 Simone Bösch
Simone Bösch Lucinda Westerman
Lucinda Westerman Nina Renshaw2
Nina Renshaw2 Igor Pravst
Igor Pravst- 1SICABO Consulting, London, United Kingdom
- 2NCD Alliance, Geneva, Switzerland
- 3Nutrition and Public Health Research Group, Nutrition Institute, Ljubljana, Slovenia
COVID-19 has brought to center stage the most important health issue of our era, largely ignored by policymakers and the public to date: non-communicable diseases (NCDs), the cause of 71% of deaths per year worldwide. People living with NCDs, and particularly those living with cardiovascular disease (CVD), are at higher risk of severe symptoms and death from COVID-19. As a result, the urgent need for policy measures to protect cardiovascular health is more apparent than ever. One example of “low-hanging fruit” in the prevention of CVD is the elimination of industrially-produced trans fatty acids (iTFA). Their removal from the global food supply could prevent up to 17 million deaths by 2040 and would be the first time an NCD risk factor has been eliminated.
Introduction
COVID-19 has illustrated the importance of public health and disease prevention measures, not only for infectious diseases, but also for NCD prevention and care. It is now recognized that COVID-19 and NCDs, often referred to as “underlying conditions,” are deeply linked. It is estimated that 1.7 billion people worldwide are at an increased risk of severe COVID-19 should they become infected, mostly as a result of living with one or more NCDs (1). These vulnerabilities include diet-related NCDs such as CVD and type 2 diabetes which are to a large extent preventable. The deadly interplay of NCDs, inequities and COVID-19 has illuminated the need to respond to the current crisis by breaking down silos and addressing interlinkages as a syndemic [formed from “syn-” = together and (epi)demic].
The Syndemic of COVID-19 and NCDs
COVID-19 and NCDs interact to form a syndemic—parallel epidemics of health problems which interact synergistically, have intertwined risk factors and mutually enhance each other against a background of shared social and economic inequalities (2). The COVID-19 pandemic is occurring against the backdrop of a steadily rising NCD burden. NCDs are the leading cause of mortality worldwide with 41 million deaths annually, of which 32 million occur in low- and middle-income countries (LMICs) and 18 million are due to CVD (2, 3). NCDs and COVID-19 share factors which influence health-seeking behavior, health decision-making, access to healthcare and other services, and risk exposure: poverty, discrimination, cultural norms and gender (4).
NCDs and infectious diseases have often been addressed in silos, yet their interlinkages are well-known (5). Infectious diseases can be a risk factor for several NCDs, such as HIV and chlamydia for CVD (6), while NCDs increase the susceptibility to and disease severity of infectious diseases. NCDs were a predictor of disease severity for Middle East Respiratory Syndrome (MERS) and Severe Acute Respiratory Syndrome (SARS) (7, 8). Consequently, the 2018 High-Level Political Declaration on NCDs (9) called for the integration of responses to NCDs and infectious diseases.
COVID-19 has also worsened the obesogenic environment by limiting opportunities for physical activity and decreasing food quality for many, thus negatively impacting two of the main NCD risk factors (10, 11). Access to fresh food has become more limited for many. Lockdown measures and a decline in purchasing power increase reliance on cheap foods and foods with a long shelf life, both of which are often ultra-processed and unhealthy. In many countries, consumers have been targeted with new, unhealthy offerings by the food industry, with marketing messages tailored to exploit the pandemic context (12). Decreased dietary quality may persist even after COVID-19 is under control due to economic pressures in the pandemic's aftermath (10–14).
COVID-19—A Historic Opportunity to Scale Up Health-Promoting Policy Measures
The interlinkage between infectious diseases, health emergencies and NCDs has brought about an unprecedented acknowledgment and visibility of the urgent need to address the ever-growing NCD burden. Unchecked, NCDs cause social and economic harm that far exceeds the damage caused by COVID-19. COVID-19 presents a historic imperative to prioritize and invest in public health by adopting health-promoting policy measures, including iTFA elimination. These measures must also address modifiable risk factors—including nutrition, hypertension and obesity—that drive both COVID-19 and the NCD burden.
Population groups of lower socio-economic status tend to consume higher amounts of iTFA and are therefore at higher risk of iTFA-attributable CVD. iTFA elimination can thus help reduce both CVD mortality and morbidity as well as health inequalities (15–18).
Nutrition Policy to Address the Modifiable Risk Factors of NCDs
Currently, almost all countries are off-track to achieve the World Health Organization's target of reducing overall mortality from the four main NCDs—CVD, cancers, diabetes, and chronic respiratory diseases—by 25% by 2025 (19), and Sustainable Development Goal 3.4 to reduce premature mortality from NCDs by a third by 2030 (20, 21). Implementing strong nutrition policies will save lives, accelerate progress toward these global NCD targets, and build healthier, more equitable and resilient populations that are better prepared to deal with future health emergencies.
