UB) for classifying Nova group 4 (Ultra-processed foods).
Associations were investigated between the consumption of the 4 Nova groups and objective biomarkers related to food processing. Associations of industrial ITFA plasma levels (elaidic acid) with intakes of the different Nova groups in g/day, kcal/day, % of g/day and % of kcal/day were investigated in a subset of subjects from the nested case-control studies embedded in EPIC (N = 9,460) and are presented in Table 3. The % of grams and energy derived from UPF (Nova group 4) were fair to moderately and statistically significantly positively correlated with ITFA (elaidic acid) plasma levels (Spearman r for middle bound scenario = 0.37 and 0.54, respectively), while inverse or lower positive correlations were found with any other Nova group (see Table 3). Nova group 1 (fresh and minimally processed foods) also showed a positive association when considering % grams/day (Spearman r for middle bound scenario = 0.17) but an inverse association when considering % kcal/day (Spearman r for middle bound scenario =−0.07). Overall, the correlations of the middle bound scenario (the most likely scenario) were most in line with our hypotheses that higher intakes of UPF would lead to higher plasma ITFA levels compared to the lower and upper bound scenario; this suggests better performance of this most likely scenario.
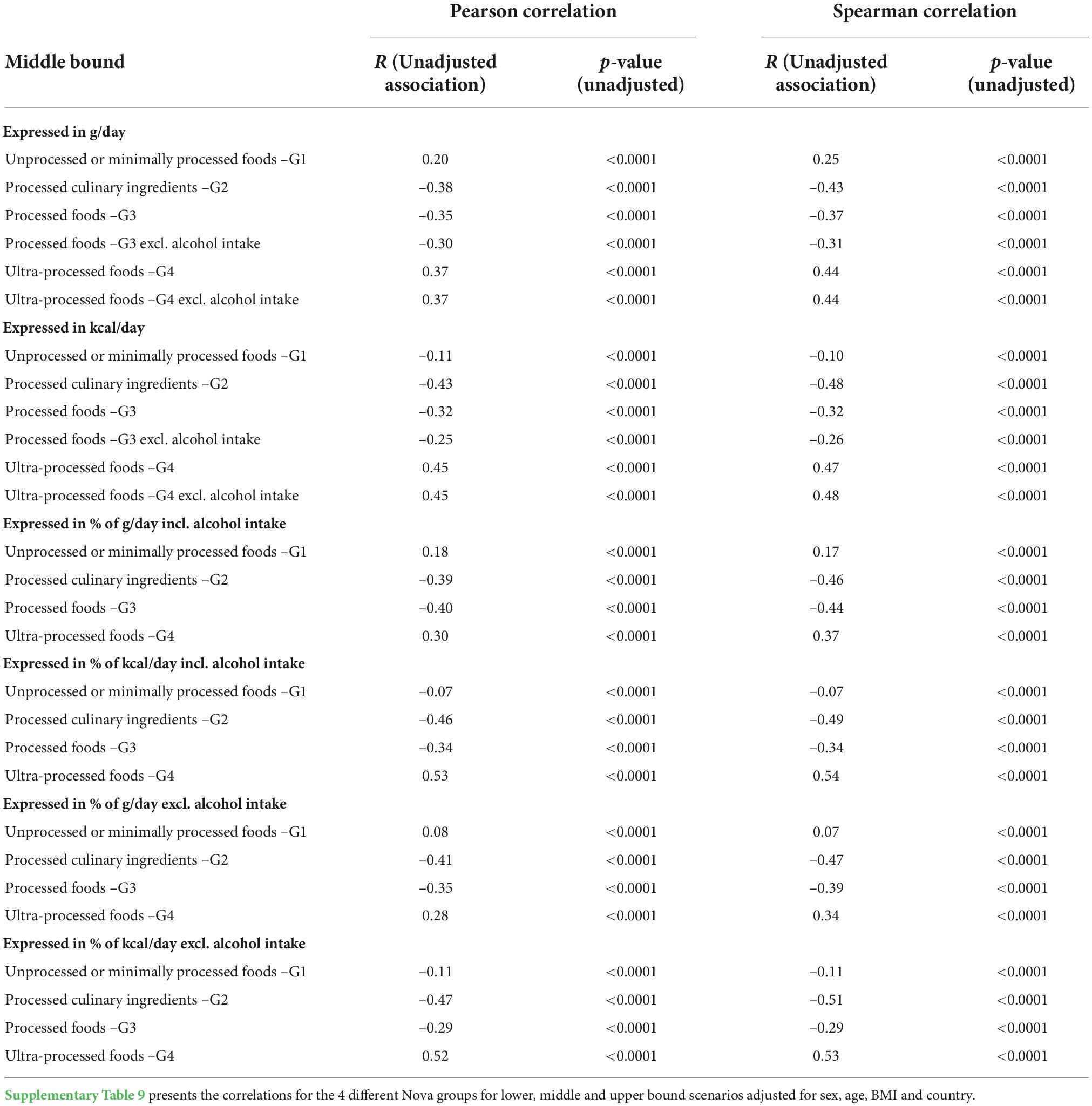
Table 3. Unadjusted associations of elaidic acid levels in plasma with the daily grams, energy, % grams and % energy intake from the 4 different Nova groups and middle bound scenario (N = 9460).
