 Li Ding
Li Ding Qinglin Yang
Qinglin Yang Zhongming Sun
Zhongming Sun Lu Liu1
Lu Liu1 Na Tao
Na Tao Jun Liu
Jun Liu
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Nutr. , 10 October 2022
Sec. Nutritional Epidemiology
Volume 9 - 2022 | https://doi.org/10.3389/fnut.2022.1002044
This article is part of the Research Topic Diet Behavior and Heart Health View all 21 articles
Background and aims: There are limited studies describing the association between dietary intake of one-carbon metabolism nutrients and hyperglycemia. The present study aimed to investigate the association of habitual dietary intake of one-carbon metabolism nutrients with hyperglycemia in a fluorosis area in China, and explored the interaction between these nutrients and fluorosis related to hyperglycemia.
Method: In a cross-sectional study, we recruited 901 villagers, ages ranging from 18–75, in Guizhou Province. Dietary data and other covariate data were obtained through an interviewer-administered questionnaire. We collected venous blood samples from participants who had fasted for one night to obtain fasting blood glucose levels and we categorized dietary intake of betaine, total choline, methionine, folate, vitamins B6 and B12, and choline subclasses into quartiles (Q1–Q4). The lowest quartile (Q1) served as the reference group. An unconditional logistic regression model was used to evaluate the protective effects of a dietary intake of one-carbon nutrients against hyperglycemia. We calculated Odds Ratios (ORs) with 95% confidence intervals (CIs). A presence or absence of fluorosis subgroup analysis was performed to determine the potential effect of fluorosis on hyperglycemia.
Result: After adjusting for potential confounding factors, we found that a greater intake of dietary vitamin B6, total choline and methyl-donor index was inversely associated with the occurrence of hyperglycemia (P-trend <0.05). However, there were no significant associations between hyperglycemia and the dietary intake of folate, vitamin B12, methionine, and betaine. As for the choline subgroups, it showed that the dietary intake of free choline, phosphatidylcholine, and glycerol phosphatidylcholine was negatively correlated with the occurrence of hyperglycemia (P < 0.05). In contrast, there was no statistical association between dietary phosphatidylcholine and sphingomyelin and hyperglycemia (all P > 0.05). The results of subgroup analysis showed that dietary intake of folate, vitamin B6, total choline, free choline, glycerol phosphorylcholine, and phosphocholine had a protective effect against the occurrence of hyperglycemia in the non-fluorosis subgroup, although no effects were observed in the fluorosis subgroup. There were significant interactions between these nutrients and fluorosis (P = 0.010–0.048).
Conclusion: The study demonstrated that higher dietary intake of vitamin B6, total choline, methyl-donor index, free choline, glycerol phosphorylcholine, and phosphocholine in choline compounds were associated with a lower incidence of hyperglycemia. Moreover, the associations were modified by the presence or absence of fluorosis. Further investigation is needed to test the association in large-scale follow-up studies.
Hyperglycemia is an asymptomatic disease involving the development of cardiovascular problems and diabetes. According to the 2017 Global Burden of Disease study, about 1.02 million died from diabetes worldwide; 15.09 million died of cardiovascular and cerebrovascular diseases, among which about 3.54 million died of hyperglycemia (1). The global prevalence of diabetes is estimated at 9.3% (463 million) in 2017 and is predicted to increase to 10.2% (578.8 million) by 2030 (2). Therefore, hyperglycemia is a notably high risk chronic disease (3, 4). Hyperglycemia is preventable through healthy eating, maintaining a normal weight, and physical activity. An intervention study has shown that nutritional supplementation with folic acid, vitamin B12, vitamin B6, choline, and protein altered the cardiometabolic risk profiles of older adults (5). Therefore, this has aroused considerable interest in identifying the association between one-carbon metabolism nutrients and hyperglycemia.
One-carbon metabolites are a series of interconnected metabolic pathways, including the folate and methionine cycles, which provide methyl groups for the synthesis of DNA (6, 7). DNA methylation plays a key role in cardiovascular disease (CVD) and diabetes. The function of one-carbon metabolites and the availability of adequate methyl groups depend on essential nutrients, such as folate, methionine, choline, betaine, vitamin B6, and vitamin B12 (8, 9). Many studies have explored the effect of one-carbon metabolism nutrients on diabetes and CVDs (10, 11). However, most studies have drawn inconsistent conclusions whether hyperglycemia, a risk factor for diabetes and CVDs, is affected by one-carbon metabolism nutrients (12–16). Moreover, evidence from choline and betaine is limited. Studies reported hyperglycemia was associated with choline and betaine in Norway (17) and Newfoundland population (18). However, these associations have not been established in Canadian women (19) and American (20). These studies suggested that the results were inconsistent across countries because of dietary habits. Therefore, it needs to be clarified the association between one-carbon metabolism nutrients and hyperglycemia among Chinese. However, no studies have explored the association of habitual dietary intake of choline and betaine and with risk of hyperglycemia in China.
Previous studies observed a positive effect of fluoride on the incidence and prevalence of diabetes in the USA and Canada (21, 22). It was reported that a higher intake of one-carbon metabolism nutrients was associated with a lower occurrence of fluorosis (23). The interaction between one-carbon metabolism nutrients and fluorosis related to glucose levels needs to be clarified.
The present study aims to comprehensively investigate the associations between dietary intake of six one-carbon metabolism nutrients (betaine, choline, methionine, folate, vitamin B6 and vitamin B12) and hyperglycemia among a Chinese population in areas known for coal-burning fluorosis. The study also explores whether the associations between one-carbon metabolism nutrient intake and hyperglycemia are modified by the presence or absence of fluorosis.
We used a cross-sectional study design conducted in Zhijin County, Guizhou province, China. A two-stage cluster sampling method was used in this study. The three towns of Chadian, Chengguang, and Puweng were selected by simple random sampling approach from 10 towns in Zhijin County. From each of these towns, we selected four villages at random. The 12 villages were Dazai, Ganhe, Gaofeng, Guihua, Guohua, Hehua, Hualuo, Jiangyan, Shangzai, Yutang, Xianfeng, and Moda. Participants were recruited through village doctors and the Center for Disease Control and Prevention from each selected village. Participants diagnosed with either dental fluorosis or skeletal fluorosis were identified as fluorosis patients. The diagnoses of dental fluorosis (WS/T208-2011, China) and skeletal fluorosis (GB 16396–1996) were performed by a specialist from the CDC. A detailed description of the method is described in our previous studies (24, 25). We used the following participant inclusion criteria: (1) participants must have lived in Zhijin County for at least 10 years; and (2) be between 18 and 75 years old. We used the following exclusion criteria: (1) Participants had a prior history of cancer, coronary heart disease, stroke, gout, or kidney disease; (2) Participants' whose eating habits had changed significantly over the past 5 years; (3) Participants who currently had a chronic medical condition that may affect their eating habits, such as cancer, gout or hypertension; (4) Participants with incomplete questionnaire information. The final analyses involved 901 subjects. We obtained post-fasting blood data from all the 901 participants who attended the interview. All of the subjects in this study were provided written informed consent before the interview. This study protocol was approved by the Ethics Committee of Zunyi Medical University.
