 Jyh-Jou Chen1,2
Jyh-Jou Chen1,2 Chen-Yuan Hsu
Chen-Yuan Hsu
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Nutr. , 26 November 2021
Sec. Eating Behavior
Volume 8 - 2021 | https://doi.org/10.3389/fnut.2021.741647
Dietary behavior is a critical lifestyle factor affecting health. This study aimed to investigate food away from home (FAFH) and its effect on gastrointestinal (GI) health. A questionnaire-based survey was conducted with 300 participants at a hospital in Liouying, Taiwan. The survey collected demographic information and data on FAFH and GI health. The association of GI health with FAFH consumption behavior was significant (t-test, p < 0.05). Bodyweight status was associated with age (F = 5.01, p = 0.01), dietary situation (F = 1.96, p = 0.04), number of meals (F = 1.85, p = 0.03), dietary preferences (F = 2.84, p = 0), reasons for FAFH (F = 1.86, p = 0.02), FAFH types (F = 2.01, p = 0), and outcomes associated with FAFH (F = 2.51, p = 0). Gastrointestinal condition was associated with the number of meals (F = 2.55, p = 0), the level of activity after meals (F = 2.16, p = 0.02), and FAFH type (F = 1.48, p = 0.04). The results indicated that the participants aged 20–40 years had more problems related to their self-perceived body weight status than those aged 41–50 years. The results of this study clarify the FAFH among people in Taiwan and the effects on GI health and may serve as a reference for relevant behavioral research in food and health studies.
Economic development and changes in lifestyle and diseases have an impact on health demands (1, 2); thus, investigating the relationship between dietary behavior as one major component of lifestyle and human health is critical. Economic development and lifestyle changes have also led to an increasing number of people consuming food away from home (FAFH) (3–5). Clarifying the effect of health-related factors, such as dietary behavior, on gastrointestinal (GI) health is paramount (6, 7). Dietary behavior is a major lifestyle factor affecting health (8–12); relevant studies have reported that nutritional knowledge affects the lifestyle of people and may even cause health risks because of the correlation between dietary behaviors and lifestyle (13–16). However, studies on the impact of FAFH and its effect on GI health are relatively scant; thus, this topic merits further research.
Unhealthy dietary habits are a major cause of disease in individuals of all ages (17, 18). Food away from home has been reported to shift with social changes and dietary development, particularly among those aged >50 years (4, 10). Furthermore, researchers have suggested that awareness of healthy diets with respect to FAFH should be promoted among older people because of the health needs of an aging population (4, 10). A study of people aged >50 years regarding eating-out behavior in Taiwan did not identify an association between FAFH and self-perceived GI health status (4). The researchers attributed this finding to the tendency among the participants to avoid consuming salty and spicy FAFH and to limit their overall FAFH consumption. The study did not observe an association between GI symptoms, such as abdominal pain, GI discomfort, constipation, and FAFH consumption behaviors (4). Therefore, the age factor should receive more attention when considering food consumption behaviors and whether they are associated with GI health.
Studies have also indicated that sex differences may affect health behaviors related to diet (18, 19). A study of FAFH consumption among Korean adolescents (18) revealed that adolescents favored spicy and salty foods, which is indicative of fast-food and processed food consumption. Another study indicated that Iranian female adolescents had high scores for snacking; their eating patterns were also associated with more mental health problems (19).
Several other international studies have revealed that food (20–24), diet (25–27), diet quality (28, 29), and eating behaviors (30) are associated not only with obesity and health problems but also with the quality of life (31–35) and related life satisfaction (36). The effects of FAFH on GI health merit greater attention. In this study, we explored FAFH and its effect on GI health.
A questionnaire-based survey was conducted with 300 participants aged 20–80 years at the Chi Mei Medical Center (Liouying District, Tainan City, Taiwan) from July 2016 to June 2017. The sample size had power of 0.8 with an alpha significance of 0.05 and an effect size of 0.8 (37). The study participants were required to speak Mandarin or Taiwanese Hoklo dialect and to have no cognitive disorders that could affect their participation. The study was conducted in accordance with the STROBE (Equator Guidelines). All the participants provided written informed consent.
