
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CLINICAL TRIAL article
Front. Nutr., 02 November 2022
Sec. Clinical Nutrition
Volume 9 - 2022 | https://doi.org/10.3389/fnut.2022.1030380
This article is part of the Research TopicIntermittent Fasting and Time-Restricted Eating in Health, Physical Performance, and Disease PreventionView all 6 articles
 Anika M. Hartmann1,2*‡
Anika M. Hartmann1,2*‡ Melanie Dell'Oro2Michaela Spoo2,3
Melanie Dell'Oro2Michaela Spoo2,3 Jan Moritz Fischer2‡
Jan Moritz Fischer2‡ Nico Steckhan2,4‡
Nico Steckhan2,4‡ Michael Jeitler2,3‡
Michael Jeitler2,3‡ Thomas Häupl2,5‡
Thomas Häupl2,5‡ Farid I. Kandil2,6‡Andreas Michalsen2,3‡Daniela A. Koppold-Liebscher2,3†‡
Farid I. Kandil2,6‡Andreas Michalsen2,3‡Daniela A. Koppold-Liebscher2,3†‡ Christian S. Kessler2,3†‡
Christian S. Kessler2,3†‡Background: Fasting is beneficial in many diseases, including rheumatoid arthritis (RA), with lasting effects for up to 1 year. However, existing data dates back several decades before the introduction of modern therapeutic modalities.
Objective: This exploratory RCT compares the effects of a 7-day fast followed by a plant-based diet (PBD) to the effects of the dietary recommendations of the German society for nutrition (Deutsche Gesellschaft für Ernährung, DGE) on RA disease activity, cardiovascular (CV) risk factors, and well-being.
Methods: In this RCT we randomly assigned 53 RA patients to either a 7-day fast followed by an 11-week PBD or a 12-week standard DGE diet. The primary endpoint was the group change from baseline to 12 weeks on the Health Assessment Questionnaire Disability Index (HAQ-DI). Further outcomes included other disease activity scores, body composition, and quality of life.
Results: Of 53 RA patients enrolled, 50 participants (25 per group) completed the trial and were included into the per-protocol analysis. The primary endpoint was not statistically significant. However, HAQ-DI improved rapidly in the fasting group by day 7 and remained stable over 12 weeks (Δ-0.29, p = 0.001), while the DGE group improved later at 6 and 12 weeks (Δ-0.23, p = 0.032). DAS28 ameliorated in both groups by week 12 (Δ-0.97, p < 0.001 and Δ-1.14, p < 0.001; respectively), with 9 patients in the fasting but only 3 in the DGE group achieving ACR50 or higher. CV risk factors including weight improved stronger in the fasting group than in the DGE group (Δ-3.9 kg, p < 0.001 and Δ-0.7 kg, p = 0.146).
Conclusions: Compared with a guideline-based anti-inflammatory diet, fasting followed by a plant-based diet showed no benefit in terms of function and disability after 12 weeks. Both dietary approaches had a positive effect on RA disease activity and cardiovascular risk factors in patients with RA.
Clinical trial registration: https://clinicaltrials.gov/ct2/show/NCT03856190, identifier: NCT03856190.
Rheumatoid arthritis (RA), one of the most common inflammatory diseases on a global scale, is associated with a high individual and socioeconomic burden (1, 2). Its etiology is considered multifactorial but remains largely unknown (3). Alongside a genetic predisposition, environmental factors seem to influence the onset and development of RA. This includes dysbiosis of the oral and intestinal microbiota, such as oral commensals like Aggregatibacter actinomycetemcomitans, which promotes citrullination of autoantigens, as well as colonic commensals like Prevotella copri (4). The theory of a gut-joint axis is supported by a growing body of literature on mechanisms of immune-mediated diseases (5–10).
In search for further non-pharmacological and cost-effective therapeutic approaches, nutrition has emerged as a relevant variable modulating the immune-system directly via pro- and anti-inflammatory food components as well as indirectly by influencing the gut microbiota toward an (anti-)inflammatory reaction (11, 12). Research on the effects of nutrition in RA suggests that certain dietary patterns, such as Mediterranean or pesco-vegetarian diets, may improve clinical symptoms of RA (13–16). Additionally, diet can positively influence common comorbidities of RA including risk factors determining morbidity and mortality, such as obesity, hypertension and dyslipidemia, as well as psychological conditions (17–20).
Recently, the French association for rheumatology has addressed the need for data-based dietary recommendations for rheumatologic patients (21). The society has presented a first set of dietary recommendations for French rheumatologic patients, essentially supporting weight loss for overweight patients, a Mediterranean-type diet and Omega-3 supplementation. According to this guideline, fasting and plant-based diets should not be proposed to patients. The authors conclude that vegetarian or vegan diets do not appear to have any relevant effects and question the sustainability of demonstrated fasting effects after resumption of the diet. This statement is based on three clinical fasting studies, the most recent dating back to 1991 (22), and six trials on plant-based diets dating back to 1979 (23).
Previous recent studies have indicated that caloric restriction may remarkably affect health, aging, and disease, including RA (24–26). Regarding RA, only the mentioned, almost historic clinical trials exist on the effect prolonged/periodic fasting (PF; <300 kcal/day) (22, 23). Despite the moderate study quality and age of the data, they show a significant positive impact of a 7 day fast on disease activity in RA for up to 1 year.
It has been hypothesized that a subsequent anti-inflammatory diet following fasting may sustain the beneficial effects beyond the days of the fast (27). A plant-based diet (PBD) seems to fit this demand best: it can reduce leukocyte counts (especially monocytes), can modulate inflammatory biomarkers such as CRP, possibly by altering the mTOR signaling pathway, and can positively impact gut microbiota (28–32).
While the recent extensive research on fasting and fasting mimicking diets is mostly experimental, most clinical trials on fasting or specific diets were performed before the widespread use of the new generation of disease-modifying antirheumatic drugs (DMARDs). Our objective was a) to generate a dietary therapeutic concept for patients with RA involving prolonged fasting followed by plant-based diet and b) to compare it in an explorative manner to an established guideline-based anti-inflammatory diet in patients with RA.
NutriFast was an open label, monocentric, randomized, controlled, parallel-group, explorative clinical trial. We registered the trial with ClinicalTrials.gov (NCT03856190) and published the study protocol in 2021 (33). The study was approved by the local ethics committee (EA 4/005/17) and conducted in accordance with the standards set out in the Declaration of Helsinki. All participants gave written informed consent prior to enrolment.
We included patients of 18–79 years of age with RA diagnosed by a specialist. Eligibility criteria targeted patients on stable medication healthy enough to participate in an outpatient fasting program. Key exclusion criteria were arthritis other than RA, underweight, previous eating disorders, severe comorbidities, a strict PBD and/or fasting within the last 6 months or changes in therapy with DMARDs in the last 8 weeks before enrolment (33).
The dietary interventions were delivered as an intensive group-based behavioral intervention in an outpatient setting and have been described elsewhere (33). In brief, the intervention consisted of a 7-day fast with a daily energy intake of 300–350 kcal/day through vegetable juices and vegetable broth. After fasting, participants were instructed to eat a subsequent plant-based diet for 11 weeks, integrating the concept of time-restricted eating (TRE) and anti-inflammatory spices. The control group followed the current dietary guidelines for RA of the German society for nutrition (Deutsche Gesellschaft für Ernährung, DGE) for 12 weeks. These recommendations are mainly based on a reduction in arachidonic acid intake, which is found in foods of animal origin.