The data that related to sociodemographic characteristics (age, sex, marital status, education level, average yearly household income, ethnicity, smoking status, and alcohol consumption) and disease history (cancer, endemic fluorosis, coronary heart disease, stroke, gout, and kidney disease) were collected by questionnaires. Smokers were defined as those who smoke cigarettes ≥1/day for at least 1 year. Alcohol drinkers were defined as those who drink ≥50 g alcohol/day for at least 1 year.
Dietary nutrient intake information was collected through a valid and reliable food-frequency questionnaire (FFQ). The participants gave frequency of consumption information (never, daily, weekly, monthly, yearly) for each food item over the previous year. The 75-item FFQ involved seven categories including fruits, animal products, cereals, beans, vegetables, algae and nuts, beverage drinks and soups. Pictures of food portion sizes were offered to help participants to estimate the quantity of food consumption. Then portion size of each food was converted to grams. Daily dietary intakes of one-carbon metabolism nutrients were estimated by multiplying the consumption frequency and portion size of each food by the nutrient content based on the Chinese Food Composition Database. We used the Chinese food composition database to calculate the estimated intake of vitamin B6, B12, folate, and methionine (26). In addition, the USDA choline content database was used to calculate the estimated intake of betaine, choline, and choline subclasses, including free choline, glycerol phosphorylcholine, phosphocholine, phosphatidylcholine, and sphingomyelin (27). Total choline intake was calculated as the sum of choline intake from glycerophosphocholine, phosphocholine, phosphatidylcholine, sphingomyelin and free choline. Previous studies have shown high correlations between USDA and Chinese database estimates for common nutrient intakes. For example, r > 0.90 for B vitamins and methionine indicates the validity of using the USDA database in the Chinese population to evaluate the intake of choline and betaine (28).
Waist Circumference (WC), weight, and body height were measured following a standardized protocol, and body mass index (BMI) was calculated as weight divided by height2 (kg/m2). Weight was measured to the nearest 0.1 kg, and height and WC were measured to the nearest 0.1 cm. Venous blood samples were collected from 7 to 9 am following an overnight fast of at least 8 h. A drop of venous blood was used for bedside measurement of blood glucose, using the Accu-Chek Active glucometer (Roche Diagnostics GmbH, Germany). According to the World Health Organization (WHO) (29), patients with fasting glucose ≥6.1 mmol/L were diagnosed hyperglycemia.
All statistical analyses were performed using SPSS software (version 17.0). All P-values were two-sided, and the level of significance was set at 0.05. Continuous variables were reported as means and standard deviations or median values, while categorical variables were expressed as numbers and percentages. Analyses of two independent sample t-tests were used to analyze the normally distributed mean differences between the participants' characteristics. The Mann-Whitney test was used to compare the median consumption levels, which did not have a normal distribution. Chi square (χ2) tests were used to compare the among dietary frequency categories between hyperglycemic and normal blood glucose level participants. A logistic regression model was applied to estimate the association between dietary intake of one-carbon metabolism nutrients and hyperglycemia. Odds Ratios (ORs) with 95% confidence intervals (95% CIs) were reported for each quartile of one-carbon metabolism nutrient intake. The first quartile was considered as a reference. The multivariable models were adjusted for age, BMI, sex, marital status, family income, education level, smoking status, alcohol consumption, total energy intake, and dietary fiber intake. Moreover, all six nutrients were placed in a single model, with adjustment of the risk factors listed above. Because one-carbon metabolism–related nutrients are thought to influence disease risk by donating methyl groups for methylation reactions (30, 31), we also calculated a “methyl-donor index” as a composite measure of dietary methyl intake by standardizing the nutrient intake levels on the log-scale ([nutrient value – mean] / standard deviation) then summed across all six nutrients, as described previously (32). The methyl-donor index also was adjusted for total calorie intake using the residual method then categorized into quartile. Trend tests were performed by using the sequential values of the quartiles of dietary one-carbon metabolism nutrients as a continuous variable. Moreover, we evaluated if associations were modified by the presence or absence of fluorosis. The multivariable models were adjusted for age, BMI, and gender. Trend tests were conducted by entering the ordinal values of the quartile of dietary one-carbon metabolism nutrients as continuous variables in the models.
In this cross-sectional study, we collected blood glucose level data from 901 subjects including 417 males (46.28%) and 484 females (53.27%). According to blood glucose levels, they were divided into a hyperglycemic group (n = 184, 20.42%) and a normal group (n = 717, 79.58%). The general information and measurement indicators are shown in Table 1. The average age of the participant was 49 years old, and the average age of the hyperglycemic group (52.99 ± 12.76) was higher than the normal glucose level group (48.59 ± 13.01). There was a significant difference in age, BMI, and waist circumference between the two groups (P < 0.001–P = 0.005), although the differences in gender, education level, ethnicity, per capita annual income, marital status, smoking, alcohol consumption, height, weight and fluorosis between the two groups were not observed (P > 0.05).
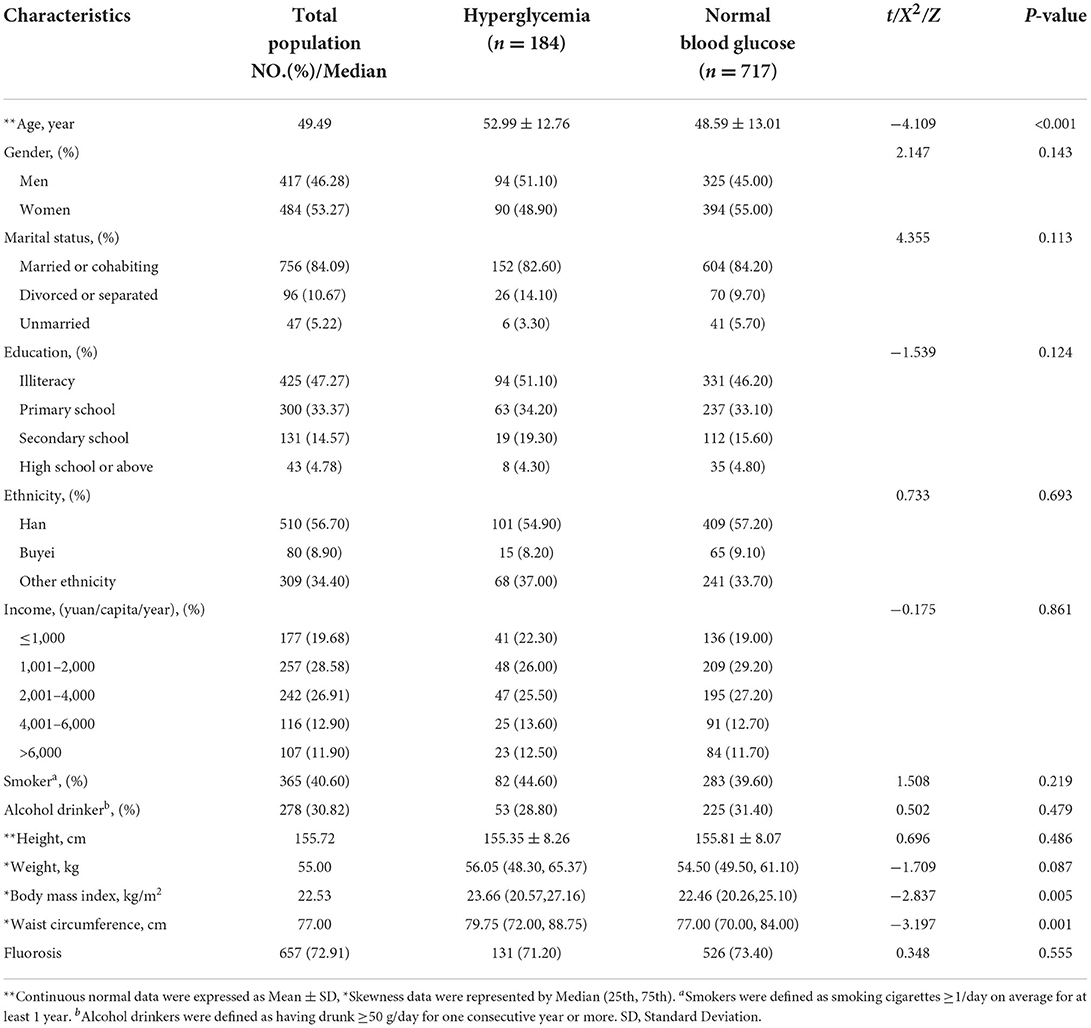
Table 1. The general information of participants.
