
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CASE REPORT article
Front. Med., 20 December 2022
Sec. Nuclear Medicine
Volume 9 - 2022 | https://doi.org/10.3389/fmed.2022.1078560
This article is part of the Research TopicTumor Microenvironment and Beyond: Imaging Systemic Immunity with PETView all 5 articles
 Karim Amrane1,2*†
Karim Amrane1,2*† Coline Le Meur1†
Coline Le Meur1† Philippe Thuillier3,4
Philippe Thuillier3,4 Pierre Alemany5Clémence Niel6David Renault6
Pierre Alemany5Clémence Niel6David Renault6 Ronan Abgral4,7
Ronan Abgral4,7Eosinophilic fasciitis (EF) is a rare connective tissue disorder causing inflammation and fibrosing of fascia. In this study, we present a very rare case of an immune checkpoint inhibitor (ICI)-induced EF revealed by 18F-fluorodesoxyglucose positron emission tomography (FDG-PET/CT) 20 months after the initiation of Pembrolizumab treatment of a relapsed non-small cell lung cancer (NSCLC). This study presents a 52-year-old Caucasian woman clinically presenting asthenia, inflammatory muscle, and joint pain associated with subcutaneous nodules and symmetrical edema of the lower limbs. Iterative 18FDG-PET/CT scans allow us to guide the therapeutic strategy due to this atypical ICI adverse event.
Eosinophilic fasciitis (EF) is a scleroderma-like syndrome, a rare connective tissue disorder causing inflammation and fibrosing of fascia with variable clinical manifestations that are occurring spontaneously (1) or being induced by immune checkpoint inhibitors (ICIs), usually late after treatment initiation (2, 3). EF is frequently progressive and associated with severe and incapacitating joint flexion contractures (1).
We present a 52-year-old woman with a previous medical history of locally advanced non-small-cell lung carcinoma (NSCLC) (Figure 1A–FDG-PET MIP: initial staging) with the PD-L1 expression level of 5%, treated by radiochemotherapy. After 2 years, she presented an adrenal relapse (Figure 1B–FDG-PET MIP: left adrenal relapse, arrow), which was treated with