 Beata Sokołowska
Beata Sokołowska Wiktor Świderski2
Wiktor Świderski2 Edyta Smolis-Bąk
Edyta Smolis-Bąk
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Comput. Neurosci. , 14 May 2024
Volume 18 - 2024 | https://doi.org/10.3389/fncom.2024.1390208
This article is part of the Research Topic 15 Years of Frontiers in Computational Neuroscience - Computational Motor Control View all 4 articles
Introduction: Novel technologies based on virtual reality (VR) are creating attractive virtual environments with high ecological value, used both in basic/clinical neuroscience and modern medical practice. The study aimed to evaluate the effects of VR-based training in an elderly population.
Materials and methods: The study included 36 women over the age of 60, who were randomly divided into two groups subjected to balance-strength and balance-cognitive training. The research applied both conventional clinical tests, such as (a) the Timed Up and Go test, (b) the five-times sit-to-stand test, and (c) the posturographic exam with the Romberg test with eyes open and closed. Training in both groups was conducted for 10 sessions and embraced exercises on a bicycle ergometer and exercises using non-immersive VR created by the ActivLife platform. Machine learning methods with a k-nearest neighbors classifier, which are very effective and popular, were proposed to statistically evaluate the differences in training effects in the two groups.
Results and conclusion: The study showed that training using VR brought beneficial improvement in clinical tests and changes in the pattern of posturographic trajectories were observed. An important finding of the research was a statistically significant reduction in the risk of falls in the study population. The use of virtual environments in exercise/training has great potential in promoting healthy aging and preventing balance loss and falls among seniors.
We are currently witnessing dynamic changes in the structure of societies around the world (Lutz et al., 2008; Sanderson and Scherbov, 2010; United Nations, 2017). Medical advances, improved living conditions and increased life expectancy are making old age an integral part of modern reality (Barbaccia et al., 2022). United Nations (UN) and World Health Organization (WHO) projections indicate that the number of seniors will double in three decades, reaching 1.5 billion people in 2050 (United Nations, 2020; World Health Organization [WHO], 2020), and people aged 60 and older will make up about 22% of the world’s population (United Nations, 2019). Old age, in addition to its inevitable time dimension, comes with limitations and difficulties in maintaining physical activity that promotes physical and mental health (Viswanathan and Sudarsky, 2012; Chen et al., 2021). These individuals are more prone to falls due to the natural aging process, which negatively affects muscle strength, tissue flexibility, and overall body stability (Moreland et al., 2004; Carapeto and Aguayo-Mazzucato, 2021). Pain and limited joint mobility are the cause of reduced physical fitness, leading to an increased risk of falls and loss of independence (Rubenstein, 2006; Bischoff-Ferrari, 2011; Stevens and Lee, 2018). Activities aimed at strengthening muscles, improving endurance, exercising cognitive function, and reaction speed help prevent falls (Nelson et al., 2007; Zhang et al., 2015; Chantanachai et al., 2021). These elements are an integral part of the recommended holistic approach to maintaining physical and psychosocial fitness in the elderly. Regular balance training in older people contributes significantly to improving stability, reducing the risk of balance loss and falls (Marzetti et al., 2017).
Among the elderly, the limited variety of exercises and their repetition is often the cause of lack of commitment and boredom. Therefore, modern training systems have begun to be introduced to complement conventional work methods and provide the much-desired element of positive and strong motivation (Evans, 1999; Ehrari et al., 2020). The dynamic development of IT/ICT technologies (information technology/information communications technology) and their use also allows the elderly to enter a new digital world – attractive virtual reality – creating an atmosphere of curiosity, even enjoyment, and a significant increase in motivation for regular exercise both in clinical facilities and at home under the supervision of a physiotherapist. Many systems have already been developed to serve these purposes by incorporating virtual reality (VR) into physical activity work. One of these is the ActivLife platform used in our study. It is tailored to prevent falls, especially in people at high risk of falling, providing appropriate and safe support/training and, just as importantly, cognitive support. The system offers a variety of physical exercises, also including a variety of tasks to improve cognitive function. This combination of activities allows us to treat elderly persons precisely holistically, and their health as a complex phenomenon, where physical health is also influenced by emotional wellbeing and cognitive health. The proposed exercises and tasks allow participants/seniors to activate each muscle group, improve joint mobility, and enhance fitness using an attractive form of interactive games, cognitively engaging and creating an atmosphere of fun. However, being in virtual environments (VEs) can be associated with adverse symptoms of cybersickness (Séba et al., 2023; Kourtesis et al., 2024). This is more often experienced by immersive VE participants, and very rarely by non-immersive VR users (Venkatakrishnan et al., 2023; Sokołowska, 2024). Despite these (a) unfavorable effects (Drazich et al., 2023; Dopsaj et al., 2024), but also (b) the lack of standardization of virtual tools/environments (Kourtesis et al., 2021; Porffy et al., 2022; Kim et al., 2023; Holmqvist et al., 2024), (c) researching to prepare recommendations for the use of VR in specific patient populations (Juras et al., 2019; Brassel et al., 2021; Liu et al., 2022; Rodríguez-Almagro et al., 2024), (d) discussing emerging user data protection/privacy issues and ethical dilemmas (Segkouli et al., 2023; Goldstein et al., 2024; Rudschies and Schneider, 2024), researchers and clinicians/physiotherapists highlight the enormous potential of innovative technologies (Jonson et al., 2021; Bateni et al., 2024; Moulaei et al., 2024). Today’s societies are aging at a very rapid pace, which necessitates measures to support the elderly in preventing falls and their serious consequences, including exercising cognitive function in progressive senile dementia (Barbaccia et al., 2022; Yang J. G. et al., 2022; Buele et al., 2023; Ren et al., 2024; Siette et al., 2024; Tortora et al., 2024; Wilf et al., 2024) – these actions are the future of modern clinical practice in (neuro)geriatrics.
Current research demonstrates that the application of virtual environments is effective in supporting such important balance training in older adults. Various virtual protocols are being proposed and tested, showing comparable or even greater benefits of VR training compared to traditional physical training. An important thread related to the development of novel technologies is the computational approach for evaluating the usability and effectiveness of various systems offered via VR (Cavedoni et al., 2020; Yang A. H. X. et al., 2022; Nieto et al., 2024; Veneziani et al., 2024; Wen et al., 2024). In clinical applications, machine learning algorithms are proving to be very useful (Bao et al., 2019; Eichler et al., 2022). Machine learning (ML) (a) is a type of artificial intelligence (AI) focused on building computer systems that learn from data, (b) is a powerful tool for solving problems, streamlining various complex operations, and automating tasks, and (c) has broad applications in many areas, for example, science, engineering, industry, economics, databases, healthcare, and medicine (Michalski et al., 2013; Alpaydin, 2016; Zhu et al., 2020; Sarker, 2021; Singh et al., 2021; Barton et al., 2024; Haimovich et al., 2024; Khalid et al., 2024). ML offers a wide range of techniques, such as decision trees, rule induction, neural networks, support vector machines (SVMs), clustering and classification methods, association rules, feature selection procedures, visualization, graphical models, or genetic algorithms; which are many more complex and use techniques well beyond traditional statistical techniques [i.e., hypothesis testing, experimental design, ANOVA, linear/logistic regression, generalized linear model (GLM), or principal component analysis (PCA)] (Mitchel, 1997; Ben-David and Shalev-Shwartz, 2014; Marsland, 2015; Arnold et al., 2019; Bradley and Trevor, 2021).
Moreover, in the context of the presented significant and already global problem of aging and the consequences of falls among seniors, methods for assessing balance and developing effective methods of maintaining it in various situations are important (Silva et al., 2017; Lo et al., 2019; Roshdibenam et al., 2021; Albites-Sanabria et al., 2024; Song et al., 2024). Posturographic techniques are often used for this purpose (Phu et al., 2019; Błaszczyk and Beck, 2023; Liang et al., 2024; Pennone et al., 2024), also in our research relies on posturography (Sokołowska et al., 2015, 2018; Sadura-Sieklucka et al., 2023).
The study aimed to evaluate and compare the effectiveness of training using a non-immersive virtual environment, such as balance-strength training, but additionally balance-cognitive training, in preventing balance loss and fall risk in older adults. The effect analysis proposed an approach using ML methods, which are increasingly used in medical applications of new technologies due to their high effectiveness.
The study included 36 women aged 62–87 who were patients of the National Institute of Geriatrics, Rheumatology and Rehabilitation in Warsaw. Before starting the training program, they were randomly assigned to two groups, with only the experimenter having knowledge of the type of group. Eighteen of them took part in balance-strength training (VR BST), and 18 in balance-cognitive training (VR BCT) using the ActivLife virtual platform (Alreh Medical, Inc., Poland). The mean age of the participants was 73.8 ± 6.2 years, height 1.61 ± 0.05 m, and weight 68.9 ± 10.6 kg. In the group with balance-strength training, the age was 73.9 ± 6.1 years, height 1.62 ± 0.04 m and weight 69.8 ± 10.2 kg. In the group with balance-cognition, age was 73.7 ± 6.6 years, height 1.60 ± 0.05 m and weight 67.9 ± 11.2 kg. Inclusion criteria for the study were age over 60 and the ability to move independently (Stuckenschneider et al., 2023). The subjects had no history of falls. Exclusion criteria included persistent or transient disturbance of consciousness, moderate and severe dementia, advanced hearing loss and visual impairment, or a serious condition of the subjects due to serious illness or major life events. The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of the National Institute of Geriatrics, Rheumatology and Rehabilitation in Warsaw for research involving humans, no. KBT-2/2/2023. All subjects gave written consent to participate in the study.
The study used standardized tests and examined static and dynamic balance, and lower limb strength to evaluate the effectiveness of training by the Timed Up and Go (TUG) test and the five-time sit-to-stand (FTSS) test (Beck Jepsen et al., 2022; Poncumhak et al., 2023). The TUG test involves getting up from a standard chair, walking a distance of 3 m, turning around, returning to the chair, and sitting. The FTSS test involves sitting and standing up straight 5 times as quickly as possible, with no breaks in between, in addition to arms crossed over the chest (Buatois et al., 2010). For these tests, lower times mean better scores and the risk of recurrent falls corresponds to times >15 s. The study assessed participants for fall risk based on the TUG test with a cutoff point of 10 s; above this value, the test subjects were classified as having an increased risk of falling (Podsiadlo and Richardson, 1991). The tests were always conducted by the same experimenter using a stopwatch.
