
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Nutr. , 18 February 2021
Sec. Nutritional Epidemiology
Volume 8 - 2021 | https://doi.org/10.3389/fnut.2021.633807
This article is part of the Research Topic Analyzing the Relationship Between Dietary Patterns, Health Outcomes and Individual Food Choices View all 23 articles
 Marlies Hörmann-Wallner1*
Marlies Hörmann-Wallner1* Raphaela Krause1
Raphaela Krause1 Begoña Alfaro2Hannah Jilani3
Begoña Alfaro2Hannah Jilani3 Monica Laureati4
Monica Laureati4 Valérie L. Almli5
Valérie L. Almli5 Mari Sandell6,7
Mari Sandell6,7 Pernilla Sandvik8Gertrude G. Zeinstra9
Pernilla Sandvik8Gertrude G. Zeinstra9 Lisa Methven10
Lisa Methven10Plant foods, rich in fibre, can offer textures that children find difficult to orally manipulate, resulting in low preferences but are important for a healthy diet and prevention of overweight in children. Our aim was to investigate preferences for food texture, intake of fibre-associated foods and the relation to BMI. Three hundred thirty European children (9–12 years, 54% female) indicated their texture preferences using the Child-Food-Texture-Preference- Questionnaire (CFTPQ), and their parents responded on fibre-associated food consumption and anthropometric information. BMI was significantly lower for children with higher intake of wholegrain alternatives of common foods; in addition to being significantly influenced by country and the wearing of a dental brace. Overall BMI-for-age-percentiles (BMI_pct) were negatively associated with the consumption of wholegrain cereals, white pasta and wholemeal products and positively associated with the intake of legumes and white biscuits. In males, BMI_pct were negatively associated with wholegrain products and dried fruits, and in females, positively with legume consumption. A few country-related associations were found for BMI_pct and wholegrain biscuits, seeds and nuts and refined products. No overall correlation was found between BMI_pct and the texture preference of soft/hard foods by CFTPQ, except in Austria. We conclude that this study revealed evidence of a connection between fibre-associated foods and children‘s BMI at a cross-cultural level and that sex is an important determinant of fibre-associated food intake and the development of overweight in childhood.
Nowadays childhood overweight/obesity is one of the most significant health problems worldwide (1). The highest levels of children with overweight and obesity have been reported in Southern Europe (Greece, Italy, Spain), whereas the ratio tends to be lower in Western and Northern Europe (2). Overweight and obesity existing already in childhood and adolescence can lead to serious chronic diseases (3, 4) and when persisting into adulthood, cardiovascular disease, diabetes and certain cancers are serious consequences (5–7). Therefore, the evaluation and classification of weight status in children is important for health assessment and- monitoring the prevention of diseases (8).
Observational studies have consistently found a positive correlation between the consumption of plant foods and improved long-term health outcomes in children (9, 10) emphasising that dietary fibre-rich plant foods, such as grains, fruits, vegetables, potatoes and legumes have positive health effects. The main effects are weight loss (10) and reduced long term risk of metabolic syndrome (11). Studies conducted in Europe, though carried out with adults, confirmed that intake of fibre-rich wholegrain pasta compared to refined pasta increased satiety and reduced hunger without changing the energy intake at subsequent meals (12, 13).
However, the intake of fruits and vegetables in European children is low (14), suggesting that only 6–24% reach the WHO recommendations, where females show a higher consumption than males (15–18). Moreover, research confirms that children with overweight/obesity consume less fruits and vegetables than children with normal weight (19). A low consumption of fruits and vegetables is not only associated with a higher risk of becoming overweight (19, 20), but also with the development of chronic diseases (21, 22). It was found that many children, instead of a diet rich in fruits and vegetables, choose rather sugar- and fat-rich snacks (23–25), which could lead to a higher energy intake (26) and consequently to overweight/obesity (27–29). However, no difference in the number of daily snacks between overweight and children with normal weight was found (23).
Eating behaviours in childhood are also often affected by picky eating (30), whereas these factors may have an influence on the development of overweight/obesity. Picky eating is very common in childhood, because children often have an avoidance of certain foods (31) and therefore show a low variety of foods in their diet.
The reasons for picky eating may be due to infancy, because food texture and the acceptance of food were related to the development of chewing (32). It has been shown that children who have early experiences with texture in their life tend to show a broader acceptance of those textures later. Demonteil et al. found that children were able to accept most textures at the age of 12 month because their chewing behaviour was established, however this was not always reflected by parental feeding practices (33). Lukasewycz and Mennella showed in their study that adults prefer harder foods and those containing more particles and children's preferences are developing with increasing age so that they become more adult-like later on (32). Szczesniak found out that children prefer food that can be easily manipulated in mouth (34). Moreover, a study from Werthmann et al. showed that children's consumption of e.g., a yoghurt decreased when the texture was modified by adding pieces to it (31). In vegetables tactile properties play a particularly important role in the rejection or acceptance (35). Therefore, the consumption of vegetables in young people is strongly related to the sensory properties of the respective vegetable variety (36–39). The structure of plants is based upon fibre, therefore, the texture of fibre-rich foods have more intensive tactile properties which may lead some children to reject such foods (31, 35). Studies show that children often reject foods with slimy, grainy or hard textures (36–39).
Little is yet known about a possible correlation between food texture preferences and overweight in children. In one previous European study a correlation was found between the preference for foods with a soft texture and food neophobia (40), which is in turn linked to the increase in body weight in adults (41).
The present study aimed to explore the relationship between weight status of European children, the consumption frequency of foods with high and low fibre content and texture preferences (soft/hard). We hypothesised that; (1) A higher intake of high fibre foods would be correlated with a lower BMI in children, potentially due to increasing satiety and reducing the intake of energy-dense foods, and (2) A higher preference for soft textures and therefore a lower consumption of plant-based high fibre foods would be connected with a higher BMI in children.
A total response of 330 children (9–12 years, 151 males, 179 females) from six European countries (Austria, Finland, Italy, Spain, Sweden and UK) and their parents was reached in this study (see Figure 1). The number of participants from each country is summarised in Table 1. The study protocol was approved by the relevant research ethics committee of each country, and written consent was obtained from the parents according to the declaration of Helsinki (Austria: No. 30-200 ex. 17/18, Finland: No. 12/2018, Italy: No. 49/17, Spain: No. PI2017180, Sweden: No 2017/549, UK: No. UREC 18/15). Inclusion criteria were the parental consent and the willingness to participate within this study. In detail, parents were informed about the procedures and were asked to sign an informed consent and therefore, children without a signed parental informed consent were excluded from the study. Children received an information sheet and gave their verbal consent to participate, none of the children declined to participate to the study. Recruitment took place in both primary and secondary schools, as children with the age between 9 and 12 years are sufficiently evolved to understand and complete the selected sensory tests (see below) (42). The study design included tests with the children which were carried out directly at school during class, as one visit per class. The parents completed questionnaires relating to their children at home via on-line links, or on-paper, as preferred by the parent. These questionnaires included personal data of their children (e.g., age, sex, height, weight), eating habits of their children (food frequency questionnaire, FFQ, mainly on fibre-rich and fibre-low foods), complementary information on their children (e.g., dental status), their familiarity with certain food items, and gave information on socio-demographic information (e.g., economic situation, education). Questionnaires and procedures for both children and parents were translated in English, reviewed by a native English speaker, and then translated in every language by two independent native speakers. The two translated versions were compared to identify discrepancies and reach consensus for an updated version. To improve comparability of the data collected in different cultures (43), procedures, experimental design and instructions to children and parents were the same in all countries and all tests were carried out within a 3-month period in the spring of 2018. After a team of trained researchers gave instructions, children worked on their own answering the questionnaires online via tablets. Children were tested by class or in smaller groups (4–5 children) on their own and were not influenced by their classmates. Tablets/computers were used by the children to complete the online questionnaire on familiarity with certain food items and the child food texture preference questionnaire (CFTPQ).
