
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Nutr. , 16 November 2022
Sec. Nutritional Epidemiology
Volume 9 - 2022 | https://doi.org/10.3389/fnut.2022.1017720
This article is part of the Research Topic Diet and Nutrition for Non-communicable Diseases in Low and Middle-Income Countries View all 30 articles
 Monireh Sadat Seyyedsalehi1,2
Monireh Sadat Seyyedsalehi1,2 Giulia Collatuzzo1
Giulia Collatuzzo1 Inge Huybrechts3
Inge Huybrechts3 Maryam Hadji2,4
Maryam Hadji2,4 Hamideh Rashidian2
Hamideh Rashidian2 Roya Safari-Faramani5
Roya Safari-Faramani5 Reza Alizadeh-Navaei6Farin Kamangar7Arash Etemadi8,9
Reza Alizadeh-Navaei6Farin Kamangar7Arash Etemadi8,9 Eero Pukkala4,10Marc J. Gunter3Veronique Chajes3Paolo Boffetta1,11*†Kazem Zendehdel2,12*†
Eero Pukkala4,10Marc J. Gunter3Veronique Chajes3Paolo Boffetta1,11*†Kazem Zendehdel2,12*†The evolving trends in colorectal cancer (CRC) as one of the most common malignancies worldwide, have likely been influenced by the implementation of screening programs and changes in lifestyle habits. Changing lifestyle, including the shift in diet composition with higher fat, sugar, and animal-source foods intake, led to an increasing burden of CRC in countries undergoing rapid socioeconomic improvement. Results for the link between specific fatty acids (FAs) and CRC are generally inconclusive and more limited in developing countries than elsewhere. This study aims to investigate the association between FA intakes and CRC and its anatomical subsites in a large Iranian case-control study. A food frequency questionnaire was used to collect information on dietary intake in 865 cases and 3206 controls. We conducted multivariate logistic regression models to calculate the odds ratio (OR) and 95% confidence interval (CI). We found positive association between CRC and high intake of dietary total fat (OR highest quartile Q4 = 1.77, 95% CI = 1.32–2.38), cholesterol (ORQ4 = 1.58, 95% CI = 1.22–2.05), and palmitoleic acid (ORQ4 = 2.16, 95% CI = 1.19, 3.91), and an inverse association with high intake of dietary heptanoic acid (ORQ4 = 0.33, 95% CI = 0.14, 0.79) and low intake of palmitic acid (OR lowest quartile Q2 = 0.53, 95% CI = 0.31–0.88). None of the fat variables were associated with rectal cancer. Our study suggests that the recommendation of limited consumption of fats may decrease the risk of CRC among the Iranian population.
Colorectal cancer (CRC) is the third most common malignancy and the second leading cause of cancer death, with an estimated 1.8 million new cases and 900,000 deaths in 2020 worldwide (1). A higher incidence rate is found in men and in highly industrialized countries (2). In Iran, CRC is the fourth most common cancer, with an age-adjusted incidence rate (ASR) of 15.9 and 11.9 for men and women, respectively (1). From 2016 to 2020, previous studies identified an increasing trend in Iran and predicted a 54% increase by 2025 (3). The changing trends in CRC have likely been influenced by two factors: (i) the implementation of screening programs; (ii) changes in lifestyle habits. Colonoscopy as a gold standard for CRC screening has on the one hand the short-term effect of apparent increasing CRC incidence due to early detection; on the other, it has been proven to reduce the incidence in the long term by the removal of precancerous lesions (4). The changing lifestyle, including the shift of diet composition toward a “westernized” pattern connoted by higher fat, sugar, and animal-source foods intake, leads to an increasing burden of CRC in countries undergoing rapid socioeconomic improvement. These situations can lead to a growing concern regarding the rising number of CRC cases, in particular among those <50 years of age (4, 5). In particular, CRC has observed an increase in the Iranian population, especially among men and in more urbanized areas (6, 7). The investigation of dietary behaviors in Iranians have been involved different study groups, being described for example by Saneei et al. Different dietary patterns have been described by residency in Iran, with higher intake of vegetables, fruit, meat, fat, saturated fatty acids (SFA), cholesterol, vitamin C, and beta-carotene and less bread, cereal, and carbohydrates in urban compared to rural dwellers. Also, similar differences in fat, SFA, MUFA, and bread consumption was seen by race, with Turkmens having higher intakes than non-Turkmens. These findings were related to the higher incidence of esophageal cancer registered in Iranians from low socioeconomic status and living in rural areas. Indeed, nutrition deficiencies may contribute to cancer by altering metabolism of carcinogens or by impairing DNA repair (8, 9). Zamaninour et al. had recently described the prevalence of unhealthy dietary habits in Iranian population, where more than 80% of people reported suboptimal intakes of fruit, dairy products and fish, and about 60% also reported suboptimal vegetables intake (10). The identification of dietary risk factor of CRC in Iranian population has been the aim of different recent studies. A case-control study conducted in Iran showed the correlation between a pro-inflammatory diet, based on high consumption of red and processed meat and fat, was associated to CRC and colorectal adenomatous polyps (11).
At least 12% of CRC cases are directly attributable to overweight/obesity according to a recent global review (12). Diets rich in fat are also a risk factor for obesity and cancer (13). According to the literature, different roles are exerted by different types of dietary fats depending on their source such as, ω-3 polyunsaturated fatty acids (PUFAs) play a role in protecting against adipose tissue inflammation, in contrast to omega-6 (ω-6) PUFAs and some saturated fatty acids (SFAs) and monounsaturated fatty acids (MUFAs), which promote inflammation (14, 15). A higher risk of CRC has been associated with high animal fat intake, but not vegetable fat (16). Although, the amount and type of different fatty acids (FAs) consumed by CRC patients resulted not to be associated either with recurrence or survival (17). To date, limited data provide the quantification of the effect exerted by FAs on CRC. Besides this, few results are available on the role played by the different types of FAs on CRC overall and by anatomical sub-sites.
Currently, screening programs in Iran are based on the identification of high-risk individuals, corresponding to first-degree relatives of CRC patients. Thus, they are based on the consultation of cancer registry. The first-degree families of CRC patients are invited to cancer screening and participate in counseling sessions, possibly leading to colonoscopy recommendation. So far, Iran does not have any screenings or plans for screening the general population at medium-risk of cancer. This makes Iran very different from most of the other countries, where non-invasive testing is purposed based on risk profile but also older age and are followed by the invasive endoscopic examination. This issue was addressed by Nikbakht et al. who conducted a study to investigate the use of immunochemical fecal occult blood test (IFOBT) in a mid-risk for CRC Iranian population. The study showed high responsiveness rates from the population, and high rates of positive IFOBT were found (18). Considering these evidence, better comprehension of CRC epidemiology in Iran results highly important for CRC control. In particular, the identification of risk factors of CRC may help preventing the disease and target high-risk population with secondary prevention, including colonoscopy.
This study aims to look at associations between fatty acid intakes and CRC risk considering overall and sub-site-specific CRC in a large Iranian case-control study. Our analysis provides useful data to deepen the knowledge on the role of fatty acids in CRC development. Moreover, we give valuable information on the consumption of fatty products in Iran and their relationship with CRC from different anatomical sites.
