
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Nutr. , 18 March 2021
Sec. Nutritional Immunology
Volume 8 - 2021 | https://doi.org/10.3389/fnut.2021.649128
This article is part of the Research Topic Coronavirus Disease (COVID-19): Diet, Inflammation and Nutritional Status View all 29 articles
 Hayder M. Al-kuraishy1
Hayder M. Al-kuraishy1 Ali I. Al-Gareeb1
Ali I. Al-Gareeb1 Hani Faidah2Thabat J. Al-Maiahy3
Hani Faidah2Thabat J. Al-Maiahy3 Natália Cruz-Martins4,5,6*
Natália Cruz-Martins4,5,6* Gaber El-Saber Batiha7*
Gaber El-Saber Batiha7*In the face of the Covid-19 pandemic, an intensive number of studies have been performed to understand in a deeper way the mechanisms behind better or worse clinical outcomes. Epidemiologically, men subjects are more prone to severe acute respiratory syndrome-coronavirus type 2 (SARS-CoV-2) infections than women, with a similar scenario being also stated to the previous coronavirus diseases, namely, SARS-CoV in 2003 and Middle East Respiratory Syndrome coronavirus diseases (MERS-CoV) in 2012. In addition, and despite that aging is regarded as an independent risk factor for the severe form of the disease, even so, women protection is evident. In this way, it has been expected that sex hormones are the main determinant factors in gender differences, with the immunomodulatory effects of estrogen in different viral infections, chiefly in Covid-19, attracting more attention as it might explain the case-fatality rate and predisposition of men for Covid-19 severity. Here, we aim to provide a mini-review and an overview on the protective effects of estrogen in Covid-19. Different search strategies were performed including Scopus, Web of Science, Medline, Pubmed, and Google Scholar database to find relative studies. Findings of the present study illustrated that women have a powerful immunomodulating effect against Covid-19 through the effect of estrogen. This study illustrates that estrogens have noteworthy anti-inflammatory and immuno-modulatory effects in Covid-19. Also, estrogen hormone reduces SARS-CoV-2 infectivity through modulation of pro-inflammatory signaling pathways. This study highlighted the potential protective effect of estrogen against Covid-19 and recommended for future clinical trial and prospective studies to elucidate and confirm this protective effect.
Coronavirus disease 19 (Covid-19) is a global pandemic danger caused by the severe acute respiratory syndrome-coronavirus type 2 (SARS-CoV-2). SARS-CoV-2 spike protein binds to angiotensin-converting enzyme 2 (ACE2) receptors (1), which are involved in the viral entry. Such receptors are highly expressed in different tissues, mainly in lung pneumocyte type II cells, with SARS-CoV-2 bindings to ACE2 leading to downregulation of protective ACE2 and induction of hyper-inflammation and oxidative stress, with consequent progress of acute lung injury (ALI) and acute respiratory distress syndrome (ARDS) (2). Also, reduction of ACE2 leads to vasoconstriction, hypertension, coagulopathy, and induction of inflammatory reactions that together increase the risk of ALI and Covid-19 severity (3).
From an epidemiological point of view, and specifically looking at gender differences, men subjects are more prone and vulnerable to SARS-CoV-2 infection than women, about 2.4 times higher due to hormonal differences and expression, as well as distribution of ACE2 (4). Previous coronavirus diseases, including severe acute respiratory syndrome coronavirus (SARS-CoV) in 2003 and the Middle East Respiratory Syndrome coronavirus disease (MERS-CoV) in 2012, showed the same pattern in gender susceptibility. For instance, in SARS-CoV, the case-fatality rate was 22% for men compared to 13% for women, while in MERS-CoV the case-fatality rate was 52% for men compared to 23% for women (5). In SARS-CoV-2, different studies have underlined that females are less prone to infection, contributing for 18% of total Covid-19 cases compared to the affected matched male subjects (6). In United Kingdom, a large-prospective cohort study illustrated that women account for 40% of Covid-19 cases with 20% lower case-fatality rate compared to men (7). However, aging is regarded as an independent risk factor for both genders in the development of severe Covid-19; even so, women protection is still evident (8). In fact, women differ from men in both nutritional requirements and energy consumption based on sex hormone differences. Also, the rate of infection in men compared to women might be due to different other reasons, including the following: men more prevalently work outside the house or work in places that put them to virus exposure; women, due to the low rate of health insurance or other social issues, less frequently go for a test and seek medical attention unless the symptoms are serious. Also, statistical bias in different studies may affect the prevalence and incidence of various infections in regard to gender difference (9). In general, women have a higher immune response against different pathogens due to underlying genetic (two X chromosomes) and hormonal differences (10). The presence of two X chromosomes in women affects the immune system even if one is inactive. The X chromosome acts on various elements of the immune system such as Toll-like receptors (TLRs) and chemokines which can be overexpressed in women and influence the response to viral infections and vaccinations (11). Likewise, the levels of activation of the immune cells affected by sex hormone are higher in women than in males, and this is linked with the stimulation of TLR7 and the production of interferon gamma (INF-γ). Hence, related to the X chromosomes, TLR7 is higher in women than in men and its expression leads to higher immune responses, although these reactions can cause autoimmune phenomena (12). Also, both immunoglobulins and circulating T cells are higher in women compared to men, so that women's immune reactivity is more active against different viral infections, which predispose them for risk of autoimmunity (13). Furthermore, women have an average higher frequency of circulating CD4 T cells than men and clinical studies reveal that men have lower CD3 and CD4 T cell counts, CD4/CD8 T cell ratios, and helper T cell type 1 (Th1) responses than women; thus, cytokine productions in response to infections are enhanced in women compared with men (13).
