 Leandro Borges
Leandro Borges Matheus Gennari-Felipe
Matheus Gennari-Felipe Beatriz Belmiro Dias
Beatriz Belmiro Dias Elaine Hatanaka
Elaine Hatanaka
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Nutr. , 26 January 2022
Sec. Nutritional Immunology
Volume 8 - 2021 | https://doi.org/10.3389/fnut.2021.821824
This article is part of the Research Topic Nutritional Modulation of Inflammation and Insulin Resistance View all 8 articles
The use of nutraceutical approaches may regulate the immune system, performing a potential strategy to contain the worst outcomes of COVID-19. We reviewed the current evidence surrounding nutritional/nutraceutical approaches for the therapy in patients with COVID-19. We searched the PubMed database to report randomized controlled trials (RCTs) and observational research that used melatonin, zinc, or vitamin C supplementation as an intervention for COVID-19 treatment. To date, we found only three concluded studies that assessed zinc supplementation and melatonin therapy in patients with COVID-19, but with inconclusive data, relatively small sample size, and early termination of the trial. On the other hand, vitamin C therapy appears to reduce hyperinflammation and improve the oxygen support status of patients with COVID-19. However, a large part of this research involves pilot trials, and there are still conflicting data regarding mortality rate, mechanical ventilation, and duration of symptoms of patients with COVID-19. Melatonin, zinc, and vitamin C supplementation should be investigated further on the nutritional status-immune response, and data from ongoing trials are needed to understand these molecules as a therapy strategy in patients COVID-19.
Coronaviruses are a family of viruses that induce intestinal and respiratory disorders in animals and humans. They generally induce mild colds in the population, but the arising of the severe acute respiratory syndrome (SARS) epidemic (2002–2003) as well as the Middle East respiratory syndrome (MERS) (2012) demonstrated that they can also induce serious illness (1). The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has confirmed diagnoses that presently exceeded 274,628,461 people worldwide and nearly 5,358,978 deaths (2). Although pharmaceutical trials are focused on new drugs for COVID-19, due to frequently occurring virus mutations and drug ineffectiveness (3), these studies are time-consuming and inconclusive. Determining a drug treatment is of utmost importance since distinct drugs may be efficient at particular stages of viral infection. For instance, adjunct approaches such as immunomodulators may be functional at an early phase of the infection, while antiviral drugs (e.g., remdesivir) can be more efficient for severe patients with COVID-19. Moreover, toxicity dose selection, as well as no side-effect, are critical components that are related to the efficacy and safety of the drug (4). In this scenario, many trials are assessing the success of safe and cheap nutritional/nutraceutical approaches targeting immune regulatory pathways, viral proteins, or the viral entry pathway, and the “nutritional status–immune response” dyad of a person becomes even more relevant during the COVID-19 pandemic (4, 5).
Some molecules and nutrients play central roles in keeping the function and integrity of the immune system, showing synergistic results in steps that are crucial for the immune response. Among these elements, melatonin, zinc, and vitamin C present robust evidence of their immunomodulating activity, such that their deficit, even if superficial, can harm the metabolism and, hence, their response on the immune system (6, 7). Additional discussion on this topic can be explored through the idea grounded by the Law of the Minimum suggested by Justus von Liebig (8) and the triage hypothesis suggested by Ames (9).
Viral infections elevate the necessity for vitamins, such as A, B, C, and D (10). Notwithstanding the absence of preclinical data of effectiveness against coronaviruses, ascorbic acid (vitamin C), a water-soluble nutrient that has antioxidant potential, is a broadly used supplement nowadays (11). In humans, preclinical trials indicate that vitamin C ameliorates immunoregulation and the outcomes of inflammation by preventing proinflammatory cytokine release, controlling reactive oxygen species, and defending host cells (12, 13). These effects, associated with low toxicity, motivated recent research to add high-dose intravenous vitamin C (HDIVC) to the regular therapy of patients with severe illnesses, such as acute respiratory distress syndrome (ARDS) (14), sepsis (14, 15), and cardiac surgery (16).
Zinc gluconate is a generally accessible over-the-counter supplement that people use for viral illnesses treatment. Zinc regulates the immune response via white blood cell and antibody production (17). Recent studies indicated that angiotensin-converting enzyme (ACE)-2 expression is modulated by Sirtuin 1 (SIRT1) and that zinc reduces SIRT1 response; therefore, the modulation of SIRT1 by zinc could reduce ACE-2 expression and lastly viral entrance into the cell (18, 19). Research in cell culture also found that zinc can restrict the RNA polymerase of SARS-CoV-1 (20), and the proteolytic processing of polyproteins in RNA viruses (21). Moreover, zinc deficiency reduces the production of antibodies and elevates proinflammatory biomarkers (22). Most relevant is the fact that continuous low serum zinc has been inversely correlated with mortality from sepsis and related to recurrent sepsis (23, 24), highlighting the value of the zinc approach in COVID-19 treatment.
Melatonin (N-acetyl-5-methoxytryptamine) is known to promote antioxidative, antiinflammatory, and immunomodulation effects (25, 26), and melatonin exposure postintubation is related to the positive result in patients with COVID-19 (27). Since melatonin is a small molecule with amphiphilic essence and can spontaneously come into all cells and quickly go through biological membranes to achieve subcellular structures and organelles (28), this indoleamine has been hypothesized to be efficient to restrain viral infections by the interaction with the coronavirus membrane and its genetic component. The SARS-CoV-2 virus stimulates the nod-like receptor family, pyrin domain-containing three inflammasome (29), activating nuclear factor kappa-B (NF-κB) and resulting in cytokines expression and release (30), and leukocyte dysfunction (31). Besides, melatonin restores the lungs from oxidative injury induced by age (32), an effect that may be significant to decrease the inflammatory damage and local oxidative in the lungs of patients with COVID-19.
Pondering over the nutritional condition–immune response in patients with COVID-19, nutraceutical approaches that can ameliorate the immune system to protect or decrease the risk of serious progression and prognosis of coronavirus infection become pertinent (Figure 1). This review aims to give a brief insight and summarize the current literature regarding the utility of melatonin, zinc, and vitamin C as possible approaches for patients with COVID-19.
