 Hexin Su
Hexin Su Yacong Bo
Yacong Bo Xiaoan Zhang3
Xiaoan Zhang3- 1The Fifth Affiliated Hospital of Zhengzhou University, Zhengzhou, China
- 2School of Public Health, Zhengzhou University, Zhengzhou, China
- 3The Third Hospital of Zhengzhou University, Zhengzhou, China
- 4NHC Key Laboratory of Birth Defects Prevention, Henan Key Laboratory of Population Defects Prevention, Zhengzhou, China
Background and aims: The evidence regarding folate intake and mortality risk among patients with type 2 diabetes (T2D) remains unclear. This study aimed to investigate the association of folate intake with the risk of mortality among individuals with T2D.
Methods: A total of 9,196 participants with T2D from the Third National Health and Nutrition Examination Survey (NHANES III) and NHANES 1999–2014 were included. The data of survival were obtained by the cohort database linked with the national death index up to 31 December 2015. The Cox proportional hazard model was used to evaluate the relationship between dietary folate with all-cause and cause-specific mortality.
Results: Among patients with T2D, dietary folate intake was negatively correlated with all-cause mortality, cardiovascular mortality, and cancer mortality in men, and for women with all-cause mortality and cardiovascular mortality. The multivariate adjustment hazard ratio (HR) (95% CIs) for men of highest vs. lowest quartile was 0.77 (0.66–0.90), 0.61 (0.45–0.83), and 0.70 (0.49–0.99) for all-cause, cardiovascular, and cancer mortality, respectively. Among women, the multivariate adjustment HR (95% CIs) of highest vs. lowest quartile was 0.77 (0.64–0.92), 0.52 (0.33–0.83), and 0.78 (0.50–1.22) for all-cause, cardiovascular, and cancer mortality, respectively.
Conclusion: Higher dietary intake of folate was significantly associated with lower all-cause and cardiovascular mortality. This cohort study suggested that increasing the dietary folate intake may reduce mortality risk among U.S. adults with T2D.
Introduction
Folate and its natural derivatives are vitamin B9-based compounds, which are essential micronutrients and are essential for normal cell function. Mammals do not have the ability to synthesize folate and must absorb folate from their diet (1).
Diabetes is one of the most common chronic ailments and a major healthcare problem in worldwide (2). Compared with healthy individuals, previous studies found that patients with T2D had significantly lower circulating folate concentrations (3). And folate has a considerable positive impact on Metabolic syndrome (4), especially diabetes (5, 6). Therefore, it is important to investigate the association of folate with long-term health outcomes in patients with T2D.
Several epidemiological studies have investigated the relationship between dietary folate intake and the risk of death (7–10). Nevertheless, most of these studies were conducted among general population or specific population, such as the elderly and cancer patients. The evidence for patients with diabetes is limited (11–14). Therefore, prospective cohort studies are needed to provide reliable estimates and accurate results for patients with diabetes. To address these research gaps, we prospectively investigated the relationship between folate dietary intake and the risk of all-cause and cause-specific mortality among U.S. patients with T2D, by using national representative sample data from the National Health and Nutrition Examination Survey (NHANES).
Materials and methods
Study population
The NHANES is conducted by the National Center for Health Statistics of the Centers for Disease Control and Prevention (CDC). It is a stratified, multistage, and national survey which uses a representative sample of the non-institutionalized civilian population of the U.S.A. (15). Information on lifestyle factors, health, and dietary folate intake status was collected from each participant. In this research, the data of NHANES III (1988–1994) and NHANES from 1999 to 2014 were used. Participants (aged ≥ 20 years old) with T2D were included. T2D was defined by fasting plasma glucose ≥7.0 mmol/L, and/or hemoglobin HbA1c level >6.5%, and/or self-reported doctor-diagnosed T2D, and/or use of insulin or oral hypoglycemic medication. A total of 9,196 patients with diabetes were included. All participants have received written informed consent.
Measurement of dietary folate intake
Dietary folate data were evaluated by trained interviewers through 24-h dietary recall. During the NHANES III and 1999–2002 survey cycles, participants conducted one single day 24-h dietary recall at the Mobile testing Center (MEC). Since 2003, two dietary recalls have been conducted. The first dietary recall was conducted in-person in MEC, and the second dietary recall was conducted 3–10 days later via telephone. Dietary folate intake was assessed using the U.S. Department of Agriculture (USDA) Food and Nutrient Database for Dietary Studies (FNDDS) version 1.0–5.0 (16).