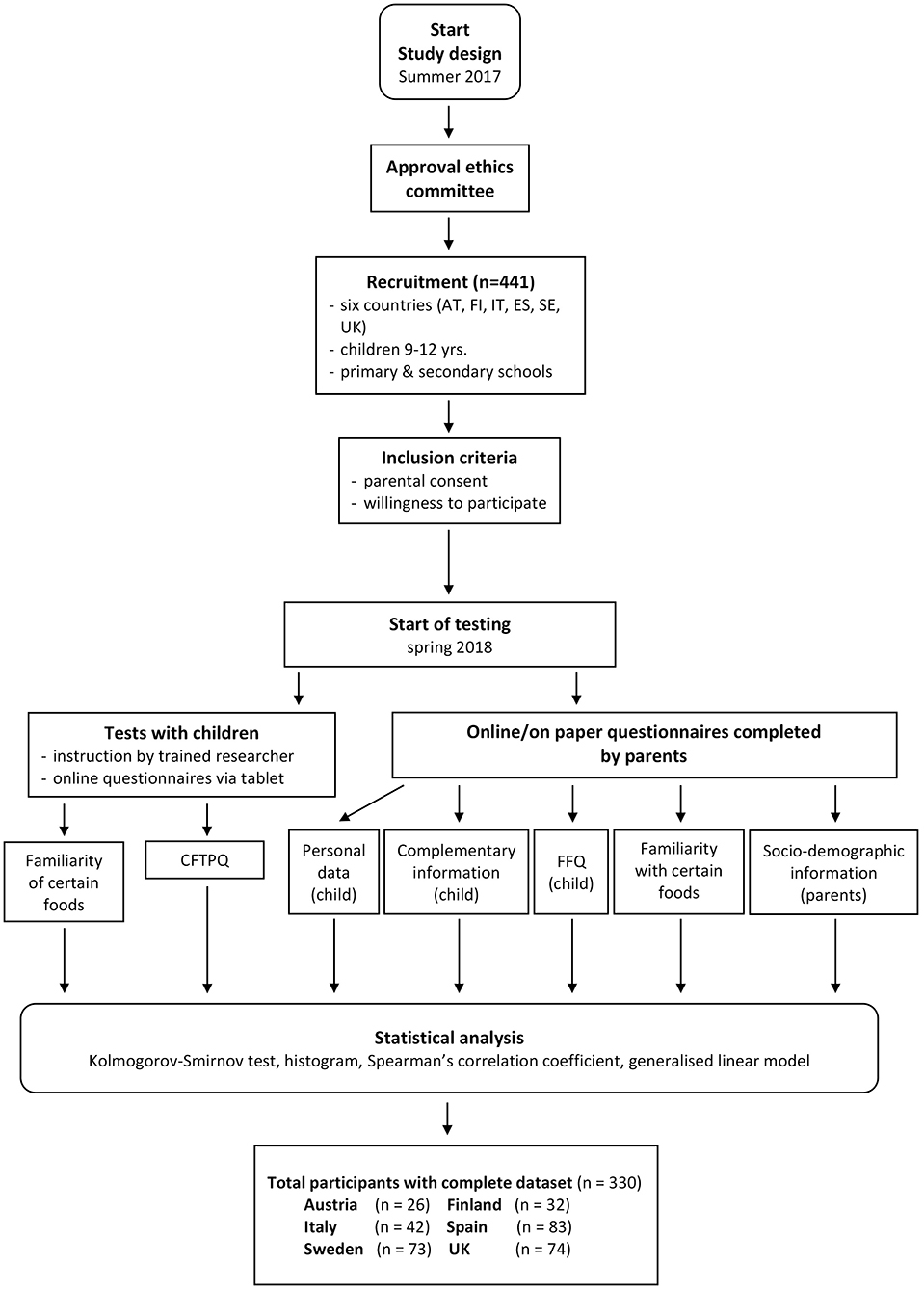
Figure 1. Flow chart of the study.
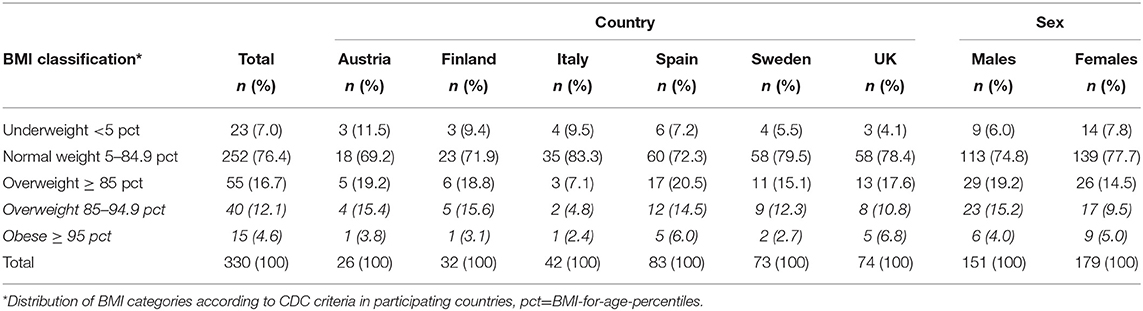
Table 1. Distribution of weight status.
The data presented in this paper were collected as part of a wider study that developed and validated the child food preference questionnaire (CFTPQ), and further details of the overall study design are reported in Laureati et al. (40).
In all six countries, the weight and the height of the children were self-reported by the parents within an online questionnaire. In addition, in Austria and the United Kingdom, the weight in kg (nearest to 0.1 kg) of the children was obtained with a portable scale (SECA). To determine children's height in cm (nearest to 0.1 cm) a portable stadiometer (SECA) in Austria and a tape measure mounted on the wall in the United Kingdom were used. The BMI was calculated by dividing the body weight in kg by the square of the height in m. High correlation coefficients of self-reported vs. measured BMI-data were obtained in UK (r = 0.82, p < 0.01) and Austria (r = 0.94, p < 0.01). This self-report validity could only be checked for UK and Austria, as there were no measured data in the other four countries. In addition to reporting numerical BMI data, BMI-for-age percentiles (BMI_pct) data are also reported in this paper. This accounts for the fact that children are individually and rapidly growing, hence the classification of weight status during childhood is complex (8). The Centers for Disease Control and Prevention (CDC), the International Obesity Task Force (IOTF) and the World Health Organisation (WHO) have developed suitable methods for BMI classification in children (44–46). CDC BMI_pct, suitable for comparing the BMI-data from different countries were used and for each participant the percentile was calculated. Furthermore, the BMI of participants was grouped into underweight (<5th percentile), normal weight (5th–84.9th percentile) or overweight (85th−94.9th percentile)/obesity (≥95th percentile) according to age- and sex-specific BMI percentiles cut-offs (46).
The detailed procedure for data collection and calculation of the CFTPQ index was previously described elsewhere (40). In brief, a questionnaire with pictures of 17 pairs of soft/smooth and hard/particulate food were presented to the child, e.g., yoghurt with pieces/yoghurt without pieces, apple/apple sauce, orange/orange juice, or toasted bread/soft bread. Of each pair, the child chose the preferred one. The children also reported their familiarity with each item. When both food pictures of a pair were also reported familiar by the child, this pair was considered as valid an included within the analysis. Children with <8 valid pairs were excluded from analysis resulting in 309 datasets from 330 children. For each time choosing the soft/smooth version a value of 1, or for choosing the hard/particulate version a value of 2 was given. Individual CFTPQ indices were calculated. The score ranged from 0 to 100 with higher scores representing a preference for the hard/particulate food items.
A 17-item questionnaire (40) of the frequency consumption of 12 fibre-rich (e.g., wholegrain products) and 5 low-fibre (e.g., refined “white” products) foods was completed by the parents for their children. Unreturned and incomplete questionnaires could not be included from the analysis (n = 111), resulting in n = 330 valid answers. Data were collected using a 6-point-category scale with answering options, less than once a month or never, 1–3 times per month, 1–3 times a week, 4–6 times a week, once a day, multiple times per day; in addition to category, I don't know. Parents were asked to recall their child‘s intake in the aforementioned categories over the previous 4—week period, and images were provided with the name of each food item. For each food item, the daily frequency equivalents (DFE) were calculated, so that the daily consumption quantity of all foods can be compared. DFE of 0= less than once a month or never, DFE of 0.07 = 1–3 times a month, DFE of 0.28 = 1–3 times a week, DFE of 0.71 = 4–6 times a week, DFE of 1 = once a day, DFE of 2.5 = multiple times a day, as published elsewhere (40).