The primary outcome was the change in the Health Assessment Questionnaire Disability Index (HAQ-DI) after 3 months. Secondary outcomes regarding disease activity included Disease Activity Score 28 (DAS28), Simplified and Clinical Disease Activity Indices (SDAI, CDAI) and the proportion of participants fulfilling the EULAR response and American College of Rheumatology (ACR20, ACR50, ACR70) response. Furthermore, questionnaires were used to assess mood (Profile of Mood States, POMS), stress (Cohen's Perceived Stress Scale, CPSS-10), quality of life (WHO-5) and subjective intensity of the main complaint on a visual analog scale (VAS).
We randomly assigned participants to the treatment arms in a 1:1 ratio. The randomization list was generated by an independent research team member using blockrand library (version 1.4) with a randomized variable block approach in R (version 3.5), consecutively numbered, sealed in opaque envelopes and concealed from the responsible study personnel. Participants were allocated after written informed consent and successful screening by the responsible study physician. Blinding of participants to the interventions was not possible due to obvious differences between the intervention arms. Similarly, blinding of outcome assessors was not feasible while ensuring medical and organizational support of patients in their specific dietary regimen.
The sample size was calculated within the context of an explorative study. Estimating the yearly RA patient turnover of associated hospitals and clinics in Berlin, we intended to enroll 84 participants in this exploratory RCT. This number was based on a repeated ANOVA design with a hypothesis only for the interaction term, a non-sphericity correction of epsilon ε= 1, an assumed correlation among repeated measures of 0.5, and a dropout rate of 10%. The calculated sample size should provide us a solid statistical power (80%) with a significance level of 5% in detecting differences with effect sizes of f = 0.20 (d = 0.40) or higher, and thus all medium and large effects. In 12/2020, it became necessary to halt recruitment by 05/2021 due to mandatory research restrictions during the Covid-19 pandemic and expiring funding. Because the recruitment rate was slower than expected and recruitment ended early as mentioned, only 53 participants were enrolled.
Analyses were based on the per-protocol treatment (PPT) population, excluding 3 early dropouts who did not start participation in either of the study interventions. Each analysis compared the outcomes between the two study arms before and after treatment. Potential differences in outcomes, were examined by χ2, analysis of variance, independent and dependent t-test as specified. We performed analyses using SPSS V.27 and RStudio Version 1.4.1106.
We enrolled 53 participants between 03/2019 and 11/2020 with follow-up at 6 months until 07/2021. Of 94 interested patients assessed per telephone, 62 patients were invited to a screening with a study physician, of which 53 fulfilled the eligibility criteria and were randomized to either fasting followed by a PBD or the standard diet according to the DGE recommendations (Figure 1). Fifty patients underwent the treatment per protocol, 3 early dropouts occurred before the start of the interventions. The follow-up at 6 months was completed by 40 participants. Demographics of the two groups were comparable at baseline and representative of a predominantly female RA population with a moderate disease activity (Table 1). Regarding baseline clinical characteristics, the fasting and PBD group demonstrated better functional ability in the HAQ-DI (Table 2).
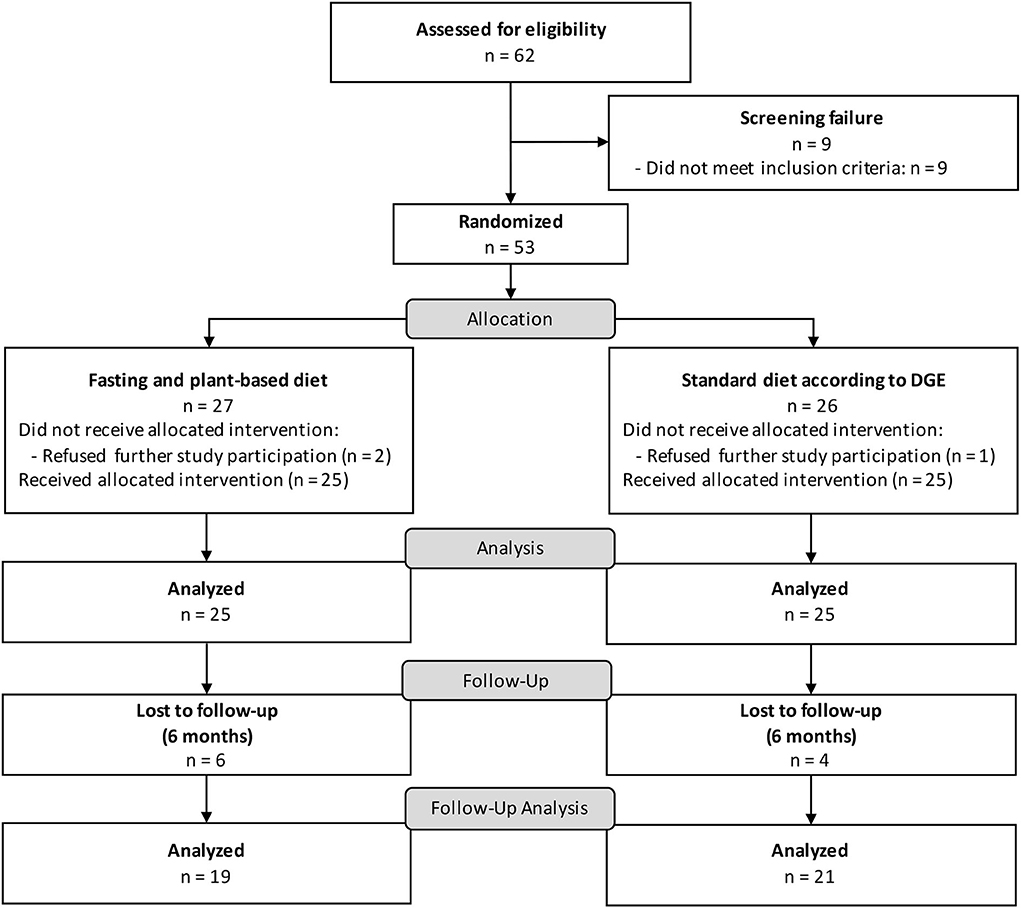
Figure 1. CONSORT flow chart NutriFast trial.
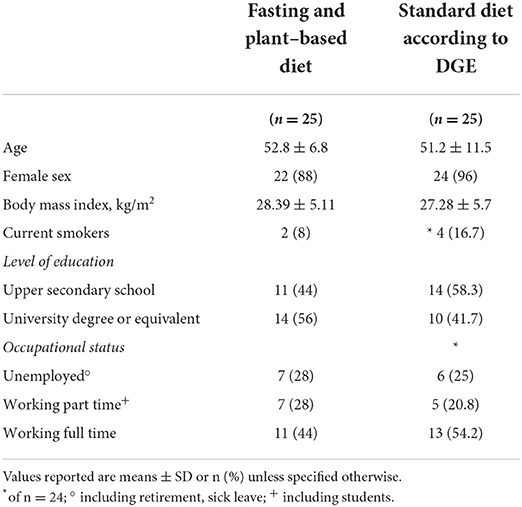
Table 1. Demographic characteristics of participants at baseline.