Ascertainment of mortality
Information on all-cause and cause-specific mortality status was obtained by linking the cohort database with the national death index up to 31 December 2015. The outcomes of the current study were all-cause mortality, cardiovascular mortality, and cancer mortality, which were determined according to the 10th revision of the International Classification of Diseases (ICD-10). Cardiovascular mortality was defined as the ICD-10 code of I00-I09, I11, I13, I20-I51, or I60-I69; and cancer mortality was defined as the ICD-10 code of C00-C97. Each individual's Time-to-event was calculated from the date of recruitment to the date of death or the censor date (31 December 2015), whichever came earlier.
Covariates
The following variables were considered as covariates based on the literature review: age (years), gender (male or female), race (Hispanic, non-Hispanic white, non-Hispanic black, and racial including multi-race), smoking (never, former, or current), alcohol drinking (never, low to moderate, or heavy), the ratio of family income to poverty (≤1, 1–3, or >3), leisure time physical activity [defined as the product of metabolic equivalent value (MET)] and self-reported cardiovascular disease (yes or no) and hypertension (yes or no). Body mass index (BMI) was calculated as weight (kg) divided by height (meters squared).
Statistical analysis
We used numbers (percentages) to describe classified variables and means (standard deviation) to describe continuous variables (17). Cox proportional hazard model was used to evaluate the relationship between dietary folate and all-cause and cause-specific mortality. Dietary folate intake was divided into four quartiles; we selected the first quartile as the reference group, and adopt two different models: not adjusted any variable with the crude model and the multivariate model adjusted for age, leisure time physical activity, ethnicity, BMI, family income, smoking, drinking, hypertension, and cardiovascular disease. Stratified analyses were conducted based on age (<60 years old or ≥60 years old), current smoker (yes or no), current drinker (yes or no), and body mass index (<30 or ≥30 kg/m2). We examined each potential correction factor separately by adding a multiplicative interaction term (i.e., continuous dietary nutrient intake parameter * potential correction factor).
To examine the relationships' robustness, we conducted two sensitivity analyses: (1) excluding participants without cardiovascular disease at baseline and (2) excluding patients who died within 2 years of follow-up. All statistical analyses were conducted using SPSS25.0. The p < 0.05 was considered to be statistically significant.
Results
General characteristics
The general characteristics of the participants are shown in Table 1. A total of 9,196 participants with T2D was included, with an average age of 61.7 (SD: 14.0) years at baseline, 4,507 men (49.01%) and 4,689 (50.99%) women. During a median follow-up of 7.3 years [interquartile range (IQR): 3.8–12.4], 3,495 participants died, including 818 from cardiovascular disease and 607 from cancer. Compared with survivors, participants who died were more likely to be elderly, female, and non-Hispanic white; less likely to be never smoker; and more likely to have hypertension and cardiovascular disease at baseline.