Furthermore, the following scores were calculated from the FFQ Items:
Total consumption of high fibre foods (12 items, DFE): DFE sum of high fibre foods
∑ [wholegrain versions of bread, porridge, cereals, biscuits, rice and pasta; fresh fruits, dried fruits, nuts/seeds, vegetables, potatoes, legumes]
Total consumption of wholemeal foods (5 items, DFE): DFE sum of wholegrain foods
∑ [wholegrain versions of bread, cereals, biscuits, rice, pasta]
Total consumption of refined foods (5 items, DFE): DFE sum of refined foods
∑ [refined versions of bread, cereals, biscuits, rice, pasta]
Wholegrain (%):
Distribution of data was tested with one sample Kolmogorov-Smirnov tests and histograms. Outlier analysis confirmed there were no outliers in BMI nor CFTPQ variables. As expected there were outliers in reported FFQ data, as the majority of children having low wholegrain consumption. However, this reflects current dietary habits and, therefore, as consumption of higher levels of wholegrain foods is of interest in this study the outliers were not removed in the primary analysis. Where significant effects relating consumption frequency to BMI were found secondary analysis was carried out excluding outliers and subsequently reported in the limitations section.
The association between BMI_pct and the consumption frequencies of specific food items and the CFTPQ index were tested with Spearman‘s correlation coefficient (Table 2). To assess the related effect of independent factors and covariates, the generalised linear model (GsLM, BMI_pct as dependent variable) was included in the analyses. As the BMI-for-age percentiles are important in the consideration of children‘s BMI and considering most of data were not normally distributed, including any transformation of BMI_pct, the generalised linear model analysis using the Tweedie model was carried out. Included (significant) factors and covariates were the country of participation, currently wearing a dental brace and total consumption of wholemeal foods (section Relationship between BMI-for-age percentiles and all other factors) whereas sex, age of introducing solids, whether parents went to university, economic situation, CFTPQ, total consumption of refined alternatives, high fibre foods and wholegrain (%) were excluded. Subsequently, single food items that significantly correlated with BMI_pct were tested within (wholegrain cereals, white biscuits, white pasta, and legumes). Four final models with one or more factor/covariate were built (models 1–4).
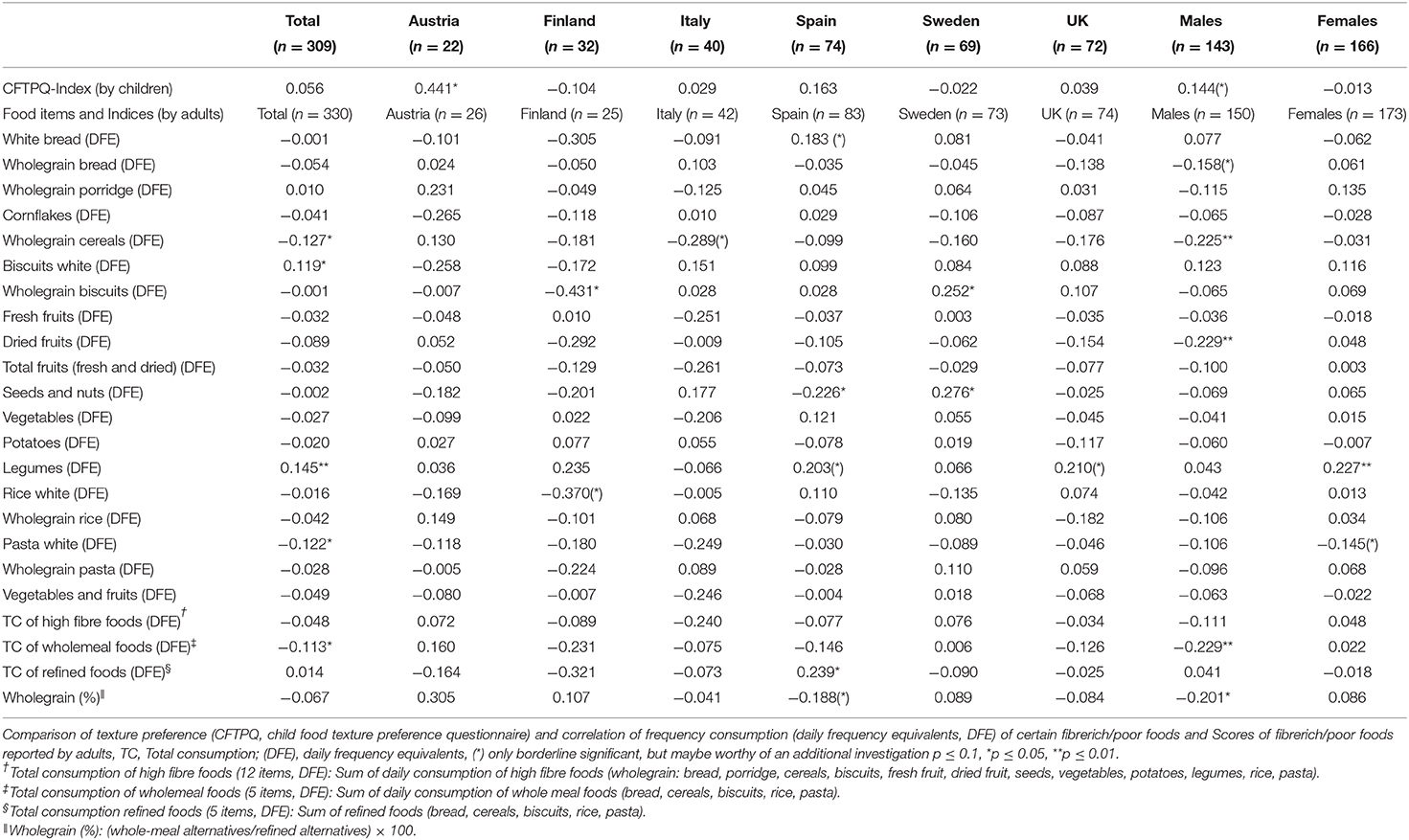
Table 2. Spearman‘s correlation coefficient of the BMI-for-age percentiles (CDC) with texture preference and eating frequency.
Effects showing a p ≤ 0.05 were considered significant, while p ≤ 0.10, although not significant but at a borderline level (47), were marked and reported as observed differences that may be worthy of additional investigation. The analysis was performed with SPSS V24 Software (IBM Analytics, USA).
Out of the 330 participating children with completed parental questionnaire, 76.4% had normal weight, 7.0% had underweight, 16.7% had overweight, whereof 4.6% had obesity (Table 1).
Taking children with overweight and obesity together, the highest proportions were reported for Spain (20.5%), followed by Austria (19.2%), Finland (18.8%), UK (17.6%). The countries with the lowest proportion of children with overweight and obesity were Sweden (15.1%) and Italy (7.1%). Partly, due to low subject numbers in many groups the differences between countries could not revealed significant.
Almost 6.0% of males and 7.8% of females had underweight, whereas 19.2% of males had overweight or obesity compared to 14.5% of females. The differences between males and females were only borderline significant (difference between males and females with overweight was p = 0.087).
Preference for softer (smooth) or harder (particulate) textures concluded from the CFTPQ index was not significantly correlated with the BMI_pct (r = 0.056, p = 0.998, n = 309). Austria was the only country showing a significant positive correlation between preference for harder/particulate textures (higher CFTPQ) and BMI_pct (r = 0.441, p = 0.040, n = 22); the positive correlation in males between texture preferences (CFTPQ) and BMI_pct was borderline significant (r = 0.144, p = 0.086, n = 143) (Table 2).
Parental responses on the 17-item food frequency questionnaire were completed and returned for 330 of the 441 participating children (Table 2). BMI_pct across the overall group correlated negatively with the reported consumption of wholegrain cereals (r = −0.127, p = 0.021), white pasta (r = −0.122, p = 0.027) and wholemeal products (r = −0.113, p = 0.04). Furthermore, BMI_pct correlated positively with the consumption frequency of white biscuits (r = 0.119, p = 0.03) and legumes (r = 0.145, p = 0.008). In summary, children with higher weight consumed less wholegrain cereals, white pasta and wholemeal products, whereas they consumed more white biscuits and legumes.
There were a number of significant, mostly weak correlations of consumption frequency and BMI_pct that were found in the data from specific countries (Table 2).
In Austria (n = 26), there was no specific correlation with the BMI_pct and any food item.
Regarding Finland (n = 25), there was a negative correlation with whole grain biscuits (r = −0.431, p = 0.032) and a negative correlation for white rice with borderline significance (r = −0.370, p = 0.069).
For Italy (n = 42) it was revealed that the consumption of wholegrain cereals was negatively associated with BMI_pct, but not significantly (r = −0.289, p = 0.064).
In Spain (n = 77), there was a significant positive correlation between BMI_pct and the consumption of refined products (r = 0.239, p = 0.029), although this only reached borderline significance for white bread (r = 0.183, p = 0.097) and legume consumption (r = 0.203, p = 0.066). Furthermore, a significant negative correlation was found between BMI_pct and consumption of seeds and nuts (r =-0.226, p = 0.040), although the negative correlation with wholegrain (%) was only borderline significant (r = −0.188, p = 0.088).
