 Tommaso Pessarelli
Tommaso Pessarelli Andrea Sorge
Andrea Sorge Luca Elli
Luca Elli Andrea Costantino
Andrea Costantino
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Nutr., 08 November 2022
Sec. Nutritional Immunology
Volume 9 - 2022 | https://doi.org/10.3389/fnut.2022.1007716
This article is part of the Research TopicThe Gluten-Free and Low-FODMAP Diet in the Management of Food IntolerancesView all 4 articles
This review summarizes current knowledge on the role of low-FODMAP diet and gluten-free diet in functional abdominal bloating and distension, an emerging disorder of gut-brain interaction characterized by remarkable costs for healthcare systems and a significant impact on the patient’s quality of life. Ingested food plays a key role in the pathophysiology of disorders of gut-brain interaction as up to 84% of patients with irritable bowel syndrome (IBS) report food-triggered symptoms. Potential pathogenetic mechanisms of food-related symptoms in these patients are discussed, focusing on bloating and abdominal distension. These mechanisms provide the rationale for dietary treatment in patients with functional abdominal bloating and distension. The role of fermentable oligosaccharides, disaccharides, monosaccharides, and polyols (FODMAPs) and gluten in functional abdominal bloating and distension is examined. Current literature evaluating the efficacy of the low-FODMAP diet and the gluten-free diet in abdominal bloating and distension is analyzed. Available evidence originates mainly from studies on patients with IBS, since clinical studies on selected cohorts of patients with only functional abdominal bloating and distension have been missing to date. Promising evidence on the potential efficacy of the low-FODMAP diet in functional abdominal bloating and distension is provided by the reduction of the bloating observed in patients with IBS. Regarding the gluten-free diet, there is insufficient evidence to recommend it to reduce bloating and abdominal distension. In conclusion, this review asserts the need for a close collaboration with experts in nutrition to optimize the management of these patients and reduce the risks associated with elimination diets.
Disorders of gut-brain interaction (DGBI), previously known as functional gastrointestinal disorders, affect approximately 40% of the population worldwide (1). Accounting for more than one third of new patient referrals to tertiary hospitals, DGBI represent one of the leading causes of gastroenterological evaluation (2) and have relevant global health care costs (3, 4). Among gastrointestinal (GI) symptoms of patients with DBGI, abdominal bloating is one of the most frequent, affecting 3.5% of the general population (Female:Male = 2:1) (1) and accounting for approximately 23% of patients referred to a general gastroenterology clinic (2). The impact of chronic abdominal bloating and distension on quality of life is substantial since 75% of patients with bloating characterize their symptoms as moderate to severe (5).
According to the Rome IV criteria, functional abdominal bloating/distension (FABD) refers to recurrent bloating (a sensation of abdominal fullness, pressure, or trapped gas) and/or distension (a measurable increase in abdominal circumference) occurring on average at least 1 day/week, in patients with insufficient criteria for a diagnosis of other DGBI. Diagnostic criteria should be fulfilled for the last 3 months with symptom onset at least 6 months prior to diagnosis (6). Mild abdominal pain related to bloating and minor bowel movement abnormalities may be present as well, but sensations of bloating and/or abdominal distension predominate (6).
Up to 96% of patients with irritable bowel syndrome (IBS) report bloating and abdominal distension, with these symptoms frequently coexisting (7–9), since abdominal distension is reported by 50–60% of patients with bloating (10).
The pathogenesis for FABD is complex, often multifactorial in nature, and incompletely understood. Altered microbiota, abnormal GI motility, abdomino-phrenic dyssynergia, pelvic floor dysfunction, and visceral hypersensitivity are possible factors involved in the physiopathology of this condition (11). A full assessment of the principal secondary aetiologies of FABD (Table 1) must be performed when facing this condition (12).
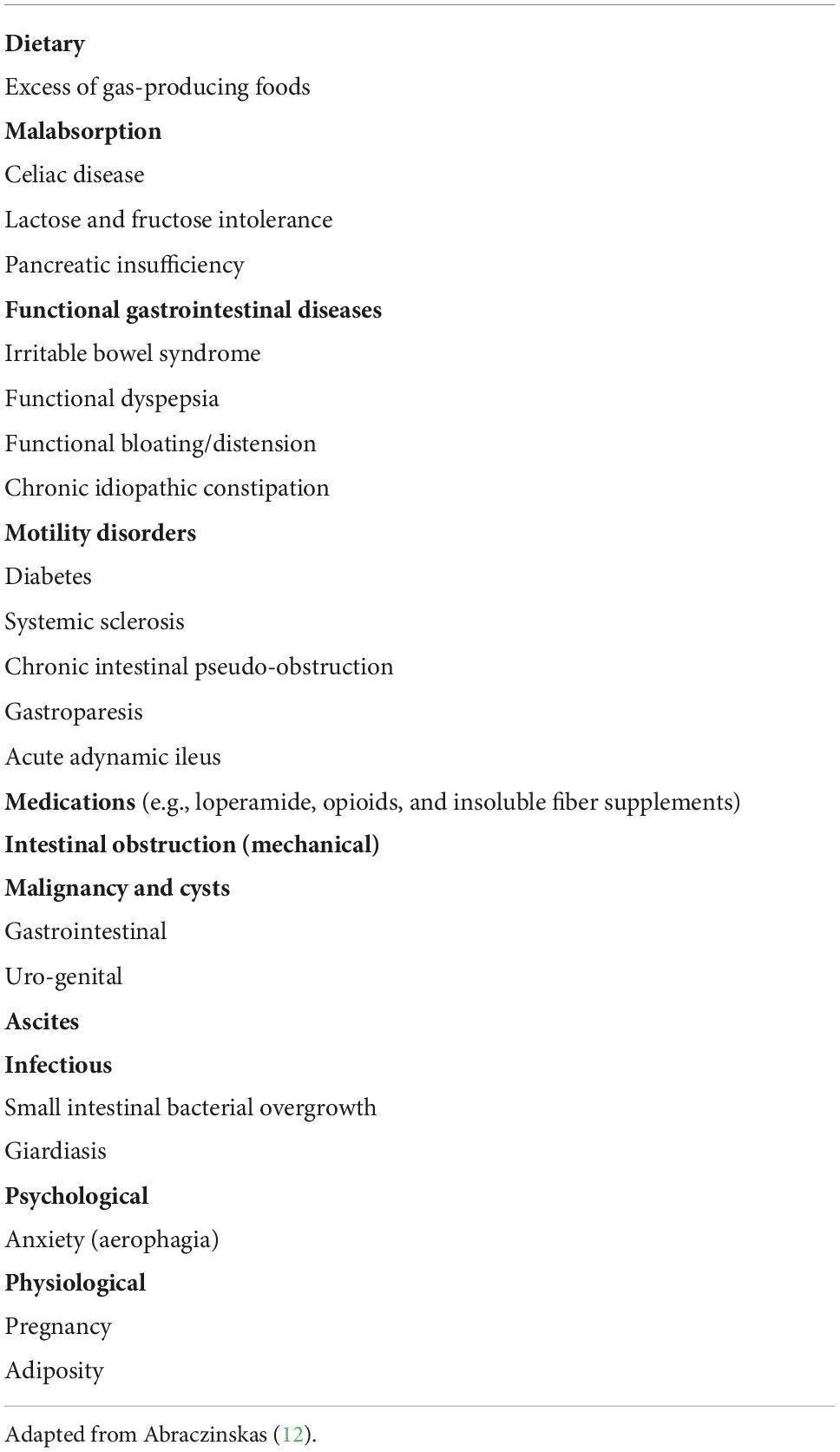
Table 1. Differential diagnosis of abdominal bloating and distension.
