 Jiaying Ni1†
Jiaying Ni1† Hao Peng
Hao Peng- 1Department of Obstetrics and Gynecology, Xinhua Hospital Affiliated to Shanghai JiaoTong University School Medicine, Shanghai, China
- 2Department of Internal Medicine, Nanjing Gaochun People's Hospital, Nanjing, China
- 3Department of General Surgery, Nanjing Gaochun People's Hospital, Nanjing, China
- 4Department of Obstetrics and Gynecology, Huangshi Central Hospital, Affiliated Hospital of Hubei Polytechnic University, Edong Healthcare Group, Huangshi, China
Objective: The results from epidemiologic studies on the relationship between intake of coffee and the risk of gestational diabetes mellitus (GDM) remain inconclusive. A meta-analysis was performed to achieve a comprehensive finding regarding the association between intake of coffee and the risk of GDM.
Methods: PubMed, Scopus, ISI Web of Science, and Google Scholar were searched to find articles published up to August 2021. Observational studies that reported risk estimates [risk ratios (RRs), hazard ratios (HRs), and odds ratios (ORs)] for the association of consumption of coffee with the risk of GDM in pregnant women were included. Random effects model was applied to calculate summarized risk estimate and 95% CIs for the highest vs. lowest categories of intake of coffee.
Results: Seven observational studies (three cohort, two case-control, and two cross-sectional studies) with 75,607 participants and 1,625 women with GDM met the inclusion criteria. The meta-analysis of comparing the highest vs. lowest intake of coffee categories showed no significant association between intake of coffee and risk of GDM (summarized risk estimate: 0.89; 95% CI: 0.76, 1.05; I2 = 63.4%). Subgroup analysis showed that consumption of coffee had an inverse relationship with GDM in studies conducted in non-Asia countries (summarized risk estimate: 0.75; 95% CI: 0.58, 0.97; I2 = 6%).
Conclusion: This study has shown that high consumption of coffee did not decrease the risk of GDM. Furthermore, large-scale cohort studies are required to confirm our findings.
Introduction
Gestational diabetes mellitus (GDM) is a disease in which pregnant women who did not have diabetes before pregnancy develops glucose intolerance because of the interference of pregnancy hormones with the action of insulin (1, 2). It has been estimated that roughly 15 to 20% of pregnant women were affected by GDM (3). High gestational age, obesity, polycystic ovary syndrome, ethnicity, glycosuria, family history of diabetes, and previous history of GDM are underlying risk factors of GDM (4). Approximately 70% of women with GDM will be affected by type 2 diabetes mellitus (T2DM) later in their life (5). Infants born to mothers with GDM are at increased risk of macrosomia, hypoglycemia, jaundice, and epigenetic changes (6). In the long term, they are prone to being obese or diabetic in childhood (7). Therefore, the identification of preventive strategies to reduce GDM has great importance.
Diet and physical activity are fundamental lifestyle interventions to control GDM (7). Using foods with a low glycemic index, high antioxidants, and also decrease in intake of energy, distribution of carbohydrates, and intake of fat or protein modification share some dietary recommendations for women with GDM (8–11).
Coffee is commonly drunk among women aged 20–50 years, and thus their possible effects on GDM absorb many interests (12). A meta-analysis of prospective cohort studies exhibited both the caffeinated and decaffeinated coffee was associated with reduced diabetes risk (13). It appears that the influence of intake of coffee on GDM may vary from T2DM in non-pregnant women. Metabolism of caffeine as the main phytochemical in coffee decreases during pregnancy (14), and subsequently, a high amount of caffeine levels in blood was related to elevating insulin resistance (15). It seems that the favorable effects of coffee are not linked to caffeine and its metabolites during pregnancy, and originated from antioxidants and prebiotic compounds, including phenolic components and micronutrients, which can improve insulin sensitivity and glycemic response (16).
The findings of studies regarding the association of intake of coffee with GDM are conflicting. A double-blind, randomized crossover study indicated that acute caffeine ingestion impairs insulin sensitivity in women with GDM (17). Furthermore, some observational studies displayed no relationship between intake of coffee and GDM (18–21), while two studies showed inverse associations (22, 23).
Based on our knowledge, there is no systematic review and meta-analysis to clarify the association between the consumption of coffee and the risk of GDM. Therefore, the purpose of this study is to achieve a solid response to this question: Is consumption of coffee associated with the risk of GDM in pregnant women?
Methods
The protocol of this study has been established based on Preferred Reporting Items of Systematic Reviews and Meta-Analysis (PRISMA) criteria (24).
Search Strategy
Two independent authors undertook a systematic search in PubMed, Scopus, ISI Web of Sciences, and Google Scholar to determine the pertinent articles with publication dates until August 2021. The search was performed using medical subject heading (MeSH) and related keywords including: coffee, caffeine diabetes, gestational, gestational diabetes, GDM or diabetes, and gestational (Mesh). No restrictions such as language were taken into account when the search was conducted. The citations of selected articles and retrieved reviews were manually checked to avoid missing any papers.
Inclusion and Exclusion Criteria
Studies with the following criteria were eligible for this review: observational studies (cohort, cross-sectional, or case-control studies), those carried out on pregnant women, studies reported risk estimates [relative risk (RR), odds ratio (OR), and hazard ratio (HR) with corresponding 95% CIs] for the association between consumption of coffee and the risk of GDM. Articles were included whether they considered total coffee or caffeinated coffee and decaffeinated coffee separately.