Nutrition policy interventions are one of the reasons high-income countries have managed to reduce CVD deaths by more than 25% since 2000 (22). Conversely, LMICs largely have yet to introduce comprehensive CVD prevention policies and bear up to 90% of the global CVD burden (23), underscoring the need to extend iTFA elimination strategies globally. This is particularly relevant in countries where Universal Health Coverage (UHC) does not yet exist, or is weak, and where primary prevention strategies such as nutrition policies can support the feasibility and sustainability of UHC.
Regulations such as mandatory iTFA limits link political will to health policy and demonstrate government commitment to addressing population health. Their adoption signals that a government is prepared to invest appropriately in public health, creates a level playing field for industry, and is a strong signal to society that a healthy diet and diet-related NCDs must be taken seriously.
What are Trans Fats?
Trans fatty acids, or trans fats, are unsaturated fatty acids of either natural or artificial origin. Naturally occurring trans fats are produced by bacteria in the gut of ruminants; dairy and meat products derived from them contain small amounts of trans fats. iTFA are created in an industrial process that adds hydrogen to vegetable oil (hydrogenation) to produce partially hydrogenated oils (PHO), which are solid or semi-solid fats.
Globally, most iTFA is consumed through PHO which are common in baked goods, pre-packaged foods and some cooking oils. iTFA have no known health benefit and are a contributor to CVD worldwide, estimated to cause around 260,000 deaths and 6,162,986 disability-adjusted life years (DALYs) annually (24). Trans fat consumption increases the risk of death from any cause by 34% and from coronary heart disease (CHD) by 28% (25). For every 1% increase in daily energy obtained from trans fats, CHD mortality raises by 12% (18). iTFA intake has also been associated with an increased risk for other NCDs and related conditions such as ovarian cancer (26), infertility, endometriosis, Alzheimer's disease, diabetes and obesity (27, 28).
iTFA consumption induces low-grade systemic inflammation and is positively associated with endothelial dysfunction (a non-obstructive coronary artery disease without blockages of heart arteries, but with the large blood vessels of the hearts surface constricting instead of dilating) (29–33). Low-grade systematic inflammation, a higher concentration of pro-inflammatory cytokines and endothelial dysfunction are also induced by overweight and obesity which are metabolic risk factors for diet-related NCDs, and particularly for heart disease (34, 35). This is relevant in the context of COVID-19 which is a disease that triggers pro-inflammatory cytokines. Patients with severe COVID-19 frequently show cytokine storms, an excessive and uncontrolled release of pro-inflammatory cytokines; cytokine storms are an indicator for poor prognosis of COVID-19 (34, 36).
WHO recommends that total trans fat intake does not exceed 1% of total energy intake, which translates to >2.2 g/day for a 2,000-calorie diet (37).
iTFA can be replaced in foods with healthier fats and oils containing polyunsaturated (preferred) or monounsaturated fats without impacting their consistency and taste (38).
Benefits of iTFA Elimination
Worldwide iTFA elimination could save 17 million lives by 2040 (39). Countries that have eliminated iTFA from their food supply have seen substantial health benefits:
• Argentina: iTFA elimination is associated with an estimated annual 1.3–6.3% reduction in CHD events (40).
• Denmark: In the 3 years following the implementation of an iTFA limit in 2004, CVD mortality decreased 3.2% in relation to comparable countries without iTFA regulation (41).
• England and Wales: iTFA elimination across the two countries is estimated to result in around 1,600 fewer deaths and 4,000 fewer hospital admissions per year (18).
• New York: Counties in the state of New York with iTFA restrictions saw 7.8% fewer hospital admissions for heart attacks between 2007 and 2013 than counties without iTFA restrictions (42).
The prevention of death and disease attributable to iTFA consumption lessens the burden on health systems, which is particularly important for health facilities overwhelmed by the COVID-19 response and where treatment services for CVD and other NCDs have been disrupted.
The economic value of investing in global iTFA elimination has not been calculated but local estimates demonstrate the intervention's cost-effectiveness.
• Argentina: iTFA elimination would save US$17-87 million annually in costs associated with the management of CHD complications and follow-up. These cost savings include implementation costs of the policy incurred by the Ministry of Health, but do not include other economic costs (e.g., lost productivity due to CVD) (40).
• Australia: iTFA elimination would save AU$80 million (US$60 million) in healthcare costs related to ischemic heart disease during the first 10 years and AU$538 (US$407 million) over the population lifetime. Policy costs would near AU$22 million (US$17 million) during the first 10 years and AU$56 million (US$42 million) over the population lifetime, mostly consisting of monitoring costs to government (17).
• European Union: Prior to adopting a mandatory 2% iTFA limit, the European Union estimated that phasing out iTFA would result in direct and indirect cost savings of €58–304 billion (US$68–358 billion) over 85 years (16).