Static posturography can be used as an objective tool to complement clinical balance tests to assess and control balance (Błaszczyk and Beck, 2023). The posturography exam was performed with a 30-s Romberg test with eyes open (EO) and eyes closed (EC), using a FreeMed Maxi posturography mat (Koordynacja, Inc., Poland) by the same experimenter. The Romberg test is performed as follows: (a) the subject stands with feet together, eyes open and hands spread to the sides, and then (b) the subject closes the eyes while the examiner observes the person for 30 s. An important feature of this test is that the person becomes more unsteady with eyes closed. The FreeMed Maxi consists of a plate equipped with sensors that measure the distribution of pressure force and changes in the projection of the center of pressure (COP) on the support surface. The body sways can be translated into COP values in the medial-lateral and anterior-posterior directions, and the trajectory (stabilogram/posturogram) represents the displacement of COP in these two directions, projection onto the X and Y axis, respectively, during the posturographic exam (Sokołowska et al., 2018; Sadura-Sieklucka et al., 2023). The following COP trajectory (posturogram) parameters were recorded and calculated: total COP path length (TL), average COP velocity (V), COP ellipse area (predictive ellipse area with 95% COP values) (EA), and two lengths of directional components of sways in left-to-right frontal and forward-backward plane movements (LRL and FBL, respectively).
In the present study, clinical tests (TUG, FTSS, and Romberg with EO and EC) were conducted twice, i.e., before participation in a 10-day training program using a non-immersive virtual environment and immediately after its completion. The training sessions used the ActivLife platform, which offers various virtual physical and cognitive exercises. The ActivLife system consists of a parapodium-based frame equipped with a corset with a seat and an integrated GymUp system (to assist in getting up from a squat), a large screen and a Kinect 3D camera, as shown in Figure 1.

Figure 1. View of ActiveLive set with a GymUp technology corset, screen, and Kinect 3D camera. (The material comes from our NIGRiR repository).
The outcome measures were as follows: (a) the primary outcome was functional balance assessed by TUG and FTSS scores and (b) the secondary outcomes were static balance parameters assessed by the posturographic trajectory pattern in the Romberg test with EO and EC.
The subjects participated in a 10-day program that included conventional physical training and exercises in a VE created by the ActivLife platform. A single session lasted about 30 min. Each group included 15 min of exercises on a bicycle ergometer, followed by 15 min of exercises aimed at improving lower limb strength, trunk stabilization, and balance in balance-strength training in group 1 (Figure 2), corresponding strength and cognitive exercises in balance-cognitive training in group 2 (Figure 3). The progression of exercises in subsequent sessions of the program consisted of increasing their intensity, the speed at which each exercise/task was performed, and increasing the number of repetitions. One of the common and effective machine learning algorithms, based on the k-nearest neighbors (k-NN) learning rule, was used to evaluate the effects of the training program.

Figure 2. Illustration of a virtual balance-strength training session. The left panel presents the “Right Leg Push-up” exercise. The starting position is a standing position with hands resting freely on the handle. The exercise aims to inflate the car tire as quickly as possible by bending the knee and hip joints. Increasing the difficulty of an exercise increases its duration. The right panel presents the “Stairs” exercise. The starting position is standing and the hands hold specially adapted handles. The exercise aims to climb the appropriate number of stairs by performing a full squat and returning to the starting position. The difficulty level of the exercise concerns increasing its frequency, i.e., shortening the interval between steps and increasing the number of steps. (The material comes from our NIGRiR repository).

Figure 3. Illustration of a virtual balance-cognitive training session. The left panel shows the “Counting” exercise. The starting position is standing with arms along the body. The exercise aims to reflect the number on the side by adding bags. The bags are added up by touching and highlighting them. The difficulty level of the task concerns increasing the range of numbers. The right panel illustrates the “Ambulance” exercise. The starting position is with arms resting freely, and the exercise is aimed at avoiding cars in front of the ambulance by side-bending the torso. Increasing the difficulty level of the task is to accelerate the ambulance and reduce the distance between the cars. (The material comes from our NIGRiR repository).
Machine learning is often classified by the way an algorithm learns to become more accurate in its predictions. There are four basic types of machine learning, such as supervised, unsupervised, semi-supervised, and reinforcement learning (Bishop, 2006; Kroese et al., 2019; Alnuaimi and Albaldawi, 2024a,b). In supervised learning, data scientists provide algorithms with labeled training data and define variables. Both the input and output of the algorithm are specified in supervised learning. There are several supervised learning algorithms. Some of the commonly used algorithms of supervised learning are k-NN, naive Bayes classifiers, decision trees, logistic regression, and SVMs (Hastie et al., 2009; Pandey et al., 2019).
The k-NN is a non-parametric supervised learning classifier that uses proximity to make classifications or predictions about the grouping of an individual data point (an object), which is simple to implement, performs well in practice and can be easily extended to new data. In classification problems, the class label is assigned based on the majority vote – i.e., the label that is most frequently represented around a given data point is used, as shown in Figure 4 (Devijver and Kittler, 1982; Duda et al., 2000; Jain et al., 2000). The classifier quality criterion, depending on the number of the k-nearest neighbors, is called the error or misclassification rate (Er), defined as Er = m/n, where m is the number of misclassified objects, and n is the total number of the objects in the reference set. The Er is calculated for all possible values of k using the leave-one-out method (Duda et al., 2000). A value of k should be determined in such a way that offers the smallest probability of misclassification. The lower the Er, the easier it is to differentiate classes. The k-NN makes no assumptions about the data, which means it can be used to solve a wide variety of problems (Figure 5).
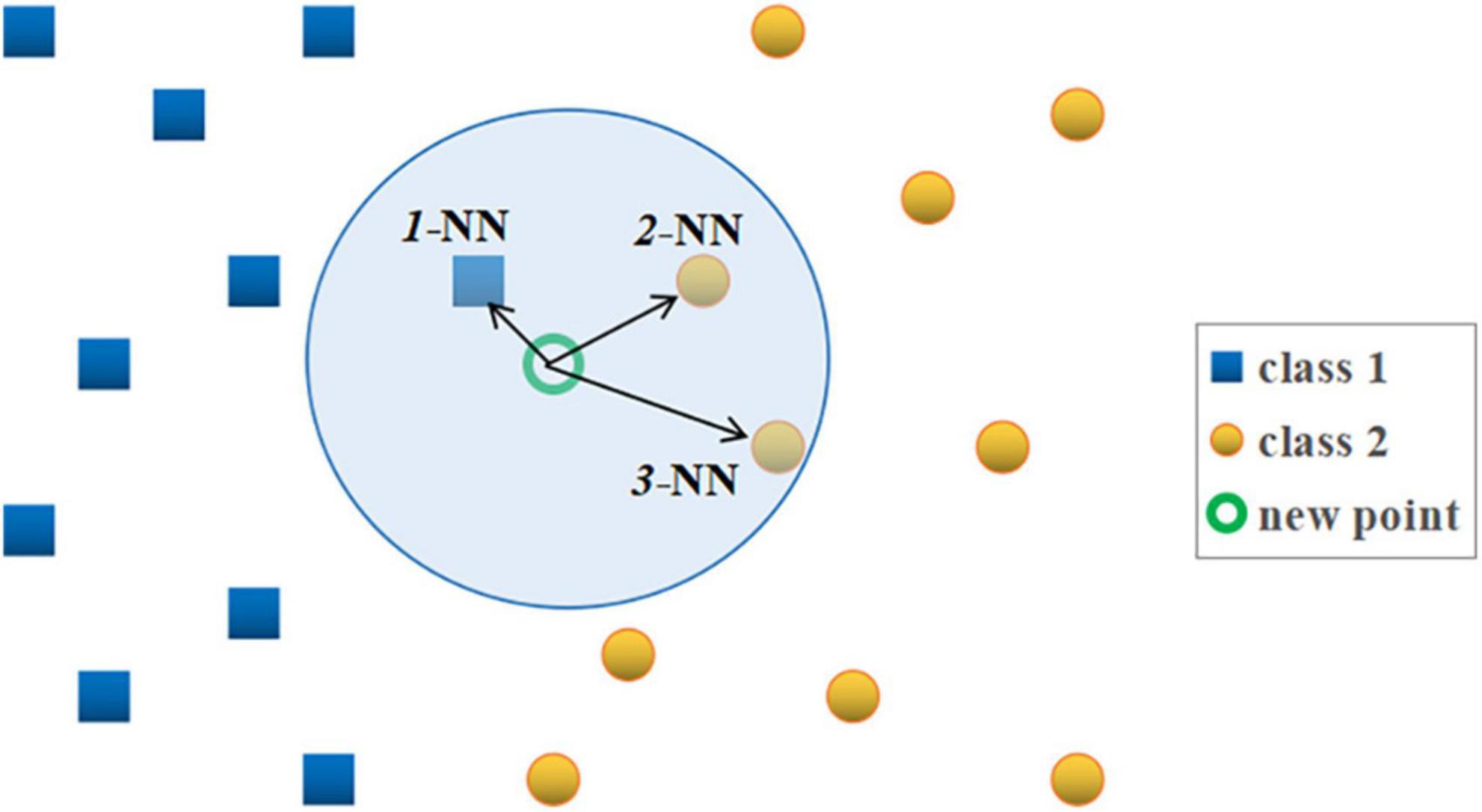
Figure 4. Illustration of the standard k-NN rule. “Blue cube” – points belonging to class 1 and “yellow ball” – points belonging to class 2. The symbols 1-NN, 2-NN, and 3-NN stand for the first, second and third nearest neighbor of the new classified point (marked with a “green circle”), respectively. According to the 3-NN rule, the new point “circle” is assigned to class 2, since two, out of its three nearest neighbors are from class 2 (“cube” – points from class 1, “ball” – points belonging to class 2).