We excluded one study that assessed the association between coffee and tea and the risk of GDM (25). Tea has a different nutritional composition as compared with coffee, and therefore, the compounds in tea are likely to have different effects, and assessment of a combination of coffee and tea unable us to find a pure effect of coffee. Furthermore, irrelevant papers, abstracts, unpublished essays, review articles, commentary, editorial, or letters were removed.
Quality Assessment
Newcastle-Ottawa Scale (NOS) was used to determine the risk of bias of each article included (26). If one study acquires a score of ≥7, it is contemplated as high quality. Two researchers evaluated the methodological quality of each study independently. If they could not reach any consensus, a third party (Principal investigator) decided by a discussion with them.
Data Extraction and Abstraction
Two investigators exploited separately the desired information using prespecified forms, and in case when they faced disagreements, they discussed it with the third author to reach a firm opinion. The following data were extracted: surname of the first author, date of publication, study design, geographic region, age, gender, follow-up duration (in prospective cohort studies), sample size, number of cases, number of controls in case-control studies, categories of intake of coffee, estimated risk (RR, HR, OR), diagnostic criteria for GDM, dietary measurement method, and adjusted variables. In the terms of estimated risk with different adjustment models, we choose that one controlled the greatest number of main covariates. If one study reported a separate risk estimate for caffeinated and decaffeinated coffee rather than the total consumption of coffee, we included a risk estimate for caffeinated coffee in the principal analysis.
Statistical Analysis
In the meta-analysis comparing high vs. low intake categories of coffee, we used a random effects model to combine risk estimates (including RRs, HRs, and ORs) and 95% CIs of GDM. To assess the weight of each study, the standard error for the log RR/HR/OR of each study was regarded as the estimated variance of the log RR, using inverse variance methods (27). Cochrane Q-test and I2-test were used to assess heterogeneity among pertinent studies. Cochrane Q test, with P < 0.1 indicating significant between-study heterogeneity. The values I2 of 25–50, 50–75, and >75% were considered as low, moderate, and high heterogeneity, respectively (28). Subgroup analysis was implemented to identify sources of heterogeneity according to the relevant variables: geographic region, study design, number of cases, sample size, diagnostic criteria for GDM, dietary assessment method, adjustment to dietary energy intake, and body mass index (BMI), and quality of studies. Inspection of the funnel plots for asymmetry and Egger test (P < 0.10) were employed to detect publication bias (29). A sensitivity analysis was carried out to investigate the dependency of overall effect size to each study by leaving one study and repeating the analysis. All statistical analyses were performed using STATA software version 15.1 (Stata Corporation, College Station, Texas, USA). The P > 0.05 was speculated as significant.
Results
The flowchart of study selection was displayed in Figure 1. The title and abstract of 162 records identified through the initial search were screened following inclusion and exclusion criteria. After deleting unrelated papers, the full-texts of a total of 17 remained articles were checked. In this stage, 10 articles were omitted because of the following reasons: irrelevant articles (n = 9) and consideration of both tea and coffee as exposure (n = 1). Finally, seven epidemiologic studies possessed eligibility to this study (18–23, 30).
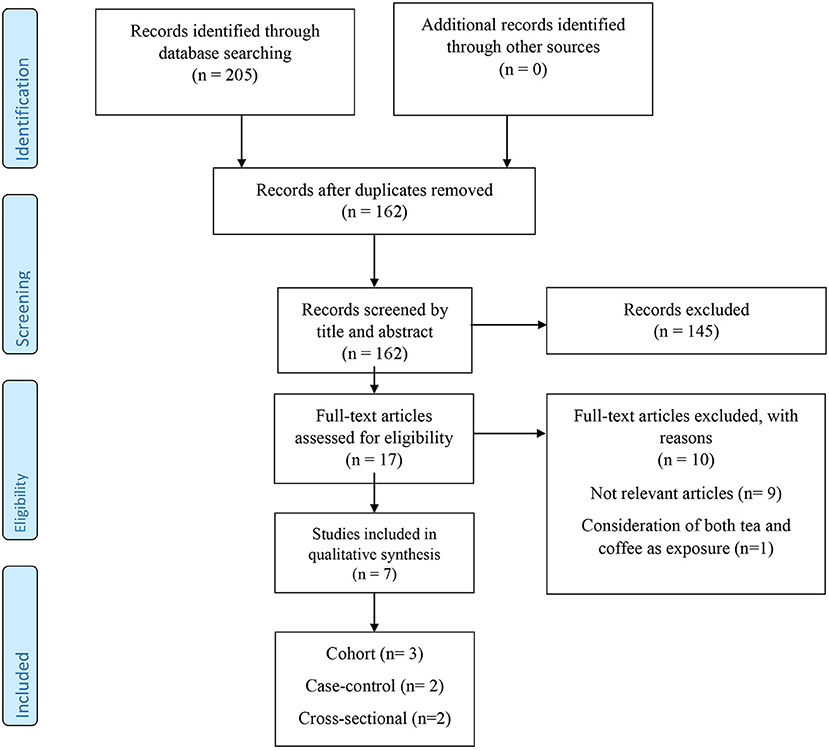
Figure 1. The flow diagram of study selection.