A flowchart of participant recruitment is provided in Figure 1. We assessed 308 participants for eligibility, and 8 participants were excluded: 5 declined to complete the survey, 2 did not meet the age criterion, and 1 did not meet the language criterion. Therefore, we completed the data collection in 300 participants.

Figure 1. A flowchart of participant recruitment.
The study was conducted in accordance with the Declaration of Helsinki and approved by the regional ethics committee of the Institutional Review Board of Chi Mei Medical Center, Tainan, Taiwan (IRB Serial No: 10406-L01).
The survey was a self-reported structured questionnaire (38) to collect demographic data and to assess the FAFH and GI health of respondents. Demographic information was collected on age, sex, ethnicity, education level, marital status, and religion. The questionnaire on FAFH contained 40 questions in eight categories: dietary situation, number of meals, dining situation, level of activity after meals, dietary preferences, the reason for FAFH, FAFH types, and outcomes associated with FAFH (38). Answers were provided on a five-point scale (0, never; 1, rarely; 2, occasionally; 3, often; and 4, always) (38). The higher the score means the seriousness of FAFH behavior. The Cronbach's α for the questionnaire was 0.85, revealing favorable internal consistency (38).
The dietary situation was assessed with three questions as eating habits, on whether the participants regularly consumed breakfast, lunch, and dinner. For the number of meals that the participants consumed per day, five questions were employed (one, two, three, four, or five or more meals per day).
The dining situation was assessed with four questions about religious or medical food restrictions, perceived comfort with the dining environment, the experience of pain and discomfort during meals, and consumption of nutritional food supplements (38).
For the level of activity after meals, the participants rated three items: working, resting, or walking. For dietary preferences, the participants rated five items: salty, spicy, sour, sweet, or plain foods. The reasons for FAFH included five questions related to family composition, which family members were involved in food preparation and the availability and convenience of various FAFH options. Preferred FAFH types of participants were assessed through nine questions. The FAFH types included vegetarian cuisine, Japanese cuisine, Chinese cuisine, Western cuisine, local cuisine, foods from quick-service restaurants, casual dining, food from buffet restaurants, and food from night markets. Finally, the survey also included six questions on outcomes associated with FAFH, such as frequency of FAFH [e.g., occasional, almost daily, during weekends and public holidays, during visits to relatives and friends, and during travel or special anniversaries; (38)].
The assessment of GI health included two items: body weight status and GI condition. Bodyweight status included five questions: self-perceived assessment of being overweight, being underweight, having abdominal obesity (e.g., potbelly and beer belly), having lipedema (accumulation of fat cells in the tissues under the skin), and being obese. The self-perceived assessment of GI condition included 11 questions about gastroesophageal reflux disease (GERD), heartburn, nausea, dysphagia, swallowing difficulties, hyperchlorhydria, hypochlorhydria (a low level of stomach acid), duodenal ulcer, food absorption problems, colon-related complications, and constipation. Answers were provided on a five-point scale (0, never; 1, rarely; 2, occasionally; 3, often; and 4, always) (38). The higher the score, the more problems related to their self-perceived GI health. The Cronbach's α for the questionnaire was 0.84, revealing favorable internal consistency (38).
All statistical analyses were performed using SPSS version 22.0 (SPSS Inc., Chicago, IL, USA). The data were analyzed using frequencies and percentages, t-tests, and Scheffe's test. The resulting content validity index was 0.85, confirming that the questionnaire was appropriate and applicable. The reliability of our research was assessed using Cronbach's α to assess internal consistency. Cronbach's α ranged from 0.84 to 0.85. For all statistical tests, p < 0.05 indicated significance.
The participants had a mean age of 41 years (SD: 12 years). Most of the participants (63%) were aged 20–40 years, and they were more likely to be women (n = 221, 73.7%), Hoklo Taiwanese (n = 274, 91.3%), college or university graduates (n = 181, 60.3%), and married (n = 186, 62%); the most common religion was Taoism (n = 129, 43%; Table 1).