The quality of ingested food plays a key role in the pathophysiology of DGBI and patients’ perception of symptoms (13). Nevertheless, there are no dietary guidelines for FABD due to the lack of high-quality studies on this specific condition. Currently, the most widely adopted dietary approaches for FABD are a low fermentable oligosaccharides, disaccharides, monosaccharides, and polyols (FODMAP) diet and the gluten-free diet (GFD). With regards to these exclusion diets the evidence supporting them is limited, especially for the GFD.
The aim of this review is to summarize the most relevant and recent evidence on the effects of GFD and the low-FODMAP diet (LFD) in the management of FABD, therefore providing an updated guide for clinicians in real-life daily practice to optimize the dietary management of these patients.
In recent years, clinical studies evaluating the relationship between dietary interventions and functional GI disorders have increased noticeably. As showed by Böhn et al. up to 84% of IBS patients and a large proportion of subjects with DGBI refer to food-triggered symptoms (13, 14). Several pathophysiological mechanisms have already been proposed to explain the impact of food on the onset of GI symptoms. One of these involves an alteration of GI mechanoreceptors, chemoreceptors, and thermoreceptors responsible for nutrients sensing (15, 16). Another possible underlining mechanism may be a defective processing of nutrients, as some studies suggested a potential role of fructose (17) or lactose intolerance (18) and of lactase-isomaltase polymorphism (19) in patients with DGBI. Food-triggered symptoms might also derive from the hypersensitivity to the distension of the bowel lumen, worsened by ingestion of low-absorbable high-osmolarity aliments (e.g., FODMAPs) (20). Aberrant gut microbiota is another etiologic factor often involved since it may increase FODMAP fermentation leading to lumen distension, production of neuroactive mediators with nociceptive signaling effect and increase of visceral hypersensitivity (21, 22).
According to another hypothesis, an immune-allergic reaction might lead to food-triggered symptoms in DGBI (23). According to this possible mechanism, increased GI permeability and the consequent passage of antigens through the tight junctions might induce a mast-cell mediated reaction leading to symptoms (24, 25).
The available evidence, despite mostly deriving from studies on food-related symptoms in patients with IBS, supports the key role of dietary interventions in the management of patients with DGBI, thus including FABD.
Not all patients with FABD are optimal candidates to dietary prescriptions. In fact, dietary interventions may be mostly effective in patients with meal-related GI symptoms, especially in those who are motivated to introduce the necessary changes in their daily diet. Before dietary prescription, a full nutritional assessment is recommended since restrictive diets should be avoided in patients at risk for malnutrition (26). Moreover, a careful evaluation of dietary history is key since elimination diets may exacerbate psychiatric eating disorders (26). Therefore, a close collaboration with dietitians and nutrition specialists should be offered to optimize the management of these patients. Despite its importance, access to these professional figures can be limited in some healthcare systems.
Due to the lack of clear evidence on symptoms improvement with specific diets in FABD, current dietary prescriptions are mainly based on an empirical approach. A possible approach for FABD patients is the elimination of gas-producing foods (e.g., onions, legumes, cauliflower, celery, bananas, apricots, prunes, broccoli, and wheat bran) and the recommendation of healthy eating habits [e.g., regular meals; restriction of alcohol, coffee, and spicy foods (27, 28)]. In addition, patients are often advised to eliminate foods that trigger their GI symptoms (29). Apart from these approaches, the two most frequently adopted dietary prescriptions are the LFD and the GFD (11).
Fermentable oligosaccharides, disaccharides, monosaccharides, and polyols include lactose, fructose in excess of glucose, sugar polyols (sorbitol and mannitol), fructans, and galacto-oligosaccharides (30). The role of FODMAPs in pathogenesis of functional GI symptoms has been studied mainly in IBS patients. However, due to the significant symptomatic and pathogenetic overlap between FABD and IBS, is conceivable that the same pathophysiological mechanisms are involved (Figure 1). A clear mechanism involves bowel distension; small molecules like fructose, mannitol, sorbitol, and lactulose all exert a direct osmotic force, which increases intraluminal water (31). This has been demonstrated in studies in which a diet high in sucrose, polyols and fermentable carbohydrates significantly increased total effluent wet weight from ileostomy (32, 33). It was then confirmed in studies that measured small bowel water content through magnetic resonance imaging (MRI), which revealed a significant increase in intestinal water volume after ingestion of 17.5 g mannitol solutions or 40 g of fructose (34, 35). On the other hand, longer molecules or fermentable carbohydrates non-digested and/or non-absorbed in the small intestine distend the colon through hydrogen and methane produced by microbial fermentation (35). Interestingly, a recent study revealed that, after FODMAPs ingestion, breath hydrogen, and colonic volume kinetics measured by MRI were equally increased in IBS patients and healthy individuals (36).
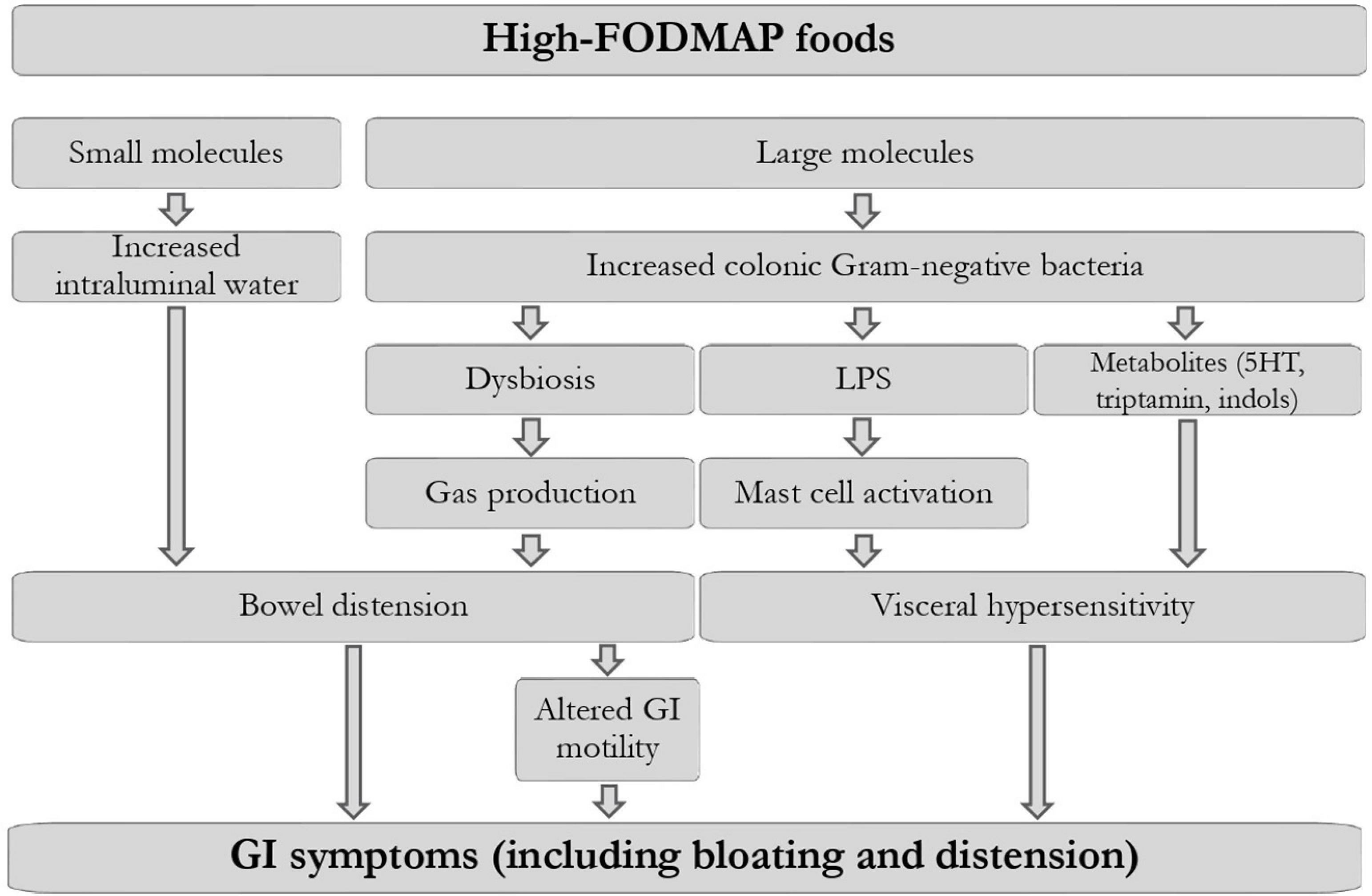
Figure 1. Proposed pathogenetic mechanisms leading to gastrointestinal symptoms, including bloating, after FODMAPs ingestion in predisposed individuals. Modified from Singh et al. (47) and Van den Houte et al. (16). LPS, lipopolysaccharide; 5HT, 5-hydroxytryptamine; GI, gastrointestinal.