• United Kingdom: One study found that iTFA regulation in England would result in cost savings of around £297 million (US$379 million), consisting of £42 million (US$54 million) in direct healthcare costs, £196 million (US$250 million) in informal care costs, and £59 million (US$75 million) in averted productivity loss over 5 years. Considering implementation costs to government and industry, net cost savings would range from £64–264 million (US$82–337 million) (15). Another study calculated that mandatory iTFA elimination in England and Wales over a 10-year period would bring cost savings of £755 million to £1.54 billion (US$965 million to US$1.97 billion), comprising £95–201 million (US$121–257 million) in direct healthcare costs, £368–727 million (US$470–929 million) in informal care costs, and £292–613 million (US$373–783 million) in averted productivity loss (18).
• United States: The removal of PHO over a 20-year time interval is estimated to result in net benefits of US$130 billion. The analysis included lives saved and non-fatal illnesses prevented as benefits, and as costs product reformulation and relabelling, increased costs of substitute ingredients, costs to consumers from changing recipes, reduced product acceptances, shorter product shelf life, and restaurants and bakeries learning how to operate without PHO (43).
WHO deems iTFA elimination a cost-effective and feasible intervention (a so-called “best buy” policy measure), recommended for implementation by all countries to prevent NCDs (44).
WHO's REPLACE Initiative
To support national governments to reach the goal of global iTFA elimination by 2023, WHO launched the REPLACE initiative in May 2018. The REPLACE action package (45) provides governments with evidence-based tools across six strategic areas to eliminate iTFA from their national food supply (see Figure 1). REPLACE is the first global initiative to eliminate an NCD risk factor. In September 2020, WHO announced a certification scheme which will recognize countries that achieve iTFA elimination, similar to the WHO certification scheme for polio eradication (47). Countries must show that they have implemented a best-practice iTFA policy and that effective monitoring and enforcement is in place to qualify for certification (48). This initiative is the first time that WHO has introduced certification to recognize government's achievements in addressing a modifiable NCD risk factor.
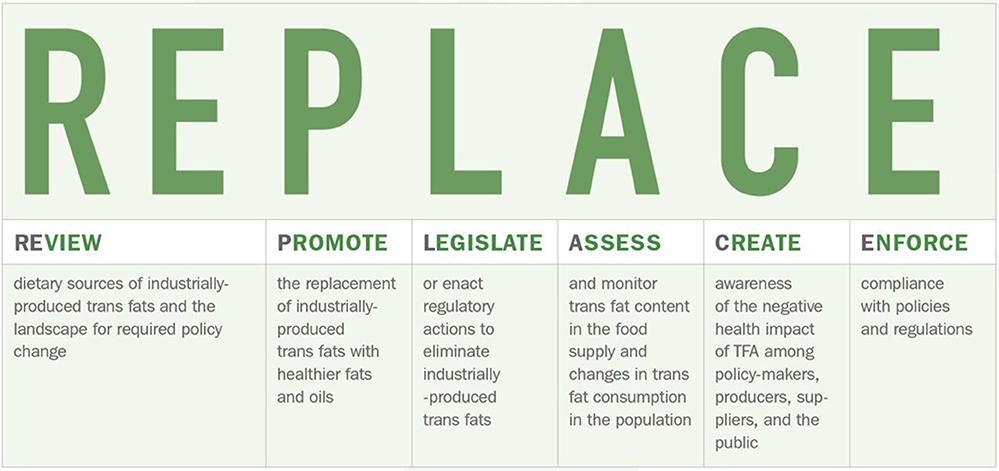
Figure 1. The six areas of WHO's REPLACE action package to eliminate iTFA (46).
3.2 Billion People will be Protected by iTFA Policies by 2021 but Over 100 Countries Have Yet to Act
Substantial progress has been made in the last 10 years to remove iTFA from the global food supply. To date, 32 countries have enacted laws and regulations that currently protect 2.4 billion people from this harmful substance. Another 26 countries have passed laws and regulations that will come into effect in the next 2 years, covering a further 815 million people. Encouragingly, an increasing number of countries are introducing best practice policies, which include setting a compulsory limit of 2 g of iTFA per 100 g of total fat/oil in all foods and/or banning PHO (the main source of iTFA). While in 2010 only two countries had a best practice policy in effect, this number has risen to 14 by 2020 and will reach 40 by 2022 (49). These developments show that adopting legal instruments to limit iTFA or ban PHO is politically, economically, and technically feasible (50).
Regional approaches to iTFA elimination have also progressed. Member States of the Pan American Health Organization (PAHO, WHO's Americas region) unanimously approved a Regional Plan of Action to Eliminate Industrially Produced Trans-Fatty Acids 2020–2025 (51), the first of its kind globally. Regional regulations include the European Union's 2% iTFA limit for all foods adopted in 2019 (52), a Gulf Cooperation Council standard limiting iTFA to 2% for fats and oils and 5% for other foods in 2015 (53), and the Eurasian Economic Union's 2% iTFA limit for oils and fats adopted in 2015 (54). Such regulatory approaches have the added benefit of spill-over effects, forcing countries surrounding these regions to consider iTFA elimination policies to allow for continued trade in foods.