On the other hand, it has been proposed that pathogen-associated molecular patterns (PAMPs) bind to TLRs. TLR2 and TLR4 which bind bacterial cell wall proteins are more evident in men compared to TLR3, TLR7, and TLR9 which bind viral proteins in women (14). Thus, the production of interferon (mediated by TLR7) and IL-10 (mediated by TLR9) are lower in men during viral infections (15, 16). Also, women tend to activate type 2 immune response, which engaged with the production of anti-inflammatory cytokines, while men tend to activate type 1 immune response, which are involved in the production of pro-inflammatory cytokines (17). Taken together, men subjects have a lower level of regulatory T cells (Treg) during cytomegalovirus infections compared to women, suggesting a propensity for activation of type 1 immune response in men with production of pro-inflammatory cytokines (18, 19). Different studies have documented that sex steroids are the main determinant factors in gender immune differences mainly at the reproductive age (20), with the immunomodulatory effects of estrogen, progesterone, and androgen in different viral infections, chiefly in Covid-19, attracting more attention as it might explain the case-fatality rate and men's predisposition for Covid-19 severity, since serum concentrations of sex hormones change across life span (21). Here, we aim to provide an overview on the gender-specific immunological profile and the protective effects of estrogen in Covid-19.
The literature and study search were performed according to the guideline of systemic review. We search PubMed, Scopus, Web of Science, and Google Scholar database by using sequence keywords including (SARS-CoV-2 OR Covid-19) AND (acute respiratory syndrome OR acute lung injury), (SARS-CoV-2 OR Covid-19) AND (Gender differences OR hormonal effects), (SARS-CoV-2 OR Covid-19) AND (Estrogen OR estrogen agonists), (SARS-CoV-2 OR Covid-19) AND (women OR men), and (SARS-CoV-2 OR Covid-19) AND (immunological differences OR Covid-19 manifestations). The literature search was organized independently by all authors throughout searching the titles and abstracts of regained articles. All of the published and preprinted studies were integrated in this study without limitation of languages. Following the preliminary search and screening, the selected articles were experienced for eligibility and summarized in a mini-review (Figure 1).
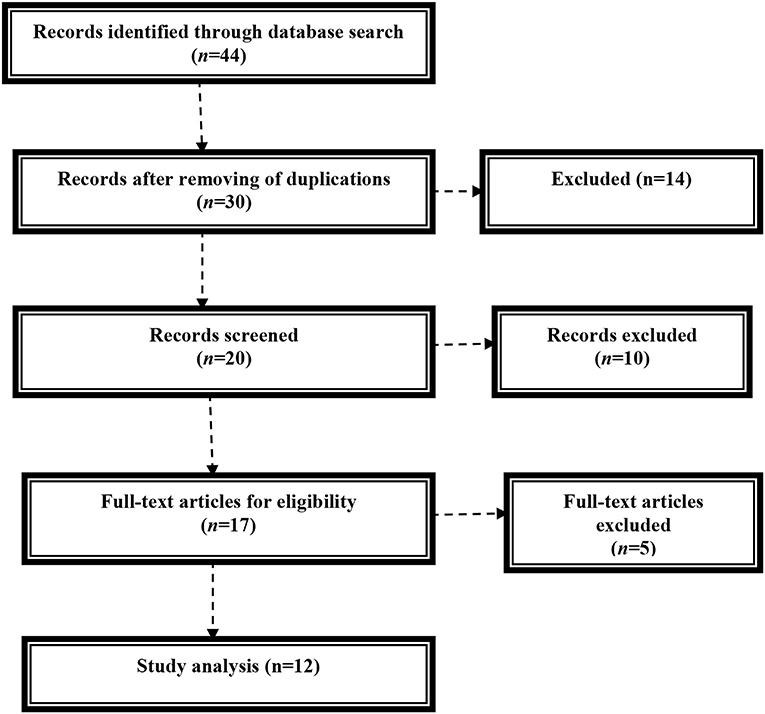
Figure 1. Consort flowchart of the present study.
Estradiol (E2) binds to the cytoplasmic estrogenic receptors (ER-α and ER-β) that are expressed on T cells and B cells, respectively (22). Momentarily, E2 activates humoral immunity and antibody production against different viral infections (23). High E2 concentration is correlated with immune-reactivity around ovulation (24). Both hormone replacement therapy after menopause and use of combined contraceptive pills produce a similar potent immune response and protection against viral infections (25). Besides, progesterone and testosterone have immunosuppressive effects on cell-mediated response and innate immunity. However, progesterone inhibits type 1 immune response as well as cytotoxic T and natural kill cells with activation of type 2 immune response, and this might explain the association between the use of progestin-only contraceptive depot and the risk of human immune deficiency virus (HIV) (26). Ruggieri et al. (27) found the association between testosterone use and the risk of viral infections including hepatitis C and B due to suppression of T cells and production of interferon gamma (IFN-γ). E2 has potent anti-inflammatory and immunomodulation effects in both humans and animals. E2 inhibits innate immunity through suppression of immune cell migration, mainly neutrophils and monocytes to the inflamed area. This effect attenuates the development and progression of cytokine storm (CS) via inhibition of pro-inflammatory cytokine release (i.e., IL-1β, IL-6, IL-17, TNF-α, and chemokines) (28). CS is regarded as a major cause for the development of ALI, ARDS, multiorgan failure, and death in Covid-19 (29). In addition, physiological E2 activates the production of anti-inflammatory cytokines (IL-4, IL-10) and promotes immune tolerance through stimulation of CD4 and regulatory T cells (Treg), although low dose of E2 promotes pro-inflammatory activation (30). However, Bommer et al. (31) showed that higher E2 concentration during pregnancy inhibits the anti-inflammatory IL-10 without effect on the pro-inflammatory profile. In Covid-19, a higher circulating Treg and anti-inflammatory cytokines have been linked to a rapid recovery and good clinical outcomes (32). In fact, a case–control study by Neumann et al. (33) proposed that higher IL-10-producing Treg cells are linked to Covid-19 severity. However, high IL-10-producing Treg cells might be a compensatory mechanism to overcome high pro-inflammatory cytokines (34). In addition, E2 inhibits the synthesis and release of IL-6 in different acute and chronic inflammatory disorders, like ALI by inhibiting IL-6 (35). Indeed, IL-6 antagonist tocilizumab is an effective agent in the ARDS management of Covid-19, suggesting the critical role of IL-6 in ALI pathogenesis and Covid-19 severity (36). Experimental studies have shown that lipopolysaccharide (LPS)-induced ALI and high IL-6 levels are higher in ovariectomized female and male mice (37).
