 Fangbo Lin
Fangbo Lin
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Immunol. , 10 January 2025
Sec. Systems Immunology
Volume 15 - 2024 | https://doi.org/10.3389/fimmu.2024.1543009
This article is part of the Research Topic Harnessing Big Data for Precision Medicine: Revolutionizing Diagnosis and Treatment Strategies View all 33 articles
Tuberculous meningitis (TBM), a severe form of non-purulent meningitis caused by Mycobacterium tuberculosis (Mtb), is the most critical extrapulmonary tuberculosis (TB) manifestation, with a 30–40% mortality rate despite available treatment. The absence of distinctive clinical symptoms and effective diagnostic tools complicates early detection. Recent advancements in nucleic acid detection, genomics, metabolomics, and proteomics have led to novel diagnostic approaches, improving sensitivity and specificity. This review focuses on nucleic acid-based methods, including Xpert Ultra, metagenomic next-generation sequencing (mNGS), and single-cell sequencing of whole brain Tissue, alongside the diagnostic potential of metabolomic and proteomic biomarkers. By evaluating the technical features, diagnostic accuracy, and clinical applicability, this review aims to inform the optimization of TBM diagnostic strategies and explores the integration and clinical translation of multi-omics technologies.
Tuberculous meningitis (TBM), caused by Mycobacterium tuberculosis (Mtb), is a fatal form of non-purulent meningitis and one of the deadliest types of extrapulmonary tuberculosis (TB). Despite the availability of anti-TB treatment, the mortality rate for TBM exceeds 30% (1), with even higher rates in HIV co-infected individuals (2). Early diagnosis and treatment are essential, but challenges persist due to TBM’s nonspecific clinical signs and the low Mtb load in cerebrospinal fluid (CSF). Traditional diagnostic methods, such as acid-fast staining, have low sensitivity, while Mtb culture is time-consuming (3–7). Recent advancements in diagnostics, such as Xpert Ultra and mNGS, have improved sensitivity and shortened diagnostic delays (8–10). Additionally, metabolomic and proteomic biomarkers, such as elevated citrulline, lactate, apoB, and NELL2, hold promise for diagnosis and differential diagnosis (11, 12).
Furthermore, single-cell sequencing and omics technologies offer new insights into TBM pathogenesis and potential therapeutic targets (13, 14). This review provides an overview of recent advances in TBM diagnostics and therapeutics, covering nucleic acid detection, omics-based biomarker discovery, pharmacological therapies, and adjunctive strategies, offering a comprehensive reference for clinical practice (Figure 1).
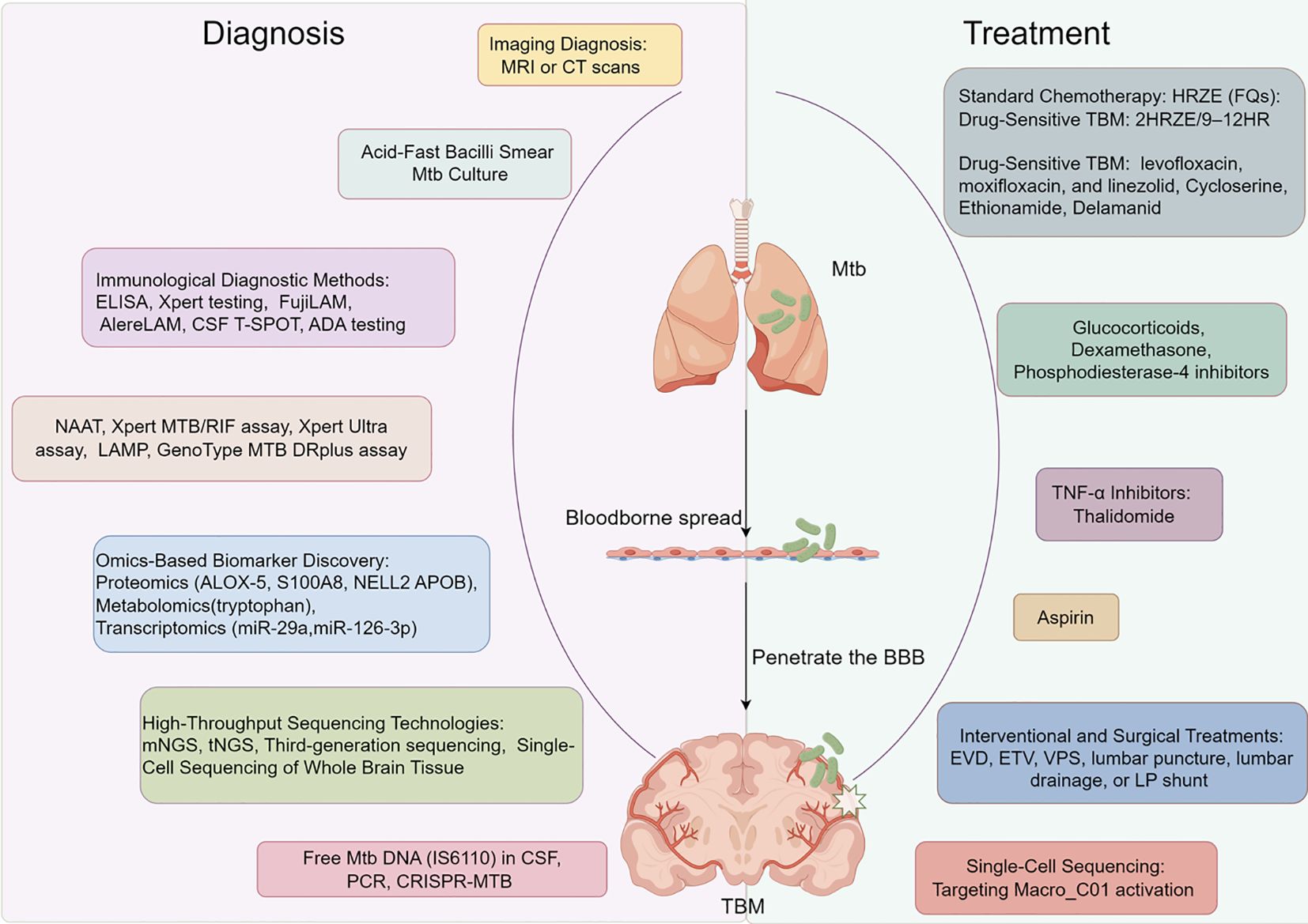
Figure 1. Tuberculous meningitis diagnosis and treatment.