Intake of folate, vitamin B6, total choline and methyl-donor index in the hyperglycemia group was lower than that in the normal blood glucose level group (P = 0.035, P = 0.011, P = 0.006, P = 0.002, respectively). As for the choline subclass, the intake of free choline, glycerol phosphorylcholine, phosphatidylcholine, and phosphocholine had significant differences between the two groups (all P < 0.05). Dietary choline intake of the hyperglycemic group was lower than the normal glucose level group. However, no differences in energy intake, vitamin B12, methionine, betaine and sphingomyelin intake between the two groups were observed (P = 0.074–0.384). The overall intake of one-carbon metabolism nutrients was generally lower in the hyperglycemic group (Table 2).
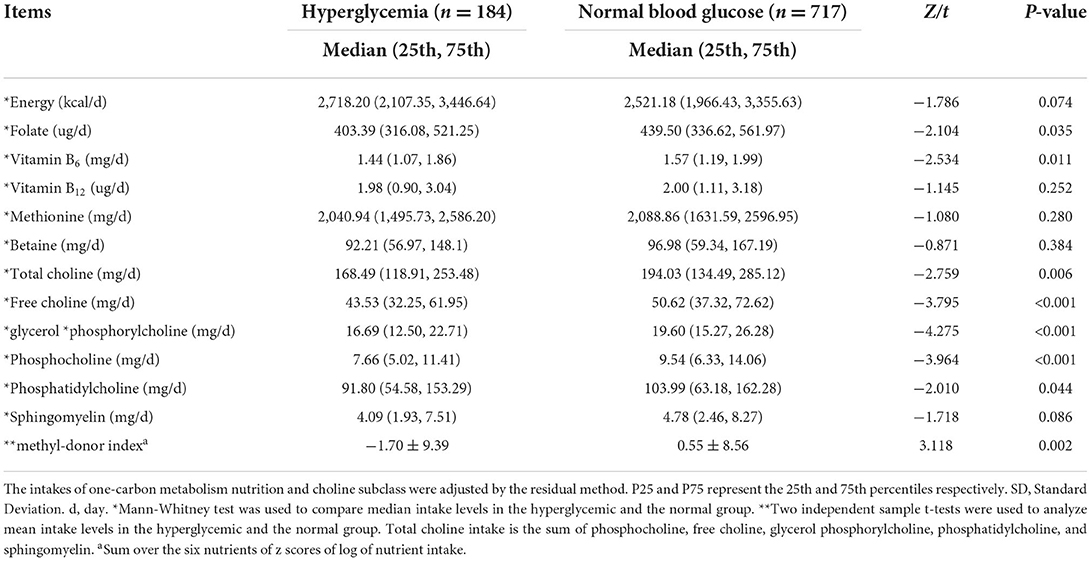
Table 2. Comparison of energy, one-carbon metabolism nutrients intake between hyperglycemia and normal blood.
The ORs (95% CI) for the occurrence of hyperglycemia according to quartiles of one-carbon metabolism nutrient intake and methyl-donor index are presented in Table 3. After adjusting for age, sex, marital status, education level, average yearly household income, ethnicity, smoking status, and alcohol consumption, we found a greater intake of dietary vitamin B6 and total choline were inversely associated with the occurrence of hyperglycemia. The adjusted OR (95% CI) in the highest quartile compared with the lowest was 0.599 (0.365, 0.984) for total choline and 0.579 (0.349, 0.961) for vitamin B6. The inverse associations remained after further adjustments for total energy and dietary fiber. There also was a suggestion that methyl-donor index was inversely associated with the occurrence of hyperglycemia, with adjustment for potential confounding factors (P = 0.011). However, there were no significant associations between the intake of folate, vitamin B12, methionine, betaine and hyperglycemia after adjusting for non-dietary and dietary factors.