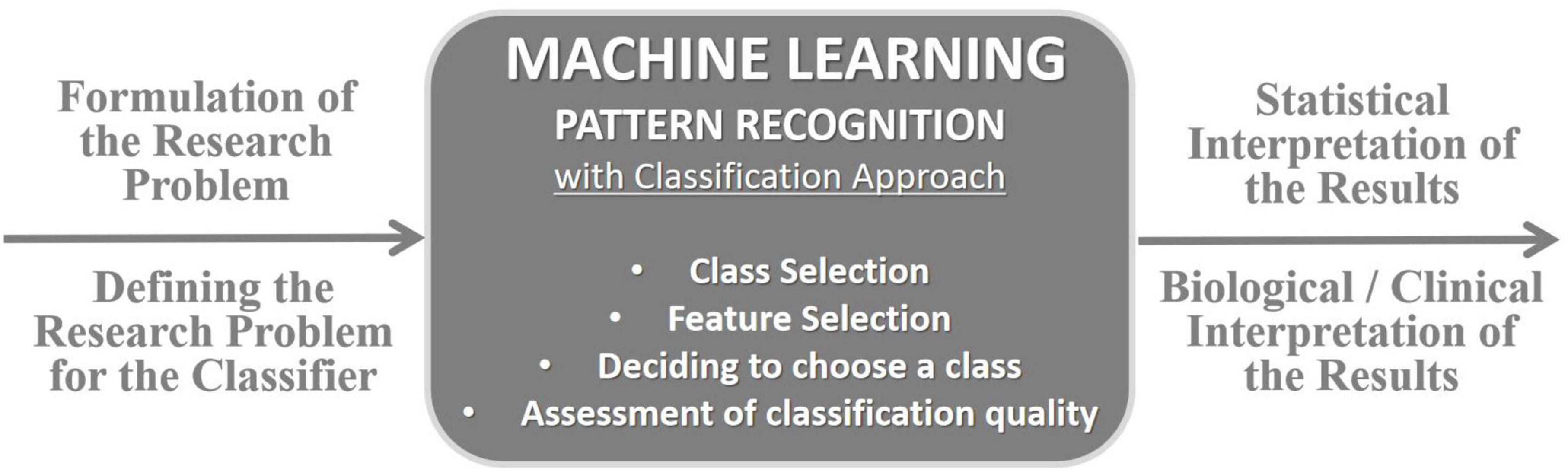
Figure 5. Model of analysis approach based on machine learning with supervised classification employed in our research, e.g., in Sokolowska and Jozwik (2007), Maciejewska et al. (2008), Sokołowska et al. (2008, 2018), Jóźwik et al. (2011), and Sokołowska and Sokołowska (2019).
In agreement with the aim of the study, in the analysis using the k-NN classifier, two classes were defined corresponding to the two test groups: class 1 was the balance-strength training group (VR BST), and class 2 was the balance-cognitive one (VR BCT), which additionally takes into account an important cognitive component in balance training. Both primary clinical and secondary posturographic outcomes were analyzed. Based on the posturographic measurements, the effects before and after 10 VR sessions were analyzed: feature 1 – total length of the posturographic trajectory (TL), feature 2 – velocity of body swings (V), feature 3 – ellipse area of the trajectory (EA), feature 4 – length of left-to-right frontal plane motions, as X displacement (LRL), and feature 5 – length of the forward-backward length of movements in the sagittal plane, as Y displacement (FBL). The analysis was performed for the Romberg test with EO and EC, additionally without and with the feature selection procedure (to indicate the features most strongly related to the classes). The redundant features make the classification more complex and spoil its performance. For this reason, the feature selection is recommended. We should select the feature set, out of all available features, which offers the minimum value of the error rate for the optimum k-NN rule. A similar analytical approach was used in our research using a posturography platform, e.g., in Sokołowska et al. (2015, 2018), Sadura-Sieklucka et al. (2023), among others. Figures 4, 5 illustrate the operation of the k-nearest neighbors rule and the classification model approach adopted in our research.
The statistical package STATISTICA (StatSoft Poland Inc., version 12) was used, as well as computational algorithms based on the standard k-NN learning rule (for Euclidean distance) and the leave-one-out method for assessing the quality of classification, and also a feature selection procedure. These algorithms are presented and described in Maciejewska et al. (2008), Jóźwik et al. (2011), Sokołowska et al. (2018), among others. Additionally, the analysis used (a) a two-factor repeated measures ANOVA with the Tukey HSD test as a post-hoc test (Table 1), and (b) a χ2 test with Yates’s correction or Fisher’s exact test (Table 3) to assess the level of statistical significance of the obtained results (for two VR programs before and after VR training). A Shapiro–Wilk test was performed to evaluate the normality of parameters in each group. The value of statistical significance was p < 0.05.
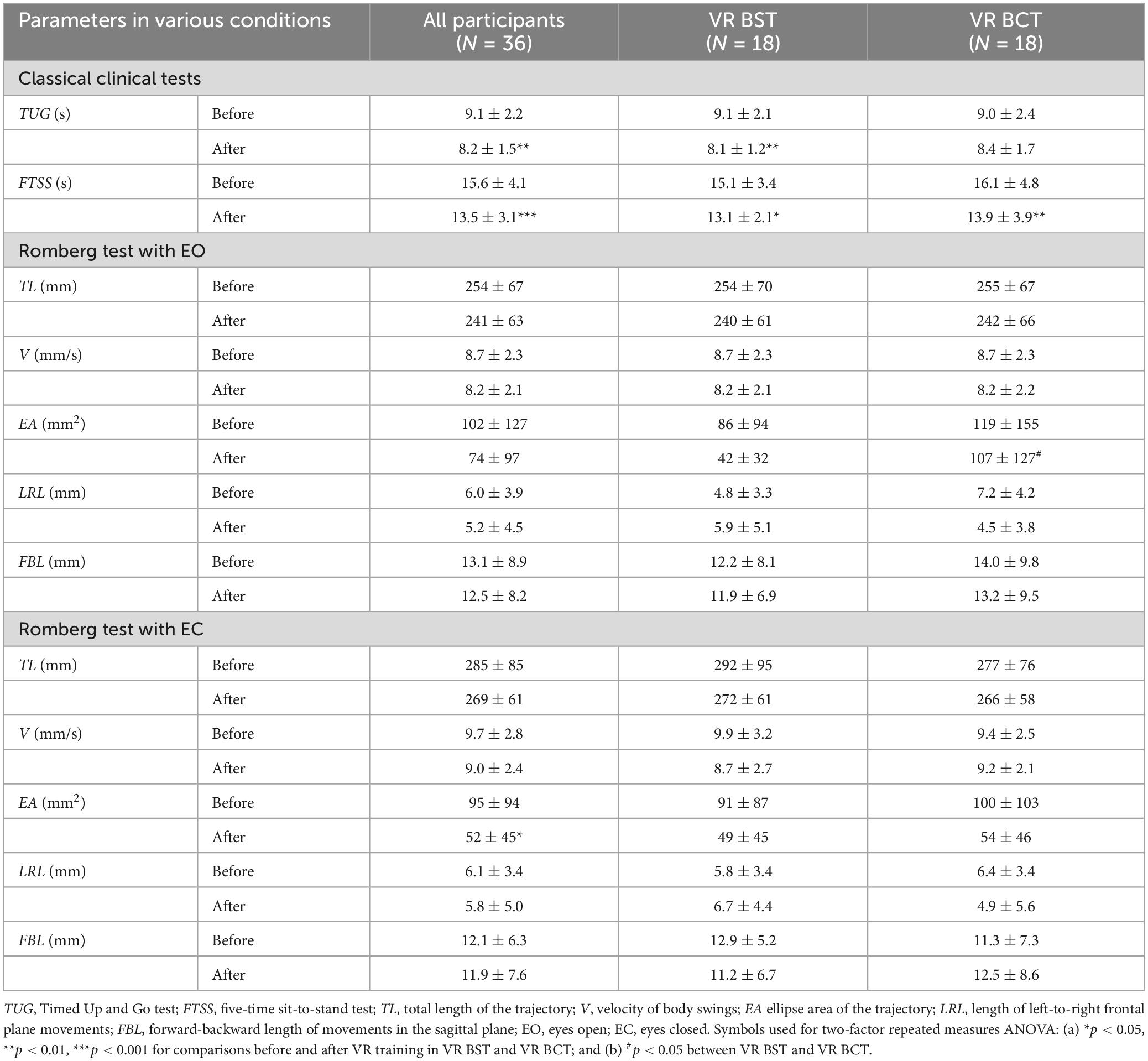
Table 1. Meanand standard deviation of parameters of clinical balance tests before and after training sessions using VR for balance-strength training (BST) and balance-cognitive training (BCT).
The results obtained by the participants in the TUG and FTSS tests before and after the 10-day training program in the non-immersive virtual environment are shown in Table 1. The results (of all participants) demonstrate statistically significant favorable changes in both tests between pre- to post-training values, from 9.1 ± 2.2 and 15.6 ± 4.1 to 8.2 ± 1.5 and 13.5 ± 3.1 s, respectively. Moreover, among the subjects, TUG test values >10 s were found in 13 subjects (36%) before training (7 in group 1 and 6 in group 2), and after training in only two of them (6%) (one each in both groups). These changes indicate a statistically significant reduction in the risk of falls in individuals from both groups (p = 0.0015). However, the observed differences in these clinical tests between the two training groups are small and do not reach statistical significance. This indicates similarly favorable effects achieved by exercise participants in groups 1 and 2, i.e., equally effective fall prevention and balance maintenance. Table 1 also presents the results of the Romberg test with eyes open and closed for posturographic trajectory parameters, and showed non-significant differences between both virtual training sessions, except the EA parameter during EO, whose value significantly decreases after VR BST compared to VR BCT, i.e., (a) before 86 ± 94 versus 119 ± 155 mm2 (p = 0.453), and (b) after 42 ± 32 versus 107 ± 127 mm2 (p = 0.043), respectively. In turn, the same parameter in the EC test decreased statistically significantly after the virtual program (of all participants), i.e., from 95 ± 94 (value before) to 52 ± 45 mm2 (value after) (p = 0.014), but this change does not reach statistical significance in either VR BST (from 91 ± 87 to 49 ± 45 mm2, p = 0.079) or VR BCT (from 100 ± 103 to 54 ± 46 mm2, p = 0.093) independently.
An analytical model based on machine learning algorithms with supervised learning, i.e., a k-NN classifier with known class membership, was proposed and used to evaluate the effects of the VR program. The estimation was based primarily on class recognition of the posturographic trajectory pattern. Table 2 shows the results of distinguishing the training program into two classes, class 1 – virtual balance-strength training (VR BST) and class 2 – virtual balance-cognitive training (VR BCT) for each feature independently, i.e., recorded/calculated posturographic parameters. Table 3 shows the results of analyzing a set of all these features together before and after feature selection, indicating the features that best differentiate the classes (feature selection reduced the error rate). Table 4 summarizes the results of the k-NN-based classification (after feature selection) in the form of confusion and confidence matrices.