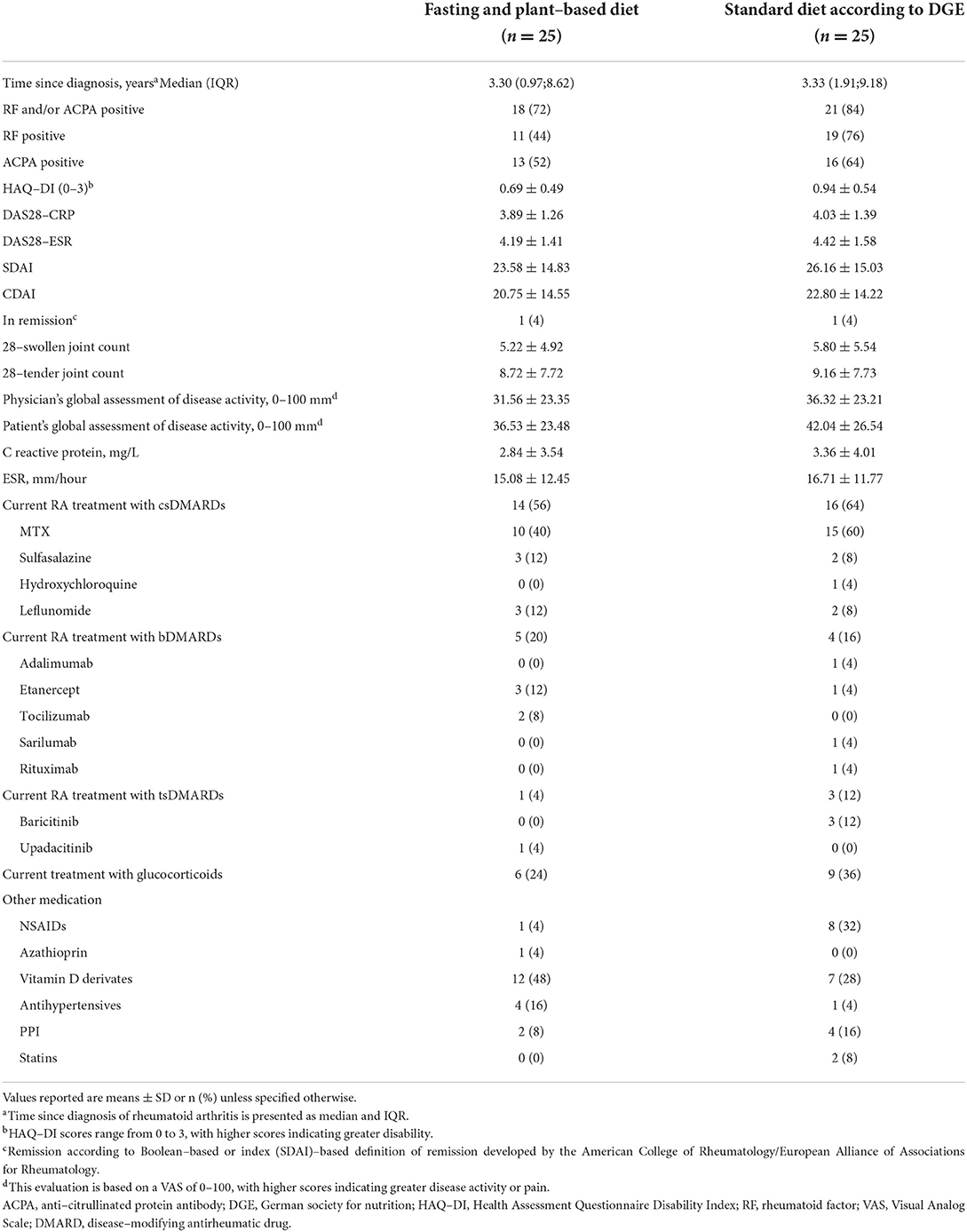
Table 2. Disease status and medication at baseline.
Study outcomes are presented in Table 3 and in the Supplementary Appendix. The explorative primary endpoint, the between-group difference in the change from baseline to 12 weeks for the HAQ-DI, was not statistically significant (p = 0.663) (see Table 3). However, further analysis revealed a clinically relevant intra-group difference over time (Figure 2); the minimum clinically important difference (MCID) in RCTs currently being a change of 0.22–0.25 in the HAQ-DI (34, 35). The intervention group achieved a HAQ-DI reduction of-−0.24 ± 0.22 already at day 7 of the fast, which was sustained throughout the whole study period up until week 12 (Δ- 0.29 ± 0.38) and even to the 6-month follow-up (Δ-0.29 ± 0.37, Figure 2A). In the DGE group a similar functional enhancement was seen from study week 6 on (Δ-0.24 ± 0.49) up to 6 months (Δ-0.21 ± 0.44).
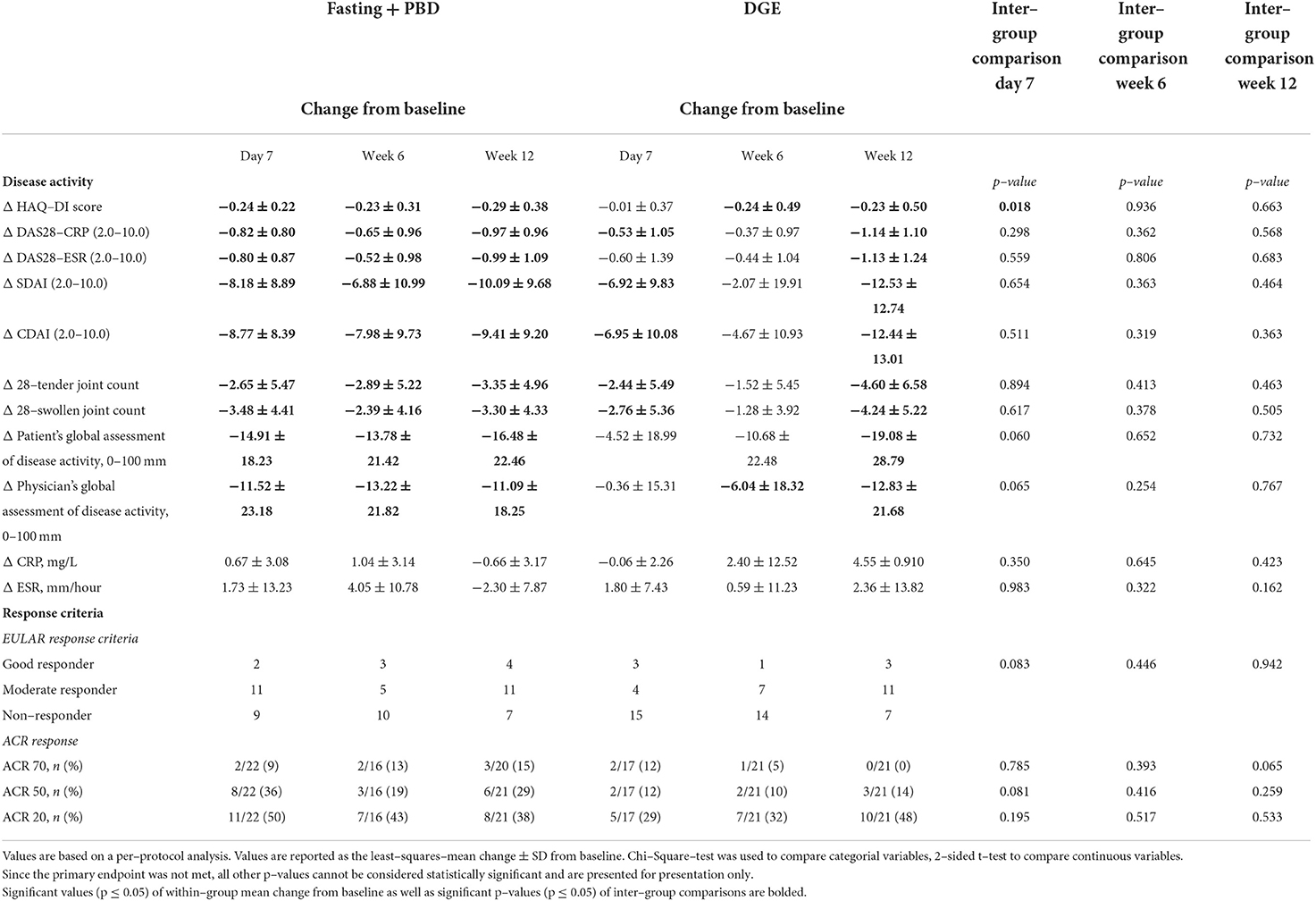
Table 3. Efficacy outcome change from baseline to day 7, week 6 and 12 for both treatment arms.