Radiologically, TBM presents with basal cistern and meningeal enhancement, brain infarction, hydrocephalus, and tuberculomas, with basal meningeal enhancement being a key feature (15). Contrast-enhanced MRI or CT should be performed before and after treatment to monitor progression. Thoracic CT and other imaging techniques help identify active TB lesions (16, 17). Pathologically, TBM includes inflammatory exudates, granulomas, and vasculitis, with 77% of patients showing cerebral arteritis, leading to infarction and hydrocephalus (2, 18). Rare cases, such as brain tuberculomas post-BCG vaccination, emphasize vigilance in vaccinated infants (19). Some patients exhibit pituitary adenoma-like lesions with headaches and vision loss. Combining imaging and histopathology is essential for accurate diagnosis (20).
The gold standard for TBM diagnosis is detecting Mtb in CSF. However, due to low bacterial load, conventional bacteriological tests show limited sensitivity (3, 4). Enhancing sensitivity remains a major research focus.
Acid-fast staining is rapid and cost-effective but has low sensitivity (<20%), occasionally near 0% (2, 21). Modified techniques, such as centrifuging larger CSF volumes and using fluorescence microscopy, have improved positivity rates to 60% (21). Mtb culture remains the “gold standard.” Liquid cultures are about 10% more sensitive than solid cultures but are prone to cross-contamination, while solid cultures have low sensitivity (4.3%) and take up to 56 days (22) (Table 1). Repeated CSF sampling and modified acid-fast staining can improve results, though challenges persist (23, 24). Fluorescence microscopy, including LED fluorescence, offers higher sensitivity at lower costs (16), though resource limitations hinder its widespread use (22).
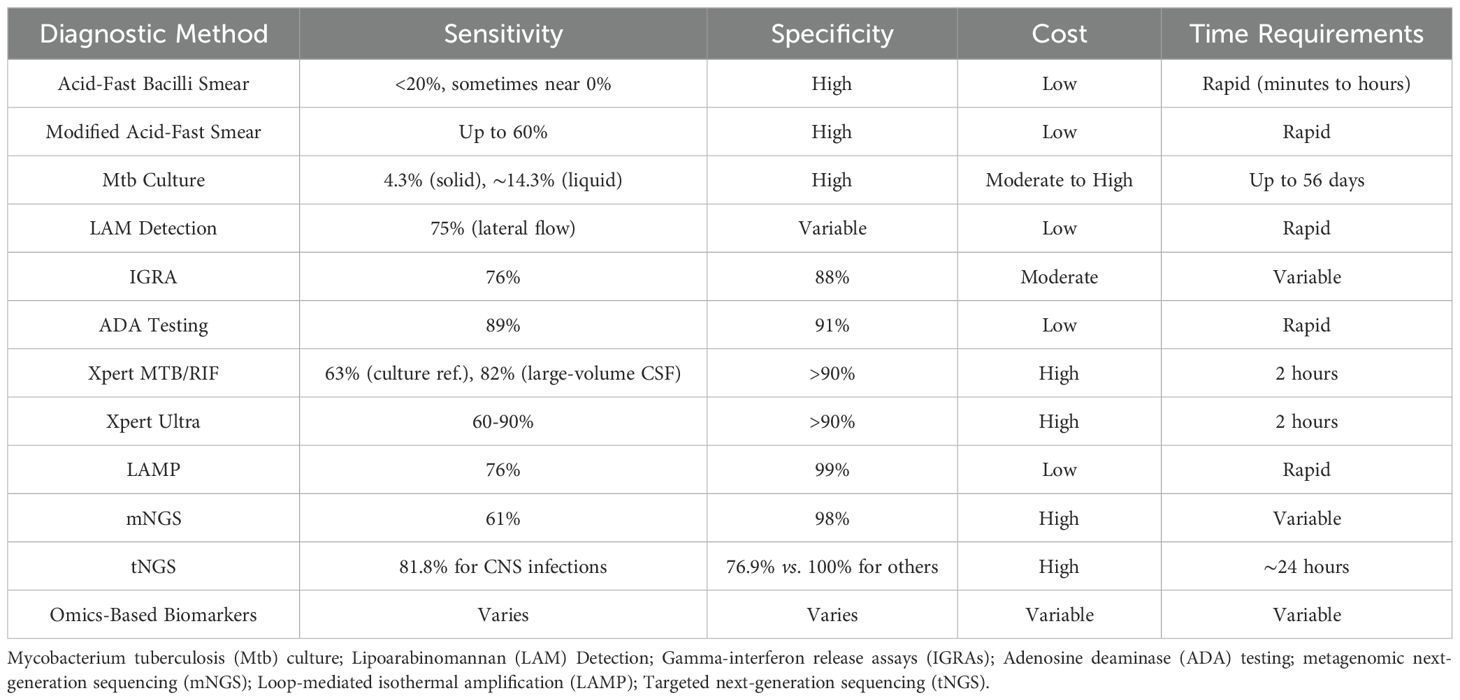
Table 1. Comparison of diagnostic methods for tuberculous meningitis.