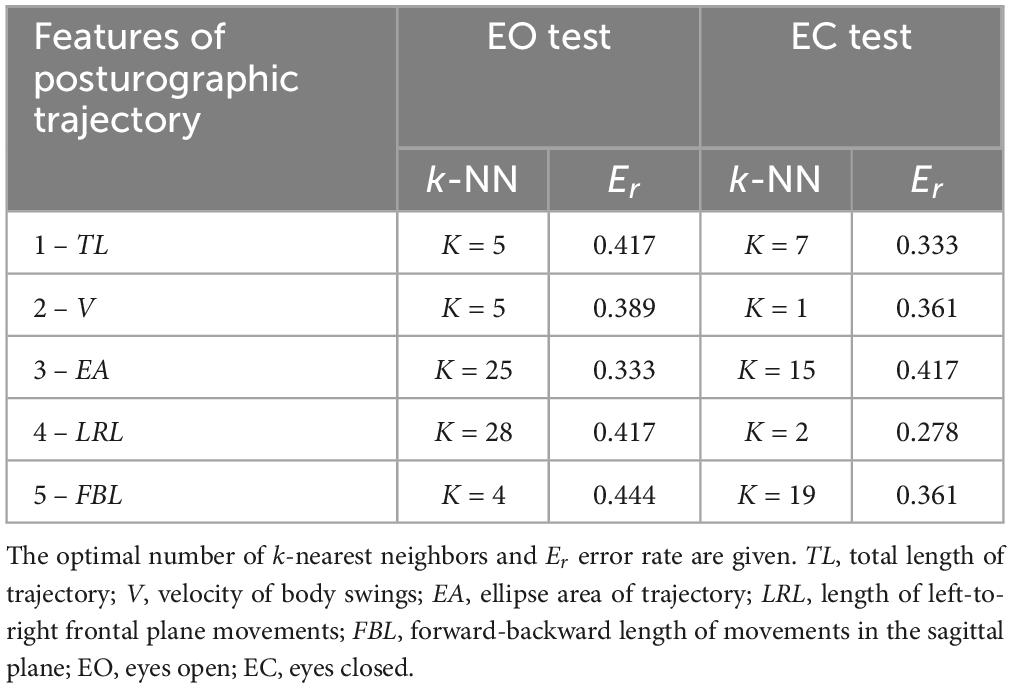
Table 2. Results of the k-NN analysis for single posturographic features/parameters in distinguishing between two classes, corresponding to VR BST and VR BCT (for EO and EC tests).
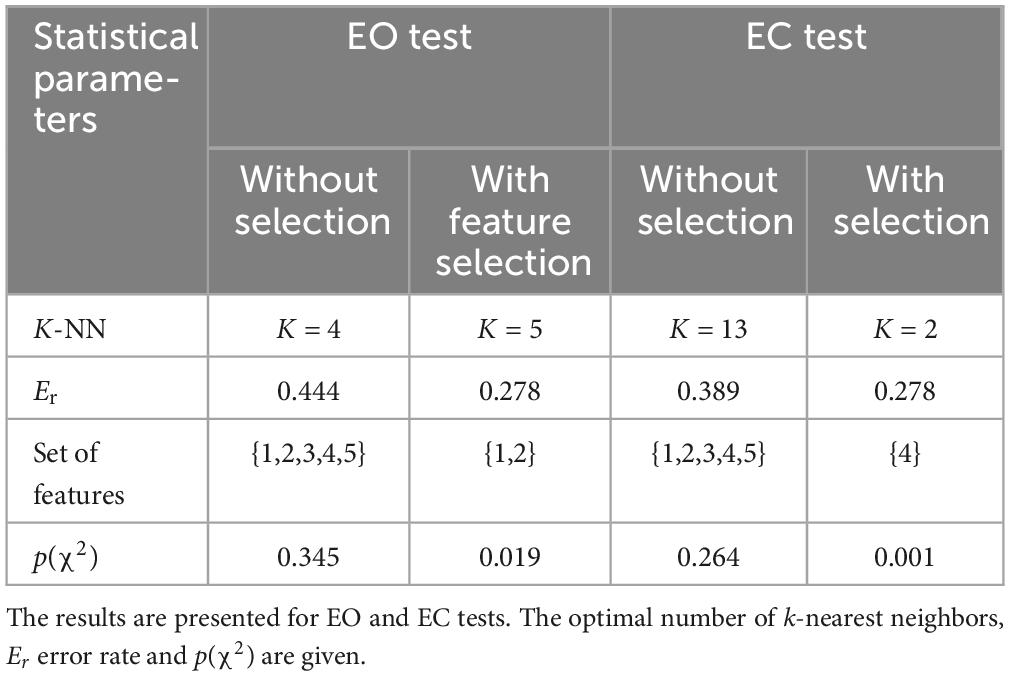
Table 3. Results of k-NN analysis for the full set of features/posturographic parameters in distinguishing two classes, corresponding to VR BST and VR BCT, without and with feature selection.
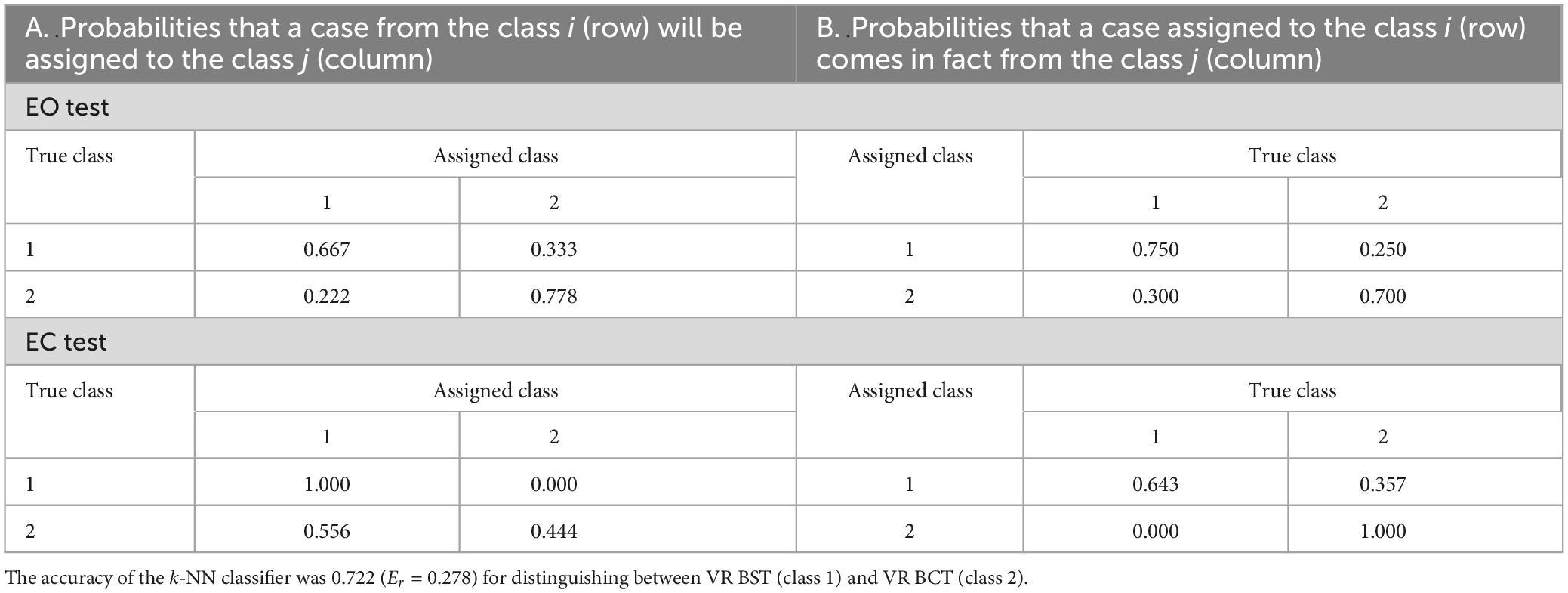
Table 4. Confusion (panel A) and confidence (panel B) matrices for a priori and a posteriori probabilities for selected posturographic features for EO ({TL,V}) and EC ({LRL}) tests.
As shown in Table 2, in the posturography exam with EO, lower misclassification errors (Er) are offered by single features no. 2 and 3, relating the parameters of V and EA. However, in the EC test, lower Er values (compared to the EO test) were observed for other features no. 1 and 4, corresponding to TL and LRL. Additional differentiation (not shown in the table) of the two virtual training according to the TUG test yields an Er equal to 0.333 (3-NN), and Er = 0.361 (4-NN) according to the FTSS test. The set of these clinical tests together {TUG,FTSS} gives an Er equal to 0.361 (6-NN). Therefore, it is more effective to distinguish between classes according to the TUG feature, correctly identifying both classes in 67% (p = 0.046). As Table 3 shows, considering all features (all posturographic parameters), i.e., the set of features {1,2,3,4,5}, yields a large Er (0.444 in the EO test and a slightly lower 0.389 in the EC one). This situation is improved by the feature selection, which also indicates important parameters in recognizing training effects (classes considered). After feature selection, a set of two features {1,2} is significant in the EO test, i.e., TL and V (Er = 0.278). In the EC test, a single feature no. 4, i.e., LRL, at the same Er differentiated the two classes. As shown in Table 4, the confusion matrix for selected features (i.e., panel A for a priori probabilities), (a) can be seen that (a) the fraction of correct decision was obtained for class 1, 0.667 for the EO test and 1.000 for the EC test, (b) for class 2 was 0.778 for EO and only 0.444 for EC. In addition, panel B also shows a confidence matrix (for a posteriori probabilities), i.e., the probabilities that the case assigned to a row class comes, in fact, from a column class. As can be seen, (a) in the case of EO, slightly more correct assignment decisions apply to class 1 compared to class 2 (the probabilities of correct decisions are 0.750 and 0.700, respectively, (b) while for EC, class 2 was precisely assigned (1.000), class 1 was correctly assigned with a probability of 0.643. The accuracy of the k-NN classifier in distinguishing between VR BST and VR BCT was 0.722 (Er = 0.278).
As expected, while differentiating the effects of virtual sessions, the inclusion of two additional features in the considered set of posturographic features (related to the TUG and FTSS tests) does not improve the results based on the posturographic pattern. For such an extended set of features, Er = 0.472 (13-NN) was obtained in the EO test and Er = 0.472 (8-NN) in the EC test, and after feature selection, those lower values of 0.278 (9-NN) and 0.333 (1-NN) were observed, respectively.
All participants reported that the exercises were attractive and engaging. None of them experienced adverse virtual symptoms during the VR program.
Our research deals with a computational approach based on machine learning algorithms in the very timely topic of using cutting-edge VR-based technologies to prevent falls, a very serious problem in the elderly. The study involved 36 women aged 62–87. They participated in two different training sessions with the same non-immersive VR platform designed for fall prevention training, i.e., VR BST (n = 18) and VR BCT (n = 18). The main difference between the VR sessions was the inclusion of cognitive tasks in the VR BCT in addition to the required strength exercises. The results of classical clinical tests such as the TUG and FTSS showed similarly beneficial effects of both virtual training. Clinical Romberg tests along with posturographic trajectory pattern analysis were also used to evaluate the effects of virtual training. The analytical model was based on both classical statistics and the ML supervised learning algorithm with the k-NN classifier. Distinguishing the effects of VR BST and VR BCT was a difficult task for the classifier, which it handled well, achieving an accuracy of 0.722 (72%) based on a set of posturographic features/parameters along with the use of a feature selection procedure. In the classical statistical analysis, the vast majority of comparisons did not reach statistical significance.
