
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CASE REPORT article
Front. Med., 09 January 2023
Sec. Infectious Diseases: Pathogenesis and Therapy
Volume 9 - 2022 | https://doi.org/10.3389/fmed.2022.1062450
 Federico Baldi1,2*
Federico Baldi1,2* Chiara Dentone2Malgorzata Mikulska1,2
Chiara Dentone2Malgorzata Mikulska1,2 Daniela Fenoglio3,4Michele Mirabella2Federica Magnè2Federica Portunato2
Daniela Fenoglio3,4Michele Mirabella2Federica Magnè2Federica Portunato2 Tiziana Altosole3
Tiziana Altosole3 Chiara Sepulcri1,2
Chiara Sepulcri1,2 Daniele Roberto Giacobbe1,2*Chiara Uras3Graziana Scavone4Lucia Taramasso2
Daniele Roberto Giacobbe1,2*Chiara Uras3Graziana Scavone4Lucia Taramasso2 Andrea Orsi1,5Giuseppe Cittadini6
Andrea Orsi1,5Giuseppe Cittadini6 Gilberto Filaci3,4Matteo Bassetti1,2
Gilberto Filaci3,4Matteo Bassetti1,2COVID-19 in immunocompromised patients is difficult to treat. SARS-CoV-2 interaction with the host immune system and the role of therapy still remains only partly understood. There are no data regarding the use of monoclonal antibodies and the combination of two antivirals in fighting viral replication and disease progression. We report the cases of two patients, both treated with rituximab for non-Hodgkin lymphoma and granulomatosis with polyangiitis, respectively, and both hospitalized for COVID-19 with positive SARS-CoV-2 RNAemia, who were successfully treated with a salvage combination therapy with sotrovimab, remdesivir and nirmatrelvir/ritonavir.
There have been several advances among the available therapies for coronavirus disease 2019 (COVID-19), with the development of new oral antivirals and monoclonal antibodies (1–13). Immunocompromised patients have an increased mortality linked to SARS-CoV-2 infection compared to the general population, with high hospitalization and mortality rates of 39 and 34%, respectively (14–17). Furthermore, in this population the negative prognosis seems more related to the virologic phase than to the inflammatory phase (16–18), and the virologic phase could be prolonged with the presence of SARS-CoV-2 in the blood months after the beginning of the infection (19). In a study of 20 patients with lymphoma or undergoing hematopoietic stem cell transplantation, viable virus from nasopharyngeal (NP) swabs was detected by cell culture up to 60 days after the onset of infection (20), while in other reports of hematological patients with SARS-CoV-2 infection the shedding of the viable virus was even more prolonged: 59, 70, 119, and 238 days, respectively (19, 21–23).
The progression over time of SARS-CoV-2 infection in the immunocompromised host can be different than in the general population, and antivirals could maintain a therapeutic role even beyond the first 5–10 days from the beginning of symptoms (24–27).
We report two cases of immunocompromised patients hospitalized in our Infectious Diseases (ID) Unit for COVID-19 pneumonia with SARS-CoV-2 positive RNAemia that were successfully treated with a combination therapy including of anti-Spike monoclonal antibodies (sotrovimab) and oral (nirmatrelvir/ritonavir) and intravenous (remdesivir) antivirals. We also performed the immunological analysis of cellular T responses, before and at the end of salvage therapy, when SARS-CoV-2 RNAemia became negative.
A 47-year-old man was admitted to our ID unit in February 2022 for fever, dyspnea, and confusion. He had a history of mantle cell non-Hodgkin lymphoma, treated with autologous hematopoietic stem-cell transplantation in July 2019, on maintenance therapy with rituximab every 6 months (last administration of rituximab in December 2021). The patient was vaccinated against SARS-CoV-2 with two doses of mRNA vaccine (the last dose in April 2021). In January 2022 he had mild COVID-19 not requiring hospitalization, with spontaneous resolution of symptoms and with consecutive negative molecular NP swabs. At the beginning of February, he developed fever (maximum 39°C), accompanied after 4 days by the onset of dry cough. This event was interpreted as a bacterial lower respiratory tract infection, and the patient was treated at home with empirical oral antibiotic therapy (no corticosteroids were used), without resolution of symptoms. Due to worsening conditions, with spikes of high fever, sweating, persistence of dry cough, and confusion, he was admitted to our ID unit.
Blood tests were performed at hospital admission (Day 0): white blood cell 2,640/μl (range 4,500–9,800), neutrophils 2.130/μl (range 1,800–7,800), creatinine 1.2 mg/dl (range 0.67–1.17), mild elevation of liver enzymes (ALT/AST 50/61 UI/ml, range 0–40, 0–40, respectively), lactate dehydrogenase 444U/L (range 135–225), ferritin 1,972 mcg/L (range 30–400), C reactive protein 89.4 mg/L (range 0–3), Interleukin-6 46.5 ng/L (normal value, n.v., <3.4).
SARS-CoV-2 serology resulted non-reactive: IgG anti Receptor-Binding Domain (RBD) < 1 U/ml < 12 negative), IgG anti Spike 1 (S1) < 1 U/ml (<21 negative), IgG anti Spike 2 (S2) < 1 U/ml (<9 negative), IgG anti Nucleocapsid < 1 U/ml (<23 negative). Rapid antigenic test and molecular test for SARS-CoV-2 performed on NP swabs were negative on Day 1. Computed tomography (CT) scan performed on Day 1 showed extensive bilateral ground-glass opacities with crazy-paving aspects and more consolidated components, greater at lower lobes in subpleural location (Figure 1A).