A total of 4,149 participants, including 906 CRC cases with pathologic diagnosis and 3,243 controls were recruited between May 2017 and 2020 from the main cancer clinic and hosptals in 7 provinces of Iran (Tehran, Fars, Mazandaran, Kerman, Golestan, Kermanshah, and Mashhad). They were part of the IROPICAN study, a multicenter case-control study coducted in 10 Iranian provinces, which was designed to examine the link between opium use and the development of lung, colorectal, bladder, and head and neck cancers (19). For the analysis of dietary intakes of fat, we excluded participants without the pathological report diagnoses confirmation (n = 18); those with missing information on dietary intake and those in the highest or lowest 1% of the distribution for the ratio of energy intake to estimated energy requirement (n = 60). We included 865 cases and 3,206 controls in our analysis (Figure 1). Controls were enrolled concurrently with the cases among the healthy visitors of non-oncology wards. The controls had to be free of cancer at the date of recruitment. The mean age at recruitment was 58.5 years and 57.1 years for the cases and controls, respectively. In this study, we estimated around 800 colorectal cancer cases using the OR and CI95 reported by previous studies (20–22), assuming 20 and 30% exposure prevalence among controls and 80% power.

Figure 1. Flow diagram of the population enrollment based on the inclusion and exclusion criteria in IROPICAN study.
CRC cases was defined by the International Classification of Diseases (ICD-O-3) as tumors of the colon (C18) or rectum (C19–C20). Colon cancer may be categorized as proximal (from cecum to splenic flexure, C18.0–C18.5) and distal (from descending colon to sigmoid colon, C18.6–C18.7), while rectum cancer occurs from the recto-sigmoid junction (C19) down to the rectum. Anus tumors were excluded from the study. Also, all histological types of CRC except melanoma and sarcoma were included.
During a face-to-face interview, lifestyle questionnaires were used to collect information about education, tobacco use, opium use, socioeconomic status (SES), physical activity, previous illness, and use of nonsteroidal anti-inflammatory drugs (NSAIDs). At the time of enrollment, trained professionals generally measured the standing height of participants (cm). The body mass index (BMI) was calculated as weight/height squared (kg/m2). Cases were asked about their body weight before cancer diagnosis, while controls were measured their body weight at the time of the interview. Based on the Finland Job Exposure Matrix (FINJEM) (23, 24) we analyzed the estimated perceived physical activity workload (PPWL). A principal component analysis was used to calculate the socioeconomic status (SES) of the participants, and the SES was calculated based on the number of years of education the participants had and whether they owned any assets like vacuum cleaners, clothes washers, dishwashers, freezers, internet access, microwaves, laptops, mobile phones, cars, and shops (25).
Dietary intakes were assessed with validated qualitatively Persian Cohort FFQ (26) administered by trained interviewers. The usual intake of 131 food items in separate parts including bread and cereal, meat, vegetables and fruits, dietary products, oils, sugars, species, and other group (113 items), dietary supplements (17 items), and water in the last year before cancer diagnosis were collected. For each food item, the reported frequency of consumption (daily, weekly, monthly, or yearly) was converted to frequency per day and was multiplied by the standard portion size (grams) using household measures to calculate grams per day. Using the food composition database developed for the Iranian population based on USDA food composition (27), Near-East food composition (28), and Bahrain food composition (29), macronutrients and micronutrients were calculated.
Regarding this analysis, we calculated the intake of 50 dietary fats based on our food composition table. According to previous studies (21, 22, 30) and the importance and commonplace of FAs in daily food, the gram per day of following FAs were considered in this study: (a) total fat; (b) cholesterol; (c) total SFAs, myristic acid pentadecanoic acid, palmitic acid, heptadecanoic acid, stearic acid; (d) total MUFAs, palmitoleic acid, oleic acid; (e) total PUFAs.
The means and standard deviations (±SD) for continuous variables and the frequencies for categorical variables were calculated for descriptive statistics of baseline characteristics and intake of dietary factors of cases and controls.
The normality tested by comparing a histogram of the data to a normal probability curve. After examining the distribution of the data, all nutrient intakes were log-transformed to improve normality.
For the analysis of the association between dietary fat and different type of FFAs; SFAs, PUFAs, MUFAs, and cholesterol and CRC, we conducted unconditional multivariable logistic regression models to estimate the odds ratios (ORs) and 95% CIs. Before multivariate logistic regression, correlations between different exposures were checked and ORs were adjusted by gender (male/female), age (continuous), province, BMI (continuous), tobacco (smoking and water pipe) consumption (Never /Ever), aspirin use (Yes/No), opium use (no user / irregular users / regular users'), SES (Low/ Medium/ High), work-related physical activity (sedentary/Moderate/Heavy), processed meat intake including mortadella, hamburger and sausage (continuous, g/day), calcium (continuous, mg/day), fiber intake (continuous, g/day), and energy (continuous, kcal/day). Participants with missing data for physical activity (24.93 %) were coded as distinct categories during the analysis. Quartile were calculated based on the distribution of different type of fat intake between controls of study. Besides the main analysis, continuous analyses were also run across quartiles. Furthermore, analyses were stratified by age (under and over 50), BMI, gender, SES, physical activity, and vegetable intake for comparing quartile 4 to quartile1 of different types of fat intake. Nevertheless, according to significant interaction (P-heterogeneity < 0.05) analysis we only report age category results. We repeated the analyses for all CRC patients and then after stratification for sub-sites, including colon overall, proximal colon, distal colon, and rectum. All statistical analyses were carried out using Stata 14 (Stata Statistical Software: Release 14. College Station, TX: Stata Corp LLC). We considered p values <0.05 as statistically significant.
The study was approved by the Ethics Committee of the National Institute for Medical Research Development (NIMAD) (Code: IR.NIMAD.REC.1394.027). All participants signed a written informed consent to participate in the study.
The current study included a total of 865 incident CRC cases, 434 cancers of the colon, 404 rectal cancer cases, 27 cases from unknown sub-site, and 3,206 controls; their socio-demographic characteristics, dietary factors intakes, and the distribution of selected CRC risk factors are shown in Table 1. One-third (N = 145) of the colon cancers were in the proximal colon, 42% (N = 185) in the distal colon, and 23% (N = 104) to the overlapping region between proximal and distal colon. In our study, the male to female ratio was 2, and around 76% of all participants were older than 50 years of age. Fars and Tehran provinces had the largest share of the study population. Significant differences between cases and controls were observed for tobacco use, family history, socioeconomic status, and opium use, but not for BMI and physical activity. CRC cases reported higher dietary energy intake (2,406 kcal/day) compared to controls (2,319 kcal/day). Higher levels of FAs and cholesterol were reported by cases than controls (Table 1).