The brief information of each selected study has been described in Table 1. Three cohort studies (18, 19, 30), two case-control studies (20, 22), and two cross-sectional studies (21, 23) were imported to meta-analysis. The studies were published between 2007 and 2021, and these were conducted in the US (18), Denmark (19), Indonesia (22), Oman (20), Spain (21), Malaysia (30), and Ethiopia (23). Women with GDM were aged between 13 and 49 years. A total of 75,607 pregnant women participated, 1,625 of whom were diagnosed with GDM. Three studies used a food frequency questionnaire (FFQ) (18, 21, 30), one 24-h food recall (23), and others used a dietary questionnaire (19, 20, 22). The method of GDM diagnosis was oral glucose tolerance test (OGTT) for four studies (18, 21, 23, 30) and medical records (22) or questionnaire (19, 20) for the others. Four studies controlled the covariates (18, 19, 23, 30), and others did not adjust. Three studies had high-methodological quality (score ≥ 7) (18, 19, 23) (Table 1).
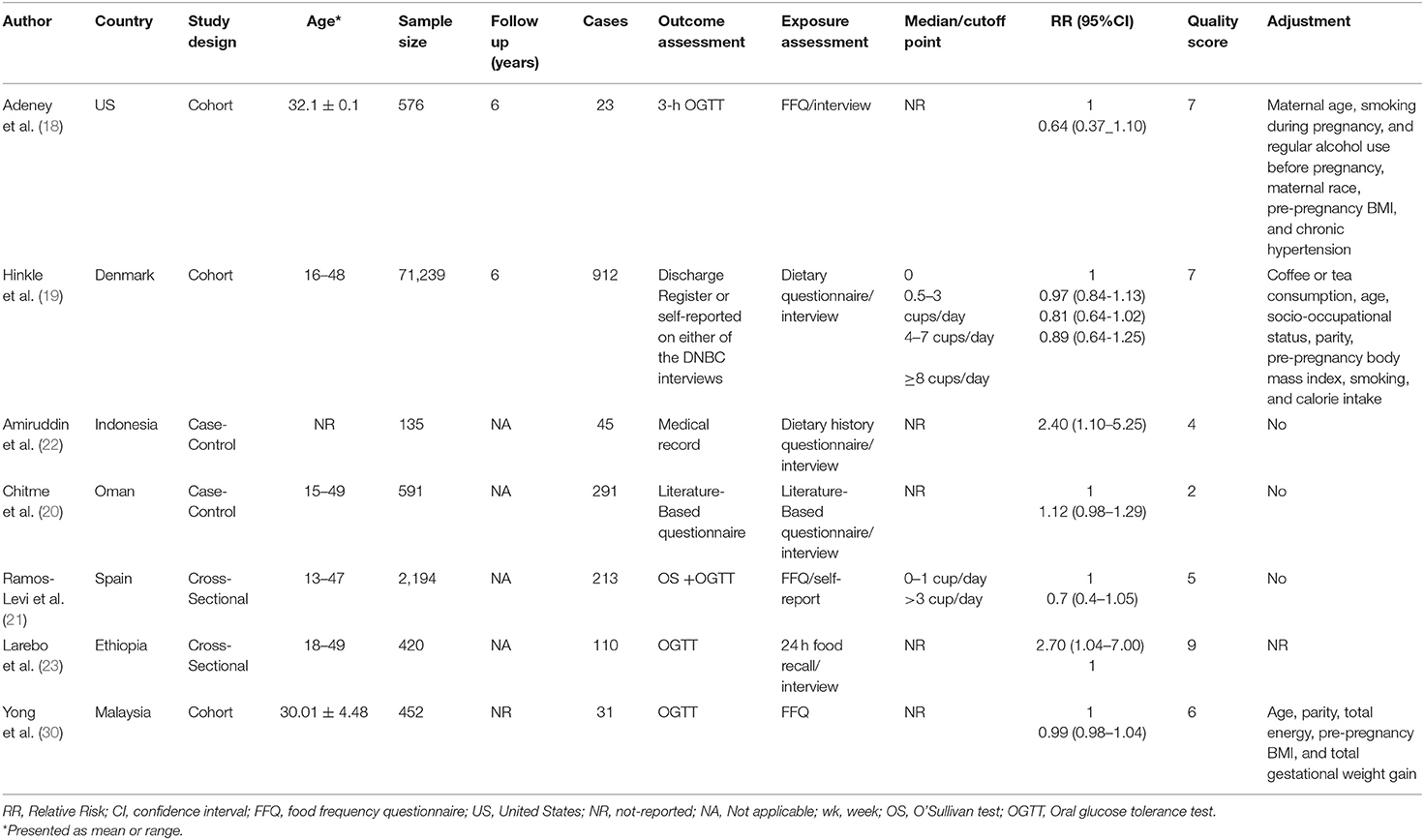
Table 1. Characteristics of included studies on the association between coffee intake and gestational diabetes mellitus.