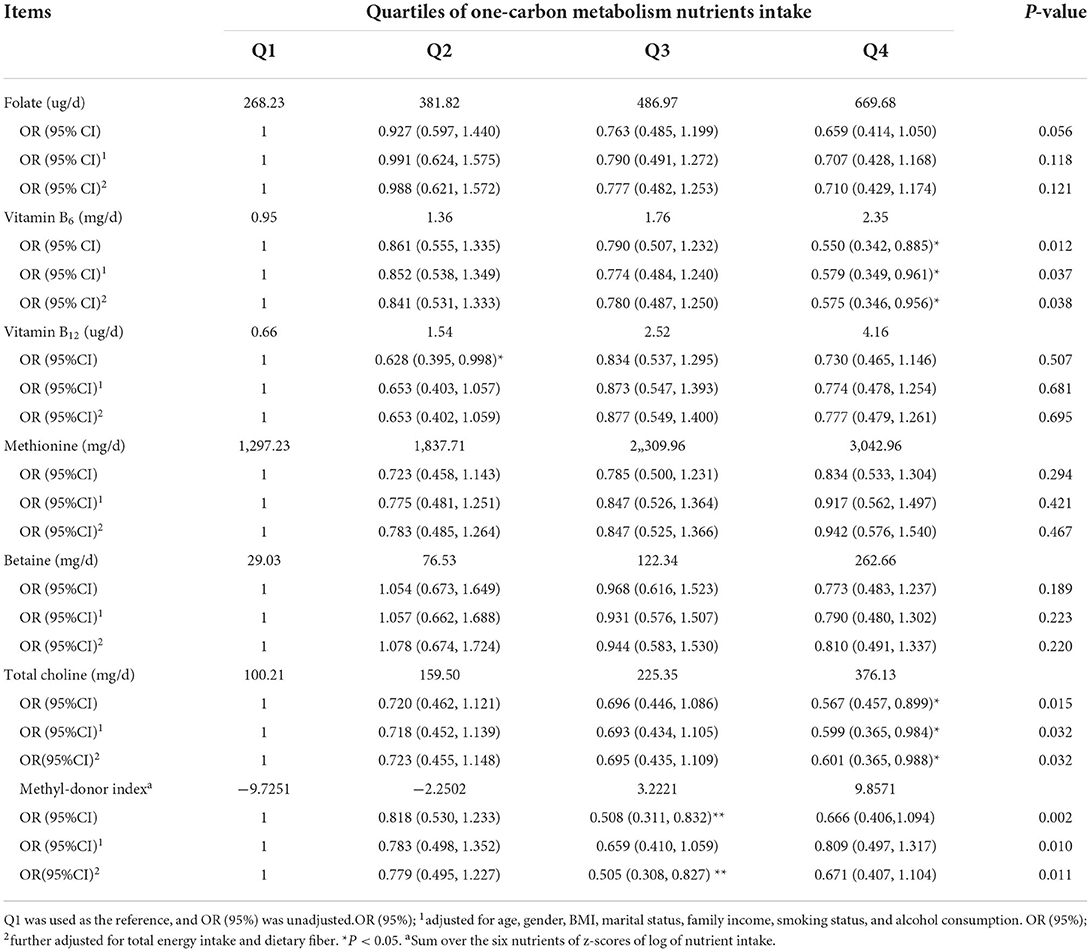
Table 3. Odds Ratios (ORs) and 95% confidence intervals (95%CIs) of hyperglycemia according to quartiles of one-carbon metabolism intake.
The OR (95% CI) for the occurrence of hyperglycemia according to quartiles of five choline intakes subclasses is presented in Table 4. In the unadjusted model, compared with the lowest quartile, the ORs (95% CIs) of hyperglycemia for the highest quartile intakes of free choline, glycerol phosphatidylcholine, and phosphocholine were 0.414 (0.259, 0.661), 0.490 (0.306, 0.783), and 0.420 (0.260, 0.678), respectively. The observed inverse associations remained after further adjustment for potential confounding factors. In contrast, no statistical association between dietary intake of phosphatidylcholine and sphingomyelin and hyperglycemia was observed (P > 0.05).
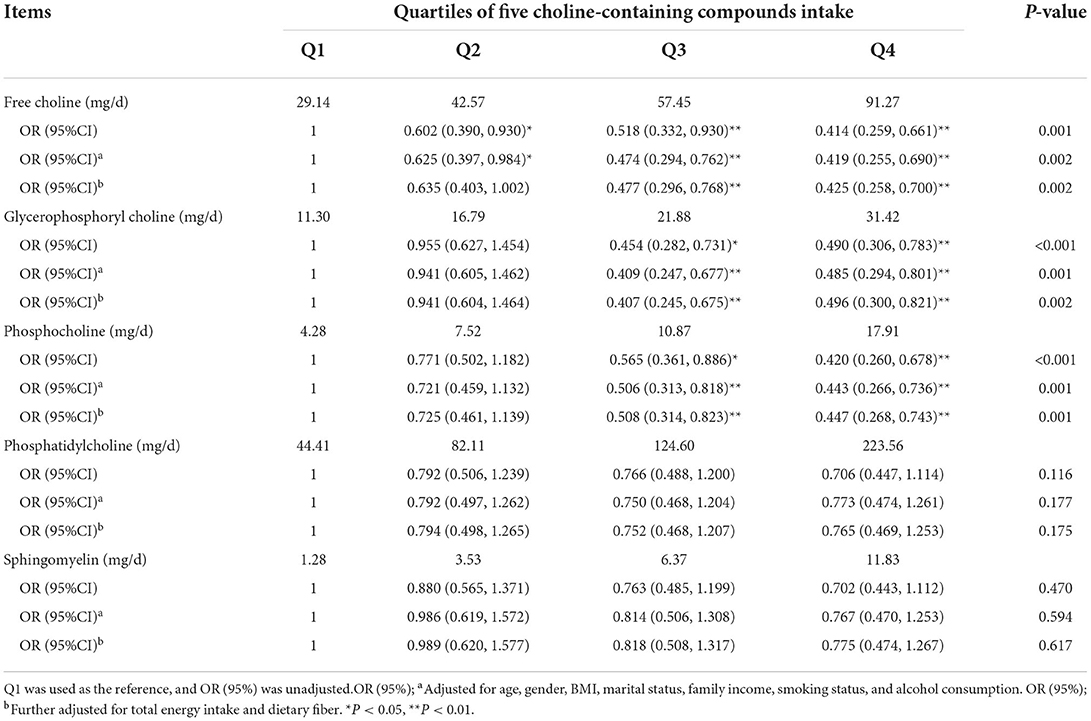
Table 4. Odds Ratios (ORs) and 95% confidence intervals (95%CIs) of hyperglycemic according to quartiles of five choline-containing compounds intake.
We further assessed the associations between one-carbon metabolism nutrients and hyperglycemia across subgroups stratified by the presence or absence of fluorosis, shown in Tables 5, 6. We observed that the nutrients folate, vitamin B6, total choline, free choline, glycerol phosphorylcholine, and phosphocholine had a protective effect against the occurrence of hyperglycemia in the non-fluorosis subgroup. There were inverse associations of the above nutrients with hyperglycemia in the non-fluorosis subgroup (P < 0.05), but not in the fluorosis subgroup (P > 0.05). There were significant interactive effects for the above nutrient intakes with fluorosis (P-interaction = 0.010 P=0.048). There was no significant interactive effect for the other nutrients betaine, methionine, vitamin B12, phosphatidylcholine, sphingomyelin, and methyl-donor index with fluorosis (P-interaction = 0.077 to 0.527).

Table 5. Odds Ratios (OR) and 95% confidence intervals (95%CIs) of hyperglycemia according to quartiles of one-carbon metabolism nutrients by fluorosis.
