
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CLINICAL TRIAL article
Front. Med. , 20 September 2022
Sec. Nephrology
Volume 9 - 2022 | https://doi.org/10.3389/fmed.2022.887609
This article is part of the Research Topic Peritoneal Dialysis: Recent Advances and State of the Art View all 24 articles
 Pablo Maggiani-Aguilera1,2Jonathan S. Chávez-Iñiguez1,2Guillermo Navarro-Blackaller1,2Karla Hernández-Morales1,2Ariadna Lizbeth Geraldo-Ozuna1,2Luz Alcantar-Villín1,2Olivia Montoya-Montoya2Víctor Hugo Luquín-Arellano1,2
Pablo Maggiani-Aguilera1,2Jonathan S. Chávez-Iñiguez1,2Guillermo Navarro-Blackaller1,2Karla Hernández-Morales1,2Ariadna Lizbeth Geraldo-Ozuna1,2Luz Alcantar-Villín1,2Olivia Montoya-Montoya2Víctor Hugo Luquín-Arellano1,2 Guillermo García-García1,2*
Guillermo García-García1,2*Background: Fluid overload (FO) is a common problem in patients with peritoneal dialysis (PD), it is associated with adverse outcomes and may persist despite adjustements in PD therapy.
Objective: To evaluate the feasibility and safety of stimulated diaphoresis to reduce FO with the use of a portable sauna bath.
Methods: Open-label pilot study in patients on continuous ambulatory peritoneal dialysis (CAPD) and FO. The primary outcome was the treatment-related adverse events; secondary outcomes were changes in over-hydration (OH), body weight and blood pressure, FO symptoms, and sleep quality. Dialysis prescription and daily data were recorded. The intervention period consisted in a 30-min, 45°C sauna bath, daily for 10 days, using a portable sauna bath.
Results: Fifty-one out of 54 total sauna bath sessions were well tolerated. In three (5.5%) sessions adverse effects were reported: transient dizziness in two cases, and a second-degree skin burn in a patient with advanced diabetic neuropathy. OH (6.3 ± 1.2 L vs. 5.5 ± 1.3 L, p = 0.05), body weight (67.7 ± 11.4 vs. 66.8 ± 3.8 kg, p = 0.003), diastolic blood pressure (92 ± 13.5 vs. 83 ± 13.3 mmHg, P = 0.003) and PSQI score (7.3 ± 3.7 vs. 5.1 ± 3.2, p = 0.02) improved significantly between the control and intervention period, respectively.
Conclusions: Stimulated diaphoresis with a portable sauna bath could be a novel, safe, and effective alternative way to reduce FO in CAPD patients. Larger studies are needed to confirm our results.
Clinical trial registration: ClinicalTrials.gov, identifier: NCT03563898.
FO is a common complication in end-stage renal disease (1, 2), and it has been associated to arterial hypertension, left ventricular hypertrophy, malnutrition and inflammation in the end-stage kindey disease (3–7), as well as to all-cause mortality in patients with kidney replacement therapy (KRT) (8–12).
The need of high ultrafiltration rates increases the risk of intradialytic hypotension, cramps, and the impossibility to reach dry weight in the short term (13). In pertioneal dialysis (PD) patients, the use of hypertonic solutions can increase the ultrafiltrate volume, but unfortunately, it may also lead to a more rapid deterioration of peritoneal membrane function, and potentially to the loss of residual renal function (14). Despite improvements in the methods of KRT as well as other techniques in PD patients, the problem of FO persists in the PD population.
Few studies have examined fluid losses through diaphoresis in patients with kidney disease, indicating that fluid loss through diaphoresis can be substantial (15–17). Body sweat is produced by 2–3 million sweat glands to control body temperature (18). Healthy people can secrete up to 4 L of water in sweat in 1 h with appropriate stimuli (15). Exocrine secretion also contains factors that regulate skin flora and reduce the risk of infections (19). Hot water baths performed in two patients induced water losses of 566 ± 160 and 813 ± 62 ml / h, respectively (15). Additionally, improvement of uremic symptoms has been described (17). Our protocol offers a technique not previously used with a portable sauna bath, which is affordable and easy to use at home in patients with PD. We hypothesize that the stimulation of diaphoresis in PD patients with portable sauna can be a safe and effective strategy to reduce FO.