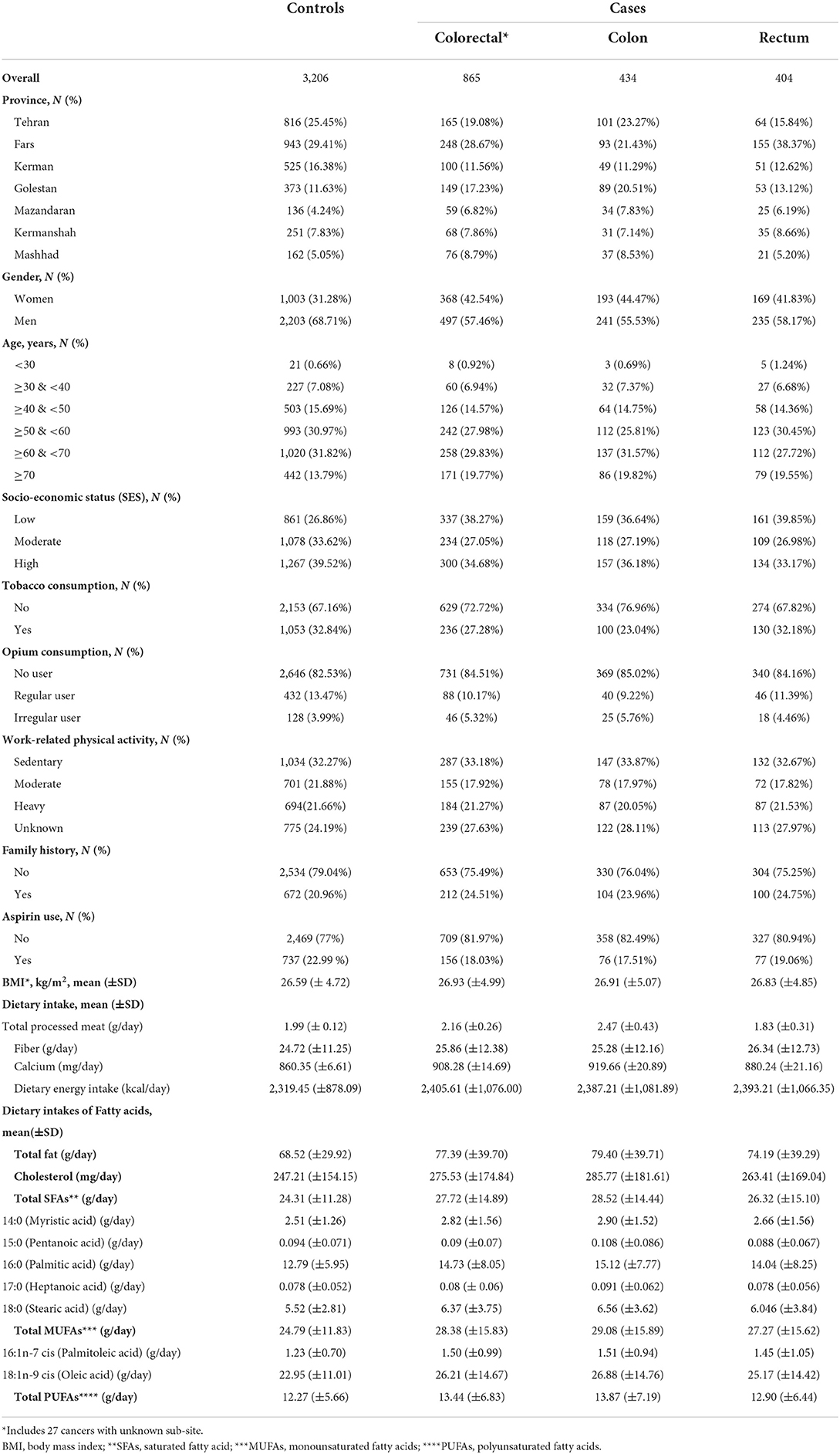
Table 1. Selected baseline demographic and lifestyle characteristics of study participants by colorectal cancer status, IROPICAN study.
There was a statistically significant positive association between CRC and high intake (quartile 4) of dietary total fat (meanQ4 = 111 g/day, ORQ4 = 1.77, 95% CI = 1.32–2.38), cholesterol (meanQ4 = 437 mg/day, ORQ4 = 1.58, 95% CI = 1.22–2.05), and palmitoleic acid (meanQ4 = 2.24 g/day, ORQ4 = 2.16, 95% CI = 1.19–3.91), as well as an inverse association with high intake of dietary heptanoic acid (meanQ1: 0.147 g/day, ORQ4 = 0.33, 95% CI = 0.14, 0.79), low intake (quartile 2) of palmitic acid (meanQ2 = 10.45 g/day, ORQ2 = 0.53, 95% CI = 0.31–0.88) (Table 2).
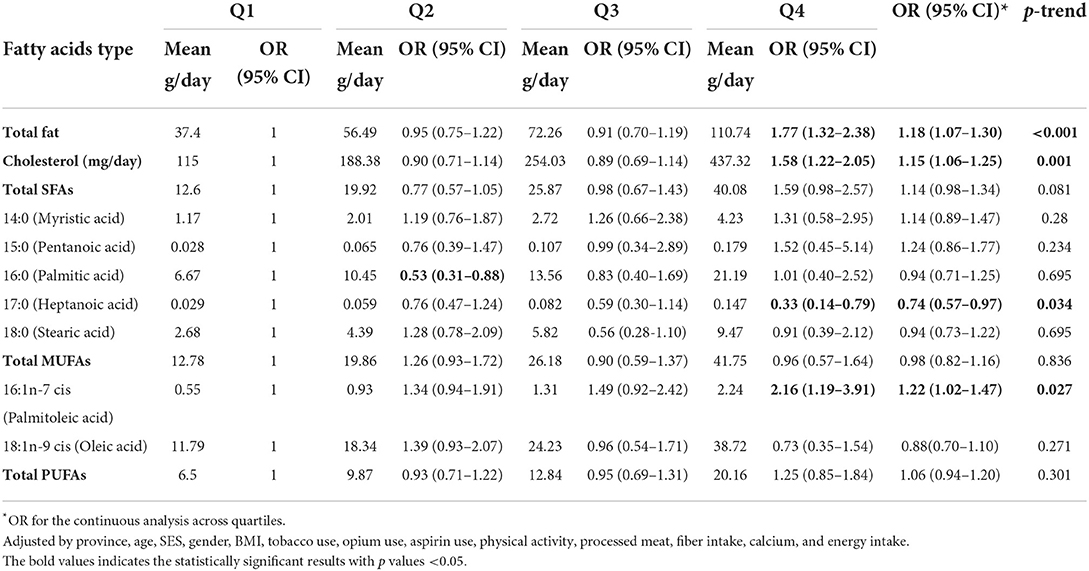
Table 2. Dietary estimates of fatty acids and risk of colorectal cancer.
Additional analyses were performed on specific subsites of CRC cases. CRC were classified as colon, proximal or distal colon cancer, and rectum cancer. Based on stratified analyses by anatomical site, we identified a positive association between total fat and colon cancer [OR comparing highest to lowest quartile (Q4 vs. Q1) = 1.30, 95% CI = 1.14–1.48] as well as proximal [ORQ4vs.Q1 = 1.43, 95% CI; 1.15–1.77], and distal colon [ORQ4vs.Q1 = 1.25, 95% CI = 1.03–1.50].
Also, cholesterol intake was positively associated with colon [ORQ4vs.Q1 = 1.22, 95% CI = 1.09–1.36] and proximal colon cancer risk [ORQ4vs.Q1 = 1.25, 95% CI = 1.04–1.51].