Associations of urinary methyl syringol sulfate with intakes of the different Nova groups (in g/day, kcal/day, % of g/day and % of kcal/day) were similarly investigated in another subset of subjects, derived from the EPIC calibration study (N = 417) and are presented in Table 4. These results also demonstrated fair correlations between the UPF (Nova 4) group and this food processing metabolite while inverse associations for Nova groups 1 and 2 and null for Nova group 3 (except for the Nova group 1 values expressed in grams/day). Associations were again strongest for the middle bound scenario and when using the % kcal/day units.
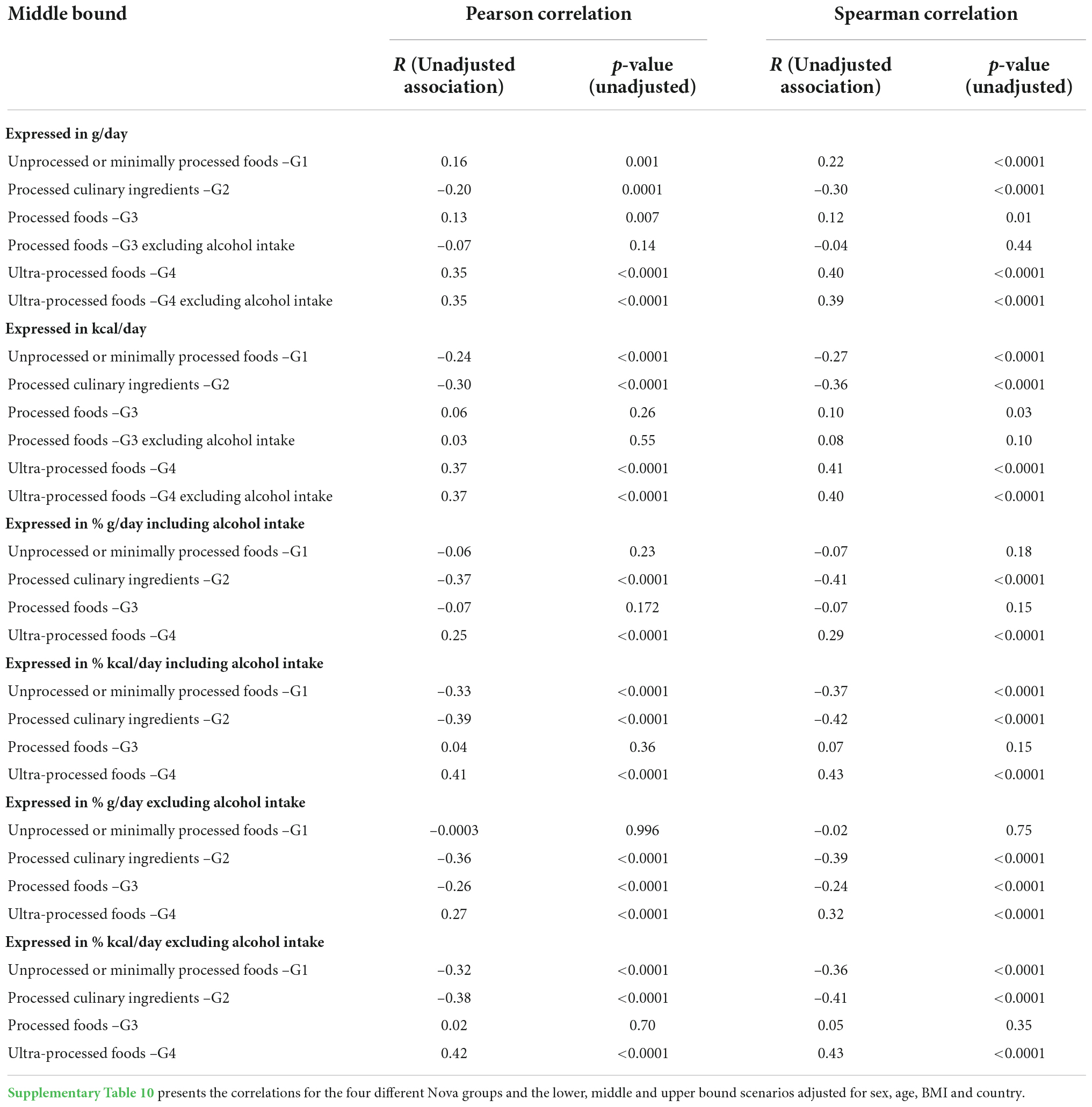
Table 4. Unadjusted associations of urinary methylsyringol sulfate with the daily grams, energy, % grams and % energy intake from the 4 different Nova groups and middle bound scenario (N = 417).