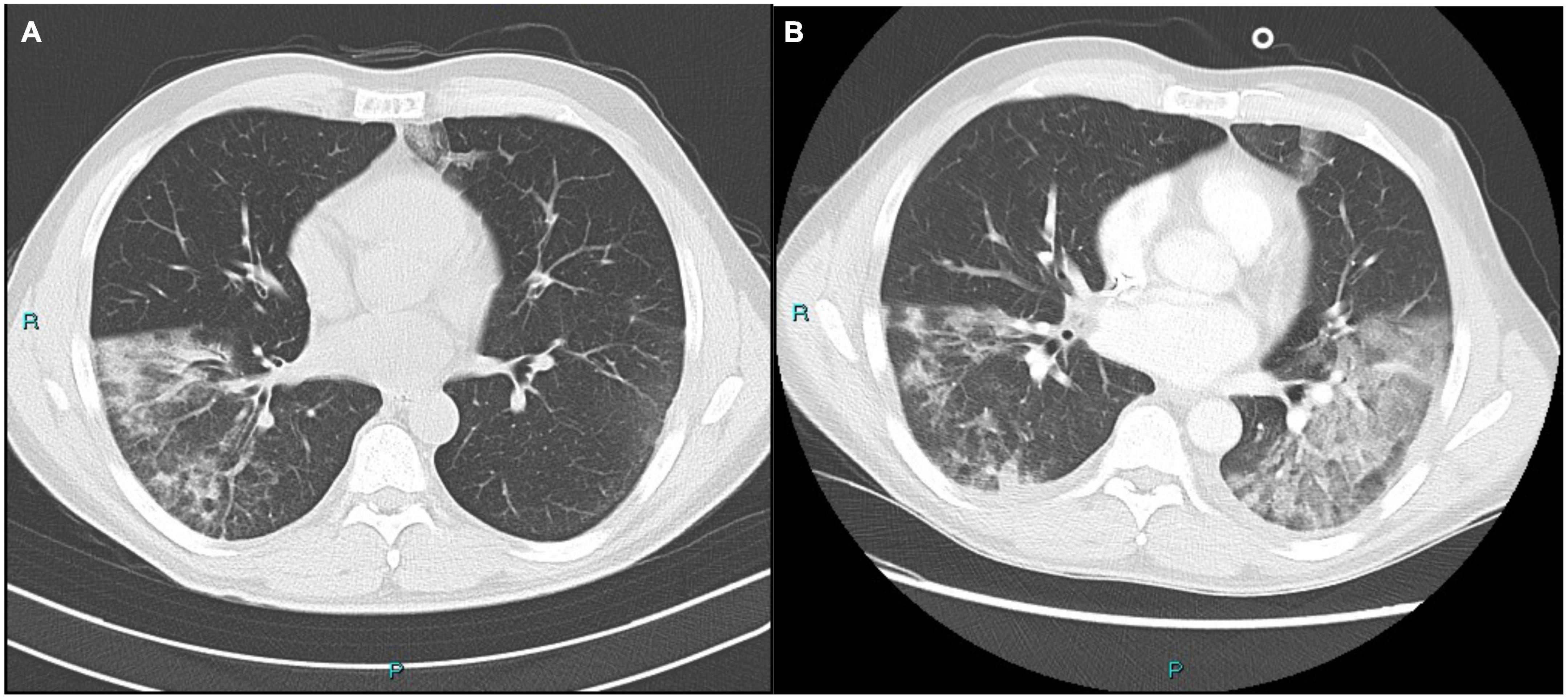
Figure 1. (A) Bilateral ground-glass opacities with crazy-paving aspects and more consolidated components, greater at right lower lobe. (B) Extension of pulmonary opacities at the left basal lobe compared to the previous imaging.
Given the radiological evidence of pneumonia in a suspected bacterial infection after the recent SARS-CoV2 infection, a bronchoalveolar lavage (BAL) was performed. Empirical antibiotic therapy with ceftobiprole and levofloxacin was started.
On day 7, due to the worsening clinical conditions, with fever up to 40.5°C and need for supplemental oxygen, he underwent a second CT scan, showing the extension of pulmonary opacities at the left basal lobe compared to the previous imaging (Figure 1B). The antibiotic therapy was changed to ceftolozane/tazobactam plus linezolid.
The same day a RT-PCR on BAL resulted positive for SARS-CoV-2, showing no other concomitant bacterial/fungal/viral infections (culture tests for common bacteria – Aspergillus spp. – M. tuberculosis, M. tuberculosis DNA, Pneumocystis jirovecii DNA, serum β-D-glucan, BAL galactomannan, BAL CMV-DNA, all tested negative). Blood testing for SARS-CoV-2 RNAemia was performed as well on day 7 and resulted positive.
In consideration of worsening bilateral pneumonia in an immunocompromised hematological patient with COVID-19 and no other clear alternative diagnoses for pneumonia, an off-label combination of sotrovimab 500 mg in a single infusion, a seven-day course of IV remdesivir (200 mg of loading dose, 100 mg of maintenance dose) plus a five-day course of oral nirmatrelvir/ritonavir 300 mg/100 mg q12h and intravenous (IV) corticosteroids was then started on day 7. The patient signed the informed consent for off-label treatment.
Sotrovimab was chosen over casirivimab/imdevimab due to the prevalence of variant of concern Omicron BA.1 at that time in Italy, on which the latter has reduced efficacy.
Adjunctive anti-inflammatory treatment (i.e., IL-6 or IL-1 receptor inhibitors) were not deemed necessary considering the presence of SARS-CoV-2 positive RNAemia and the absence of SARS-CoV-2-related inflammatory pattern.
No adverse effects were observed during the course of treatment.
From day 9 the patient remained afebrile, with clinical improvement and consequent reduction in oxygen demand on day 10, until complete weaning to room air on day 13.
On day 12 SARS-CoV-2 RNAemia resulted negative, as well as RT-PCR on NP swab. A follow up PET scan for the non-Hodgkin lymphoma was performed, showing uptake exclusively at the level of the ground-glass pulmonary thickening, suggesting local inflammatory signs of infection and thus ruling out any sign of progression of his hematological disease.
In consideration of the improved conditions and of the reduction of inflammatory parameters, the patient was discharged on day 17.
The second case refers to a 75-year-old man with a history of granulomatosis with polyangiitis with renal involvement on maintenance therapy with rituximab 500 mg every 6 months and prednisone 5 mg q24h (last administration of rituximab in December 2021), a recent finding of atrial fibrillation, and a mitral prolapse. He was vaccinated with three doses of mRNA vaccine (the last in November 2021). He had mild COVID-19 in January 2022, with fever, asthenia and wheezing cough at the onset and a positive SARS-CoV-2 antigenic nasopharyngeal swab, that turned negative 8 days later. Due to the recurrent fever up to 38°C starting at the beginning of February 2022, he underwent a chest CT scan with findings of interstitial pneumonia with peripheral small nodules and ground glass opacities (Figure 2A). He received a 7-day course of oral levofloxacin without resolution of symptoms and was then admitted to our ID unit (day 0). A new SARS-CoV-2 RT-PCR NP swab was performed, which resulted negative.