Another study based on computed tomography imaging showed that luminal gas increases only in 25% of patients with functional GI disorders during a spontaneous episode of abdominal distension or following consumption of a “high-flatulence” diet, thus questioning the role of luminal distension in the genesis of bloating and abdominal distension (37). Hence, visceral hypersensitivity to distension rather than excess of colonic gas may be largely responsible for food-related symptoms (38).
Another possible mechanism underlying FODMAP-related symptoms in FABD is aberrant intestinal motility since bowel distension can lead to an acceleration of bowel transit. Madsen et al. showed that the small intestinal transit time is decreased following ingestion of a 30 g fructose-sorbitol mixture in healthy individuals (39).
A high-FODMAP diet may also lead to dysbiosis and visceral hypersensitivity, pathogenetic factors strictly related with FABD. Rodent studies suggest that FODMAPs may cause dysbiosis and an increase in gram-negative bacteria, and consequently the luminal lipopolysaccharide, which can activate mast-cells (22, 40). Subsequently, tryptase, histamine, and prostaglandin E2 released by mast-cells can increase intestinal permeability and cause visceral sensitivity. Furthermore, a FODMAP-rich meal has been shown to increase hydrogen production and induce GI symptoms in IBS, in association with metabolome and microbiota alterations (41). In fact, an imbalance in the intestinal microbiota species may lead to aberrant by-products (e.g., methane and hydrogen) showing that the relationship between microbiota and FODMAP-containing food in the genesis of bloating and abdominal distension could be bidirectional (42).
Several studies reported the average FODMAP content of the majority of foods (43–45). Consequently, the criteria for classifying a food as low in FODMAPs were defined according to specific cut-off values for each FODMAP element including fructose in excess of glucose, oligosaccharides (fructans plus galacto-oligosaccharides), polyols (sorbitol and mannitol), and lactose (46). More specifically a low-FODMAP food must contain:
– less than 0.3 g per serve (g/serve) or less than 0.2 g/serve of oligosaccharides (for core grain products, legumes, nuts and seeds or for vegetables, fruits, and all other products, respectively)
– less than 0.4 g/serve of total polyols
– less than 0.4 g/serve of excess fructose
– less than 1 g/serve of lactose.
The LFD consists of three phases. In the first phase, ideally lasting 2–8 weeks, the aim is to restrict the intake of high-FODMAP foods, substituting them with suitable low-FODMAP aliments of the same food group (47). In the absence of clinical benefit after this period, a trial with an alternative treatment is advisable. In the second phase, a rechallenge with single high-FODMAPs-containing foods, gradually reintroduced by patient’s nutritional needs and preferences, is performed every 2–3 days to enable identification of specific food triggers and reintroduction of tolerated foods into the diet (48). In the third phase a personalized maintenance diet should be defined, by avoidance of foods causing severe symptoms and reintroduction of well-tolerated, FODMAPs-containing foods. Notably, adherence to the second and third phases might be unsatisfying in the absence of support by a dietitian. New technologies, such as mobile applications (49) or telemedicine (50) may be helpful in increasing adherence to dietician recommendations and improving outcomes.
In the last decade, some randomized controlled trials (RCTs) and meta-analyses showed that the first phase of the diet is efficacious for global IBS symptoms (51–53). Thus, both the National Institute for Health and Care Excellence guidelines and the American College of Gastroenterology guidelines recommend the LFD for the management of IBS (27, 54), with both guidelines underlining the necessity of a trained GI dietician to monitor patients during the diet. In fact, the dietician’s work is key to tailor a balanced, varied and minimally restrictive diet.
Although studies evaluating the effects of LFD on selected cohorts of patients with FABD are scant, a low-FODMAPs diet may have a beneficial effect in FABD through the proposed pathogenetic mechanisms (see Paragraph 3.1.1).
Indirect evidence on the potential efficacy of LFD in FABD is provided by the reduction of bloating in patients with IBS. We included in this narrative review all meta-analysis assessing the effects of LFD on bloating in patients with IBS. Clinical trials contained in the meta-analysis were not discussed singularly to avoid redundancy. We also summarized some recent RCTs studying the efficacy of LFD on bloating and abdominal distention in other conditions than IBS.
The meta-analysis by Marsh et al. included six RCTs in which bloating (among other GI symptoms) was assessed at baseline and after 3–6 weeks in a total of 182 patients who underwent restriction of high-FODMAP foods and in 172 patients of control groups who continued their standard diet (55). This study showed a significant reduction of bloating, assessed through the IBS severity scoring system (IBS-SSS), in patients following the LFD.
In a more recent meta-analysis, Black et al. selected 12 RCTs that studied the effect of an LFD on GI symptoms, including abdominal bloating and distension in adult patients with IBS of any subtype (56). Trials that were included in this meta-analysis compared the effects of 3–6 weeks of LFD with an alternative intervention that could consist of any of habitual diet, sham dietary advice, a high-FODMAP diet or alternative dietary advice. The LFD ranked first in bloating improvement compared to all other dietary interventions, with statistical significance if compared with British Dietetic Association dietary advice. Another meta-analysis including three RCTs comparing 4 weeks LFD versus traditional IBS diet, three RCTs comparing LFD and high-FODMAP diet (11 days to 3 weeks of intervention) and six cohort studies comparing IBS symptoms (including bloating) at basal level and after 3 weeks to 15 months of LFD revealed a significant improvement of bloating in the low-FODMAP groups (57).