Meta-Analysis
Three cohorts, two case-control, and two cross-sectional studies were included in the meta-analysis (18–23, 30). When extreme categories were compared, no significant association was detected between intake of coffee and risk of GDM (summarized risk estimate: 0.89; 95% CI: 0.76, 1.05; I2 = 63.4%) (Figure 2). Subgroup analysis found study design, study location, sample size, dietary assessment tool, study quality, adjustment, and controlling for energy and BMI as sources of heterogeneity (Table 2). Furthermore, subgroup analysis showed that consumption of coffee had an inverse relationship with GDM in studies conducted in non-Asia countries (Table 2). Sensitivity analysis was performed to assess the effect of each study on overall effect size (Supplementary Figure 1). A study performed by Amiruddin et al. (22) considered both GDM and prediabetes as the outcome. Therefore, we excluded it and carried out the analysis. No significant association was found (summarized risk estimate: 0.95; 95% CI: 0.83, 1.09; I2 = 53.6%). Furthermore, it seems that studies of Chitme et al. (20) and Yong et al. (30) had an influence on overall effect size. After removing these studies step by step and reanalyzing, we observed that high-coffee intake significantly decreased GDM (summarized risk estimate: 0.75; 95% CI: 0.57, 0.98; I2 = 62.1%), and marginally decline risk of GDM (summarized risk estimate: 0.73; 95% CI: 0.53, 1.02; I2 = 71.6%) compared to women with low intake, respectively. We did not identify the evidence of publication bias by Egger test (P = 0.116) and inspection of funnel plot (Supplementary Figure 2).
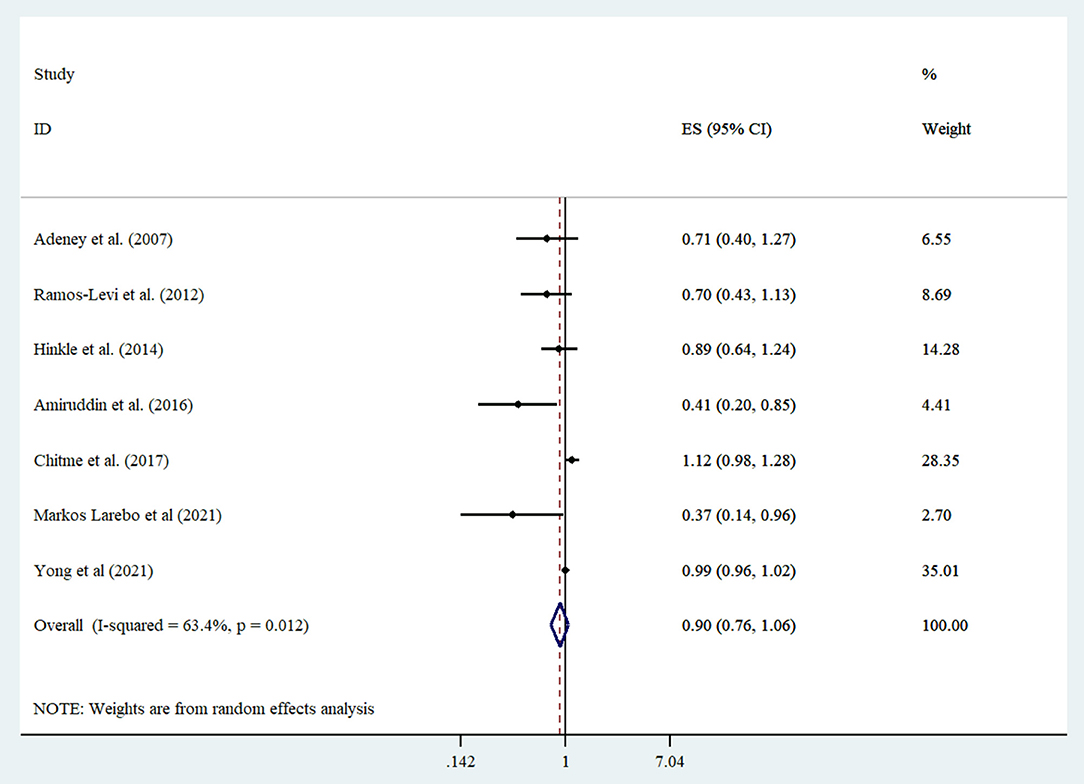
Figure 2. Forest plot derived from random effects meta-analysis of studies investigating the association between high vs. low intake of consumption of coffee and gestational diabetes mellitus. CI, confidence interval; ES, effect size.