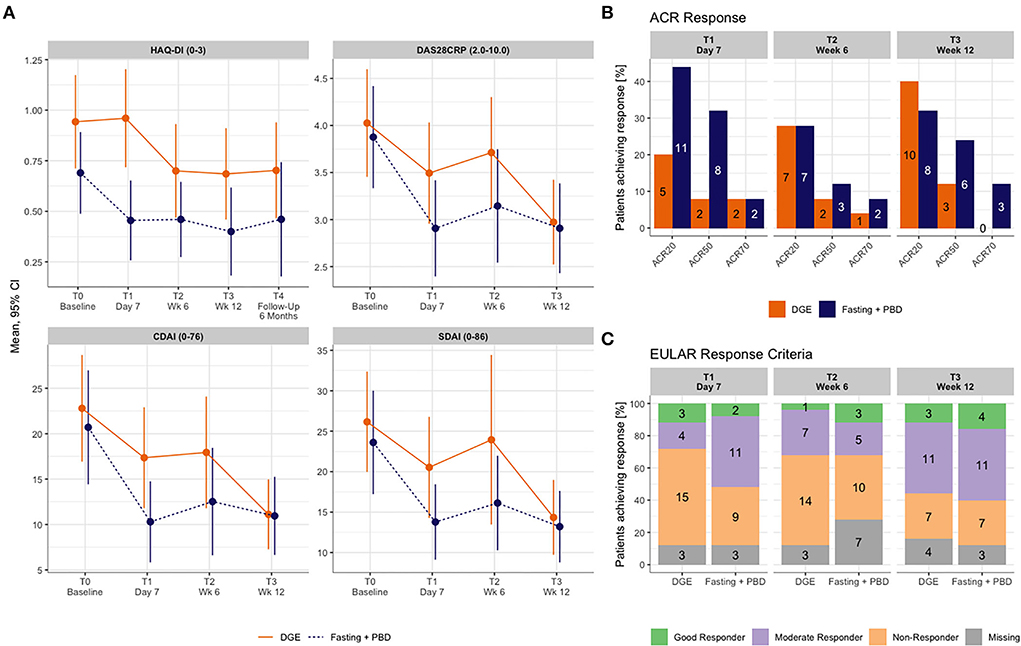
Figure 2. (A) HAQ-DI until 6 months and disease activity outcomes until week 12. (B) EULAR response until week 12. (C) ACR Response until week 12. ACR, American College of Rheumatology; CDAI, clinical disease activity score; CI, confidence interval; DAS28CRP, disease activity score 28 with CRP; DGE, Deutsche Gesellschaft für Ernährung (German society for nutrition); HAQ-DI, health assessment questionnaire disability index; PBD, plant-based diet; SDAI, simplified disease activity index.
Post-hoc sensitivity analysis of the primary endpoint did not detect any correlations with antibody status, prior dietary habit, naturopathic treatment, and mode of dietary coaching (online vs. personal contact; see Supplementary File 1); however, data should be interpreted cautiously due to small subgroups.
Changes from baseline in disease activity followed a similar pattern as the primary outcome. DAS28CRP, DAS28ESR, SDAI and CDAI declined in the fasting and PBD group after 7 days and remained stable throughout the whole study period (Figure 2A). Disease activity in the DGE group declined by day 7, reverted slightly by week 6, and dropped significantly by week 12.
Fasting and PBD participants responded earlier to the dietary intervention (n = 13 of good and moderate EULAR response, n = 10 of ACR50 or higher response at day 7) compared with participants of the DGE group (n = 7 of good and moderate EULAR response, n = 4 of ACR50 or higher at day 7). By week 12, the fasting and PBD group still achieved a better response rate in the ACR response criteria (n = 9 and n = 3 with ACR50 or higher response, Figure 2B); however, by EULAR criteria, both intervention performed similarly (n = 15 and n = 14 with good and moderate EULAR response, respectively, Figure 2C).
Lower scores in the profile of mood states indicated stabilization of emotions during the study period (Supplementary File 3, 4). Overall quality of life, measured by the WHO-Five Well-Being Index (WHO5), decreased by approximately 10 percentage points in the fasting and PBD group, with a significant difference from the DGE group at 6 months.
Results of both groups indicated a trend toward decreasing CRP and ESR levels over 12 weeks (Table 3, Supplementary File 4). As previously described, liver enzymes, uric acid, and non-HDL cholesterol rose substantially during the fast and declined to normal levels after resuming a normocaloric diet, here by week 6 (Supplementary File 5). In the fasting and PBD group, eosinophiles and reticulocytes dropped during fasting (day 7) but returned to baseline values afterwards. Lymphocytes sank during the PBD while the leukocyte count remained stable. Vitamin B12 levels decreased in the fasting and PBD group within the reference range during the study period.
Participants in the fasting and PBD group achieved a clinically relevant weight loss (-4.5 kg) by week 6, which they maintained until the end of the study period (-3.9 kg), compared to the control group (−0.8 and −0.7 kg, respectively) (Figures 3A,B). Waist-to-hip-ratio (WHR) improved and both groups reached the reference range of normal weight with no significant between-group difference. Neither dietary protocol lowered systolic blood pressure nor heart rate within 12 weeks. Yet fasting seemed to favorably affect diastolic blood pressure (Figure 3B). Blood lipids and fasting glucose were also positively influenced by fasting and PBD by 3 months. Triglycerides, total, non-HDL- and LDL-Cholesterol were considerably reduced by week 6 through week 12. Fasting glucose considerably lowered within the standard range by day 7 of the fast and normalized through week 12 (Figure 3C, Supplementary File 5).