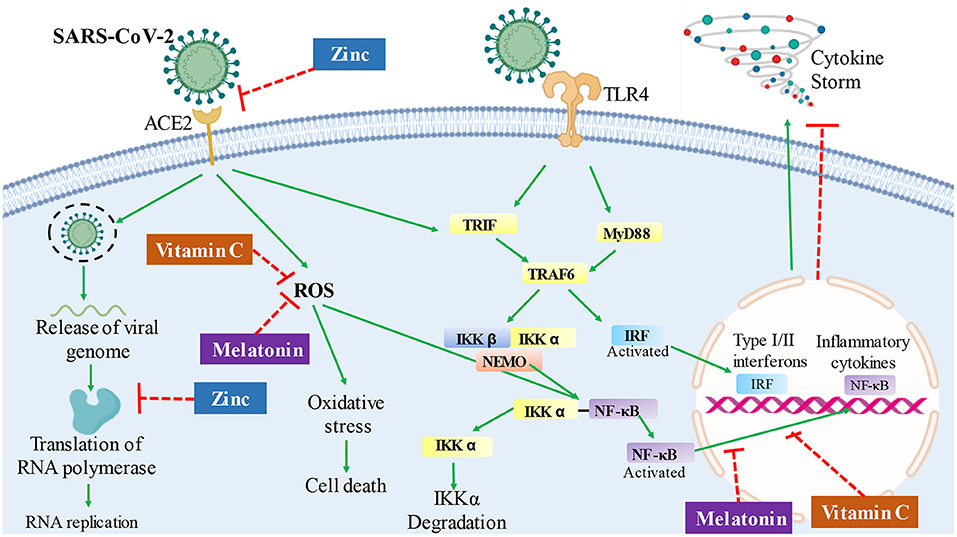
Figure 1. Hypothesis of potential routes and mechanisms, in which melatonin, zinc, or vitamin C therapy could affect the infection response in patients with COVID-19. The overreactive immune system response, followed by severe inflammation and oxidative stress, can contribute to COVID-19 pathology, leading to a cytokine storm. Vitamin C has an antioxidant activity, which could prevent oxidative stress and regulate cytokine production by deactivating the NF-kB signaling cascade in patients with COVID-19. Melatonin also has antioxidant activity and decreases NF-kB activation, which could contribute to the inhibition of cytokine storm. Besides, zinc could act by decreasing viral replication by inhibiting RNA polymerase and reverse transcriptase activity; in addition, it could decrease the expression of the ACE2 receptor and inhibits the interaction of SARS-CoV-2 with this receptor. SARS-CoV-2, severe acute respiratory syndrome coronavirus 2; ACE2, angiotensin-converting enzyme 2; ROS, reactive oxygen species; TLR4, toll-like receptor 4; TRIF, TLR-like receptor-associated interferon factor; MyD88, myeloid differentiation factor 88; TRAF6, tumor receptor-associated factor 6; IKK, ikappaB kinase; NEMO, ikappaB kinase gamma; IRF, interferon regulatory factor; NF-κB, nuclear factor kappa B.
The main question of the present review is: What are the completed randomized controlled trials (RCTs) and observational research, published in the literature, that studied melatonin, zinc, or vitamin C supplementation in the treatment of patients with COVID-19?
Due to the lack of concluded RCTs that assessed nutritional/nutraceutical treatments with melatonin, zinc, or vitamin C during the COVID-19 pandemic, this research is a narrative review with qualitative data in design but followed general guidelines used to establish sources from the literature. Thus, studies reporting RCTs or observational research were searched by PubMed database and the search plan explored Medical Subject Headings (MeSH) terms and free text search. The search terms and synonyms were divided into three main categories and lastly blended into one search sequence. Supplementary Table 1 shows the logical structure of the current search strategy with all the Boolean operators and descriptors used in the PubMed database. The reference lists of pertinent papers were also inspected to recognize additional suitable trials on the search criteria.
Inclusion criteria were peer-reviewed RCTs and observational studies that evaluated patients with COVID-19 who underwent any treatment involving melatonin, zinc, or vitamin C; written in any language. Letters, editorials, and studies with a survey, questionnaire, case reports, or protocol without results were excluded. RCTs that used only a combination of supplements (e.g., ivermectin plus zinc) without the use of a specific treatment group involving melatonin, zinc, or vitamin C were also excluded. Moreover, research that studied patients with another type of coronavirus (e.g., MERS) as well as parenteral nutrition or trials that used melatonin, zinc, or vitamin C as a comparator control group, instead of using a placebo, were also excluded to avoid data confounding. The literature search was conducted from inception to October 04 (2021), with results being exported on the same day. Two independent reviewers read the titles and abstracts of the studies, and mutual conclusions were summarized. In cases of discrepancy, a third reviewer decided on the inclusion of the study. The restricted review was developed using RayyanQatar Computing Research Institute QCRI (http://rayyan.qcri.org) to select the included studies.
Among 108 coronavirus-associated melatonin articles extracted and assessed for eligibility, three studies with a melatonin approach were included (33–35). Moreover, among the 399 coronavirus-associated zinc studies extracted and evaluated for eligibility, three studies entered the inclusion criteria (36–38), whereas among 344 coronavirus-associated vitamin C (or ascorbic acid) papers initially extracted and analyzed for eligibility, a total of 10 papers were also included as RCTs or observational research (37, 39–47).
Current observational research and RCTs on COVID-19 and nutraceutical approaches regarding melatonin, zinc, and vitamin C are summarized in Table 1 (melatonin), Table 2 (zinc), and Table 3 (vitamin C). Among the studies included, all reports included a control group that received placebo or standard therapy. Twelve studies were developed with patients with COVID-19 admitted to the hospital, two studies with ICU patients, and one study with ambulatory patients (Tables 1–3).