Sensitivity analyses were run for the Nova groups (the three different scenarios and expressed as g/day, kcal/day, % of g/day and % of kcal/day) using partial correlations adjusted for sex, age and BMI which gave very similar results as for the unadjusted analyses, while additionally adjusting for country attenuated the correlations (see Supplementary Tables 9, 10).
The results from this multicenter European study, demonstrate sociodemographic and geographical differences in the consumption of UPF. Furthermore, the comparison with the objective biomarkers, i.e., plasma ITFA and a urinary methylsyringol metabolite showed fair to moderate correlations with the % energy derived from UPF further supporting that the Nova classification is generally suitable for the evaluation of food according to the degree of processing among European populations. The broad variety of foods included in the UPF (Nova 4) group may partially explain the fair to moderate correlations found in relation to the food processing biomarkers. The higher correlations found when considering energy intakes instead of grams of UPF in relation to the food processing biomarkers may be due to the higher energy content of foods high in trans-fat and smoked meat.
The correlation with the food processing biomarkers was slightly higher for the middle bound scenario than for the lower and upper bound scenarios, which suggests better performance of this most likely scenario. Hence, future analyses investigating disease outcomes in relation to the consumption of UPF using the Nova classification are advised to predominantly use the middle bound scenario.
Adjusting the analyses for sex, age and BMI had overall little impact on the correlations with the food processing biomarkers. However, adjustment for country attenuated the correlations (Supplementary Tables 9, 10). These reduced correlations when adjusting for country could potentially be due to loss in power. In addition, the different number of food items in the questionnaires of the various countries (Supplementary Table 1) may also contribute to this attenuation when adjusting for country (e.g., FFQs with fewer food items and less details may underestimate transfatty acid intakes).
Characterisation of the degree of food processing in EPIC demonstrated differences between countries, with contributions of UPF intake to the overall diet in grams/day varying from 7% (France) to 23% (Norway) and their contributions to overall energy intake varying from 16% (Spain and Italy) to 46% (the Norway). In addition, differences were also found between sociodemographic groups in the consumption of ultra-processed and minimally processed foods. Indeed, participants in the highest fourth of UPF consumption tended to be younger, taller, more often current smokers, more physically active, have a lower level of attained education, have a higher reported intake of energy and lower reported intake of alcohol. These results on the characterisation of the degree of food processing in EPIC are in line with the findings from the NutriNet-Santé Cohort (apart from the result for physical activity, showing higher consumption of UPF among highly active people in EPIC) (16, 52). However, overall the consumption of UPF in EPIC was lower than in other surveys and cohorts while the consumption of minimally processed foods was overall higher in comparison with recent studies from the UK and France for instance (13, 16, 19, 52, 53) and a comparison across the nineteen countries (53). This difference may potentially be due to the fact that the baseline data in EPIC, used in this study, have been collected in the late 1990s, when dietary patterns in many European countries may still have been predominantly based on fresh food products and, to a lower extent, UPF. It should also be noted that the characteristics investigated in Table 1 should be interpreted with caution as factors such as age, sex, country, etc. may also play a role in some of these findings (e.g., higher consumers of UPF may potentially be more active because they are younger).