Total SFAs intake was not associated with different sub-anatomical location of colon cancer, but we found a positive association for individual SFAs: pentanoic acid and colon cancer [ORQ4vs.Q1 = 1.81, 95% CI = 1.14–2.87], myristic acid [ORQ4vs.Q1 = 1.91, 95% CI = 1.09–3.34] and proximal colon cancer. Also, an inverse association was observed for heptanoic acid and colon cancer [ORQ4vs.Q1 = 0.66, 95% CI = 0.47–0.94]. Intake of oleic acid, which is one of the important MUFAs, was inversely associated with colon [ORQ4vs.Q1 = 0.70, 95% CI = 0.52–0.95] and proximal colon cancer risk [ORQ4vs.Q1 = 0.50, 95% CI = 0.30–0.83]. Conversely, no significant associations were observed for total MUFAs and PUFAs. Rectal cancer was not associated with any FA (Table 3 and Figure 2). A further analysis between different types of FAs and all sub-anatomical locations of CRC according to different quartiles indicated a positive association between stearic acid and proximal colon cancer [ORQ4 = 8.33; 95% CI = 1.02–67.65].
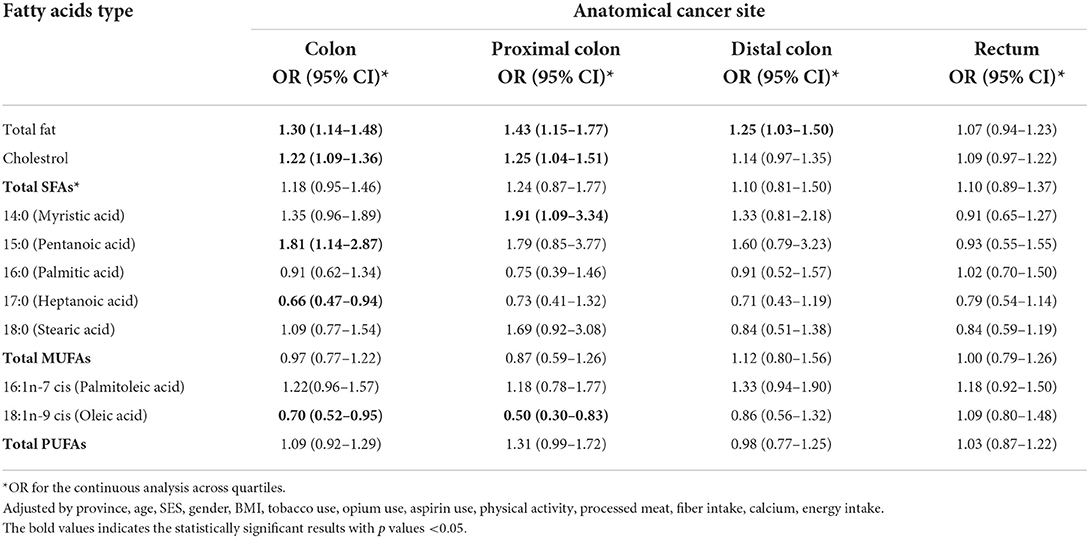
Table 3. Odds ratios and 95% confidence intervals of colorectal cancer and specific fatty acids intakes stratified by colorectal tumor location.
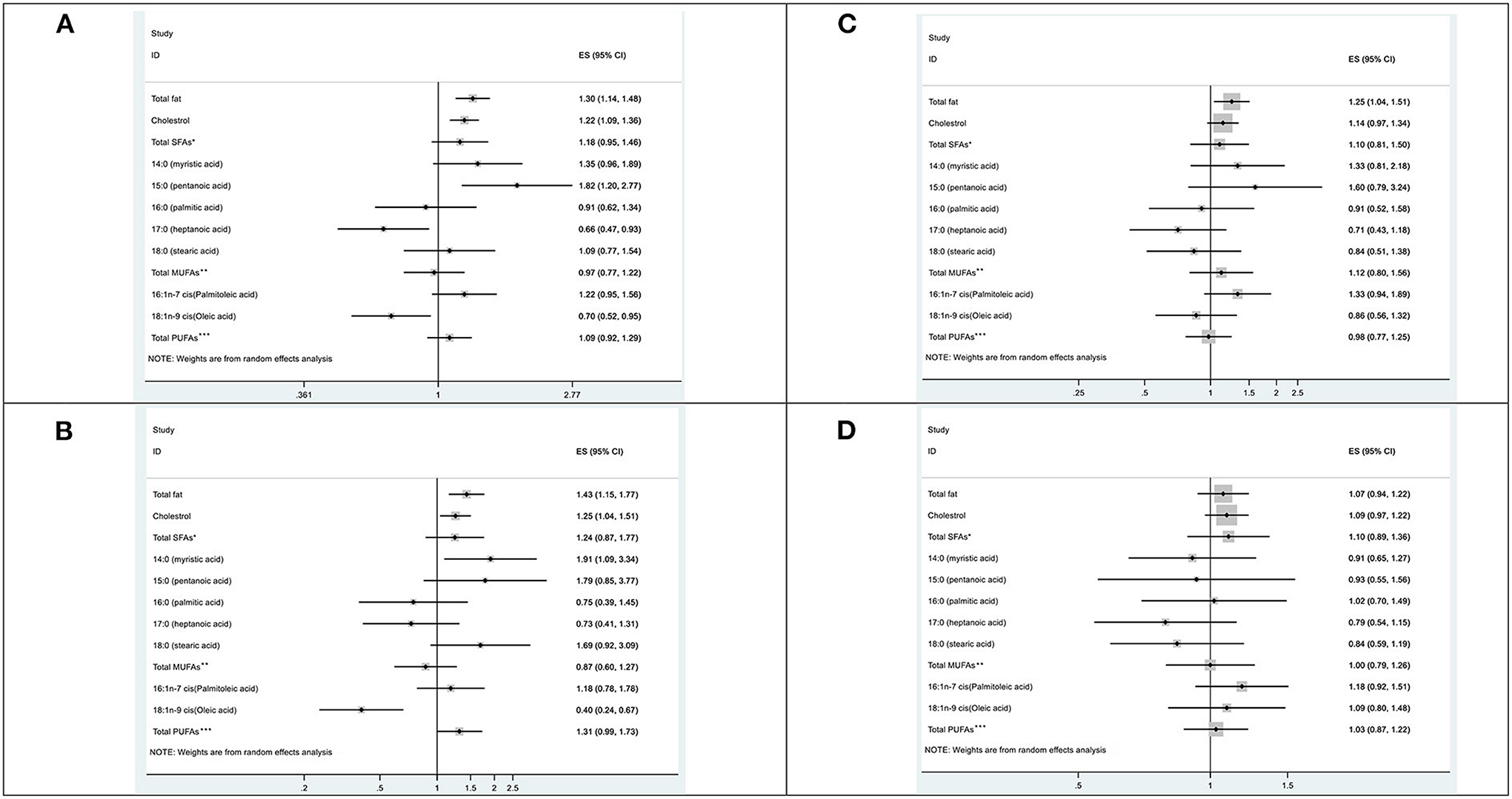
Figure 2. Forst plots according to the odds ratios, and 95% confidence intervals for colorectal cancer risk associated with different fat intake, by anatomical sub-site; (A) Colon cancer, (B) Proximal colon cancer, (C) Distal colon cancer, (D) Rectum cancer. *Saturated fatty acids; **Monounsaturated fatty acids; ***Polyunsaturated fatty acides.
According to the analyses stratified by age category, the statistically significant association persisted for total fat and CRC [ORQ4vs.Q1 = 1.30, 95% CI = 1.16–1.46, p = 0.006 for the interaction], as well as for colon [ORQ4vs.Q1 = 1.38, 95% CI = 1.18–1.61, p = 0.024 for the interaction] in subjects older than 50. Furthermore, a significant positive association was reported between cholesterol with CRC [ORQ4vs.Q1 = 1.22, 95% CI = 1.11–1.35, p = 0.019 for the interaction], colon [ORQ4vs.Q1 = 1.30, 95% CI = 1.14–1.48, p = 0.038 for the interaction]. There was no association between FAs intake and any of the cancer sub-sites among participants under 50 years old (Table 4).