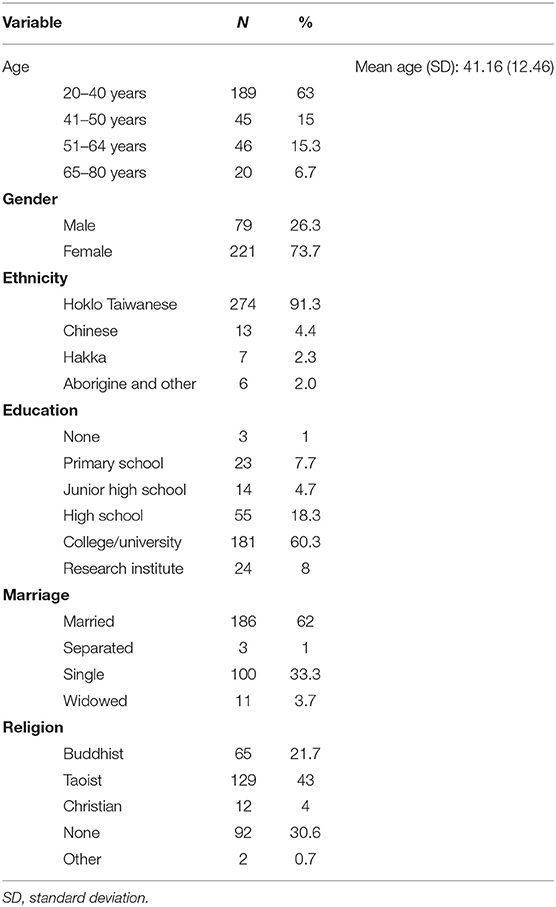
Table 1. Participant demographics (N = 300).
The results of the survey showed that dietary situation, number of meals, dining situation, level of activity after meals, dietary preferences, reason of FAFH, FAFH types, and outcomes associated with FAFH were significantly different among the participants (Table 2).
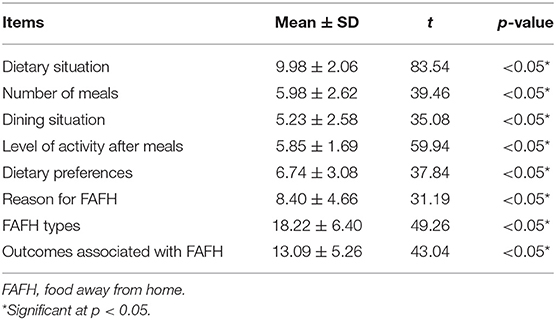
Table 2. FAFH consumption behavior scores of the participants (N = 300).
Self-perceived abdominal obesity (e.g., having a potbelly or a beer belly) had the highest score (1.96 ± 1.34) in the bodyweight status category, followed by being overweight (1.84 ± 1.36), being obese (1.75 ± 1.39), having lipedema (1.62 ± 1.28), and being underweight (0.54 ± 0.89) (Table 3; Figure 2).
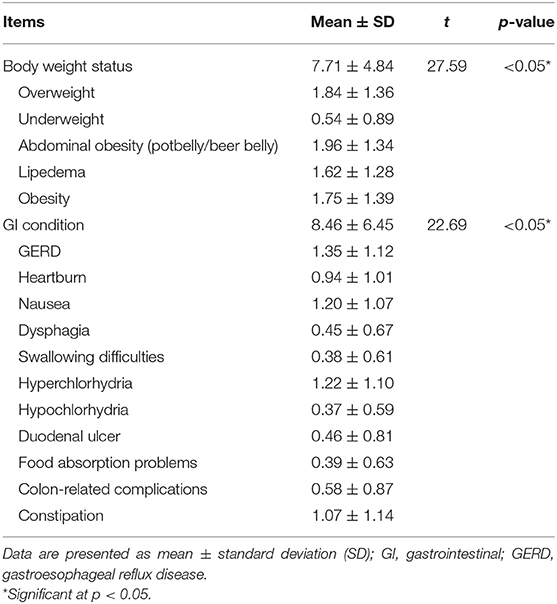
Table 3. Predictors of GI health of the participants (N = 300).