This was an open-label, interventional and treatment purpose pilot study, in 9 PD patients with FO from the Hospital Civil de Guadalajara. To evaluate its safety, the sauna therapy was implemented in hospitalized patients, under medical supervision. Inclusion criteria were being on CAPD for at least 3 months, diagnosis of FO (OH > 2 L measured with bioelectrical impedance BCM, Fresenius (R), stable clinical condition, and availability to give informed consent. Exclusion criteria were any cardiovascular event in the last 12 months (acute myocardial infarction, NYHA Heart Failure III-IV, cardiac arrhythmia, cerebral vascular event, unstable-stable angina), peritonitis, or pregnancy. A subgroup analysis was made between responders and non-responders to sauna therapy. Responders were defined as an average decrease in the degree of OH between the control and the intervention period of at least 500 ml. The study was approved by the institutional ethical committee of the Hospital Civil de Guadalajara and registered at ClinicalTrials.gov (NCT03563898). The study was conducted in accordance with the Declaration of Helsinki and follows the CONSORT specifications.
The study was carried out in two intervals, the control and the intervention period. The control period consisted of observation for 10 days, where characteristics of the PD status, vital signs, bioimpedance spectroscopy (BIA) data, and questionnaires were recorded. Patients were weighed wearing underwear. Blood samples for chemistry, electrolytes, and blood count were collected. Blood pressure was taken daily after a 10-min rest. Questionnaire about symptoms of FO (NYHA Functional Classification of breathlessness), sleep quality scale, and antihypertensive regimens were applied to each patient. FO measurement by BIA was performed on the first day, and also daily body weight. PD treatment (volume infused, dextrose concentration, ultrafiltrate volume, and the number of exchanges per day) was recorded. A graduated glass with measurements in milliliters was provided, and the patients were instructed to record the amount of fluids ingested daily. A 24-h urine sample was collected on day one. In this phase, patients did not use the portable sauna bath.
During the intervention period, patients used the sauna bath daily, 30 min at 45°C, sitting on a chair, for 10 consecutive days (Figure 1). Time and/or temperature of the bath was reduced according to patient's tolerance. Ten minutes before taking the sauna bath, blood pressure and weight were recorded. No special recommendation on fluid intake was made. Nephrology staff was present during the bath. Patients informed of symptoms that occurred during the intervention. After finishing the bath, they stayed 15 min to dry the body with a towel. The wet catheter dressing was changed to a dry one impregnated with mupirocin spray at the exit site, and the patient's weigth and blood pressure were recorded. During the intervention period, the same information as in the control phase was collected.
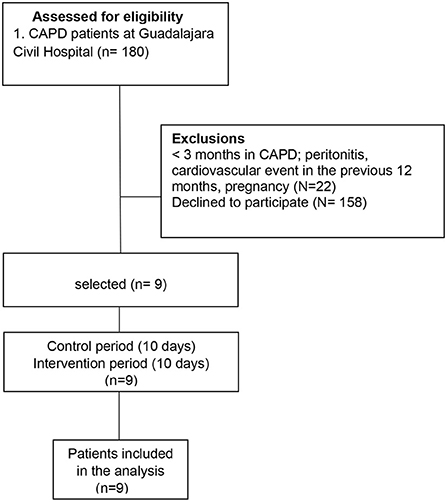
Figure 1. Portable sauna bath.
The primary outcome was treatment-related adverse events (grade two or above) as measured by CTCAE v 4.0. Secondary outcomes were the degree of OH (measured by BIA), decrease in patient's weight, blood pressure, blood test, FO symptoms (NYHA Functional Classification of breathlessness) and changes in sleep quality (PSQI score) between the two periods.