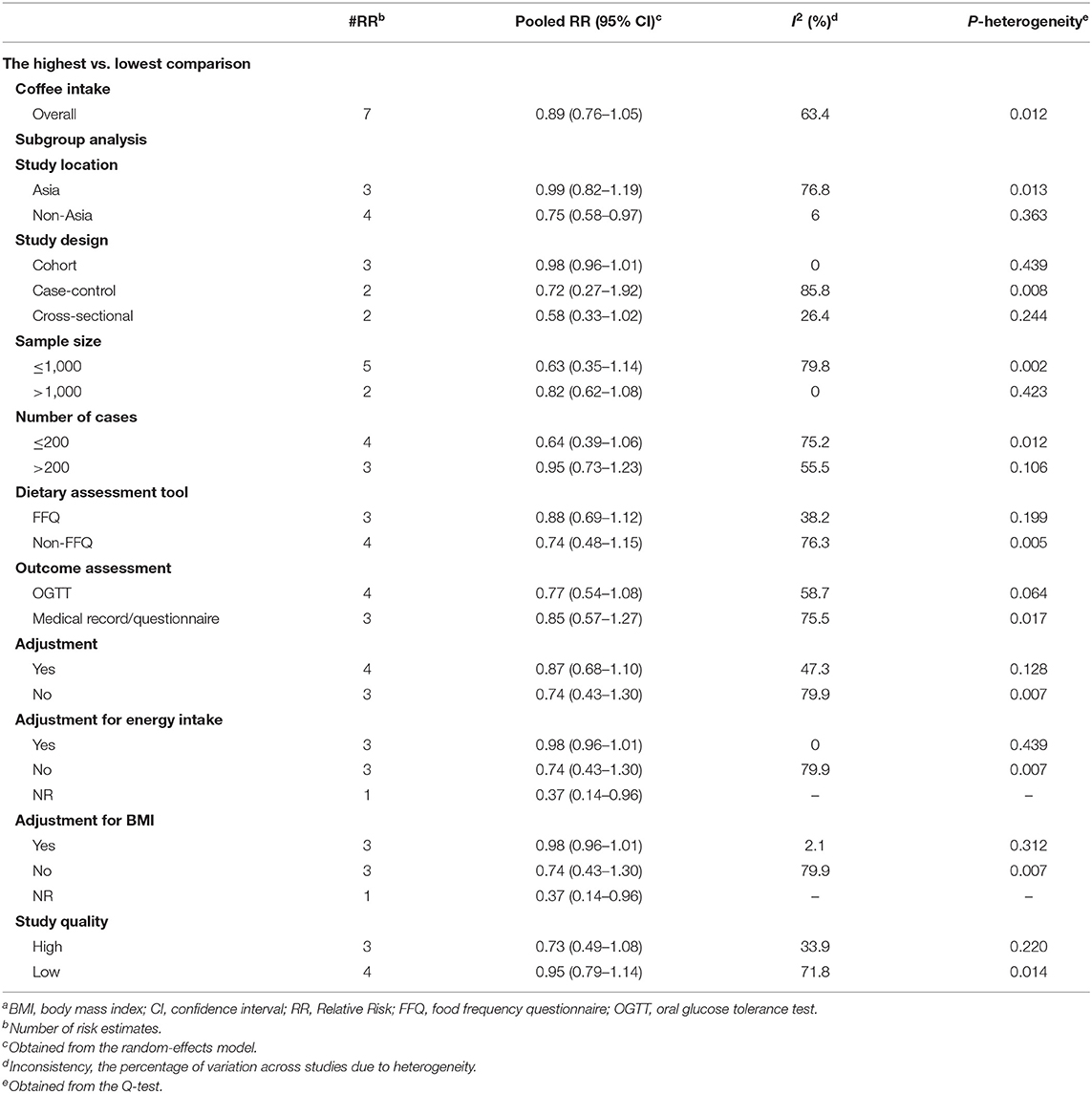
Table 2. Summary risk estimates for the association between coffee consumption and risk gestational diabetes mellitus in subgroup analysisa.
Discussion
This meta-analysis of seven observational studies demonstrated that intake of coffee is not linked with GDM. However, a significant inverse association was indicated between intake of coffee and GDM in studies conducted in non-Asia countries. To date, no systematic review and meta-analysis addressing a correlation between intake of coffee and GDM.
Coffee is a common drink all over the world and consists of a combination of antioxidants and micronutrients, which possess favorable effects on cardiovascular disease (31, 32). In this review, we saw no significant reduced risk of GDM among high-coffee consumers compare to those with low intake. Inline with our finding, a cross-sectional study conducted on 785 adult pregnant women in São Paulo illustrated no association between consumption of coffee and tea and GDM (25). In 2018, one meta-analysis investigated the association of poly-phenol-rich foods and the risk of gestational diabetes. This study captured no connection between non-alcoholic beverages (coffee, tea, and juice) and GDM (33). On the other hand, the evidence shows a relationship between GDM and T2DM, and women with GDM are prone to T2D in the future (7). A recent meta-analysis of 30 cohort studies depicts that the risk of T2D lowered by 6% for each cup-per-day increment in consumption of coffee (34). Furthermore, one cup increase of caffeinated and decaffeinated consumption of coffee in a day leads to a 7 and 6% reduced risk of diabetes, respectively (13). Moreover, a clinical trial study found that intake of caffeine was related to impaired insulin sensitivity in women with GDM early in their third trimester but not in controls without GDM (17).
Some potential reasons can be considered for these inconsistencies. First, intake of caffeine during pregnancy has been related to adverse outcomes including low birth weight, elevated risk of delivering, impaired fetal length growth, and an infant with small-for-gestational-age (35–37). According to the guidelines of the American College of Obstetrics and Gynecology (ACOG), daily intake of up to two cups of moderate-strength coffee may be safe for pregnant women (38). It has been demonstrated that pregnant women significantly decline their intakes of caffeine, particularly coffee during pregnancy (39, 40). The low intake of coffee among pregnant women in the most included studies may explain finding any significant association. This study showed an inverse association between intake of coffee and risk of GDM among pregnant women who lived in the western countries. People in the western countries consume higher coffee as compared with Asia countries. In the United States, about 25% of women aged between 20 and 29 years, and 46% of women aged between 30 and 39 years, drink coffee daily (41).