Different clinical studies documented the protective role through various pathways. In Italy, the case-fatality rate is higher in men at about 63.9% compared with affected women due to hormonal changes and lifestyle diversity (38). Shabbir et al.'s (39) observational study involved 162,392 Covid-19 patients which showed that 74% of affected patients were men compared to 26% women due to the protective effect of estrogen. Moreover, Garg et al. (40) revealed that the mortality rate was higher in postmenopausal (12.8%) compared with premenopausal women (8.6%), highlighting the protective role of estrogen against Covid-19.
On the other hand, it has been reported that endogenous E2 leads to significant pulmonary protection against influenza and SARS viruses in previous preclinical studies through anti-inflammatory effects. Also, the use of fulvestrant (ER full antagonist) in women increases the risk of SARS-induced ALI comparable to men, suggesting of a potential lung-protective effect of endogenous estrogen (41). Likewise, selective estrogen receptor modulators (SERMs), like tamoxifen and toremifene, have noteworthy protective effects against ALI in SARS-CoV and MERS-CoV. Also, these drugs have antiviral effects against different coronaviruses through inhibition of viral entry and replication, along with cytopathic effects (42). Specifically, tamoxifen blocks the mitochondrial complex and oxygen consumption of infected cells through activation of AMPK signaling. In addition, endogenous estrogen and SERMs modulate the SARS-CoV-2 binding to the entry point ACE2 (43). Since SARS-CoV has a higher similarity with SARS-CoV-2, thus estrogen may be an effective agent against Covid-19-induced ARDS. Therefore, the net effects of estrogen on the inflammatory profile during SARS-CoV-2 are summarized (Figure 2).
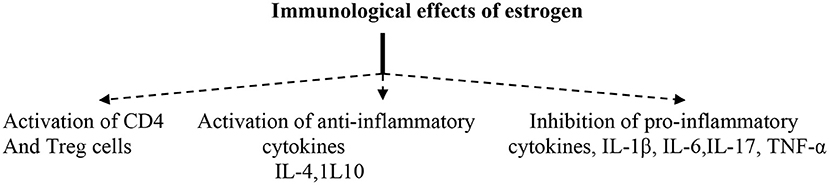
Figure 2. Immunological effects of estrogens.
The renin–angiotensin system (RAS) is highly deteriorated during SARS-CoV-2 infection, as SARS-CoV-2 spike protein binds to ACE2, leading to a significant downregulation of protective ACE2. ACE2 is involved in the metabolism and conversion of angiotensin I (Ang I) to Ang1–9 and Ang II to Ang1–7. Both Ang1–9 and Ang1–7 have protective effects, exerting anti-inflammatory, anti-apoptotic, and anti-fibrotic effects through activation of Mas receptors (Figure 3) (45). Therefore, reduction and downregulation of ACE2 by SARS-CoV-2 lead to an elevation of vasoconstrictor Ang II causing vasoconstriction, hypertension, and induction of inflammatory and pro-inflammatory activations. A high Ang II concentration is directly linked to ALI and ARDS in Covid-19, so that both angiotensin-converting enzyme inhibitors (ACEIs) and angiotensin receptor blockers (ARBs) are able to reduce the harmful effect of Ang II on the lung through ACE2 upregulation (44).