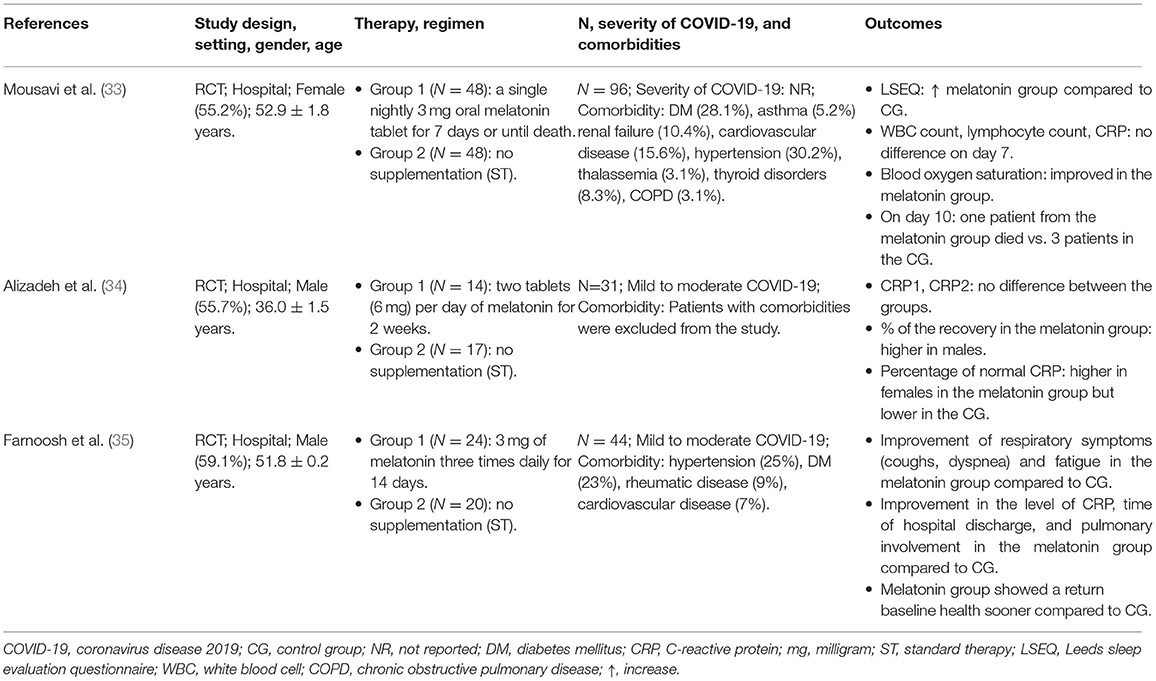
Table 1. Summary of findings from studies that included melatonin supplementation in the COVID-19 treatment.
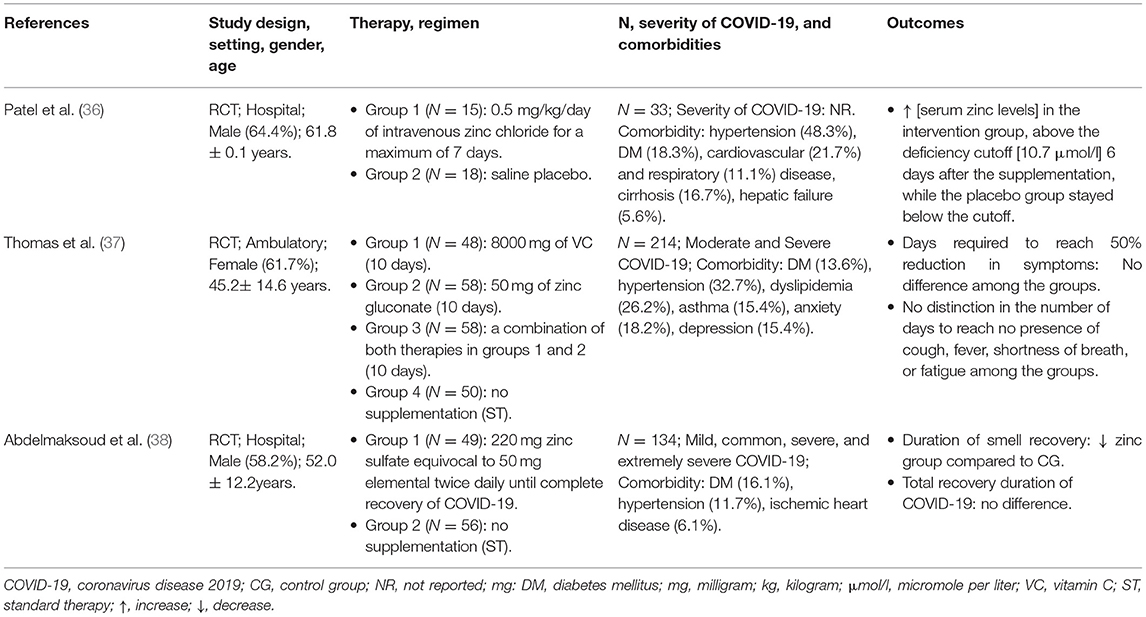
Table 2. Summary of findings from studies that included zinc supplementation in the COVID-19 treatment.