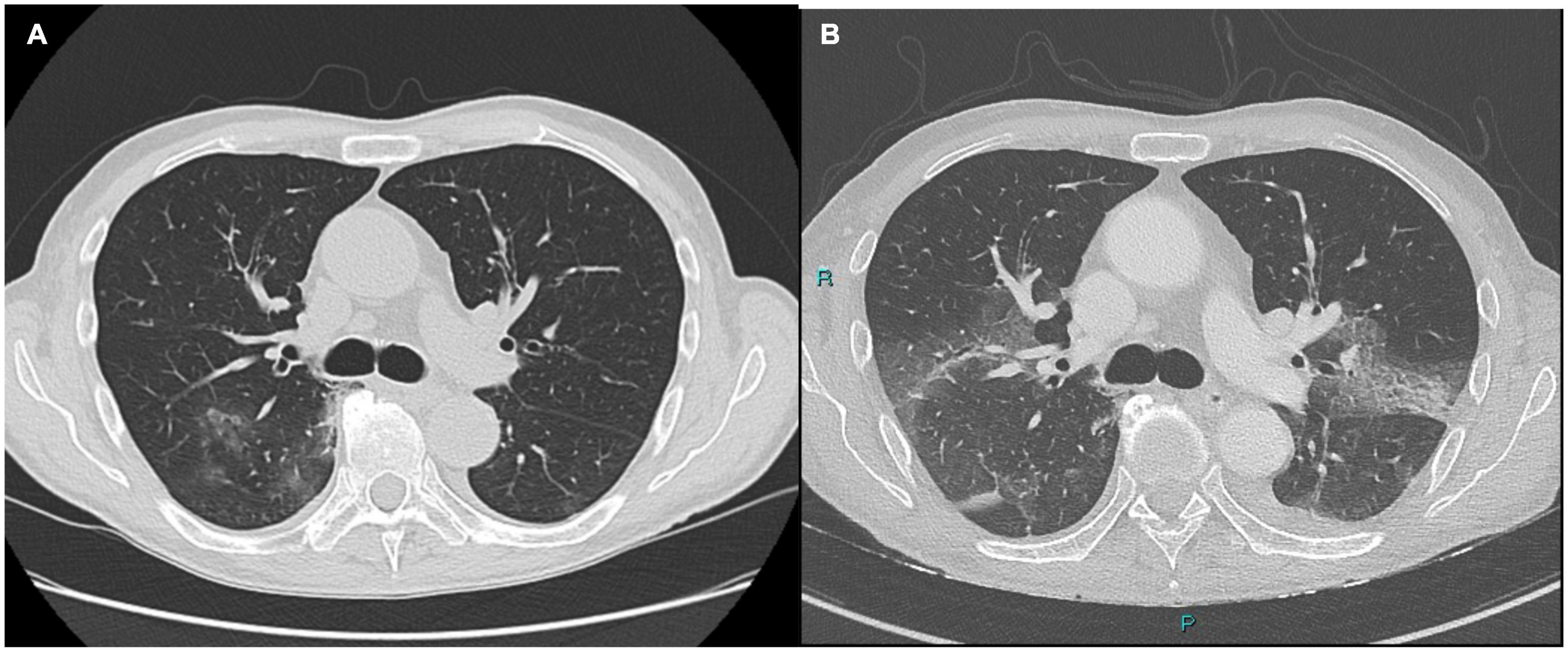
Figure 2. (A) Interstitial pneumonia with peripheral small nodules. Postero-basal and para-scissural opacities. (B) Ground-glass opacities at the bases of the upper lobes dorsally, with partial periscissural consolidative area. Moderate bilateral pleural effusion with associated disventilatory area.
Blood tests on day 0 showed a normal white blood cell count, D-dimer 428 mcg/L (range 0-500), normal liver function, creatinine 1.0 mg/dL (range 0.67–1.17), hyponatremia (128 mmol/L, range 135–150), C reactive protein 85 mg/L (range 0–3), Interleukin-6 8.8 ng/L (n.v. < 3.4).
SARS-CoV-2 serology resulted non-reactive: IgG anti Receptor-Binding Domain (RBD) < 1 U/ml < 12 negative), IgG anti Spike 1 (S1) < 1 U/ml (<21 negative), IgG anti Spike 2 (S2) < 1 U/ml (<9 negative), IgG anti Nucleocapsid < 1 U/ml (<23 negative).
A new chest CT scan was performed on day 3 and showed extension of the ground-glass opacities at the bases of the upper lobes dorsally, with partial periscissural consolidative area and moderate bilateral pleural effusion with associated disventilatory area (Figure 2B).
To investigate the possible causes of pneumonia, a BAL was requested, however, due to a worsening of the respiratory conditions and hypotension, it was not performed, and an empirical antibiotic therapy with ceftobiprole 500 mg q8gh and methylprednisolone 40 mg q12h was started.
To rule out a possible recrudescence of COVID-19, in the impossibility to perform a BAL, a blood sample was analyzed for SARS-CoV-2 RNAemia and resulted positive (day 6).
An off-label combination therapy of monoclonal antibodies and antivirals was then started on day 6: a single infusion of IV sotrovimab 500 mg, a 7-day course of IV remdesivir (200 mg of loading dose, 100 mg of maintenance dose) plus 5 days of oral nirmatrelvir/ritonavir 300 mg/100 mg q12h.
No adjunctive anti-inflammatory treatment (i.e., IL-6 or IL-1 receptor inhibitors) were deemed necessary due to the presence of SARS-CoV-2 positive viremia and the absence of SARS-CoV-2 – related inflammatory pattern.
No adverse effects were observed.
Five days later, on day 11, SARS-CoV-2 RNAemia resulted negative and on day 12 the patient was weaned off oxygen therapy, with stable peripheral saturation values on room air until discharge from our ID unit on day 14.
In Supplementary Figures 1 and 2 are reported the timelines of clinical conditions, virological tests and different therapies of case 1 and case 2, respectively.
For both patients we performed immunological analysis addressing the dynamics of peripheral T cell populations before and at the end of salvage therapy when viremia became negative.
Peripheral blood mononuclear cells (PBMC) were purified from heparinized blood samples by centrifugation on Ficoll-Hypaque (Euroclone) gradient. Immunofluorescence analyses were performed on freshly isolated 1 × 106 cells in 100 μl of PBS incubating with specific fluorochrome-conjugated monoclonal antibodies (mAbs) (all reagents for T cell characterization are listed in Table 1 and have been purchased from BD Biosciences). With regards to the analysis strategy to follow the maturation of the CD4+ and CD8+ T populations, T cell maturation has been delineated using a set of canonical markers, i.e., CD45RA, CCR7 as naive (TNAIVE), central memory (TCM), effector memory (TEM), and terminal effector (TTEM).