However, over 100 countries have yet to act, and of the 15 countries with the highest proportion of CHD deaths due to trans fat intake, only four (Canada, Latvia, Slovenia, and USA) have introduced regulations to remove iTFA from their food supply. Ten countries (Azerbaijan, Bangladesh, Bhutan, Ecuador, Egypt, Iran, Mexico, Nepal, Pakistan, and Republic of Korea) have yet to do so, while India is on track for a best practice policy (49).
Countries with comparatively low iTFA intake and associated mortality also benefit from adopting iTFA regulations. Introducing regulation is a preventive measure to avoid increasing intakes of iTFA and associated health risks in the future, and to guard against food manufacturers increasing sales of iTFA-containing foods (“dumping”) in unregulated markets. Additionally, average iTFA intake levels at national level may conceal high iTFA exposure levels in pockets of the population—regulation ensures that health disparities due to iTFA intake are minimized. And implementation of iTFA regulation is easier and cheaper when national levels of iTFA are low, also presenting an opportunity to strengthen regulatory capacity and systems in food safety (55).
Disparities in protection from iTFA also persist. Most laws and regulations have been adopted in high-income or upper-middle-income countries in Europe and the Americas. No low- or lower-middle-income country has implemented a best practice policy to date, resulting in geographic and socio-economic inequalities (49). This is particularly worrying given that CVD associated mortality is higher in LMICs than high-income countries (56).
Mandatory Regulation is Preferable to Voluntary Commitments to Phase Out iTFA
In 2019, member organizations of the International Food & Beverage Alliance (IFBA) committed to limit iTFA to 2 g per 100 g fat/oil in their food products worldwide by 2023 and to reformulation without increasing the content of saturated fat (57). It will be important that adherence to and impact of these commitments is independently and transparently monitored and evaluated.
In the 2008 Trans Fat Free Americas Declaration (58), backed by PAHO, representatives of Latin America's major food companies (including some IFBA members), cooking oil companies and industry associations, together with delegates of national public health authorities, committed to a 2% iTFA limit in oils and margarines and a 5% limit in other foods.
These voluntary efforts, however, only cover a small percentage of packaged foods worldwide (49), and the food industry and suppliers of oils and fats have generally been slow to voluntarily phase out iTFA. Many large food producers have replaced iTFA with healthier fats in products sold to high-income countries—many of which have regulated iTFA—while resisting the replacement of iTFA in LMICs (49, 59).
Food industry and oil and fat suppliers may be reluctant to phase out iTFA for fear of competitors moving into the market if regulation is absent to create a level playing field. Additionally, compliance with voluntary commitments cannot be enforced by governments. Research shows that voluntary approaches are less effective than mandatory regulation in reducing iTFA content in foods (28, 60). Therefore, compulsory regulation combined with strong enforcement mechanisms is recommended over voluntary schemes.
iTFA Elimination Should be Embedded in a Comprehensive Policy Approach
Diet is one of the key modifiable risk factors to address underlying conditions of severe COVID-19. Therefore, including iTFA elimination in a comprehensive policy approach to improve the food environment will address both NCDs and the ongoing pandemic. It will also improve preparedness for and resilience to future pandemics, as a healthier population with a lower prevalence of NCDs is less susceptible to infections and better equipped to fight them.
In addition to iTFA regulation, a comprehensive policy package to prevent diet-related NCDs should comprise mandatory food labeling (ingredient lists, nutrient panels declaring trans fats, interpretative front-of-pack labeling based on nutrient profiles, rules on nutrient and health claims), restrictions on food marketing aimed at children and adolescents, mandatory standards for healthy school food, limits on salt/sodium content (61), and nutrition standards for public procurement. These policy measures can be accompanied by public awareness campaigns to educate consumers on healthy nutrition.
At the healthcare level, policy actions should include preventative measures such as blood pressure checks and hypertension control (62), weight-management support and nutrition counseling.
Additionally, taxing unhealthy foods and beverages alongside alcohol and tobacco—and removing any market-distorting subsidies—would reduce their intake and, in some cases, incentivize reformulation while mobilizing domestic revenue, which could be invested in health system strengthening and Universal Health Coverage. Such investments would not only contribute to future health, but also pandemic preparedness and health systems' resilience. Notably, if used progressively, such revenue would benefit poorer households and help tackle poverty and inequality. For example, raising the price of sugar-sweetened beverages, alcohol, and tobacco by 50% could raise around US$24.7 billion in 54 LMICs by 2030 (63).
Conclusion
Including iTFA elimination alongside a comprehensive policy approach including food policy, healthcare and taxation strategies—many of them WHO “best buys”—in recovery packages will strengthen global health systems, as compared to pre-pandemic levels. Using these population-wide primary prevention strategies in the COVID-19 response will serve as a stepping stone to tackle the world's biggest killer, cardiovascular disease; support economic recovery from the pandemic; and increase health security by making future generations more resilient to infectious diseases.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Author Contributions
This perspectives paper was conceived and written by SB. NR, LW, and IP reviewed the manuscript. All authors read and approved the final manuscript.