CSF antigen-antibody detection has long been studied but is hindered by poor sensitivity and specificity of many tests. A 2015 study reported sensitivities of 75% and 43% for detecting lipoarabinomannan (LAM) with lateral flow and ELISA methods, respectively, while Xpert testing showed 100% sensitivity (25). Although FujiLAM is more sensitive than AlereLAM in urine (26), its diagnostic value in CSF is unclear. Gamma-interferon release assays (IGRAs), such as CSF T-SPOT, detect TBM infection by measuring gamma-interferon levels, with sensitivity of 76% and specificity of 88%. However, it requires large CSF volumes (>6 mL) and has a 15% indeterminate rate (27). Adenosine deaminase (ADA) testing in CSF shows 89% sensitivity and 91% specificity of TBM, but ADA levels in bacterial and viral meningitis complicate interpretation due to unclear diagnostic cut-offs (28).
Nucleic acid amplification tests (NAAT) are essential for TBM diagnosis, enhancing sensitivity (82%) and specificity (99%) versus culture, and 68% sensitivity with 98% specificity against clinical diagnosis (29, 30). The World Health Organization (WHO)-recommended Xpert MTB/RIF detects TB and rifampin resistance within 2 hours (31), with 63% sensitivity versus culture, increasing to 82% with large-volume CSF (32, 33). Xpert Ultra, with a sevenfold lower detection threshold (22, 31), achieves 60–90% sensitivity and >90% specificity (34, 35) but is limited by high cost and equipment requirements (36, 37). Loop-mediated isothermal amplification (LAMP) offers 76% sensitivity and 99% specificity (38), reaching 88% sensitivity and 100% specificity when multiple targets are used, though contamination risks persist (39). The GenoType MTB DRplus assay detects Mtb and resistance genes with 33% sensitivity and 98% specificity, constrained by complexity and cost (40).
Advances in omics technologies offer promising avenues for identifying TBM-specific biomarkers, as CSF may harbor distinct markers due to the unique pathogenic mechanisms of TBM.
(і) Proteomics: Limited studies include Kataria et al. (41), who identified 19 differential proteins with ALOX-5 as a potential marker; Ou et al. (42), who confirmed the association of S100A8 and APOB using ELISA; and Mu et al. (43), who found 111 differential proteins, highlighting NELL2 and APOB. These studies require larger, more diverse samples for validation.
(іі) Metabolomics: Li et al. (44) identified 25 metabolites differing between TBM and viral meningitis using 1H-NMR, while another study (45) reported significant changes in CSF and blood metabolites, particularly reduced tryptophan correlated with prognosis. Multicenter validation is needed.
(ііі) Transcriptomics: MicroRNAs such as miR-29a (46) and miR-126-3p (47) show potential as diagnostic markers for TBM, but further research is necessary across different diagnoses.
mNGS sequences genetic material using random primers, filtering out host DNA to identify microorganisms present (39, 48). It outperforms traditional methods in detecting Mtb, viruses, anaerobes, and fungi, particularly in cases missed by Xpert Ultra or culture (48). A 2019 study reported mNGS sensitivity of 66.67% for TBM, higher than smear (33.33%), PCR (25%), and culture (8.33%) (3), with meta-analyses showing 61% sensitivity and 98% specificity (49). However, mNGS may detect contaminants causing false positives (50–52). Low Mtb sequences in CSF due to DNA extraction issues can be improved with optimized centrifugation (50, 53), with optimized centrifugation improving sensitivity (53). Combining mNGS with other methods may enhance detection rates (3, 6, 54, 55).
tNGS combines targeted PCR amplification with high-throughput sequencing, focusing on specific nucleic acid regions to reduce interference from human genes and background flora, thus decreasing detection costs and time (around 24 hours) (56, 57). However, tNGS can only detect predefined targets, limiting its ability to identify unknown pathogens and relying on clinician judgment (58). DeeplexMyc-TB, introduced in 2019, uses tNGS to identify 18 drug resistance genes in the Mtb complex and detect resistance to multiple anti-tuberculosis drugs (59). tNGS has demonstrated high efficiency in detecting drug-resistant TB (60). Although its effectiveness in TBM diagnosis remains untested, studies show tNGS achieves 81.8% sensitivity for CNS infections, surpassing culture and smear (13.6%), though with lower specificity (76.9% vs. 100%) (61). In one case, tNGS successfully detected Mtb in a patient with negative mNGS results for bronchoalveolar lavage fluid and lung tissue, confirming secondary tissue-associated pneumonia. The patient improved significantly after anti-TB therapy (62).
Third-generation sequencing enables direct analysis of single DNA or RNA molecules without the need for fragmentation or amplification, providing longer reads ideal for studying high-repeat, GC-rich Mtb sequences (63). The PacBio SMRT platform detects fluorescence signals during nucleotide incorporation, aiding in the identification of Mtb genomic methylation sites and revealing lineage-specific and resistance-associated methylation patterns (64–68). These profiles correlate with transcription levels, nitrogen metabolism, and protein interactions (66, 67). Oxford Nanopore Technologies (ONT) uses nanopore sequencing, which detects changes in electrical current as nucleic acids pass through pores. The MinION platform offers rapid detection of Mtb resistance genes. Despite higher error rates, ONT’s calibration aligns its results with second-generation sequencing, achieving 94.8% sensitivity and 98.0% specificity with shorter detection times (69–75).
Using 10X Genomics, Zhang et al. identified 15 cell types in whole brain tissue and observed inflammatory transcriptional changes across them. Stat1 and IRF1 were found to mediate inflammatory responses in macrophages and microglia, while decreased oxidative phosphorylation in neurons correlated with neurodegeneration in TBM patients. Reduced Frmd4a in ependymal cells was linked to hydrocephalus and neurodegeneration (13). Through motif enrichment analysis (miReact), they constructed miRNA-mRNA networks, including immune-inflammatory networks in macrophages and microglia, oxidative phosphorylation networks in neurons, and ion and protein transport networks in ependymal cells. qRT-PCR and RNA scope revealed significantly elevated miR-21a-3p levels in TBM brain tissue compared to normal tissue, suggesting its potential as a diagnostic biomarker (14).