stereotactic radiotherapy and pembrolizumab (4), achieving a complete response (CR) after 15 months of treatment (20 cycles) [Figure 1C–FDG-PET MIP: complete response with diffuse immune hypothyroidism corresponding to immune-induced hypothyroidism by ICI (CTCAE 5.0 grade 2) that had been treated by supplementation].
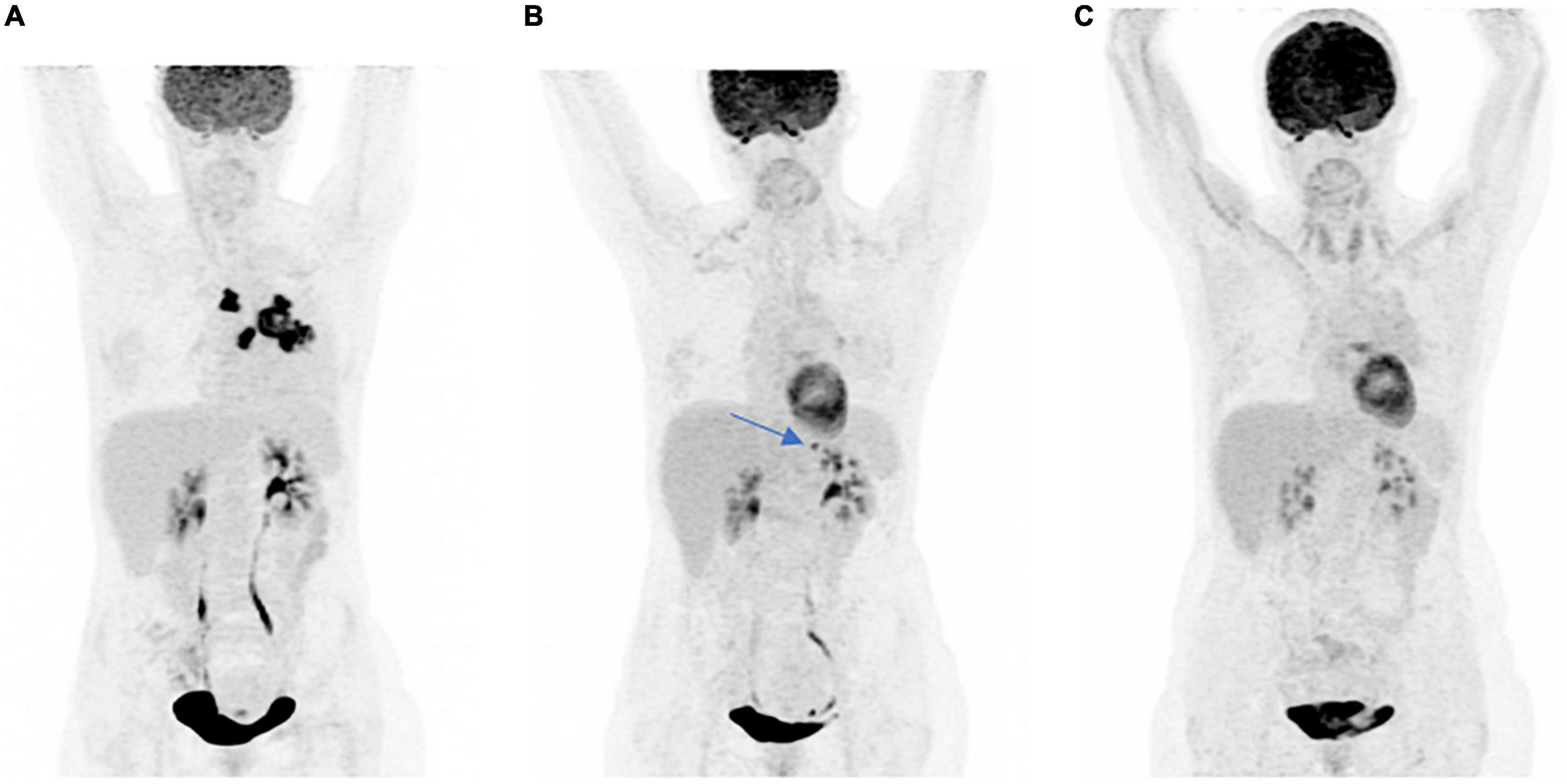
Figure 1. (A) FDG-PET MIP: initial staging, (B) FDG-PET MIP: left adrenal relapse, arrow, and (C) FDG-PET MIP: complete response with diffuse immune hypothyroidism.
After six cycles of treatment with pembrolizumab, a 2-deoxy-2-[18F] fluoro-D-glucose positron emission tomography-computed tomography (18F-FDG-PET/CT) evaluation showed the persistence of CR, however, revealing the appearance of subcutaneous and fascial hypermetabolism (Figure 2A) without any morphological or clinical translation except a transitory elevation of eosinophil count on biological analysis. This asymptomatic state did not justify the introduction of therapy. After four cycles of treatment with Pembrolizumab, the patient complained of CTCAE 5.0 grade 2 asthenia, inflammatory muscle, and joint pain associated with subcutaneous nodules and symmetrical edema of the lower limbs. The blood test revealed a slightly elevated CRP of 20.5 mg/L, with normal levels of cortisol and TSH. A new evaluation by FDG-PET/CT was performed, showing no cancer progression but an increase in the number and intensity of hypermetabolic subcutaneous nodules and muscle fascia (limbs, paravertebral) lesions and the appearance of diffuse tracer uptake on the synovial walls of both knees (Figure 2B). The SUVmax on fascia was 12.3 and on subcutaneous nodules was 9.5. To explore these hypermetabolic findings (Figures 3A, B coronal and axial FDG PET-CT views), a subcutaneous nodule biopsy was performed and histologic analysis revealed panniculitis with septal inflammation. This septal infiltrate was mostly composed of lymphocytes and few histiocytes; vessels were well seen, without vasculitis (Figure 3C HES x40).