Furthermore, studies reported the amount of coffee used as “cups” without expressing the volume of the cup. Therefore, the lack of standardization in the measurement of coffee must be taken into account. Besides, coffee is commonly drunk along with sugar, creamer, or milk, which attenuates the beneficial impact of coffee on GDM since fructose worsens hepatic insulin resistance (42). Finally, the degree of roasting and the method of preparation of coffee including coffee-grind setting and brew type may be different in varied populations.
Caffeine and its metabolites such as paraxanthine accumulate in the blood during pregnancy because of a decrease in the metabolism of caffeine (14). High concentrations of coffee and its metabolites have been associated with elevated insulin resistance during pregnancy (15). Therefore, it appears that the favorable effect of coffee on GDM may originate from components of non-caffeine, including micronutrients and phenolic compounds, which have antioxidant and prebiotic traits (16). The evidence indicated that coffee constitutes 60%, or nearly 11.1 mmol, of the total intake of daily antioxidant (43). Chlorogenic acid is the main polyphenol in coffee and is assumed to be the main antioxidant of coffee (44). Coffee also contains potassium, magnesium, niacin, and other antioxidants, which may have beneficial effects on glucose metabolism and insulin resistance (45). Furthermore, habitual intake of coffee declines subclinical inflammation and augments adiponectin levels (46, 47) that may improve insulin sensitivity (48).
This study has some limitations that should be considered once we interpret the findings. First, the small number of studies and a moderate amount of heterogeneity among them are the main limitations. We tried to find the sources of heterogeneity through subgroup analysis. Second, four of the seven included studies have case-control or cross-sectional designs. These kinds of studies possess some biases such as recall and selection biases. Third, measurement errors may occur when estimating consumption of coffee, particularly for those with low intake. Fourth, studies applied different methods for the diagnosis of GDM. Fifth, some studies did not control covariates, or they may ignore to adjust some underlying residual confounding. For example, only three studies controlled energy intake, which is an important risk factor for GDM. Moreover, most studies did not have any information on the intake of coffee of women before pregnancy. Finally, a lack of control for these dietary factors could disable us to identify a firm finding.
In conclusion, this systematic review and meta-analysis of seven observational studies have depicted no relationship between extreme intake of coffee and the risk of GDM. Furthermore, prospective cohort studies with a large sample size are obligatory to understand the relationship between coffee and GDM. Given that, the circulating level of caffeine and its metabolites are different in patients with GDM, future studies are required to examine biomarkers of coffee and its metabolites, including serum caffeine and paraxanthine.
Author Contributions
JN and PW designed the work and extracted the data. TZ and LL analyzed the data. HP wrote the first draft of the manuscript. All authors critically read and approved the final version of the manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
The authors wish to thank Huangshi Central Hospital for their support.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnut.2021.739359/full#supplementary-material
References
1. Gavin JR III, Alberti K, Davidson MB, DeFronzo RA. Report of the expert committee on the diagnosis and classification of diabetes mellitus. Diabetes Care. (1997) 20:1183. doi: 10.2337/diacare.20.7.1183
2. Carr DB, Gabbe S. Gestational diabetes: detection, management, and implications. Clin Diabetes. (1998) 16:4–12.
3. Association AD. Standards of medical care in diabetes-−2010. Diabetes Care. (2010) 33 (Suppl. 1):S11–61. doi: 10.2337/dc10-S011
5. Kim C, Newton KM, Knopp RH. Gestational diabetes and the incidence of type 2 diabetes: a systematic review. Diabetes Care. (2002) 25:1862–8. doi: 10.2337/diacare.25.10.1862
6. Moore TR, Hauguel-De Mouzon S, Catalano P. Diabetes in Pregnancy. Maternal-Fetal Medicine: Principles and Practice. 5th ed. Philadelphia, PA: Saunders (2004). 1023–61p.