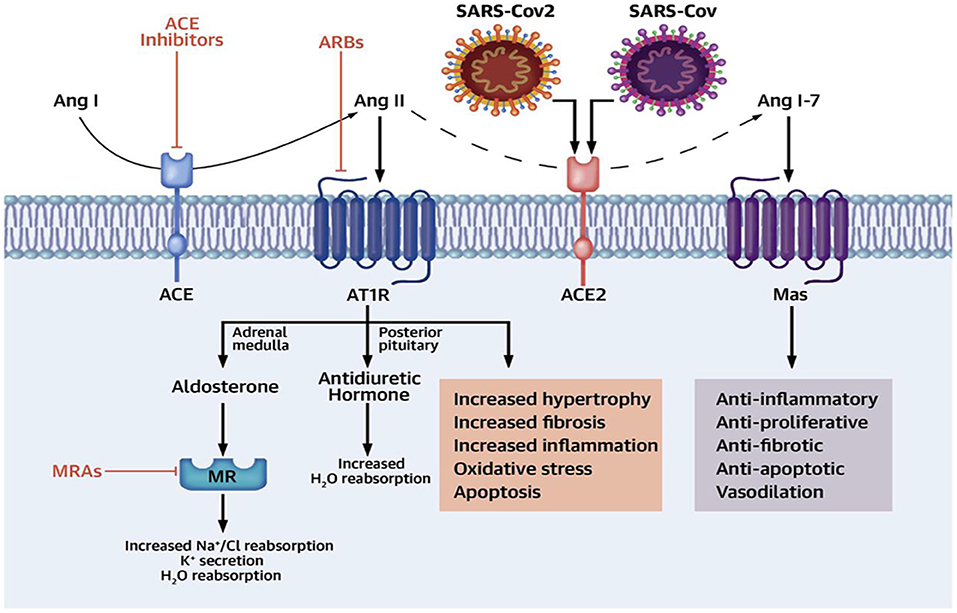
Figure 3. Renin–angiotensin system (RAS) and SARS-CoV-2 infection [adopted from Yehualashet et al. (44)].
It has been reported that E2 increases the expression of ACE2 and production of Ang1-7 (46) so it may counteract the deleterious effect of high Ang II-induced-ALI and ARDS. Tao et al. (47) confirmed the association between high Ang II concentration and ALI in mice. Thereby, estrogen therapy may have an important step in the management of Covid-19 patients. Shabbir et al. (39) illustrated that estrogen therapy mitigates endoplasmic reticulum stress (ER) induced by SARS-CoV-2 invasion through activation of cellular unfold protein response and regulation of inositol triphosphate (IP3) and phospholipase C. Baran-Gale et al. (48) reported that E2 inhibits type II transmembrane protease serine (TMPRSS2), necessary for trimming and activation of SARS-CoV-2 spike protein to bind ACE2. Indeed, it has been reported that TMPRSS2 inhibitors, such as camostat and nafamostat, block SARS-CoV-2 entry, mainly in lung cells (49). Different studies have also illustrated that E2 increases the expression of A Disintegrin And Metalloproteinase (ADAMs) mainly ADAM-17, which is involved in cleaving of the ACE2 ectodomain, leading to high-circulating soluble ACE2 that neutralizes SARS-CoV-2 and prevents its binding to the ACE2 membrane (50). Thus, E2 reduces SARS-CoV-2 infectivity through modulation of cellular ACE2/TMPRSS2/ADAM-17 axis expression.
The Covid-19 severity is linked to the activation of inflammasomes, which are multi-protein complexes that control the activation of pro-inflammatory cytokines through intracellular caspase-1. The nod-like receptor pyrin domain 3 (NLRP3) is the most common inflammasome engaged with immunity against different pathogens (51). Raut et al. (52) illustrated that estrogen therapy inhibits the activation of NLRP3 inflammasomes, so E2 ameliorates airway inflammation and hyper-responsiveness through inhibition of NLRP3 inflammasome-induced proinflammatory cytokine release (53), therefore attenuating the SARS-CoV-2-induced hyper-inflammation and ALI.
Furthermore, protease dipeptidyl peptidase 4 (DPP4) is also regarded as an entry point for SARS-CoV-2 and linked to viral pathogenesis and hyper-inflammation. Besides, DPP4 inhibitors mitigate SARS-CoV-2 infections and reduce the mortality in severe Covid-19 patients (54). It has been shown that E2 by ER-α inhibits DPP4 gene transcription through suppression of NF-kB signaling (55), and for that reason, high E2 levels in women may reduce DPP4 expression in lung and adipose tissues, thereby lessening the infectivity and pathogenicity of SARS-CoV-2.
Moreover, the active site of DPP4 (CD26) contains adenosine deaminase (ADA) which is involved in the metabolism of adenosine to inosine. Adenosine has anti-inflammatory and immunosuppressive effects and can protect against ALI and ARDS development (56). Therefore, ADA inhibitors, such as pentostatin, may have a role in preventing and attenuating SARS-CoV-2 infection and associated hyper-inflammation in the late phase of Covid-19 (57). Mohamadi et al. (58) illustrated that E2 through ER-α activates adenosine receptors, so that estrogen might be of value in repressing ALI and ARDS in the late phase of Covid-19 through modulation of the DPP4/CD26/adenosine signaling pathway.
Moreover, the receptor for advanced glycation end products (RAGE) is a member of immunoglobulin superfamily proteins, present in two forms, membrane RAGE (mRAGE) and soluble RAGE (sRAGE). mRAGE has inflammatory effects through activation of NF-kB, while sRAGE has anti-inflammatory effects through upregulation of ACE2 and anti-inflammatory cytokines. The RAGE pathway is mainly expressed in lung tissue and linked to development of acute and chronic lung injuries (59). In Covid-19, SARS-CoV-2 activates mRAGE at pulmonary alveolar cells leading to induction of severe inflammatory reactions (60). Indeed, it has been reported that sRAGE concentration is reduced with aging, which might explain the susceptibility of the elderly to Covid-19. However, in young and asymptomatic Covid-19 patients, the sRAGE concentration is high, while in severe Covid-19, the sRAGE level is significantly reduced, and so a low sRAGE level is linked to the development of ALI and ARDS (61). Finally, it has been shown that estrogen modulates the RAGE pathway through upregulation of sRAGE and reduction of mRAGE (62), so that the administration of E2 in patients with severe Covid-19 may have a lung-protective effect through modulation of the lung RAGE signaling pathway (Figure 4).