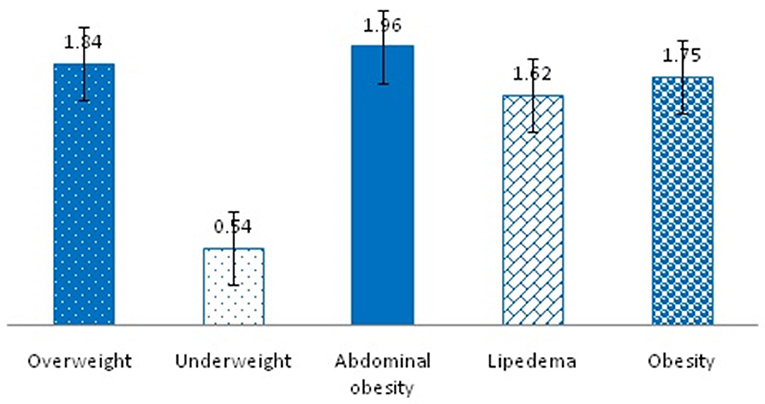
Figure 2. Self-perceived in the bodyweight status.
Self-perceived GERD had the highest score (1.35 ± 1.12) in the GI condition category, followed by hyperchlorhydria (1.22 ± 1.1), nausea (1.20 ± 1.07), constipation (1.07 ± 1.14), heartburn (0.94 ± 1.01), colon-related complications (0.58 ± 0.87), duodenal ulcer (0.46 ± 0.81), dysphagia (0.45 ± 0.67), food absorption problems (0.39 ± 0.63), swallowing difficulties (0.38 ± 0.61), and hypochlorhydria (0.37 ± 0.59) (Table 3; Figure 3).
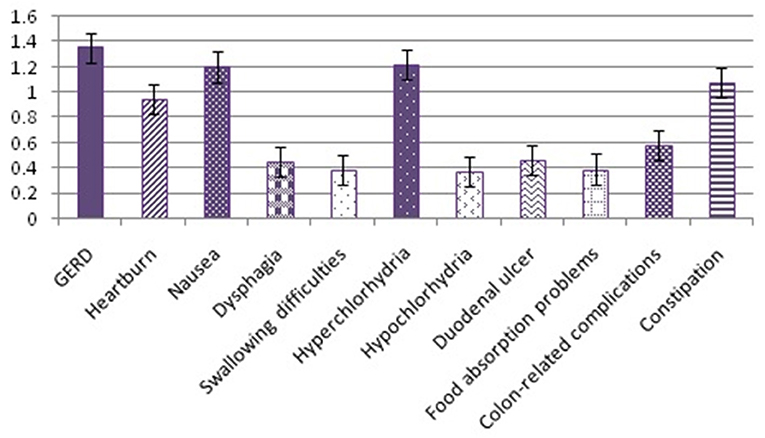
Figure 3. Self-perceived in the gastrointestinal (GI) condition.
Both body weight status and GI condition were significant predictors of GI health (Table 3).
The predictors of GI health are listed in Table 4. Subsequent comparisons using Scheffe's post-hoc analysis also revealed significant differences (1>2); an age factor of 1, 2, 3, and 4 represented those aged 20–40 years, 41–50 years, 51–64 years, and 65–80 years, respectively. The results indicated that the participants aged 20–40 years had more problems related to their self-perceived body weight status than those aged 41–50 years.
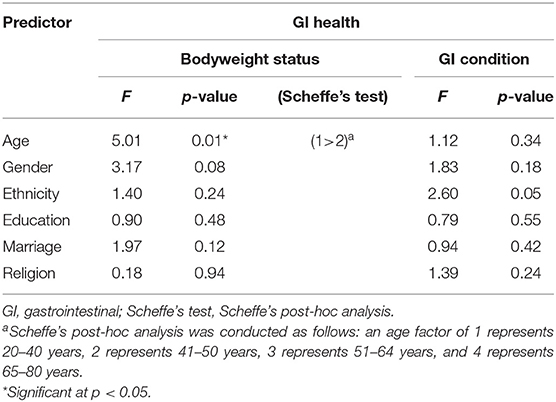
Table 4. Predictors of GI health (N = 300).