7. Lehnen H, Zechner U, Haaf T. Epigenetics of gestational diabetes mellitus and offspring health: the time for action is in early stages of life. Mol Hum Reproduct. (2013) 19:415–22. doi: 10.1093/molehr/gat020
8. Hernandez TL, Van Pelt RE, Anderson MA, Reece MS, Reynolds RM, Becky A, et al. Women with gestational diabetes mellitus randomized to a higher–complex carbohydrate/low-fat diet manifest lower adipose tissue insulin resistance, inflammation, glucose, and free fatty acids: a pilot study. Diabetes Care. (2016) 39:39–42. doi: 10.2337/dc15-0515
9. Moses RG, Barker M, Winter M, Petocz P, Brand-Miller JC. Can a low–glycemic index diet reduce the need for insulin in gestational diabetes mellitus? A randomized trial. Diabetes Care. (2009) 32:996–1000. doi: 10.2337/dc09-0007
10. Sarathi V, Kolly A, Chaithanya HB, Dwarakanath CS. Effect of soya based protein rich diet on glycaemic parameters and thyroid function tests in women with gestational diabetes mellitus. Rom J Diabetes Nutr Metab Dis. (2016) 23:201–8. doi: 10.1515/rjdnmd-2016-0024
11. Daneshzad E, Tehrani H, Bellissimo N, Azadbakht L. Dietary total antioxidant capacity and gestational diabetes mellitus: a case-control study. Oxid Med Cell Longev. (2020) 2020:5471316. doi: 10.1155/2020/5471316
12. Frary CD, Johnson RK, Wang MQ. Food sources and intakes of caffeine in the diets of persons in the United States. J Am Diet Assoc. (2005) 105:110–3. doi: 10.1016/j.jada.2004.10.027
13. Ding M, Bhupathiraju SN, Chen M, van Dam RM, Hu FB. Caffeinated and decaffeinated coffee consumption and risk of type 2 diabetes: a systematic review and a dose-response meta-analysis. Diabetes Care. (2014) 37:569–86. doi: 10.2337/dc13-1203
14. Grosso LM, Bracken MB. Caffeine metabolism, genetics, and perinatal outcomes: a review of exposure assessment considerations during pregnancy. Ann Epidemiol. (2005) 15:460–6. doi: 10.1016/j.annepidem.2004.12.011
15. Laughon SK, Powers RW, Roberts JM, Parana S, Catov J. Caffeine and insulin resistance in pregnancy. Am J Perinatol. (2011) 28:571–8. doi: 10.1055/s-0031-1274511
16. Tunnicliffe JM, Shearer J. Coffee, glucose homeostasis, and insulin resistance: physiological mechanisms and mediators. Appl Physiol Nutr Metab. (2008) 33:1290–300. doi: 10.1139/H08-123
17. Robinson LE, Spafford C, Graham TE, Smith GN. Acute caffeine ingestion and glucose tolerance in women with or without gestational diabetes mellitus. J Obstetr Gynaecol Canada. (2009) 31:304–12. doi: 10.1016/S1701-2163(16)34147-0
18. Adeney KL, Williams MA, Schiff MA, Qiu C, Sorensen TK. Coffee consumption and the risk of gestational diabetes mellitus. Acta Obstetr Gynecol Scand. (2007) 86:161–6. doi: 10.1080/00016340600994992
19. Hinkle SN, Laughon SK, Catov JM, Olsen J, Bech BH. First trimester coffee and tea intake and risk of gestational diabetes mellitus: a study within a national birth cohort. BJOG Int J Obstetr Gynaecol. (2015) 122:420–8. doi: 10.1111/1471-0528.12930
20. Chitme HR, Al Shibli SAS, Al-Shamiry RM. Factors influencing the incidence of gestational diabetes mellitus in omani patients. Int J Nutr Pharmacol Neurol Dis. (2017) 7:1–7. doi: 10.4103/2231-0738.199067
21. Ramos-Leví AM, Pérez-Ferre N, Fernández MD, Del Valle L, Bordiu E, Bedia AR, et al. Risk factors for gestational diabetes mellitus in a large population of women living in Spain: implications for preventative strategies. Int J Endocrinol. (2012) 2012:312529. doi: 10.1155/2012/312529
22. Amiruddin R, Asrianti T, Abdullah MT. Fiber, coffee, cigarette and gestational diabetes mellitus in Makassar Indonesia. Asian J Epidemiol. (2017) 10:26–31. doi: 10.3923/aje.2017.26.31
23. Larebo YM, Ermolo NA. Prevalence and risk factors of gestational diabetes mellitus among women attending antenatal care in hadiya zone public hospitals, southern nation nationality people region. Biomed Res Int. (2021) 2021:5564668. doi: 10.1155/2021/5564668
24. Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. (2015) 4:1. doi: 10.1186/2046-4053-4-1
25. Zuccolotto DCC, Crivellenti LC, Franco LJ, Sartorelli DS. Dietary patterns of pregnant women, maternal excessive body weight and gestational diabetes. Rev Saude Public. (2019) 53:52. doi: 10.11606/S1518-8787.2019053000909
26. Zhang Y, Huang L, Wang D, Ren P, Hong Q, Kang D. The ROBINS-I and the NOS had similar reliability but differed in applicability: a random sampling observational studies of systematic reviews/meta-analysis. J Evid Based Med. (2021) 14:112–22. doi: 10.1111/jebm.12427
27. Marín-Martínez F, Sánchez-Meca J. Weighting by inverse variance or by sample size in random-effects meta-analysis. Educ Psychol Measure. (2010) 70:56–73. doi: 10.1177/0013164409344534
28. Higgins JP, Green S. Cochrane Handbook for Systematic Reviews of Interventions. Chichester; Hoboken, NJ: Wiley-Blackwell (2008). doi: 10.1002/9780470712184
29. Egger M, Smith GD, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. (1997) 315:629–34. doi: 10.1136/bmj.315.7109.629