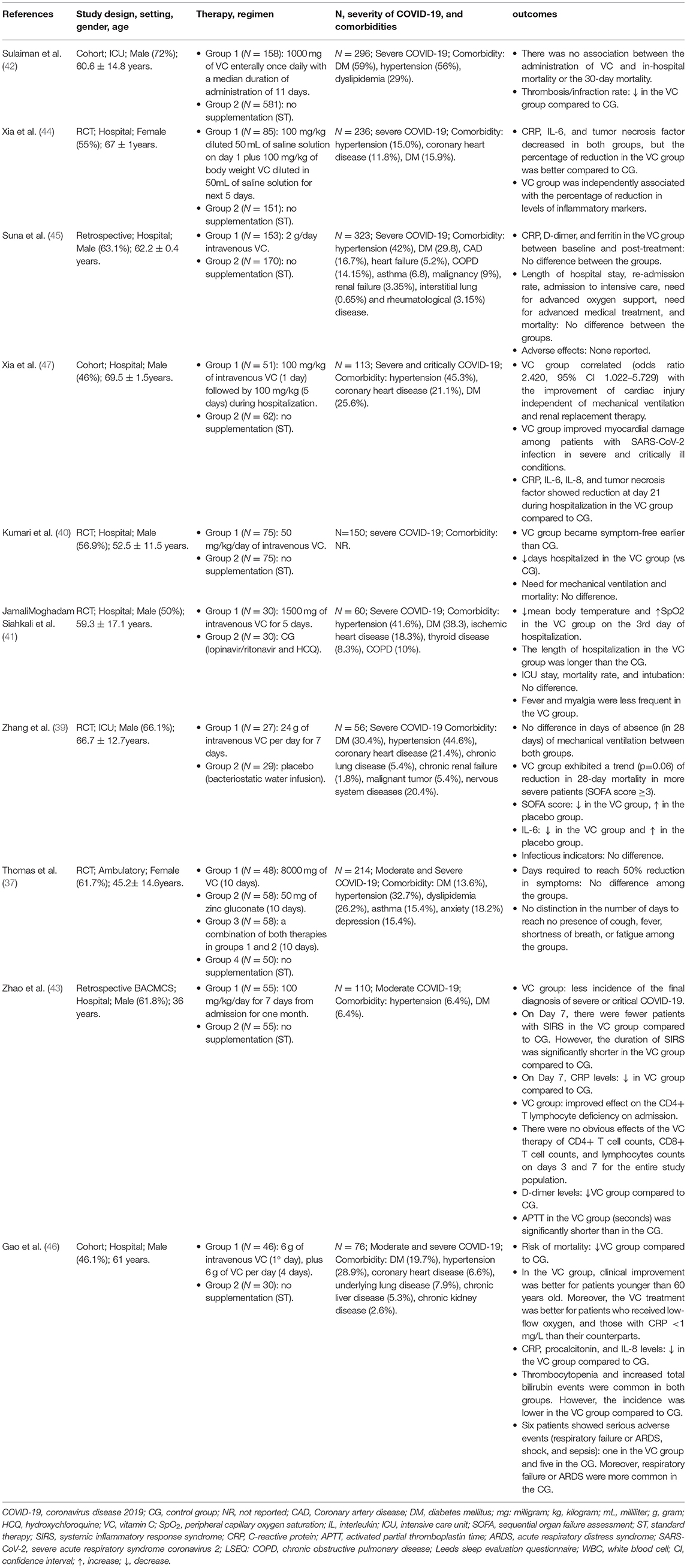
Table 3. Summary of findings from studies that included vitamin C supplementation in the COVID-19 treatment.
Besides the indirect antiviral responses due to melatonin immunomodulatory, antioxidant, antiinflammatory, and immune-enhancing characteristics (48), recent multidrug repurposing research on 26,779 participants affected by COVID-19 showed that increased melatonin levels were related to a 28% (general population) and 52% (African Americans) decreased likelihood of a SARS-CoV-2 infection (49).
Randomized controlled trials are the gold standard for clinical studies, and they are crucial for establishing whether there is a real clinical advantage in using therapy to manage COVID-19. Clinical trials that preceded the COVID-19 pandemic found adequate safety outcomes when this endogenous indolamine was orally supplemented at different concentrations (3, 6, and 10 mg) in patients from intensive care units (ICU) (50, 51). Currently, eight clinical studies with melatonin treatment (or melatonin agonist therapy) in patients with COVID-19 are reported at clinicaltrials.gov. In highlight, three of them have already initiated enrolling subjects, and two trials have the recruitment status of “complete” (NCT04570254, NCT04568863) (Supplementary Table 2).
In the context of the COVID-19 pandemic, Farnoosh et al. developed a small (N = 44) RCT to study a group of patients with COVID-19 treated additionally with melatonin (3 mg for 2 weeks) and found a more rapid hospital discharge and return to baseline health in the melatonin group, as well as relevant improvement in the pulmonary involvement and clinical symptoms such as cough, dyspnea, and fatigue, and also the level of CRP (35). Corroborating the findings, a pilot randomized study (N = 31) in patients with COVID-19 also showed that melatonin intervention (6 mg for 2 weeks) increased the percentage of recovery (based on symptoms) when compared with patients in the control group (34). Moreover, Mousavi et al. assessed the effectiveness of adding melatonin treatment (3 mg plus standard care for 7 days or until death) on sleep quality and outcomes of patients with COVID-19 (N = 96). They found that the mean of the Leeds Sleep Evaluation Questionnaire scores was higher in the melatonin group; however, there was no difference in laboratory data (lymphocyte count, white blood cell count, CRP levels), except for blood oxygen saturation, which has improved in the melatonin group (33).
Before the current pandemic, clinical outcomes have emphasized a relevant function for vitamin C among individuals in ICU with pneumonia, sepsis, ARDS, and multiorgan failure (52). For instance, a meta-analysis of 12 RCTs showed that ascorbic acid low ICU permanence on average by 8% in sepsis condition or cardiac surgery patients involving different clinical conditions (e.g., atrial fibrillation and coronary artery bypass grafting patients) (53). The results of vitamin C on distinct groups of respiratory viruses appear to be non-specific (54); therefore, it seems reasonable that this nutritional therapy may also have outcomes on the new coronavirus.
Vitamin C treatment appears to have a partial clinical improvement effect in patients with COVID-19. For instance, the pilot trial developed by Zhang et al. found that HDIVC [24 g; N = 27] failed to ameliorate the invasive mechanical ventilation-free days in 28 days when compared to the control group [N = 29]. On the other hand, the authors showed that HDIVC reduced IL-6 levels, and the treatment might also show a possible signal of benefit in oxygenation by the improvement of partial pressure of oxygen (PaO2/FiO2) for severely ill patients with COVID-19 (39). Similarly, Kumari et al. showed that the treatment with intravenous vitamin C in patients with COVID-19 also failed to reduce mortality and the necessity for mechanical ventilation between the therapy [50 mg/kg/day; N = 75] and the control group [N = 75]; however, they found that vitamin C therapy allowed patients with COVID-19 a shorter hospital stay, and these patients became symptom-free earlier compared to patients using standard treatment only (40).
Thomas et al. did not find a decrease in the duration of symptoms in patients with SARS-CoV-2 infection supplemented with vitamin C [8,000 mg for 10 days; N = 48] (37). On the other hand, Jamali Moghadam Siahkali et al. showed amelioration in body temperature and peripheral oxygen saturation in serious patients with COVID-19 with HDIVC therapy [6g/day; N = 30]. However, the authors did not find better outcomes in the vitamin C group in addition to the main treatment regimen at discharge (41).