This was due, among other things, to the fact that there were common elements of exercising motor functions (in terms of balance, coordination, and reaction speed) to maintain a stable posture in both proposed training sessions. The training programs were designed to effectively support individuals at (high) risk of falling (in the case of the presented study of seniors). It is worth emphasizing that posturography is one of the objective methods/techniques of evaluating the human balance system both in healthy and unhealthy individuals (Lipowicz et al., 2023; Oczadło et al., 2023). In particular, static posturography is a simple non-invasive technique commonly used in modern laboratories and clinics to quantify the adaptive mechanisms of the central nervous system involved in postural and balance control (Błaszczyk and Beck, 2023). The main value of a posturography exam is the objective information it provides, making it possible to evaluate: (a) different sensory systems involved in balance (vestibular, visual, and somatosensory), (b) changes of automatic and voluntary motor responses, (c) postural strategies, (d) deviations from the center of gravity, and (e) changes of limits of stability (Schubert et al., 2012a,b; Błaszczyk and Beck, 2023; Oczadło et al., 2023). Posturography is, therefore, an adequate tool for conducting our research with seniors, both now and in the future [including dynamic or virtual posturography (Sokołowska et al., 2020, 2022)]. As expected, the results show that choosing a posturographic exam with the Romberg test with EO, that is, under the subjects’ visual control, effective in analyzing body swings in terms of total trajectory length and sway velocity. Other, slightly more favorable balance-stabilizing changes compared to VR BST (group 1) were observed in VR BCT (group 2), with slightly smaller swings and velocities on average. They allowed 78% of participants in this group to be identified (p = 0.019). On the other hand, the results of the EC test (in the absence of visual control) indicate another change in the pattern by a slight decrease in the average LRL in group 2, while it increases in group 1. This direction of change allows 100% of participants in group 1 to be identified (p = 0.0014) and is probably due to the predominance of motor tasks and, consequently, the greater ranges of motion required in balance-strength tasks compared to group 2 in balance-cognitive tasks.
Summarizing the results of our study, we note that both virtual training sessions, according to the results of the clinical TUG and FTSS tests, are effective in reducing the risk of falls and balance loss in participants. As Bohannon points out (Bohannon, 2006), the FTSS test is used to assess the functional capabilities of the elderly population. Both training programs also exercised the lower limbs, resulting in improved scores on the FTSS one. In our study, we observed slightly different directions of changes in the pattern describing posturographic trajectories in the two VR training groups based on the posturographic exam with EO and EC in the Romberg test. This indicates that the strategies developed by the participants in the VR BST and the VR BCT were slightly different. It should also be noted that both training programs proved equally effective in achieving the stated goal of the 10-day sessions using the VE, i.e., reducing the risk of falls and postural stabilization. Those who took part in the training did not experience any symptoms related to the use of VR. They also all found the activities attractive and were eager to participate. For example, Liang et al. (2024) also demonstrated the effectiveness of the ML (machine learning) and XAI (explainable artificial intelligence) approach with (static) posturographic parameters to classify fall risk based on TUG scores in older adults. Bao et al. (2019), on the other hand, in their study, proposed an automated balance assessment using trunk sway data and ML methods. Their model, evaluated in a leave-one-participant-out scheme, achieved a classification accuracy of 82%. The authors suggested that the ML technique could provide accurate assessments during standing balance exercises. Such automated assessments could reduce physiotherapists’ consultation time and increase users’ adherence to recommendations outside the clinic. This research model may also be a good suggestion for balance assessments, such as home programs/exercises for the elderly in fall prevention. In turn, Eichler et al. (2022) also noted the importance of developing automation of fall risk assessment in an efficient and non-invasive way, especially in older adults. This approach could provide a basis for screening individuals for fall risk and determining their need for participation in fall prevention programs. The authors proposed an automated and effective fall risk evaluation system based on a human motion tracking system using a multi-depth camera and the validated Berg Balance Scale (BBS). Trained machine learning classifiers predict the subjects’ 14 scores for BBS tasks. In addition, researchers proposed their efficient BBS system (referred to as E-BBS), which reduces the number of tasks in a conventional BBS test by about 50% (from 14 to just 4–6 tasks) while maintaining 97% accuracy. The authors concluded that their ML-based approach enables the effective diagnosis/recognition of people at risk of falling in a way that does not require significant time or resources from the medical community. The researchers emphasize that the technology and ML algorithms can be implemented in other sets of clinical tests and evaluations. An example of such a universal approach using ML methods can be seen in our current (and previous) research. Interesting results are presented by Yousefi Babadi and Daneshmandi (2021), who analyzed the effect of VR compared to conventional balance training on the balance of elderly people. The researchers showed that after the intervention/training, there were significant improvements in both groups (p < 0.05), and the beneficial changes were similar (p > 0.05). The authors concluded that both VR and conventional balance training methods are equally effective. They also suggested that VR training programs could be used as a new home training method to improve the balance of the elderly. The researchers also pointed out important facts such as that (a) VR training is a fun way to improve physical activity for the older participants, and (b) VR is a great way to simulate movement and transfer it to real-world tasks. A study by Lima Rebêlo et al. (2021) found that immersive VR was effective in rehabilitating older adults with balance disorders and fall risk, and similarly, VR training (VRT) was no better than conventional physiotherapy. Moreover, improvements in functional balance after 2 months were maintained after both trainings. In contrast, Liu et al. (2022) quantitatively analyzed the effects of VRT on functional mobility and balance in healthy older adults in their systematic review and meta-analysis, conducted in 15 studies on a total of 704 participants. The analysis showed that compared to traditional physical therapy (TPT), VRT significantly improved TUG. The researchers indicated that VRT can be more effective than TPT in improving functional mobility and balance in the study population of healthy seniors. Similarly, Rodríguez-Almagro et al. (2024) reviewed recent evidence on the effectiveness of VR in improving balance and gait among healthy older adults compared to other therapies. The researchers concluded that VR therapy was more effective than minimal intervention or usual care in improving static balance, dynamic balance, and gait in healthy seniors. The authors indicated that VR therapy gives even better results compared to conventional balance training and exercise in improving balance and gait in this senior population. The authors also confirmed the effectiveness of both virtual and conventional methods. Interesting approaches combining both forms of training are also being used. An example is the study by Sadeghi et al. (2021), which evaluated the effects of 8-week conventional balance training, virtual training, and combined exercise (MIX) in older men. The researchers demonstrated that MIX induced the greatest improvements in lower limb muscle strength, balance and functional mobility of all these workouts, and recommended that MIX is an effective method for reducing the risk of falls among older adults.
As emphasized in the Introduction, it is VEs that offer new, highly attractive, interesting, engaging, and motivating conditions (both in the clinic and at home) designed not only for short-term exercise (e.g., our study), but also provide the opportunity to exercise for longer periods, without fatigue or boredom, depending on the needs and abilities of the exercising individuals. Our research combines conventional training with a virtual environment, thus leveraging the advantages of each for the greater benefit of program participants (e.g., increasing the appeal, engagement, and direct impact of the participant on the training through an interactive game format). Since we use novel VEs in our research, it is worth noting that sometimes users in virtual worlds may experience adverse symptoms due to cybersickness (Lima Rebêlo et al., 2021; Sokołowska, 2023, 2024; Kourtesis et al., 2024). Cybersickness is accompanied by a mix of unfavorable symptoms such as headache, nausea, dizziness, fatigue, oculomotor, and postural disturbances (Kourtesis et al., 2023; Venkatakrishnan et al., 2023). An interesting overview of research on this problem using the machine learning approach was presented by Yang A. H. X. et al. (2022). ML can be used to detect them and is a step toward overcoming these adverse limitations of new technologies. The researchers concluded that while various models for detecting cybersickness have been developed, there is no model to predict early adverse events in VEs. Future, more accurate and effective ML approaches will undoubtedly be inspired by current knowledge of how the brain works, as well as the new brain/organism models/approaches being developed and linking them to these bio-digital frontiers (Benelli et al., 2023; Daşdemir, 2023; Yang et al., 2023). These and similar studies (Chang et al., 2023; Souchet et al., 2023) indicate, as does our research, that we are still at the beginning of understanding the potentially beneficial and detrimental effects of digital worlds on their users, especially older adults (Drazich et al., 2023; Séba et al., 2023).
It should also be noted that, as outlined above, ML techniques have enormous potential, particularly in computational neuroscience. These methods have several key advantages over traditional statistical techniques, including learning from data and making predictions based on patterns and relationships present/hidden in the data (Cristancho Cuervo et al., 2022). Consequently, ML methods in neuroscience and contemporary medical practice provide very effective support for accurate diagnosis (Rosenfelder et al., 2023), assessment of beneficial or adverse effects of therapy and rehabilitation (Yang A. H. X. et al., 2022), as well as natural aging using innovative IT/ICT technologies, which can effectively help maintain joy/satisfaction and good quality of life for the elderly (Yousefi Babadi and Daneshmandi, 2021).
A limitation of our study is the small number of participants. In the future, it would be necessary not only to increase the number of subjects but also to include men. The training program included only 10 sessions in the virtual environment, and increasing the number of sessions would enhance the beneficial effects, and the effects would also be worth evaluating in the longer term. A longer training period allows the exerciser to become more familiar with the techniques and develop a habit of regular physical activity, which can result in long-term maintenance of the positive effects of training (Cadore et al., 2013). Sherrington et al.’s (2017) research indicates the beneficial effects on balance and often strength after longer periods of training. Characteristic problems of the senior population are muscle weakness and balance disorders. It would be interesting to be able to continue training not only as presented in a medical facility, but also at home, under the remote supervision of a physical therapist. To put in perspective, virtual environments can simulate real-life situations and challenges related to balance and fall risks in the elderly while providing them with a safe, controlled, and engaging/motivating training environment in which they can practice and effectively improve their balance.