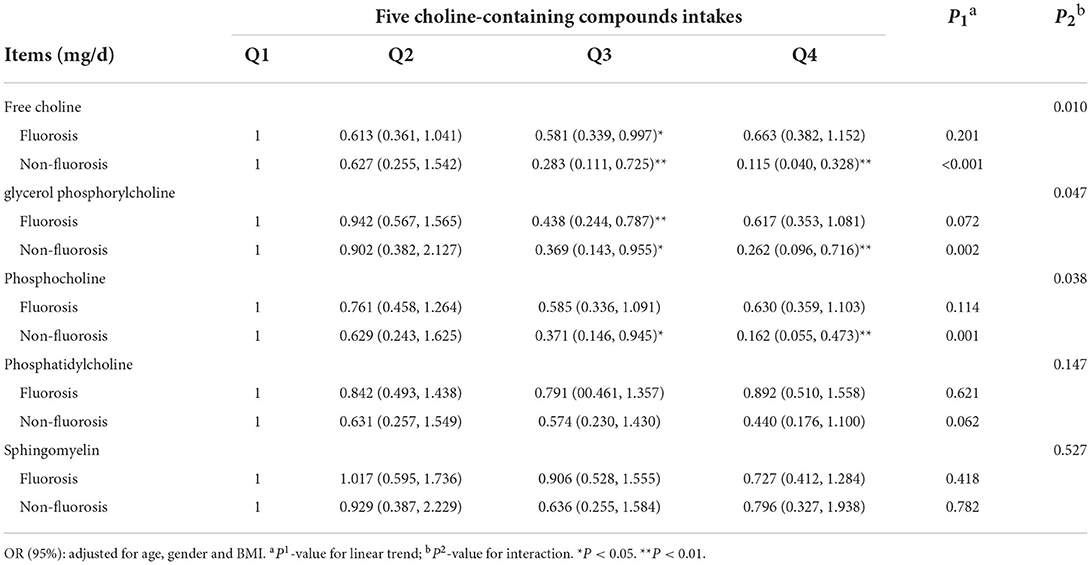
Table 6. Odds Ratios (OR) and 95% confidence intervals (95%CIs) of hyperglycemia according to quartiles of five choline-containing compounds by fluorosis.
In the present study, we found the intake of vitamin B6, total choline, methyl-donor index, free choline, glycerol phosphorylcholine, and phosphocholine were inversely associated with the occurrence of hyperglycemia in Guizhou province, China. Additionally, we also observed that there were interactions between one carbon metabolic nutrients and fluorosis, such as vitamin B6, total choline, free choline, glycerol phosphorylcholine, and phosphocholine.
Hyperglycemia is an important risk factor for diabetes and CVDs. Limited studies evaluated the association of choline and betaine with hyperglycemia and suggested that the results may be inconsistent due to participants from different countries had different dietary habits (17–20). Previous studies reported there was a positive effect of fluoride on the incidence and prevalence of diabetes (21, 22). It is well known that the interaction between nutrition and environment plays an important role in disease. However, whether there is a different relationship between one-carbon metabolism nutrients and hyperglycemia in coal-burning fluorosis areas and how does fluorosis modify the association needs to be evaluated. Therefore, we conducted this study in fluorosis area. To our knowledge we first found protective associations of total choline, free choline, glycerol phosphorylcholine, and phosphocholine with the occurrence of hyperglycemia in Chinese population. Furthermore, these associations were modified by fluorosis. Studies on the association between dietary intake of choline and betaine and hyperglycemia are limited. Some studies explored the relationship of dietary or blood serum choline and betaine with glucose and type 2 diabetes. A cross-sectional study involving 2,394 subjects reported dietary choline intake was negatively associated with fasting blood glucose levels in Newfoundland (18). A cohort study involving 2,332 men (33) found the highest choline and phosphatidylcholine intake was associated with a 25 and a 41% reduction, respectively, in the risk of type 2 diabetes, compared with the lowest quartile in Finland. Moreover, a randomized clinical trial, reported that compared with placebo, betaine tended to reduce fasting glucose levels but had no effect on glycemia and insulin sensitivity (34). It was indicated that betaine may prevent hyperglycemia, even be a potential therapy for the progression of diabetes-induced hyperglycemia. However, choline can be transformed into betaine and phosphatidylcholine through various chemical reactions in the body, which jointly participate in one-carbon metabolism and affect blood glucose levels. More studies are needed to confirm the association between choline, betaine and blood glucose levels.
Vitamin B6 and B12 are important co-factors in the one-carbon metabolic pathway. Jin et al. (35) reported that vitamin B6 and B12 intake was inversely associated with the risk of diabetes in the National Health and Nutrition Examination Survey (NHANES) of 2007–2016. Compared with the lowest quartile, the ORs (95% CIs) of diabetes for the highest quartile intake of vitamin B6 was 0.61 (0.42–0.89), the OR (95% CI) of diabetes for the third quartile of dietary vitamin B12 was 0.76 (0.60–0.97). A linear inverse relationship was found between vitamin B12 and diabetes, and a nonlinear inverse relationship was found between dietary vitamin B6 and diabetes. Several small studies explored the association between vitamin B6 and diabetes complications and observed B6 may play a protective role against various diabetes complications (36, 37). Consistent with these results, we also found that dietary intake of vitamin B6 was a protective factor against the occurrence of hyperglycemia. Unlike vitamin B6, very few studies have investigated the independent role of vitamin B12 in glucose metabolism. China Stroke Primary Prevention Trial longitudinal analyses showed no association between baseline levels of vitamin B12 and a new-onset of diabetes or changes in fasting blood glucose levels (38). Zhu et al. (13) observed no association between the intake of vitamin B12 and diabetes incidence. Our results on the effect of vitamin B12 on hyperglycemia are consistent with these observations. However, a follow-up south Indian study involving 1,500 individuals (12) reported that the levels of vitamin B12 decreased with increasing severity of glucose tolerance. Similar results have been reported in another study (39). The inconsistent results could be attributed to the patients countries. Additionally, baseline serums reflect short-term intake levels, whereas FFQ-based surveys on behavior long-term intake levels. More studies combining dietary intake and blood serum levels are needed to investigate the association between vitamin B6/B12 and blood glucose.
A number of studies have examined the role of folate on glucose and type 2 diabetes, though the results have been inconsistent. In a meta-analysis of 29 randomized controlled trials (RCTs), Lind et al. (14) found that folate supplementation have no overall effect on fasting glucose levels. Recently, Akbari et al. (40) conducted a meta-analysis on RCTs and also observed no significant changes in fasting blood glucose and HbA1c levels among participants with metabolic diseases after folate supplementation, although folate supplementation resulted in decreased plasma insulin levels and insulin resistance. The present study was consistent with the result of RCTs. However, there are two studies that found an inverse association between dietary folate and diabetes risk in Korean (41) and Japanese (42) adults. The Korean study observed that higher dietary folate intake was associated with a lower risk of developing type 2 diabetes for women but not men (41). However, the present study showed no significant association between folate intake and hyperglycemia and no gender difference (Supplementary Tables 1, 2). The reasons for the different results may relate to the adjustment of confounding factors and the use of folate supplements. Additionally, we found that methionine intake was not associated with the occurrence of hyperglycemia. There are few studies methionine and blood glucose. More epidemiological studies are needed to clarify the association between methionine and hyperglycemia.