Although a few observational research and preliminary clinical studies on vitamin C in patients with COVID-19 corroborate their findings by noting a reduction in hyper inflammation (43, 44, 47), improvement in the oxygen support status (39, 41, 46, 47), lower incidence of thrombosis (42), and also the reduced disease aggravation in the early stage of COVID-19 pneumonia (43), the mortality rate is still controversial among the studies. Some authors found a reduction in mortality (46) whereas other studies with vitamin C did not observe a difference in mortality when compared to patients in the control group (40, 42, 45). Controversial research with vitamin C also demonstrated failure to ameliorate the mechanical ventilation of patients with COVID-19 (39, 40) and did not find a substantial decrease in the duration of symptoms (37). Therefore, further studies are required to confirm these findings since limited evidence based on small samples precludes definitive conclusions.
Currently, more than 60 ongoing trials are studying SARS-CoV-2 and oral and/or intravenous ascorbic acid treatment, twenty-four of which have started the recruitment of participants, and 15 of which have already been finished (Supplementary Table 2).
Zinc treatment investigation is rational in COVID-19 since reduced zinc concentrations seem frequent in patients with COVID-19 (55, 56) and due to the protective response of zinc on viral replication. In this sense, zinc seems to restrain coronavirus RNA polymerase response in vitro (20), which could grant this metal a function in avoiding virus entrance into cells and decreasing the virulence of SARS-CoV (57). Moreover, zinc toxicity hardly happens in sporadic cases in contrast to numerous other metal ions with close chemical features (58).
Interestingly, patients with COVID-19 with decreased zinc concentrations demonstrated higher mortality on hospital admission (55). Thus, it has been hypothesized that the temporary zinc deficit that takes place in COVID-19 infection could produce a hyperinflammatory state. On the other hand, the antiinflammatory response of zinc has been evidenced by the restriction of IkappaB kinase response, modulation of T-cell function, and NF-κB signaling with a simultaneous decrease in the concentrations of proinflammatory biomarkers (59). Moreover, zinc therapy is suggested to decrease inflammatory cytokines (IL-1 and IL-6), an event that could improve the protective type-I IFN response in COVID-19 (7).
Patel et al. performed a pilot trial (N = 33) in hospitalized COVID-19 patients and found high serum zinc levels in the intervention group supplemented with zinc [0.5 mg/kg/day] (above the deficiency cutoff of 10.7 μmol/l) 6 days after the treatment, while the placebo group stayed below the cutoff (36). However, Abdelmaksoud et al. showed that the zinc status of patients with COVID-19 did not exhibit a relevant role in the disease severity or in the development of hyposmia and/or anosmia. The same authors also found that the median duration of recovery of olfactory and/or gustatory role was shorter among patients with COVID-19 who had zinc therapy (N = 49; 220 mg zinc sulfate equivocal to 50 mg elemental zinc two times daily, until complete recovery of COVID-19) than those who did not receive zinc (N = 56) (38).
Thomas et al. studied patients treated with high-dose zinc gluconate [50 mg; N = 58] for 10 days in ambulatory patients with SARS-CoV-2 infection with the primary endpoint being the number of days needed to reach a 50% decrease in symptoms, such as the severity of fatigue, cough, fever, and shortness of breath. They found no decreases in the duration of symptoms in patients supplemented with high-dose zinc when compared with the standard of care (N = 50). In fact, the authors had to interrupt the trial due to the low conditional power for benefit among the participants (37).
To date, contrasting and scarce clinical outcomes on zinc treatment efficacy on COVID-19 are accessible, especially in the outpatient setting. It is also pertinent to note that numerous clinical protocols planned to utilize zinc in association with azithromycin or hydroxychloroquine (e.g., NCT04370782, NCT04377646), and it is unknown how the absence of proof encouraging the utilization of hydroxychloroquine will reflect in research with zinc treatment.
Presently, more than 50 trials (more than 15 identified with “in recruitment” status and “completed” status) are reported with the purpose to use zinc supplementation in a therapeutic or preventative way, and the outcomes of these trials will be significant to authenticate the efficiency of zinc as a secondary approach in SARS-CoV-2 (Supplementary Table 2).
Besides the fact that nutritional supplementation is usually cost-effective, research with melatonin, zinc, and vitamin C are reported with antiinflammatory and antioxidative attributes, and the deficiency of these nutraceutical supports represents a higher risk for severe progression of COVID-19. Our data showed that, to date, most RCTs with the use of melatonin, zinc, or vitamin C in patients with COVID-19 are still in the development stage and, even though some trials already have the status of “completed,” as demonstrated in Supplementary Table 2, there is still no forecast for the publication of these studies.
Considering only the data with a statistical difference, we could hypothesize that zinc therapy has the potential to increase the serum zinc levels (above the deficiency cutoff) (36) and could promote shorter duration in the recovery of gustatory and/or olfactory function in patients with COVID-19 (38). Furthermore, the hypothesis involving the treatment with melatonin in patients with COVID-19 may suggest improved blood oxygen saturation and better sleep quality (33), as well as faster hospital discharge and improvement in the clinical symptoms (34, 35). However, the studies mentioned have inconclusive data with a relatively small sample size and early termination of the trial.
Among the research that used vitamin C therapy, there appears to be an agreement in observing a reduction in hyperinflammation (39, 43, 44, 47) and improvement in the oxygen support status of patients with COVID-19 (39, 41, 46, 47). However, there are still conflicting data regarding mortality rate, mechanical ventilation, and duration of the symptoms of patients with COVID-19. One important limitation among the studies was the lack of reports around the baseline vitamin C status of the patients with COVID-19. Since there is a great change in dietary vitamin C intake and thereafter in baseline plasma concentrations, if baseline concentrations are elevated, then the therapy with vitamin C could be less probable to promote an effect than when baseline concentrations are low.
Another important limitation of the studies in this review is related to the gender imbalance among the participants. Since the inflammatory response is influenced by sex (60) and there were a greater number of studies with male participants, caution should be exercised when extrapolating the findings to both genders. In addition, due to the lack of trials presenting zinc supplementation without combination with hydroxychloroquine, this review included only three studies using zinc therapy in patients with COVID-19. It is also worth mentioning that one of these studies had to discontinue the trial due to the low conditional power for benefit related to COVID-19 symptoms (37).