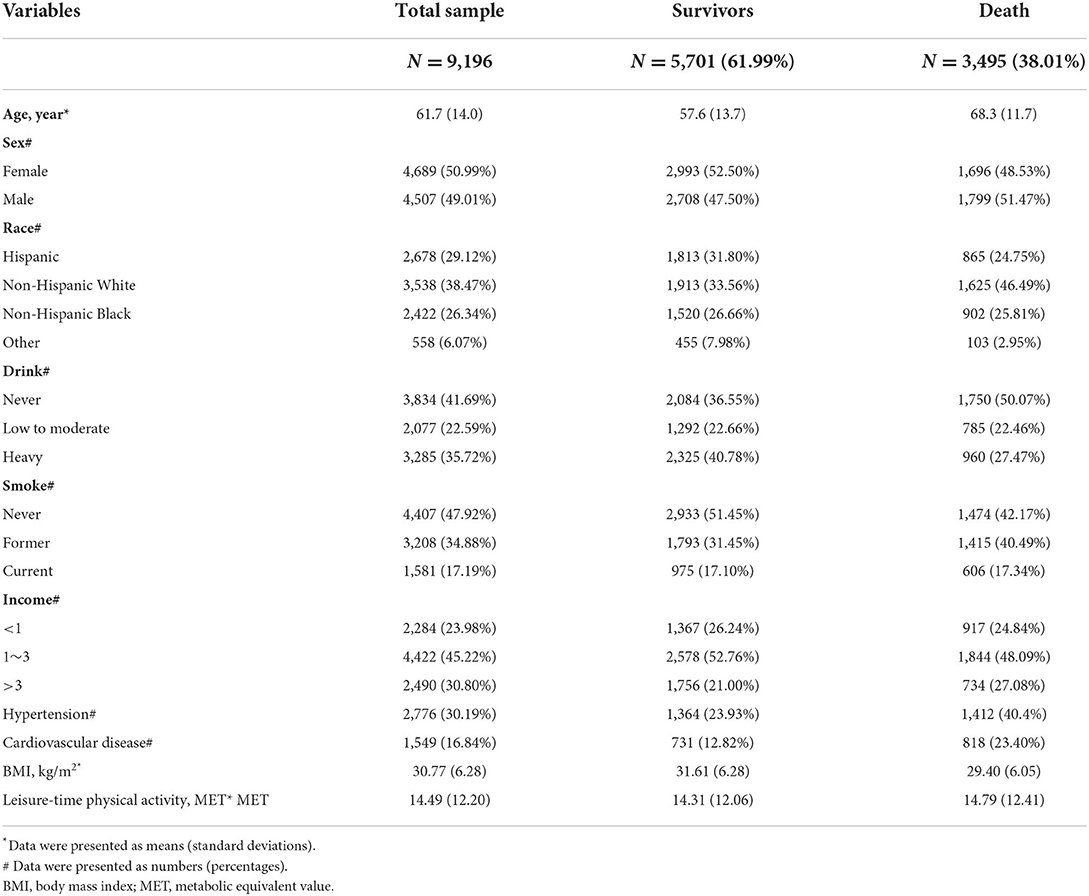
Table 1. Baseline characteristics of the study population.
Dietary folate with all-cause and cause-specific mortality
The sex-specific relationship between dietary folate intake and all-cause and cause-specific mortality among patients with T2D is shown in Table 2. In men, we found that folate intake was negatively correlated with all-cause mortality, cardiovascular mortality, and cancer mortality. The multivariate adjustment hazard ratio (HR) (95% CIs) of men highest vs. lowest quartile was 0.77 (0.66–0.90), 0.61 (0.45–0.83), and 0.70 (0.49–0.99) for all-cause mortality, cardiovascular mortality, and cancer mortality, respectively. In women, folate intake was negatively correlated with all-cause mortality and cardiovascular mortality, but not with cancer mortality. The highest vs. lowest quartile HR (95% CIs) was 0.77 (0.64–0.92), 0.52 (0.33–0.83), and 0.78 (0.50–1.22) for all-cause, cardiovascular, and cancer mortality, respectively.
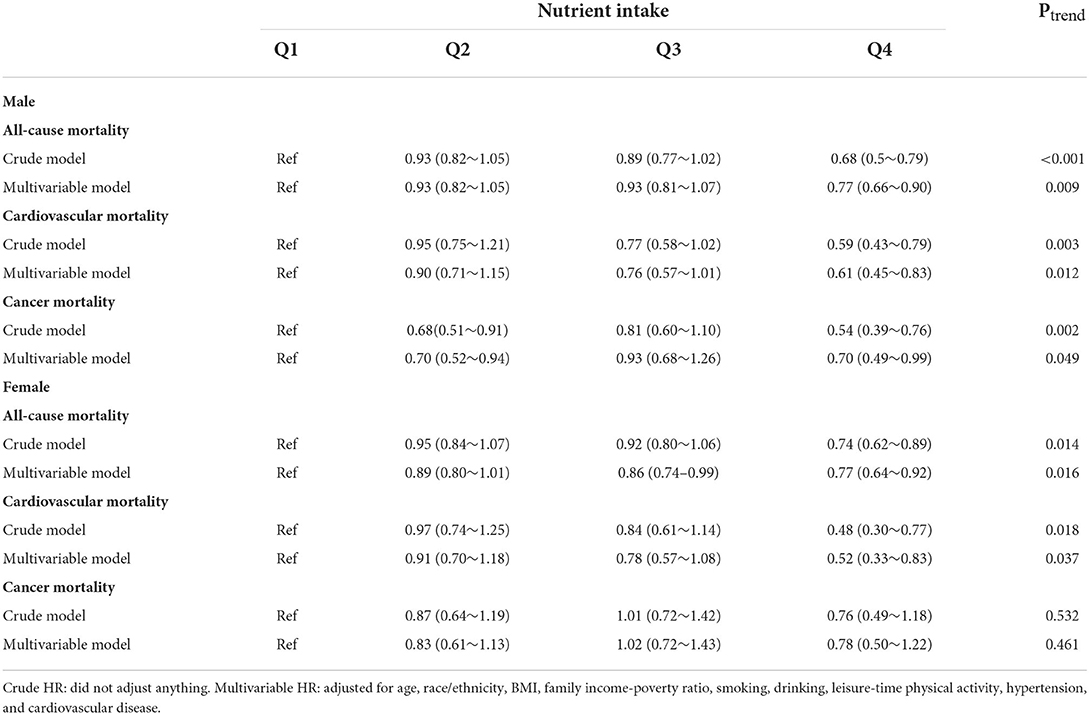
Table 2. Hazard ratio (HRs) and 95% CIs for all-cause and cause-specific mortality according to Quintiles of dietary Folate.