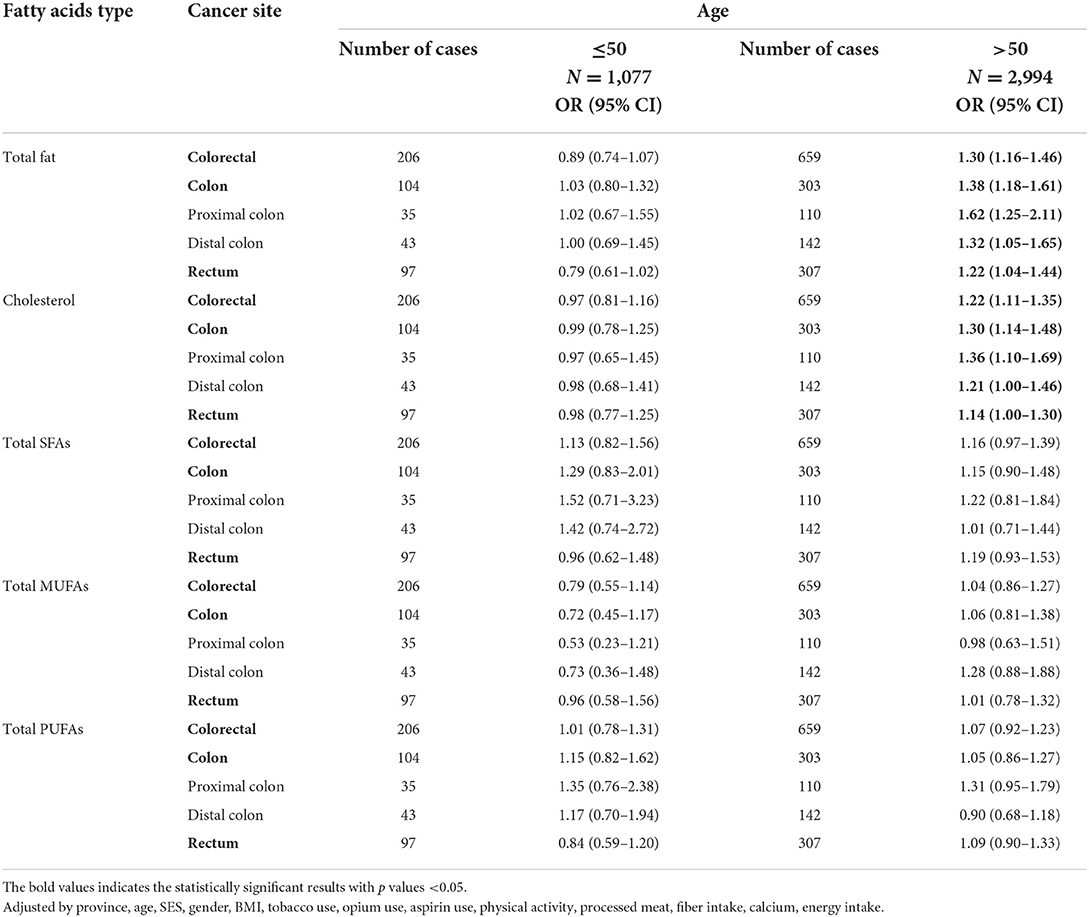
Table 4. Odds ratios and 95% confidence intervals of colorectal cancer and specific fatty acids intakes stratified by age.
We found a positive relationship between total fat, cholesterol, myristic acid, pentanoic acid, and a high intake of palmitoleic acid, with CRC, with a stronger effect on colon and proximal colon cancer. The associations were stronger in subjects older than 50 and absent in younger ones. A high intake of heptanoic acid, Oleic acid, and a low intake of palmitic acid showed inverse associations with CRC and colon cancer. We couldn't find any relation between rectal cancer and different kinds of FAs. Total PUFAs did not appear to have a significant effect on CRC in our study.
High dietary fat intake resulted in an increase in CRC risk of about 60%. The effect appeared to be exerted on the colon rather than the rectum, especially on the proximal section rather than the distal. Studies also have shown that FAs have different effects depending on the anatomical region of the colon (proximal and distal) and the source of the fat (14, 20, 21, 30–32). For example, in our study, plant-sourced fats such as heptanoic acid and oleic acid, or animal fats such as palmitic acid, stearic acid, and myristic acid obtained from meat and dairy products, show different effect on sub-site of colon and rectum. Indeed, a large body of literature described the enhanced risk of colon cancer with high fat intake (16, 33, 34), despite several studies finding no association between FAs and CRC overall (35). A recent meta-analysis found weak evidence of a correlation between FAs and CRC in Chinese men (36). According to a world cancer research fund international (WCRF) report published in 2018, evidence of the association between fats and different fatty acid types is limited and requires further investigation (22).
A number of mechanisms contributed to the effect of FAs on CRC risk, such as (1) pro-inflammatory effects that may be triggered by interaction between dietary fat and gut microbiota, which play a role in the metabolism of bile acids (BA) (37, 38). In fact, BA supports the concept of CRC. Evidence of selective uptake of PUFAs from CRC cells have been provided (39). (2) Oils and fats as the highest sources of polycyclic aromatic hydrocarbons (PAH) (40) can damage DNA in several target tissues when consumed through saturated fat (41). (3) A higher intake of saturated fat has been associated with increased oxidative damage and lipid peroxidation based on the in-vivo and in-vitro studies (42, 43). (4) Lipids have also been shown to affect cell membrane structure and function, signaling pathways, and gene expression (44). (5) Moreover, obesity is a major risk factor for CRC, with a preponderant role of visceral adiposity (45). A double-blind trial reported subjects overfed with highly SFAs foods underwent more visceral adiposity accumulation than subjects overfed with foods rich in PUFAs showing a distinct effect on fat accumulation in humans, which can in turn be differently related to CRC (46).
Our results showed IROPICAN study population reported a higher daily intake of total fat (70 grams/day, 27% of kcal energy), cholesterol (253 mg/day), and saturated fat (25 grams/day, 10% of kcal energy) than recommendations, coupled with a lower intake of total PUFAs (5% of total kcal energy), reflecting previous studies regarding the amount of dietary fat from different sources in Iranian populations (47, 48). The benefit of unsaturated FA, PUFAs, and MUFAs derived from an overall positive metabolic effect, with inhibition of inflammation and balance of microbiota composition (49). Total MUFAs and total PUFAs do not appear to be associated with CRC in our study. Fish and oily fish are the main sources of ω3 PUFAs (50), while ω6 PUFAs are obtained from vegetable oil, nuts, and egg (51). In terms of fish and seafood consumption, there is a big difference between Iran and other countries, and most PUFAs in the Iranian diet are supplied from other sources such as liquid vegetable oils (Sunflower, maize oil) (52, 53). For human health, it is essential to have a balanced ratio between the two types of PUFAs (54, 55). In this study, we did not investigate the effect of different types of PUFAs on CRC, as we plan to address this topic in a separate paper.