The lack of data on the monitoring of melatonin, zinc, and vitamin C therapy made it unclear whether these nutraceutical approaches have a direct antiviral response against SARS-CoV-2. Besides, a direct comparative investigation of the nutraceutical approaches comparing intravenous vs. oral supplementation can benefit current literature. Therefore, caution should be taken when extrapolating the outcomes on a larger scale, and additional data from the ongoing trials are needed to acquire more reports on the application of these molecules as a prevention and/or therapy in the present pandemic.
LB developed the idea and wrote the manuscript. BD and MG-F collected and prepared the study data. EH reviewed and edited the manuscript. All authors have read and agreed to the published version of the manuscript.
This work was supported by the CAPES (Coordenação de Aperfeiçoamento de Pessoal de Nível Superior) [grant numbers 88882.314890/2013-01 and 88882.365204/2019-01, Finance Code 001]; and CNPq (Conselho Nacional de Desenvolvimento Científico e Tecnológico) [grant number 308700/2017-1].
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnut.2021.821824/full#supplementary-material
1. Cui J, Li F, Shi Z-L. Origin and evolution of pathogenic coronaviruses. Nat Rev Microbiol. (2019) 17:181–92. doi: 10.1038/s41579-018-0118-9
2. WHO. WHO Coronavirus (COVID-19) Dashboard. (2021). Available online at: https://covid19.who.int/ (accessed December 22, 2021).
3. Shariare MH, Parvez MAK, Karikas GA, Kazi M. The growing complexity of COVID-19 drug and vaccine candidates: challenges and critical transitions. J Infect Public Health. (2021) 14:214–20. doi: 10.1016/j.jiph.2020.12.009
4. Sanders JM, Monogue ML, Jodlowski TZ, Cutrell JB. Pharmacologic treatments for coronavirus disease 2019 (COVID-19): a review. JAMA. (2020) 323:1824–36. doi: 10.1001/jama.2020.6019
5. Naja F, Hamadeh R. Nutrition amid the COVID-19 pandemic: a multi-level framework for action. Eur J Clin Nutr. (2020) 74:1117–21. doi: 10.1038/s41430-020-0634-3
6. Wu D, Lewis ED, Pae M, Meydani SN. Nutritional modulation of immune function: analysis of evidence, mechanisms, and clinical relevance. Front Immunol. (2018) 9:3160. doi: 10.3389/fimmu.2018.03160
7. Corrao S, Mallaci Bocchio R, Lo Monaco M, Natoli G, Cavezzi A, Troiani E, et al. Does evidence exist to blunt inflammatory response by nutraceutical supplementation during COVID-19 pandemic? an overview of systematic reviews of vitamin D, vitamin C, melatonin, and zinc. (2021) 13:1261. doi: 10.3390/nu13041261
8. Kaspari M, Powers JS. Biogeochemistry and geographical ecology: embracing all twenty-five elements required to build organisms. Am Nat. (2016) 188(Suppl):S62–73. doi: 10.1086/687576
9. Ames BN. Low micronutrient intake may accelerate the degenerative diseases of aging through allocation of scarce micronutrients by triage. Proc Natl Acad Sci U S A. (2006) 103:17589–94. doi: 10.1073/pnas.0608757103
10. Jayawardena R, Sooriyaarachchi P, Chourdakis M, Jeewandara C, Ranasinghe P. Enhancing immunity in viral infections, with special emphasis on COVID-19: a review. Diabetes Metab Syndr. (2020) 14:367–82. doi: 10.1016/j.dsx.2020.04.015
11. Feyaerts AF, Luyten W. Vitamin C as prophylaxis and adjunctive medical treatment for COVID-19? Nutrition. (2020) 79–80:110948. doi: 10.1016/j.nut.2020.110948
12. Vassilakopoulos T, Karatza M-H, Katsaounou P, Kollintza A, Zakynthinos S, Roussos C. Antioxidants attenuate the plasma cytokine response to exercise in humans. J Appl Physiol. (2003) 94:1025–32. doi: 10.1152/japplphysiol.00735.2002
13. Nieman DC, Peters EM, Henson DA, Nevines EI, Thompson MM. Influence of vitamin C supplementation on cytokine changes following an ultramarathon. J Interf cytokine Res Off J Int Soc Interf Cytokine Res. (2000) 20:1029–35. doi: 10.1089/10799900050198480
14. Fowler AA 3rd, Truwit JD, Hite RD, Morris PE, DeWilde C, Priday A, et al. Effect of vitamin c infusion on organ failure and biomarkers of inflammation and vascular injury in patients with sepsis and severe acute respiratory failure: the CITRIS-ALI randomized clinical trial. JAMA. (2019) 322:1261–70. doi: 10.1001/jama.2019.11825
15. Fujii T, Luethi N, Young PJ, Frei DR, Eastwood GM, French CJ, et al. Effect of vitamin c, hydrocortisone, and thiamine vs hydrocortisone alone on time alive and free of vasopressor support among patients with septic shock: the VITAMINS randomized clinical trial. JAMA. (2020) 323:423–31. doi: 10.1001/jama.2019.22176
16. Hu X, Yuan L, Wang H, Li C, Cai J, Hu Y, et al. Efficacy and safety of vitamin C for atrial fibrillation after cardiac surgery: a meta-analysis with trial sequential analysis of randomized controlled trials. Int J Surg. (2017) 37:58–64. doi: 10.1016/j.ijsu.2016.12.009
17. Gammoh NZ, Rink L. Zinc in Infection and Inflammation. Nutrients. (2017) 9:624–49. doi: 10.20944/preprints201705.0176.v1
18. Cao J-W, Duan S-Y, Zhang H-X, Chen Y, Guo M. Zinc deficiency promoted fibrosis via ROS and TIMP/MMPs in the myocardium of mice. Biol Trace Elem Res. (2020) 196:145–52. doi: 10.1007/s12011-019-01902-4