Funding
The development of the manuscript was supported through a grant to the NCD Alliance from Resolve to Save Lives, an initiative of Vital Strategies.
Conflict of Interest
SB consults for both the NCD Alliance and Resolve to Save Lives. NR and LW are employees of NCD Alliance. IP led and participated in various research projects in the area of nutrition, public health, and food technology, including a project “Trans fats in foods,” funded by the Slovenian Research Agency, Ministry of Health of the Republic of Slovenia, and food businesses.
Acknowledgments
The authors are grateful to Dr. Laura Cobb and Lindsay Steele (Resolve to Save Lives) and Ana Larrañaga (Salud Crítica, Mexico) for input to a policy brief which served as basis for this perspective paper.
References
1. Clark A, Jit M, Warren-Gash C, Guthrie B, Wang HHX, Mercer SW, et al. Global, regional, and national estimates of the population at increased risk of severe COVID-19 due to underlying health conditions in 2020: a modeling study. Lancet. (2020) 8:e1003–17. doi: 10.1016/S2214-109X(20)30264-3
2. Bambra C, Riordan R, Ford J, Matthews F. The COVID-19 pandemic and health inequalities. J Epidemiol Community Health. (2020) 74:964–8. doi: 10.1136/jech-2020-214401
3. World Health Organization. Noncommunicable Diseases: Key Facts. Geneva. (2018). Available online at: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (accessed November 17, 2020).
4. World Health Organization and the United Nations Development Programme. Responding to Non-Communicable Diseases During and Beyond the COVID-19 Pandemic. (2020). Available online at: https://www.undp.org/content/undp/en/home/librarypage/hiv-aids/responding-to-non-communicable-diseases-during-and-beyond-the-co.html (accessed November 17, 2020).
5. NCD Alliance. Briefing Note: Impacts of COVID-19 on People Living With NCDs. (2020). Available online at: https://ncdalliance.org/sites/default/files/resource_files/COVID-19_%26_NCDs_BriefingNote_27April_FinalVersion_0.pdf (accessed November 17, 2020).
6. Ogoina D, Onyemelukwe GC. The role of infections in the emergence of non-communicable diseases (NCDs): compelling needs for novel strategies in the developing world. J Infect Public Health. (2009) 2:14–29. doi: 10.1016/j.jiph.2009.02.001
7. Centers for Disease Control and Prevention. About MERS: Symptoms & Complications. (2019). Available online at: https://www.cdc.gov/coronavirus/mers/about/index.html (accessed November 17, 2020).
8. Lu L, Zhong W, Bian Z, Li Z, Zhang K, Liang B, et al. A comparison of mortality-related risk factors of COVID-19, SARS, and MERS: a systematic review and meta-analysis. J Infect. (2020) 81:e18–25. doi: 10.1016/j.jinf.2020.07.002
9. United Nations Digital Library. Resolution A/RES/73/2. Political declaration of the 3rd High-Level Meeting of the General Assembly on the Prevention and Control of Non-Communicable Diseases. (2018). Available online at: https://digitallibrary.un.org/record/1648984?ln=en (accessed November 17, 2020).
10. Ammar A, Brach M, Trabelsi K, Chtourou H, Boukhris O, Masmoudi L, et al. Effects of COVID-19 home confinement on eating behaviour and physical activity: results of the ECLB-COVID19 international online survey. Nutrients. (2020) 12:1583. doi: 10.3390/nu12061583
11. Mattioli AV, Sciomer S, Cocchi C, Maffei S, Gallina S. Quarantine during COVID-19 outbreak: changes in diet and physical activity increase the risk of cardiovascular disease. Nutr Metabol Cardiovasc Dis. (2020) 30:1409–17. doi: 10.1016/j.numecd.2020.05.020
12. Collin J, Ralston R, Hill SE, Westerman L. Signalling Virtue, Promoting Harm: Unhealthy commodity industries and COVID-19. NCD Alliance, SPECTRUM. (2020). Available online at: https://ncdalliance.org/resources/signalling-virtue-promoting-harm (accessed November 17, 2020).