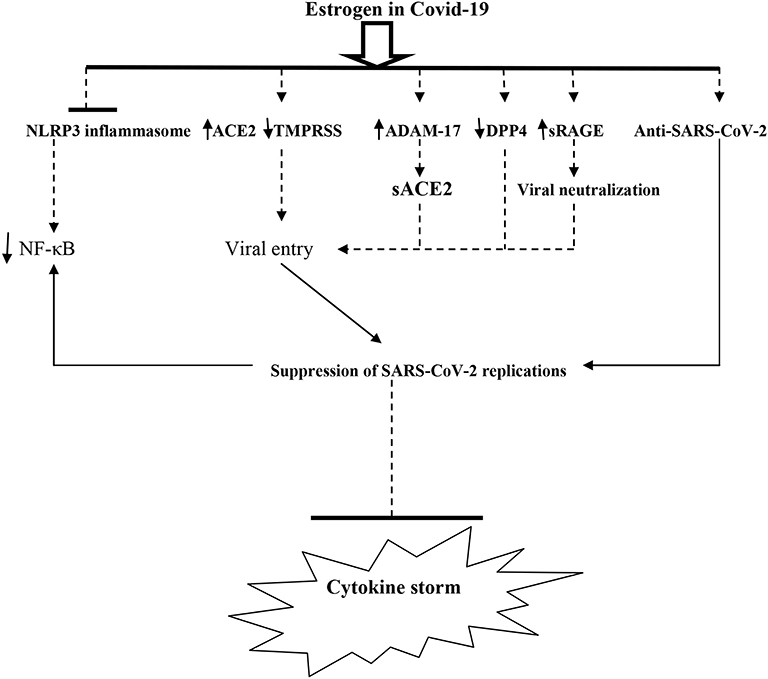
Figure 4. The potential role of estrogen against SARS-CoV-2 pathogenesis and cytokine storm. TMPRRSS, type II transmembrane protease serine; ADAMA-17, A Disintegrin And Metalloproteinase-17; DPP4, Dipeptidyl Peptidase 4; sRAGE, soluble receptor for advanced glycation end-Product; sACE2, soluble angiotensin-converting enzyme 2.
From the above, the diverse effects of estrogen on SARS-CoV-2 genome replication and associated immunological response in Covid-19 favor the hypothesis of an interplayed action among SARS-CoV-2 infection, immune response, and estrogen hormone which determine and regulate the gender-dependent final outcomes of Covid-19. Up to date, available data on the precise mechanisms determining the diverse predisposition and outcomes of SARS-CoV-2 infection, either hormonal or immunological, are fragmented and not comprehensive, but the disclosure in order to ascertain gender-specific molecular pathways involved is hopeful. Therefore, emergence of future clinical trials and large-scale prospective studies are warranted in this regard to confirm the supreme importance of estrogen therapy in the management of Covid-19 mainly in postmenopausal women.
This study illustrates that estrogens have noteworthy anti-inflammatory and immunomodulation effects in Covid-19. Also, estrogen hormone reduces SARS-CoV-2 infectivity through modulation of pro-inflammatory signaling pathways. This study highlighted the potential protective effect of estrogen against Covid-19 and recommended for future clinical trials and prospective studies to elucidate and confirm this protective effect.
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
NC-M acknowledges the Portuguese Foundation for Science and Technology under the Horizon 2020 Program (PTDC/PSI-GER/28076/2017). HA-k acknowledges medical staff members of Al-Shiffa Medical Center, Baghdad, Iraq for their participations.
1. Al-Kuraishy HM, Al-Naimi MS, Lungnier CM, Al-Gareeb AI. Macrolides and COVID-19: an optimum premise. Biomed Biotechnol Res J. (2020) 4:189. doi: 10.4103/bbrj.bbrj_103_20
2. Al-Kuraishy HM, Hussien NR, Al-Naimi MS, Al-Buhadily AK, Al-Gareeb AI, Lungnier C. Is ivermectin–Azithromycin combination the next step for COVID-19?. Biomed Biotechnol Res J. (2020) 4:101. doi: 10.4103/bbrj.bbrj_109_20
3. Al-Kuraishy HM, Hussien NR, Al-Naimi MS, Al-Buhadily AK, Al-Gareeb AI, Lungnier C. Renin–Angiotensin system and fibrinolytic pathway in COVID-19: One-way skepticism. Biomed Biotechnol Res J. (2020) 4:33. doi: 10.4103/bbrj.bbrj_105_20
4. Conti P, Younes A. Coronavirus COV-19/SARS-CoV-2 affects women less than men: clinical response to viral infection. J Biol Regul Homeost Agents. (2020) 34:339–43.