Within the data of Sweden (n = 72), two positive correlations between BMI_pct and the consumption of whole grain biscuits (r = 0.252, p = 0.031) and seeds and nuts (r = 0.276, p = 0.018) was found.
Finally, in the UK (n = 74) a positive correlation but only borderline significant was found for the consumption of legumes and BMI_pct (r = 0.210, p = 0.073).Sex-related differences
Males with higher BMI_pcts consumed less dried fruits (r = −0.229, p = 0.005). Furthermore, the consumption of wholegrain products decreased with increasing BMI_pct (wholemeal products (r = −0.229, p = 0.005), wholegrain cereals (r = −0.225, p = 0.006), and only borderline significantly wholegrain bread (r = −0.158, p = 0.054) and wholegrains (%) (r = −0.201, p = 0.014).
In females, the BMI_pct positively correlated with the consumption of legumes (r = 0.227, p = 0.003) and negatively but only borderline significantly with the consumption of white pasta (r = −0.145, p = 0.069). No further sex-related correlations were revealed.
Additional analysis was carried out to investigate relationships between BMI_pct, socio-demographic, texture preference, and food intake. GsLM found that country had no significant effect on BMI_pct (p = 0.095, model 1), however, both wearing braces (p = 0.045, B = −10.75) and total consumption of wholemeal foods were significantly related to lower BMI_pct (p = 0.037, B = −4.56, model 2). The median BMI_pct for those wearing a dental brace was 37 compared to 55 for those without. There was no overall significant effect of texture preference (CFTPQ) on BMI_pct. Separate models were performed to check the effects of reported consumption of individual foods, each model considering groups of food items which did not correlate with one another. In model 3 a significant relationship was found between BMI_pct and wholegrain cereals (p = 0.034, B = −10.17), white pasta (p = 0.020, B = −8.698) but not for white biscuits (p = 0.347) and in model 4 between BMI_pct and legumes (p = 0.041, B = 16.05) and wholegrain cereals (p = 0.034, B = −9.93).
Once the outlying data were removed, secondary analysis (regression and GsLM) found no significant relationship between wholegrain consumption and BMI_pct.
This study aimed to explore the relationship between the weight status of 9–12 years old children across Europe, their consumption of fibre rich foods and their preference for soft or hard food textures. The main findings are:
◦ The proportion of overall children with overweight or obesity was 16.7% and with underweight 7.0%.
◦ BMI_pct had significant negative associations with the overall consumption frequency of wholegrain cereals, white pasta and wholemeal products, and was positively associated with consumption frequency of legumes and white biscuits.
◦ Country-related associations were found for BMI_pct and wholegrain biscuits (negative, Finland; positive, Sweden), seeds and nuts (negative, Spain; positive Sweden) and refined products (positive, Spain).
◦ BMI_pct had a significantly negative association with frequency of consuming wholemeal (-products) and dried fruits, but only in males.
◦ The BMI_pct was significantly higher with a higher consumption of legumes, but only in females.
◦ No differences in texture preference (CFTPQ) for hard/particulate or soft/smooth food pairs according to BMI_pct were found, except a significant positive correlation for Austria.
The prevalence of children with overweight (including obesity) was found from highest to lowest in Spain (20.5%), Finland (18.8%), Austria (19.2%), the UK (17.6%), Sweden (15.1%), and by far lowest in Italy (7.1%). With the exception of Spain, our study found lower counts of children with overweight compared to literature (Spain: 19.2%, Finland: 23%, Austria: 25.2%, UK: 28%, Sweden: 17.7%, Italy: 20.8%) (48–51).
We assume that the lower reported distribution of overweight in these countries in our study might be explained by underreporting (52, 53) and/or the fact that the data were recorded in defined regions and are not representative for the whole country. For example, previous data has shown that inhabitants of Northern Italy have lower weight compared to people in the South (54, 55), and in line with this, children in our study were recruited in Northern Italy (Milano, Lombardy region). In England, the proportion of children with obesity has been found to be higher in areas of deprivation, significantly so for females (51). In the UK, part of the children in our study were recruited from urban areas in the South East which is not a region of high deprivation in England (56).
In Austria and the UK, measured and reported parental data of the children‘s height and weight (calculated BMI) had a very high agreement (respectively, 0.94 and 0.82, both p < 0.001). Furthermore, the use of different criteria in classification of weight status might limit the comparison between study results. In children, BMI for age and sex specific cut-off points are used according to population specific data e.g., WHO (45), CDC (46), or IOTF (44, 57). In our case, the CDC BMI-for-age percentiles were used. This classification is slightly different compared to the WHO criteria (57). There are high contrasts across different studies, as in an Italian sample only 2.7% children with underweight and 20.9% children with overweight were reported using WHO criteria (58).
There is less information on the proportion of children with underweight from studies in Europe compared to studies revealing overweight. Our study found rates of >7% in 4 out of 6 countries, in Italy (9.5%), Finland (9.4%), Austria (11.5%), and Spain (7.2%) still considering that these were self-reported data. In Spain, for 6–14 years old children, a mean prevalence of 10.2% for underweight was reported (59) using IOTF criteria, which is comparable to the present results.
Interestingly, we did not observe a tendency towards a lower BMI in southern compared to northern countries which was also noted in two recent epidemiological studies (2, 60). One might speculate, that diet styles might be changing, from the traditional southern Mediterranean diet, that is considered rich in fruits, vegetables and olive oil (61), towards more snacking and consumption of highly processed foods (62). This issue was addressed in recent studies found that a large part of the population of children and adolescents in the Southern countries have poor adherence to their traditional diet (63, 64). On the other hand, non-Mediterranean populations have been the major benefactors, since during the same period they have adopted a Mediterranean dietary pattern (65).
Another interesting result was that wearing a dental brace was accounting for a lower BMI (GsLM models; section 3.6) and this issue was already addressed elsewhere (66, 67). It is assumed that manipulating food is more difficult (68) and total food consumption might be lower (67) compared to children without wearing a dental brace. One previous study has reported mean body weight to significantly decrease during orthodontic treatment (from pre-treatment to 1 month into treatment), predominantly due to discomfort, however the study was of a limited size (n = 30) and in adults rather than children (66) Furthermore, a previous study found that increasing leptin-levels were reported in adults with orthodontic appliances, which might also lead to lower appetite and therefore to reduced food intake (69) and might contribute to a reduced BMI. In this context previous orthodontic research has found that adolescents with obesity had an increased initial tooth displacement and a higher rate of tooth movement compared to a normal-weight group, and it has been proposed that this may affect the treatment period (70–72), and therefore it is perhaps unsurprising that we found a difference in BMI related to wearing a dental brace.
We did not find any association between children's weight status and the preference for soft/smooth or harder/particulate structure of foods reflected by the CFTPQ index, either across the study population as a whole or country wise, except for Austria. In Austria the correlation was significant and quite high (r = 0.441), however the number of children was low (n = 22) and should be interpreted carefully. So to speculate for Austria it is indicated that with increasing weight children do like the particulate/harder foods e.g., chocolate bar, crunchy cornflakes or whole carrots. This is an unexpected result as food requiring more oral processing (e.g., hard, crunchy, thick food) has previously been associated with lower eating rate, a consequent increase of satiety and reduced energy intake (73). One study of eating rate in children (4–5 years) found that those who ate faster had higher energy intake, and this was associated with increased BMI z-score and adiposity (74). It should be underlined that texture preferences were investigated with a picture-based questionnaire (CFTPQ) with items that were not necessarily representative of fibre-rich foods, and thus may only partially have captured the link between fibre consumption and texture-driven preferences. More research is needed to better understand this complex and interrelated association.
Fibre consumption and consumption of fibre-rich foods in European countries does not meet current recommended daily intake guidelines (75–80), thus we anticipated that a consumption of high fibre foods would be negatively associated with BMI as indicated in literature (81, 82). In this study we found a weak, but significant association of increasing BMI_pct with a decreasing consumption frequency of wholegrain cereals and wholemeal products (bread, cereals, biscuits, pasta, rice). These results are mainly driven by Italy (cereals), Finland, Spain and the UK (wholemeal products) and by males (Table 2). Furthermore, both wholegrain products and wholegrain cereals were significant predictors of BMI percentiles, across the respective regression and GsLM models (section Relationship between BMI-for-age percentiles and all other factors). Koo et al. previously stated the importance of increasing wholegrain consumption on the management of childhood obesity (83), although studies show diverse results. In adults, within an intervention trial (n = 316) it was revealed that wholegrain consumption did not reduce body weight or fat (%) (10, 84). However, systematic reviews have concluded that the intake of high fibre cereals can lead to modest weight reduction in adults (10, 85). This was further confirmed by another survey (n = 716) on fibre intake in adolescents in schools. In one study it was revealed that fibre intake below the recommendations is associated with a higher risk of becoming overweight (81).