The effect of one-carbon metabolism nutrients on hyperglycemia may be partly related to DNA methylation in epigenetics. DNA methylation during glucose metabolism was implicated in the pathogenesis of type 2 diabetes (43–45). Deficiency or excess of nutrients can affect one-carbon metabolism, which changes the availability of S-adenosyl methionine (SAM) in the methionine cycle and interferes with DNA and histone methylation patterns (46). holine supplementation (1 mM) increased global DNA methylation and DNA methyltransferase expression in both low-glucose (5 mM) and high-glucose (35 mM) conditions. Choline supplementation increased the expression of peroxisomal acyl-coenzyme A oxidase 1 (ACOX1), which mediates fatty acid β-oxidation, especially in high-glucose conditions. High-glucose exposure increased the transcription of the gluconeogenic gene phosphoenolpyruvate carboxykinase (PEPCK), while choline supplementation mitigated increase. Compared to HepG2 cells, the placenta-derived BeWo cells were relatively unresponsive to either high-glucose or high-choline treatment (47). In a word, choline and glucose interacted to affect macronutrient metabolic genes, yet there was no indication that choline may worsen glycemic control in these in vitro human cell culture models. Another mechanism may be related to oxidative stress. Oxidative stress leads to impaired glucose uptake in muscle and fat cells and decreases insulin secretion from beta cells (48, 49). Mitochondrial respiration is the major cellular source of reactive oxygen species (ROS), and this production is balanced by through antioxidant systems superoxide dismutase (SOD). In hyperglycemic states, such as prediabetes and diabetes, ROS can accumulate and lead to non-specific oxidative damage to DNA (50). One-carbon metabolism nutrients can directly scavenge reactive oxygen species and can act as an antioxidant in vivo (51). In a word, insufficient intake of dietary one-carbon metabolism nutrients may affect the methylation and of ROS, which may prevent the occurrence of hyperglycemia.
We evaluated the associations whether or not be modified by fluorosis due to this cross-sectional study was conducted in fluorosis area. In the present study, we first observed the interactions between vitamin B6, total choline, etc and fluorosis. The result showed that the nutrients folate, vitamin B6, total choline, free choline, glycerol phosphorylcholine, and phosphocholine had a protective effect on the occurrence of hyperglycemia in the non-fluorosis subgroup, but not in the fluorosis subgroup. Two studies found that fluoride was significantly and positively associated with increases in both the incidence and prevalence of diabetes (21, 22). Previous animal studies have shown that exposure to high levels of fluoride would decrease insulin mRNA and its secretion from beta-cells, and affect the OGTT (52). Thus, the protective effect hyperglycemia disappeared due to the toxicity of fluorosis. Fluorosis decreased superoxide dismutase (SOD) activity, accompanied by an increase in the generation of superoxide anion and decreased mitochondrial membrane potential in fluoride exposed cells (52). However, one-carbon metabolism nutrients may influence fluorosis by means of their antioxidant properties, as they are well documented antioxidant compounds that reduce the risk of diseases (53, 54). Furthermore, DNA methylation plays an important role in fluorosis (55), one-carbon metabolism nutrients as methyl donors may prevent the change of DNA methylation induced by fluoride. Further studies are warranted to elucidate the competing pathophysiological mechanisms.
The present study has several limitations. First, it did not clearly identify the causal relationship between one-carbon metabolism-related nutrients and hyperglycemia. This was in part because of a cross-sectional study design, even though we minimized the potential reverse causation by excluding participants with other diseases. Second, we could not avoid memory recall bias, although we emphasized unbiased investigative techniques and objective data, discrepancies could exist between what answer was given in the questionnaire and real life behaviors. Thirdly, we cannot exclude the influence of fluorosis, but the subgroup analysis showed that the protective effect was observed in non-fluorosis subgroup against the occurrence of hyperglycemia was consistent with our participant group as a whole. Additionally, our findings generalized to brick-tea or drinking water fluorosis affected areas should be with caution due to this study was conducted in coal-burning fluorosis areas. Fourthly, serum levels of the one-carbon metabolism nutrients were not detected because of traumatic, low-cooperative and expensive, but we investigated dietary intake in a non-invasive and low-cost manner using an FFQ. Finally, we only collected sedentary frequency without detailed physical activity level, so only sedentary frequency was adjusted to control for the effect of activity level. Furthermore, although we adjusted for many factors during statistical analysis, residual confounding factors were still unavoidable.
In conclusion, higher dietary intakes of vitamin B6, total choline, free choline, glycerol phosphorylcholine, and phosphocholine in choline subgroups are associated with a lower incidence of hyperglycemia. This protective effect was modified by the presence or absence of fluorosis. This finding provides a nutritional basis for the prevention of hyperglycemia in patients with fluorosis.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author/s.
The studies involving human participants were reviewed and approved by Zunyi Medical University. The patients/participants provided their written informed consent to participate in this study.
LD was responsible for analysis and wrote the first draft of the manuscript. QY responsible for data management and revised manuscript. ZS, LL, and ZM assisted in conducting research and data collection. NT carried out the survey and determination. XZ was responsible for organization and survey. JL designed and conducted the study and revised the manuscript. All authors contributed to the article and approved the submitted version.
This study was supported by the National Natural Science Foundation of China (grant number 82060595), Guizhou Provincial Natural Science Foundation (QKHJC-ZK[2022]YB598 and QKHJCZK[2022]YB663), and Guizhou Provincial Health Commission Foundation (gzwkj2021-411).