Over time, the type of oil available on the Iranian market has changed. According to a WHO report published in 2018, Iranian households consume a great deal of cooking oil made from partially hydrogenated vegetable oils, a major source of trans fatty acids (TFAs) (56). In recent years, many activities have been conducted with the goal of increasing awareness of solid/semisolid hydrogenated oils and reducing their consumption in Iran (57, 58). People who are 50 or older seem to use more of this type of fat than people who are younger. TFAs could influence cholesterol balance and the effect exerted by the amount of total fat intake (59). This can be seen in our results, where total fat increases the risk of CRC according to the proportion of TFAs intake. Nevertheless, this suggestion requires further studies.
To our knowledge, this is the first study to investigate the magnitude of different types of FAs on CRC in a large Iranian population from different provinces and in the EMRO region. Our data are characterized by high quality because (i) information were collected by trained interviewers, (ii) same standardized validated FFQs and questioning tools were used in the different centers, and (iii) all cases were provided with pathological confirmation and allowed us analyses by subsites.
Two potential limitations of our study include: (i) selection bias, because the controls were not chosen on a population-based approach in the primary study (IROPICAN) but were rather taken among the healthy visitors who did not have CRC or other diseases. However, our validation study showed that due to appropriate using healthy visitors instead of disease controls such bias is minimal (60); (ii) reporting and recall bias, especially regarding the FFQ, because of the dependence on memory and possibly case-control status. However, it is likely that this bias might have operated in a similar way in cases and controls, resulting in non-differential misclassification and underestimation of the associations. Furthermore, diet might have changed among cases because of disease development. To allay this concern and risk of reverse causation bias, we collected dietary information one year before the data of cancer diagnosis among cases. Also, food composition tables may have some limitations, and matching is not always straightforward, so that the results may be impaired by residual confounding. Anyway, the different results between colon and rectal cancer argue against a strong role of selection or information bias. Finally, we could not report different group of FAs based on specific source such as animal, vegetables, seeds, so on. Future studies should explore the relationship between different type of FAs and CRC by considering the source intake. Also, comparing dietary and plasma levels of FAs can be interesting.
In this large CRC case-control study, total fat, cholesterol, and higher intake of myristic acid, palmitic acid, palmitoleic acid from animal sources were associated with increased risk of CRC, and some FAs from plant sources such as heptanoic acid or oleic acid- the main FA in olive oil- decreased particularly colon cancer risk, after accounting for major adjustments. Moreover, subgroup analyses by age revealed that participants older than 50 years had a higher risk of CRC due to consumption of a high FAs diet. This may be due to the cohort effect and changes on the amount, and type of FAs intake over time. Our study improves general knowledge on CRC epidemiology and offers important insights on CRC in Iranian population. These data may be useful for the identification of high-risk individuals and public awareness to promote prevention of CRC in Iran and other LMICs that facing the increasing pattern in the incidence of CRC. In line with international evidence, the promotion of a decrease in fat consumption, especially FAs from industrial and animal sources, may decrease the risk of CRC among the Iranian population. Along these lines, a number of restrictions have been imposed in Iran since 1025 on oil products, including trans and saturated fat, aimed at controlling and preventing non-communicable diseases, including CRC (61).
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The study was approved by the Ethics Committee of the National Institute for Medical Research Development (NIMAD) (Code: IR.NIMAD.REC.1394.027). Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
MSS, KZ, and PB designed research. MSS, KZ, RA-N, RS-F, HR, and MH conducted research. MSS, GC, KZ, and PB analyzed data, performed statistical analysis, and wrote the paper. FK, AE, MG, VC, IH, and EP contributed in the editing of the preliminary results and draft. KZ had primary responsibility for final content. All authors read and approved the final manuscript.
This study was funded by National Institute of Medical Research Development (NIMAD) (Code: IR.NIMAD.REC.1394.027) and particularly supported by Investigator Grant No. 24706 of Fondazione AIRC. Italy.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Where authors are identified as personnel of the International Agency for Research on Cancer / World Health Organization, the authors alone are responsible for the views expressed in this article and they do not necessarily represent the decisions, policy or views of the International Agency for Research on Cancer / World Health Organization.
ASR, age-standardized incidence rate; BMI, body mass index; CI, confidence interval; CRC, colorectal cancer; EMRO, Eastern Mediterranean Region; FAs, fatty acids; FFAs, free fatty acids; FFQ, Food Frequency Questionnaire; LMIC, low and middle-income countries; MUFAs, monounsaturated fatty acids; OR, odds ratio; PUFAs, polyunsaturated fatty acids; SFAs, saturated fatty acid; TFAs, trans fatty acids; WCRF, World Cancer Research Fund.
1. Hyuna S, Jacques F, Rebecca ME, Mathieu L, Isabelle S, Ahmedin J, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. (2021) 71:209–49. doi: 10.3322/caac.21660
2. Keum N, Giovannucci E. Global burden of colorectal cancer: emerging trends, risk factors and prevention strategies. Nat Rev Gastroenterol Hepatol. (2019) 16:713–32. doi: 10.1038/s41575-019-0189-8
3. Gholamreza R, Jacques F, Ali Gh-M, Elham P, Fereshteh S, Kimia A, et al. Cancer in Iran 2008 to 2025: Recent incidence trends and short-term predictions of the future burden. Cancer Epidemiol. (2021) 149:594–605. doi: 10.1002/ijc.33574