Stratified analyses and sensitivity analysis
The relationships between dietary folate intake and all-cause and cause-specific mortality were generally similar among subgroups, although some differences were not statistically significant, as shown in Table 3. A statistically significant interaction was observed for some factors. We observed that folate intake had a stronger negative correlation with all-cause and cause-specific mortality in the obese men. For female participants, folate intake was negatively correlated with all-cause mortality and cause-specific mortality of recent smoking and drinking patients. Sensitivity analysis showed that the excluding of participants died within 2 years of follow-up (Table 4) or excluding participants who had cardiovascular disease at baseline (Table 5), the significant association between dietary folate and the risk of mortality was still similar.
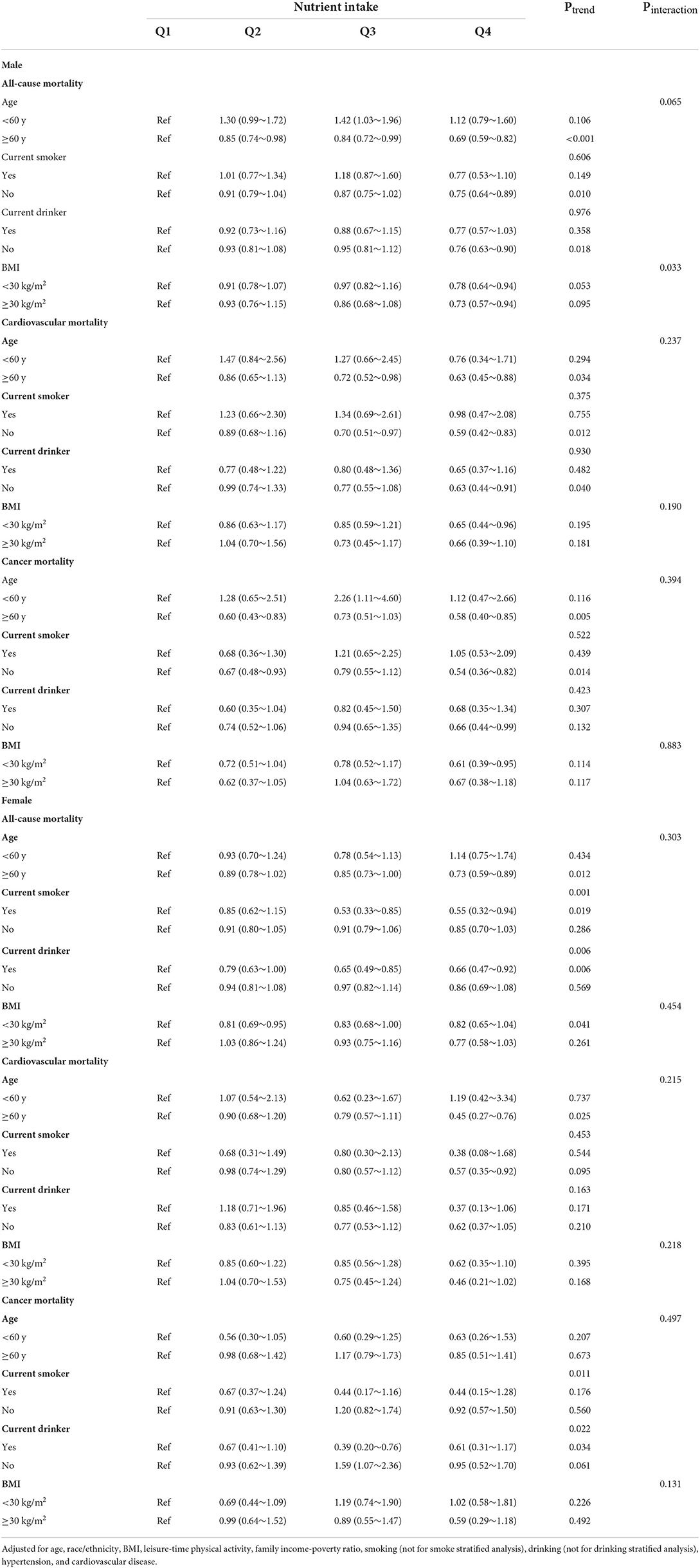
Table 3. Stratified analyses of the associations between dietary folate intake with all-cause and cause-specific mortality.