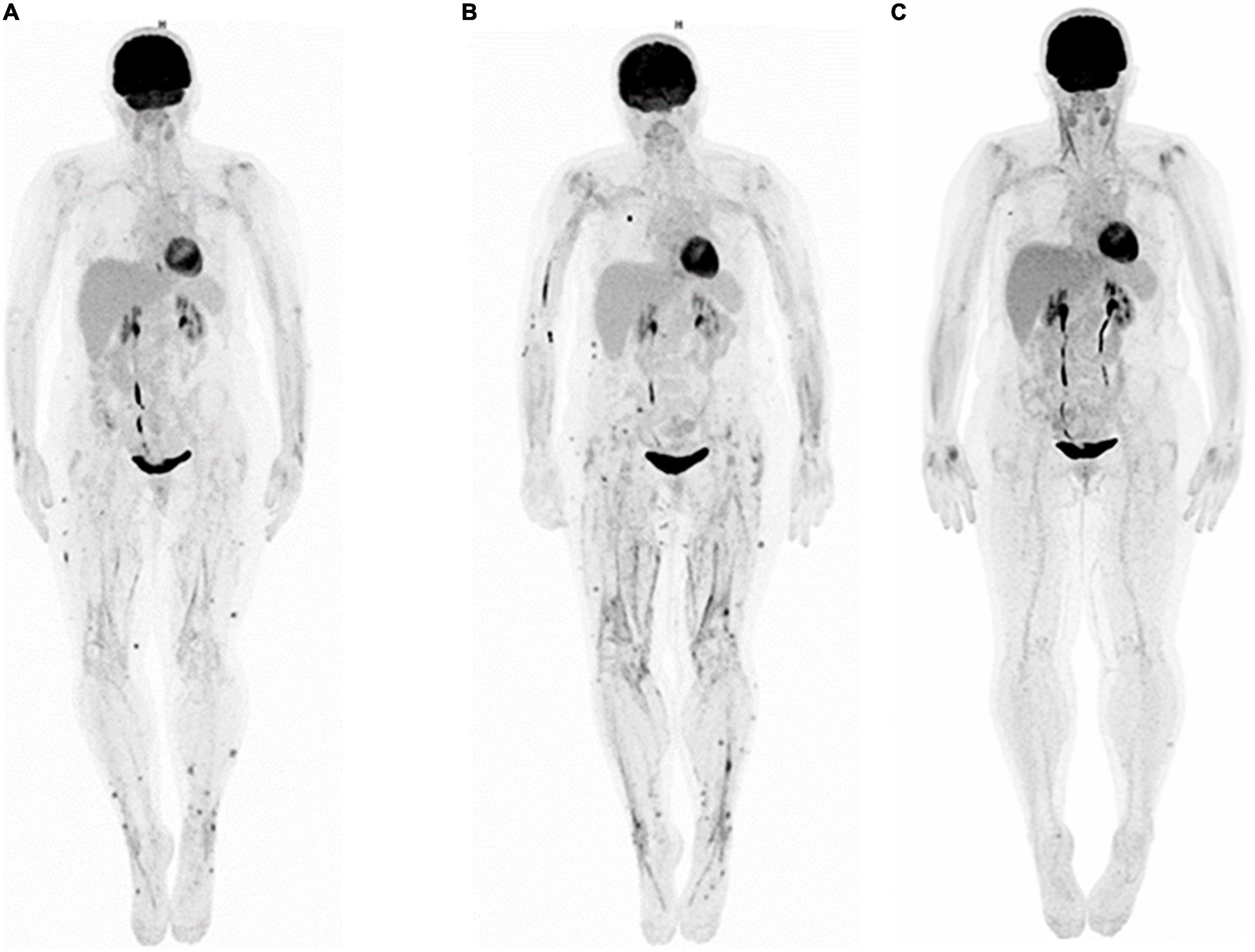
Figure 2. Whole-body FDG-PET MIP: (A) appearance of subcutaneous and fascial hypermetabolism, (B) increase of subcutaneous and fascial hypermetabolism, and (C) disappearance of subcutaneous and fascial hypermetabolism, after corticotherapy.