Statistical analysis was conducted using R Studio. Because this is a pilot study, no power calculation was performed. Quantitative variables were expressed as mean ± standard deviation, or as median (range), as appropriate. The Wilcoxon Signed-Rank Test was used to determine the differences in the data collected between the two periods. A two-tailed p <0.05 was consider statistically significant. A subgroup analysis was made between responders and non-responders to sauna therapy. A logistic regression model was built to try to identify factors associated to non-respond.
Among the 180 patients dialyzed on our CAPD program, we excluded 158 because they had < 3 months in CAPD, they had peritonitis or a cardiovascular event in the last 12 months, or declined to participate in the study. Nine patients fulfilled the inclusion criteria and all were included in the analysis, (Figure 2). No patients interrupted the treatment during the study period. Patient's clinical baseline characteristics are shown in Table 1. The mean age was 36 (23–68) years, 77% were females, one-third were diabetic, and only two had diuresis > 500 ml/24 h; the remaining seven patients were considered anuric (urine outout < 100 ml/24 h); baseline systolic and dyastolic blood pressure was 147 ± 10 mmHg and 93 ± 12.3 mmHg, respectively. The overhydration index was 6.3 (2.7–15.3) L, and they had a dialysis vintage of 25 (5–72) months; more than half were using a 1.5% dextrose concentration PD fluid. All participants were hypertensive and only two were not using diuretics.

Figure 2. Cohort selection. CAPD, continuous ambulatory peritoneal dialysis.
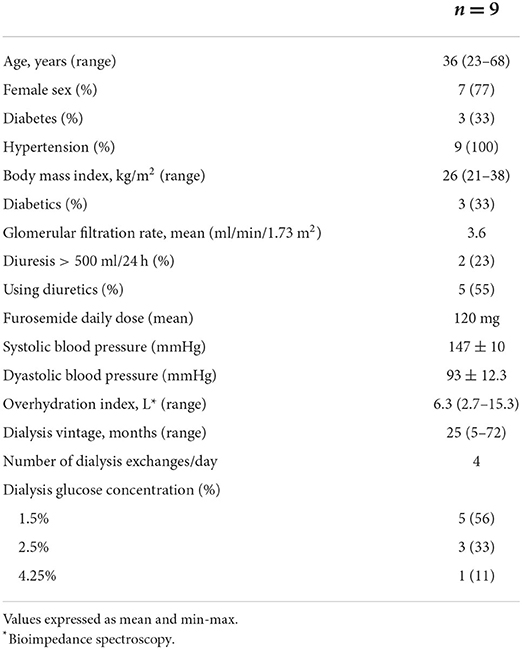
Table 1. Patient clinical characteristics.
Fifty-one of the 54 total sauna bath sessions were well tolerated; in three (5.5%) sessions adverse events were reported (Table 2). Two patients rerported momentary dizziness without hypotension at the first session, 20 min after being on the sauna bath, and these events were considered mild. These two patients received 20 min of of therapy in subsequent sessions, without any adverse effect. A patient with advanced diabetic neuropathy presented a second-degree burn, that was treated with topical analgesics and antibiotics, event that was considered moderate.
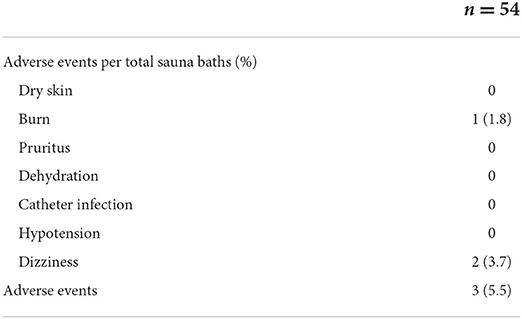
Table 2. Adverse events per total sauna baths sessions.