Our study is the largest ongoing multicentre cohort study conducted in Europe with a large battery of detailed participant information. Except for a study investigating associations between UPF consumption and urinary concentrations of phthalates and bisphenol (two biomarkers for exposure to packaging materials) in a nationally representative sample of the US population (54), and two studies investigating metabolic biomarkers of diet quality and UPF in European children (55, 56), according to our knowledge this is the first study that investigates the validity of the Nova classification by comparison with food processing biomarkers in blood and urine. Strengths are the wide range of exposures covered by the 9 different European countries, the use of the standardized methodology and procedures to collect participant information, the use of validated FFQs and standardized methods for classifying food items regarding processing with nutritional experts. Still some limitations need to be acknowledged. Dietary questionnaires provide less detailed information on food processing than data from 24 h recalls or food diaries; though the EPIC questionnaires are very detailed, delivering a food list of more than 11,000 food items after decomposing recipes into ingredients. We acknowledge that differences in dietary questionnaires between the EPIC centres could potentially affect the Nova food processing categories. However, a standardized data coding protocol was employed across the EPIC centres, which included disaggregation of homemade recipes into ingredients (commercial recipes were not decomposed into ingredients). This disaggregation into ingredients was essential to correctly assess the consumption of culinary ingredients (Nova group 2); however, this may have led to an overrepresentation of foods classified as Nova group 1 and 2 items instead of group 3 and group 4 items as some of these ingredients may have been processed (e.g., canned) while this level of detail is not available in dietary questionnaires. In addition, recipes that were made at home in the 1990s may nowadays be industrially processed. All the data used in these methodological analyses, namely the dietary intakes as well as the food processing biomarkers were collected at baseline. It should be considered that for some products, the food processing techniques might have changed over time (e.g., recent trans-fat ban in several countries) (57). To consider such potential changes over time in future etiological analyses, three different scenarios were created, namely lower, middle and upper bound scenarios. Although the middle bound scenario compares best with the objective ITFA measurements also taken at baseline, the lower and upper bound scenarios can still be used in sensitivity analyses to explore the potential impact of further industrialisation of food products and of changes in consumer habits to convenience foods over time (considering that the food environment may have changed over time compared to baseline). Still, the lack of dietary follow-up data could be considered as a potential limitation for etiological analyses. Finally it should also be noted that the objective biomarkers for food processing conveniently available and used in this study (elaidic acid and a syringol metabolite) are only reflecting part of the industrial processes. Therefore, the use of extra food processing biomarkers is recommended for future analyses when resources for additional measurements (e.g., additives metabolites, furan compounds, pyrrole compounds and pyrazine compounds) are available. It should also be noted that dietary biomarkers are also prone to within person variability (depending on people’s recent dietary intakes and the time of specimen collection), while unfortunately only one single biospecimen collection was available for all subjects. In addition, consumption of naturally smoked foods classified as processed foods may also contribute to the measurement of syringol metabolites in addition to the consumption of UPF.
In conclusion, our analyses on the characterisation of the degree of food processing among various participating countries in the EPIC cohort demonstrated a pronounced gradient between and within countries, with higher consumption of UPF in individuals who were younger, taller, current smokers, more physically active, and with lower level of attained education, higher reported intake of energy and lower reported intake of alcohol. In addition, the comparison with the objective biomarkers, i.e., plasma ITFA and urinary syringol metabolites showed fair to moderate correlations with the % energy derived from UPF, supporting that the Nova classification is generally suitable for the evaluation of UPF among European populations.
The data analyzed in this study is subject to the following licenses/restrictions: EPIC data and biospecimens are available for investigators who seek to answer important questions on health and disease in the context of research projects that are consistent with the legal and ethical standard practices of IARC/WHO and the EPIC centres. The primary responsibility for accessing the data, including the NOVA categories obtained in the frame of the present publication, belongs to the EPIC centres that provided them. The use of a random sample of anonymised data from the EPIC study can be requested by contacting ZXBpY0BpYXJjLmZy. The request will then be passed to members of the EPIC Steering Committee for deliberation. Requests to access these datasets should be directed to ZXBpY0BpYXJjLmZy.
The studies involving human participants were reviewed and approved by IARC Ethics Committee (IEC). The patients/participants provided their written informed consent to participate in this study.
IH: conceptualization and writing – original draft. IH, CB, CC, and GN: data curation. NK, RW, CB, and CC: formal analysis. IH and CM: funding acquisition. IH, FR, GN, CC, NK, RW, CB, CM, and RL: investigation. MG, CM, and RL: supervision. All authors: writing – review and editing and approved the submitted version.
The coordination of EPIC was financially supported by International Agency for Research on Cancer (IARC) and also by the Department of Epidemiology and Biostatistics, School of Public Health, Imperial College London which has additional infrastructure support provided by the NIHR Imperial Biomedical Research Centre (BRC). The national cohorts are supported by: Danish Cancer Society (Denmark); Ligue Contre le Cancer, Institut Gustave Roussy, Mutuelle Générale de l’Education Nationale, Institut National de la Santé et de la Recherche Médicale (INSERM) (France); German Cancer Aid, German Cancer Research Center (DKFZ), German Institute of Human Nutrition Potsdam-Rehbruecke (DIfE), Federal Ministry of Education and Research (BMBF) (Germany); Associazione Italiana per la Ricerca sul Cancro-AIRC-Italy, Compagnia di SanPaolo and National Research Council (Italy); Dutch Ministry of Public Health, Welfare and Sports (VWS), Netherlands Cancer Registry (NKR), LK Research Funds, Dutch Prevention Funds, Dutch ZON (Zorg Onderzoek Nederland), World Cancer Research Fund (WCRF), Statistics Netherlands (Netherlands); Health Research Fund (FIS) - Instituto de Salud Carlos III (ISCIII), Regional Governments of Andalucía, Asturias, Basque Country, Murcia and Navarra, and the Catalan Institute of Oncology - ICO (Spain); Swedish Cancer Society, Swedish Research Council and County Councils of Skåne and Västerbotten (Sweden); and Cancer Research UK (14136 to EPIC-Norfolk; C8221/A29017 to EPIC-Oxford), Medical Research Council (1000143 to EPIC-Norfolk; MR/M012190/1 to EPIC-Oxford) (United Kingdom).