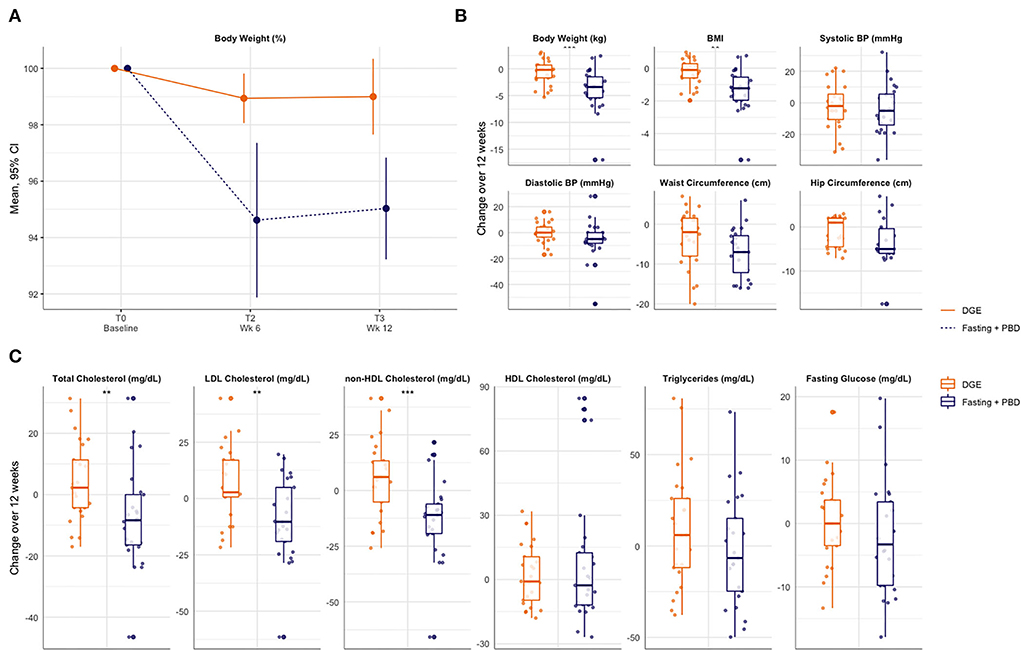
Figure 3. Cardiovascular risk profile through 12 weeks. (A) Relative change in body weight until week 12. (B) Change in clinical cardiovascular risk factors until week 12. (C) Change in laboratory cardiovaskular risk factors until week 12. BMI, body mass index; BP, blood pressure; DGE, Deutsche Gesellschaft für Ernährung (German society for nutrition); PBD, plant-based diet.
We observed one non-treatment emerged serious adverse event unlikely to be associated with the intervention (partial kidney resection) in the fasting and PBD group and no deaths in any of the groups (Supplementary File 6). Sixteen adverse events (AE) occurred in 10 participants (40%) undergoing fasting and PBD, and 9 AEs occurred in 6 participants (24%) consuming a DGE diet. No participants withdrew from the trial due to any AEs, which included diarrhea, paraesthesia, and fatigue. No major change in basic medication was made (Supplementary File 7).
In this study, we presented a dietary therapeutic approach for patients with RA involving prolonged fasting followed by a plant-based diet and evaluated its effects compared with an anti-inflammatory diet according to the DGE.
Regarding the primary endpoint, the change in HAQ-DI from baseline to 12 weeks, we found no significant inter-group difference of fasting followed by a plant-based diet to an anti-inflammatory guideline-based diet.
Having a look at within-group differences, fasting alleviated the subjective disease activity rapidly within 7 days. This gain was maintained through a PBD for up to 6 months and was not influenced by antibody status, delivery mode of the intervention or previous dietary patterns. The conventional guideline-based anti-inflammatory diet caused similar benefits by week 12, but at a slower rate. Regarding CV risk factors, fasting and PBD seem to reduce body weight and blood lipids in a sustainable way. Fasting and PBD resulted in a decrease of vitamin B12 levels within the reference range over 12 weeks.
We were able to observe improvement in RA disease activity by fasting which had been documented in previous trials (22, 23, 36, 37). At day 7, a clear difference to the anti-inflammatory DGE diet could be seen, which highlights the rapid onset of fasting effects. This characteristic suggests the suitability of fasting as a possible element of a short-term therapy i) for acute RA flares and ii) for patients preferring short-term rather than long-term changes in diet. Our data are consistent with other dietary interventions in RA, such as the ADIRA diet, which have led to similar effects in the mid-term above minimal important differences (MID) (13, 35).
Put into context of conventional therapies, we may have observed little effects on RA disease activity, possibly due to the comparatively strong impact of medication as well as an optimized lifestyle among our participants. This includes a previous diet including an already favorable omega-3 (Ω3) to omega-6 (Ω6) fatty acid ratio (38). Omega-3 fatty acids are known to reduce antibody-production in lupus-prone mice and inflammatory mediators (39, 40).
All-cause mortality among patients with RA is 54% higher than the general population, mostly due to CV disease. The underlying pathophysiological mechanisms of systemic inflammation in the CV system, such as elevated oxidative stress, endothelial dysfunction, and changes in lipid profiles, overlap with those of common CV risk factors and comorbidities of RA. For optimal CV disease management these risk factors need to be addressed. Here, patients undergoing fasting achieved clinically relevant weight loss and reduction in waist circumference which they maintained by a PBD including TRE. Owing to not measuring weight directly after fasting, we cannot differentiate between weight loss caused by prolonged fasting or PBD and TRE, both being known for their weight-lowering effectiveness. We observed ameliorated levels of atherogenic lipoproteins, as previously described by Grundler et al. (41). One could speculate whether further determinants such as the gut-derived metabolite trimethylamine N-oxide (TMAO) are favorably affected by long-term fasting and PBD. TMAO serum levels have been linked to CV disease and possible mechanisms such as impaired cholesterol transport, glucose tolerance, and insulin signaling (42). Intermittent fasting appears to reduce TMAO levels, either by diminishing the microbiota count or depriving TMAO precursors, namely animal-based protein (43, 44). These factors may also apply to long-term fasting and PBD.
A plant-based diet is known to lower vitamin B12 levels as it mainly occurs in animal products nowadays (45). Since vitamin B12 stores remain stable for up to several years, we did not substitute during the study and monitored serum levels after 12 weeks (46). As expected, these decreased significantly, but were still within the reference range. However, vitamin B12 would have to be substituted in the case of a permanent purely plant-based diet for more than 3 months.
Regarding inflammatory parameters, eosinophils sank while fasting as well as lymphocyte counts during the following PBD. The reduction in lymphocytes and white blood cells has also been documented in a randomized pilot-trial for a fasting-mimicking diet and ketogenic diet in patients with multiple sclerosis (47). This phenomenon falls in line with recent observations on T and B cells in murine models. Collins et al. demonstrated homing of memory T cells to the bone marrow in response to a 50% dietary restriction; hence plasma lymphocyte levels decreased, survival and protective function enhanced, and mTOR signaling declined (48). Choi et al. observed that a fasting mimicking diet increased the apoptosis rate of autoimmune T lymphocytes in a murine model for multiple sclerosis (26, 47). Nagai et al. reported on emptying B-cell pools in peyer's patches in short-term fasting either due to migration to the bone marrow (naive B-cells) or to apoptosis (germinal center and IgA+ B-cells). Upon refeeding, peyer's patches are replenished with naïve B-cells (49). Given that a vegan diet did not affect lymphocyte count in a study on a PBD in healthy participants, fasting rather than PBD might have caused this cell decline (28). Therefore, we speculate that dietary interventions, such as fasting, provide a supportive state for immune cells also in rheumatic diseases, although further investigation is required to test this hypothesis.