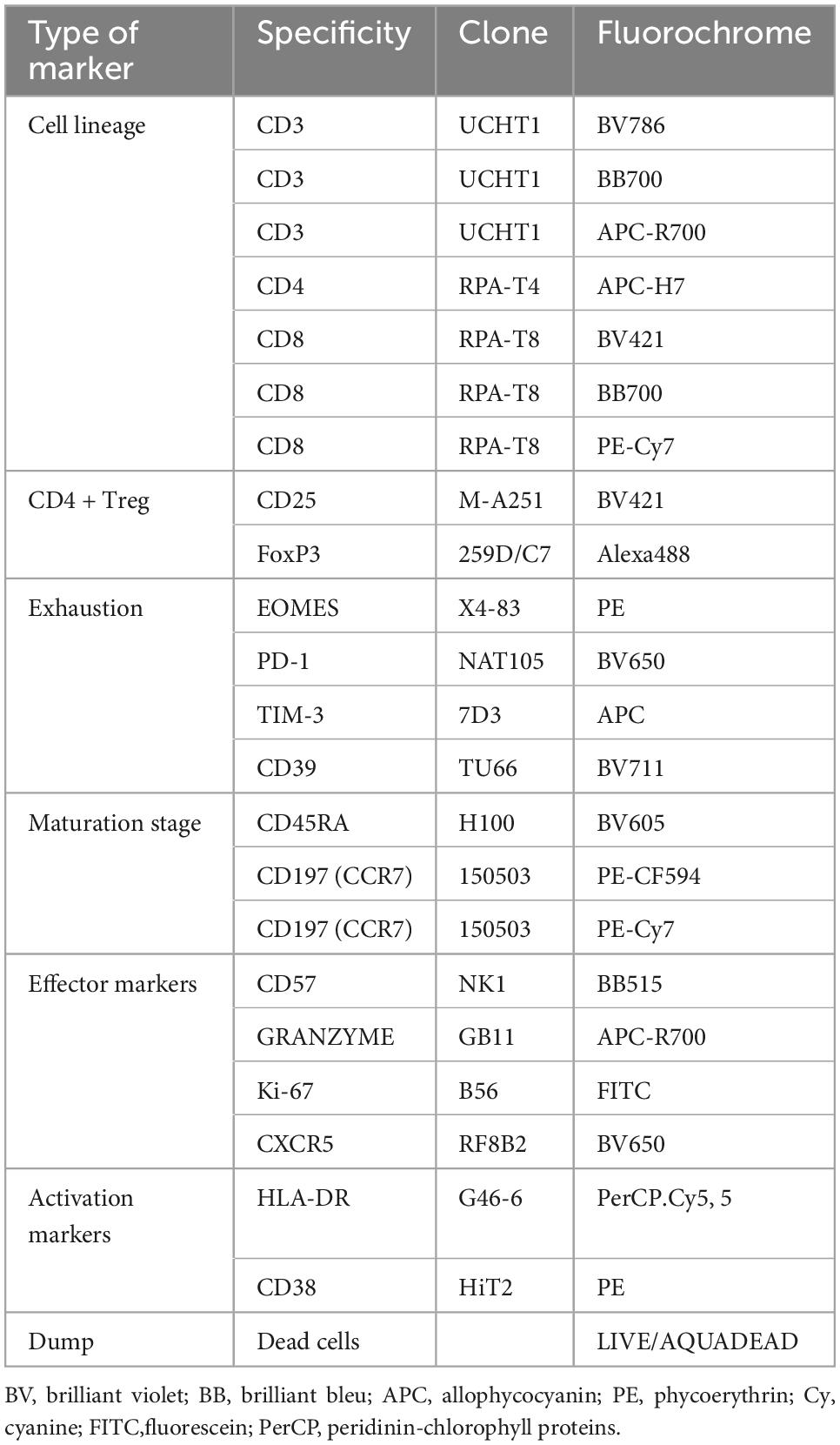
Table 1. Reagents used for T cell characterization.
Flow Cytometry Standard (FCS) 3.0 files generated were imported into FlowJo software version 10.7.1 (Becton Dickinson, San Josè, CA), and analyzed by standard gating strategy, and to identify CD3+ CD4+ T cells and CD3+ CD8+ T subpopulations. For each panel data were displayed using t-SNE plot showing median intensity fluorescence of markers with relevant differences between before and after therapies of concatenated samples.
The peripheral T cell populations showed that CD4+ and CD8+ T cells clustered differently in samples derived before therapies and after therapies, highlighting profound modifications in both the regulatory and the effector arms of T cell adaptive immunity. Firstly, we observed a decrease in the percentage of circulating CD4+ T lymphocytes and a consequent elevation of the CD8+ counterpart in both patients (Figure 3A) after therapies. As a consequence of this drastic decrease in circulating TCD4+, we also recorded an important reduction in the frequency of circulating CD4 + FoxP3 + CD25 high Treg lymphocytes after therapies (Figure 3B). Multidimensional data reduction analyses (t-SNE analysis) performed on peripheral CD4+ and CD8+ T cell populations before and after therapies further highlighted profile expression differences between the two groups of samples derived before therapies and after therapies with regard to maturation, senescence, exhaustion, effector and activation markers. In particular:
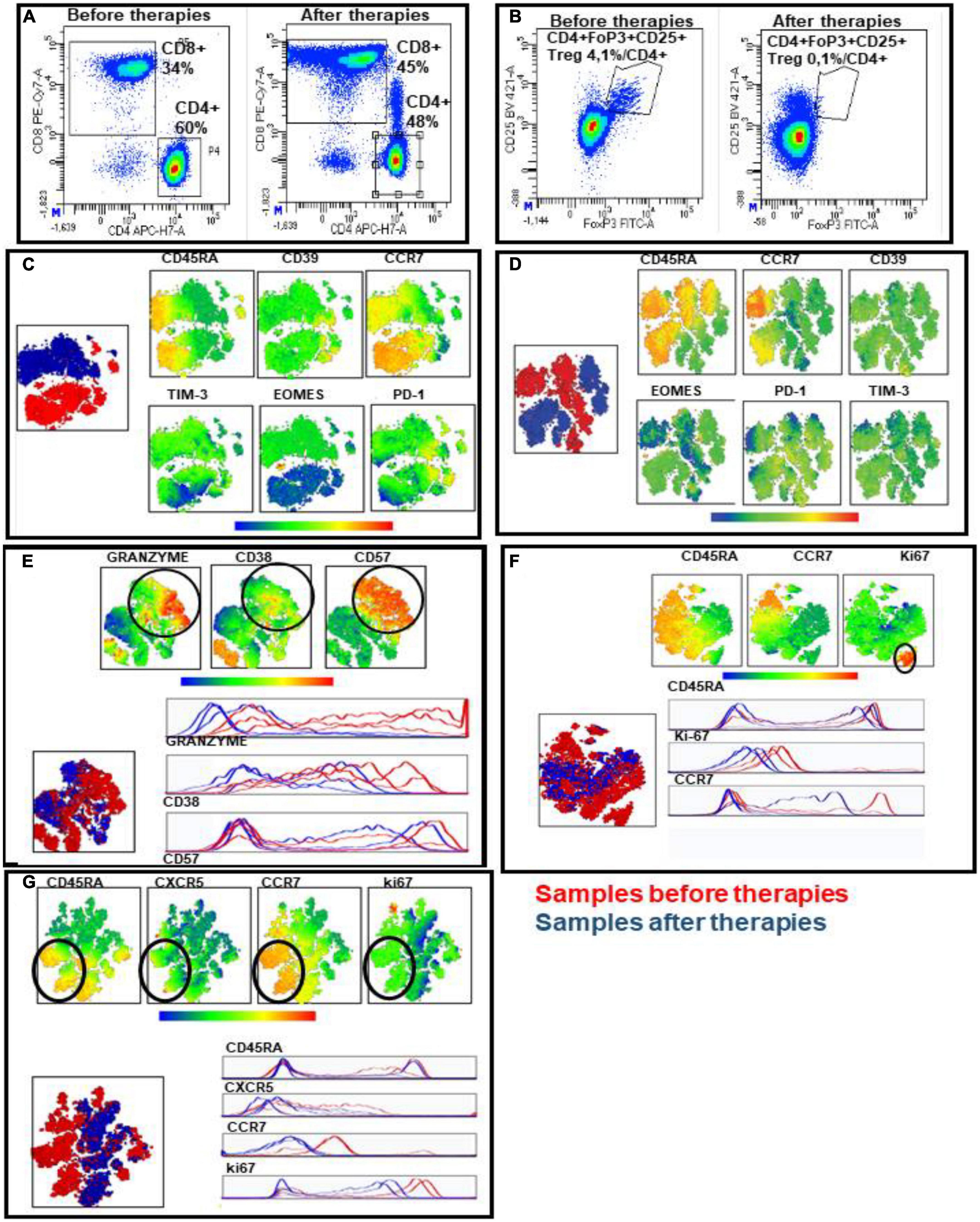
Figure 3. Immunofluorescence analyses of two patients with RT-PCR SARS-CoV-2 positive viremia and bronchoalveolar lavage fluid. (A,B) Representative examples of CD4+ and CD8+ T subset percentages on peripheral CD3+ T cells derived from before and after therapies (A) and frequency of circulating CD4+ Treg (CD4 + FoxP3 + CD25 +) on circulating CD4+ T population derived from before and after therapies (B). (C–G) Multidimensional data reduction analysis. t-SNE analysis of maturation, senescence, exhaustion, effector and activation markers of circulating CD4+ and CD8+ T cells on merged samples derived before (red clusters) and after (bleu clusters) therapies. In particular: the analysis of maturation and exhaustion marker expression in CD4+ (C) and CD8+ (D) T subsets; the analysis of maturation, senescence and granzyme effector molecule in CD8+ T cells (E); the evaluation of cycling cells by ki-67 marker in CD8+ (F) and CD4+ (G) T subsets.
1) The analysis of maturation curve and immune checkpoint expression confirmed the different dynamic in samples derived before therapies and after therapies both in CD4+ and CD8+ subsets due to the different viral pressure: (a) to concern the maturative status of CD4+ T lymphocytes, we observed a major cluster of central memory (CM) in samples before therapies, whereas effector memory (EM) and terminal effector memory (TEM) prevail in samples after therapies; consequentially, a major expression of immune checkpoints has been observed in samples after therapies, particularly for transcription factor EOMES analysis (Figure 3C); (b) the t-SNE maps of CD8+ T cells relative to the maturation curve also exhibit a progression versus advanced memory cells and a concomitant major expression of immune checkpoints, as EOMES and PD-1 (Figure 3D);