First, our study demonstrated the effectiveness of the proposed research approach, using a combination of traditional and VR-based balance/cognitive training, dedicated to people at high risk of falls, including seniors. Second, the results showed that the proposed VR training positively improved TUG and FTSS, i.e., a statistically significant reduction in the risk of falls in the research population of seniors. Third, the analytical approach based on machine learning algorithms is also useful in VE, not only confirming the effectiveness of the proposed virtual training but also indicating a change in the pattern of posturographic trajectory depending on the type of virtual training, VR BST or VR BCT.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by the Ethics Committee of the National Institute of Geriatrics, Rheumatology and Rehabilitation in Warsaw. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
BS: Writing –original draft, Writing –review & editing. WŚ: Writing –original draft, Writing –review & editing. ES-B: Writing –original draft, Writing –review & editing. ES: Writing –original draft, Writing –review & editing. TS-S: Writing –original draft, Writing –review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors would like to thank Alreh Medical, Inc. (Poland) for the opportunity to use the VR ActivLife platform in the presented research. The authors also thank Professor Adam Jóźwik for his cooperation in machine learning methods in various biomedical research.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Albites-Sanabria, J., Palumbo, P., Helbostad, J., Bandinelli, S., Mellone, S., Palmerini, L., et al. (2024). Real-world balance assessment while standing for fall prediction in older adults. IEEE Trans. Biomed. Eng. 71, 1076–1083. doi: 10.1109/TBME.2023.3326306
Alnuaimi, A., and Albaldawi, T. H. (2024a). “Concepts of statistical learning and classification in machine learning: An overview,” in Proceedings of the BIO Web of Conferences, Vol. 97, (Les Ulis: EDP Sciences), 00129.
Alnuaimi, A., and Albaldawi, T. H. (2024b). “An overview of machine learning classification techniques,” in Proceedings of the BIO Web of Conferences, Vol. 97, (Les Ulis: EDP Sciences), 00133.
Arnold, T., Kane, M., and Lewis, B. (2019). A Computational Approach to Statistical Learning. New York, NY: Chapman and Hall/CRC.
Bao, T., Klatt, B., Whitney, S., Sienko, K., and Wiens, J. (2019). Automatically evaluating balance: A machine learning approach. IEEE Trans. Neural. Syst. Rehabil. Eng. 27, 179–186. doi: 10.1109/TNSRE.2019.2891000
Barbaccia, V., Bravi, L., Murmura, F., Savelli, E., and Viganò, E. (2022). Mature and older adults’ perception of active ageing and the need for supporting services: Insights from a qualitative study. Int. J. Environ. Res. Public Health 19:7660. doi: 10.3390/ijerph19137660
Barton, H., Maru, A., Leaf, M., Hekman, D., Wiegmann, D., Shah, M., et al. (2024). Academic detailing as a health information technology implementation method: Supporting the design and implementation of an emergency department-based clinical decision support tool to prevent future falls. JMIR Hum. Fact. 11:e52592. doi: 10.2196/52592
Bateni, H., Carruthers, J., Mohan, R., and Pishva, S. (2024). Use of virtual reality in physical therapy as an intervention and diagnostic tool. Rehabil. Res. Pract. 2024:1122286. doi: 10.1155/2024/1122286
Beck Jepsen, D., Robinson, K., Ogliari, G., Montero-Odasso, M., Kamkar, N., Ryg, J., et al. (2022). Predicting falls in older adults: An umbrella review of instruments assessing gait, balance, and functional mobility. BMC Geriatr. 22:615. doi: 10.1186/s12877-022-03271-5
Ben-David, S., and Shalev-Shwartz, S. (2014). Understanding Machine Learning: From Theory to Algorithms. Cambridge, MA: Cambridge University Press.
Benelli, A., Neri, F., Cinti, A., Pasqualetti, P., Romanella, S., Giannotta, A., et al. (2023). Frequency-dependent reduction of cybersickness in virtual reality by transcranial oscillatory stimulation of the vestibular cortex. Neurotherapeutics 20, 1796–1807. doi: 10.1007/s13311-023-01437-6
Bischoff-Ferrari, H. (2011). The role of falls in fracture prediction. Curr. Osteoporos. Rep. 9, 116–121. doi: 10.1007/s11914-011-0059-y
Bishop, C. (2006). Pattern Recognition and Machine Learning. New York, NY: Springer, doi: 10.1007/978-0-387-45528-0
Błaszczyk, J., and Beck, M. (2023). Posturographic standards for optimal control of human standing posture. J. Hum. Kinet. 86, 7–15. doi: 10.5114/jhk/159452
Bohannon, R. (2006). Reference values for the five-repetition sit-to-stand test: A descriptive meta-analysis of data from elders. Percept. Mot. Skills 103, 215–222. doi: 10.2466/pms.103.1.215-222
Bradley, E., and Trevor, H. (2021). Computer Age Statistical Inference: Algorithms, Evidence, and Data Science. Cambridge, MA: Cambridge University Press.
Brassel, S., Power, E., Campbell, A., Brunner, M., and Togher, L. (2021). Recommendations for the design and implementation of virtual reality for acquired brain injury rehabilitation: Systematic review. J. Med. Internet Res. 23, e26344. doi: 10.2196/26344
Buatois, S., Perret-Guillaume, C., Gueguen, R., Miget, P., Vançon, G., Perrin, P., et al. (2010). A simple clinical scale to stratify risk of recurrent falls in community-dwelling adults aged 65 years and older. Phys. Ther. 90, 550–560. doi: 10.2522/ptj.20090158
Buele, J., Varela-Aldás, J., and Palacios-Navarro, G. (2023). Virtual reality applications based on instrumental activities of daily living (iADLs) for cognitive intervention in older adults: A systematic review. J. Neuroeng. Rehabil. 20:168. doi: 10.1186/s12984-023-01292-8
Cadore, E., Rodríguez-Mañas, L., Sinclair, A., and Izquierdo, M. (2013). Effects of different exercise interventions on risk of falls, gait ability, and balance in physically frail older adults: A systematic review. Rejuvenation Res. 16, 105–114. doi: 10.1089/rej.2012.1397
Carapeto, P., and Aguayo-Mazzucato, C. (2021). Effects of exercise on cellular and tissue aging. Aging 13, 14522–14543. doi: 10.18632/aging.203051
Cavedoni, S., Chirico, A., Pedroli, E., Cipresso, P., and Riva, G. (2020). Digital Biomarkers for the Early Detection of Mild Cognitive Impairment: Artificial Intelligence Meets Virtual Reality. Front. Hum. Neurosci. 14:245. doi: 10.3389/fnhum.2020.00245
Chang, E., Billinghurst, M., and Yoo, B. (2023). Brain activity during cybersickness: A scoping review. Virtual Real. 27, 2073–2097. doi: 10.1007/s10055-023-00795-y
Chantanachai, T., Sturnieks, D., Lord, S., Payne, N., Webster, L., and Taylor, M. E. (2021). Risk factors for falls in older people with cognitive impairment living in the community: Systematic review and meta-analysis. Ageing Res. Rev. 71:101452. doi: 10.1016/j.arr.2021.101452
Chen, W., Li, Y. T., Tung, T., Chen, C., and Tsai, C. (2021). The relationship between falling and fear of falling among community-dwelling elderly. Medicine 100:e26492. doi: 10.1097/MD.0000000000026492
Cristancho Cuervo, J., Delgado Saa, J., and Ripoll Solano, L. (2022). Analysis of instantaneous brain interactions contribution to a motor imagery classification task. Front. Comput. Neurosci. 16:990892. doi: 10.3389/fncom.2022.990892
Daşdemir, Y. (2023). Classification of emotional and immersive outcomes in the context of virtual reality scene interactions. Diagnostics 13:3437. doi: 10.3390/diagnostics13223437
Devijver, P., and Kittler, J. (1982). Pattern Recognition: A Statistical Approach. London: Prentice-Hall.
Dopsaj, M., Tan, W., Perovic, V., Stajic, Z., Milosavljevic, N., Paessler, S., et al. (2024). Novel neurodigital interface reduces motion sickness in virtual reality. Neurosci. Lett. 825:137692. doi: 10.1016/j.neulet.2024.137692
Drazich, B., McPherson, R., Gorman, E., Chan, T., Teleb, J., Galik, E., et al. (2023). In too deep? A systematic literature review of fully-immersive virtual reality and cybersickness among older adults. J. Am. Geriatr. Soc. 71, 3906–3915. doi: 10.1111/jgs.18553
Ehrari, H., Larsen, R., Langberg, H., and Andersen, H. (2020). Effects of playful exercise of older adults on balance and physical activity: A randomized controlled trial. J. Popul. Ageing 13(Suppl.2), 207–222. doi: 10.1007/s12062-020-09273-8
Eichler, N., Raz, S., Toledano-Shubi, A., Livne, D., Shimshoni, I., and Hel-Or, H. (2022). Automatic and efficient fall risk assessment based on machine learning. Sensors 22:1557. doi: 10.3390/s22041557
Evans, W. (1999). Exercise training guidelines for the elderly. Med. Sci. Sports Exerc. 31, 12–17. doi: 10.1097/00005768-199901000-00004
Goldstein, S., Nebeker, C., Ellis, R., and Oser, M. (2024). Ethical, legal, and social implications of digital health: A needs assessment from the Society of Behavioral Medicine to inform capacity building for behavioral scientists. Transl. Behav. Med. 14, 189–196. doi: 10.1093/tbm/ibad076
Haimovich, A., Shah, M., Southerland, L., Hwang, U., and Patterson, B. (2024). Automating risk stratification for geriatric syndromes in the emergency department. J. Am. Geriatr. Soc. 72, 258–267. doi: 10.1111/jgs.18594
Hastie, T., Tibshirani, R., and Friedman, J. (2009). The Elements of Statistical Learning: Data Mining, Inference, and Prediction, Vol. 2. New York, NY: Springer.