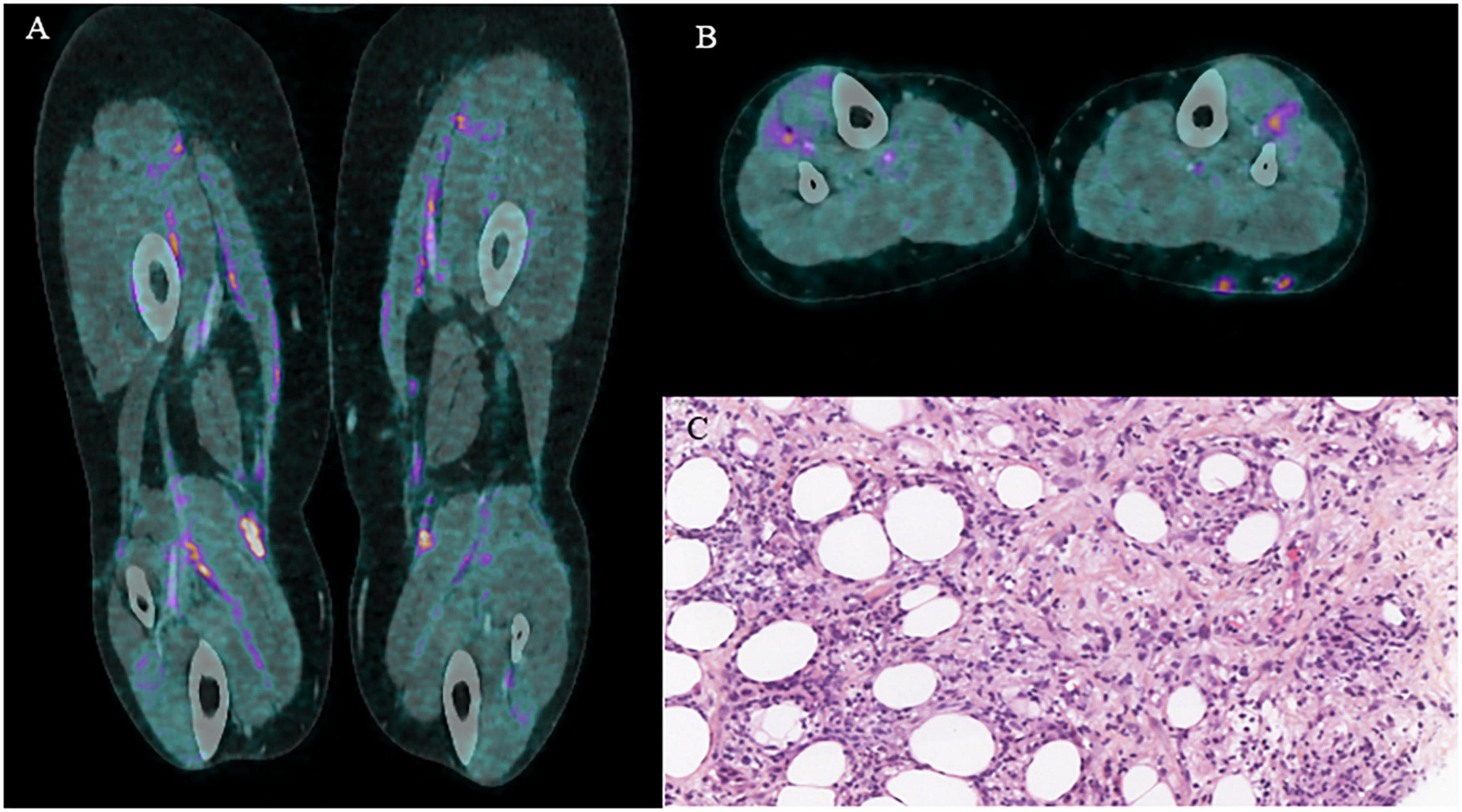
Figure 3. (A) Coronal l FDG PET-CT. (B) Axial FDG PET-CT. (C) Histologic feature of eosinophilic fasciitis.