Some RCTs investigated the effects of LFD in other conditions than IBS. In a recent RCT, 19 patients with ulcerative colitis in remission and concomitant IBS underwent an 8-week randomized FODMAP elimination with double-blinded, crossover provocations of FODMAP and placebo (58). Eliminating FODMAPs-containing foods for 2 weeks resulted in a 56% reduction of bloating, assessed through Visual Analog Scale (VAS). Eliminating FODMAPs-containing foods for 2 weeks resulted in a 56% reduction of bloating, assessed through the visual analog scale. After the subsequent provocations, bloating scores returned to baseline levels in both FODMAPs and placebo groups, perhaps due to the known nocebo effect in patients with DGBI (59, 60).
In another RCT, patients with a quiescent inflammatory bowel disease and functional GI symptoms responsive to the LFD were allocated either to a 3-day fructan challenge or a 3-day glucose challenge. There was greater severity of bloating on the final day of the fructan challenge compared with glucose (61).
In another RCT, 105 patients with functional dyspepsia were randomized in the LFD group and in a traditional dietary advice group. This study revealed that the subgroup of patients with associated bloating had significantly better symptomatic response with LFD and on multivariate analysis, one of the two factors predicting response to LFD was bloating (62).
Celiac Disease (CD) and Wheat Allergy (WA) are classically considered as the two main gluten-related diseases, accounting for 1% prevalence in general population and pediatric population, respectively (63, 64). CD diagnosis requires clinical, serological and histological parameters while diagnosis of WA requires typical allergic symptoms associated with wheat assumption and the presence of specific IgE (65, 66).
In the last decade, a considerable rise in self-reported wheat sensitivity and avoidance of gluten in absence of a diagnosis of CD has been described (67) and it has been suggested that gluten might also play a role in DGBI, as some patients with IBS report GI and extra-intestinal symptoms after the ingestion of gluten (68). Consequently, the gluten-free industry grew exponentially, reaching estimated yearly retail sales of USD 24 billion (69). Large population studies suggested a prevalence of self-reported wheat sensitivity between 4 and 15% of the general population (67, 69–71).
The Salerno Experts’ Criteria defined non-celiac gluten sensitivity (NCGS) as a condition characterized by intestinal symptoms, the most frequent being bloating and abdominal pain, and extra-intestinal symptoms related to the ingestion of gluten-containing food in subjects where CD and WA had been excluded (72). A full diagnostic workup for NCGS should assess the clinical response to a GFD and then measure the effect of a gluten challenge (72).
A realistic estimate of non-celiac gluten/wheat sensitivity (NCGWS) world prevalence is lacking, mainly due to high rates of self-diagnosis and lack of standardized international diagnostic criteria or biomarkers (73), but it has been suggested that NCGWS might affect a large proportion of the population ranging from 0.6 to 13% (74, 75).
The clinical presentation of NCGWS may be indistinguishable from that of many DGBI (thus including FABD), leading some experts to suggest that NCGWS may represent a subgroup of IBS (wheat-sensitive IBS) (76, 77). Nevertheless, approximately 70% of patients considered to have NCGWS report bloating (11, 78), thus supporting the potential beneficial effect of the GFD in highly selected patients with FABD.
A commonly accepted cut-off to define the gluten contamination potentially generating symptoms and/or histologic alterations in celiac patients is 10 mg of gluten, or 500 g of food containing 20 milligrams/kilogram of gluten. However, there is a tremendous degree of variability within this population, since some patients may have worsening histological changes with very low daily gluten exposure (79). Due to clinical overlap with other DGBI, a similar cut-off was not defined for NCGWS patients. The average daily gluten intake in a Western diet is thought to vary from 5 to 20 g/day, with wheat-containing bread being one of major sources of gluten (each slice of bread contains approximately 4 g of gluten) (80).
A strict adherence to the GFD is the only safe and recommended treatment for patients with CD, whereas for patients with NCGWS and wheat-sensitive IBS a clear benefit is far from being proven.
The GFD consists of the complete exclusion of wheat, rye, and barley from the diet. Although commercial oat products are frequently labeled as gluten-free, they might be are often contaminated (81). Besides gluten, several components of these cereals are potentially involved in the pathogenesis of GI diseases and symptoms (82). As an example, amylase–trypsin inhibitors can cause wheat allergies and FODMAPs can induce symptoms of IBS (83).
GFD is associated with potential drawbacks. When eliminating gluten, patients may reduce variety, balance, and nutritive value of their diet, as gluten-free products are often low in fiber, vitamins, and other micronutrients (e.g., calcium, iron, and magnesium). In any case, common gluten-free products are often enriched to reduce the risk of nutritional imbalances. Higher levels of lipids, trans fat, protein, and salt were reported in studies evaluating the nutritional composition of processed gluten-free products (84–87). Notably, poor nutrition is not the only potential issue of the GFD. Although the overall effect of the GFD on cardiovascular risk is unclear, many studies showed that it may increase total cholesterol, high-density lipoprotein, fasting glycemia, and body mass index (88–91). Thus, to ensure the safety and efficacy of the GFD, the indication should be evaluated by a specialized gastroenterologist and a dietary planning guidance from a nutritionist or dietitian should be provided to assess the fulfillment of all nutritional needs and prevent deficiency of key nutrients and malnutrition (68, 92). To avoid the risk of malnutrition in patients with gluten-related disorders, a combination of the Mediterranean diet and the GFD has been proposed as an alternative to reach a healthy gluten-free state (93). In addition, the GFD may have a considerable psychological impact and interfere with social life, also due to low availability, high costs, and food labeling of gluten-free products, which may also limit adherence to the diet (94).
Considering the clinical overlap between NCGWS and DGBI (including FABD), there may be a rationale for prescribing the GFD to highly selected patients with FABD, especially to those reporting gluten-related symptoms. However, as for the LFD, scientific data about the effects of GFD in patients with FABD are lacking and the few results on the potential efficacy of GFD in bloating and abdominal distension come from studies on patients with IBS. We analyzed the only two RCTs and the only meta-analysis evaluating the effects of GFD on bloating in IBS. We also reported the only clinical trial assessing the effects of a gluten challenge on bloating in NCGS and the only meta-analysis comparing LFD, GFD and balanced traditional diet on bloating in IBS.
A RCT of 34 IBS patients symptomatically controlled on a GFD showed a significant worsening of symptoms, including bloating, after ingestion of gluten for up to 6 weeks compared to the placebo control group (95).
In another double-blind randomized placebo-controlled trial, 72 IBS patients followed a GFD for up to 6 weeks and then either received powdered gluten or placebo. In the gluten-containing group all symptoms, including bloating, significantly improved after 6 weeks of GFD and significantly increased after 1 week of gluten reintroduction (96).
A recent meta-analysis including the two previously reported RCTs showed results that were not statistically significant due to the low number of studies and patients, and the high heterogeneity between individual trial results. This suggests that there is insufficient evidence to recommend a GFD to reduce bloating and abdominal distension (53).
In another RCT, 61 adults with a diagnosis of NCGS were assigned to groups given either low quantities of gluten or a placebo for 1 week, with subsequent crossover. This study revealed that intake of gluten significantly increased the severity of abdominal bloating (97).