Holmqvist, S., Jobson, K., Desalme, D., Simone, S., Tassoni, M., McKniff, M., et al. (2024). Preliminary validation of the Virtual Kitchen Challenge as an objective and sensitive measure of everyday function associated with cerebrovascular disease. Alzheimers Dement. 16:e12547. doi: 10.1002/dad2.12547
Jain, A., Duin, R., and Mao, J. (2000). Statistical pattern recognition: A review. IEEE Trans. Pattern Anal. Mach. Intell. 22, 4–37. doi: 10.1109/34.824819
Jonson, M., Avramescu, S., Chen, D., and Alam, F. (2021). The role of virtual reality in screening, diagnosing, and rehabilitating spatial memory deficits. Front. Hum. Neurosci. 15:628818. doi: 10.3389/fnhum.2021.628818
Jóźwik, A., Sokołowska, B., Niebroj-Dobosz, I., Janik, P., and Kwieciński, H. (2011). Extraction of biomedical traits for patients with amyotrophic lateral sclerosis using parallel and hierarchical classifiers. Int. J. Biom. 3, 85–94. doi: 10.1504/IJBM.2011.037716
Juras, G., Brachman, A., Michalska, J., Kamieniarz, A., Pawłowski, M., Hadamus, A., et al. (2019). Standards of virtual reality application in balance training programs in clinical practice: A systematic review. Games Health J. 8, 101–111. doi: 10.1089/g4h.2018.0034
Khalid, U. B., Naeem, M., Stasolla, F., Syed, M., Abbas, M., and Coronato, A. (2024). Impact of AI-powered solutions in rehabilitation process: Recent improvements and future trends. Int. J. Gen. Med. 17, 943–969. doi: 10.2147/IJGM.S453903
Kim, K., Choi, J., Chin, J., Lee, B., Choi, J., and Na, D. (2023). Development and preliminary validation of a virtual reality memory test for assessing visuospatial memory. Front. Aging Neurosci. 15:1236084. doi: 10.3389/fnagi.2023.1236084
Kourtesis, P., Amir, R., Linnell, J., Argelaguet, F., and MacPherson, S. (2023). Cybersickness, cognition, & motor skills: The effects of music, gender, and gaming experience. IEEE Trans. Vis. Comput. Graph. 29, 2326–2336. doi: 10.1109/TVCG.2023.3247062
Kourtesis, P., Collina, S., Doumas, L., and MacPherson, S. (2021). Validation of the Virtual Reality Everyday Assessment Lab (VR-EAL): An immersive virtual reality neuropsychological battery with enhanced ecological validity. J. Int. Neuropsychol. Soc. 27, 181–196. doi: 10.1017/S1355617720000764
Kourtesis, P., Papadopoulou, A., and Roussos, P. (2024). Cybersickness in virtual reality: The role of individual differences, its effects on cognitive functions and motor skills, and intensity differences during and after immersion. Virtual Worlds 3, 62–93. doi: 10.3390/virtualworlds3010004
Kroese, D., Botev, Z., and Taimre, T. (2019). Data Science and Machine Learning: Mathematical and Statistical Methods. London: Chapman and Hall.
Liang, H., Ameri, R., Band, S., Chen, H., Ho, S., Zaidan, B., et al. (2024). Fall risk classification with posturographic parameters in community-dwelling older adults: A machine learning and explainable artificial intelligence approach. J. Neuroeng. Rehabil. 21:15. doi: 10.1186/s12984-024-01310-3
Lima Rebêlo, F., de Souza Silva, L., Doná, F., Sales Barreto, A., and de Souza Siqueira Quintans, J. (2021). Immersive virtual reality is effective in the rehabilitation of older adults with balance disorders: A randomized clinical trial. Exp. Gerontol. 149:111308. doi: 10.1016/j.exger.2021.111308
Lipowicz, A., Bugdol, M., Graja, K., Nowakowska-Lipiec, K., Jochymczyk-Woźniak, K., Fryc, D., et al. (2023). Relationship between body sway and body build in healthy adult men and women. Anthropol. Rev. 86, 45–61. doi: 10.18778/1898-6773.86.4.04
Liu, M., Zhou, K., Chen, Y., Zhou, L., Bao, D., and Zhou, J. (2022). Is virtual reality training more effective than traditional physical training on balance and functional mobility in healthy older adults? A systematic review and meta-analysis. Front. Hum. Neurosci. 16:843481. doi: 10.3389/fnhum.2022.843481
Lo, Y., Lynch, S., Urbanowicz, R., Olson, R., Ritter, A., Whitehouse, C., et al. (2019). Using machine learning on home health care assessments to predict fall risk. Stud. Health Technol. Inform. 264, 684–688. doi: 10.3233/SHTI190310
Lutz, W., Sanderson, W., and Scherbov, S. (2008). The coming acceleration of global population ageing. Nature 451, 716–719. doi: 10.1038/nature06516
Maciejewska, A., Jóźwik, A., Kuśmierek, J., and Sokołowska, B. (2008). Application of the k-NN classifier for mutagenesis tests. Recognition of wild type and defective in DNA repair bacterial strains on the basis of adaptive response to alkylating agents. Biocybern. Biomed. Eng. 28, 45–50.
Marsland, S. (2015). Machine Learning - An Algorithmic Perspective, 2edn Edn. London: Chapman & Hall.
Marzetti, E., Calvani, R., Tosato, M., Cesari, M., Di Bari, M., Cherubini, A., et al. (2017). Physical activity and exercise as countermeasures to physical frailty and sarcopenia. Aging Clin. Exp. Res. 29, 35–42. doi: 10.1007/s40520-016-0705-4
Michalski, R., Carbonell, J., and Mitchell, T. (2013). Machine Learning: An Artificial Intelligence Approach. Cham: Springer Science & Business Media.
Moreland, J., Richardson, J., Goldsmith, C., and Clase, C. (2004). Muscle weakness and falls in older adults: A systematic review and meta-analysis. J. Am. Geriatr. Soc. 52, 1121–1129. doi: 10.1111/j.1532-5415.2004.52310.x
Moulaei, K., Sharifi, H., Bahaadinbeigy, K., and Dinari, F. (2024). Efficacy of virtual reality-based training programs and games on the improvement of cognitive disorders in patients: A systematic review and meta-analysis. BMC Psychiatry 24:116. doi: 10.1186/s12888-024-05563-z
Nelson, M., Rejeski, W., Blair, S., Duncan, P., Judge, J., King, A., et al. (2007). Physical activity and public health in older adults: Recommendation from the American College of Sports Medicine and the American Heart Association. Circulation 116, 1094–1105. doi: 10.1161/CIRCULATIONAHA.107.185650
Nieto, N., Sánchez, J., Aguirre, M., Félix, F., and Muñoz, L. (2024). “Optimizing robotic automatic suturing through VR-enhanced data generation for reinforcement learning algorithms,” in Proceeding of the 2024 IEEE International Conference on Artificial Intelligence and eXtended and Virtual Reality (AIxVR), (Los Angeles, CA: IEEE), 375–383. doi: 10.1109/AIxVR59861.2024.00064
Oczadło, A., Kowacka, U., Lewicka, B., and Matusik, E. (2023). The applications of posturography in selected neurological disorders. Ann. Acad. Med. Siles 77, 158–165. doi: 10.18794/aams/162542
Pandey, D., Niwaria, K., and Chourasia, B. (2019). Machine learning algorithms: A review. Mach. Learn. 6, 916–922.
Pennone, J., Aguero, N., Martini, D., Mochizuki, L., and do Passo Suaide, A. (2024). Fall prediction in a quiet standing balance test via machine learning: Is it possible? PLoS One 19:e0296355. doi: 10.1371/journal.pone.0296355
Phu, S., Vogrin, S., Al Saedi, A., and Duque, G. (2019). Balance training using virtual reality improves balance and physical performance in older adults at high risk of falls. Clin. Interv. Aging. 14, 1567–1577. doi: 10.2147/CIA.S220890
Podsiadlo, D., and Richardson, S. (1991). The timed “Up & Go”: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 39, 142–148. doi: 10.1111/j.1532-5415.1991.tb01616.x
Poncumhak, P., Srithawong, A., Duangsanjun, W., and Amput, P. (2023). Comparison of the ability of static and dynamic balance tests to determine the risk of falls among older community-dwelling individuals. J. Funct. Morphol. Kinesiol. 8:43. doi: 10.3390/jfmk8020043
Porffy, L., Mehta, M., Patchitt, J., Boussebaa, C., Brett, J., D’Oliveira, T., et al. (2022). A novel virtual reality assessment of functional cognition: Validation study. J. Med. Internet Res. 24:e27641. doi: 10.2196/27641
Ren, Y., Wang, Q., Liu, H., Wang, G., and Lu, A. (2024). Effects of immersive and non-immersive virtual reality-based rehabilitation training on cognition, motor function, and daily functioning in patients with mild cognitive impairment or dementia: A systematic review and meta-analysis. Clin. Rehabil. 38, 305–321. doi: 10.1177/02692155231213476
Rodríguez-Almagro, D., Achalandabaso-Ochoa, A., Ibáñez-Vera, A., Góngora-Rodríguez, J., and Rodríguez-Huguet, M. (2024). Effectiveness of virtual reality therapy on balance and gait in the elderly: A systematic review. Healthcare 12:158. doi: 10.3390/healthcare12020158
Rosenfelder, M., Spiliopoulou, M., Hoppenstedt, B., Pryss, R., Fissler, P., Della Piedra Walter, M., et al. (2023). Stability of mental motor-imagery classification in EEG depends on the choice of classifier model and experiment design, but not on signal preprocessing. Front. Comput. Neurosci. 17:1142948. doi: 10.3389/fncom.2023.1142948
Roshdibenam, V., Jogerst, G., Butler, N., and Baek, S. (2021). Machine learning prediction of fall risk in older adults using timed up and go test kinematics. Sensors 21:3481. doi: 10.3390/s21103481
Rubenstein, L. (2006). Falls in older people: Epidemiology, risk factors and strategies for prevention. Age Ageing 35(Suppl.2), ii37–ii41. doi: 10.1093/ageing/afl084
Rudschies, C., and Schneider, I. (2024). Ethical, legal, and social implications (ELSI) of virtual agents and virtual reality in healthcare. Soc. Sci. Med. 340:116483. doi: 10.1016/j.socscimed.2023.116483
Sadeghi, H., Jehu, D., Daneshj, A., Shakoor, E., Razeghi, M., Amani, A., et al. (2021). Effects of 8 weeks of balance training, virtual reality training, and combined exercise on lower limb muscle strength, balance, and functional mobility among older men: A randomized controlled trial. Sports Health 13, 606–612. doi: 10.1177/1941738120986803
Sadura-Sieklucka, T., Czerwosz, L., Kądalska, E., Kożuchowski, M., Księżopolska-Orłowska, K., and Targowski, T. (2023). Is balance training using biofeedback effective in the prophylaxis of falls in women over the age of 65? Brain Sci. 13:629. doi: 10.3390/brainsci13040629
Sanderson, W., and Scherbov, S. (2010). Demography. Remeasuring aging. Science 329, 1287–1288. doi: 10.1126/science.1193647
Sarker, I. (2021). Machine learning: Algorithms, real-world applications and research directions. SN Comput. Sci. 2:160. doi: 10.1007/s42979-021-00592-x
Schubert, P., Kirchner, M., Schmidtbleicher, D., and Haas, C. (2012a). About the structure of posturography: Sampling duration, parametrization, focus of attention (part I). J. Biomed. Sci. Eng. 5, 496–507. doi: 10.4236/jbise.2012.59062
Schubert, P., Kirchner, M., Schmidtbleicher, D., and Haas, C. (2012b). About the structure of posturography: Sampling duration, parametrization, focus of attention (part II). J. Biomed. Sci. Eng. 5, 508–516. doi: 10.4236/jbise.2012.59063
Séba, M., Maillot, P., Hanneton, S., and Dietrich, G. (2023). Influence of normal aging and multisensory data fusion on cybersickness and postural adaptation in immersive. Virtual Real. Sens. 23:9414. doi: 10.3390/s23239414
Segkouli, S., Giakoumis, D., Votis, K., Triantafyllidis, A., Paliokas, I., and Tzovaras, D. (2023). Smart Workplaces for older adults: Coping ‘ethically’ with technology pervasiveness. Univers. Access Inf. Soc. 22, 37–49. doi: 10.1007/s10209-021-00829-9
Sherrington, C., Michaleff, Z., Fairhall, N., Paul, S., Tiedemann, A., Whitney, J., et al. (2017). Exercise to prevent falls in older adults: An updated systematic review and meta-analysis. Br. J. Sports Med. 51, 1750–1758. doi: 10.1136/bjsports-2016-096547
Siette, J., Campbell, C., Adam, P., and Harris, C. (2024). Exploring the usability of the virtual reality module LEAF CAFÉ: A qualitative think-aloud study. BMC Geriatr. 24:162. doi: 10.1186/s12877-024-04767-y
Silva, J., Madureira, J., Tonelo, C., Baltazar, D., Silva, C., Martins, A., et al. (2017). Comparing machine learning approaches for fall risk assessment. Biosignals 10, 223–230. doi: 10.5220/0006227802230230
Singh, K. K., Elhoseny, M., Singh, A., and Elngar, A. A. (2021). Machine Learning and the Internet of Medical Things in Healthcare. New York, NY: Academic Press.