Furthermore, in the current study a lower consumption of dried fruits was associated with higher BMI_pct in males. It was reported that males eat less fruits than females and in this survey the preferences for fruit and vegetable was the main predictor (81%) of the sex difference here (16). Generally, independent of sex, a lower intake of fruits and vegetables which are high in fibre (and also vitamins and minerals) is associated with overweight in children (19) and also in adults (86, 87). In the survey on children‘s eating behavior (n = 39), it was shown that children with overweight and obesity ate significantly less fruits and vegetables than children with normal weight, but no sex differences for intake were found here (19). However, in the survey of Fogel and Blisserr (n = 99), the intake of fruits and vegetables did not show a significant correlation with BMI in 5–9 year old school children and again did not report on sex differences (88).
Legumes are fibre-rich and we hypothesised that the consumption would be lower in children with higher BMI_pct, as fibres are known to facilitate earlier satiation and improve diet quality (89). Moreover, intake of legumes in adults is associated with other health benefits such as reduced risk of cancer, cardiovascular disease (90) and metabolic syndrome (11). In contrast, we found that the legume consumption, especially in females, was positively associated with BMI (Table 2) and was further included within GsLM (section Relationship between BMI-for-age percentiles and all other factors) models. This result was mainly influenced by data from UK and Spain and we assume the result is related to typical preparation methods and combination with energy dense foods and ingredients. In Spain, the traditional way to prepare legume-dishes involves adding stewed vegetables and pork (chorizo, blood sausage, and ribs). Particularly, the combination with meat might increase the energy density in these dishes. In the UK, this higher legume intake may have been partly driven by a higher consumption of pre-prepared soft baked beans and/or cooked lentils as Dhal, very popular, easy and fast cooked affordable food (91, 92). Baked beans are generally high in sugar (91, 92) and Dhal high in fat. If used frequently in the diet in place of non-sugared/low-fat vegetables and legumes, it is perhaps more likely to contribute to higher rather than lower weight status. Moreover, our recent finding that children with higher legume consumption like softer texture fits here—as canned beans and boiled legumes are soft in their texture (40).
A few limitations could have affected our results such as that we mainly analysed BMI from self-reported data. Here, to consider a qualitative procedure child‘s weight and height was asked via the same question in all countries. Therefore, correlation of self-reported BMI-data vs. measured ones could only be analysed for Austria and UK. We want to acknowledge that consistency in measurement is fundamental in clinical and epidemiological research and that discrepancy and bias might have effect our BMI data. Furthermore, different classification methods limit the comparability with other study results on BMI. The estimation of daily food intake in children is important and often performed by using a FFQ. This is a widely applied and relevant instrument in epidemiological investigations in assessing children nutrition (93). FFQs are simple to administer and cost-efficient, although have limited validity and reliability in the context of over- and underestimation and overly rely on subject‘s memory (94). Some of these limitations are exacerbated where the questionnaire incorporates a higher number of food items. The use of indices which summarise food items and groups are of interest to reduce complexity and have been shown to be valid in young children, as have FFQs which use shorter recall reporting periods (95). Furthermore, using pictures combined with portion sizes, clear instructions and question period (e.g., last month) are relevant in valid food questionnaire instruments, especially in epidemiological approaches (96, 97). Therefore, in this study we utilised a FFQ that was short be containing only 17 items of direct relevance to the study, it asked parents only to remember the last 4 week period, and it provided images of each food item. The item number might have been too few to determine more specific differences (e.g., for legumes) and information on preparation methods would have been helpful. A further improvement in future studies would be to add portion size. As exact fibre intake could not be calculated, we were only able to estimate the intake of foods by daily frequencies portions. Very few children in the study consumed a high proportion of wholegrain foods. Where significant relationships were found between consumption of wholemeal products and BMI_pct, it must be noted that the consumption data contained outliers. Whereas, half of the children in the study consumed less than half of a daily equivalent of wholemeal alternatives (wholegrain bread, cereals, biscuits, rice or pasta), there were only 23 children (7%) reported to consume 2 or more DFEs of these alternatives. Once the outlying data were removed, secondary analysis (GsLM) found no significant relationship between wholegrain consumption and BMI-pct. We suggest this justifies the need for intervention studies of children in this age group comparing high wholegrain diets to standard diets. Furthermore, as food high in fibre also contains minerals, vitamins, and phytochemicals which are known to have positive health effects, this might additionally influence to the BMI related outcomes. Finally, even though the sample size was appropriate overall (n=330), we acknowledge the fact that for some variables (e.g., country-related differences) a larger sample size would have been beneficial. Future studies should confirm and extend our findings, here, the parental compliance should be considered as we were faced with low response.
Significant associations between parent-reported intake of fibre rich and also fibre poor foods and the child BMI-for-age percentile were found, but were depended on specific foods and sex. Overall there was a weak, but significant, negative association between the total consumption of wholemeal products (wholegrain equivalent of bread, cereals, biscuits, rice, and pasta) and weight status. Furthermore, there was no direct evidence that texture preference for soft and hard food is associated with BMI_pct of 9–12-year-old children. Moreover, cultural differences and sex need to be considered as determinants of food preferences. Further research encompassing a wider range of single foods including preparation methods and full recipes could assist in gaining deeper insights in the relationship of weight status, fibre consumption, and texture preferences of children.
The raw data supporting the conclusions of this article may be made available by the authors pending a specific request at the discretion of the Data Access and Management Commission of the E3S - Working group on Children.
The studies involving human participants were reviewed and approved by Austria: No. 30-200 ex. 17/18, Finland: No. 12/2018, Italy: No. 49/17, Spain: No. PI2017180, Sweden: No 2017/549, UK: No. UREC 18/15. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
HJ, ML, VA, MS, PS, and GZ: conceptualisation. RK, BA, ML, MS, PS, GZ, and LM: data curation. MH-W, BA, ML, VA, MS, and PS: funding acquisition. MH-W, RK, and LM: writing–original draft. BA, HJ, ML, VA, MS, PS, and GZ: writing–review & editing. All authors contributed to the article and approved the submitted version.
This cross-national study was conducted by members of the European Sensory Science Society (E3S) Children working group and was funded by the University of Milan (Italy) Piano di Sviluppo Unimi project (ML, 2015–20117): Sensory and behavioral determinants of childhood obesity: A role for personalized nutritional interventions. Additional funding support was received from the Basque Government (Spain) through CM Programme (BA, 2017–2018 NUTRISEN project), the Crown princess Margarets memorial foundation (PS Sweden), the Academy of Finland (MS, MS309408), and the Research Council of Norway and the Norwegian Fund for Research Fees for Agricultural Products (FFL) (VA, 233831/E50 and NRC314318). Furthermore, the study was financially supported by the Styrian Government (Austria), Section 8: Health, Care and Research, Division R&D (MH-W, ABT08-160762/2019-10). The funders had no role in the design, analysis or writing of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Mads Erling Pedersen is kindly acknowledged for programming the surveys. Noelia Da Quinta, Saila Mattila, Tabitha Reynolds, Annika Pichler, Emma Rosendahl, and Hanna Frommelin are kindly acknowledged for their help in data collection. Mariano Garelli and Ileana Antonini are kindly acknowledged for their help in taking the pictures of the CFTPQ food products. Anna Lena Aufschnaiter is kindly acknowledged for her support in manuscript preparation. All the teachers, children, and their families are kindly acknowledged for participating in the study.