5. Ahmadzadeh J, Mobaraki K, Mousavi SJ, Aghazadeh-Attari J, Mirza-Aghazadeh-Attari M, Mohebbi I. The risk factors associated with MERS-CoV patient fatality: a global survey. Diagn Microbiol Infect Dis. (2020) 96:114876. doi: 10.1016/j.diagmicrobio.2019.114876
6. Wu Y, Lin H, Xie Q, Chen Q, Huang Y, Zhu Y, et al. COVID-19 in a patient with pre-existing acute lymphoblastic leukaemia. Br J Haematol. (2020) 190:e13–5. doi: 10.1111/bjh.16799
7. Perez-Guzman PN, Daunt A, Mukherjee S, Crook P, Forlano R, Kont MD, et al. Clinical characteristics and predictors of outcomes of hospitalized patients with coronavirus disease 2019 in a multiethnic London national health service trust: a retrospective cohort study. Clin Infect Dis. (2020) 7:1–1. doi: 10.1093/cid/ciaa1091
8. Klein SL, Dhakal S, Ursin RL, Deshpande S, Sandberg K, Mauvais-Jarvis F. Biological sex impacts COVID-19 outcomes. PLoS Pathogens. (2020) 16:e1008570. doi: 10.1371/journal.ppat.1008570
9. Sun C, Zhai Z. The efficacy of social distance and ventilation effectiveness in preventing COVID-19 transmission. Sustain Cities Soc. (2020) 62:102390. doi: 10.1016/j.scs.2020.102390
10. Quakkelaar ED, Melief CJ. Experience with synthetic vaccines for cancer and persistent virus infections in nonhuman primates and patients. Adv Immunol. (2012) 114:77–106. doi: 10.1016/B978-0-12-396548-6.00004-4
11. Souyris M, Cenac C, Azar P, Daviaud D, Canivet A, Grunenwald S, et al. TLR7 escapes X chromosome inactivation in immune cells. Sci Immunol. (2018) 3:eaap8855. doi: 10.1126/sciimmunol.aap8855
12. Scully EP, Haverfield J, Ursin RL, Tannenbaum C, Klein SL. Considering how biological sex impacts immune responses and COVID-19 outcomes. Nat Rev Immunol. (2020) 20:442–7. doi: 10.1038/s41577-020-0348-8
13. Meester I, Rivera-Silva GF, González-Salazar F. Immune system sex differences may bridge the gap between sex and gender in fibromyalgia. Front Neurosci. (2020) 13:1414. doi: 10.3389/fnins.2019.01414
14. Roberts BJ, Dragon JA, Moussawi M, Huber SA. Sex-specific signaling through Toll-like receptors 2 and 4 contributes to survival outcome of Coxsackievirus B3 infection in C57Bl/6 mice. Biol Sex Diff. (2012) 3:1–3. doi: 10.1186/2042-6410-3-25
15. Pratap UP, Hima L, Kannan T, Thyagarajan C, Priyanka HP, Vasantharekha R, et al. Sex-based differences in the cytokine production and intracellular signaling pathways in patients with rheumatoid arthritis. Arch Rheumatol. (2020) 35:545–57. doi: 10.46497/ArchRheumatol.2020.7481
16. Moore SE, Voss JG, Webel AR. Sex-based differences in plasma cytokine concentrations and sleep disturbance relationships among people living with HIV. J Assoc Nurs AIDS Care. (2020) 31:249–54. doi: 10.1097/JNC.0000000000000125
17. Bouman A, Schipper M, Heineman MJ, Faas MM. Gender difference in the non-specific and specific immune response in humans. Am J Reprod Immunol. (2004) 52:19. doi: 10.1111/j.1600-0897.2004.00177.x
18. Taneja V. Sex hormones determine immune response. Front Immunol. (2018) 9:1931. doi: 10.3389/fimmu.2018.01931
19. van der Heiden M, Berbers GA, Fuentes S, van Zelm MC, Boots AM, Buisman AM. An explorative biomarker study for vaccine responsiveness after a primary meningococcal vaccination in middle-aged adults. Front Immunol. (2018) 8:1962. doi: 10.3389/fimmu.2017.01962
20. Foo YZ, Nakagawa S, Rhodes G, Simmons LW. The effects of sex hormones on immune function: a meta-analysis. Biol Rev. (2017) 92:551–71. doi: 10.1111/brv.12243
21. Khan D, Ansar Ahmed S. The immune system is a natural target for estrogen action: opposing effects of estrogen in two prototypical autoimmune diseases. Front Immunol. (2016) 6:635. doi: 10.3389/fimmu.2015.00635
22. Tecalco-Cruz AC, Pérez-Alvarado IA, Ramírez-Jarquín JO, Rocha-Zavaleta L. Nucleo-cytoplasmic transport of estrogen receptor alpha in breast cancer cells. Cell Signal. (2017) 34:121–32. doi: 10.1016/j.cellsig.2017.03.011
23. Littauer EQ, Skountzou I. Hormonal regulation of physiology, innate immunity and antibody response to H1N1 influenza virus infection during pregnancy. Front Immunol. (2018) 9:2455. doi: 10.3389/fimmu.2018.02455
24. Aguilar-Pimentel JA, Cho YL, Gerlini R, Calzada-Wack J, Wimmer M, Mayer-Kuckuk P, et al. Increased estrogen to androgen ratio enhances immunoglobulin levels and impairs B cell function in male mice. Sci Rep. (2020) 10:1–4. doi: 10.1038/s41598-020-75059-9