4. Arnold M, Sierra MS, Laversanne M, Soerjomataram I, Jemal A, Bray F. Global patterns and trends in colorectal cancer incidence and mortality. Gut. (2017) 66:683–91. doi: 10.1136/gutjnl-2015-310912
5. Akimoto N, Ugai T, Zhong R, Hamada T, Fujiyoshi K, Giannakis M. Rising incidence of early-onset colorectal cancer - a call to action. Nat Rev Clin Oncol. (2021) 18:230–43. doi: 10.1038/s41571-020-00445-1
6. Hasanpour-Heidari FA, Semnani S, Khandoozi SR, Amiriani T, Sedaghat S, Hosseinpoor R, et al. Temporal and geographical variations in colorectal cancer incidence in Northern Iran 2004-2013. Cancer Epidemiol. (2019) 59:143–7. doi: 10.1016/j.canep.2019.02.003
7. Roya D, Mohammad Hossein S, Iraj AK, Morteza Gh, Mohamad Asghari J, Faris F, et al. Increased colorectal cancer incidence in Iran: a systematic review and meta-analysis. BMC Public Health. (2015) 15. doi: 10.1186/s12889-015-2342-9
8. Saneei P, Esmaillzadeh A, Keshteli AH, Feizi A, Feinle-Bisset C, Adibi P. Patterns of dietary habits in relation to obesity in Iranian adults. Eur J Nutr. (2016) 55:713–28. doi: 10.1007/s00394-015-0891-4
9. Islami F, Malekshah AF, Kimiagar M, Pourshams A, Wakefield J, Goglani G, et al. Patterns of food and nutrient consumption in northern Iran, a high-risk area for esophageal cancer. Nutr Cancer. (2009) 61:475–83. doi: 10.1080/01635580902803735
10. Zamaninour N, Yoosefi M, Soleimanzadehkhayat M, Pazhuheian F, Saeedi Moghaddam S, Djalalinia S, et al. Distribution of dietary risk factors in Iran: national and sub-national burden of disease. Arch Iran Med. (2021) 24:48–57. doi: 10.34172/aim.2021.08
11. Rafiee P, Shivappa N, Hébert JR, Nasab SJ, Bahrami A, Hekmatdoost A, et al. Dietary inflammatory index and odds of colorectal cancer and colorectal adenomatous polyps in a case-control study from Iran. Nutrients. (2019) 11:1213. doi: 10.3390/nu11061213
12. Whiteman DC, Wilson LF. The fractions of cancer attributable to modifiable factors: a global review. Cancer Epidemiol. (2016) 44:203–21. doi: 10.1016/j.canep.2016.06.013
13. Bojková B, Winklewski PJ, Wszedybyl-Winklewska M. Dietary fat and cancer—which is good, which is bad, and the body of evidence. Int J Mol Sci. (2020) 21:4114. doi: 10.3390/ijms21114114
14. May-Wilson S, Sud A, Law PJ, Palin K, Tuupanen S, Gylfe A, et al. Pro-inflammatory fatty acid profile and colorectal cancer risk: a Mendelian randomisation analysis. Eur J Cancer. (2017) 84:228–38. doi: 10.1016/j.ejca.2017.07.034
15. Wan Y, Wu K, Wang L, Song M, Giovannucci EL, Willett WC. Dietary fat and fatty acids in relation to risk of colorectal cancer. Eur J Nutr. (2022) 61:1863–73. doi: 10.1007/s00394-021-02777-9
16. Willett WC, Stampfer MJ, Colditz GA, Rosner BA, Speizer FE. Relation of meat, fat, and fiber intake to the risk of colon cancer in a prospective study among women. N Engl J Med. (1990) 323:1664–72. doi: 10.1056/NEJM199012133232404
17. Van Blarigan EL, Ou FS, Niedzwiecki D, Zhang S, Fuchs CS, Saltz L, et al. Dietary fat intake after colon cancer diagnosis in relation to cancer recurrence and survival: CALGB 89803 (Alliance). Cancer Epidemiol Biomarkers Prev. (2018) 27:1227–30. doi: 10.1158/1055-9965.EPI-18-0487
18. Nikbakht HA, Shokri-Shirvani J, Ashrafian-Amiri H, Ghaem H, Jafarnia A, Alijanpour S, et al. The first screening program for colorectal cancer in the north of Iran. J Gastrointest Cancer. (2020) 51:165–71. doi: 10.1007/s12029-019-00226-9
19. Hadji M, Rashidian H, Marzban M, Gholipour M, Naghibzadeh-Tahami A, Mohebbi E, et al. The Iranian study of opium and cancer (IROPICAN): rationale, design, and initial findings. Arch Iran Med. (2021) 24:167–76. doi: 10.34172/aim.2021.27
20. Mo A, Wu R, Grady JP, Hanley MP, Toro M, Helen Swede, et al. Associations of dietary fat with risk of early neoplasia in the proximal colon in a population-based case-control study. Cancer Causes Control. (2018) 29:667–74. doi: 10.1007/s10552-018-1039-7
21. Slattery ML, Potter JD, Duncan DM, Berry TD Dietary Dietary fats and colon cancer: assessment of risk associated with specific fatty acids. Int J Cancer Detection and Prevention. (1997) 73:670–7. doi: 10.1002/(SiCi)1097-0215(19971127)73:5<670::AID-ijc10>3.0.CO;2-a
22. Nguyen S, Li H, Yu D, Cai H, Gao J, Gao Y, et al. Dietary fatty acids and colorectal cancer risk in men: a report from the Shanghai Men's Health Study and a meta-analysis. Int J Cancer. (2021) 148:77–89. doi: 10.1002/ijc.33196
23. Kauppinen T, Toikkanen J, Pukkala E. From cross-tabulations to multipurpose exposure information system: a new job-exposure matrix. Am J Ind Med. (1998) 33:409–17. doi: 10.1002/(sici)1097-0274(199804)33:4<409::aid–ajim12>3.0.co;2–2
24. Kauppinen T, Heikkila P, Plato N, Woldbaek T, Lenvik K, Hansen J, et al. Construction of job-exposure matrices for the Nordic occupational cancer study. Acta Oncol. (2009) 48:791–800. doi: 10.1080/02841860902718747
25. Mohebbi E, Hadji M, Rashidian H, Rezaianzadeh A, Marzban M, Haghdoost AA, et al. Opium use and the risk of head and neck squamous cell carcinoma. Int J Cancer. (2021) 148:1066–76. doi: 10.1002/ijc.33289
26. Hossein P, Sareh E, Farin K, Etemadi A, Keshtkar AA, Hekmatdoost A, et al. Prospective epidemiological research studies in Iran (the PERSIAN Cohort Study): rationale, objectives, and design. Am J Epidemiol. (2018) 187:647–55. doi: 10.1093/aje/kwx314
27. Ahuja DB, Wu JKC, Somanchi X, Nickle M, Nguyen M, Roseland QA, et al. USDA National Nutrient Database for Standard Reference. Legacy Release, Nutrient Data Laboratory, Beltsville Human Nutrition Research Center, Haytowitz. Washington, DC: USDA (2019).
29. Musaiger AO. Food Composition Tables for Kingdom of Bahrain. Manama: Arab Center for Nutrition (2011).
30. Aglago EK, Murphy N, Huybrechts I, Nicolas G, Casagrande C, Fedirko V, et al. Dietary intake and plasma phospholipid concentrations of saturated, monounsaturated and trans fatty acids and colorectal cancer risk in the European Prospective Investigation into Cancer and Nutrition cohort. Int J Cancer. (In Press). doi: 10.1002/ijc.33615
31. Nkondjock A, Shatenstein B, Maisonneuve P, Ghadirian P. Specific fatty acids and human colorectal cancer: an overview. Cancer Detect Prev. (2003) 27:55–66. doi: 10.1016/S0361-090X(02)00179-4
32. Schloss I, Kidd MSG, Tichelaar HY, Young GO, O'Keefe SJ. Dietary factors associated with a low risk of colon cancer in coloured West Coast fishermen. S Afr Med J. (1997) 87:152–8.