2) The t-SNE maps of CD8+ effector population showed that granzyme, relevant effector molecule for cytotoxic activity of T cells, resulted a highly discriminating factor when comparing the samples before and after therapies, in fact, we observed a reduction of granzyme positivity in CD57+ cells, a marker of terminally differentiated cells in non-RNAemic samples; furthermore, the activation level, evaluated by CD38 expression decreased in samples after therapies as expected at the solution of a viral infection (Figure 3E);
3) The evaluation of cycling cells by ki-67 marker shows that: (a) there is a cluster of activated and highly proliferative memory CD8+ T cells (ki-67+, CD45RA-CCR7-) in samples before therapies (Figure 3F); (b) CD4+ T cell comparison also showed a cluster of ki-67+ cells in samples before therapies which exhibits expression of CCR7, CXCR5 markers, showing a presence of T helper follicular (TFH) cells only in samples before therapies (Figure 3G). Therefore, the analysis of the CD4+ and CD8+ T cell maps analyzed before and after combination therapy in RNAemic and non-RNAemic samples, respectively, would seem to highlight immunological patterns indicative of a resolution of the infection in the samples derived after therapies, such as the decrease of EOMES expression, the activation status and the reduction of granzyme level.
We analysed the same cellular pattern in another patient with mantle cell lymphoma who underwent treatment with rituximab, bendamustine, cytarabine, with consequent lymphopenia and hypogammaglobulinemia. He was treated in RNAemic phase as antiviral therapy with remdesivir only and steroids and we did not find the same T cellular pattern, but we highlighted in the non-RNAemic phase an increase of granzyme in CD57+ cells and an increase of CD45+ TEM as higher pattern of cytotoxic cells, expression of infection not under control. In fact, that patient developed after few days later a new RNAemic phase of COVID-19 (19).
To confirm if these cellular features observed in CD4+ and CD8+ T cell populations were related to the therapy used, we studied also the circulating CD4+ and CD8+ T cells derived by two other patients (not immunocompromised and not under steroids) treated only with monoclonal antibodies. The t-SNE maps showed that CD4+ and CD8+ T cells clustered in a superimposable way in samples derived before therapies and after therapies not showing significantly different patterns in relation to maturation, activation and exhaustion markers (data not shown).
SARS-CoV-2 infection manifests with diverse clinical pictures, suggesting that the severity of symptoms might depend on the outcome of the SARS-CoV-2 immune system interaction within the patient (28–30).
The prolonged shedding of virus and persistent symptomatic SARS-CoV-2 infection have been reported in the immunocompromised patients, mainly in hematological, after B-cell depletion with anti-CD20 antibodies (19, 31–33).
As recently suggested by other experiences, combination therapy with monoclonal antibodies and one antiviral, also for a prolonged time, could contribute to virological success in immunocompromised patients (34, 35).
Sotrovimab and nirmatrelvir/ritonavir are two of the main drugs currently approved for the prevention of severe disease in the outpatient setting, but they are still not approved in the setting of COVID-19 hospitalized patients (36) RECOVERY was the first randomized, controlled, open-label trial to demonstrate the efficacy of the monoclonal antibodies casirivimab/imdevimab (3). Omicron variant showed reduced susceptibility to the use of casirivimab/imdevimab, thus leading to the use of other monoclonal antibodies, such as sotrovimab, in spite of the lack of high certainty evidence for hospitalized COVID-19 patients (37, 38).