This study has several limitations. First, as most behavioral therapies, full blinding was not possible. For practical reasons, recruitment only took place in Berlin and surroundings, impairing generalization of our findings. Due to the Covid-19 pandemic and slower recruitment than expected we did not reach the calculated sample size. Both intervention groups consisted mainly of women, typical for RA but also a problem of dietary trials; our findings may therefore not apply to men with RA. The investigated population was healthy enough to complete an outpatient fasting program; hence our results might not be generalizable to more vulnerable individuals with RA, such as those having severe comorbidities and sarcopenia. Furthermore, we did not have any restrictions regarding disease activity, possibly resulting in a study population with too low or heterogeneous disease activity to achieve clinically relevant improvement. Despite randomization, the intervention groups differed significantly in their baseline HAQ-DI values, which is why we analyzed all outcomes regarding their performance over time. For ethical reasons and patient recruitment, we enrolled patients regardless of their pharmacologic therapies except that therapy had to have been stable for at least 8 weeks.
Lastly, both studied dietary forms may resemble each other to a certain extent, except from fasting, as both a plant-based diet and the DGE recommendations reduce the intake of AA. In previous studies other dietary concepts with reduced AA consumption alleviated RA symptoms, albeit not reaching statistical significance (13, 50).
In summary, our results show that both interventions, fasting followed by PBD and an anti-inflammatory DGE diet, improve functionality (HAQ-DI) and disease activity (DAS28/CDAI/SDAI) in RA and are not significantly different in the long term, but fasting acts faster. Relevant clinical improvements were seen within both dietary arms over the length of the study period, also in case of remote dietary counseling sessions. Hence, this trial supports the idea of dietary interventions as low-cost supportive elements to be included in an integrative therapeutic approach for patients with RA.
Further clinical studies are necessary to confirm our findings. A larger sample size and a more sensitive primary endpoint that could also be assessed after a longer follow-up period, e.g., one year, would be desirable. The study design could ideally include a third comparison arm that does not receive a therapeutic intervention. In addition, it would be of interest to incorporate patient treatment preference into the study design, as this could increase the attractiveness of study participation. It would also be interesting to investigate whether patients in an acute RA flare benefit from fasting.
This exploratory study is a first approach to generate a dietary therapeutic concept for patients with RA involving prolonged fasting. There was no benefit of fasting followed by a plant-based diet regarding function and disability compared to a guideline-based anti-inflammatory diet after 12 weeks. However, fasting effects on disease activity set in more rapidly already by day 7. Both dietary concepts positively impacted RA disease activity and cardiovascular risk factors.
In clinical practice, some patients with RA are asking for ways to actively participate in treating their disease. Our data provide a starting point for confirmatory studies that need to validate such approaches with larger sample sizes. Further studies on the suitability of fasting as a possible element of a short-term therapy i) for acute RA flares and ii) for patients preferring short-term rather than long-term dietary interventions would be of scientific interest as well.
Because side effects of such dietary interventions are rare, the two nutritional approaches presented here can be offered to patients in clinical contexts. These can then be tested according to individual preferences and interest.
The results of this study can contribute to personalized medical approaches for patients with RA.
Data are available upon request. Requests on data sharing can be made by contacting the corresponding author. Data will be shared after review and approval by the trial scientific board, and terms of collaboration will be reached together with a signed data access agreement.
The studies involving human participants were reviewed and approved by Institutional Ethics Committee of Charité—Universitätsmedizin Berlin. The patients/participants provided their written informed consent to participate in this study.
AMH, MD, TH, AM, DK-L, and CK designed the study. AMH, MD, MS, AM, DK-L, and CK developed the interventional concept. TH and AM procured funding. AMH, MD, MS, and JMF were responsible for patient recruitment and clinical data acquisition. AMH, NS, and FK analyzed the clinical data. AMH, MD, JMF, NS, MJ, FK, AM, DK-L, and CK interpreted the results. AMH wrote the initial draft of the manuscript and coordinated the editing process. MD, MS, JMF, NS, MJ, TH, FK, AM, DK-L, and CK contributed equally with edits, comments, and feedback. All authors read and approved the final manuscript.
Supported by Corona Foundation (Corona Stiftung, Deutsches Stiftungszentrum Essen), grant number S199/10063/2016.
The results were presented in part at the European Congress of Rheumatology 2022, Copenhagen, Denmark (1–4 June) and published as a conference abstract (abstract number POS0583). We would like to show our gratitude to all participating patients as well as to all cooperating rheumatologists for supporting patient recruitment. We thank our study nurses Nadine Sylvester and Miriam Rösner for their excellent assistance in study organization and data collection; Alexandra Pruess and Jessica Torres for assisting with dietary consultation; and Dr. Dania Schumann for her contribution in designing this trial. Thanks to Wolfgang Keicher, AHG Ayurveda Handels GmbH, Hamburg and Seyfrieds Naturwaren, Osnabrück for donating Pippali (Piper longum).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnut.2022.1030380/full#supplementary-material
Supplementary File 1. Post-hoc sensitivity analysis of the primary endpoint regarding antibody status, prior dietary habit, naturopathic treatment, and mode of dietary coaching (online vs. personal contact).
Supplementary File 2. Patient reported outcome measures including WHO5, Cohen perceived stress scale and profile of mood states over 6 months.
Supplementary File 3. Patient reported outcome measures including WHO5, Cohen perceived stress scale and profile of mood states over 6 months.
Supplementary File 4. CRP levels, ESR levels, swollen and tender joint count over 12 weeks.
Supplementary File 5. Laboratory results over 12 weeks.
Supplementary File 6. Overview of adverse events.
Supplementary File 7. Medication during the study period.
ACR20/50/70, American College of Rheumatology response; AE, adverse event; CV, cardiovascular; CDAI, Clinical Disease Activity Index; CrP, c-reactive protein; CPSS-10, Cohen's Perceived Stress Scale; DGE, German society for nutrition (Deutsche Gesellschaft für Ernährung); DAS28, Disease Activity Score 28; DMARD, disease-modifying antirheumatic drug; ESR, erythrocyte sedimentation rate; HAQ-DI, Health Assessment Questionnaire Disability Index; MCID, minimum clinically important difference; MID, minimal important difference; PBD, plant-based diet; RA, rheumatoid arthritis; POMS, Profile of Mood State; PPT, per-protocol treatment; RCT, randomized controlled trial; SDAI, Simplified Disease Activity Index; TMAO, trimethylamine N-oxide; TRE, time-restricted eating; VAS, visual analog scale; WHR, Waist-to-hip-ratio.