A significant difference was observed in the degree of OH measured by bioimpedance between the control and the intervention period (6.3 ± 1.2 L vs. 5.5 ± 1.3 L, p = 0.05). A significant decrease in mean body weight between the two periods was observed (67.7 ± 11.4 kg vs. 66.8 ± 3.8 kg, p = 0.003). Individual weight losses are shown in Table 3. Additionally, there was a significant decrease in diastolic blood pressure (92 ± 13.5 mmHg vs. 83 ± 13.3 mmHg, p = 0.003), but not in the systolic blood pressure (148 ± 12 mmHg vs. 144 ± 16 mmHg, p = 0.42). An improvement in sleep quality was observed, mainly in a decrease in nocturnal awakenings and in time of falling asleep at bedtime between the two periods (Global PSQI score, 7.3 ± 3.7 vs. 5.1 ± 3.2, P = 0.02). There was no significant difference in the ultrafiltrate or the water intake between the two periods. The summary of anthropomorphic parameters and blood tests during the two periods are shown in Table 4. We applied the Subjective Global Assessment of nutritional status in all patients on the first day of the protocol. Seven of them had normal nutritional status and two moderately malnourished. Table 5 summarizes the patient's nutritional status and their relationship with FO, time on dialysis, albumin, and C- reactive protein.
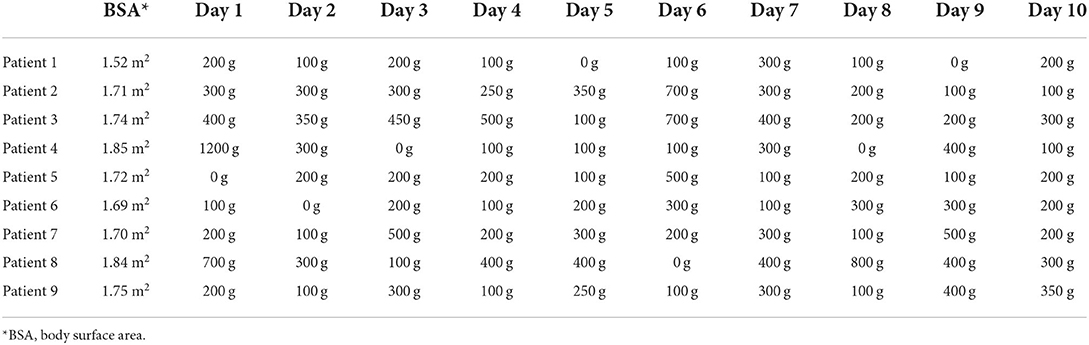
Table 3. Weight loss per patient per sauna session.
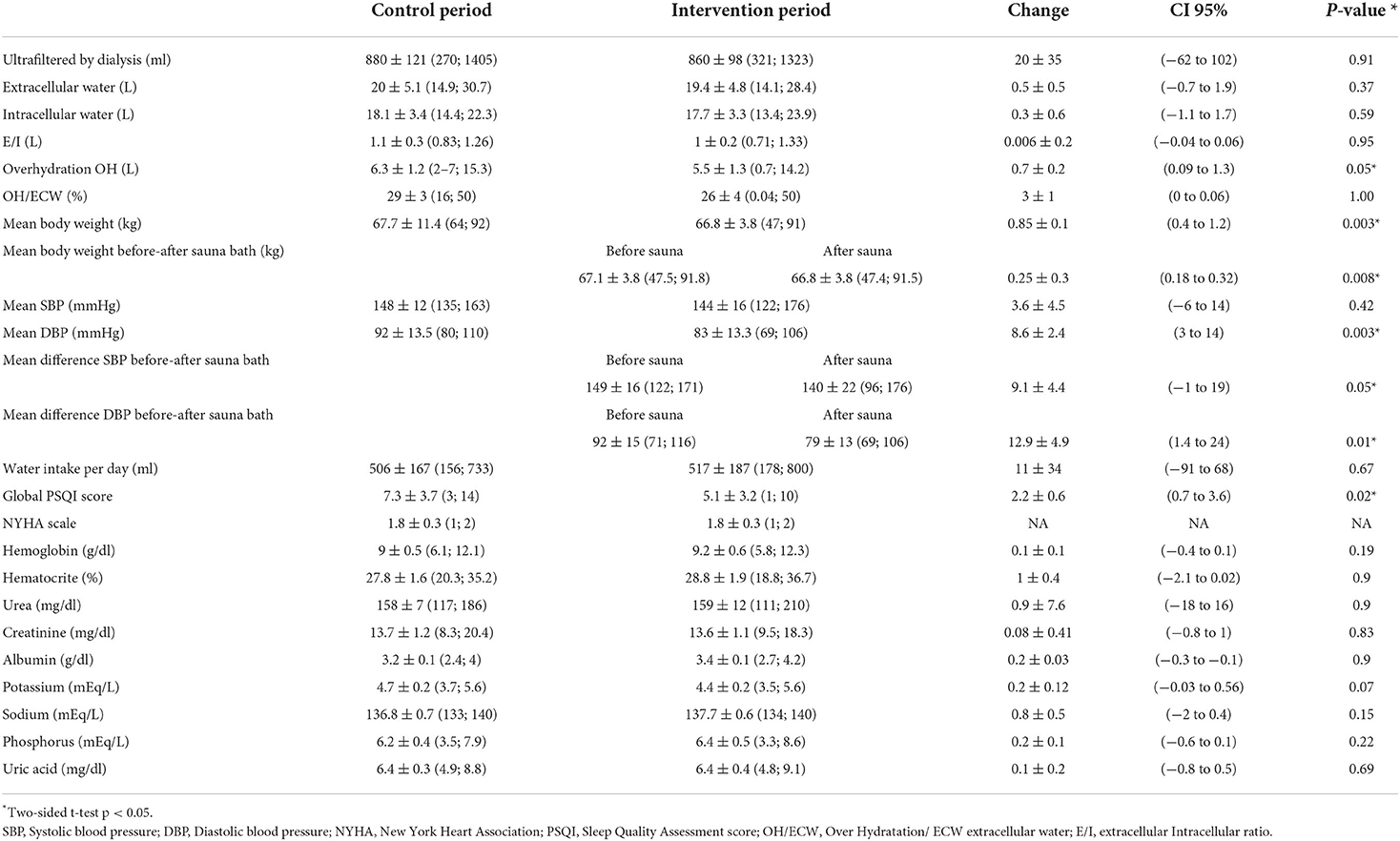
Table 4. Anthropomorphic parameters and electrolytes during the control and the intervention period.
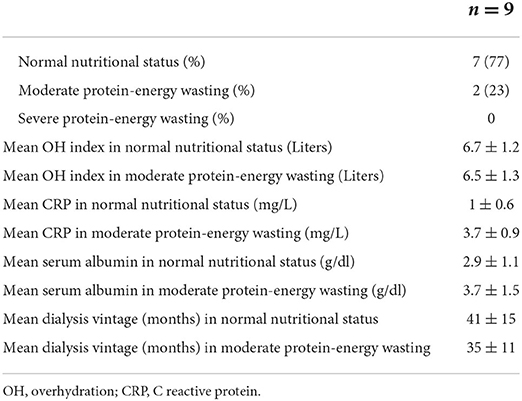
Table 5. Nutritional status by SGA.
In a subgroup analysis between responders and non-responders to therapy, six patients were classified as responders, and three as non-responders. Only the presence of moderate malnutrition was associated with an increased risk of being a non-responder (OR 2.14, 95% CI 1.40–3.26, p = 0.03) in the univariate and multivariate logistic regression model (Table 6).