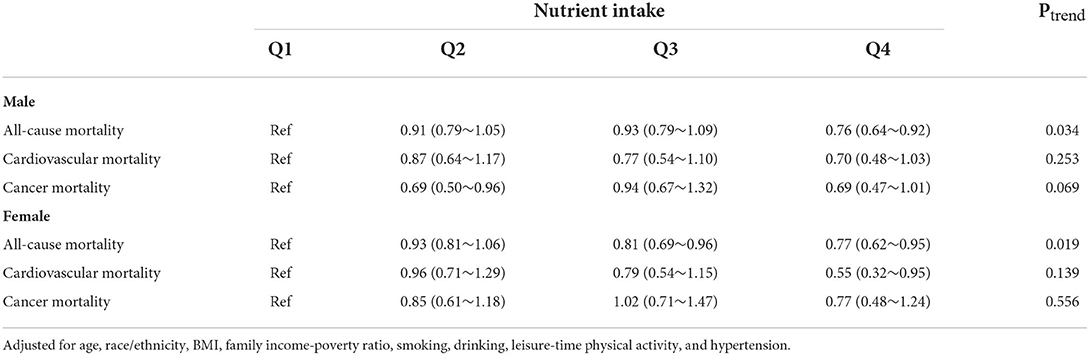
Table 4. Hazard ratio and 95% CIs for all-cause and cause-specific mortality according to quartiles of dietary folate intake after excluding participants with cardiovascular disease at baseline.
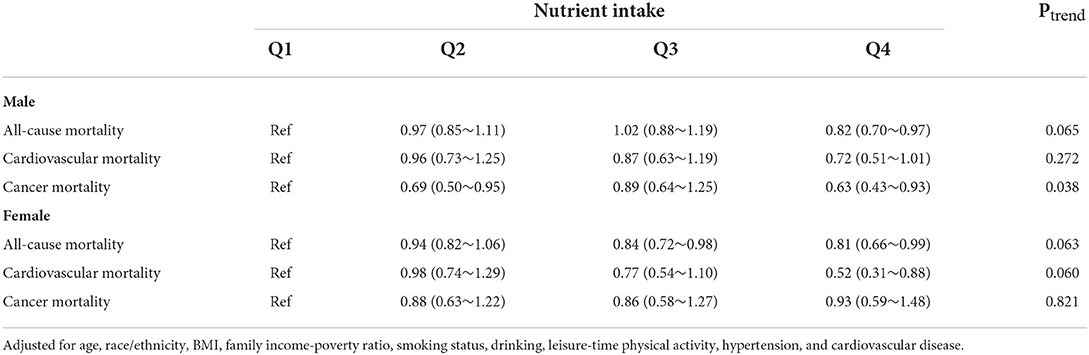
Table 5. Hazard ratios and 95% CIs for all-cause and cause-specific mortality according to quartiles of dietary folate intake after excluding participants who were died within 2 years of follow-up.