During the study period, in our region, the prevalence of Omicron, BA.1 variant, was more than 80%.
Based on the previous assumption and on the therapeutic rationale of applying a combination of different molecules with different mechanisms of action, we chose to adopt an off-label combination therapy of monoclonal antibodies plus two antivirals.
The use of antiviral agents with monoclonal antibodies can have a potential advantage of higher efficacy due to a combination of two different antiviral mechanisms, since antiviral monotherapy might be an insufficient treatment option in the absence of humoral immunity (39). In the case of SARS-CoV-2 infection, in vitro data showed synergistic/additive activity of molnupiravir in combination with nirmatrelvir/ritonavir (40). Some recent experiences reported a successful use of combination therapy with antiviral and convalescent plasma or monoclonal antibodies (19, 41).
As of our knowledge, there are no data in literature regarding the use in combination at the same time of sotrovimab, remdesivir and nirmatrelvir/ritonavir, neither in vitro nor in vivo. Our patients were both treated with this off-label combination with an excellent and rapid clinical response, undetectable SARS-CoV-2 RNAemia and negative RT-PCR SARS-CoV-2 in NP swab.
Concerning the adaptive immune cellular response, all these observations seem to indicate that:
a) The immune system resulted activated and highly responsive to infection in samples before therapies, as demonstrated by the progression to advanced maturational states, positivity for ki-67 marker proliferation and CXCR5 expression in CD4+ T cells significative of active engagement of follicular T helper (TFH) cells.
b) After therapies, the dynamic of the clusters of the CD4+ and CD8+ T populations seem to indicate the conditions of an immune system oriented toward the resolution of the infection, as demonstrated by the expression of exhaustion markers, by the reduction of activation levels, absent expression of effector molecules (granzyme) and the decreased proliferative activity.
The humoral or cell-mediated immunity induced by active immunization or response to natural infection, may not develop or develop ineffectively or erratically, thus complicating the assessment of the cause of clinical worsening, thus requiring a different kind of treatment (42, 43). The introduction of new therapeutic options for the treatment of early infection and prevention of progression toward the severe form has further modified the timing of SARS-CoV-2 infection, with the possibility of a late onset of severe clinical manifestations of pneumonia after a few weeks from the onset of symptoms (44).
In our patients, the CD4+ and CD8+ T cells response detected an immunological patterns of a controlled infection as documented in the non-RNAemic samples after therapies, with the decrease of EOMES expression, the activation status and the reduction of granzyme level. These features are different in immunocompromised patient treated with remdesivir alone without control of RNAemic infection phase or in not immunocompromised patients treated only with monoclonal antibodies.
Several studies have now confirmed reduced antibody levels and seroconversion rates in anti-CD20 treated patients following SARS-CoV-2 infection; as B cell could play a role as antigen- presenting cells to naïve T cells, the question remains as whether B-cell depleted patients could still mount functional T cell responses to SARS-CoV-2 (45, 46).
This empiric combination of sotrovimab, remdesivir and nirmatrelvir/ritonavir was safe and apparently effective in our COVID-19 patients with positive RNAemia and a state of immunosuppression, although the inherent limitations of case reports in terms of generalization should be necessary acknowledged. Nonetheless, if confirmed by further investigation, this possible strategy of using a combination of different drugs at the same time could change the approach and the way of how we treat COVID-19 in the immunocompromised patient.
The original contributions presented in this study are included in the article/Supplementary material, further inquiries can be directed to the corresponding authors.
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
FB, CD, MiM, FM, FP, LT, CS, and MaM cared for the patient and supervised diagnostic and therapeutic strategies. DF, CU, GS, and GF supervised and performed immunological analysis. GC provided CT scan and interpretations. AO provided virological analysis. FB and CD wrote the manuscript. DG provided critical review of the manuscript contents and interpretation of data. FB, CD, and MaM performed literature review and provided concepts. MB supervised the analysis and provided concepts. All authors read and approved the final manuscript.
Thanks to the patients and their families for enduring the hardest times with dignity and determination and for always trusting us.
Outside the submitted work, DG reports investigator-initiated grants from Pfizer, Shionogi, and Gilead Italia and speaker fees and/or advisor fees from Pfizer and Tillotts Pharma. Outside the submitted work, MB reports research grants and/or personal fees for advisor/consultant and/or speaker/chairman from Bayer, BioMérieux, Cidara, Cipla, Gilead, Menarini, MSD, Pfizer, and Shionogi.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2022.1062450/full#supplementary-material
1. Beigel JH, Tomashek KM, Dodd LE, Mehta AK, Zingman BS, Kalil AC, et al. Remdesivir for the treatment of COVID-19 — final report. N Engl J Med. (2020) 383:1813–26. doi: 10.1056/NEJMoa2007764
2. Weinreich DM, Sivapalasingam S, Norton T, Ali S, Gao H, Bhore R, et al. REGEN-COV antibody combination and outcomes in outpatients with COVID-19. N Engl J Med. (2021) 385:e81. doi: 10.1056/NEJMoa2108163
3. Group Recovery Collaborative. Casirivimab and imdevimab in patients admitted to hospital with COVID-19 (RECOVERY): a randomised, controlled, open-label, platform trial. Lancet. (2022) 399:665–76. doi: 10.1016/S0140-6736(22)00163-5
4. Dougan M, Nirula A, Azizad M, Mocherla B, Gottlieb RL, Chen P, et al. Bamlanivimab plus etesevimab in mild or moderate COVID-19. N Engl J Med. (2021) 385:1382–92. doi: 10.1056/NEJMoa2102685
5. Gupta A, Gonzalez-Rojas Y, Juarez E, Casal MC, Moya J, Falci DR, et al. Early treatment for COVID-19 with SARS-CoV-2 neutralizing antibody sotrovimab. N Engl J Med. (2021) 385:1941–50. doi: 10.1056/NEJMoa2107934
6. Jayk Bernal A, Gomes da Silva M, Musungaie D, Kovalchuk E, Gonzalez A, Delos RV, et al. Molnupiravir for oral treatment of COVID-19 in nonhospitalized patients. N Engl J Med. (2022) 386:509–20. doi: 10.1056/NEJMoa2116044
7. Hammond J, Leister-Tebbe H, Gardner A, Abreu P, Bao W, Wisemandle W, et al. Oral nirmatrelvir for high-risk, nonhospitalized adults with COVID-19. N Engl J Med. (2022) 386:1397–408. doi: 10.1056/NEJMoa2118542
8. Gottlieb RL, Vaca CE, Paredes R, Mera J, Webb BJ, Perez G, et al. Early remdesivir to prevent progression to severe COVID-19 in outpatients. N Engl J Med. (2022) 386:305–15. doi: 10.1056/NEJMoa2116846
9. Eli Lilly and Company. A randomized, double-blind, placebo-controlled, phase 2 study to evaluate the efficacy and safety of mono and combination therapy with monoclonal antibodies in participants with mild to moderate COVID-19 illness (BLAZE-4). (2021). Available online at: https://clinicaltrials.gov/ct2/show/NCT04634409 (accessed March 15, 2022).