The implementation and application of high-throughput technologies can significantly enhance diagnostic accuracy and speed, thereby improving patient outcomes. However, simplified procedures and user-friendly interfaces can further facilitate the adoption of these technologies by non-experts, making their integration into clinical workflows more effective.
Emerging molecular detection methods show promise in diagnosing TBM but require further validation for clinical use. Li et al. (76) found that free Mtb DNA (IS6110) in CSF exhibited a 56.5% sensitivity in 46 clinically diagnosed TBM patients, surpassing smear (2.2%), culture (13%), and Xpert (23.9%). Shao et al. (77) reported a 93.3% sensitivity for free Mtb DNA in 84 suspected TBM cases, matching Xpert Ultra and outperforming culture (13.3%). Li et al. (78) used digital PCR to detect IS6110 in CSF from 101 HIV-negative TBM patients, achieving a sensitivity of 70%, higher than Xpert (30%). Ai et al. (79) applied CRISPR technology for diagnosing pulmonary and extrapulmonary TB, requiring smaller samples and shorter detection times. In a study of 27 TBM patients, CRISPR-MTB sensitivity was 73%, outperforming Xpert (54%) and culture (25%). Larger studies are necessary to validate these methods for wider clinical adoption.
Diagnostic methods for TBM each have distinct strengths and limitations. Traditional techniques like acid-fast smear and culture are widely accessible but suffer from low sensitivity and long turnaround times. Nucleic acid amplification methods (e.g., Xpert MTB/RIF, mNGS) offer higher sensitivity and rapid results but are costly and require specialized equipment (80). Immunological assays provide quick diagnostics but often lack specificity. Omics-based approaches (proteomics, metabolomics, transcriptomics) show promise for identifying specific biomarkers but need further validation (81). Integrating multiple diagnostic modalities, such as combining nucleic acid amplification with omics biomarkers, may enhance sensitivity and specificity, enabling earlier detection and better differentiation from other forms of meningitis. Future research should focus on validating combined strategies in diverse clinical settings to improve TBM diagnosis.
Treatment for drug-sensitive TBM typically includes a combination of rifampin (R), isoniazid (H), ethambutol (E), and pyrazinamide (Z) (HRZE), supplemented by fluoroquinolones (FQs), with a treatment duration of over nine months (82). Increasingly, adjunctive immunotherapy and interventional therapies are used. Key considerations include selecting drugs with good blood-brain barrier (BBB) permeability, adjusting dosages, and combining FQs to optimize outcomes. For multidrug-resistant (MDR) TBM, regimens must include at least four effective first- or second-line drugs, with attention to BBB penetration and prolonged treatment (83).
WHO recommends an initial 2-month intensive HRZE regimen, followed by 9–12 months of HR consolidation therapy (2HRZE/9–12HR) (84). However, this approach, based on pulmonary TB protocols, does not fully address BBB drug penetration. Pyrazinamide, with excellent BBB penetration, is crucial, and higher doses may optimize therapy (85). Isoniazid also effectively crosses the BBB, though high-dose efficacy remains unclear, with a recommended dose of 300–600 mg/day (86). Rifampin is essential, but its CSF concentration often falls below the minimum inhibitory concentration (MIC). High-dose rifampin (20–35 mg/kg) may improve efficacy, though its impact on survival needs further study (84, 85, 87, 88). Recent research suggests that combining high-dose rifampin with levofloxacin during the intensive phase does not significantly improve survival, though it raises rifampin CSF concentrations (89). Additionally, other treatment strategies can be classified based on drug-sensitive TBM. For instance, adjunctive therapies such as glucocorticoids and aspirin are primarily recommended for drug-sensitive cases to reduce inflammation and prevent neurological complications (90). These treatments are integrated with standard chemotherapy to enhance patient outcomes. Furthermore, immunomodulatory agents like TNF-α inhibitors may also be considered, although their use is more cautiously approached in drug-sensitive TBM due to potential side effects (91).
WHO guidelines for MDR and rifampin-resistant (RR-TB) TBM emphasize DST-guided therapy and the use of drugs with high BBB permeability (92, 93). Key agents include levofloxacin, moxifloxacin, and linezolid, which have good CNS penetration (85, 94). Linezolid improves clinical parameters such as body temperature, CSF leukocyte count, and treatment success rates, although its safety and efficacy in resistant TBM require further investigation (95, 96). Cycloserine and ethionamide are viable alternatives to ethambutol but are associated with neurotoxicity and gastrointestinal side effects (97). Delamanid offers superior survival outcomes in drug-resistant TBM due to excellent CNS penetration (85). In contrast, drugs like para-aminosalicylic acid and ethambutol have poor permeability and limited effectiveness (94). Moreover, certain treatment strategies are more effective for drug-resistant TBM. For example, the use of second-line anti-TB drugs such as bedaquiline and linezolid is crucial in managing MDR-TBM. These drugs, often combined with fluoroquinolones and other agents with good BBB penetration, provide a tailored approach to overcoming resistance (98). Additionally, adjunctive therapies like aspirin and glucocorticoids may be utilized to mitigate inflammatory responses, although their roles are more prominently defined in drug-sensitive TBM (99). The differentiation in treatment approaches underscores the importance of accurate TBM classification to optimize therapeutic efficacy.
Glucocorticoids, primarily dexamethasone, reduce inflammation, repair BBB damage, and decrease brain edema, improving survival in HIV-negative TBM patient (85, 100, 101). Hydrocortisone is used for hyponatremia due to cerebral salt wasting, however, they do not lower long-term neurological sequelae risks or clearly prevent strokes (85, 101). Combining glucocorticoids with anti-TB therapy reduces acute-phase mortality and neurological damage, though CNS damage may persist after tapering dexamethasone (102, 103). Phosphodiesterase-4 inhibitors (102) and thalidomide has shown some efficacy as adjunct therapy in selected cases but is limited by significant side effects (103, 104). Although extending dexamethasone treatment may improve outcomes, CNS damage risk persists after dose tapering or discontinuation (103). Most guidelines recommend adjunctive corticosteroids in the acute phase, but long-term efficacy and safety warrant further study (102, 103).