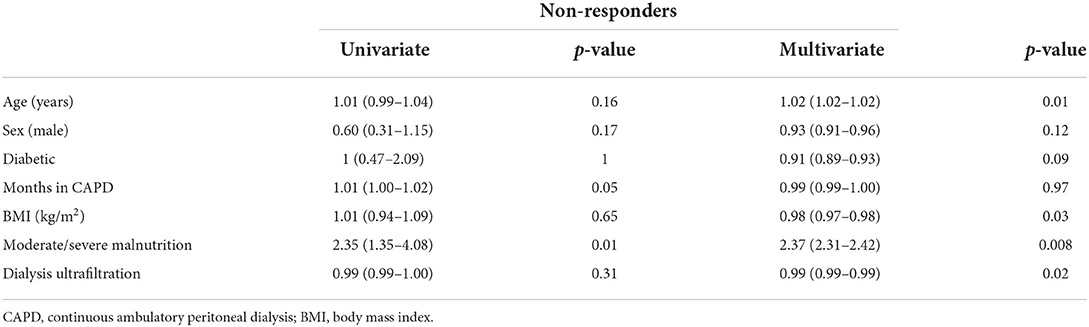
Table 6. Logistic regression model to identify non-responders to sauna treatment.
In this-single center, clinical pilot study, the use of a portable sauna bath in CAPD FO patients to stimulate diaphoresis was safe, and resulted in a significant decrease in FO, diastolic blood pressure and body weight. It could be safe to use in patients on DP, however, surveillance and grooming measures must be taken by the patient, and its use should be reconsidered in patients whose sensitivity is decreased, as it was the case in the patient with advanced diabetic neuropathy.
We found a significant decrease in OH, with a mean reduction of 0.7 ± 0.2 L. The decrease in FO was similar to the results of daily sauna baths in eight patients reported by Snyder and Merrill (17) in 1966 and Pruijm in 2013 (20). In our study, average weight loss per sauna bath during 20 to 30 min/day, was 250 ± 300 g. The total amount of sweat loss varied with some patients reaching 100 to 550 g, while other studies reported losses of up to 1,430 g (17). This suggests that some persons are more responsive to stimulated sweating therapies than others, explained in part by the difference in body surface area. Indeed. Although not statistically significant, we were able to observe a larger BSA in patients who responded to the sauna bath vs. non-responders (1.75 ± 0.1 m2 vs. 1.64 ± 0.1 m2, p = 0.06), suggesting that the larger the BSA, the greater the number of functioning sweat glands. We could identify that the presence of moderate/severe malnutrition, is a risk factor that reduces the response to fluid loss with the use of sauna bath (Table 5). Although hot weather plays a role in sweating, we do not think it influenced our results. The study was carried out during the months of January to March, when the maximum temperature in Guadalajara ranged between 24°C and 28°C.
We observed that diastolic blood pressure also presented a significant decrease before and after the therapy. This could be explained by a decrease in FO. However, this effect may be only a reflection of the heat-mediated vasodilatation of the sauna, so a larger study is necessary in which the patients be exposed to more days to therapy to confirm our hypothesis.
An improvement in sleep quality was also observed, mainly in a decrease in nocturnal awakenings and in time of falling asleep at bedtime between the two periods, using the Global PSQI score (Sleep Quality Assessment score), with a mean change of two points in the score. This result could positively contribute to the quality of life of patients. Sauna bathing could generate a gratifying and relaxing sensation, a fact that should be considered. It is possible that the good tolerance to sauna-bath stimulated diaphoresis in our population was related to our younger PD population; however, tolerance could be different in older patients.
No changes in electrolytes and urea were observed, perhaps explained by the short time of the study period. Water ingestion per day was not different between the control and the intervention period (506 ± 167 vs. 517 ± 187, respectively), which suggests that the use of sauna bathing did not cause more thirst in these patients.
Keller et al. described how perspiration has been of historical interest in the management of chronic kidney disease, due to its ability to eliminate fluids, electrolytes, and uremic toxins through the sweat glands, as well as the potential risks of exposure to heat in the sauna, such as burns and hypovolemia; despite its biological rationale, there have been only seven studies with a total of 60 patients who have explored perspiration in end stage kidney disease (21).