19. Patel VB, Zhong J-C, Grant MB, Oudit GY. Role of the ACE2/Angiotensin 1-7 axis of the renin-angiotensin system in heart failure. Circ Res. (2016) 118:1313–26. doi: 10.1161/CIRCRESAHA.116.307708
20. te Velthuis AJW, van den Worm SHE, Sims AC, Baric RS, Snijder EJ, van Hemert MJ. Zn(2+) inhibits coronavirus and arterivirus RNA polymerase activity in vitro and zinc ionophores block the replication of these viruses in cell culture. PLoS Pathog. (2010) 6:e1001176. doi: 10.1371/journal.ppat.1001176
21. Lanke K, Krenn BM, Melchers WJG, Seipelt J, van Kuppeveld FJM. PDTC inhibits picornavirus polyprotein processing and RNA replication by transporting zinc ions into cells. J Gen Virol. (2007) 88:1206–17. doi: 10.1099/vir.0.82634-0
22. Sapkota M, Knoell DL. Essential role of zinc and zinc transporters in myeloid cell function and host defense against infection. J Immunol Res. (2018) 2018:4315140. doi: 10.1155/2018/4315140
23. Hoeger J, Simon T-P, Beeker T, Marx G, Haase H, Schuerholz T. Persistent low serum zinc is associated with recurrent sepsis in critically ill patients - a pilot study. PLoS ONE. (2017) 12:e0176069. doi: 10.1371/journal.pone.0176069
25. Borges LDS, Dermargos A, Junior EPDS, Weimann E, Lambertucci RH, Hatanaka E. Melatonin decreases muscular oxidative stress and inflammation induced by strenuous exercise and stimulates growth factor synthesis. J Pineal Res. (2015) 58:166–72. doi: 10.1111/jpi.12202
26. Ishihara R, Barros MP, Silva CMD, Borges LDS, Hatanaka E, Lambertucci RH. Melatonin improves the antioxidant capacity in cardiac tissue of Wistar rats after exhaustive exercise. Free Radic Res. (2021) 55:776–91. doi: 10.1080/10715762.2021.1939024
27. Ramlall V, Zucker J, Tatonetti N. Melatonin is significantly associated with survival of intubated COVID-19 patients. medRxiv Prepr Serv Heal Sci. (2020). doi: 10.1101/2020.10.15.20213546
28. Amin AH, El-Missiry MA, Othman AI. Melatonin ameliorates metabolic risk factors, modulates apoptotic proteins, and protects the rat heart against diabetes-induced apoptosis. Eur J Pharmacol. (2015) 747:166–73. doi: 10.1016/j.ejphar.2014.12.002
29. van den Berg DF, Te Velde AA. Severe COVID-19: NLRP3 inflammasome dysregulated. Front Immunol. (2020) 11:1580. doi: 10.3389/fimmu.2020.01580
30. Ratajczak MZ, Kucia M. SARS-CoV-2 infection and overactivation of Nlrp3 inflammasome as a trigger of cytokine “storm” and risk factor for damage of hematopoietic stem cells. Leukemia. (2020) 34:1726–9. doi: 10.1038/s41375-020-0887-9
31. Borges L, Pithon-Curi TC, Curi R, Hatanaka E. COVID-19 and neutrophils: the relationship between hyperinflammation and neutrophil extracellular traps. Mediators Inflamm. (2020) 2020:8829674. doi: 10.1155/2020/8829674
32. Acuña-Castroviejo D, Carretero M, Doerrier C, López LC, García-Corzo L, Tresguerres JA, et al. Melatonin protects lung mitochondria from aging. Age. (2012) 34:681–92. doi: 10.1007/s11357-011-9267-8
33. Mousavi SA, Heydari K, Mehravaran H, Saeedi M, Alizadeh-Navaei R, Hedayatizadeh-Omran A, et al. Melatonin effects on sleep quality and outcomes of COVID-19 patients: An open-label, randomized, controlled trial. J Med Virol. (2021) 94:263–71. doi: 10.1002/jmv.27312
34. Alizadeh Z, Keyhanian N, Ghaderkhani S, Dashti-Khavidaki S, Shokouhi Shoormasti R, Pourpak Z, et al. Pilot study on controlling coronavirus disease 2019 (COVID-19) inflammation using melatonin supplement. Iran J Allergy Asthma Immunol. (2021) 20:494–9. doi: 10.18502/ijaai.v20i4.6959
35. Farnoosh G, Akbariqomi M, Badri T, Bagheri M, Izadi M, Saeedi-Boroujeni A, et al. Efficacy of a low dose of melatonin as an adjunctive therapy in hospitalized patients with COVID-19: a randomized, double-blind clinical trial. Arch Med Res. (2021). doi: 10.1016/j.arcmed.2021.06.006
36. Patel O, Chinni V, El-Khoury J, Perera M, Neto AS, McDonald C, et al. A pilot double-blind safety and feasibility randomized controlled trial of high-dose intravenous zinc in hospitalized COVID-19 patients. J Med Virol. (2021) 93:3261–7. doi: 10.1002/jmv.26895
37. Thomas S, Patel D, Bittel B, Wolski K, Wang Q, Kumar A, et al. Effect of high-dose zinc and ascorbic acid supplementation vs usual care on symptom length and reduction among ambulatory patients with SARS-CoV-2 infection: the COVID A to Z randomized clinical trial. JAMA Netw Open. (2021) 4:e210369. doi: 10.1001/jamanetworkopen.2021.0369
38. Abdelmaksoud AA, Ghweil AA, Hassan MH, Rashad A, Khodeary A, Aref ZF, et al. Olfactory disturbances as presenting manifestation among egyptian patients with COVID-19: possible role of zinc. Biol Trace Elem Res. (2021) 199:4101–8. doi: 10.1007/s12011-020-02546-5
39. Zhang J, Rao X, Li Y, Zhu Y, Liu F, Guo G, et al. Pilot trial of high-dose vitamin C in critically ill COVID-19 patients. Ann Intensive Care. (2021) 11:5. doi: 10.1186/s13613-020-00792-3
40. Kumari P, Dembra S, Dembra P, Bhawna F, Gul A, Ali B, et al. The role of vitamin C as adjuvant therapy in COVID-19. Cureus. (2020) 12:e11779. doi: 10.7759/cureus.11779