25. Graham JH, Yoachim SD, Gould KA. Estrogen receptor alpha signaling is responsible for the female sex bias in the loss of tolerance and immune cell activation induced by the lupus susceptibility locus Sle1b. Front Immunol. (2020) 11:582214. doi: 10.3389/fimmu.2020.582214
26. Curtis KM, Hannaford PC, Rodriguez MI, Chipato T, Steyn PS, Kiarie JN. Hormonal contraception and HIV acquisition among women: an updated systematic review. BMJ Sex Reprod Health. (2020) 46:8–16. doi: 10.1136/bmjsrh-2019-200509
27. Ruggieri A, Gagliardi MC, Anticoli S. Sex-dependent outcome of hepatitis B and C viruses infections: synergy of sex hormones and immune responses?. Front Immunol. (2018) 9:2302. doi: 10.3389/fimmu.2018.02302
28. AbdulHussain G, Azizieh F, Makhseed MA, Raghupathy R. Effects of progesterone, dydrogesterone and estrogen on the production of Th1/Th2/Th17 cytokines by lymphocytes from women with recurrent spontaneous miscarriage. J Reprod Immunol. (2020) 140:103132. doi: 10.1016/j.jri.2020.103132
29. Ragab D, Salah Eldin H, Taeimah M, Khattab R, Salem R. The COVID-19 cytokine storm; what we know so far. Front Immunol. (2020) 11:1446. doi: 10.3389/fimmu.2020.01446
30. Maglione A, Rolla S, Mercanti SF, Cutrupi S, Clerico M. The adaptive immune system in multiple sclerosis: an estrogen-mediated point of view. Cells. (2019) 8:1280. doi: 10.3390/cells8101280
31. Bommer I, Muzzio DO, Zygmunt M, Jensen F. Progesterone and estradiol exert an inhibitory effect on the production of anti-inflammatory cytokine IL-10 by activated MZ B cells. J Reprod Immunol. (2016) 116:113–6. doi: 10.1016/j.jri.2016.05.008
32. Liu Y, Qi G, Bellanti JA, Moser R, Ryffel B, Zheng SG. Regulatory T cells: a potential weapon to combat COVID-19?. MedComm. (2020) 1:157–64. doi: 10.1002/mco2.12
33. Neumann J, Prezzemolo T, Vanderbeke L, Roca CP, Gerbaux M, Janssens S, et al. An open resource for T cell phenotype changes in COVID-19 identifies IL-10-producing regulatory T cells as characteristic of severe cases. medRxiv [Preprint]. (2020). doi: 10.1101/2020.05.31.20112979
34. Brinkhoff A, Sieberichs A, Engler H, Dolff S, Benson S, Korth J, et al. Pro-inflammatory Th1 and Th17 cells are suppressed during human experimental endotoxemia whereas anti-inflammatory IL-10 producing T-cells are unaffected. Front Immunol. (2018) 9:1133. doi: 10.3389/fimmu.2018.01133
35. Hsieh YC, Frink M, Hsieh CH, Choudhry MA, Schwacha MG, Bland KI, et al. Downregulation of migration inhibitory factor is critical for estrogen-mediated attenuation of lung tissue damage following trauma-hemorrhage. Am J Physiol Lung Cell Mol Physiol. (2007) 292:L1227–32. doi: 10.1152/ajplung.00479.2006
36. Scherger S, Henao-Martínez A, Franco-Paredes C, Shapiro L. Rethinking interleukin-6 blockade for treatment of COVID-19. Med Hypotheses. (2020) 144:110053. doi: 10.1016/j.mehy.2020.110053
37. Speyer CL, Rancilio NJ, McClintock SD, Crawford JD, Gao H, Sarma JV, et al. Regulatory effects of estrogen on acute lung inflammation in mice. Am J Physiol Cell Physiol. (2005) 288:C881–90. doi: 10.1152/ajpcell.00467.2004
38. Froldi G, Dorigo P. Endothelial dysfunction in coronavirus disease (2019). (COVID-19): gender and age influences. Med Hypotheses. (2020) 144:110015. doi: 10.1016/j.mehy.2020.110015
39. Shabbir S, Hafeez A, Rafiq MA, Khan MJ. Estrogen shields women from COVID-19 complications by reducing ER stress. Med Hypotheses. (2020) 143:110148. doi: 10.1016/j.mehy.2020.110148
40. Garg R, Agrawal P, Gautam A, Pursnani N, Agarwal M, Agarwal A, et al. COVID-19 outcomes in postmenopausal and perimenopausal females: is estrogen hormone attributing to gender differences? J Midlife Health. (2020) 11:250. doi: 10.4103/jmh.jmh_287_20
41. Breithaupt-Faloppa AC, Correia CD, Prado CM, Stilhano RS, Ureshino RP, Moreira LF. 17β-Estradiol, a potential ally to alleviate SARS-CoV-2 infection. Clinics. (2020) 75L:e1980. doi: 10.6061/clinics/2020/e1980
42. Almosawey HA, AL-Khikani FH, Hameed RM, Abdullah YJ, Al-Ibraheemi MK, Al-Asadi AA. Tamoxifen from chemotherapy to antiviral drug: possible activity against COVID-19. Biomed Biotechnol Res J. (2020) 4:108.