Discussion
Our study has shown that, among patients with T2D, dietary folate intake was negatively correlated with all-cause, cardiovascular, and cancer mortality in men, and negatively correlated with all-cause and cardiovascular mortality in women. And the excluding of participants who were died within 2 years of follow-up or those who had cardiovascular disease at baseline, the conclusion did not change. The association might because of glucose homeostasis (18), vascular protection (19, 20), or homocysteine methylation (21, 22) which benefit from dietary folate.
This reverse relationship is consistent with findings from previous studies. A non-linear correlation was found between serum folate levels with CVD morbidity and all-cause mortality in 7,700 American adults with T2D (23). The Swedish cohort study showed that dietary folate intake was negatively correlated with the risk of all-cause mortality among women who were diagnosed with breast cancer (24). A Collaborative Cohort study from Japan found that dietary folate intake was negatively correlated with heart failure mortality in men and coronary heart disease mortality and total cardiovascular mortality in women (25). A Spanish ecological study showed that folate intake was inversely associated with coronary artery disease mortality and cerebrovascular disease mortality in men and cerebrovascular disease mortality in women, and the protective effect is positively correlated with folate intake (26). However, no previous studies investigated the relationship of dietary folate intake with mortality among patients with T2D. In the present study, we found a negative relationship between folate intake and cardiovascular and all-cause mortality among 9,196 U.S. adults with T2D, which provided further evidence for the prevention of premature death in this specific population.
However, it is inconsistent with the results of some related studies in the U.S.A. A study by the American Association of Retirement Diet and Health found no significant relationship between folate intake and liver disease mortality (27). Another study suggested that dietary folate was not associated with breast cancer-specific mortality or all-cause mortality (28). Other studies have shown that serum folate levels are not associated with CVD mortality in participants with T2D (29). These inconsistencies may be caused by series of factors, which include differences of research methods and inadequate data collection, as well as differences in the populations or health outcomes.
In this study, a representative American population was obtained by using a complex, stratified, and multi-stage probability sampling method. The large sample size enabled us to obtain relatively robust and accurate estimates. In addition, based on the comprehensive data collected by NHANES, a wide range of potential confounding factors was adjusted.
Our research also had several limitations. First, dietary folate intake was collected through one or two 24-h dietary recalls at a single point, which may not well-reflect long-term intake because of large changes in daily food intake. In addition, the information of folate intake was evaluated by questionnaire, which may bring recall bias. However, this measurement bias seems to be random, and there is no evidence suggesting that the potential measurement bias is different between the participants who survived and those who died. We thus speculate that this limitation should not affect the study's conclusion. Second, most diabetic patients received different diets and drugs because of their symptoms. Metformin, as the first choice for diabetes, may significantly reduce folate absorption, and critically ill patients may have more folate intake and higher mortality, so the possibility of “causality inversion” can't be ruled out. Third, the level of folate intake varied between different studies, which make it difficult to compare our results with other studies directly. In addition, residues or unknown mixtures cannot be completely excluded.
Conclusion
In conclusion, using the data NHANES, we found that dietary folate intake was negatively correlated with all-cause mortality, cardiovascular mortality, and cancer mortality in men and with all-cause mortality and cardiovascular mortality in women who were diagnosed with T2D. This study suggested the increasing of intake of dietary folate may reduce the risk of mortality in U.S. adults with T2D.
Data availability statement
Publicly available datasets were analyzed in this study. This data can be found at: https://wwwn.cdc.gov/nchs/nhanes/Default.aspx.
Ethics statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. The patients/participants provided their written informed consent to participate in this study.
Author contributions
YB and ZY: conceptualization and supervision. ZG and JZ: methodology. HS: data curation and writing—original draft preparation. HS, YB, and ZY: writing—review and editing. ZY: project administration. All authors contributed to the article and approved the submitted version.
Funding
This work was supported by Special Major Public Welfare Project of Henan Province No. 201300310800 and Open Research Fund of National Health Commission Key Laboratory of Birth Defects Prevention and Henan Key Laboratory of Population Defects Prevention No. ZD202203.