A recent clinical trial investigated the effects of 4 weeks of LFD, GFD, and a balanced traditional diet (12 total weeks of diet) on 42 IBS patients, showing a beneficial effect of all three diets on bloating (98). The comparison of the three diets revealed a superiority of the LFD over the others in decreasing abdominal bloating. However, a limitation of this study is that LFD was administered as a first diet in all patients, thus potentially contributing to this result.
Functional abdominal bloating/distension is a highly prevalent clinical entity that, due to the clinical overlap with IBS and other DGBI, is frequently underdiagnosed. Hence, studies on selected cohorts of patients with this condition are lacking. Dietary treatment is currently a cornerstone of the management of several DGBI, including FABD.
Currently, two of the most frequently prescribed dietary regimens in FABD are the LFD and the GFD. Although specific studies on patients with FABD are needed to investigate the role of different dietary regimens, current evidence may justify the prescription of the LFD in these patients, while the recommendation of the GFD is not currently supported by clear evidence.
In conclusion, although studies in patients with IBS and bloating revealed promising results, especially for the LFD, interventional studies on patients affected by FABD are needed to increase our knowledge on the efficacy of dietary interventions in this condition.
TP, AS, and AC: conceptualization. TP and AS: writing of the original draft. TP, AS, LE, and AC: critical revision of the manuscript and editing. All authors contributed to the article and approved the submitted version.
This study was partially funded by the Italian Ministry of Health, Current Research IRCCS.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Sperber AD, Bangdiwala SI, Drossman DA, Ghoshal UC, Simren M, Tack J, et al. Worldwide prevalence and burden of functional gastrointestinal disorders, results of rome foundation global study. Gastroenterology. (2021) 160:99.e–114.e. doi: 10.1053/j.gastro.2020.04.014
2. Shivaji UN, Ford AC. Prevalence of functional gastrointestinal disorders among consecutive new patient referrals to a gastroenterology clinic. Frontline Gastroenterol. (2014) 5:266–71. doi: 10.1136/flgastro-2013-100426
3. Sandler RS, Everhart JE, Donowitz M, Adams E, Cronin K, Goodman C, et al. The burden of selected digestive diseases in the United States. Gastroenterology. (2002) 122:1500–11. doi: 10.1053/gast.2002.32978
4. Tack J, Stanghellini V, Mearin F, Yiannakou Y, Layer P, Coffin B, et al. Economic burden of moderate to severe irritable bowel syndrome with constipation in six European countries. BMC Gastroenterol. (2019) 19:69. doi: 10.1186/s12876-019-0985-1
5. Spiegel B, Strickland A, Naliboff BD, Mayer EA, Chang L. Predictors of patient-assessed illness severity in irritable bowel syndrome. Am J Gastroenterol. (2008) 103:2536–43. doi: 10.1111/j.1572-0241.2008.01997.x
6. Drossman DA. Functional gastrointestinal disorders: History, pathophysiology, clinical features and Rome IV. Gastroenterology. (2016) S0016–5085:223–7.
7. Tuteja AK, Talley NJ, Joos SK, Tolman KG, Hickam DH. Abdominal bloating in employed adults: Prevalence, risk factors, and association with other bowel disorders. Am J Gastroenterol. (2008) 103:1241–8. doi: 10.1111/j.1572-0241.2007.01755.x
8. Talley NJ, Boyce P, Jones M. Identification of distinct upper and lower gastrointestinal symptom groupings in an urban population. Gut. (1998) 42:690–5. doi: 10.1136/gut.42.5.690
9. Jiang X, Locke GR III, Choung RS, Zinsmeister AR, Schleck CD, Talley NJ. Prevalence and risk factors for abdominal bloating and visible distention: A population-based study. Gut. (2008) 57:756–63. doi: 10.1136/gut.2007.142810
10. Serra J, Azpiroz F, Malagelada JR. Impaired transit and tolerance of intestinal gas in the irritable bowel syndrome. Gut. (2001) 48:14–9. doi: 10.1136/gut.48.1.14
11. Lacy BE, Cangemi D, Vazquez-Roque M. Management of chronic abdominal distension and bloating. Clin Gastroenterol Hepatol. (2021) 19:219.e–31.e. doi: 10.1016/j.cgh.2020.03.056
12. Abraczinskas D. Overview of intestinal gas and bloating. In: Post TW editor. UpToDate. Waltham, MA: UpToDate (2022).
13. Böhn L, Störsrud S, Törnblom H, Bengtsson U, Simrén M. Self-reported food-related gastrointestinal symptoms in IBS are common and associated with more severe symptoms and reduced quality of life. Am J Gastroenterol. (2013) 108:634–41.s doi: 10.1038/ajg.2013.105
14. Simrén M, Månsson A, Langkilde AM, Svedlund J, Abrahamsson H, Bengtsson U, et al. Food-related gastrointestinal symptoms in the irritable bowel syndrome. Digestion. (2001) 63:108–15. doi: 10.1159/000051878
15. Farré R, Tack J. Food and symptom generation in functional gastrointestinal disorders: Physiological aspects. Am J Gastroenterol. (2013) 108:698–706. doi: 10.1038/ajg.2013.24
16. Van den Houte K, Bercik P, Simren M, Tack J, Vanner S. Mechanisms underlying food-triggered symptoms in disorders of gut-brain interactions. Am J Gastroenterol. (2022) 117:937–46. doi: 10.14309/ajg.0000000000001812
17. Melchior C, Douard V, Coëffier M, Gourcerol G. Fructose and irritable bowel syndrome. Nutr Res Rev. (2020) 33:235–43. doi: 10.1017/S0954422420000025
18. Vesa TH, Seppo LM, Marteau PR, Sahi T, Korpela R. Role of irritable bowel syndrome in subjective lactose intolerance. Am J Clin Nutr. (1998) 67:710–5. doi: 10.1093/ajcn/67.4.710
19. Henström M, Diekmann L, Bonfiglio F, Hadizadeh F, Kuech EM, von Köckritz-Blickwede M, et al. Functional variants in the sucrase-isomaltase gene associate with increased risk of irritable bowel syndrome. Gut. (2018) 67:263–70. doi: 10.1136/gutjnl-2016-312456
20. Staudacher HM, Irving PM, Lomer MC, Whelan K. Mechanisms and efficacy of dietary FODMAP restriction in IBS. Nat Rev Gastroenterol Hepatol. (2014) 11:256–66. doi: 10.1038/nrgastro.2013.259
21. Zhou SY, Gillilland M III, Wu X, Leelasinjaroen P, Zhang G, Zhou H, et al. FODMAP diet modulates visceral nociception by lipopolysaccharide-mediated intestinal inflammation and barrier dysfunction. J Clin Invest. (2018) 128:267–80. doi: 10.1172/JCI92390