The suspicion of EF seemed obvious given the isotopic presentation and confirmation of the subcutaneous nodule lymphocytic infiltration (5). Both autoantibody assay (antinuclear antibodies, rheumatoid factors, anti-cyclic citrullinated peptide, and anti-Scl70) and electroneuromyogram were negatives, ruling out differential diagnoses such as scleroderma and other scleroderma-like syndromes (6).
The management of this disease consisted of discontinuing Pembrolizumab as it was responsible for this immune-induced adverse event and starting corticosteroid therapy (CST) at 0.5mg/kg in decreasing doses for 3 months for their immunomodulatory effect (7), resulting in resolution of symptoms and reduction and then disappearance of subcutaneous and fascial hypermetabolisms (Figure 2C FDG-PET MIP).
Interestingly, to the best of our knowledge, we found that there are only 16 cases of ICI-induced EF in the literature and none in major therapeutic trials. Among these 16 cases, 50% (8/16) were in CR at the time of onset of this adverse event and 25% (4/16) were in progression disease, mainly in urothelial and renal tumors. Only 12.5% (2/16) were fortuitously revealed by FDG-PET/CT, none in the case of lung cancer (6, 8). The analysis of 16 reported cases shows that the time of onset is late following the initiation of ICI, ranging from 8 to 15 months, except for 2 clinical cases where the time of onset was 3 months. In our case, the time of onset was late since it was 19 months, which is consistent with the trend found in the literature.
Although magnetic resonance imaging (MRI) seems to have a better diagnostic performance than FDG-PET/CT due to its high sensitivity for soft tissue analysis that can show thickening of the muscular fascias in high signal intensity (9, 10), this examination is only performed in the case of diagnostic suspicion and mostly after the onset of symptoms. However, 18F-FDG-PET/CT has the advantage of being a whole-body examination for which the additional acquisition of images on the limbs is slightly longer (1–2 min) and does not reach more radiation exposure for the patient. In addition to the assessment of tumor response to ICI, 18F-FDG-PET/CT is useful for subclinical detection of fascia tracer uptake, allowing early treatment of EF (11) and also remains an interesting tool for its multifocal involvement evaluation (12, 13).
This case of ICI-induced EF suggests the usefulness of consistently performing a whole-body 18F-FDG-PET/CT examination in a patient treated by immunotherapy for not overlooking subcutaneous nodules and fascia FDG uptakes that could guide the early management of this adverse event.
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent from the patients/participants OR patients/participants legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
KA and RA provided the details of the patient and provided an initial draft of the submission. CN and DR provided the details of the patient. PT, PA, and RA provided the images and image analysis and helped in drafting the initial submission. CL helped in drafting the initial submission. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Shulman LE. Diffuse fasciitis with hypergammaglobulinemia and eosinophilia: a new syndrome? J Rheumatol. (1984) 11:569–70.