The authors thank all EPIC participants and staff for their outstanding contribution to the study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Where authors are identified as personnel of the International Agency for Research on Cancer/World Health Organization, the authors alone are responsible for the views expressed in this article and they do not necessarily represent the decisions, policy or views of the International Agency for Research on Cancer/World Health Organization.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnut.2022.1035580/full#supplementary-material
1. El Kinany K, Mint Sidi Deoula M, Hatime Z, Boudouaya HA, Huybrechts I, El Asri A, et al. Consumption of modern and traditional Moroccan dairy products and colorectal cancer risk: a large case control study. Eur J Nutr. (2020) 59:953–63. doi: 10.1007/s00394-019-01954-1
2. Deoula MS, El Kinany K, Huybrechts I, Gunter MJ, Hatime Z, Boudouaya HA, et al. Consumption of meat, traditional and modern processed meat and colorectal cancer risk among the Moroccan population: a large-scale case-control study. Int J Cancer. (2020) 146:1333–45. doi: 10.1002/ijc.32689
3. Canella DS, Levy RB, Martins APB, Claro RM, Moubarac J-C, Baraldi LG, et al. Ultra-processed food products and obesity in Brazilian households (2008–2009). PLoS One. (2014) 9:e92752. doi: 10.1371/journal.pone.0092752
4. Juul F, Hemmingsson E. Trends in consumption of ultra-processed foods and obesity in Sweden between 1960 and 2010. Public Health Nutr. (2015) 18:3096–107. doi: 10.1017/S1368980015000506
5. Juul F, Martinez-Steele E, Parekh N, Monteiro CA, Chang VW. Ultra-processed food consumption and excess weight among US adults. Br J Nutr. (2018) 120:90–100. doi: 10.1017/S0007114518001046
6. Lavigne-Robichaud M, Moubarac J-C, Lantagne-Lopez S, Johnson-Down L, Batal M, Laouan Sidi EA, et al. Diet quality indices in relation to metabolic syndrome in an Indigenous Cree (Eeyouch) population in northern Québec. Canada. Public Health Nutr. (2018) 21:172–80. doi: 10.1017/S136898001700115X
7. Louzada ML, Baraldi LG, Steele EM, Martins AP, Canella DS, Moubarac JC, et al. Consumption of ultra-processed foods and obesity in Brazilian adolescents and adults. Prev Med. (2015) 81:9–15.
8. Mendonca RD, Lopes AC, Pimenta AM, Gea A, Martinez-Gonzalez MA, Bes-Rastrollo M. Ultra-processed food consumption and the incidence of hypertension in a mediterranean cohort: the Seguimiento universidad de navarra project. Am J Hypertens. (2017) 30:358–66. doi: 10.1093/ajh/hpw137
9. Mendonca RD, Pimenta AM, Gea A, de la Fuente-Arrillaga C, Martinez-Gonzalez MA, Lopes AC, et al. Ultraprocessed food consumption and risk of overweight and obesity: the university of Navarra follow-up (SUN) cohort study. Am J Clin Nutr. (2016) 104:1433–40. doi: 10.3945/ajcn.116.135004
10. Nardocci M, Leclerc B-S, Louzada M-L, Monteiro CA, Batal M, Moubarac J-C. Consumption of ultra-processed foods and obesity in Canada. Can J Public Health. (2018) 110:4–14. doi: 10.17269/s41997-018-0130-x
11. Rauber F, Campagnolo P, Hoffman D, Vitolo M. Consumption of ultra-processed food products and its effects on children’s lipid profiles: a longitudinal study. Nutr Metab Cardiovasc Dis. (2015) 25:116–22. doi: 10.1016/j.numecd.2014.08.001
12. Canhada SL, Luft VC, Giatti L, Duncan BB, Chor D, Fonseca M, et al. Ultra-processed foods, incident overweight and obesity, and longitudinal changes in weight and waist circumference: the Brazilian longitudinal study of adult health (ELSA-Brasil). Public Health Nutr. (2020) 23:1076–86. doi: 10.1017/S1368980019002854
13. Rauber F, Steele EM, Louzada M, Millett C, Monteiro CA, Levy RB. Ultra-processed food consumption and indicators of obesity in the United Kingdom population (2008–2016). PLoS One. (2020) 15:e0232676. doi: 10.1371/journal.pone.0232676
14. Srour B, Fezeu LK, Kesse-Guyot E, Allès B, Debras C, Druesne-Pecollo N, et al. Ultraprocessed food consumption and risk of type 2 diabetes among participants of the NutriNet-santé prospective cohort. JAMA Intern Med. (2019) 180:283–91. doi: 10.1001/jamainternmed.2019.5942