TNF-α plays a key role in TBM pathogenesis by activating macrophages and forming caseous granulomas. Thalidomide, a TNF-α inhibitor, reduces inflammation and improves survival in TBM animal models, halving mortality rates. However, its teratogenicity and potential to activate T-cells limit its use in pregnant women and broader clinical application (105, 106).
Aspirin provides antithrombotic and anti-inflammatory effects by inhibiting cyclooxygenase and reducing prostaglandin release, lowering stroke risk in TBM (100). Misra et al. (107) found that while aspirin did not significantly reduce stroke incidence, it reduced mortality. Higher doses improved therapeutic outcomes (108, 109). Yadav (110) suggested combining aspirin with corticosteroids to reduce TBM mortality, forming a basis for Phase III trials. Rizvi et al. (111) showed that while aspirin combined with anti-TB regimens did not lower mortality, it significantly reduced stroke risk without increasing adverse events compared to placebo. Current evidence supports aspirin’s efficacy in mitigating stroke risk, but more studies are needed to confirm long-term benefits when combined with corticosteroids (107).
TBM patients often develop hydrocephalus and brain edema (112). Surgical interventions like external ventricular drainage (EVD), third ventriculostomy (ETV), or ventriculoperitoneal shunting (VPS) can relieve intracranial pressure when conventional treatments fail (113). Other options include lumbar puncture, lumbar drainage, or lumbar-peritoneal (LP) shunt to avoid cranial surgery. Endoscopic third ventriculostomy is suitable for non-communicating hydrocephalus. Loan et al. (113) reported a 1-month mortality rate of 33.3%-61.9% in HIV-positive adults undergoing VPS for TBM, though further studies are needed. Kamat et al. found VPS blockage rates of 27.5% in pediatric and 25.5% in adult TBM patients. High CSF protein concentration (2.94 g/L in blocked cases vs. 1.76 g/L in non-blocked cases) was identified as a risk factor, emphasizing the need to reduce CSF protein levels before VPS (114).
Single-cell transcriptomics by Mo et al. identified 33 monocyte populations in CSF and PBMCs of children with TBM, highlighting distinct myeloid clusters and CD4/CD8 T-cell subsets with unique effector functions. Complement-activated microglial cells (Macro_C01) were linked to neuroinflammatory responses associated with persistent meningitis, amplifying inflammatory signaling through interactions with CD4_C04 subsets. Targeting Macro_C01 activation has been suggested as a therapeutic approach for pediatric TBM. Elevated C1Q, CRP, and cytokines (TNF-α, IL-6) in CSF further indicate their potential as TBM diagnostic biomarkers (115).
TBM remains highly lethal and disabling due to its complex pathophysiology and the lack of sensitive, specific diagnostics, which delay early diagnosis and treatment. Recent advancements in laboratory diagnostics, including nucleic acid-based methods, proteomics, and metabolomics, have enhanced diagnostic sensitivity and specificity despite technical challenges. Therapeutically, combining traditional anti-tuberculous treatments with adjunctive therapies has improved survival rates and reduced complications. Surgical innovations like ventriculoperitoneal shunting and third ventriculostomy effectively manage TBM-related hydrocephalus and intracranial hypertension. Additionally, single-cell sequencing and transcriptomics are identifying therapeutic targets, advancing precision medicine. Integrating these diagnostic and therapeutic strategies with public health initiatives is essential to reduce TBM’s global burden and improve patient outcomes.
FL: Funding acquisition, Writing – original draft, Writing – review & editing.
The author declare financial support was received for the research, authorship, and/or publication of this article. This study was provided by Hunan Provincial Natural Science Foundation of China (No.2024JJ9510).
The author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Foppiano Palacios C, Saleeb PG. Challenges in the diagnosis of tuberculous meningitis. J Clin Tuberc Other Mycobact Dis. (2020) 20:100164. doi: 10.1016/j.jctube.2020.100164
2. Wilkinson RJ, Rohlwink U, Misra UK, van Crevel R, Mai NTH, Dooley KE, et al. Tuberculous meningitis. Nat Rev Neurol. (2017) 13:581–98. doi: 10.1038/nrneurol.2017.120
3. Wang S, Chen Y, Wang D, Wu Y, Zhao D, Zhang J, et al. The feasibility of metagenomic next-Generation sequencing to identify pathogens causing tuberculous meningitis in cerebrospinal fluid. Front Microbiol. (2019) 10:1993. doi: 10.3389/fmicb.2019.01993
4. Stadelman AM, Ssebambulidde K, Buller A, Tugume L, Yuquimpo K, Bakker CJ, et al. Cerebrospinal fluid AFB smear in adults with tuberculous meningitis: A systematic review and diagnostic test accuracy meta-analysis. Tuberculosis (Edinb). (2022) 135:102230. doi: 10.1016/j.tube.2022.102230
5. Wang T, Feng GD, Pang Y, Yang YN, Dai W, Zhang L, et al. Sub-optimal specificity of modified ziehl-Neelsen staining for quick identification of tuberculous meningitis. Front Microbiol. (2016) 7:2096. doi: 10.3389/fmicb.2016.02096
6. Lin Y, Zhang W, Xiong Y, Wang Y, Yu Q, Ma Y, et al. Comparative performance of microbiological methods for the detection of tuberculous meningitis pathogens in cerebrospinal fluid. Diagn Microbiol Infect Dis. (2023) 107:116025. doi: 10.1016/j.diagmicrobio.2023.116025
7. Tortoli E, Cichero P, Piersimoni C, Simonetti MT, Gesu G, Nista D. Use of BACTEC MGIT 960 for recovery of mycobacteria from clinical specimens: multicenter study. J Clin Microbiol. (1999) 37:3578–82. doi: 10.1128/JCM.37.11.3578-3582.1999