43. Vatansev H, Kadiyoran C, Cure MC, Cure E. COVID-19 infection can cause chemotherapy resistance development in patients with breast cancer and tamoxifen may cause susceptibility to COVID-19 infection. Med Hypotheses. (2020) 143:110091. doi: 10.1016/j.mehy.2020.110091
44. Yehualashet AS, Belachew TF. ACEIs and ARBs and their correlation with COVID-19: a review. Infect Drug Resist. (2020) 13:3217. doi: 10.2147/IDR.S264882
45. Danser AJ, Epstein M, Batlle D. Renin-angiotensin system blockers and the COVID-19 pandemic: at present there is no evidence to abandon renin-angiotensin system blockers. Hypertension. (2020) 75:1382–5. doi: 10.1161/HYPERTENSIONAHA.120.15082
46. Mompeón A, Lázaro-Franco M, Bueno-Betí C, Pérez-Cremades D, Vidal-Gómez X, Monsalve E, et al. Estradiol, acting through ERα, induces endothelial non-classic renin-angiotensin system increasing angiotensin 1–7 production. Mol Cell Endocrinol. (2016) 422:1–8. doi: 10.1016/j.mce.2015.11.004
47. Tao W, Li PS, Xu G, Luo Y, Shu YS, Tao YZ, et al. Soluble epoxide hydrolase plays a vital role in angiotensin II-induced lung injury in mice. Shock. (2018) 50:589–94. doi: 10.1097/SHK.0000000000001067
48. Baran-Gale J, Purvis JE, Sethupathy P. An integrative transcriptomics approach identifies miR-503 as a candidate master regulator of the estrogen response in MCF-7 breast cancer cells. RNA. (2016) 22:1592–603. doi: 10.1261/rna.056895.116
49. Rahman N, Basharat Z, Yousuf M, Castaldo G, Rastrelli L, Khan H. Virtual screening of natural products against Type II transmembrane serine protease (TMPRSS2), the priming agent of coronavirus 2 (SARS-CoV-2). Molecules. (2020) 25:2271. doi: 10.3390/molecules25102271
50. Ragia G, Manolopoulos VG. Assessing COVID-19 susceptibility through analysis of the genetic and epigenetic diversity of ACE2-mediated SARS-CoV-2 entry. Pharmacogenomics. (2020) 21:1311–29. doi: 10.2217/pgs-2020-0092
51. Rodrigues TS, de Sá KS, Ishimoto AY, Becerra A, Oliveira S, Almeida L, et al. Inflammasomes are activated in response to SARS-CoV-2 infection and are associated with COVID-19 severity in patients. J Exp Med. (2021) 218:e20201707. doi: 10.1084/jem.20201707
52. Raut PK, Kim SH, Choi DY, Jeong GS, Park PH. Growth of breast cancer cells by leptin is mediated via activation of the inflammasome: critical roles of estrogen receptor signaling and reactive oxygen species production. Biochem Pharmacol. (2019) 161:73–88. doi: 10.1016/j.bcp.2019.01.006
53. Cheng C, Wu H, Wang M, Wang L, Zou H, Li S, et al. Estrogen ameliorates allergic airway inflammation by regulating activation of NLRP3 in mice. Biosci Rep. (2019) 39:BSR20181117. doi: 10.1042/BSR20181117
54. Du H, Wang DW, Chen C. The potential effects of DPP-4 inhibitors on cardiovascular system in COVID-19 patients. J Cell Mol Med. (2020) 24:10274–8. doi: 10.1111/jcmm.15674
55. Bruzzese L, Fromonot J, By Y, Durand-Gorde JM, Condo J, Kipson N, et al. NF-κB enhances hypoxia-driven T-cell immunosuppression via upregulation of adenosine A2A receptors. Cell Signal. (2014) 26:1060–7. doi: 10.1016/j.cellsig.2014.01.024
56. Köhler D, Streißenberger A, Morote-García JC, Granja TF, Schneider M, Straub A, et al. Inhibition of adenosine kinase attenuates acute lung injury. Crit Care Med. (2016) 44:e181. doi: 10.1097/CCM.0000000000001370
57. Geiger JD, Khan N, Murugan M, Boison D. Possible role of adenosine in COVID-19 pathogenesis and therapeutic opportunities. Front Pharmacol. (2020) 11:594487. doi: 10.3389/fphar.2020.594487
58. Mohamadi A, Aghaei M, Panjehpour M. Estrogen stimulates adenosine receptor expression subtypes in human breast cancer MCF-7 cell line. Res Pharm Sci. (2018) 13:57. doi: 10.4103/1735-5362.220968
59. Dozio E, Sitzia C, Pistelli L, Cardani R, Rigolini R, Ranucci M, et al. Soluble receptor for advanced glycation end products and its forms in COVID-19 patients with and without diabetes mellitus: a pilot study on their role as disease biomarkers. J Clin Med. (2020) 9:3785. doi: 10.3390/jcm9113785
60. Yalcin Kehribar D, Cihangiroglu M, Sehmen E, Avci B, Capraz A, Yildirim Bilgin A, et al. The receptor for advanced glycation end product (RAGE) pathway in COVID-19. Biomarkers. (2020) 26:114–8. doi: 10.1080/1354750X.2020.1861099
61. De Francesco EM, Vella V, Belfiore A. COVID-19 and diabetes: the importance of controlling RAGE. Front Endocrinol. (2020) 11:526. doi: 10.3389/fendo.2020.00526
Keywords: Covid-19, estrogen, angiotensin converting enzyme-2, SARS-CoV-2, patients outcomes
Citation: Al-kuraishy HM, Al-Gareeb AI, Faidah H, Al-Maiahy TJ, Cruz-Martins N and Batiha G-S (2021) The Looming Effects of Estrogen in Covid-19: A Rocky Rollout. Front. Nutr. 8:649128. doi: 10.3389/fnut.2021.649128
Received: 03 January 2021; Accepted: 15 February 2021;
Published: 18 March 2021.
Edited by:
Ioannis Zabetakis, University of Limerick, IrelandReviewed by:
Markus Xie, Genentech, United StatesCopyright © 2021 Al-kuraishy, Al-Gareeb, Faidah, Al-Maiahy, Cruz-Martins and Batiha. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Natália Cruz-Martins, bmNtYXJ0aW5zQG1lZC51cC5wdA==; Gaber El-Saber Batiha, Z2FiZXJiYXRpaGFAZ21haWwuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.