The authors want to thank the study subjects for their participation and the students who are taking part in the recruitment of subjects and the interviews in the investigation. We also thank the CDC of Zhijin Country for providing administrative support to our study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnut.2022.1002044/full#supplementary-material
1. GDB 2017 Risk Factor Collaborators. Global, regional, and national comparative risk assessment of 84 behavioral, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. (2018) 392:1923-94. doi: 10.1016/s0140-6736(18)32225-6
2. Saeedi P, Petersohn I, Salpea P, Malanda B, Karuranga S, Unwin N, et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res Clin Pract. (2019) 157:107843. doi: 10.1016/j.diabres.2019.107843
3. Campos C. Chronic hyperglycemia and glucose toxicity: pathology and clinical sequelae. Postgrad Med. (2012) 124:90–7. doi: 10.3810/pgm.2012.11.2615
4. Jia G, Whaley-Connell A, Sowers JR. Diabetic cardiomyopathy: a hyperglycemia- and insulin-resistance-induced heart disease. Diabetologia. (2018) 61:21–8. doi: 10.1007/s00125-017-4390-4
5. Gillies NA, Franzke B, Wessner B, Schober-Halper B, Hofmann M, Oesen S, et al. Nutritional supplementation alters associations between one-carbon metabolites and cardiometabolic risk profiles in older adults: a secondary analysis of the Vienna active ageing study. Eur J Nutr. (2022) 61:169–82. doi: 10.1007/s00394-021-02607-y
6. Newman AC, Maddocks OD. One-carbon metabolism in cancer. Br J Cancer. (2017) 116:1499–504. doi: 10.1038/bjc.2017.118
7. Ducker GS, Rabinowitz JD. One-carbon metabolism in health and disease. Cell Metab. (2017) 25:27–42. doi: 10.1016/j.cmet.2016.08.009
8. Mentch SJ, Locasale JW. One-carbon metabolism and epigenetics: understanding the specificity. Ann N Y Acad Sci. (2016) 1363:91–8. doi: 10.1111/nyas.12956
9. Luciano-Mateo F, Hernández-Aguilera A, Cabre N, Camps J, Fernández-Arroyo S, Lopez-Miranda J, et al. Nutrients in energy and one-carbon metabolism: learning from metformin users. Nutrients. (2017) 9:121. doi: 10.3390/nu9020121
10. Spratlen MJ, Grau-Perez M, Umans JG, Yracheta J, Best LG, Francesconi K, et al. Arsenic, one carbon metabolism and diabetes-related outcomes in the strong heart family study. Environ Int. (2018) 121(Pt 1):728-40. doi: 10.1016/j.envint.2018.09.048
11. Peng Y, Dong B, Wang Z. Serum folate concentrations and all-cause, cardiovascular disease and cancer mortality: a cohort study based on 1999-2010 National Health and Nutrition Examination Survey (NHANES). Int J Cardiol. (2016) 219:136–42. doi: 10.1016/j.ijcard.2016.06.024
12. Jayashri R, Venkatesan U, Rohan M, Gokulakrishnan K, Shanthi Rani CS, Deepa M, et al. Prevalence of vitamin B deficiency in South Indians with different grades of glucose tolerance. Acta Diabetol. (2018) 55:1283–93. doi: 10.1007/s00592-018-1240-x
13. Zhu J, Chen C, Lu L, Yang K, Reis J, He K. Intakes of folate, vitamin B, and vitamin B in relation to diabetes incidence among American young adults: a 30-year follow-up study. Diabet Care. (2020) 43:2426–34. doi: 10.2337/dc20-0828
14. Lind MV, Lauritzen L, Kristensen M, Ross AB, Eriksen JN. Effect of folate supplementation on insulin sensitivity and type 2 diabetes: a meta-analysis of randomized controlled trials. Am J Clin Nutr. (2019) 109:29–42. doi: 10.1093/ajcn/nqy234
15. Asbaghi O, Ashtary-Larky D, Bagheri R, Moosavian SP, Olyaei HP, Nazarian B, et al. Folic acid supplementation improves glycemic control for diabetes prevention and management: a systematic review and dose-response meta-analysis of randomized controlled trials. Nutrients. (2021) 13:2355. doi: 10.3390/nu13072355
16. Yan S, Li M, Ma X, Jiang S, Sun M, Wang C, et al. Association of multiple mineral and vitamin B group intake with blood glucose using quantile regression analysis: NHANES 2007-2014. Adv Food Nutr Res. (2019) 63:3560. doi: 10.29219/fnr.v63.3560
17. Konstantinova SV, Tell GS, Vollset SE, Nygard O, Bleie Ø, Ueland PM. Divergent associations of plasma choline and betaine with components of metabolic syndrome in middle age and elderly men and women. J Nutr. (2008) 138:914–20. doi: 10.1093/jn/138.5.914
18. Gao X, Wang Y, Sun G. High dietary choline and betaine intake is associated with low insulin resistance in the Newfoundland population. Nutrition. (2017) 33:28–34. doi: 10.1016/j.nut.2016.08.005
19. Gao X, Randell E, Tian Y, Zhou H, Sun G. Low serum choline and high serum betaine levels are associated with favorable components of metabolic syndrome in Newfoundland population. J Diabetes Complicat. (2019) 33:107398. doi: 10.1016/j.jdiacomp.2019.06.003
20. Dibaba DT, Johnson KC, Kucharska-Newton AM, Meyer K, Zeisel SH, Bidulescu A. The Association of dietary choline and betaine with the risk of type 2 diabetes: the Atherosclerosis Risk in Communities (ARIC) study. Diabetes Care. (2020) 43:2840–6. doi: 10.2337/dc20-0733
21. Fluegge K. Community water fluoridation predicts increase in age-adjusted incidence and prevalence of diabetes in 22 states from 2005 and 2010. J Water Health. (2016) 14:864–77. doi: 10.2166/wh.2016.012
22. Chafe R, R. Aslanov, A Sarkar, P Gregory, A ComeauL, A Newhook. Association of type 1 diabetes and concentrations of drinking water components in Newfoundland and Labrador, Canada. BMJ Open Diabetes Res Care. (2018) 6:e000466. doi: 10.1136/bmjdrc-2017-000466
23. Huang JY, Butler LM, Wang R, Jin A, Koh WP, Yuan JM, et al. Association between dietary intake of one-carbon metabolism-related nutrients and fluorosis in Guizhou, China. Front Nutr. (2021) 8:700726. doi: 10.3389/fnut.2021.700726
24. Liu J, Yang S, Luo MJ, Chen T, Ma XJ, Tao N, et al. Association between dietary patterns and fluorosis in Guizhou, China. Front Nutr. (2019) 6:189. doi: 10.3389/fnut.2019.00189
25. Jun LI, Sheng YA, Luo MJ, Xun ZH, Zhang YM, Ya LU. Association of dietary carotenoids intake with skeletal fluorosis in the coal-burning fluorosis area of Guizhou province. Biomed Environ Sci. (2018) 31:438–47.
26. Alvi S, Khan KM, Sheikh MA. Shahid M. Analysis Chinese food composition tables. (1990) 3:189. doi: 10.1016/0889-1575(90)90025-H
28. Yang JJ, Lipworth LP, Shu XO, Blot WJ, Xiang YB, Steinwandel MD, et al. Associations of choline-related nutrients with cardiometabolic and all-cause mortality: results from three prospective cohort studies of blacks, whites, and Chinese. Am J Clin Nutr. (2020) 111:644–56. doi: 10.1093/ajcn/nqz318
29. American Diabetes Association. Classification and diagnosis of diabetes: standards of medical care in diabetes-2019. Diabetes Care. (2019) 42(Suppl 1):S13-s28. doi: 10.2337/dc19-S002
30. Anderson OS, Sant KE, Dolinoy DC. Nutrition and epigenetics: an interplay of dietary methyl donors, one-carbon metabolism and DNA methylation. J Nutr Biochem. (2012) 23:853–9. doi: 10.1016/j.jnutbio.2012.03.003
31. Mahmoud AM, Ali MM. Methyl Donor Micronutrients that modify DNA methylation and cancer outcome. Nutrients. (2019) 11:608. doi: 10.3390/nu11030608
32. Chamberlain JA, Dugué PA, Bassett JK, Hodge AM, Brinkman MT, Joo JE, et al. Dietary intake of one-carbon metabolism nutrients and DNA methylation in peripheral blood. Am J Clin Nutr. (2018) 108:611–21. doi: 10.1093/ajcn/nqy119
33. Virtanen JK, Tuomainen TP, Voutilainen S. Dietary intake of choline and phosphatidylcholine and risk of type 2 diabetes in men: the Kuopio Ischaemic heart disease risk factor study. Eur J Nutr. (2020) 59:3857–61. doi: 10.1007/s00394-020-02223-2
34. Grizales AM, Patti ME, Lin AP, Beckman JA, Sahni VA, Cloutier E, et al. Metabolic effects of betaine: a randomized clinical trial of betaine supplementation in prediabetes. J Clin Endocrinol Metab. (2018) 103:3038–49. doi: 10.1210/jc.2018-00507
35. Jin G, Wang J, Jiang X. Association of folate, vitamin B-12 and vitamin B-6 intake with diabetes and prediabetes in adults aged 20 years and older Asia Pacific. Clin Nutr. (2021) 30:75–86.