13. Brenner H. Will there be an epidemic of corollary illnesses linked to a COVID-19–related recession? AJPH. (2020) 110:974–75. doi: 10.2105/AJPH.2020.305724
14. Kluge HHP, Wickramasinghe K, Rippin HL, Mendes R, Peters DH, Kontsevaya A, et al. Prevention and control of non-communicable diseases in the COVID-19 response. Lancet. (2020) 395:1678–80. doi: 10.1016/S0140-6736(20)31067-9
15. Allen K, Pearson-Stuttard J, Hooton W, Diggle P, Capewell S, O'Flaherty M. Potential of trans fats policies to reduce socioeconomic inequalities in mortality from coronary heart disease in England: cost effectiveness modelling study. BMJ. (2015) 351:h4583. doi: 10.1136/bmj.h4583
16. European Commission. Commission staff working document. Impact assessment accompanying the document Commission Regulation (EU) amending Annex III to Regulation (EC) No 1925/2006 of the European Parliament and of the Council as regards trans fat, other than trans fat naturally occurring in animal fat, in foods intended for the final consumer. (2019). Available online at: https://ec.europa.eu/food/sites/food/files/safety/docs/fs_labelling-nutrition_transfats_swd_ia-pt01.pdf (accessed November 17, 2020).
17. Marklund M, Zheng M, Veerman JL, Wu JHY. Estimated health benefits, costs, and cost-effectiveness of eliminating industrial trans-fatty acids in Australia: a modelling study. PLoS Med. (2020) 17:e1003407. doi: 10.1371/journal.pmed.1003407
18. Pearson-Stuttard J, Hooton W, Critchley J, Capewell S, Collins M, Mason H, et al. Cost-effectiveness analysis of eliminating industrial and all trans fats in England and Wales: modelling study. J Pub Health. (2017) 39:574–82. doi: 10.1093/pubmed/fdw095
19. World Health Organization. NCD Global Monitoring Framework. (2013). Available online at: https://www.who.int/nmh/global_monitoring_framework/en/ (accessed November 17, 2020).
20. Sustainable Development Solutions Network. Indicators and a Monitoring Framework for the Sustainable Development Goals. Target 3.4. (2016). Available online at: https://indicators.report/targets/3-4/ (accessed November 17, 2020).
21. NCD Countdown 2030 collaborators. NCD countdown 2030: pathways to achieving Sustainable Development Goal target 3.4. Lancet. (2020) 396:918–34. doi: 10.1016/S0140-6736(20)31761-X
22. Agyemang C, van den Born BJ. Limited access to CVD medicines in low-income and middle-income countries: poverty is at the heart of the matter. Lancet Global Health. (2018) 6:234–5. doi: 10.1016/S2214-109X(18)30048-2
23. Owolabi M, Miranda JJ, Yaria J, Ovbiagele B. Controlling cardiovascular diseases in low and middle income countries by placing proof in pragmatism. BMJ Global Health. (2016) 1:e000105. doi: 10.1136/bmjgh-2016-000105
24. Afshin A, Sur PJ, Fay KA, Cornaby L, Ferrara G, Salama JS, et al. Health effects of dietary risks in 195 countries, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. (2019) 393:1958–72. doi: 10.1016/S0140-6736(19)30041-8
25. De Souza R, Mente A, Maroleanu A, Cozma AI, Ha V, Kishibe T, et al. Intake of saturated and trans unsaturated fatty acids and risk of all-cause mortality, cardiovascular disease, and type 2 diabetes: systematic review and meta-analysis of observational studies. BMJ. (2015) 351:h3978. doi: 10.1136/bmj.h3978
26. Yammine S, Huybrechts I, Biessy C, Dossus L, Aglago EK, Naudin S, et al. Dietary and circulating fatty acids and ovarian cancer risk in the European Prospective Investigation into Cancer and Nutrition. Cancer Epidemiol Biomarkers Prev. (2020) 29:1739–49. doi: 10.1158/1055-9965.EPI-19-1477
27. Micha R, Mozzaffarian D. Trans fatty acids: effects on cardiometabolic health and implications for policy. Prostag Leukotr Ess. (2008) 79:147–52. doi: 10.1016/j.plefa.2008.09.008
28. Downs SM, Thow AM, Leeder SR. The effectiveness of policies for reducing dietary trans fat: a systematic review of the evidence. Bull World Health Organ. (2013) 91:262–9H. doi: 10.2471/BLT.12.111468
29. Bendsen NT, Stender S, Szecsi PB, Larsen TM, Haugaard SB, Astrup A, et al. Effect of industrially produced trans fat on markers of systemic inflammation: evidence from a randomized trial in women. J Lipid Res. (2011) 52:1821–8. doi: 10.1194/jlr.M014738
30. Lopez-Garcia E, Schulze MB, Meigs JB, Manson JE, Rifai N, Stampfer MJ, et al. Consumption of trans fatty acids is related to plasma biomarkers of inflammation and endothelial dysfunction. J Nutr. (2005) 135:562–6. doi: 10.1093/jn/135.3.562
31. Mozaffarian D, Rimm EB, King IB, Lawler RL, McDonald GB, Levy WC. trans Fatty acids and systemic inflammation in heart failure. Am J Clin Nutr. (2004) 80:1521–5. doi: 10.1093/ajcn/80.6.1521
32. Mozaffarian D, Pischon T, Hankinson SE, Rifai N, Joshipura K, Willet WC, et al. Dietary intake of trans fatty acids and systemic inflammation in women. Am J Clin Nutr. (2004) 79:606–12. doi: 10.1093/ajcn/79.4.606
33. Esmaillzadeh A, Azadbakht L. Home use of vegetable oils, markers of systemic inflammation, and endothelial dysfunction among women. Am J Clin Nutr. (2008) 88:913–21. doi: 10.1093/ajcn/88.4.913
34. Kim J, Nam J-H. Insight into the relationship between obesity-induced low-level chronic inflammation and COVID-19 infection. Int J Obes. (2020) 44:1541–2. doi: 10.1038/s41366-020-0602-y
35. Sanchis-Gomar F, Lavie CJ, Mehra MR, Henry BM, Lippi G. Obesity and outcomes in COVID-19: when an epidemic and pandemic collide. Mayo Clin Proc. (2020) 95:1445–53. doi: 10.1016/j.mayocp.2020.05.006
36. Tang Y, Liu J, Zhang D, Xu Z, Ji J, Wen C. Cytokine storm in COVID-19: the current evidence and treatment strategies. Front Immunol. (2020) 11:1708. doi: 10.3389/fimmu.2020.01708
37. World Health Organization. Guidelines: Saturated fatty acid and trans-fatty acid intake for adults and children. 2018 (draft issued for public consultation). Available online at: https://extranet.who.int/dataform/upload/surveys/666752/files/Draft%20WHO%20SFA-TFA%20guidelines_04052018%20Public%20Consultation.pdf (accessed November 17, 2020).