Acknowledgments
The authors sincerely thank the NHANES of the CDC for providing the publicly available data.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Toit AID. Synthetic folic acid - food folate and 5-mthf are not the same thing. Medical Chronicle. (2019 December, 30). Available online at: https://hdl.handle.net/10520/EJC-1370319f85
2. Legenbauer T, Benecke A, Beutel ME. Diabetes Mellitus und Essstörungen: Herausforderungen für die interdisziplinäre Behandlung. Berlin, Boston, MA: De Gruyter (2021). doi: 10.1515/9783110583205
3. Malaguarnera G, Gagliano C, Salomone S, Giordano M, Bucolo C, Pappalardo A, et al. Folate status in type 2 diabetic patients with and without retinopathy. Clin Ophthalmol. (2015) 9:1437–42. doi: 10.2147/OPTH.S77538
4. Ashok T, Puttam H, Tarnate VCA, Jhaveri S, Avanthika C, Trejo Treviño AG, et al. Role of vitamin B12 and folate in metabolic syndrome. Cureus. (2021) 13:e18521. doi: 10.7759/cureus.18521
5. Gargari BP, Aghamohammadi V, Aliasgharzadeh A. Effect of folic acid supplementation on biochemical indices in overweight and obese men with type 2 diabetes. Diabetes Res Clin Pract. (2011) 94:33–8. doi: 10.1016/j.diabres.2011.07.003
6. Asbaghi O, Ashtary-Larky D, Bagheri R, Moosavian SP, Olyaei HP, Nazarian B, et al. Folic acid supplementation improves glycemic control for diabetes prevention and management: a systematic review and dose-response meta-analysis of randomized controlled trials. Nutrients. (2021) 13:2355. doi: 10.3390/nu13072355
7. Danaei G, Ding EL, Mozaffarian D, Taylor B, Rehm J, Murray CJ, et al. The preventable causes of death in the United States: comparative risk assessment of dietary, lifestyle, and metabolic risk factors. PLoS Med. (2009) 6:e1000058. doi: 10.1371/journal.pmed.1000058
8. Zhu J, Chen C, Lu L, Yang K, Reis J, He K. Intakes of folate, vitamin B(6), and vitamin B(12) in relation to diabetes incidence among American young adults: a 30-year follow-up study. Diabetes Care. (2020) 43:2426–34. doi: 10.2337/dc20-0828
9. Xu X, Wei W, Jiang W, Song Q, Chen Y, Li Y, et al. Association of folate intake with cardiovascular-disease mortality and all-cause mortality among people at high risk of cardiovascular-disease. Clin Nutr. (2022) 41:246–54. doi: 10.1016/j.clnu.2021.11.007
10. Bo Y, Xu H, Zhang H, Zhang J, Wan Z, Zhao X, et al. Intakes of folate, vitamin B6, and vitamin B12 in relation to all-cause and cause-specific mortality: a national population-based cohort. Nutrients. (2022) 14:2253. doi: 10.3390/nu14112253
11. El-Khodary NM, Dabees H, Werida RH. Folic acid effect on homocysteine, Sortilin levels and glycemic control in type 2 diabetes mellitus patients. Nutr Diabetes. (2022) 12:33. doi: 10.1038/s41387-022-00210-6
12. Li K, Chen X, Hu Y, Gao B. Folic acid supplementation diminishes diabetes induced neural tube defects by recovering impaired embryo gene expression through its antioxidant activity. J Pharm Res Int. (2021) 33:258–71. doi: 10.9734/jpri/2021/v33i62A35204
13. Hayden MR, Tyagi SC. Impaired folate-mediated one-carbon metabolism in type 2 diabetes, late-onset Alzheimer's disease and long COVID. Medicina. (2021) 58:16. doi: 10.3390/medicina58010016
14. Keerti A, Jankar J. Role of folic acid in type 2 diabetes. J Pharm Res Int. (2021) 33:137–43. doi: 10.9734/jpri/2021/v33i60A34465
15. Archer E, Pavela G, Lavie CJ. The inadmissibility of what we eat in America and Nhanes dietary data in nutrition and obesity research and the scientific formulation of national dietary guidelines. Mayo Clin Proc. (2015) 90:911–26. doi: 10.1016/j.mayocp.2015.04.009
16. U.S. Department of Agriculture Food Surveys Research Group. Food and Nutrient Database for Dietary Studies. Beltsville, Md. Available online at: Https://Www.Ars.Usda.Gov/Northeast-Area/Beltsville-Md-Bhnrc/Beltsville-Human-Nutrition-Research-Center/Food-Surveys-Research-Center/Food-Surveys-Research-Group/Docs/Fndds/ (accessed December 2, 2021).