15. Srour B, Fezeu LK, Kesse-Guyot E, Allès B, Méjean C, Andrianasolo RM, et al. Ultra-processed food intake and risk of cardiovascular disease: prospective cohort study (NutriNet-Santé). BMJ. (2019) 365:l1451. doi: 10.1136/bmj.l1451
16. Fiolet T, Srour B, Sellem L, Kesse-Guyot E, Allès B, Méjean C, et al. Consumption of ultra-processed foods and cancer risk: results from NutriNet-Santé prospective cohort. BMJ. (2018) 360:k322. doi: 10.1136/bmj.k322
17. Monteiro CA, Cannon G, Levy RB, Moubarac JC, Louzada ML, Rauber F, et al. Ultra-processed foods: what they are and how to identify them. Public Health Nutr. (2019) 22:936–41. doi: 10.1017/S1368980018003762
18. Srour B, Touvier M. Ultra-processed foods and human health: what do we already know and what will further research tell us? EClinicalMedicine. (2021) 32:100747. doi: 10.1016/j.eclinm.2021.100747
19. Adams J, White M. Characterisation of UK diets according to degree of food processing and associations with socio-demographics and obesity: cross-sectional analysis of UK National diet and nutrition survey (2008–12). Int J Behav Nutr Phys Activ. (2015) 12:160. doi: 10.1186/s12966-015-0317-y
20. Cediel G, Reyes M, da Costa Louzada ML, Steele EM, Monteiro CA, Corvalán C, et al. Ultra-processed foods and added sugars in the Chilean diet (2010). Public Health Nutr. (2018) 21:125–33. doi: 10.1017/S1368980017001161
21. Costa Louzada DML, Martins APB, Canella DS, Baraldi LG, Levy RB, Claro RM, et al. Ultra-processed foods and the nutritional dietary profile in Brazil. Rev Saude Publica. (2015) 49:38. doi: 10.1590/S0034-8910.2015049006132
22. Moubarac JC, Batal M, Louzada ML, Martinez Steele E, Monteiro CA. Consumption of ultra-processed foods predicts diet quality in Canada. Appetite. (2017) 108:512–20. doi: 10.1016/j.appet.2016.11.006
23. Moubarac JC, Martins AP, Claro RM, Levy RB, Cannon G, Monteiro CA. Consumption of ultra-processed foods and likely impact on human health. Evidence from Canada. Public Health Nutr. (2013) 16:2240–8. doi: 10.1017/S1368980012005009
24. Poti JM, Mendez MA, Ng SW, Popkin BM. Is the degree of food processing and convenience linked with the nutritional quality of foods purchased by US households? Am J Clin Nutr. (2015) 101:1251–62. doi: 10.3945/ajcn.114.100925
25. Slimani N, Deharveng G, Southgate Dat, Biessy C, Chajès V, van Bakel MME, et al. Contribution of highly industrially processed foods to the nutrient intakes and patterns of middle-aged populations in the European prospective investigation into cancer and nutrition study. Eur J Clin Nutr. (2009) 63(Suppl. 4):S206–25. doi: 10.1038/ejcn.2009.82
26. Steele EM, Baraldi LG, da Costa Louzada ML, Moubarac J-C, Mozaffarian D, Monteiro CA. Ultra-processed foods and added sugars in the US diet: evidence from a nationally representative cross-sectional study. BMJ Open. (2016) 6:e009892. doi: 10.1136/bmjopen-2015-009892
27. Rauber F, da Costa Louzada ML, Steele EM, Millett C, Monteiro CA, Levy RB. Ultra-processed food consumption and chronic non-communicable diseases-related dietary nutrient profile in the UK (2008?2014). Nutrients. (2018) 10:587. doi: 10.3390/nu10050587
28. Martínez Steele E, Monteiro CA. Association between dietary share of ultra-processed foods and urinary concentrations of phytoestrogens in the US. Nutrients. (2017) 9:209. doi: 10.3390/nu9030209
29. Louzada M, Ricardo CZ, Steele EM, Levy RB, Cannon G, Monteiro CA. The share of ultra-processed foods determines the overall nutritional quality of diets in Brazil. Public Health Nutr. (2018) 21:94–102. doi: 10.1017/S1368980017001434
30. Cediel G, Reyes M, Corvalán C, Levy RB, Uauy R, Monteiro CA. Ultra-processed foods drive to unhealthy diets: evidence from Chile. Public Health Nutr. (2020) 24:1698–707. doi: 10.1017/S1368980019004737