38. World Health Organization. Module 2: promote. How-to guide for determining the best replacement oils and interventions to promote their use. In: REPLACE trans fat: an action package to eliminate industrially produced trans-fatty acids. (2019). Available online at: https://www.who.int/docs/default-source/replace-transfat/replace-module-2-p.pdf?sfvrsn=e9f83030_4 (accessed November 18, 2020).
39. Kontis V, Cobb LK, Mathers CD, Frieden TR, Ezzati M, Danaei G. Three public health interventions could save 94 million lives in 25 years. Circulation. (2019) 140:715–25. doi: 10.1161/CIRCULATIONAHA.118.038160
40. Rubinstein A, Elorriaga N, Garay OU, Poggio R, Caporale J, Matta MG, et al. Eliminating artificial trans fatty acids in Argentina: estimated effects on the burden of coronary heart disease and costs. Bull World Health Organ. (2015) 93:614–22. doi: 10.2471/BLT.14.150516
41. Restrepo BJ, Rieger M. Denmark's policy on artificial trans fat and cardiovascular disease. AJPM. (2016) 15:P69–76. doi: 10.1016/j.amepre.2015.06.018
42. Brandt EJ, Myerson R, Perraillon MC, Polonsky TS. Hospital admissions for myocardial infarction and stroke before and after the trans-fatty acid restrictions in New York. JAMA Cardiol. (2017) 2:627–34. doi: 10.1001/jamacardio.2017.0491
43. Bruns R. Estimate of Costs and Benefits of Removing Partially Hydrogenated Oils (PHOs) from the US Food Supply. Memorandum from the Office of the Commissioner to the Office of Food Additive Safety, U.S. Department of Health and Human Services, Food and Drug Administration. (2015). Available online at: https://www.who.int/docs/default-source/documents/replace-transfats/l-elements-of-economic-analysis.pdf?sfvrsn=be3a5f02_2 (accessed November 17, 2020).
44. World Health Organization. Tackling NCDs. “Best Buys” and Other Recommended Interventions for the Prevention and Control of Noncommunicable Diseases. (2017). Available online at: https://apps.who.int/iris/handle/10665/259232 (accessed November 17, 2020).
45. World Health Organization. REPLACE: Trans Fat Free by 2023. (2020). Available online at: https://www.who.int/teams/nutrition-and-food-safety/replace-transfat (accessed November 17, 2020).
46. World Health Organization. REPLACE Trans Fat – An Action Package To Eliminate Industrially-Produced Trans Fat From The Global Food Supply. (2018). Available online at: https://apps.who.int/iris/bitstream/handle/10665/331303/WHO-NMH-NHD-18.6-eng.pdf (accessed November 17, 2020).
47. World Health Organization. WHO Director-General's opening remarks at the launch of Countdown to 2023: WHO Report on Global Trans Fat Elimination 2020. (2020). Available online at: https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-launch-of-countdown-to-2023-who-report-on-global-trans-fat-elimination-2020 (accessed November 17, 2020).
48. World Health Organization. WHO announces certification programme for trans fat elimination. (2020). Available online at: https://www.who.int/news/item/17-11-2020-who-announces-certification-programme-for-trans-fat-elimination (accessed November 19, 2020).
49. World Health Organization. Countdown to 2023: WHO Report on Global Trans Fat Elimination 2020. (2020). Available online at: https://apps.who.int/iris/bitstream/handle/10665/334170/9789240010178-eng.pdf (accessed November 17, 2020).