2. Khoja L, Maurice C, Chappell M, MacMillan L, Al-Habeeb AS, Al-Faraidy N, et al. Eosinophilic fasciitis and acute encephalopathy toxicity from pembrolizumab treatment of a patient with metastatic melanoma. Cancer Immunol Res. (2016) 4:175–8. doi: 10.1158/2326-6066.CIR-15-0186
3. Bronstein Y, Ng CS, Hwu P, Hwu WJ. Radiologic manifestations of immune-related adverse events in patients with metastatic melanoma undergoing anti-CTLA-4 antibody therapy. AJR Am J Roentgenol. (2011) 197:W992–1000.
4. Herbst RS, Baas P, Kim D-W, Kim DW, Felip E, Pérez-Gracia JL, et al. Pembrolizumab versus docetaxel for previously treated, PD-L1-positive, advanced non-small-cell lung cancer (KEYNOTE-010): a randomised controlled trial. Lancet Lond Engl. (2016) 387:1540–50. doi: 10.1016/S0140-6736(15)01281-7
5. Pinal-Fernandez I, Selva-O’ Callaghan A, Grau JM. Diagnosis and classification of eosinophilic fasciitis. Autoimmun Rev. (2014) 13:379–82.
6. Zampeli E, Zervas E. Eosinophilic fasciitis following checkpoint inhibitor therapy with pembrolizumab. Mediterr J Rheumatol. (2021) 32:376–7.
7. Mendoza FA, Bai R, Kebede AG, Jimenez SA. Severe eosinophilic fasciitis: comparison of treatment with D-penicillamine plus corticosteroids vs. corticosteroids alone. Scand J Rheumatol. (2016) 45:129–34. doi: 10.3109/03009742.2015.1067713
8. Chan KK, Magro C, Shoushtari A, Rudin C, Rotemberg V, Rossi A, et al. Eosinophilic fasciitis following checkpoint inhibitor therapy: four cases and a review of literature. Oncologist. (2019) [Online ahead of print]. doi: 10.1634/theoncologist.2019-0508
9. Moulton SJ, Kransdorf MJ, Ginsburg WW, Abril A, Persellin S. Eosinophilic fasciitis: spectrum of MRI findings. AJR Am J Roentgenol. (2005) 184:975–8. doi: 10.2214/ajr.184.3.01840975
10. Desvignes-Engelbert A, Saulière N, Loeuille D, Blum A, Chary-Valckenaere I. From diagnosis to remission: place of MRI in eosinophilic fasciitis. Clin Rheumatol. (2010) 29:1461–4. doi: 10.1007/s10067-010-1508-1
11. Bisschop C, de Heer EC, Brouwers AH, Hospers GAP, Jalving M. Rational use of 18F-FDG PET/CT in patients with advanced cutaneous melanoma: a systematic review. Crit Rev Oncol Hematol. (2020) 153:103044. doi: 10.1016/j.critrevonc.2020.103044
12. Kim HJ, Lee S-W, Kim GJ, Lee JH. Usefulness of FDG PET/CT in the diagnosis of eosinophilic fasciitis. Clin Nucl Med. (2014) 39:801–2. doi: 10.1097/RLU.0000000000000260
Keywords: NSCLC, eosinophilic fasciitis, 18F-FDG-PET/CT, pembrolizumab, ICI
Citation: Amrane K, Le Meur C, Thuillier P, Alemany P, Niel C, Renault D and Abgral R (2022) Case report: Eosinophilic fasciitis induced by pembrolizumab with high FDG uptake on 18F-FDG-PET/CT. Front. Med. 9:1078560. doi: 10.3389/fmed.2022.1078560
Received: 24 October 2022; Accepted: 28 November 2022;
Published: 20 December 2022.
Edited by:
Madhavi Tripathi, All India Institute of Medical Sciences, IndiaReviewed by:
Ryogo Minamimoto, National Center For Global Health and Medicine, JapanCopyright © 2022 Amrane, Le Meur, Thuillier, Alemany, Niel, Renault and Abgral. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Karim Amrane, ✉ a2FtcmFuZUBjaC1tb3JsYWl4LmZy
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.