1. Abarca-Gómez L, Abdeen ZA, Hamid ZA, Abu-Rmeileh NM, Acosta-Cazares B, Acuin C, et al. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: a pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. Lancet. (2017) 390:2627–42. doi: 10.1016/S0140-6736(17)32129-3
2. Spinelli A, Buoncristiano M, Kovacs VA, Yngve A, Spiroski I, Obreja G, et al. Prevalence of severe obesity among primary school children in 21 European countries. Obes Facts. (2019) 12:244–58. doi: 10.1159/000500436
3. Biro FM, Wien M. Childhood obesity and adult morbidities. Am J Clin Nutr. (2010) 91:1499–505. doi: 10.3945/ajcn.2010.28701B
4. Whitaker RC, Wright JA, Pepe MS, Seidel KS, Dietz WH. Predicting obesity in young adulthood from childhood and parental obesity. N Engl J Med. (1997) 337:869–73. doi: 10.1056/NEJM199709253371301
5. Guh DP, Zangh W, Bansback N, Amarsi Z, Birmingham CL, Anis AH. The incidence of co-morbidities related to obesity and overweight: a systematic review and meta-analysis. BMC Public Health. (2009) 9:88. doi: 10.1186/1471-2458-9-88
6. Van Kruijsdijk RC, Van der Wall E, Visseren FL. Obesity and cancer: the role of dysfunctional adipose tissue. Cancer Epidemiol Biomarkers Prev. (2009) 18:2569–78. doi: 10.1158/1055-9965.EPI-09-0372
7. Nejat EJ, Polotsky AJ, Pal L. Predictors of chronic disease at midlife and beyond - the health risks of obesity. Maturitas. (2010) 65:106–11. doi: 10.1016/j.maturitas.2009.09.006
8. Li K, Haynie D, Lipsky L, Palla H, Iannotti RJ, Simons-Morton B. Assessment of adolescent weight status: similarities and differences between CDC, IOTF, and WHO references. Prev Med. (2016) 87:151–4. doi: 10.1016/j.ypmed.2016.02.035
9. Marlett JA, McBurney MI, Slavin JL. Position of the American dietetic association: health implications of dietary fiber. J Am Diet Assoc. (2002) 102:993–1000. doi: 10.1016/S0002-8223(02)90228-2
10. Brownlee IA, Chater PI, Pearson JP, Wilcox MD. Dietary fibre and weight loss: Where are we now? Food Hydrocoll. (2017) 68:186–91. doi: 10.1016/j.foodhyd.2016.08.029
11. Wei B, Liu Y, Lin X, Fang Y, Cui J, Wan J. Dietary fiber intake and risk of metabolic syndrome: A meta-analysis of observational studies. Clin Nutr. (2018) 37:1935–1942. doi: 10.1016/j.clnu.2017.10.019
12. Cioffi I, Ibrugger S, Bache J, Thomassen MT, Contaldo F, Pasanisi F, et al. Effects on satiation, satiety and food intake of wholegrain and refined grain pasta. Appetite. (2016) 107:152–8. doi: 10.1016/j.appet.2016.08.002
13. Martini D, Brusamolino A, Del Bo C, Laureati M, Porrini M, Riso P. Effect of fiber and protein-enriched pasta formulations on satiety-related sensations and afternoon snacking in Italian healthy female subjects. Physiol Behav. (2017) 185:61–9. doi: 10.1016/j.physbeh.2017.12.024
14. Yngve A, Poortvliet E, Elmadfa I, Brug J, Ehrenblad B, Franchini B, et al. Fruit and vegetable intake in a sample of 11-year-old children in 9 European countries: the pro children cross-sectional survey. Ann Nutr Metab. (2005) 49:236–45. doi: 10.1159/000087247
15. Dibsdall L, Lambert N, Bobbin R, Frewer L. Low-income consumers' attitudes and behaviour towards access, availability and motivation to eat fruit and vegetables. Public Health Nutr. (2003) 6:159–68. doi: 10.1079/PHN2002412
16. Bere E, Brug J, Klepp K-I. Why do boys eat less fruit and vegetables than girls? Public Health Nutr. (2008) 11:321–5. doi: 10.1017/S1368980007000729
17. Friel S, Newell J, Kelleher C. Who eats four or more servings of fruit and vegetables per day? Multivariate classification tree analysis of data from the 1998 survey of lifestyle, attitudes and nutrition in the republic of Ireland. Public Health Nutr. (2005) 8:159–69. doi: 10.1079/PHN2004670
18. Rasmussen M, Krølner R, Klepp K-I, Lytle L, Brug J, Bere E, et al. Determinants of fruit and vegetable consumption among children and adolescents: a review of the literature. Part I: quantitative studies. Int J Behav Nutr Phys Act. (2006) 3:1–19. doi: 10.1186/1479-5868-3-22
19. Miller P, Moore R, Kral T. Children's daily fruit and vegetable intake: associations with maternal intake and child weight status. J Nutr Educ Behav. (2011) 43:396–400. doi: 10.1016/j.jneb.2010.10.003
20. Guenther PM, Dodd KW, Reedy J, Krebs-Smith SM. Most Americans eat much less than recommended amounts of fruits and vegetables. J Am Diet Assoc. (2006) 106:1371–9. doi: 10.1016/j.jada.2006.06.002
21. Pryor WA, Stahl W, Rock CL. Beta carotene: from biochemistry to clinical trials. Nutr Rev. (2009) 58:39–53. doi: 10.1111/j.1753-4887.2000.tb07810.x
22. Steinmetz K, Potter J. Vegetables, fruits and cancer. I. Epidemiology. Cancer Causes Control. (1991) 2:325–57. doi: 10.1007/BF00051672
23. Ha A, Bae S, Urrutia-Rojas X, Singh KP. Eating and physical activity practices in risk of overweight and overweight children: compliance with US department of agriculture food guide pyramid and with national association for sport and physical activity guidelines for children. Nutr Res. (2005) 25:905–15. doi: 10.1016/j.nutres.2005.09.010
24. Jahns L, Siega-Riz AM, Popkin BM. The increasing prevalence of snacking among US children from 1977 to 1996. J Pediatr. (2001) 138:493–8. doi: 10.1067/mpd.2001.112162
25. Cross A, Babicz D, Cushman LF. Snacking patterns among 1,800 adults and children. J Am Diet Assoc. (1994) 94:1398–403. doi: 10.1016/0002-8223(94)92542-9
26. Samuelson G, Bratteby L, Enghardt H, Hedgren M. Food habits and energy and nutrient intake in Swedish adolescents approaching the year 2000. Acta Paediatr Suppl. (1996) 11:1651–2227. doi: 10.1111/j.1651-2227.1996.tb14268.x
27. Heald FP. Fast food and snakc fod: Beneficial or deleterious. J Adolesc Health. (1992) 13:380–3. doi: 10.1016/1054-139X(92)90033-8
28. Jeffery RW, French SA. Epidemic obesity in the United States: are fast foods and television viewing contributing? Am J Public Health. (1998) 88:277–80. doi: 10.2105/AJPH.88.2.277
29. Gortmaker S, Dietz W, Cheung L. Inactivity, diet, and the fattening of America. J Am Diet Assoc. (1990) 90:1247–1252.5.