22. Singh P, Grabauskas G, Zhou SY, Gao J, Zhang Y, Owyang C. High FODMAP diet causes barrier loss via lipopolysaccharide-mediated mast cell activation. JCI Insight. (2021) 6:e146529. doi: 10.1172/jci.insight.146529
23. Tack J, Schol J, Van den Houte K, Huang IH, Carbone F. Paradigm Shift: Functional dyspepsia-A “Leaky Gut”. Disorder? Am J Gastroenterol. (2021) 116:274–5. doi: 10.14309/ajg.0000000000001077
24. Nojkov B, Zhou SY, Dolan RD, Davis EM, Appelman HD, Guo X, et al. Evidence of duodenal epithelial barrier impairment and increased pyroptosis in patients with functional dyspepsia on confocal laser endomicroscopy and “Ex Vivo” Mucosa analysis. Am J Gastroenterol. (2020) 115:1891–901. doi: 10.14309/ajg.0000000000000827
25. Vanuytsel T, van Wanrooy S, Vanheel H, Vanormelingen C, Verschueren S, Houben E, et al. Psychological stress and corticotropin-releasing hormone increase intestinal permeability in humans by a mast cell-dependent mechanism. Gut. (2014) 63:1293–9. doi: 10.1136/gutjnl-2013-305690
26. Chey WD, Hashash JG, Manning L, Chang L. AGA clinical practice update on the role of diet in irritable bowel syndrome: Expert review. Gastroenterology. (2022) 162:1737.e–45.e. doi: 10.1053/j.gastro.2021.12.248
27. Hookway C, Buckner S, Crosland P, Longson D. Irritable bowel syndrome in adults in primary care: Summary of updated NICE guidance. BMJ. (2015) 350:h701. doi: 10.1136/bmj.h701
28. McKenzie YA, Bowyer RK, Leach H, Gulia P, Horobin J, O’Sullivan NA, et al. British dietetic association systematic review and evidence-based practice guidelines for the dietary management of irritable bowel syndrome in adults (2016 update). J Hum Nutr Diet. (2016) 29:549–75. doi: 10.1111/jhn.12385
29. Algera J, Colomier E, Simrén M. The Dietary management of patients with irritable bowel syndrome: A narrative review of the existing and emerging evidence. Nutrients. (2019) 11:2162. doi: 10.3390/nu11092162
30. Gibson PR. History of the low FODMAP diet. J Gastroenterol Hepatol. (2017) 32(Suppl. 1):5–7. doi: 10.1111/jgh.13685
31. Barrett JS, Gearry RB, Muir JG, Irving PM, Rose R, Rosella O, et al. Dietary poorly absorbed, short-chain carbohydrates increase delivery of water and fermentable substrates to the proximal colon. Aliment Pharmacol Ther. (2010) 31:874–82. doi: 10.1111/j.1365-2036.2010.04237.x
32. Berghouse L, Hori S, Hill M, Hudson M, Lennard-Jones JE, Rogers E. Comparison between the bacterial and oligosaccharide content of ileostomy effluent in subjects taking diets rich in refined or unrefined carbohydrate. Gut. (1984) 25:1071–7. doi: 10.1136/gut.25.10.1071
33. Langkilde AM, Andersson H, Schweizer TF, Würsch P. Digestion and absorption of sorbitol, maltitol and isomalt from the small bowel. A study in ileostomy subjects. Eur J Clin Nutr. (1994) 48:768–75.
34. Spiller R. How do FODMAPs work? J Gastroenterol Hepatol. (2017) 32(Suppl. 1):36–9. doi: 10.1111/jgh.13694
35. Murray K, Wilkinson-Smith V, Hoad C, Costigan C, Cox E, Lam C, et al. Differential effects of FODMAPs (fermentable oligo-, di-, mono-saccharides and polyols) on small and large intestinal contents in healthy subjects shown by MRI. Am J Gastroenterol. (2014) 109:110–9. doi: 10.1038/ajg.2013.386
36. Major G, Pritchard S, Murray K, Alappadan JP, Hoad CL, Marciani L, et al. Colon hypersensitivity to distension, rather than excessive gas production, produces carbohydrate-related symptoms in individuals with irritable bowel syndrome. Gastroenterology. (2017) 152:124.e–33.e. doi: 10.1053/j.gastro.2016.09.062
37. Bendezú RA, Barba E, Burri E, Cisternas D, Malagelada C, Segui S, et al. Intestinal gas content and distribution in health and in patients with functional gut symptoms. Neurogastroenterol Motil. (2015) 27:1249–57. doi: 10.1111/nmo.12618
38. Zhu Y, Zheng X, Cong Y, Chu H, Fried M, Dai N, et al. Bloating and distention in irritable bowel syndrome: The role of gas production and visceral sensation after lactose ingestion in a population with lactase deficiency. Am J Gastroenterol. (2013) 108:1516–25. doi: 10.1038/ajg.2013.198
39. Madsen JL, Linnet J, Rumessen JJ. Effect of nonabsorbed amounts of a fructose-sorbitol mixture on small intestinal transit in healthy volunteers. Dig Dis Sci. (2006) 51:147–53. doi: 10.1007/s10620-006-3100-8
40. Ford AC, Moayyedi P, Chey WD, Harris LA, Lacy BE, Saito YA, et al. American college of gastroenterology monograph on management of irritable bowel syndrome. Am J Gastroenterol. (2018) 113(Suppl 2):1–18. doi: 10.1038/s41395-018-0084-x
41. Ong DK, Mitchell SB, Barrett JS, Shepherd SJ, Irving PM, Biesiekierski JR, et al. Manipulation of dietary short chain carbohydrates alters the pattern of gas production and genesis of symptoms in irritable bowel syndrome. J Gastroenterol Hepatol. (2010) 25:1366–73. doi: 10.1111/j.1440-1746.2010.06370.x
42. El-Salhy M, Hatlebakk JG, Hausken T. Diet in irritable bowel syndrome (IBS): Interaction with gut microbiota and gut hormones. Nutrients. (2019) 11:1824. doi: 10.3390/nu11081824
43. Muir JG, Shepherd SJ, Rosella O, Rose R, Barrett JS, Gibson PR. Fructan and free fructose content of common Australian vegetables and fruit. J Agric Food Chem. (2007) 55:6619–27. doi: 10.1021/jf070623x
44. Muir JG, Rose R, Rosella O, Liels K, Barrett JS, Shepherd SJ, et al. Measurement of short-chain carbohydrates in common Australian vegetables and fruits by high-performance liquid chromatography (HPLC). J Agric Food Chem. (2009) 57:554–65. doi: 10.1021/jf802700e
45. Biesiekierski JR, Rosella O, Rose R, Liels K, Barrett JS, Shepherd SJ, et al. Quantification of fructans, galacto-oligosacharides and other short-chain carbohydrates in processed grains and cereals. J Hum Nutr Diet. (2011) 24:154–76. doi: 10.1111/j.1365-277X.2010.01139.x
46. Varney J, Barrett J, Scarlata K, Catsos P, Gibson PR, Muir JG. FODMAPs: Food composition, defining cutoff values and international application. J Gastroenterol Hepatol. (2017) 32(Suppl. 1):53–61. doi: 10.1111/jgh.13698
47. Singh P, Tuck C, Gibson PR, Chey WD. The role of food in the treatment of bowel disorders: Focus on irritable bowel syndrome and functional constipation. Am J Gastroenterol. (2022) 117:947–57. doi: 10.14309/ajg.0000000000001767