Our study has several limitations. The number of participants was small. The duration of the study period was short, with an exposure to therapy for only 10 days. It was a pilot study and was performed in a single center. We did not evaluate the urea and potassium kinetics, solutes that may have changed during the intervention but were not considered as objective of our study. The absence of a control group.The study was carried out in a selected group of PD patients, which may not be representative of the entire PD population, Finally, the conditions of the sauna bath sessions, such as temperature and duration, were established based on the capabilities set by the manufacturer of the equipment. We do not rule out that other parameters could be evaluated in these patients to make it more effective and tailored to the tolerance for each patient. In our opinion, patients could undergo two sauna bath sessions per day since it was very well tolerated. However, we did not have enough personnel to supervise more than one sauna session per day.
In conclusion, in PD patients with FO, stimulated diaphoresis with sauna baths can be an effective, safe and sustained way to reduce FO. However, surveillance and grooming measures must be taken by the patient, and its use should be avoided in patients whose sensitivity is decreased, as it was the case in our patient with advanced diabetic neuropathy.
We believe that more studies are needed to evaluate a longer time the use of the sauna bath in a certain type of patient on PD or HD, especially the those with anuria and poor ultrafiltrate.
The original contributions presented in the study are included in the article/supplementary materials, further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by Comité de Etica e Investigacion, Hospital Civil de Guadalajara Fray Antonio Alcalde. The patients/participants provided their written informed consent to participate in this study.
PM-A, JC-I, and GG-G were responsible for the conception and design of the work, the acquisition, analysis, and interpretation of data, drafting the work, and approving the version for publication and are accountable for the aspects of the study that this entailed. PM-A and JC-I were responsible for the analyses and interpretation of data, critical revision of the draft for important intellectual concepts, and approving the version for publication. GN-B, KH-M, AG-O, LA-V, OM-M, and VL-A were responsible for the acquisition of data and final approval of the version for publication and are accountable for the aspects of the study that this entailed. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Blake PG, Bargman JM, Brimble KS, Davison SN, Hirsch D, McCormick BB, et al. Clinical practice guidelines and recommendations on peritoneal dialysis adequacy 2011. Perit Dial Int. (2011) 31:218–39. doi: 10.3747/pdi.2011.00026
2. Wabel P, Moissl U, Chamney P, Jirka T, Machek P, Ponce P, et al. Towards improved cardiovascular management: the necessity of combining blood pressure and fluid overload. Nephrol Dial Transplant. (2008) 23:2965–71. doi: 10.1093/ndt/gfn228
3. Chazot C, Wabel P, Chamney P, Moissl U, Wieskotten S, Wizemann V. Importance of normohydration for the long term survival of haemodialysis patients. Nephrol Dial Transplant. (2012) 27:2404–10. doi: 10.1093/ndt/gfr678
4. Agarwal R. Hypervolemia is associated with increased mortality among hemodialysis patients. Hypertension. (2010) 56:512–7. doi: 10.1161/HYPERTENSIONAHA.110.154815
5. Paniagua R, Ventura M, Avila-Díaz M, Hinojosa-Heredia H, Méndez-Durán A, Cueto-Manzano A, et al. NTproBNP, fluid volume overload and dialysis modality are independent predictors of mortality in ESRD patients. Nephrol Dial Transplant. (2010) 25:551–7. doi: 10.1093/ndt/gfp395