41. JamaliMoghadamSiahkali S, Zarezade B, Koolaji S, SeyedAlinaghi S, Zendehdel A, Tabarestani M, et al. Safety and effectiveness of high-dose vitamin C in patients with COVID-19: a randomized open-label clinical trial. Eur J Med Res. (2021) 26:20. doi: 10.1186/s40001-021-00490-1
42. Al Sulaiman K, Aljuhani O, Saleh KB, Badreldin HA, Al Harthi A, Alenazi M, et al. Ascorbic acid as an adjunctive therapy in critically ill patients with COVID-19: a propensity score matched study. Sci Rep. (2021) 11:17648. doi: 10.1038/s41598-021-96703-y
43. Zhao B, Liu M, Liu P, Peng Y, Huang J, Li M, et al. High dose intravenous vitamin C for preventing the disease aggravation of moderate COVID-19 pneumonia. A Retrospective Propensity Matched Before-After Study. Front Pharmacol. (2021) 12:638556. doi: 10.3389/fphar.2021.638556
44. Xia G, Fan D, He Y, Zhu Y, Zheng Q. High-dose intravenous vitamin C attenuates hyperinflammation in severe coronavirus disease 2019. Nutrition. (2021) 91–92:111405. doi: 10.1016/j.nut.2021.111405
45. Suna K, Melahat US, Murat Y, Figen ÖE, Ayperi Ö. Effect of high-dose intravenous vitamin C on prognosis in patients with SARS-CoV-2 pneumonia. Med Clin. (2021). doi: 10.1016/j.medcli.2021.04.010
46. Gao D, Xu M, Wang G, Lv J, Ma X, Guo Y, et al. The efficiency and safety of high-dose vitamin C in patients with COVID-19: a retrospective cohort study. Aging. (2021) 13:7020–34. doi: 10.18632/aging.202557
47. Xia G, Qin B, Ma C, Zhu Y, Zheng Q. High-dose vitamin C ameliorates cardiac injury in COVID-19 pandemic: a retrospective cohort study. Aging. (2021) 13:20906–14. doi: 10.18632/aging.203503
48. Ferlazzo N, Andolina G, Cannata A, Costanzo MG, Rizzo V, Currò M, et al. Is melatonin the cornucopia of the 21st century? Antioxidants. (2020) 9:1088. doi: 10.3390/antiox9111088
49. Zhou Y, Hou Y, Shen J, Mehra R, Kallianpur A, Culver DA, et al. A network medicine approach to investigation and population-based validation of disease manifestations and drug repurposing for COVID-19. PLoS Biol. (2020) 18:e3000970. doi: 10.1371/journal.pbio.3000970
50. Mistraletti G, Umbrello M, Sabbatini G, Miori S, Taverna M, Cerri B, et al. Melatonin reduces the need for sedation in ICU patients: a randomized controlled trial. Minerva Anestesiol. (2015) 81:1298–310.
51. Bourne RS, Mills GH, Minelli C. Melatonin therapy to improve nocturnal sleep in critically ill patients: encouraging results from a small randomised controlled trial. Crit Care. (2008) 12:R52. doi: 10.1186/cc6871
52. Cerullo G, Negro M, Parimbelli M, Pecoraro M, Perna S, Liguori G, et al. The long history of vitamin C: from prevention of the common cold to potential aid in the treatment of COVID-19. Front Immunol. (2020) 11:574029. doi: 10.3389/fimmu.2020.574029
53. Hemilä H, Chalker E. Vitamin C can shorten the length of stay in the ICU: a meta-analysis. Nutrients. (2019) 11:708. doi: 10.3390/nu11040708
55. Jothimani D, Kailasam E, Danielraj S, Nallathambi B, Ramachandran H, Sekar P, et al. COVID-19: poor outcomes in patients with zinc deficiency. Int J Infect Dis IJID Off Publ Int Soc Infect Dis. (2020) 100:343–9. doi: 10.1016/j.ijid.2020.09.014
56. Yasui Y, Yasui H, Suzuki K, Saitou T, Yamamoto Y, Ishizaka T, et al. Analysis of the predictive factors for a critical illness of COVID-19 during treatment - relationship between serum zinc level and critical illness of COVID-19. Int J Infect Dis IJID Off Publ Int Soc Infect Dis. (2020) 100:230–6. doi: 10.1016/j.ijid.2020.09.008
57. Han Y-S, Chang G-G, Juo C-G, Lee H-J, Yeh S-H, Hsu JT-A, et al. Papain-like protease 2 (PLP2) from severe acute respiratory syndrome coronavirus (SARS-CoV): expression, purification, characterization, and inhibition. Biochemistry. (2005) 44:10349–59. doi: 10.1021/bi0504761
58. Chasapis CT, Loutsidou AC, Spiliopoulou CA, Stefanidou ME. Zinc and human health: an update. Arch Toxicol. (2012) 86:521–34. doi: 10.1007/s00204-011-0775-1
59. Wessels I, Haase H, Engelhardt G, Rink L, Uciechowski P. Zinc deficiency induces production of the proinflammatory cytokines IL-1β and TNFα in promyeloid cells via epigenetic and redox-dependent mechanisms. J Nutr Biochem. (2013) 24:289–97. doi: 10.1016/j.jnutbio.2012.06.007
Keywords: SARS-CoV-2, clinical trial, observational study, therapy, hyperinflammation
Citation: Borges L, Gennari-Felipe M, Dias BB and Hatanaka E (2022) Melatonin, Zinc, and Vitamin C: Potential Adjuvant Treatment for COVID-19 Patients. Front. Nutr. 8:821824. doi: 10.3389/fnut.2021.821824
Received: 24 November 2021; Accepted: 27 December 2021;
Published: 26 January 2022.
Edited by:
Carol Gois Leandro, Federal University of Pernambuco, BrazilReviewed by:
Adriano Lima-Silva, Federal Technological University of Paraná, BrazilCopyright © 2022 Borges, Gennari-Felipe, Dias and Hatanaka. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Leandro Borges, c2JsZWFuZHJvQHlhaG9vLmNvbS5icg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.