Food away from home is presented in Table 5. Significant differences were observed in the dietary situation, the number of meals, dietary preferences, reasons for FAFH, FAFH types, and outcomes associated with FAFH in relation to body weight status (p < 0.05). Significant differences were also noted in the number of meals, level of activity after meals, and FAFH types in relation to GI condition (p < 0.05).
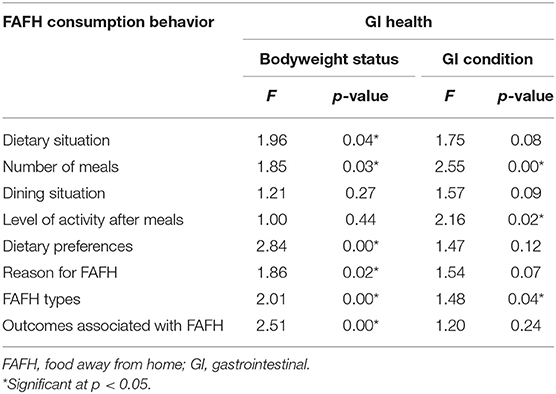
Table 5. Association of GI health with FAFH consumption behavior (N = 300).
This study investigated FAFH and its effect on GI health among people in a single-center hospital setting in Taiwan. Significant differences were observed in all eight measures used to measure FAFH. These results are consistent with those of previous studies. The relationship between diet and health is associated with changes in lifestyle patterns (3–5, 39, 40); thus, attention should be paid to the increase in FAFH that accompanies economic development and lifestyle changes.
The significant differences in body weight status and GI condition are also consistent with the results of previous studies (8, 9, 14, 16). Further research is warranted to clarify how GI health status affects overall health needs. The association between age and body weight status was also consistent with the findings of previous studies (3, 4, 6, 7). Given that the FAFH of adults also changes because of social changes and economic development, adopting healthy dietary habits to maintain GI health should be emphasized. Notably, although no significant relation was observed between gender and body weight, the finding almost reached significance and is consistent with the finding of a related study (41). The influence of sex and body weight status on FAFH merits further research.
This study suggested that healthcare providers and professionals should prioritize dietary recommendations and health topics according to the health behaviors of individuals and should adopt health education according to their ages. For example, individuals aged 20–40 years might benefit from food education on body weight control, FAFH, and GI health. Developing more effective education strategies by adding new topics (e.g., major food safety concerns, behavioral nutrition, dietary prevention of GI disease, and dietary behavior screening) to enable in their daily lives implement correctly eating behavior to improve the overall GI health of the individual.
The results of this study address a gap in knowledge about the effect of FAFH on GI health in a single-center hospital setting in Taiwan. However, this study has some limitations. First, this study has not asked participants their primary reasons for coming to the hospital. This, obviously, might have put a major bias, such as the participants were referred or they came to the hospital only for their actual/self-perceived gastrointestinal problems, which could directly interfere with the main outcome of this study, i.e., it might be possible that to overestimate the score of participants with self-perceived GI health status. Second, this study used a self-reported survey to explore FAFH and GI health; thus, responses may not be a full expression of the actual lifestyles of the participants. Third, this study was conducted at a single center in Taiwan; generalizing the results to other populations should, therefore, be undertaken with caution. In particular, some of the questions addressed sensitive topics, such as the level of activity after meals and reasons for FAFH. The sensitivity of these topics may have led to a reporting bias; it may need a further deep interview or discussion. Last, this study has collected some data on marital status, religion, and gender but did not explore the association with FAFH; it might be intuitively logical to think that marital (being married) and employment status (being unemployed or both husband and wife are employed, etc.) and the gender of the spouse of the participants might affect dietary behaviors, such as FAFH. Consequently, these might have affected their willingness to respond correctly/honestly. Hence, as a suggestion for future studies, such factors must be considered in further designs.