48. Tuck C, Barrett J. Re-challenging FODMAPs: The low FODMAP diet phase two. J Gastroenterol Hepatol. (2017) 32 Suppl 1:11–5. doi: 10.1111/jgh.13687
49. Dimidi E, Whelan K, Lomer MCE. FODMAP-specific mobile application: Impact on gut symptoms in 11,689 people, and dietary triggers in 2,053 people. Proc Nutr Soc. (2020) 79:E8. doi: 10.1017/S0029665119001290
50. Costantino A, Roncoroni L, Noviello D, Nandi N, Lombardo V, Scricciolo A, et al. Nutritional and gastroenterological monitoring of patients with celiac disease during COVID-19 pandemic: The emerging role of telemedicine and point-of-care gluten detection tests. Front Nutr. (2021) 8:622514. doi: 10.3389/fnut.2021.622514
51. Eswaran SL, Chey WD, Han-Markey T, Ball S, Jackson K. A randomized controlled trial comparing the low FODMAP Diet vs. Modified NICE guidelines in US adults with IBS-D. Am J Gastroenterol. (2016) 111:1824–32. doi: 10.1038/ajg.2016.434
52. van Lanen AS, de Bree A, Greyling A. Efficacy of a low-FODMAP diet in adult irritable bowel syndrome: A systematic review and meta-analysis. Eur J Nutr. (2021) 60:3505–22. doi: 10.1007/s00394-020-02473-0
53. Dionne J, Ford AC, Yuan Y, Chey WD, Lacy BE, Saito YA, et al. A systematic review and meta-analysis evaluating the efficacy of a gluten-free diet and a low FODMAPs diet in treating symptoms of irritable bowel syndrome. Am J Gastroenterol. (2018) 113:1290–300. doi: 10.1038/s41395-018-0195-4
54. Lacy BE, Pimentel M, Brenner DM, Chey WD, Keefer LA, Long MD, et al. ACG clinical guideline: Management of irritable bowel syndrome. Am J Gastroenterol. (2021) 116:17–44. doi: 10.14309/ajg.0000000000001036
55. Marsh A, Eslick EM, Eslick GD. Does a diet low in FODMAPs reduce symptoms associated with functional gastrointestinal disorders? A comprehensive systematic review and meta-analysis. Eur J Nutr. (2016) 55:897–906. doi: 10.1007/s00394-015-0922-1
56. Black CJ, Staudacher HM, Ford AC. Efficacy of a low FODMAP diet in irritable bowel syndrome: Systematic review and network meta-analysis. Gut. (2022) 71:1117–26. doi: 10.1136/gutjnl-2021-325214
57. Altobelli E, Del Negro V, Angeletti PM, Latella G. Low-FODMAP diet improves irritable bowel syndrome symptoms: A meta-analysis. Nutrients. (2017) 9:940. doi: 10.3390/nu9090940
58. Melgaard D, Sørensen J, Riis J, Ovesen TS, Leutscher P, Sørensen S, et al. Efficacy of FODMAP elimination and subsequent blinded placebo-controlled provocations in a randomised controlled study in patients with ulcerative colitis in remission and symptoms of irritable bowel syndrome: A feasibility study. Nutrients. (2022) 14:1296. doi: 10.3390/nu14061296
59. Ballou S, Beath A, Kaptchuk TJ, Hirsch W, Sommers T, Nee J, et al. Factors associated with response to placebo in patients with irritable bowel syndrome and constipation. Clin Gastroenterol Hepatol. (2018) 16:1738.e–44.e. doi: 10.1016/j.cgh.2018.04.009
60. Kaptchuk TJ, Kelley JM, Conboy LA, Davis RB, Kerr CE, Jacobson EE, et al. Components of placebo effect: Randomised controlled trial in patients with irritable bowel syndrome. BMJ. (2008) 336:999–1003. doi: 10.1136/bmj.39524.439618.25
61. Cox SR, Prince AC, Myers CE, Irving PM, Lindsay JO, Lomer MC, et al. Fermentable carbohydrates [FODMAPs] exacerbate functional gastrointestinal symptoms in patients with inflammatory bowel disease: A randomised, double-blind, placebo-controlled, cross-over, re-challenge trial. J Crohns Colitis. (2017) 11:1420–9. doi: 10.1093/ecco-jcc/jjx073
62. Goyal O, Nohria S, Batta S, Dhaliwal A, Goyal P, Sood A. Low fermentable oligosaccharides, disaccharides, monosaccharides, and polyols diet versus traditional dietary advice for functional dyspepsia: A randomized controlled trial. J Gastroenterol Hepatol. (2022) 37:301–9. doi: 10.1111/jgh.15694
63. Cianferoni A. Wheat allergy: Diagnosis and management. J Asthma Allergy. (2016) 9:13–25. doi: 10.2147/JAA.S81550
64. Catassi C, Gatti S, Fasano A. The new epidemiology of celiac disease. J Pediatr Gastroenterol Nutr. (2014) 59(Suppl. 1):S7–9. doi: 10.1097/01.mpg.0000450393.23156.59
65. Al-Toma A, Volta U, Auricchio R, Castillejo G, Sanders DS, Cellier C, et al. European society for the study of coeliac disease (ESsCD) guideline for coeliac disease and other gluten-related disorders. United Eur Gastroenterol J. (2019) 7:583–613. doi: 10.1177/2050640619844125
66. Costantino A, Aversano GM, Lasagni G, Smania V, Doneda L, Vecchi M, et al. Diagnostic management of patients reporting symptoms after wheat ingestion. Front Nutr. (2022) 9:1007007. doi: 10.3389/fnut.2022.1007007
67. Cabrera-Chávez F, Dezar GV, Islas-Zamorano AP, Espinoza-Alderete JG, Vergara-Jiménez MJ, Magaña-Ordorica D, et al. Prevalence of self-reported gluten sensitivity and adherence to a gluten-free diet in argentinian adult population. Nutrients. (2017) 9:81. doi: 10.3390/nu9010081
68. Dale HF, Biesiekierski JR, Lied GA. Non-coeliac gluten sensitivity and the spectrum of gluten-related disorders: An updated overview. Nutr Res Rev. (2019) 32:28–37. doi: 10.1017/S095442241800015X
69. Aziz I. The global phenomenon of self-reported wheat sensitivity. Am J Gastroenterol. (2018) 113:945–8. doi: 10.1038/s41395-018-0103-y
70. Tanpowpong P, Ingham TR, Lampshire PK, Kirchberg FF, Epton MJ, Crane J, et al. Coeliac disease and gluten avoidance in New Zealand children. Arch Dis Child. (2012) 97:12–6. doi: 10.1136/archdischild-2011-300248
71. Golley S, Corsini N, Topping D, Morell M, Mohr P. Motivations for avoiding wheat consumption in Australia: Results from a population survey. Public Health Nutr. (2015) 18:490–9. doi: 10.1017/S1368980014000652
72. Catassi C, Elli L, Bonaz B, Bouma G, Carroccio A, Castillejo G, et al. Diagnosis of non-celiac gluten sensitivity (NCGS): The salerno experts’ Criteria. Nutrients. (2015) 7:4966–77. doi: 10.3390/nu7064966
73. Vazquez-Roque M, Oxentenko AS. Nonceliac gluten sensitivity. Mayo Clin Proc. (2015) 90:1272–7. doi: 10.1016/j.mayocp.2015.07.009
74. Aziz I, Dwivedi K, Sanders DS. From coeliac disease to noncoeliac gluten sensitivity; should everyone be gluten free? Curr Opin Gastroenterol. (2016) 32:120–7. doi: 10.1097/MOG.0000000000000248