10. Levin M, Ustianowski A, De Wit S, Launay O, Avila M, Seegobin S, et al. PROVENT: phase 3 study of efficacy and safety of AZD7442 (tixagevimab/ cilgavimab) for pre-exposure prophylaxis of COVID-19 in adults. Open Forum Infect Dis. (2021) 8(Suppl. 1):S810. doi: 10.1093/ofid/ofab466.1646
11. Group Recovery Collaborative. Tocilizumab in patients admitted to hospital with COVID-19 (RECOVERY): a randomised, controlled, open-label, platform trial. Lancet. (2021) 397:1637–45. doi: 10.1016/S0140-6736(21)00676-0
12. Kyriazopoulou E, Poulakou G, Milionis H, Metallidis S, Adamis G, Tsiakos K, et al. Early treatment of COVID-19 with anakinra guided by soluble urokinase plasminogen receptor plasma levels: a double-blind, randomized controlled phase 3 trial. Nat Med. (2021) 27:1752–60. doi: 10.1038/s41591-021-01499-z
13. Marconi VC, Ramanan AV, de Bono S, Kartman CE, Krishnan V, Liao R, et al. Efficacy and safety of baricitinib for the treatment of hospitalised adults with COVID-19 (COV-BARRIER): a randomised, double-blind, parallel-group, placebo-controlled phase 3 trial. Lancet Respir Med. (2021) 9:1407–18. doi: 10.1016/S2213-2600(21)00331-3
14. Passamonti F, Cattaneo C, Arcaini L, Bruna R, Cavo M, Merli F, et al. Clinical characteristics and risk factors associated with COVID-19 severity in patients with haematological malignancies in Italy: a retrospective, multicentre, cohort study. Lancet Haematol. (2020) 7:e737–45. doi: 10.1016/S2352-3026(20)30251-9
15. Vijenthira A, Gong IY, Fox TA, Booth S, Cook G, Fattizzo B, et al. Outcomes of patients with hematologic malignancies and COVID-19: a systematic review and meta-analysis of 3377 patients. Blood. (2020) 136:2881–92. doi: 10.1182/blood.2020008824
16. Ljungman P, de la Camara R, Mikulska M, Tridello G, Aguado B, Zahrani M, et al. COVID-19 and stem cell transplantation; results from an EBMT and GETH multicenter prospective survey. Leukemia. (2021) 35:2885–94. doi: 10.1038/s41375-021-01302-5
17. Spanjaart A, Ljungman P, de La Camara R, Tridello G, Ortiz-Maldonado V, Urbano-Ispizua A, et al. Poor outcome of patients with COVID-19 after CAR T-cell therapy for B-cell malignancies: results of a multicenter study on behalf of the European society for blood and marrow transplantation (EBMT) infectious diseases working party and the European hematology association (EHA) lymphoma group. Leukemia. (2021) 35:3585–8. doi: 10.1038/s41375-021-01466-0
18. Ljungman P, Mikulska M, de la Camara R, Basak G, Chabannon C, Corbacioglu S, et al. The challenge of COVID-19 and hematopoietic cell transplantation; EBMT recommendations for management of hematopoietic cell transplant recipients, their donors, and patients undergoing CAR T-cell therapy. Bone Marrow Transplant. (2020) 55:2071–6. doi: 10.1038/s41409-020-0919-0
19. Sepulcri C, Dentone C, Mikulska M, Bruzzone B, Lai A, Fenoglio D, et al. The longest persistence of viable SARS-CoV-2 with recurrence of viremia and relapsing symptomatic COVID-19 in an immunocompromised patient—a case study. Open Forum Infect Dis. (2021) 8:ofab217. doi: 10.1093/ofid/ofab217
20. Aydillo T, Gonzalez-Reiche A, Aslam S, van de Guchte A, Khan Z, Obla A, et al. Shedding of viable SARS-CoV-2 after immunosuppressive therapy for cancer. N Engl J Med. (2020) 383:2586–8. doi: 10.1056/NEJMc2031670
21. Avanzato V, Matson M, Seifert S, Pryce R, Williamson B, Anzick S, et al. Case study: prolonged infectious SARS-CoV-2 shedding from an asymptomatic immunocompromised individual with cancer. Cell. (2020) 183:1901–12.e9. doi: 10.1016/j.cell.2020.10.049
22. Baang JH, Smith C, Mirabelli C, Valesano AL, Manthei DM, Bachman MA, et al. Prolonged severe acute respiratory syndrome coronavirus 2 replication in an immunocompromised patient. J Infect Dis. (2021) 223:23–7. doi: 10.1093/infdis/jiaa666
23. Nakajima Y, Ogai A, Furukawa K, Arai R, Anan R, Nakano Y, et al. Prolonged viral shedding of SARS-CoV-2 in an immunocompromised patient. J Infect Chemother. (2021) 27:387–9. doi: 10.1016/j.jiac.2020.12.001
24. Cesaro S, Ljungman P, Mikulska M, Hirsch HH, von Lilienfeld-Toal M, Cordonnier C, et al. Recommendations for the management of COVID-19 in patients with haematological malignancies or haematopoietic cell transplantation, from the 2021 European conference on infections in leukaemia (ECIL 9). Leukemia. (2022) 36:1467–80. doi: 10.1038/s41375-022-01578-1
25. Choi B, Choudhary M, Regan J, Sparks JA, Padera RF, Qiu X, et al. Persistence and evolution of SARS-CoV-2 in an immunocompromised host. N Engl J Med. (2020) 383:2291–3. doi: 10.1056/NEJMc2031364
26. Helleberg M, Niemann CU, Moestrup KS, Kirk O, Lebech A, Lane C, et al. Persistent COVID-19 in an immunocompromised patient temporarily responsive to two courses of remdesivir therapy. J Infect Dis. (2020) 222:1103–7. doi: 10.1093/infdis/jiaa446
27. Akinosoglou K, Paliogianni F, Spyridonidis A, Symeonidis A, Alexopoulos LG, Ziazias D, et al. SARS-CoV-2 persistence and non-protective immunity in infected haematological patients. Br J Haematol. (2020) 192:e51–4. doi: 10.1111/bjh.17212
28. Mehta P, McAuley D, Brown M, Sanchez E, Tattersall R, Manson JJ. COVID-19: consider cytokine storm syndromes and immunosuppression. Lancet. (2020) 395:1033–4. doi: 10.1016/S0140-6736(20)30628-0
29. Siddiqi H, Mehra MR. COVID-19 illness in native and immunosuppressed states: a clinical–therapeutic staging proposal. J Heart Lung Transplant. (2020) 39:405–7. doi: 10.1016/j.healun.2020.03.012
30. Robinson PC, Liew DF, Tanner HL, Grainger JR, Dwek RA, Reisler RB, et al. COVID-19 therapeutics: challenges and directions for the future. Proc Natl Acad Sci USA. (2022) 119:e2119893119. doi: 10.1073/pnas.2119893119
31. Lee C, Shah M, Hoyos D, Solovyov A, Douglas M, Taur Y, et al. Prolonged SARS-CoV-2 infection in patients with lymphoid malignancies. Cancer Discov. (2022) 12:62–73.