Sokołowska, B. (2023). Impact of virtual reality cognitive and motor exercises on brain health. Int. J. Environ. Res. Public Health 20:4150. doi: 10.3390/ijerph20054150
Sokołowska, B. (2024). Being in virtual reality and its influence on brain health-an overview of benefits. Limit. Prospects Brain Sci. 14:72. doi: 10.3390/brainsci14010072
Sokołowska, B., Czerwosz, L., Hallay-Suszek, M., Sadura-Sieklucka, T., and Księżopolska-Orłowska, K. (2015). Posturography in patients with rheumatoid arthritis and osteoarthritis. Adv. Exp. Med. Biol. 833, 63–70. doi: 10.1007/5584_2014_29
Sokolowska, B., and Jozwik, A. (2007). “Recognition of cycles of repeated hypoxia on the basis of time periods in biological model,” in Computer Recognition Systems 2. Advances in Soft Computing, Vol. 45, eds M. Kurzynski, E. Puchala, M. Wozniak, and A. Zolnierek (Heidelberg: Springer), 778–785. doi: 10.1007/978-3-540-75175-5_96
Sokołowska, B., Rekawek, A., and Jozwik, A. (2008). “Recognition of the ventilatory response to the intermittent chemical stimuli in awake animals,” in Information Technologies in Biomedicine. Advances in Soft Computing, Vol. 47, eds E. Pietka and J. Kawa (Heidelberg: Springer), 488–494. doi: 10.1007/978-3-540-68168-7_55
Sokołowska, B., Sadura-Sieklucka, T., Czerwosz, L., Hallay-Suszek, M., Lesyng, B., and Księżopolska-Orłowska, K. (2018). Estimation of posturographic trajectory using k-nearest neighbors classifier in patients with rheumatoid arthritis and osteoarthritis. Adv. Exp. Med. Biol. 1070, 85–95. doi: 10.1007/5584_2018_150
Sokołowska, B., and Sokołowska, E. (2019). “Machine Learning algorithms to study of laterality in Virtual Reality,” in Proceedings of the Annual INCF Congress of NeuroInformatics 2019, (Warsaw), doi: 10.12751/incf.ni2019.0053
Sokołowska, B., Sokołowska, E., and Sadura-Sieklucka, T. (2020). Applications and perspectives of virtual posturography in neurological and neuromuscular disorders. Abstract. Folia Neuropathol. 58, 401. doi: 10.5114/fn.2020.102442
Sokołowska, B., Sokołowska, E., and Sadura-Sieklucka, T. (2022). Virtual and biological parameters/markers in neuroscience. Abstract. Folia Neuropathol. 60:16. doi: 10.5114/fn.2022.121852
Song, W., Latham, N., Liu, L., Rice, H., Sainlaire, M., Min, L., et al. (2024). Improved accuracy and efficiency of primary care fall risk screening of older adults using a machine learning approach. J. Am. Geriatr. Soc. 72, 1145–1154. doi: 10.1111/jgs.18776
Souchet, A., Lourdeaux, D., Burkhardt, J., and Hancock, P. (2023). Design guidelines for limiting and eliminating virtual reality-induced symptoms and effects at work: A comprehensive, factor-oriented review. Front. Psychol. 14:1161932. doi: 10.3389/fpsyg.2023.1161932
Stevens, J., and Lee, R. (2018). The potential to reduce falls and avert costs by clinically managing fall risk. Am. J. Prev. Med. 55, 290–297. doi: 10.1016/j.amepre.2018.04.035
Stuckenschneider, T., Schmidt, L., Speckmann, E., Koschate, J., and Zieschang, T. (2023). Recruiting patients for falls prevention in the emergency department - worth the challenge. BMC Geriatr. 23:880. doi: 10.1186/s12877-023-04607-5
Tortora, C., Di Crosta, A., La Malva, P., Prete, G., Ceccato, I., Mammarella, N., et al. (2024). Virtual reality and cognitive rehabilitation for older adults with mild cognitive impairment: A systematic review. Ageing Res. Rev. 93:102146. doi: 10.1016/j.arr.2023.102146
United Nations (2017). World Population Prospects: The 2017 Revision, DVD Edition. New York, NY: United Nations.
United Nations (2019). World Population Ageing 2019: Highlights (ST/ESA/SER.A/430). New York, NY: United Nations.
United Nations (2020). United Nations of Decade Of Healthy Ageing: 2021-2030. Available onlin at: https://social.desa.un.org/sdn/decade-of-healthy-ageing-2021-2030 (accessed February 21, 2024).
Veneziani, I., Marra, A., Formica, C., Grimaldi, A., Marino, S., Quartarone, A., et al. (2024). Applications of artificial intelligence in the neuropsychological assessment of dementia: A systematic review. J. Pers. Med. 14:113. doi: 10.3390/jpm14010113
Venkatakrishnan, R., Venkatakrishnan, R., Raveendranath, B., Sarno, D. M., Robb, A. C., Lin, W. C., et al. (2023). The effects of auditory, visual, and cognitive distractions on cybersickness in virtual reality. IEEE Trans. Vis. Comput. Graph. 7, 1–16. doi: 10.1109/TVCG.2023.3293405
Viswanathan, A., and Sudarsky, L. (2012). Balance and gait problems in the elderly. Handb. Clin. Neurol. 103, 623–634. doi: 10.1016/B978-0-444-51892-7.00045-0
Wen, E., Gupta, C., Sasikumar, P., Billinghurst, M., Wilmott, J., Skow, E., et al. (2024). VR.net: A real-world dataset for virtual reality motion sickness research. IEEE Trans. Vis. Comput. Graph. 30, 2330–2336. doi: 10.1109/TVCG.2024.3372044
Wilf, M., Korakin, A., Bahat, Y., Koren, O., Galor, N., Dagan, O., et al. (2024). Using virtual reality-based neurocognitive testing and eye tracking to study naturalistic cognitive-motor performance. Neuropsychologia 194:108744. doi: 10.1016/j.neuropsychologia.2023.108744
World Health Organization [WHO] (2020). World Health Organization of Angeing and Health Unit. Available online at: https://www.who.int/teams/maternal-newborn-child-adolescent-health-and-ageing/ageing-and-health/research-evidence-and-data (accessed February 21, 2024).
Yang, A. H. X., Kasabov, N., and Cakmak, Y. (2022). Machine learning methods for the study of cybersickness: A systematic review. Brain Inform. 9:24. doi: 10.1186/s40708-022-00172-6
Yang, A., Kasabov, N., and Cakmak, Y. (2023). Prediction and detection of virtual reality induced cybersickness: A spiking neural network approach using spatiotemporal EEG brain data and heart rate variability. Brain Inform. 10:15. doi: 10.1186/s40708-023-00192-w
Yang, J. G., Thapa, N., Park, H., Bae, S., Park, K., Park, J., et al. (2022). Virtual reality and exercise training enhance brain, cognitive, and physical health in older adults with mild cognitive impairment. Int. J. Environ. Res. Public Health 19:13300. doi: 10.3390/ijerph192013300
Yousefi Babadi, S., and Daneshmandi, H. (2021). Effects of virtual reality versus conventional balance training on balance of the elderly. Exp. Gerontol. 153:111498. doi: 10.1016/j.exger.2021.111498
Zhang, X., Shuai, J., and Li, L. (2015). Vision and relevant risk factor interventions for preventing falls among older people: A network meta-analysis. Sci. Rep. 5:10559. doi: 10.1038/srep10559
Keywords: machine learning, k-NN algorithm, virtual reality, body balance, postural stability, balance and cognitive training, aging, fall risk
Citation: Sokołowska B, Świderski W, Smolis-Bąk E, Sokołowska E and Sadura-Sieklucka T (2024) A machine learning approach to evaluate the impact of virtual balance/cognitive training on fall risk in older women. Front. Comput. Neurosci. 18:1390208. doi: 10.3389/fncom.2024.1390208
Received: 22 February 2024; Accepted: 02 May 2024;
Published: 14 May 2024.
Edited by:
Eliane Schochat, University of São Paulo, BrazilReviewed by:
Givago Silva Souza, Federal University of Pará, BrazilCopyright © 2024 Sokołowska, Świderski, Smolis-Bąk, Sokołowska and Sadura-Sieklucka. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Beata Sokołowska, YmV0YS5zb2tvbG93c2thQGdtYWlsLmNvbQ==; Teresa Sadura-Sieklucka, dGVyZXNhLnNhZHVyYS1zaWVrbHVja2FAc3BhcnRhbnNrYS5wbA==
†ORCID: Beata Sokołowska, orcid.org/0000-0002-0547-303X; Edyta Smolis-Bąk, orcid.org/0000-0002-8706-4247; Ewa Sokołowska, orcid.org/0000-0001-8637-7906; Teresa Sadura-Sieklucka, orcid.org/0000-0003-3698-8885
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.