31. Machado PP, Steele EM, Levy RB, Sui Z, Rangan A, Woods J, et al. Ultra-processed foods and recommended intake levels of nutrients linked to non-communicable diseases in Australia: evidence from a nationally representative cross-sectional study. BMJ open. (2019) 9:e029544. doi: 10.1136/bmjopen-2019-029544
32. Marrón-Ponce JA, Flores M, Cediel G, Monteiro CA, Batis C. Associations between consumption of ultra-processed foods and intake of nutrients related to chronic non-communicable diseases in Mexico. J Acad Nutr Diet. (2019) 119:1852–65. doi: 10.1016/j.jand.2019.04.020
33. Martínez Steele E, Popkin BM, Swinburn B, Monteiro CA. The share of ultra-processed foods and the overall nutritional quality of diets in the US: evidence from a nationally representative cross-sectional study. Popul Health Metr. (2017) 15:6. doi: 10.1186/s12963-017-0119-3
34. Fardet A. Characterization of the degree of food processing in relation with its health potential and effects. Adv Food Nutr Res. (2018) 85:79–129. doi: 10.1016/bs.afnr.2018.02.002
35. Monteiro CA, Cannon G, Lawrence M, Costa Louzada ML, Pereira Machado P. Ultra-Processed Foods, Diet Quality, and Health Using the NOVA Classification System. Rome: FAO (2019).
36. Gibney MJ. Ultra-processed foods: definitions and policy issues. Curr Dev Nutr. (2019) 3:nzy077. doi: 10.1093/cdn/nzy077
37. Astrup A, Monteiro CA. Does the concept of “ultra-processed foods” help inform dietary guidelines, beyond conventional classification systems? NO. Am J Clin Nutr. (2022) 1–3. doi: 10.1093/ajcn/nqac230
38. Braesco V, Souchon I, Sauvant P, Haurogné T, Maillot M, Féart C, et al. Ultra-processed foods: how functional is the NOVA system? Eur J Clin Nutr. (2022) 76:1245–53. doi: 10.1038/s41430-022-01099-1
39. Chajès V, Biessy C, Byrnes G, Deharveng G, Saadatian-Elahi M, Jenab M, et al. Ecological-level associations between highly processed food intakes and plasma phospholipid elaidic acid concentrations: results from a cross-sectional study within the European prospective investigation into cancer and nutrition (EPIC). Nutr Cancer. (2011) 63:1235–50. doi: 10.1080/01635581.2011.617530
40. Wedekind R, Keski-Rahkonen P, Robinot N, Viallon V, Ferrari P, Engel E, et al. Syringol metabolites as new biomarkers for smoked meat intake. Am J Clin Nutr. (2019) 110:1424–33. doi: 10.1093/ajcn/nqz222
41. Stender S, Dyerberg J, Astrup A. High levels of industrially produced trans fat in popular fast foods. N Engl J Med. (2006) 2006:1650–2. doi: 10.1056/NEJMc052959
42. Stender S, Dyerberg J, Bysted A, Leth T, Astrup AV. [High levels of industrially produced trans fatty acids in popular fast food–but not in Denmark – secondary publication]. Ugeskrift Laeger. (2006) 168:1654–7. doi: 10.1056/NEJMc052959
43. Riboli E, Hunt KJ, Slimani N, Ferrari P, Norat T, Fahey M, et al. European prospective investigation into cancer and nutrition (EPIC): study populations and data collection. Public Health Nutr. (2002) 5:1113–24. doi: 10.1079/PHN2002394
44. Wareham NJ, Jakes RW, Rennie KL, Schuit J, Mitchell J, Hennings S, et al. Validity and repeatability of a simple index derived from the short physical activity questionnaire used in the European prospective investigation into cancer and nutrition (EPIC) study. Public Health Nutr. (2003) 6:407–13. doi: 10.1079/PHN2002439
45. Klipstein-Grobusch K, Georg T, Boeing H. Interviewer variability in anthropometric measurements and estimates of body composition. Int J Epidemiol. (1997) 26(Suppl. 1):S174–80. doi: 10.1093/ije/26.suppl_1.S174
46. Low Energy Ovens Project. Bakery and Bake off–Market Study FP7 ‘Low Energy Ovens’ Project (nr. 613581). (2007).
47. Slimani N, Kaaks R, Ferrari P, Casagrande C, Clavel-Chapelon F, Lotze G, et al. European prospective investigation into cancer and nutrition (EPIC) calibration study: rationale, design and population characteristics. Public Health Nutr. (2002) 5:1125–45. doi: 10.1079/PHN2002395
48. Open Food Facts,. A Collaborative, Free and Open Database of Food Products from Around the World. (2022). Available online at: https://fr.openfoodfacts.org/ (accessed November 29, 2022).