The current results revealed a significant association between GI health and the FAFH of the study participants. In particular, significant differences were noted in dietary situations, the number of meals, dietary preferences, the reason for FAFH, FAFH types, and outcomes associated with FAFH according to body weight status. Significant differences were also observed in the number of meals, level of activity after meals, and FAFH types according to GI condition. Collectively, these results indicate that FAFH can associate with GI health and should thus be further explored. The current results expand the knowledge of the relationship between FAFH and GI health and, thus, may serve as a reference for relevant behavioral research in food and health studies.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by the Regional Ethics Committee of the Institutional Review Board of Chi Mei Medical Center, Tainan, Taiwan (IRB Serial No: 10406-L01). Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
J-JC and C-YH: conceptualization, formal analysis, resources, and writing original draft preparation. C-YH: methodology, software, data curation, writing—review and editing, visualization, supervision, project administration, and funding acquisition. J-JC, L-YT, J-MT, and C-YH: validation. J-JC: investigation. All authors contributed to the article and approved the submitted version.
This research was supported by the Chi Mei Medical Center Research Fund (Grant No. 10406-L01).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors thank all the participants from the Chi Mei Medical Center, Liouying, Taiwan. This manuscript was edited by Wallace Academic Editing.
1. Kennedy E, Offutt SE. Healthy lifestyles for healthy Americans: report on USDA's year 2000 behavioral nutrition roundtable. Nutr Today. (2000) 35:84–8. doi: 10.1097/00017285-200005000-00002
2. Tang HC, He MS, Lin WY, Wu JL, Wang TW, Wang WB. Research of between health promotion life state and harm healthy behavior. J Far East Collect. (2007) 24:43–54.
3. Chen NW, Chang TH, Chang SP, Sung HY. The association of health promoting lifestyle and quality of life among nurses. Cheng Ching Med J. (2011) 7:27–37. doi: 10.30156/CCMJ.201104.0004
4. Chou HL, Lee MH, Lu C, Lee SC. A study of relationships in senior out-dining behavior and self-conscious health. J Leis Sports Health. (2011) 2:112–29. doi: 10.6204/JRSHP.2011.02.08
5. Fu A, Jien J. The impact of college students' attributes on nutrition knowledge, dietary attitudes, and dietary practices in Taiwan. Nutr Sci J. (2009) 34:142–54. doi: 10.6691/NSJ.200912_34(4)0.0004
6. Ibiebele TI, Taylor AR, Whiteman DC, van der Pols JC. Eating habits and risk of esophageal cancers: a population-based case-control study. Cancer Causes Control. (2010) 21:1475–84. doi: 10.1007/s10552-010-9576-8
7. Koritar P, Philippi ST, dos Santos Alvarenga M. Attitudes toward health and taste of food among women with bulimia nervosa and women of a non-clinical sample. Appetite. (2017) 113:172–7. doi: 10.1016/j.appet.2017.02.029
8. Bostic SM, McClain AC. Older adults' cooking trajectories: shifting skills and strategies. Br Food J. (2017) 119:1102–15. doi: 10.1108/BFJ-09-2016-0436
9. Chang RCY. The influence of attitudes towards healthy eating on food consumption when travelling. Curr Issues Tour. (2017) 20:369–90. doi: 10.1080/13683500.2014.890579
10. Chen FS. Effect of diet on life-style diseases and its role in disease prevention. J Long Term Care. (2005) 9:32–8. doi: 10.6317/LTC.200503_9(1)0.0002
11. Chen YK, Lee CH, Wu IC, Liu JS, Wu DC, Lee JM, et al. Food intake and the occurrence of squamous cell carcinoma in different sections of the esophagus in Taiwanese men. Nutrition. (2009) 25:753–61. doi: 10.1016/j.nut.2009.02.002
12. Loureiro LMR, Almeida LFF, Machado CJ, Pessoa MC, Duarte MSL, Franceschini SCC, et al. Food consumption and characteristics associated in a Brazilian older adult population: a cluster analysis. Front Nutr. (2021) 8:641263. doi: 10.3389/fnut.2021.641263
13. Lai CY. The effects of nutrition knowledge and healthy lifestyle on college students' healthy eating behavior. Yu Da Acad J. (2008) 22:239–53.