33. Tuyns AJ, Haelterman M, Kaaks R. Colorectal cancer and the intake of nutrients: oligosaccharides are a risk factor. Nutr Cancer. (1987) 10:181–96. doi: 10.1080/01635588709513956
34. Butler LM, Wang R, Koh WP, Stern MC, Yuan JM, Yu MC. Marine n-3 and saturated fatty acids in relation to risk of colorectal cancer in Singapore Chinese: a prospective study. Int J Cancer. (2009) 124:678–86. doi: 10.1002/ijc.23950
35. Beyaz S, Mana MD, Roper J, Kedrin D, Saadatpour A, Hong S-J, et al. High-fat diet enhances stemness and tumorigenicity of intestinal progenitors. Nature. (2016) 531:53–8. doi: 10.1038/nature17173
36. Kim M, Park K. Dietary fat intake and risk of colorectal cancer: a systematic review and meta-analysis of prospective studies. Nutrients. (2018) 10:1963. doi: 10.3390/nu10121963
37. World Cancer Research Fund/American Institute of Cancer Research. Diet, Nutrition, Physical Activity and Cancer: A Global Perspective on Behalf of AICR, WCRF, and WKOF. London: World Cancer Research Fund/American Institute of Cancer Research
38. Ocvirk S, O'Keefe SJD. Dietary fat, bile acid metabolism and colorectal cancer. Semin Cancer Biol. (2021) 73:347–55. doi: 10.1016/j.semcancer.2020.10.003
39. Ocvirk S, O'Keefe SJ. Influence of bile acids on colorectal cancer risk: potential mechanisms mediated by diet -gut microbiota interactions. Curr Nutr Rep. (2017) 46:315–22. doi: 10.1007/s13668-017-0219-5
40. Diggs DL, Huderson AC, Harris KL, Myers JN, Banks LD, Rekhadevi PV, et al. Polycyclic aromatic hydrocarbons and digestive tract cancers: a perspective. J Environ Sci Health C Environ Carcinog Ecotoxicol Rev. (2011) 29:324–57. doi: 10.1080/10590501.2011.629974
41. Walker SA, Addai AB, Mathis M, Ramesh A. Effect of dietary fat on metabolism and DNA adduct formation after acute oral exposure of F-344 rats to fluoranthene. J Nutr Biochem. (2007) 18:236–49. doi: 10.1016/j.jnutbio.2006.04.001
42. Vogel U, Danesvar B, Autrup H, Risom L, Weimann A, Poulsen HE, et al. Effect of increased intake of dietary animal fat and fat energy on oxidative damage, mutation frequency, DNA adduct level and DNA repair in rat colon and liver. Free Radical Res. (2003) 37:947–56. doi: 10.1080/1071576031000150779
43. Hietanen E, Bartsch H, Bereziat JC, Ahotupa M, Camus AM, Cabral JR, et al. Quantity and saturation degree of dietary fats as modulators of oxidative stress and chemically induced liver tumors in rats. Int J Cancer. (1990) 46:640–7. doi: 10.1002/ijc.2910460415
44. Chapkin RS, McMurray DN, Lupton R. Colon cancer, fattyacids and anti-inflammatory compounds. Curr Opin Gastroenterol. (2007) 23:48–54. doi: 10.1097/MOG.0b013e32801145d7
45. Mika A, Kobiela J, Pakiet A, Czumaj A, Sokołowska E, Makarewicz W, et al. Preferential uptake of polyunsaturated fatty acids by colorectal cancer cells. Sci Rep. (2020) 10:1954. doi: 10.1038/s41598-020-58895-7
46. Rosqvist F, Iggman D, Kullberg J, Cedernaes J, Johansson HE, Larsson A, et al. Overfeeding polyunsaturated and saturated fat causes distinct effects on liver and visceral fat accumulation in humans. Diabetes. (2014) 63:2356–68. doi: 10.2337/db13-1622
47. Micha R, Khatibzadeh S, Shi P, Fahimi S, Lim S, Kathryn G, et al. Global, regional, and national consumption levels of dietary fats and oils in 1990 and 2010: a systematic analysis including 266 country-specific nutrition surveys. BMJ. (2014) 348:1–20. doi: 10.1136/bmj.g2272
48. Liu AG, Ford NA, Hu FB, Zelman KM, Mozaffarian D, Kris-Etherton PM, et al. healthy approach to dietary fats: understanding the science and taking action to reduce consumer confusion. Nutr J. (2017) 16:53. doi: 10.1186/s12937-017-0271-4
49. Silva Figueiredo P, Carla Inada A, Marcelino G, Lopes Cardozo CM, de Cássia Freitas K, de Cássia Avellaneda Guimarães R, et al. Fatty acids consumption: the role metabolic aspects involved in obesity and its associated disorders. Nutrients. (2017) 9:1158. doi: 10.3390/nu9101158
50. Gammone MA, Riccioni G, Parrinello G, D'Orazio N. Omega-3 polyunsaturated fatty acids: benefits and endpoints in sport. Nutrients. (2018) 11:46. doi: 10.3390/nu11010046
51. D D'Angelo S, Motti ML, Meccariello R. ω-3 and ω-6 polyunsaturated fatty acids, obesity and cancer. Nutrients. (2020) 12:2751. doi: 10.3390/nu12092751
52. Adeli A, Hasangholipour T, Hossaini A, Shabanpour B. Status of fish consumption per capita of Tehran citizens. Iran J Fisheries Sci. (2011) 10:546–56.
53. Daryani A, Becker W, Vessby B, Andersson A. Dietary fat intake, fat sources and fatty acid composition in serum among immigrant women from Iran and Turkey compared with women of Swedish ethnicity. Scand J Nutr. (2016) 49:106–15. doi: 10.1080/11026480510044536
54. Simopoulos AP. The importance of the ratio of omega-6/omega-3 essential fatty acids. Biomed Pharmacother. (2002) 56:365–79. doi: 10.1016/S0753-3322(02)00253-6
55. Yang K LH, Dong J, Dong Y, Wang CZ. Expression profile of polyunsaturated fatty acids in colorectal cancer. World J Gastroenterol. (2015) 21:2405–12. doi: 10.3748/wjg.v21.i8.2405
56. World Health Organization. Cutting into Trans-fat Consumption in Iran. (2018). Available online at: https://www.who.int/news-room/feature-stories/detail/cutting-into-trans-fat-consumption-in-iran (accessed April 15, 2022).
57. Jafari F, Kholdi N, Davati A, Nezamdust Z. The study of oils consumption pattern and its related factors in east Tehran. J Fasa Univ Med Sci. (2013) 3:202–7.
58. Salehzadeh H, Soori M, Sadeghi S, Shahsawari S, Mohammadi S, Saifi M, et al. The type and amount of household oil consumption and the influential factors in Sanandaj city, Iran. J Adv Environ Health Res. (2019) 7:1–7. doi: 10.22102/JAEHR.2019.125492.1070
59. Stender S, Astrup A. Ruminant and industrially produced trans fatty acids: health aspects. Food Nutr Res. (2008) 52. doi: 10.3402/fnr.v52i0.1651
60. Rashidian H, Hadji M, Marzban M, Gholipour M, Rahimi-Movaghar A, Kamangar F, et al. Sensitivity of self-reported opioid use in case-control studies: Healthy individuals versus hospitalized patients. PLoS ONE. (2017) 12:e0183017. doi: 10.1371/journal.pone.0183017
Keywords: gastrointestinal neoplasms, food frequency questionnaire, fat, diet, colorectal cancer
Citation: Seyyedsalehi MS, Collatuzzo G, Huybrechts I, Hadji M, Rashidian H, Safari-Faramani R, Alizadeh-Navaei R, Kamangar F, Etemadi A, Pukkala E, Gunter MJ, Chajes V, Boffetta P and Zendehdel K (2022) Association between dietary fat intake and colorectal cancer: A multicenter case-control study in Iran. Front. Nutr. 9:1017720. doi: 10.3389/fnut.2022.1017720
Received: 12 August 2022; Accepted: 24 October 2022;
Published: 16 November 2022.
Edited by:
Mainul Haque, National Defense University of Malaysia, MalaysiaReviewed by:
Sumaira Mubarik, Wuhan University, ChinaCopyright © 2022 Seyyedsalehi, Collatuzzo, Huybrechts, Hadji, Rashidian, Safari-Faramani, Alizadeh-Navaei, Kamangar, Etemadi, Pukkala, Gunter, Chajes, Boffetta and Zendehdel. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Paolo Boffetta, cGFvbG8uYm9mZmV0dGFAdW5pYm8uaXQ=; Kazem Zendehdel, a3plbmRlaEB0dW1zLmFjLmly
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.