75. Potter M, Walker MM, Talley NJ. Non-coeliac gluten or wheat sensitivity: Emerging disease or misdiagnosis? Med J Aust. (2017) 207:211–5. doi: 10.5694/mja17.00332
76. Makharia A, Catassi C, Makharia GK. The overlap between irritable bowel syndrome and non-celiac gluten sensitivity: A clinical dilemma. Nutrients. (2015) 7:10417–26. doi: 10.3390/nu7125541
77. Catassi C, Alaedini A, Bojarski C, Bonaz B, Bouma G, Carroccio A, et al. The overlapping area of non-celiac gluten sensitivity (NCGS) and wheat-sensitive irritable bowel syndrome (IBS): An update. Nutrients. (2017) 9:1268. doi: 10.3390/nu9111268
78. Fernández-Bañares F, Arau B, Raga A, Aceituno M, Tristán E, Carrasco A, et al. Long-term effect of a gluten-free diet on diarrhoea- or bloating-predominant functional bowel disease: Role of the ‘Low-Grade Coeliac Score’ and the ‘Coeliac Lymphogram’ in the response rate to the diet. Nutrients. (2021) 13:1812. doi: 10.3390/nu13061812
79. Hollon JR, Cureton PA, Martin ML, Puppa EL, Fasano A. Trace gluten contamination may play a role in mucosal and clinical recovery in a subgroup of diet-adherent non-responsive celiac disease patients. BMC Gastroenterol. (2013) 13:40. doi: 10.1186/1471-230X-13-40
80. Biesiekierski JR. What is gluten? J Gastroenterol Hepatol. (2017) 32(Suppl. 1):78–81. doi: 10.1111/jgh.13703
81. Rodríguez JM, Estévez V, Bascuñán K, Ayala J, Araya M. Commercial oats in gluten-free diet: A persistent risk for celiac patients. Front Nutr. (2022) 9:986282. doi: 10.3389/fnut.2022.986282
82. Gibson PR, Muir JG, Newnham ED. Other dietary confounders: FODMAPS et al. Dig Dis. (2015) 33:269–76. doi: 10.1159/000371401
83. Gibson PR, Skodje GI, Lundin KE. Non-coeliac gluten sensitivity. J Gastroenterol Hepatol. (2017) 32(Suppl. 1):86–9. doi: 10.1111/jgh.13705
84. Saturni L, Ferretti G, Bacchetti T. The gluten-free diet: Safety and nutritional quality. Nutrients. (2010) 2:16–34. doi: 10.3390/nu2010016
85. Maggio A, Orecchio S. Fatty acid composition of gluten-free food (Bakery Products) for celiac people. Foods. (2018) 7:95. doi: 10.3390/foods7060095
86. Segura ME, Rosell CM. Chemical composition and starch digestibility of different gluten-free breads. Plant Foods Hum Nutr. (2011) 66:224–30. doi: 10.1007/s11130-011-0244-2
87. Wild D, Robins GG, Burley VJ, Howdle PD. Evidence of high sugar intake, and low fibre and mineral intake, in the gluten-free diet. Aliment Pharmacol Ther. (2010) 32:573–81. doi: 10.1111/j.1365-2036.2010.04386.x
88. Potter MDE, Brienesse SC, Walker MM, Boyle A, Talley NJ. Effect of the gluten-free diet on cardiovascular risk factors in patients with coeliac disease: A systematic review. J Gastroenterol Hepatol. (2018) 33:781–91. doi: 10.1111/jgh.14039
89. Bakker SF, Tushuizen ME, von Blomberg ME, Mulder CJ, Simsek S. Type 1 diabetes and celiac disease in adults: Glycemic control and diabetic complications. Acta Diabetol. (2013) 50:319–24. doi: 10.1007/s00592-012-0395-0
90. Casella S, Zanini B, Lanzarotto F, Villanacci V, Ricci C, Lanzini A. Celiac disease in elderly adults: Clinical, serological, and histological characteristics and the effect of a gluten-free diet. J Am Geriatr Soc. (2012) 60:1064–9. doi: 10.1111/j.1532-5415.2012.03997.x
91. Barone M, Della Valle N, Rosania R, Facciorusso A, Trotta A, Cantatore FP, et al. A comparison of the nutritional status between adult celiac patients on a long-term, strictly gluten-free diet and healthy subjects. Eur J Clin Nutr. (2016) 70:23–7. doi: 10.1038/ejcn.2015.114
92. Mariani P, Viti MG, Montuori M, La Vecchia A, Cipolletta E, Calvani L, et al. The gluten-free diet: A nutritional risk factor for adolescents with celiac disease? J Pediatr Gastroenterol Nutr. (1998) 27:519–23. doi: 10.1097/00005176-199811000-00004
93. Bascuñán KA, Elli L, Vecchi M, Scricciolo A, Mascaretti F, Parisi M, et al. Mediterranean gluten-free diet: Is it a fair bet for the treatment of gluten-related disorders? Front Nutr. (2020) 7:583981. doi: 10.3389/fnut.2020.583981
94. Roma E, Roubani A, Kolia E, Panayiotou J, Zellos A, Syriopoulou VP. Dietary compliance and life style of children with coeliac disease. J Hum Nutr Diet. (2010) 23:176–82. doi: 10.1111/j.1365-277X.2009.01036.x
95. Biesiekierski JR, Newnham ED, Irving PM, Barrett JS, Haines M, Doecke JD, et al. Gluten causes gastrointestinal symptoms in subjects without celiac disease: A double-blind randomized placebo-controlled trial. Am J Gastroenterol. (2011) 106:508–14. doi: 10.1038/ajg.2010.487
96. Shahbazkhani B, Sadeghi A, Malekzadeh R, Khatavi F, Etemadi M, Kalantri E, et al. Non-celiac gluten sensitivity has narrowed the spectrum of irritable bowel syndrome: A double-blind randomized placebo-controlled trial. Nutrients. (2015) 7:4542–54. doi: 10.3390/nu7064542
97. Di Sabatino A, Volta U, Salvatore C, Biancheri P, Caio G, De Giorgio R, et al. Small amounts of gluten in subjects with suspected nonceliac gluten sensitivity: A randomized, double-blind, placebo-controlled, cross-over trial. Clin Gastroenterol Hepatol. (2015) 13:1604.e–12.e. doi: 10.1016/j.cgh.2015.01.029
Keywords: gluten-free diet (GFD), low-FODMAP diet, gut-brain interaction, functional bloating, abdominal distension, microbiota, functional diseases, diet
Citation: Pessarelli T, Sorge A, Elli L and Costantino A (2022) The low-FODMAP diet and the gluten-free diet in the management of functional abdominal bloating and distension. Front. Nutr. 9:1007716. doi: 10.3389/fnut.2022.1007716
Received: 30 July 2022; Accepted: 17 October 2022;
Published: 08 November 2022.
Edited by:
Karla Bascuñán, University of Chile, ChileReviewed by:
Silvia Salvatore, University of Insubria, ItalyCopyright © 2022 Pessarelli, Sorge, Elli and Costantino. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Luca Elli, bHVjYS5lbGxpQHBvbGljbGluaWNvLm1pLml0
†These authors have contributed equally to this work and share first authorship
‡ORCID: Tommaso Pessarelli, orcid.org/0000-0002-8817-144X; Andrea Sorge, orcid.org/0000-0002-0285-9949; Luca Elli, orcid.org/0000-0002-0873-0759; Andrea Costantino, orcid.org/0000-0003-4345-6051
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.