14. Lee KI, Lin WT, Chiang WD. Do demographic characteristics influence the eating competence of elderly Taiwanese? Asia Pacif J Clin Nutr. (2017) 26:175–81. doi: 10.6133/apjcn.052016.01
15. Li G, Zhu C, Ren BY, Deng C, Zhang J, Zhang L, et al. Clinical effective analysis of chemo-radiotherapy for esophageal carcinoma patients with dietary and lifestyle factors of high and low risk. World Chin J Digestol. (2008) 16:771–5. doi: 10.11569/wcjd.v16.i7.771
16. Wu Y, Fan Y, Jiang Y, Wang Y, Liu H, Wei M. Analysis of risk factors associated with precancerous lesion of gastric cancer in patients from Eastern China: a comparative study. J Cancer Res Ther. (2013) 9:205–9. doi: 10.4103/0973-1482.113351
17. Kim J, Park E. Comparisons of cardiometabolic biomarkers, lifestyle behaviors, and dietary sodium and potassium intake in a representative sample of Korean adults with and without cardio-cerebrovascular diseases. Asian Nurs Res. (2017) 11:223–9. doi: 10.1016/j.anr.2017.08.002
18. Shin Y, Kang SJ. Health behaviors and related demographic factors among Korean adolescents. Asian Nurs Res. (2014) 8:150–57. doi: 10.1016/j.anr.2014.05.006
19. Abbasalizad Farhangi M, Dehghan P, Jahangiry L. Mental health problems in relation to eating behavior patterns, nutrient intakes and health related quality of life among Iranian female adolescents. PLoS ONE. (2018) 13:e0195669. doi: 10.1371/journal.pone.0195669
20. Abris GP, Provido SMP, Hong S, Yu SH, Lee CB, Lee JE. Association between dietary diversity and obesity in the Filipino Women's Diet and Health Study (FiLWHEL): a cross-sectional study. PLoS ONE. (2018) 13:e0206490. doi: 10.1371/journal.pone.0206490
21. Frison S, Smith J, Blanchet K. Does the humanitarian sector use evidence-informed standards? A review of the 2011 sphere indicators for wash, food security and nutrition, and health action. PLoS Curr Disast. (2018) 10. doi: 10.1371/currents.dis.40805a591152be1c1431b5dab43e516d
22. Magnus A, Cobiac L, Brimblecombe J, Chatfield M, Gunther A, Ferguson M, et al. The cost-effectiveness of a 20% price discount on fruit, vegetables, diet drinks and water, trialled in remote Australia to improve indigenous health. PLoS ONE. (2018) 13:e0204005. doi: 10.1371/journal.pone.0204005
23. McBurney MI, Yu EA, Ciappio ED, Bird JK, Eggersdorfer M, Mehta S. Suboptimal serum alpha-tocopherol concentrations observed among younger adults and those depending exclusively upon food sources, NHANES 2003-20061-3. PLoS ONE. (2015) 10:e0135510. doi: 10.1371/journal.pone.0135510
24. Nwankwo ONO, Mokogwu N, Agboghoroma O, Ahmed FO, Mortimer K. Knowledge, attitudes and beliefs about the health hazards of biomass smoke exposure amongst commercial food vendors in Nigeria. PLoS ONE. (2018) 13:e0191458. doi: 10.1371/journal.pone.0191458
25. Agbadi P, Urke HB, Mittelmark MB. Household food security and adequacy of child diet in the food insecure region north in Ghana. PLoS ONE. (2017) 12:e0177377. doi: 10.1371/journal.pone.0177377
26. Kabir A, Miah S, Islam A. Factors influencing eating behavior and dietary intake among resident students in a public university in Bangladesh: a qualitative study. PLoS ONE. (2018) 13:e0198801. doi: 10.1371/journal.pone.0198801
27. Oli N, Vaidya A, Pahkala K, Eiben G, Krettek A. Knowledge, attitude and practice on diet and physical activity among mothers with young children in the Jhaukhel-Duwakot health demographic surveillance site, Nepal. PLoS ONE. (2018) 13:e0200329. doi: 10.1371/journal.pone.0200329