30. Yong HY, Mohd Shariff Z, Mohd Yusof BN, Rejali Z, Tee YYS, Bindels J, et al. Beverage intake and the risk of gestational diabetes mellitus: the SECOST. Nutrients. (2021) 13:2208. doi: 10.3390/nu13072208
31. Azad BJ, Heshmati J, Daneshzad E, Palmowski A. Effects of coffee consumption on arterial stiffness and endothelial function: a systematic review and meta-analysis of randomized clinical trials. Crit Rev Food Sci Nutr. (2021) 61:1013–26. doi: 10.1080/10408398.2020.1750343
32. Ding M, Bhupathiraju SN, Satija A, van Dam RM, Hu FB. Long-term coffee consumption and risk of cardiovascular disease: a systematic review and a dose-response meta-analysis of prospective cohort studies. Circulation. (2014) 129:643–59. doi: 10.1161/CIRCULATIONAHA.113.005925
33. Pham NM, Van Do V, Lee AH. Polyphenol-rich foods and risk of gestational diabetes: a systematic review and meta-analysis. Euro J Clin Nutr. (2019) 73:647–56. doi: 10.1038/s41430-018-0218-7
34. Carlström M, Larsson SC. Coffee consumption and reduced risk of developing type 2 diabetes: a systematic review with meta-analysis. Nutr Rev. (2018) 76:395–417. doi: 10.1093/nutrit/nuy014
35. Bakker R, Steegers EA, Obradov A, Raat H, Hofman A, Jaddoe VW. Maternal caffeine intake from coffee and tea, fetal growth, and the risks of adverse birth outcomes: the Generation R Study. Am J Clin Nutr. (2010) 91:1691–8. doi: 10.3945/ajcn.2009.28792
36. Chen L-W, Fitzgerald R, Murrin CM, Mehegan J, Kelleher CC, Phillips CM, et al. Associations of maternal caffeine intake with birth outcomes: results from the lifeways cross generation cohort study. Am J Clin Nutr. (2018) 108:1301–8. doi: 10.1093/ajcn/nqy219
37. Van Der Hoeven T, Browne JL, Uiterwaal CS, Van Der Ent CK, Grobbee DE, Dalmeijer GW. Antenatal coffee and tea consumption and the effect on birth outcome and hypertensive pregnancy disorders. PLoS ONE. (2017) 12:e0177619. doi: 10.1371/journal.pone.0177619
38. Obstetricians ACo Gynecologists. Committee Opinion: Moderate Caffeine Consumption During Pregnancy. Obstetricians ACo, Gynecologists (2010).
39. Skreden M, Bere E, Sagedal LR, Vistad I, Øverby NC. Changes in beverage consumption from pre-pregnancy to early pregnancy in the Norwegian fit for delivery study. Public Health Nutr. (2015) 18:1187–96. doi: 10.1017/S136898001400189X
40. Chen L-W, Low YL, Fok D, Han WM, Chong YS, Gluckman P, et al. Dietary changes during pregnancy and the postpartum period in Singaporean Chinese, Malay and Indian women: the GUSTO birth cohort study. Public Health Nutr. (2014) 17:1930–8. doi: 10.1017/S1368980013001730
41. Bowman S, Clemens J, Friday J, Lynch K, Moshfegh A. Department of Agriculture, Food Surveys Research Group; Beltsville, MD, USA:[(Accessed on 14 February 2020)]. Food Pattern Equivalent Database (2013).
42. Ter Horst KW, Schene MR, Holman R, Romijn JA, Serlie MJ. Effect of fructose consumption on insulin sensitivity in nondiabetic subjects: a systematic review and meta-analysis of diet-intervention trials. Am J Clin Nutr. (2016) 104:1562–76. doi: 10.3945/ajcn.116.137786
43. Svilaas A, Sakhi AK, Andersen LF, Svilaas T, Strom EC, Jacobs DR Jr, et al. Intakes of antioxidants in coffee, wine, and vegetables are correlated with plasma carotenoids in humans. J Nutr. (2004) 134:562–7. doi: 10.1093/jn/134.3.562
44. Ranheim T, Halvorsen B. Coffee consumption and human health–beneficial or detrimental?–Mechanisms for effects of coffee consumption on different risk factors for cardiovascular disease and type 2 diabetes mellitus. Mol Nutr Food Res. (2005) 49:274–84. doi: 10.1002/mnfr.200400109
45. Keijzers GB, De Galan BE, Tack CJ, Smits P. Caffeine can decrease insulin sensitivity in humans. Diabetes Care. (2002) 25:364–9. doi: 10.2337/diacare.25.2.364
46. Kempf K, Herder C, Erlund I, Kolb H, Martin S, Carstensen M, et al. Effects of coffee consumption on subclinical inflammation and other risk factors for type 2 diabetes: a clinical trial. Am J Clin Nutr. (2010) 91:950–7. doi: 10.3945/ajcn.2009.28548
47. Williams CJ, Fargnoli JL, Hwang JJ, Van Dam RM, Blackburn GL, Hu FB, et al. Coffee consumption is associated with higher plasma adiponectin concentrations in women with or without type 2 diabetes: a prospective cohort study. Diabetes Care. (2008) 31:504–7. doi: 10.2337/dc07-1952
Keywords: coffee, gestational diabetes mellitus, meta-analysis, systematic review, safety
Citation: Ni J, Wang P, Zheng T, Lv L and Peng H (2021) Consumption of Coffee and Risk of Gestational Diabetes Mellitus: A Systematic Review and Meta-Analysis of Observational Studies. Front. Nutr. 8:739359. doi: 10.3389/fnut.2021.739359
Received: 10 July 2021; Accepted: 16 August 2021;
Published: 20 September 2021.
Edited by:
Mojtaba Heydari, Shiraz University of Medical Sciences, IranReviewed by:
Seyed Hamdollah Mosavat, Shiraz University of Medical Sciences, IranElnaz Daneshzad, Tehran University of Medical Sciences, Iran
Copyright © 2021 Ni, Wang, Zheng, Lv and Peng. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hao Peng, cGVuZ2hhbzE5ODYxMDI0QHNpbmEuY29t
†These authors share first authorship