1. Global regional and and national age-sex-specific mortality for 282 causes of death in 195 countries and territories 1980-2017: 1980-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. (2018) 392:1736–88. doi: 10.1016/S0140-6736(18)32203-7
2. Hsieh PH, Wu O, Geue C, McIntosh E, McInnes IB, Siebert S. Economic burden of rheumatoid arthritis: a systematic review of literature in biologic era. Ann Rheum Dis. (2020). doi: 10.1136/annrheumdis-2019-216243
3. Smolen JS, Aletaha D. Rheumatoid arthritis therapy reappraisal: strategies, opportunities and challenges. Nat Rev Rheumatol. (2015) 11:276–89. doi: 10.1038/nrrheum.2015.8
4. Scherer HU, Häupl T, Burmester GR. The etiology of rheumatoid arthritis. J Autoimmun. (2020) 110:102400. doi: 10.1016/j.jaut.2019.102400
5. Dehner C, Fine R, Kriegel MA. The microbiome in systemic autoimmune disease: mechanistic insights from recent studies. Curr Opin Rheumatol. (2019) 31:201–7. doi: 10.1097/BOR.0000000000000574
6. Ruff WE, Greiling TM, Kriegel MA. Host–microbiota interactions in immune-mediated diseases. Nat Rev Microbiol. (2020) 18:521–38. doi: 10.1038/s41579-020-0367-2
7. Scher JU, Littman DR, Abramson SB. Review: microbiome in inflammatory arthritis and human rheumatic diseases. Arthritis Rheumatol. (2016) 68:35–45. doi: 10.1002/art.39259
8. Manasson J, Blank RB, Scher JU. The microbiome in rheumatology: Where are we and where should we go? Annal Rheumatic Dis. (2020) 79:727–733. doi: 10.1136/annrheumdis-2019-216631
9. Smiljanovic B, Grützkau A, Sörensen T, Grün JR, Vogl T, Bonin M, et al. Synovial tissue transcriptomes of long-standing rheumatoid arthritis are dominated by activated macrophages that reflect microbial stimulation. Scientific Rep. (2020) 10:4. doi: 10.1038/s41598-020-64431-4
10. Xu H, Zhao H, Fan D, Liu M, Cao J, Xia Y, et al. Interactions between gut microbiota and immunomodulatory cells in rheumatoid arthritis. Mediators Inflamm. (2020) 2020:1430605. doi: 10.1155/2020/1430605
11. Wastyk HC, Fragiadakis GK, Perelman D, Dahan D, Merrill BD, Yu FB, et al. Gut-microbiota-targeted diets modulate human immune status. Cell. (2021) 184:4137–53.e14. doi: 10.1016/j.cell.2021.06.019
12. Luongo D, Treppiccione L, Sorrentino A, Ferrocino I, Turroni S, Gatti M, et al. Immune-modulating effects in mouse dendritic cells of lactobacilli and bifidobacteria isolated from individuals following omnivorous, vegetarian and vegan diets. Cytokine. (2017) 97:141–8. doi: 10.1016/j.cyto.2017.06.007
13. Vadell AKE, Bärebring L, Hulander E, Gjertsson I, Lindqvist HM, Winkvist A. Anti-inflammatory diet in rheumatoid arthritis (ADIRA)-a randomized, controlled crossover trial indicating effects on disease activity. Am J Clin Nutr. (2020) 111:1203–13. doi: 10.1093/ajcn/nqaa019
14. Häger J, Bang H, Hagen M, Frech M, Träger P, Sokolova MV, et al. The role of dietary fiber in rheumatoid arthritis patients: a feasibility study. Nutrients. (2019) 11:2392. doi: 10.3390/nu11102392
15. Tedeschi SK, Costenbader KH. Is there a role for diet in the therapy of rheumatoid arthritis? Current Rheumatol Rep. (2016) 18:575. doi: 10.1007/s11926-016-0575-y
16. Khanna S, Jaiswal KS, Gupta B. Managing rheumatoid arthritis with dietary interventions. Front Nutr. (2017) 4:52. doi: 10.3389/fnut.2017.00052
17. Minamino H, Katsushima M, Hashimoto M, Fujita Y, Torii M, Ikeda K, et al. Influence of dietary habits on depression among patients with rheumatoid arthritis: A cross-sectional study using KURAMA cohort database. PLoS ONE. (2021) 16:e0255526. doi: 10.1371/journal.pone.0255526
18. Towery P, Guffey JS, Doerflein C, Stroup K, Saucedo S, Taylor J. Chronic musculoskeletal pain and function improve with a plant-based diet. Complement Ther Med. (2018) 40:64–9. doi: 10.1016/j.ctim.2018.08.001
19. Liao KP. Cardiovascular disease in patients with rheumatoid arthritis. Trends Cardiovasc Med. (2017) 27:136–40. doi: 10.1016/j.tcm.2016.07.006
20. Hansildaar R, Vedder D, Baniaamam M, Tausche AK, Gerritsen M, Nurmohamed MT. Cardiovascular risk in inflammatory arthritis: rheumatoid arthritis and gout. Lancet Rheumatol. (2021) 3:e58–70. doi: 10.1016/S2665-9913(20)30221-6
21. Daien C, Czernichow S, Letarouilly J-G, Nguyen Y, Sanchez P, Sigaux J, et al. Dietary recommendations of the French Society for Rheumatology for patients with chronic inflammatory rheumatic diseases. Joint Bone Spine. (2022) 89:105319. doi: 10.1016/j.jbspin.2021.105319
22. Kjeldsen-Kragh J, Borchgrevink CF, Laerum E, Haugen M, Eek M, Førre O, et al. Controlled trial of fasting and one-year vegetarian diet in rheumatoid arthritis. Lancet. (1991) 338:899–902. doi: 10.1016/0140-6736(91)91770-U
23. Sköldstam L, Larsson L, Lindström FD. Effect of fasting and lactovegetarian diet on rheumatoid arthritis. Scand J Rheumatol. (1979) 8:249–55. doi: 10.3109/03009747909114631
24. De Cabo R, Mattson MP. Effects of intermittent fasting on health, aging, and disease. N Eng J Med. (2019) 381:2541–51. doi: 10.1056/NEJMra1905136
25. Valter, Mark. Fasting: molecular mechanisms and clinical applications. Cell Metab. (2014) 19:181–92. doi: 10.1016/j.cmet.2013.12.008
26. Choi IY, Lee C, Longo VD. Nutrition and fasting mimicking diets in the prevention and treatment of autoimmune diseases and immunosenescence. Mol Cell Endocrinol. (2017) 455:4–12. doi: 10.1016/j.mce.2017.01.042
27. Sköldstam L. Fasting and vegan diet in rheumatoid arthritis. Scand J Rheumatol. (1986) 15:219–21. doi: 10.3109/03009748609102091
28. Lederer AK, Maul-Pavicic A, Hannibal L, Hettich M, Steinborn C, Gründemann C, et al. Vegan diet reduces neutrophils, monocytes and platelets related to branched-chain amino acids - a randomized, controlled trial. Clin Nutr. (2020). doi: 10.1016/j.clnu.2020.02.011
29. Craddock JC, Neale EP, Peoples GE, Probst YC. Vegetarian-based dietary patterns and their relation with inflammatory and immune biomarkers: a systematic review and meta-analysis. Adv Nutr. (2019) 10:433–51. doi: 10.1093/advances/nmy103