50. Adhanom Ghebreyesus T, Frieden TR. REPLACE: a roadmap to make the world trans fat free by 2023. Lancet. (2018) 391:1978–80. doi: 10.1016/S0140-6736(18)31083-3
51. Pan American Health Organization. Plan of Action for the Elimination of Industrially Produced Trans-Fatty Acids 2020–2025. (2020). Available online at: https://iris.paho.org/handle/10665.2/51965?locale-attribute=es (accessed November 17, 2020).
52. European Commission. Commission Regulation (EU) 2019/649 of 24 April 2019 amending Annex III to Regulation (EC) No 1925/2006 of the European Parliament and of the Council as regards trans fat, other than trans fat naturally occurring in fat of animal origin. (2020). Available online at: https://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX:32019R0649&from=EN (accessed November 17, 2020).
53. GCC Standardization Organization (GSO). Gulf Technical Regulation: Trans Fatty Acids. (2015) GSO 2483:2015.
54. Demin A, Løge B, Zhiteneva O, Nishida C, Whiting S, Rippin H, et al. Trans fatty acid elimination policy in member states of the Eurasian Economic Union: implementation challenges and capacity for enforcement. J Clin Hypertens. (2020) 22:1328–37. doi: 10.1111/jch.13945
55. Resolve to Save Lives. Regulate Trans Fat. Even if the Burden is Low. (2019). Available online at: https://linkscommunity.org/assets/PDFs/trans-fat-advocacy-brief_-low-burden-regulations.pdf (accessed November 17, 2020).
56. Tzoulaki I, Elliott P, Kontis V, Ezzati M. Worldwide exposures to cardiovascular risk factors and associated health effects. Circulation. (2016) 133:2314–33. doi: 10.1161/CIRCULATIONAHA.115.008718
57. IFBA press release. Enhanced Commitment to Phase out Industrially Produced Trans-Fatty Acids. (2019). Available online at: https://ifballiance.org/uploads/press/pdf/5ccc4b8061475_IFBA%20iTFA%20Enhanced%20Commitment%2002.05.2019.pdf (accessed November 17, 2020).
58. Pan American Health Organization. Trans fat free Americas: Declaration of Rio de Janeiro. (2008). Available online at: https://www.paho.org/hq/dmdocuments/2009/transfat-declaration-rio%5B1%5D.pdf (accessed November 17, 2020).
59. Stuckler D, McKee M, Ebrahim S, Basu S. Manufacturing epidemics: the role of global producers in increased consumption of unhealthy commodities including processed foods, alcohol, and tobacco. PLoS Med. (2012) 9:e1001235. doi: 10.1371/journal.pmed.1001235
60. Monge-Rojas R, Colón-Ramos U, Jacoby E, Mozaffarian D. Voluntary reduction of trans-fatty acids in Latin America and the Caribbean: current situation. Rev Panam Salud Publica. (2011) 29:126–9. doi: 10.1590/S1020-49892011000200008
61. World Health Organization. For example, by implementing the WHO SHAKE technical package: World Health Organization. Shake the habit. The SHAKE Technical Package for Salt Reduction. (2016). Available online at: https://apps.who.int/iris/bitstream/handle/10665/250135/9789241511346-eng.pdf?sequence=1 (accessed November 18, 2020).
62. World Health Organization. For example, by implementing the WHO HEARTS technical package: World Health Organization. Hearts: technical package for cardiovascular disease management in primary health care. (2016). Available online at: https://www.who.int/cardiovascular_diseases/hearts/en/ (accessed November 18, 2020).
63. Marquez PV, Dutta S. Taxes on tobacco, alcohol, and sugar-sweetened beverages reduce health risks and expand fiscal space for Universal Health Coverage post-COVID 19. World Bank Blogs. (2020). Available online at: https://blogs.worldbank.org/health/taxes-tobacco-alcohol-and-sugar-sweetened-beverages-reduce-health-risks-and-expand-fiscal (accessed November 17, 2020).
Keywords: COVID-19, trans fat elimination, trans fatty acids, NCD prevention, food regulation, cardiovascular diseases, non-communicable disease, artificial trans-fatty acids
Citation: Bösch S, Westerman L, Renshaw N and Pravst I (2021) Trans Fat Free by 2023—A Building Block of the COVID-19 Response. Front. Nutr. 8:645750. doi: 10.3389/fnut.2021.645750
Received: 23 December 2020; Accepted: 03 February 2021;
Published: 24 March 2021.
Edited by:
Boris C. Rodríguez-Martín, Fundación Recal, SpainReviewed by:
Anna Vittoria Mattioli, University of Modena and Reggio Emilia, ItalyMaría Teresa García-Conesa, Spanish National Research Council, Spain
Copyright © 2021 Bösch, Westerman, Renshaw and Pravst. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Simone Bösch, c2ltb25lQHNpY2Fiby1jb25zdWx0aW5nLmNvbQ==