6. Tzamaloukas AH, Saddler M, Murata GH, Malhotra D, Sena P, Simon D, et al. Symptomatic fluid retention in patients on continuous peritoneal dialysis. J Am Soc Nephrol. (1995) 6:198–206. doi: 10.1681/ASN.V62198
7. Wizemann V, Wabel P, Chamney P, Zaluska W, Moissl U, Rode C, et al. The mortality risk of overhydration in haemodialysis patients. Nephrol Dial Transplant. (2009) 24:1574–9. doi: 10.1093/ndt/gfn707
8. Demirci MS1 DC. Relations between malnutrition-infl ammationatherosclerosis and volume status. The usefulness of bioimpedance analysis in peritoneal dialysis patients. Nephrol Dial Transplant. (2011) 26:1708–16. doi: 10.1093/ndt/gfq588
9. Foley RN, Herzog CA, Collins AJ. United States renal data system. Blood pressure and long-term mortality in United States hemodialysis patients: USRDS waves 3 and 4 study. Kidney Int. (2002) 62:1784–90. doi: 10.1046/j.1523-1755.2002.00636.x
10. Kalantar-Zadeh K, Regidor D, Kovesdy CP, Van Wyck D, Bunnapradist S, Horwich TB, et al. Fluid retention is associated with cardiovascular mortality in patients undergoing long-term hemodialysis. Circulation. (2009) 119:671–9. doi: 10.1161/CIRCULATIONAHA.108.807362
11. Kimmel PL, Varela MP, Peterson RA, Weihs KL, Simmens SJ, Alleyne S, et al. Interdialytic weight gain and survival in hemodialysis patients: effects of duration of ESRD and diabetes mellitus. Kidney Int. (2000) 57:1141–51. doi: 10.1046/j.1523-1755.2000.00941.x
12. Saran R, Bragg-Gresham J, Rayner HC, Goodkin DA, Keen ML, Van Dijk PC, et al. Nonadherence in hemodialysis: associations with mortality, hospitalization, and practice patterns in the DOPPS. Kidney Int. (2003) 64:254–62. doi: 10.1046/j.1523-1755.2003.00064.x
13. Charra B. Fluid balance, dry weight, and blood pressure in dialysis. Hemodial Int. (2007) 11:21–31. doi: 10.1111/j.1542-4758.2007.00148.x
14. Kim Y, Biesen WV. Fluid overload in peritoneal dialysis patients. Semin Nephrol. (2017) 37:43–53. doi: 10.1016/j.semnephrol.2016.10.006
15. Lacher JW, Schrier RW. Sweating treatment for chronic renal failure. Nephron. (1978) 21:255–9. doi: 10.1159/000181401
16. Man in 't Veld AJ, van Maanen JH, Schicht IM. Stimulated sweating in chronic renal failure. Br Med J. (1978) 2:172–3. doi: 10.1136/bmj.2.6131.172-a
17. Snyder D, Merrill JP. Sauna baths in the treatment of chronic renal failure. Trans Am Soc Artif Intern Organs. (1966) 12:188–92.
18. Shibasaki M, Crandall CG. Mechanisms and controllers of eccrine sweating in humans. Front Biosci. (2010) 2:685–96. doi: 10.2741/s94
19. Cui CY, Schlessinger D. Eccrine sweat gland development and sweat secretion. Exp Dermatol. (2015) 24:644–50. doi: 10.1111/exd.12773
20. Pruijm M, El-Housseini Y, Mahfoudh H, Jarraya F, Hachicha J, Teta D, et al. Stimulated sweating as a therapy to reduce interdialytic weight gain and improve potassium balance in chronic hemodialysis patients: a pilot study. Hemodial Int. (2013) 17:240–8. doi: 10.1111/j.1542-4758.2012.00751.x
Keywords: peritoneal dialysis, fluid overload, diaphoresis, sauna bath, chronic kidney disease
Citation: Maggiani-Aguilera P, Chávez-Iñiguez JS, Navarro-Blackaller G, Hernández-Morales K, Geraldo-Ozuna AL, Alcantar-Villín L, Montoya-Montoya O, Luquín-Arellano VH and García-García G (2022) Portable sauna stimulated-diaphoresis for the treatment of fluid-overload in peritoneal dialysis patients: A pilot study. Front. Med. 9:887609. doi: 10.3389/fmed.2022.887609
Received: 01 March 2022; Accepted: 29 August 2022;
Published: 20 September 2022.
Edited by:
John William Larkin, Fresenius Medical Care, United StatesReviewed by:
Raymond Keller, Stockton University, United StatesCopyright © 2022 Maggiani-Aguilera, Chávez-Iñiguez, Navarro-Blackaller, Hernández-Morales, Geraldo-Ozuna, Alcantar-Villín, Montoya-Montoya, Luquín-Arellano and García-García. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Guillermo García-García, Z2dhcmNpYTE5NTJAZ21haWwuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.