32. Westblade L, Brar G, Pinheiro L, Paidoussis D, Rajan M, Martin P, et al. SARS-CoV-2 viral load predicts mortality in patients with and without cancer who are hospitalized with COVID-19. Cancer Cell. (2020) 38:661–71.e2.
33. Belkin A, Leibowitz A, Shargian L, Yahav D. The unique presentation of SARS-CoV-2 Infection in patients with B-cell depletion: definition of “persistent inflammatory sero-negative COVID”. Clin Microbiol Infect. (2022). [Epub ahead of print]. doi: 10.1016/j.cmi.2022.10.007
34. Brown L, Moran E, Goodman A, Baxendale H, Bermingham W, Buckland M, et al. Treatment of chronic or relapsing COVID-19 in immunodeficiency. J Allergy Clin Immunol. (2022) 149:557–61.e1. doi: 10.1016/j.jaci.2021.10.031
35. Garzi G, Cinetto F, Firinu D, Di Napoli G, Lagnese G, Punziano A, et al. Real-life data on monoclonal antibodies and antiviral drugs in Italian inborn errors of immunity patients during COVID-19 pandemic. Front Immunol. (2022) 13:947174. doi: 10.3389/fimmu.2022.947174
36. Parums D. Editorial: current status of oral antiviral drug treatments for SARS-CoV-2 infection in non-hospitalized patients. Med Sci Monit. (2022) 28:e935952. doi: 10.12659/MSM.935952
37. Takashita E, Kinoshita N, Yamayoshi S, Sakai-Tagawa Y, Fujisaki S, Ito M, et al. «Efficacy of antibodies and antiviral drugs against COVID-19 omicron variant». N Engl J Med. (2022) 386:995–8. doi: 10.1056/NEJMc2119407
38. Zhou H, Dcosta BM, Landau NR, Tada T. «Resistance of SARS-CoV-2 omicron BA.1 and BA.2 variants to vaccine-elicited sera and therapeutic monoclonal antibodies». Viruses. (2022) 14:1334. doi: 10.3390/v14061334
39. Tepasse P, Hafezi W, Lutz M, Kühn J, Wilms C, Wiewrodt R, et al. Persisting SARS-CoV-2 viraemia after rituximab therapy: two cases with fatal outcome and a review of the literature. Br J Haematol. (2020) 190:185–8. doi: 10.1111/bjh.16896
40. Li P, Wang Y, Lavrijsen M, Lamers M, de Vries A, Rottier R, et al. SARS-CoV-2 Omicron variant is highly sensitive to molnupiravir, nirmatrelvir, and the combination. Cell Res. (2022) 32:322–4. doi: 10.1038/s41422-022-00618-w
41. Magyari F, Pinczés LI, Páyer E, Farkas K, Ujfalusi S, Diószegi Á, et al. Early administration of remdesivir plus convalescent plasma therapy is effective to treat COVID-19 pneumonia in B-cell depleted patients with hematological malignancies. Ann Hematol. (2022) 101:2337–45. doi: 10.1007/s00277-022-04924-6
42. Toor S, Saleh R, Sasidharan Nair V, Taha R, Elkord E. T-cell responses and therapies against SARS-CoV-2 infection. Immunology. (2021) 162:30–43. doi: 10.1111/imm.13262
43. Merad M, Blish C, Sallusto F, Iwasaki A. The immunology and immunopathology of COVID-19. Science. (2022) 375:1122–7. doi: 10.1126/science.abm8108
44. Tao K, Tzou P, Nouhin J, Bonilla H, Jagannathan P, Shafer R. SARS-CoV-2 antiviral therapy. Clin Microbiol Rev. (2021) 34:e0010921. doi: 10.1128/CMR.00109-21
45. Zabalza A, Caìrdenas-Robledo S, Tagliani P, Arrambide G, Otero-Romero S, Carbonell-Mirabent P, et al. COVID-19 in multiple sclerosis patients: susceptibility, severity risk factors and serological response. Eur J Neurol. (2021) 28:3384–95. doi: 10.1111/ene.14690
Keywords: salvage therapy, COVID-19, immunocompromised, monoclonal antibodies, sotrovimab, nirmatrelvir/ritonavir, remdesivir
Citation: Baldi F, Dentone C, Mikulska M, Fenoglio D, Mirabella M, Magnè F, Portunato F, Altosole T, Sepulcri C, Giacobbe DR, Uras C, Scavone G, Taramasso L, Orsi A, Cittadini G, Filaci G and Bassetti M (2023) Case report: Sotrovimab, remdesivir and nirmatrelvir/ritonavir combination as salvage treatment option in two immunocompromised patients hospitalized for COVID-19. Front. Med. 9:1062450. doi: 10.3389/fmed.2022.1062450
Received: 05 October 2022; Accepted: 12 December 2022;
Published: 09 January 2023.
Edited by:
Aleksandra Barac, University of Belgrade, SerbiaReviewed by:
Davide Firinu, Università di Cagliari, ItalyCopyright © 2023 Baldi, Dentone, Mikulska, Fenoglio, Mirabella, Magnè, Portunato, Altosole, Sepulcri, Giacobbe, Uras, Scavone, Taramasso, Orsi, Cittadini, Filaci and Bassetti. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Federico Baldi,  ZmVkZS5ibGRAZ21haWwuY29t; Daniele Roberto Giacobbe, ZGFuaWVsZXJvYmVydG8uZ2lhY29iYmVAdW5pZ2UuaXQ=
ZmVkZS5ibGRAZ21haWwuY29t; Daniele Roberto Giacobbe, ZGFuaWVsZXJvYmVydG8uZ2lhY29iYmVAdW5pZ2UuaXQ=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.