8. Chakravorty S, Simmons AM, Rowneki M, Parmar H, Cao Y, Ryan J, et al. The new xpert MTB/RIF ultra: improving detection of mycobacterium tuberculosis and resistance to rifampin in an assay suitable for point-of-Care testing. mBio. (2017) 8:e00812–17. doi: 10.1128/mBio.00812-17
9. Shen Y, Yu G, Zhao W, Lang Y. Efficacy of Xpert MTB/RIF Ultra in diagnosing tuberculosis meningitis: A systematic review and meta-analysis. Med (Baltimore). (2021) 100:e26778. doi: 10.1097/MD.0000000000026778
10. Li Y, Bian W, Wu S, Zhang J, Li D. Metagenomic next-generation sequencing for Mycobacterium tuberculosis complex detection: a meta-analysis. Front Public Health. (2023) 11:1224993. doi: 10.3389/fpubh.2023.1224993
11. Tomalka J, Sharma A, Smith AGC, Avaliani T, Gujabidze M, Bakuradze T, et al. Combined cerebrospinal fluid metabolomic and cytokine profiling in tuberculosis meningitis reveals robust and prolonged changes in immunometabolic networks. medRxiv. (2023) [Preprint]. doi: 10.1101/2023.06.26.23291676
12. Ardiansyah E, Avila-Pacheco J, Nhat LTH, Dian S, Vinh DN, Hai HT, et al. Tryptophan metabolism determines outcome in tuberculous meningitis: a targeted metabolomic analysis. Elife. (2023), 12. doi: 10.7554/eLife.85307
13. Zhang X, Zhao Z, Wu Q, Wang L, Li L, Wang M, et al. Single-cell analysis reveals changes in BCG vaccine-injected mice modeling tuberculous meningitis brain infection. Cell Rep. (2023) 42:112177. doi: 10.1016/j.celrep.2023.112177
14. Zhang X, Pan L, Zhang P, Wang L, Shen Y, Xu P, et al. Single-cell analysis of the miRNA activities in tuberculous meningitis (TBM) model mice injected with the BCG vaccine. Int Immunopharmacol. (2023) 124:110871. doi: 10.1016/j.intimp.2023.110871
15. Salvador GLO, Basso ACN, Barbieri PP, Leitao CA, Teixeira BCA, Neto AC. Central nervous system and spinal cord tuberculosis: Revisiting an important disease. Clin Imaging. (2021) 69:158–68. doi: 10.1016/j.clinimag.2020.07.020
16. Skoura E, Zumla A, Bomanji J. Imaging in tuberculosis. Int J Infect Dis. (2015) 32:87–93. doi: 10.1016/j.ijid.2014.12.007
17. Trivedi R, Saksena S, Gupta RK. Magnetic resonance imaging in central nervous system tuberculosis. Indian J Radiol Imaging. (2009) 19:256–65. doi: 10.4103/0971-3026.57205
18. Kalita J, Prasad S, Maurya PK, Kumar S, Misra UK. MR angiography in tuberculous meningitis. Acta Radiol. (2012) 53:324–9. doi: 10.1258/ar.2012.110712
19. Sharifi G, Mousavinejad SA, Moradian K, Ebrahimzadeh K, Samadian M, Zerehpoosh FB, et al. Pineal region tuberculoma caused by mycobacterium bovis as a complication of bacille calmette-guerin vaccine: case report and review of the literature. World Neurosurg. (2020) 133:416–8. doi: 10.1016/j.wneu.2019.04.008
20. Sharma MC, Arora R, Mahapatra AK, Sarat-Chandra P, Gaikwad SB, Sarkar C. Intrasellar tuberculoma–an enigmatic pituitary infection: a series of 18 cases. Clin Neurol Neurosurg. (2000) 102:72–7. doi: 10.1016/S0303-8467(00)00063-9
21. Thwaites GE, Chau TT, Farrar JJ. Improving the bacteriological diagnosis of tuberculous meningitis. J Clin Microbiol. (2004) 42:378–9. doi: 10.1128/JCM.42.1.378-379.2004
22. Venkataswamy MM, Rafi W, Nagarathna S, Ravi V, Chandramuki A. Comparative evaluation of BACTEC 460TB system and Lowenstein-Jensen medium for the isolation of M. tuberculosis from cerebrospinal fluid samples of tuberculous meningitis patients. Indian J Med Microbiol. (2007) 25:236–40. doi: 10.1016/S0255-0857(21)02112-5
23. Kennedy DH, Fallon RJ. Tuberculous meningitis. JAMA. (1979) 241:264–8. doi: 10.1001/jama.1979.03290290032021
24. Heemskerk AD, Donovan J, Thu DDA, Marais S, Chaidir L, Dung VTM, et al. Improving the microbiological diagnosis of tuberculous meningitis: A prospective, international, multicentre comparison of conventional and modified Ziehl-Neelsen stain, GeneXpert, and culture of cerebrospinal fluid. J Infect. (2018) 77:509–15. doi: 10.1016/j.jinf.2018.09.003
25. Cox JA, Lukande RL, Kalungi S, Van Marck E, Lammens M, Van de Vijver K, et al. Accuracy of lipoarabinomannan and xpert MTB/RIF testing in cerebrospinal fluid to diagnose tuberculous meningitis in an autopsy cohort of HIV-infected adults. J Clin Microbiol. (2015) 53:2667–73. doi: 10.1128/JCM.00624-15
26. Broger T, Sossen B, du Toit E, Kerkhoff AD, Schutz C, Ivanova Reipold E, et al. Novel lipoarabinomannan point-of-care tuberculosis test for people with HIV: a diagnostic accuracy study. Lancet Infect Dis. (2019) 19:852–61. doi: 10.1016/S1473-3099(19)30001-5
27. Luo Y, Xue Y, Guo X, Lin Q, Mao L, Tang G, et al. Diagnostic accuracy of T-SPOT.TB assay for tuberculous meningitis: an updated meta-analysis. Front Neurol. (2020) 11:866. doi: 10.3389/fneur.2020.00866
28. Pormohammad A, Riahi SM, Nasiri MJ, Fallah F, Aghazadeh M, Doustdar F, et al. Diagnostic test accuracy of adenosine deaminase for tuberculous meningitis: A systematic review and meta-analysis. J Infect. (2017) 74:545–54. doi: 10.1016/j.jinf.2017.02.012
29. Thwaites GE, Caws M, Chau TT, Dung NT, Campbell JI, Phu NH, et al. Comparison of conventional bacteriology with nucleic acid amplification (amplified mycobacterium direct test) for diagnosis of tuberculous meningitis before and after inception of antituberculosis chemotherapy. J Clin Microbiol. (2004) 42:996–1002. doi: 10.1128/JCM.42.3.996-1002.2004
30. Pormohammad A, Nasiri MJ, McHugh TD, Riahi SM, Bahr NC. A systematic review and meta-analysis of the diagnostic accuracy of nucleic acid amplification tests for tuberculous meningitis. J Clin Microbiol. (2019) 57:e01113–18. doi: 10.1128/JCM.01113-18
31. Automated Real-Time Nucleic Acid Amplification Technology for Rapid and Simultaneous Detection of Tuberculosis and Rifampicin Resistance: Xpert MTB/RIF Assay for the Diagnosis of Pulmonary and Extrapulmonary TB in Adults and Children: Policy Update. Geneva: WHO Guidelines Approved by the Guidelines Review Committee (2013).