30. Moding KJ, Bellows LL, Grimm KJ, Johnson SL. A longitudinal examination of the role of sensory exploratory behaviors in young children's acceptance of new foods. Physiol Behav. (2020) 218:112821. doi: 10.1016/j.physbeh.2020.112821
31. Werthmann J, Jansen A, Havermans R, Nederkoorn C, Kremers S, Roefs A. Bits and pieces. Food texture influences food acceptance in young children. Appetite. (2015) 84:181–187. doi: 10.1016/j.appet.2014.09.025
32. Lukasewycz LD, Mennella JA. Lingual tactile acuity and food texture preferences among children and their mothers. Food Qual Prefer. (2012) 26:58–66. doi: 10.1016/j.foodqual.2012.03.007
33. Demonteil L, Tournier C, Agnès M, Dusoulier M, Weenen H, Nicklaus S. Longitudinal study on acceptance of food textures between 6 and 18 months. Food Qual Prefer. (2019) 71:54–65. doi: 10.1016/j.foodqual.2018.05.010
34. Szczesniak A. Consumer awareness of and attitudes to food texture. J Texture Stud. (1972) 3:206–217. doi: 10.1111/j.1745-4603.1972.tb00624.x
35. Nederkoorn C, Jansen A, Havermans RC. Feel your food. The influence of tactile sensitivity on picky eating in children. Appetite. (2015) 84:7–10. doi: 10.1016/j.appet.2014.09.014
36. Cox DN, Melo L, Zabaras D, Delahunty CM. Acceptance of health-promoting Brassica vegetables: the influence of taste perception, information and attitudes. Public Health Nutr. (2012) 15:1474–82. doi: 10.1017/S1368980011003442
37. Dinehart ME, Hayes JE, Bartoshuk LM, Lanier SL, Duffy VB. Bitter taste markers explain variability in vegetable sweetness, bitterness, and intake. Physiol Behav. (2006) 87:304–13. doi: 10.1016/j.physbeh.2005.10.018
38. Dinnella C, Morizet D, Masi C, Cliceri D, Depezay L, Appleton KM, et al. Sensory determinants of stated liking for vegetable names and actual liking for canned vegetables: a cross-country study among European adolescents. Appetite. (2016) 107:339–47. doi: 10.1016/j.appet.2016.08.110
39. Krølner R, Rasmussen M, Brug J, Klepp K-I, Wind M, Due P. Determinants of fruit and vegetable consumption among children and adolescents: a review of the literature. Part II: qualitative studies. Int J Behav Nutr Phys Act. (2011) 8:1–38. doi: 10.1186/1479-5868-8-112
40. Laureati M, Sandvik P, Almli LV, Sandell M, Zeinstra GG, Methven L, et al. Individual differences in texture preferences among european children: development and validation of the child food texture preference questionnaire (CFTPQ). Food Qual Prefer. (2020) 80:103828. doi: 10.1016/j.foodqual.2019.103828
41. Proserpio C, Laureati M, Invitti C, Pagliarini E. Reduced taste responsiveness and increased food neophobia characterize obese adults. Food Qual Prefer. (2018) 63:73–9. doi: 10.1016/j.foodqual.2017.08.001
42. Laureati M, Pagliarini E, Toschi TG, Monteleone E. Research challenges and methods to study food preferences in school-aged children: a review of the last 15years. Food Qual Prefer. (2015) 46:92–102. doi: 10.1016/j.foodqual.2015.07.010
43. Ares G. Methodological issues in cross-cultural sensory and consumer research. Food Qual Prefer. (2018) 64:253–63. doi: 10.1016/j.foodqual.2016.10.007
44. Cole TJ, Bellizzi MC, Flegel KM, Dietz WH. Establishing a standard definition for child overweight and obesity worldwide: international survey. BMJ. (2000) 320:1240. doi: 10.1136/bmj.320.7244.1240
45. de Onis M, Onyango AW, Borghi E, Siyam A, Nishida C, Siekmann J. Development of a WHO growth reference for school-aged children and adolescents. Bull World Health Organ. (2007) 85:660–7. doi: 10.2471/BLT.07.043497
46. Kuczmarski RJ, Ogden CL, Guo SS, Grummer-Strawn LM, Flegal KM, Mei Z, et al. 2000 CDC Growth Charts for the United States: methods and development. Vital Health Stat. (2002) 246:1–190.
47. Hackshaw A, Kirkwood A. Interpreting and reporting clinical trials with results of borderline significance. BMJ. (2011) 343:d3340. doi: 10.1136/bmj.d3340
48. BMGF. Childhood Obesity Surveillance Initiative (COSI) - Bericht Österreich 2017. Vienna: BMGF (2017). 1–32p.
49. Börnhorst C, Siani A, Russo P, Kourides Y, Sion I, Molnár D, et al. Early life factors and inter-country heterogeneity in BMI growth trajectories of european children: the IDEFICS study. PLOS ONE. (2016) 11:e0149268. doi: 10.1371/journal.pone.0149268
50. Currie C, Zanotti C, Morgan A, Currie D, de Looze M, Roberts C, et al. Social Determinants of Health and Well-Being Among Young People: Health Behaviour in School-Aged Children (HBSC) Study : International Report From the 2009-2010 Survey. Copenhagen: World Health Organization, Regional Office for Europe (2012).
51. Conolly A, Craig S. Health Survey for England 2018 Overweight and Obesity in Adults and Children. London: Health and Social Care Information Centre (2019). 1–31p.
52. Rietmeijer-Mentink M, Paulis WD, van Middelkoop M, Bindels PJE, van der Wouden JC. Difference between parental perception and actual weight status of children: a systematic review. Matern Child Nutr. (2013) 9:3–22. doi: 10.1111/j.1740-8709.2012.00462.x
53. Karunanayake CP, Rennie DC, Hildebrand C, Lawson JA, Hagel L, Dosman JA, et al. Actual body weight and the parent's perspective of child's body weight among rural Canadian children. Children. (2016) 3:13. doi: 10.3390/children3030013
54. Brunello G, Labartino G. Regional differences in overweight rates: the case of Italian regions. Econ Hum Biol. (2014) 12:20–9. doi: 10.1016/j.ehb.2012.10.001
55. Cacciari E, Milani S, Balsamo A, Dammacco F, Luca FD, Chiarelli F, et al. Italian cross-sectional growth charts for height, weight and BMI (6–20 y). Eur J Clin Nutr. (2002) 56:171–80. doi: 10.1038/sj.ejcn.1601314
56. Noble S, McLennan D, Noble M, Plunkett E, Gutacker N, Silk M, et al. English Indices of Deprivation 2019: Research Report. London (2019). 1–87p. Available online at: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/833947/IoD2019_Research_Report.pdf
57. Cole TJ, Lobstein T. Extended international (IOTF) body mass index cut-offs for thinness, overweight and obesity: extended international BMI cut-offs. Pediatr Obes. (2012) 7:284–94. doi: 10.1111/j.2047-6310.2012.00064.x
58. Ashi H, Campus G, Klingberg G, Forslund HB, Lingström P. Childhood obesity in relation to sweet taste perception and dental caries – a cross-sectional multicenter study. Food Nutr Res. (2019) 63:1682. doi: 10.29219/fnr.v63.1682
59. de Ruiter I, Olmedo-Requena R, Sánchez-Cruz JJ, Jiménez-Moleón JJ. Trends in child obesity and underweight in Spain by birth year and age, 1983 to 2011. Rev Españ Cardiol. (2017) 70:646–55. doi: 10.1016/j.rec.2016.12.013
60. Ahrens W, Pigeot I, Pohlabeln H, De Henauw S, Lissner L, Molnár D, et al. Prevalence of overweight and obesity in European children below the age of 10. Int J Obes. (2014) 38:S99–107. doi: 10.1038/ijo.2014.140
61. Davis C, Bryan J, Hodgson J, Murphy K. Definition of the mediterranean diet: a literature review. Nutrients. (2015) 7:9139–53. doi: 10.3390/nu7115459
62. Fernández-Alvira JM, Bammann K, Eiben G, Hebestreit A, Kourides YA, Kovacs E, et al. Prospective associations between dietary patterns and body composition changes in European children: the IDEFICS study. Public Health Nutr. (2017) 20:3257–65. doi: 10.1017/S1368980017002361
63. Naska A, Trichopoulou A. Back to the future: The Mediterranean diet paradigm. Nutr Metab Cardiovasc Dis. (2014) 24:216–9. doi: 10.1016/j.numecd.2013.11.007
64. Rosi A, Paolella G, Biasini B, Scazzina F, Alicante P, De Blasio F, et al. Dietary habits of adolescents living in North America, Europe or Oceania: a review on fruit, vegetable and legume consumption, sodium intake, and adherence to the mediterranean diet. Nutr Metab Cardiovasc Dis. (2019) 29:544–60. doi: 10.1016/j.numecd.2019.03.003
65. da Silva R, Bach-Faig A, Raidó Quintana B, Buckland G, Vaz de Almeida MD, Serra-Majem L. Worldwide variation of adherence to the mediterranean diet, in 1961–1965 and 2000–2003. Public Health Nutr. (2009) 12:1676–84. doi: 10.1017/S1368980009990541
66. Ajwa N, Makhdoum L, Alkhateeb H, Alsaadoun A, Alqutub S, Alkhumayes H. The impact of orthodontic appliance on body weight changes, dietary habits, and self-perceived discomfort in early stages of orthodontic treatment. Glob J Health Sci. (2018) 10:11–7. doi: 10.5539/gjhs.v10n9p11
67. Schott TC, Ludwig B. Quantification of wear-time adherence of removable appliances in young orthodontic patients in relation to their BMI: a preliminary study. Pat Prefer Adher. (2014) 8:1587–95. doi: 10.2147/PPA.S69586
68. Farzanegan F, Zebarjad SM, Alizadeh S, Ahrari F. Pain reduction after initial archwire placement in orthodontic patients: a randomized clinical trial. Am J Orthod Dentofacial Orthop. (2012) 141:169–73. doi: 10.1016/j.ajodo.2011.06.042
69. Srinivasan B, Chitharanjan A, Kailasam V, Lavu V, Ganapathy V. Evaluation of leptin concentration in gingival crevicular fluid (GCF) during orthodontic tooth movement and its correlation to the rate of tooth movement. J Orthod Sci. (2019) 8:6. doi: 10.4103/jos.JOS_58_18
70. Saloom HF, Papageorgiou SN, Carpenter GH, Cobourne MT. Impact of obesity on orthodontic tooth movement in adolescents: a prospective clinical cohort study. J Dent Res. (2017) 96:547–54. doi: 10.1177/0022034516688448
71. Michelogiannakis D, Rossouw PE, Khan J, Akram Z, Menenakos E, Javed F. Influence of increased body mass index on orthodontic tooth movement and related parameters in children and adolescents: a systematic review of longitudinal controlled clinical studies. J Orthod. (2019) 46:323–34. doi: 10.1177/1465312519873669
72. von Bremen J, Lorenz N, Ludwig B, Ruf S. Increased BMI in children—an indicator for less compliance during orthodontic treatment with removable appliances. Eur J Orthod. (2018) 40:350–5. doi: 10.1093/ejo/cjy007
73. McCrickerd K, Lim CM, Leong C, Chia EM, Forde CG. Texture-based differences in eating rate reduce the impact of increased energy density and large portions on meal size in adults. J Nutr. (2017) 147:1208–17. doi: 10.3945/jn.116.244251
74. Fogel A, Goh AT, Fries LR, Sadananthan SA, Velan SS, Michael N, et al. Faster eating rates are associated with higher energy intakes during an ad libitum meal, higher BMI and greater adiposity among 4·5-year-old children: results from the growing up in Singapore towards healthy outcomes (GUSTO) cohort. Br J Nutr. (2017) 117:1042–51. doi: 10.1017/S0007114517000848
75. Elmadfa I, Institut für Ernährungswissenschaften (Wien), Österreich, Bundesministerium für Gesundheit. Österreichischer Ernährungsbericht 2012. Wien: Bundesministerium für Gesundheit (2012). 1–424p.