17. Zhang Z. Multiple imputation with multivariate imputation by chained equation (mice) package. Ann Transl Med. (2016) 4:30. doi: 10.3978/j.issn.2305-5839.2015.12.63
18. Bidhendi Yarandi R. Effect of folate supplementation on insulin sensitivity and type 2 diabetes: a meta-analysis of randomized controlled trials. Am J Clin Nutr. (2019) 109:1233. doi: 10.1093/ajcn/nqz021
19. Boykin JV Jr, Hoke GD, Driscoll CR, Dharmaraj BS. High-dose folic acid and its effect on early stage diabetic foot ulcer wound healing. Wound Repair Regen. (2020) 28:517–25. doi: 10.1111/wrr.12804
20. Wang Z, Xing W, Song Y, Li H, Liu Y, Wang Y, et al. Folic acid has a protective effect on retinal vascular endothelial cells against high glucose. Molecules. (2018) 23:2326. doi: 10.3390/molecules23092326
21. Muzurović E, Kraljević I, Solak M, Dragnić S, Mikhailidis DP. Homocysteine and diabetes: role in macrovascular and microvascular complications. J Diabetes Complications. (2021) 35:107834. doi: 10.1016/j.jdiacomp.2020.107834
22. Mursleen MT, Riaz S. Implication of homocysteine in diabetes and impact of folate and vitamin B12 in diabetic population. Diabetes Metab Syndr. (2017) 11(Suppl. 1):S141–6. doi: 10.1016/j.dsx.2016.12.023
23. Liu Y, Geng T, Wan Z, Lu Q, Zhang X, Qiu Z, et al. Associations of serum folate and vitamin B12 levels with cardiovascular disease mortality among patients with type 2 diabetes. JAMA Netw Open. (2022) 5:e2146124. doi: 10.1001/jamanetworkopen.2021.46124
24. Harris HR, Bergkvist L, Wolk A. Folate intake and breast cancer mortality in a cohort of swedish women. Breast Cancer Res Treat. (2012) 132:243–50. doi: 10.1007/s10549-011-1838-y
25. Cui R, Iso H, Date C, Kikuchi S, Tamakoshi A. Dietary folate and vitamin B6 and B12 intake in relation to mortality from cardiovascular diseases: Japan collaborative cohort study. Stroke. (2010) 41:1285–9. doi: 10.1161/STROKEAHA.110.578906
26. Medrano MJ, Sierra MJ, Almazán J, Olalla MT, López-Abente G. The association of dietary folate, B6, and B12 with cardiovascular mortality in Spain: an ecological analysis. Am J Public Health. (2000) 90:1636–8. doi: 10.2105/AJPH.90.10.1636
27. Persson EC, Schwartz LM, Park Y, Trabert B, Hollenbeck AR, Graubard BI, et al. Alcohol consumption, folate intake, hepatocellular carcinoma, and liver disease mortality. Cancer Epidemiol Biomarkers Prev. (2013) 22:415–21. doi: 10.1158/1055-9965.EPI-12-1169
28. Xu X, Gammon MD, Wetmur JG, Bradshaw PT, Teitelbaum SL, Neugut AI, et al. B-vitamin intake, one-carbon metabolism, and survival in a population-based study of women with breast cancer. Cancer Epidemiol Biomarkers Prev. (2008) 17:2109–16. doi: 10.1158/1055-9965.EPI-07-2900
Keywords: diet, folate, diabetes, mortality, cohort
Citation: Su H, Bo Y, Zhang X, Zhang J, Gao Z and Yu Z (2022) Associations of folate intake with all-cause and cause-specific mortality among individuals with diabetes. Front. Nutr. 9:1021709. doi: 10.3389/fnut.2022.1021709
Received: 17 August 2022; Accepted: 16 September 2022;
Published: 14 October 2022.
Edited by:
Xue Li, Zhejiang University, ChinaReviewed by:
Shao-Fei Liu, Charité Universitätsmedizin Berlin, GermanyYimin Qu, Chinese Academy of Medical Sciences and Peking Union Medical College, China
Copyright © 2022 Su, Bo, Zhang, Zhang, Gao and Yu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zengli Yu, emx5QHp6dS5lZHUuY24=