32. Chen YZ, Sun LC, Wen YH, Li ZW, Fan SJ, Tan HK, et al. Pooled analysis of the Xpert MTB/RIF assay for diagnosing tuberculous meningitis. Biosci Rep. (2020) 40:BSR20191312. doi: 10.1042/BSR20191312
33. Patel VB, Theron G, Lenders L, Matinyena B, Connolly C, Singh R, et al. Diagnostic accuracy of quantitative PCR (Xpert MTB/RIF) for tuberculous meningitis in a high burden setting: a prospective study. PloS Med. (2013) 10:e1001536. doi: 10.1371/journal.pmed.1001536
34. Organization WH. WHO meeting report of a technical expert consultation: non-inferiority analysis of Xpert MTB/RIF Ultra compared to Xpert MTB/RIF. World Health Organization (2017). Available at: https://www.who.int/publications/i/item/WHO-HTM-TB-2017.04.
35. Donovan J, Thu DDA, Phu NH, Dung VTM, Quang TP, Nghia HDT, et al. Xpert MTB/RIF Ultra versus Xpert MTB/RIF for the diagnosis of tuberculous meningitis: a prospective, randomised, diagnostic accuracy study. Lancet Infect Dis. (2020) 20:299–307. doi: 10.1016/S1473-3099(19)30649-8
36. Wang G, Wang S, Jiang G, Yang X, Huang M, Huo F, et al. Xpert MTB/RIF Ultra improved the diagnosis of paucibacillary tuberculosis: A prospective cohort study. J Infect. (2019) 78:311–6. doi: 10.1016/j.jinf.2019.02.010
37. Huang M, Wang G, Sun Q, Jiang G, Li W, Ding Z, et al. Diagnostic accuracy of Xpert MTB/RIF Ultra for tuberculous meningitis in a clinical practice setting of China. Diagn Microbiol Infect Dis. (2021) 100:115306. doi: 10.1016/j.diagmicrobio.2020.115306
38. Sun WW, Sun Q, Yan LP, Zhang Q. The application of IS6110-baced loop-mediated isothermal amplification (LAMP) in the early diagnosis of tuberculous meningitis. Oncotarget. (2017) 8:57537–42. doi: 10.18632/oncotarget.15734
39. Wilson MR, Sample HA, Zorn KC, Arevalo S, Yu G, Neuhaus J, et al. Clinical metagenomic sequencing for diagnosis of meningitis and encephalitis. N Engl J Med. (2019) 380:2327–40. doi: 10.1056/NEJMoa1803396
40. Solomons RS, Visser DH, Friedrich SO, Diacon AH, Hoek KG, Marais BJ, et al. Improved diagnosis of childhood tuberculous meningitis using more than one nucleic acid amplification test. Int J Tuberc Lung Dis. (2015) 19:74–80. doi: 10.5588/ijtld.14.0394
41. Kataria J, Rukmangadachar LA, Hariprasad G, O J, Tripathi M, Srinivasan A. Two dimensional difference gel electrophoresis analysis of cerebrospinal fluid in tuberculous meningitis patients. J Proteomics. (2011) 74:2194–203. doi: 10.1016/j.jprot.2011.06.020
42. Ou Q, Liu X, Cheng X. An iTRAQ approach to quantitative proteome analysis of cerebrospinal fluid from patients with tuberculous meningitis. Biosci Trends. (2013) 7:186–92. doi: 10.5582/bst.2013.v7.4.186
43. Mu J, Yang Y, Chen J, Cheng K, Li Q, Wei Y, et al. Elevated host lipid metabolism revealed by iTRAQ-based quantitative proteomic analysis of cerebrospinal fluid of tuberculous meningitis patients. Biochem Biophys Res Commun. (2015) 466:689–95. doi: 10.1016/j.bbrc.2015.08.036
44. Li Z, Du B, Li J, Zhang J, Zheng X, Jia H, et al. Cerebrospinal fluid metabolomic profiling in tuberculous and viral meningitis: Screening potential markers for differential diagnosis. Clin Chim Acta. (2017) 466:38–45. doi: 10.1016/j.cca.2017.01.002
45. van Laarhoven A, Dian S, Aguirre-Gamboa R, Avila-Pacheco J, Ricano-Ponce I, Ruesen C, et al. Cerebral tryptophan metabolism and outcome of tuberculous meningitis: an observational cohort study. Lancet Infect Dis. (2018) 18:526–35. doi: 10.1016/S1473-3099(18)30053-7
46. Pan D, Pan M, Xu YM. Mir-29a expressions in peripheral blood mononuclear cell and cerebrospinal fluid: Diagnostic value in patients with pediatric tuberculous meningitis. Brain Res Bull. (2017) 130:231–5. doi: 10.1016/j.brainresbull.2017.01.013
47. Pan L, Liu F, Zhang J, Li J, Jia H, Huang M, et al. Genome-Wide miRNA analysis identifies potential biomarkers in distinguishing tuberculous and viral meningitis. Front Cell Infect Microbiol. (2019) 9:323. doi: 10.3389/fcimb.2019.00323
48. Miao Q, Ma Y, Wang Q, Pan J, Zhang Y, Jin W, et al. Microbiological diagnostic performance of metagenomic next-generation sequencing when applied to clinical practice. Clin Infect Dis. (2018) 67:S231–40. doi: 10.1093/cid/ciy693