28. Buijsse B, Jacobs DR Jr., Steffen LM, Kromhout D, Gross MD. Plasma ascorbic acid, a priori diet quality score, and incident hypertension: a prospective cohort study. PLoS ONE. (2015) 10:e0144920. doi: 10.1371/journal.pone.0144920
29. Conrad Z, Niles MT, Neher DA, Roy ED, Tichenor NE, Jahns L. Relationship between food waste, diet quality, and environmental sustainability. PLoS ONE. (2018) 3:e0195405. doi: 10.1371/journal.pone.0195405
30. Seto E, Hua J, Wu L, Shia V, Eom S, Wang M, et al. Models of individual dietary behavior based on smartphone data: the influence of routine, physical activity, emotion, and food environment. PLoS ONE. (2016) 11:e0153085. doi: 10.1371/journal.pone.0153085
31. Marcinkevage J, Mayen AL, Zuleta C, DiGirolamo AM, Stein AD, Ramirez-Zea M. Relative validity of three food frequency questionnaires for assessing dietary intakes of Guatemalan schoolchildren. PLoS ONE. (2015) 10:e0139125. doi: 10.1371/journal.pone.0139125
32. Silva WRD, Campos J, Maroco J. Impact of inherent aspects of body image, eating behavior and perceived health competence on quality of life of University students. PLoS ONE. (2018) 13:e0199480. doi: 10.1371/journal.pone.0199480
33. Su FP, Chang LH, Mao HF, Hwang EJ. Development of the Taiwanese version of the Health Enhancement Lifestyle Profile (HELP-T). PLoS ONE. (2018) 13:e0199255. doi: 10.1371/journal.pone.0199255
34. Wang T, Jiang M, Ren Y, Liu Q, Zhao G, Cao C, et al. Health-related quality of life of community thyroid cancer survivors in Hangzhou, China. Thyroid. (2018) 28:1013–23. doi: 10.1089/thy.2017.0213
35. Zhao Z, Ma Y, Han Y, Liu Y, Yang K, Zhen S, et al. Psychosocial correlates of food addiction and its association with quality of life in a non-clinical adolescent sample. Nutrients. (2018) 10:837. doi: 10.3390/nu10070837
36. Liu R, Grunert KG. Satisfaction with food-related life and beliefs about food health, safety, freshness and taste among the elderly in China: a segmentation analysis. Food Qual Prefer. (2020) 79:103775. doi: 10.1016/j.foodqual.2019.103775
37. Polit DF, Beck CT. Nursing Research: Generating and Assessing Evidence for Nursing Practice. 9th ed. New York, NY: Wolters Kluwer Health/Lippincott Williams & Wilkins (2012).
38. Chen JJ, Hsu CY. The Investigation of the Lifestyle, Eating Out Habits and Drug Use Behavior on the Gastroenterology Outpatients (Issue Brief No. 10406-L01). Liouying: Chi Mei Medical Center (2015).
39. Chang HP, Ma CC, Chen HS. The impacts of young consumers' health values on functional beverages purchase intentions. Int J Environ Res Publ Health. (2020) 17:3479. doi: 10.3390/ijerph17103479
40. Kavian F, Mehta K, Willis E, Mwanri L, Ward P, Booth S. Migration, stress and the challenges of accessing food: an exploratory study of the experience of recent afghan women refugees in Adelaide, Australia. Int J Environ Res Publ Health. (2020) 17:1379. doi: 10.3390/ijerph17041379
Keywords: food away from home (FAFH), gastrointestinal, health, consumption behavior, dietary behavior
Citation: Chen J-J, Tsai L-Y, Tsai J-M and Hsu C-Y (2021) Food Away From Home and Self-Perceived Gastrointestinal Health. Front. Nutr. 8:741647. doi: 10.3389/fnut.2021.741647
Received: 15 July 2021; Accepted: 20 September 2021;
Published: 26 November 2021.
Edited by:
Nicholas T. Bello, Rutgers, The State University of New Jersey, United StatesReviewed by:
Reza Rastmanesh, Independent Researcher, Tehran, IranCopyright © 2021 Chen, Tsai, Tsai and Hsu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Chen-Yuan Hsu, Y2hlbjA5MDRAbWFpbC5keXUuZWR1LnR3
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.