49. Chajes V, Assi N, Biessy C, Ferrari P, Rinaldi S, Slimani N, et al. A prospective evaluation of plasma phospholipid fatty acids and breast cancer risk in the EPIC study. Ann Oncol. (2017) 28:2836–42. doi: 10.1093/annonc/mdx482
50. Deschasaux M, Huybrechts I, Murphy N, Julia C, Hercberg S, Srour B, et al. Nutritional quality of food as represented by the FSAm-NPS nutrient profiling system underlying the nutri-score label and cancer risk in Europe: results from the EPIC prospective cohort study. PLoS Med. (2018) 15:e1002651. doi: 10.1371/journal.pmed.1002651
51. Romaguera D, Norat T, Vergnaud AC, Mouw T, May AM, Agudo A, et al. Mediterranean dietary patterns and prospective weight change in participants of the EPIC-PANACEA project. Am J Clin Nutr. (2010) 92:912–21. doi: 10.3945/ajcn.2010.29482
52. Julia C, Martinez L, Allès B, Touvier M, Hercberg S, Méjean C, et al. Contribution of ultra-processed foods in the diet of adults from the French NutriNet-Santé study. Public Health Nutr. (2018) 21:27–37. doi: 10.1017/S1368980017001367
53. Monteiro CA, Moubarac JC, Levy RB, Canella DS, Louzada M, Cannon G. Household availability of ultra-processed foods and obesity in nineteen European countries. Public Health Nutr. (2018) 21:18–26. doi: 10.1017/S1368980017001379
54. Martínez Steele E, Khandpur N, da Costa Louzada ML, Monteiro CA. Association between dietary contribution of ultra-processed foods and urinary concentrations of phthalates and bisphenol in a nationally representative sample of the US population aged 6 years and older. PLoS One. (2020) 15:e0236738. doi: 10.1371/journal.pone.0236738
55. Stratakis N, Siskos AP, Papadopoulou E, Nguyen AN, Zhao Y, Margetaki K, et al. Urinary metabolic biomarkers of diet quality in European children are associated with metabolic health. Elife (2022) 11:e71332. doi: 10.7554/eLife.71332
56. Handakas E, Chang K, Khandpur N, Vamos EP, Millett C, Sassi F, et al. Metabolic profiles of ultra-processed food consumption and their role in obesity risk in British children. Clin Nutr. (2022) 41:2537–48. doi: 10.1016/j.clnu.2022.09.002
Keywords: food processing, Nova, EPIC, biomarkers, elaidic acid, syringol
Citation: Huybrechts I, Rauber F, Nicolas G, Casagrande C, Kliemann N, Wedekind R, Biessy C, Scalbert A, Touvier M, Aleksandrova K, Jakszyn P, Skeie G, Bajracharya R, Boer JMA, Borné Y, Chajes V, Dahm CC, Dansero L, Guevara M, Heath AK, Ibsen DB, Papier K, Katzke V, Kyrø C, Masala G, Molina-Montes E, Robinson OJK, Santiuste de Pablos C, Schulze MB, Simeo V, Sonestedt E, Tjønneland A, Tumino R, van der Schouw YT, Verschuren WMM, Vozar B, Winkvist A, Gunter MJ, Monteiro CA, Millett C and Levy RB (2022) Characterization of the degree of food processing in the European Prospective Investigation into Cancer and Nutrition: application of the Nova classification and validation using selected biomarkers of food processing. Front. Nutr. 9:1035580. doi: 10.3389/fnut.2022.1035580
Received: 02 September 2022; Accepted: 17 November 2022;
Published: 16 December 2022.
Edited by:
Raquel Mendonça, Universidade Federal de Ouro Preto, BrazilReviewed by:
Marialaura Bonaccio, Mediterranean Neurological Institute Neuromed (IRCCS), ItalyCopyright © 2022 Huybrechts, Rauber, Nicolas, Casagrande, Kliemann, Wedekind, Biessy, Scalbert, Touvier, Aleksandrova, Jakszyn, Skeie, Bajracharya, Boer, Borné, Chajes, Dahm, Dansero, Guevara, Heath, Ibsen, Papier, Katzke, Kyrø, Masala, Molina-Montes, Robinson, Santiuste de Pablos, Schulze, Simeon, Sonestedt, Tjønneland, Tumino, van der Schouw, Verschuren, Vozar, Winkvist, Gunter, Monteiro, Millett and Levy. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Inge Huybrechts, aHV5YnJlY2h0c0lAaWFyYy5mcg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.