36. Nix WA, Zirwes R, Bangert V, Kaiser RP, Schilling M, Hostalek U, et al. Vitamin B status in patients with type 2 diabetes mellitus with and without incipient nephropathy. Diabetes Res Clin Pract. (2015) 107:157–65. doi: 10.1016/j.diabres.2014.09.058
37. Mascolo E, Vernì F. Vitamin B6 and diabetes: relationship and molecular mechanisms. Int J Mol Sci. (2020) 21:3669. doi: 10.3390/ijms21103669
38. Liu L, Huang X, Wang B, Song Y, Lin T, Zhou Z, et al. Vitamin B and risk of diabetes: new insight from cross-sectional and longitudinal analyses of the China Stroke Primary Prevention Trial (CSPPT). BMJ Open Diabetes Res Care. (2020) 8:e001423. doi: 10.1136/bmjdrc-2020-001423
39. Satapathy S, Bandyopadhyay D, Patro BK, Khan S, Naik S. Folic acid and vitamin B12 supplementation in subjects with type 2 diabetes mellitus: a multi-arm randomized controlled clinical trial. Complement Ther Med. (2020) 53:102526. doi: 10.1016/j.ctim.2020.102526
40. Akbari M, Tabrizi R, Lankarani KB, Heydari ST, Karamali M, Keneshlou F, et al. The Effects of folate supplementation on diabetes biomarkers among patients with metabolic diseases: a systematic review and meta-analysis of randomized controlled trials. Horm Metab Res. (2018) 50:93–105. doi: 10.1055/s-0043-125148
41. Hong SM, Woo HW, Kim MK, Kim SY, Lee YH, Shin DH, et al. A prospective association between dietary folate intake and type 2 diabetes risk among Korean adults aged 40 years or older: the Korean Multi-Rural Communities Cohort (MRCohort) Study. Br J Nutr. (2017) 118:1078–88. doi: 10.1017/S0007114517003087
42. Eshak ES, Iso H, Muraki I, Tamakoshi A. Among the water-soluble vitamins, dietary intakes of vitamins C, B2 and folate are associated with the reduced risk of diabetes in Japanese women but not men. Br J Nutr. (2019) 121:1357–64. doi: 10.1017/S000711451900062X
43. Barres RJ,. Zierath R. DNA methylation in metabolic disorders. Am J Clin Nutr. (2011) 93:897s−900. doi: 10.3945/ajcn.110.001933
44. Ling C, Groop L. Epigenetics: a molecular link between environmental factors and type 2 diabetes. Diabetes. (2009) 58:2718–25. doi: 10.2337/db09-1003
45. Ling C, Rönn T. Epigenetic markers to further understand insulin resistance. Diabetologia. (2016) 59:2295–7. doi: 10.1007/s00125-016-4109-y
46. Ahmed SA, Ansari SA, Mensah-Brown EP, Emerald BS. The role of DNA methylation in the pathogenesis of type 2 diabetes mellitus. Clin Epigenetics. (2020) 12:104. doi: 10.1186/s13148-020-00896-4
47. Jiang X, E. GreenwaldC Jack-Roberts. Effects of choline on DNA methylation and macronutrient metabolic gene expression in in vitro models of hyperglycemia. Nutr Metab Insights. (2016) 9:11–7. doi: 10.4137/NMI.S29465
48. Luc K, Schramm-Luc A, Guzik TJ, Mikolajczyk TP. Oxidative stress and inflammatory markers in prediabetes and diabetes. J Physiol Pharmacol. (2019) 70:809–824. doi: 10.26402/jpp.2019.6.01
49. Maddux BA, See W, Lawrence Jr JC, Goldfine AL, Goldfine ID, Evans JL. Protection against oxidative stress-induced insulin resistance in rat L6 muscle cells by mircomolar concentrations of alpha-lipoic acid. Diabetes. (2001) 50:404–10. doi: 10.2337/diabetes.50.2.404
50. Chong CR, Clarke K, Levelt E. Metabolic remodeling in diabetic cardiomyopathy. Cardiovasc Res. (2017) 113:422–30. doi: 10.1093/cvr/cvx018
51. Assies J. Mocking RJ, Lok A, Ruhé HG, Pouwer F, Schene AH. Effects of oxidative stress on fatty acid- and one-carbon-metabolism in psychiatric and cardiovascular disease comorbidity. Acta Psychiatr Scand. (2014) 130:163–80. doi: 10.1111/acps.12265
52. García-Montalvo EA, Reyes-Pérez H, Del Razo LM. Fluoride exposure impairs glucose tolerance via decreased insulin expression and oxidative stress. Toxicology. (2009) 263:75–83. doi: 10.1016/j.tox.2009.06.008
53. Matxain JM, Padro D, Ristila M, Strid Å, Eriksson LA. Evidence of high *OH radical quenching efficiency by vitamin B6. J Phys Chem B. (2009) 113:9629–32. doi: 10.1021/jp903023c
54. Yang M, Kuang M, Wang G, Ali I, Tang Y, Yang C, et al. Choline attenuates heat stress-induced oxidative injury and apoptosis in bovine mammary epithelial cells by modulating PERK/Nrf-2 signaling pathway. Mol Immunol. (2021) 135:388–97. doi: 10.1016/j.molimm.2021.05.002
Keywords: one-carbon metabolism, hyperglycemia, betaine, choline, methionine, folate, vitamin B6, vitamin B12
Citation: Ding L, Yang Q, Sun Z, Liu L, Meng Z, Zhao X, Tao N and Liu J (2022) Association between dietary intake of one-carbon metabolism nutrients and hyperglycemia in coal-burning fluorosis areas of Guizhou, China. Front. Nutr. 9:1002044. doi: 10.3389/fnut.2022.1002044
Received: 24 July 2022; Accepted: 23 September 2022;
Published: 10 October 2022.
Edited by:
Yong Zhao, Chongqing Medical University, ChinaReviewed by:
Yanmei Yang, Harbin Medical University, ChinaCopyright © 2022 Ding, Yang, Sun, Liu, Meng, Zhao, Tao and Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Na Tao, MTIxNjcwNzAwQHFxLmNvbQ==; Jun Liu, bGl1anVuX3ptY0BzaW5hLmNvbQ==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.