30. Tomova A, Bukovsky I, Rembert E, Yonas W, Alwarith J, Barnard ND, et al. The effects of vegetarian and vegan diets on gut microbiota. Front Nutr. (2019) 6:47. doi: 10.3389/fnut.2019.00047
31. Aleksandrova K, Koelman L, Rodrigues CE. Dietary patterns and biomarkers of oxidative stress and inflammation: a systematic review of observational and intervention studies. Redox Biol. (2021) 42:101869. doi: 10.1016/j.redox.2021.101869
32. Sutliffe JT, Wilson LD, de Heer HD, Foster RL, Carnot MJ. C-reactive protein response to a vegan lifestyle intervention. Complement Ther Med. (2015) 23:32–7. doi: 10.1016/j.ctim.2014.11.001
33. Hartmann AM, Dell'Oro M, Kessler CS, Schumann D, Steckhan N, Jeitler M, et al. Efficacy of therapeutic fasting and plant-based diet in patients with rheumatoid arthritis (NutriFast): study protocol for a randomised controlled clinical trial. BMJ Open. (2021) 11:e047758. doi: 10.1136/bmjopen-2020-047758
34. Orbai AM, Bingham CO. 3rd. Patient reported outcomes in rheumatoid arthritis clinical trials. Curr Rheumatol Rep. (2015) 17:28. doi: 10.1007/s11926-015-0501-8
35. Kitchen H, Hansen B, Abetz L, Højbjerre L, Strandberg-Larsen M. Patient-reported outcome measures for rheumatoid arthritis: minimal important differences review. Arthritis Rheumatol. (2013) 65:965. Available online at: https://acrabstracts.org/abstract/patient-reported-outcome-measures-for-rheumatoid-arthritis-minimal-important-differences-review/
36. Trang LE, Lövgren O, Norlund AE, Horn R, Walaas O. Cyclic nucleotides and catecholamines in rheumatoid arthritis. Scand J Rheumatol. (1983) 12:171–6. doi: 10.3109/03009748309102906
37. Udén AM, Trang L, Venizelos N, Palmblad J. Neutrophil functions and clinical performance after total fasting in patients with rheumatoid arthritis. Ann Rheum Dis. (1983) 42:45–51. doi: 10.1136/ard.42.1.45
38. Hemshekhar M, Anaparti V, El-Gabalawy H, Mookherjee N. A bioavailable form of curcumin, in combination with vitamin-D- and omega-3-enriched diet, modifies disease onset and outcomes in a murine model of collagen-induced arthritis. Arthritis Res Ther. (2021) 23:39. doi: 10.1186/s13075-021-02423-z
39. Rajasinghe LD Li QZ, Zhu C, Yan M, Chauhan PS, Wierenga KA, et al. Omega-3 fatty acid intake suppresses induction of diverse autoantibody repertoire by crystalline silica in lupus-prone mice. Autoimmunity. (2020) 53:415–33. doi: 10.1080/08916934.2020.1801651
40. Jiang J, Li K, Wang F, Yang B, Fu Y, Zheng J, et al. Effect of marine-derived n-3 polyunsaturated fatty acids on major eicosanoids: a systematic review and meta-analysis from 18 randomized controlled trials. PLoS ONE. (2016) 11:e0147351. doi: 10.1371/journal.pone.0147351
41. Grundler F, Plonné D, Mesnage R, Müller D, Sirtori CR, Ruscica M, et al. Long-term fasting improves lipoprotein-associated atherogenic risk in humans. Eur J Nutr. (2021). doi: 10.1007/s00394-021-02578-0
42. Tang WHW, Wang Z, Levison BS, Koeth RA, Britt EB, Fu X, et al. Intestinal microbial metabolism of phosphatidylcholine and cardiovascular risk. NEng J Med. (2013) 368:1575–84. doi: 10.1056/NEJMoa1109400
43. Washburn RL, Cox JE, Muhlestein JB, May HT, Carlquist JF, Le VT, et al. Pilot study of novel intermittent fasting effects on metabolomic and trimethylamine N-oxide changes during 24-hour water-only fasting in the FEELGOOD trial. Nutrients. (2019) 11:20246. doi: 10.3390/nu11020246
44. Thomas MS, Fernandez ML. Trimethylamine N-Oxide (TMAO), diet and cardiovascular disease. Curr Atheroscler Rep. (2021) 23:12. doi: 10.1007/s11883-021-00910-x
45. Neufingerl N, Eilander A. Nutrient intake and status in adults consuming plant-based diets compared to meat-eaters: a systematic review. Nutrients. (2022) 14:29. doi: 10.3390/nu14010029
46. Herrmann W, Obeid R. Ursachen und frühzeitige Diagnostik von Vitamin-B12-Mangel. Dtsch Arztebl Int. (2008) 105:680–5. doi: 10.3238/arztebl.2008.0680
47. Choi IY, Piccio L, Childress P, Bollman B, Ghosh A, Brandhorst S, et al. A diet mimicking fasting promotes regeneration and reduces autoimmunity and multiple sclerosis symptoms. Cell Rep. (2016) 15:2136–46. doi: 10.1016/j.celrep.2016.05.009
48. Collins N, Han S-J, Enamorado M, Link VM, Huang B, Moseman EA, et al. The bone marrow protects and optimizes immunological memory during dietary restriction. Cell. (2019) 178:1088–101.e15. doi: 10.1016/j.cell.2019.07.049
49. Nagai M, Noguchi R, Takahashi D, Morikawa T, Koshida K, Komiyama S, et al. Fasting-refeeding impacts immune cell dynamics and mucosal immune responses. Cell. (2019) 178:1072–87.e14. doi: 10.1016/j.cell.2019.07.047
Keywords: rheumatoid arthritis, fasting, caloric restriction, plant-based diet, inflammation
Citation: Hartmann AM, Dell'Oro M, Spoo M, Fischer JM, Steckhan N, Jeitler M, Häupl T, Kandil FI, Michalsen A, Koppold-Liebscher DA and Kessler CS (2022) To eat or not to eat—an exploratory randomized controlled trial on fasting and plant-based diet in rheumatoid arthritis (NutriFast-Study). Front. Nutr. 9:1030380. doi: 10.3389/fnut.2022.1030380
Received: 28 August 2022; Accepted: 28 September 2022;
Published: 02 November 2022.
Edited by:
Annunziata Nancy Crupi, University of Southern California, United StatesReviewed by:
Yasmin Y. Algindan, Imam Abdulrahman Bin Faisal University, Saudi ArabiaCopyright © 2022 Hartmann, Dell'Oro, Spoo, Fischer, Steckhan, Jeitler, Häupl, Kandil, Michalsen, Koppold-Liebscher and Kessler. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Anika M. Hartmann, YW5pa2EuaGFydG1hbm5AY2hhcml0ZS5kZQ==
†These authors have contributed equally to this work and share last authorship
‡ORCID: Anika M. Hartmann orcid.org/0000-0002-0135-9643
Jan Moritz Fischer orcid.org/0000-0002-3495-6495
Nico Steckhan orcid.org/0000-0003-0245-2046
Michael Jeitler orcid.org/0000-0003-3277-9090
Thomas Häupl orcid.org/0000-0002-3792-9724
Farid I. Kandil orcid.org/0000-0003-3071-7902
Andreas Michalsen orcid.org/0000-0002-9145-7246
Daniela A. Koppold-Liebscher orcid.org/0000-0003-3367-3327
Christian S. Kessler orcid.org/0000-0001-7794-8375
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.