76. Public Health England. National Diet and Nutrition Survey. Years 1 to 9 of the Rolling Programme (2008/2009 – 2016/2017): Time Trend and Income Analyses. Public Health England (2019). 56p.
77. López-Sobaler AM, Aparicio A, Rubio J, Marcos V, Sanchidrián R, Santos S, et al. Adequacy of usual macronutrient intake and macronutrient distribution in children and adolescents in Spain: a national dietary survey on the child and adolescent population, ENALIA 2013–2014. Eur J Nutr. (2019) 58:705–19. doi: 10.1007/s00394-018-1676-3
78. Pietinen P, Paturi M, Reinivuo H, Tapanainen H, Valsta LM. FINDIET 2007 Survey: energy and nutrient intakes. Public Health Nutr. (2010) 13:920–4. doi: 10.1017/S1368980010001102
79. Moraeus L, Lemming EW, Hursti U-KK, Arnemo M, Sipinen JP, Lindroos A-K. Riksmaten adolescents 2016–17: a national dietary survey in Sweden – design, methods, and participation. Food Nutr Res. (2018) 62:1381. doi: 10.29219/fnr.v62.1381
80. Sette S, D'Addezio L, Piccinelli R, Hopkins S, Le Donne C, Ferrari M, et al. Intakes of whole grain in an Italian sample of children, adolescents and adults. Eur J Nutr. (2017) 56:521–33. doi: 10.1007/s00394-015-1097-5
81. De Carvalho ÉB, Vitolo MR, Gama CM, Lopez FA, Taddei JAC, de Morais MB. Fiber intake, constipation, and overweight among adolescents living in São Paulo city. Nutrition. (2006) 22:744–9. doi: 10.1016/j.nut.2006.05.001
82. Mann KD, Pearce MS, McKevith B, Thielecke F, Seal CJ. Whole grain intake in the UK remains low: results from the national diet and nutrition survey rolling programme years 1, 2 and 3. Proc Nutr Soc. (2015) 74:E60. doi: 10.1017/S0029665115000750
83. Koo HC, Poh BK, Ruzita AT. Intervention on whole grain with healthy balanced diet to manage childhood obesity (GReat-ChildTMtrial): study protocol for a quasi-experimental trial. Springerplus. (2016) 5:840. doi: 10.1186/s40064-016-2431-y
84. Brownlee IA, Moore C, Chatfield M, Richardson DP, Ashby P, Kuznesof SA, et al. Markers of cardiovascular risk are not changed by increased whole-grain intake: the WHOLEheart study, a randomised, controlled dietary intervention. Br J Nutr. (2010) 104:125–34. doi: 10.1017/S0007114510000644
85. Cho SS, Qi L, Fahey GC, Klurfeld DM. Consumption of cereal fiber, mixtures of whole grains and bran, and whole grains and risk reduction in type 2 diabetes, obesity, and cardiovascular disease. Am J Clin Nutr. (2013) 98:594–619. doi: 10.3945/ajcn.113.067629
86. Nour M, Lutze SA, Grech A, Allman-Farinelli M. The relationship between vegetable intake and weight outcomes: a systematic review of cohort studies. Nutrients. (2018) 10:1626. doi: 10.3390/nu10111626
87. Boeing H, Bechthold A, Bub A, Ellinger S, Haller D, Kroke A, et al. Critical review: vegetables and fruit in the prevention of chronic diseases. Eur J Nutr. (2012) 51:637–63. doi: 10.1007/s00394-012-0380-y
88. Fogel A, Blissett J. Effects of sucrose detection threshold and weight status on intake of fruit and vegetables in children. Appetite. (2014) 83:309–16. doi: 10.1016/j.appet.2014.09.003
89. Ahn CH, Bae JH, Cho YM. Premeal consumption of a protein-enriched, dietary fiber-fortified bar decreases total energy intake in healthy individuals. Diabetes Metab J. (2019) 43:879–92. doi: 10.4093/dmj.2018.0202
90. Mitchell D, Rumney J, Campbell J, Cai D, Curran J, Marinangeli C. Increasing pulse intake improves diet quality in adults in the US (P18-114-19). Cur Dev Nutr. (2019) 3:1677. doi: 10.1093/cdn/nzz039.P18-114-19
91. Statista. Canned Beans: Weekly Consumption in the UK 2006-2016/17. Statista. (2020). Available online at: https://www.statista.com/statistics/721177/weekly-uk-household-consumption-of-canned-beans-united-kingdom-uk/ (accessed February 3, 2020).
92. Rauber F, Da Costa Louzada ML, Steele EM, Millett C, Monteiro CA, Levy RB. Ultra-processed food consumption and chronic non-communicable diseases-related dietary nutrient profile in the UK (2008–2014). Nutrients. (2018) 10:587. doi: 10.3390/nu10050587
93. Vilela S, Severo M, Moreira T, Ramos E, Lopes C. Evaluation of a short food frequency questionnaire for dietary intake assessment among children. Eur. J Clin Nutr. (2019) 73:679–91. doi: 10.1038/s41430-018-0200-4
94. Bell LK, Golley RK, Magarey AM. Short tools to assess young children's dietary intake: a systematic review focusing on application to dietary index research. J Obes. (2013) 2013:709626. doi: 10.1155/2013/709626
95. Lovell A, Bulloch R, Wall CR, Grant CC. Quality of food-frequency questionnaire validation studies in the dietary assessment of children aged 12 to 36 months: a systematic literature review. J Nutr Sci. (2017) 6:e16. doi: 10.1017/jns.2017.12
96. Vuholm S, Lorenzen JK, Kristensen M. Relative validity and reproducibility of a food frequency questionnaire to assess dietary fiber intake in Danish adults. Food Nutr Res. (2014) 58:24723. doi: 10.3402/fnr.v58.24723
Keywords: texture preferences, plant foods, high/low fibre foods, overweight, BMI-for-age percentiles
Citation: Hörmann-Wallner M, Krause R, Alfaro B, Jilani H, Laureati M, Almli VL, Sandell M, Sandvik P, Zeinstra GG and Methven L (2021) Intake of Fibre-Associated Foods and Texture Preferences in Relation to Weight Status Among 9–12 Years Old Children in 6 European Countries. Front. Nutr. 8:633807. doi: 10.3389/fnut.2021.633807
Received: 26 November 2020; Accepted: 25 January 2021;
Published: 18 February 2021.
Edited by:
Francesco Visioli, University of Padua, ItalyReviewed by:
Rosa Casas Rodriguez, Institut de Recerca Biomèdica August Pi i Sunyer (IDIBAPS), SpainCopyright © 2021 Hörmann-Wallner, Krause, Alfaro, Jilani, Laureati, Almli, Sandell, Sandvik, Zeinstra and Methven. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marlies Hörmann-Wallner, bWFybGllcy5ob2VybWFubi13YWxsbmVyQGZoLWpvYW5uZXVtLmF0
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.