49. Yu G, Zhao W, Shen Y, Zhu P, Zheng H. Metagenomic next generation sequencing for the diagnosis of tuberculosis meningitis: A systematic review and meta-analysis. PloS One. (2020) 15:e0243161. doi: 10.1371/journal.pone.0243161
50. Ramachandran PS, Wilson MR. Metagenomics for neurological infections - expanding our imagination. Nat Rev Neurol. (2020) 16:547–56. doi: 10.1038/s41582-020-0374-y
51. Zhu Y, Zhao W, Yang X, Zhang Y, Lin X, Weng X, et al. Metagenomic next-generation sequencing for identification of central nervous system pathogens in HIV-infected patients. Front Microbiol. (2022) 13:1055996. doi: 10.3389/fmicb.2022.1055996
52. Chen J, Zhang R, Liu L, Qi T, Wang Z, Song W, et al. Clinical usefulness of metagenomic next-generation sequencing for the diagnosis of central nervous system infection in people living with HIV. Int J Infect Dis. (2021) 107:139–44. doi: 10.1016/j.ijid.2021.04.057
53. Ji XC, Zhou LF, Li CY, Shi YJ, Wu ML, Zhang Y, et al. Reduction of human DNA contamination in clinical cerebrospinal fluid specimens improves the sensitivity of metagenomic next-generation sequencing. J Mol Neurosci. (2020) 70:659–66. doi: 10.1007/s12031-019-01472-z
54. Chen Y, Wang Y, Liu X, Li W, Fu H, Liu X, et al. Comparative diagnostic utility of metagenomic next-generation sequencing, GeneXpert, modified Ziehl-Neelsen staining, and culture using cerebrospinal fluid for tuberculous meningitis: A multi-center, retrospective study in China. J Clin Lab Anal. (2022) 36:e24307. doi: 10.1002/jcla.24307
55. Xing XW, Zhang JT, Ma YB, He MW, Yao GE, Wang W, et al. Metagenomic next-Generation sequencing for diagnosis of infectious encephalitis and meningitis: A large, prospective case series of 213 patients. Front Cell Infect Microbiol. (2020) 10:88. doi: 10.3389/fcimb.2020.00088
56. Colman RE, Anderson J, Lemmer D, Lehmkuhl E, Georghiou SB, Heaton H, et al. Rapid drug susceptibility testing of drug-Resistant mycobacterium tuberculosis isolates directly from clinical samples by use of amplicon sequencing: a proof-of-Concept study. J Clin Microbiol. (2016) 54:2058–67. doi: 10.1128/JCM.00535-16
57. de Araujo L, Cabibbe AM, Mhuulu L, Ruswa N, Dreyer V, Diergaardt A, et al. Implementation of targeted next-generation sequencing for the diagnosis of drug-resistant tuberculosis in low-resource settings: a programmatic model, challenges, and initial outcomes. Front Public Health. (2023) 11:1204064. doi: 10.3389/fpubh.2023.1204064
58. Dai Y, Sheng K, Hu L. Diagnostic efficacy of targeted high-throughput sequencing for lower respiratory infection in preterm infants. Am J Transl Res. (2022) 14:8204–14.
59. Kambli P, Ajbani K, Kazi M, Sadani M, Naik S, Shetty A, et al. Targeted next generation sequencing directly from sputum for comprehensive genetic information on drug resistant Mycobacterium tuberculosis. Tuberculosis (Edinb). (2021) 127:102051. doi: 10.1016/j.tube.2021.102051
60. Organization WH. Use of targeted next-generation sequencing to detect drug-resistant tuberculosis: rapid communication, July 2023. World Health Organization (2023). Available at: https://www.who.int/news/item/25-07-2023-who-issues-rapid-communication-on-use-of-targeted-next-generation-sequencing-for-diagnosis-of-drug-resistant-tuberculosis.
61. vLi J, Zhang L, Yang X, Wang P, Feng L, Guo E, et al. Diagnostic significance of targeted next-generation sequencing in central nervous system infections in neurosurgery of pediatrics. Infect Drug Resist. (2023) 16:2227–36. doi: 10.2147/IDR.S404277
62. Huang LL, Wang C, Liu Y, Gu XY, Wang WX, Chen W, et al. Resolution of an insidious and migratory Mycobacterium tuberculosis-associated secondary organizing pneumonia: a case report and literature review. BMC Infect Dis. (2023) 23:372. doi: 10.1186/s12879-023-08334-5
63. Mitchell SL, Simner PJ. Next-generation sequencing in clinical microbiology: are we there yet? Clin Lab Med. (2019) 39:405–18. doi: 10.1016/j.cll.2019.05.003
64. Zhu L, Zhong J, Jia X, Liu G, Kang Y, Dong M, et al. Precision methylome characterization of Mycobacterium tuberculosis complex (MTBC) using PacBio single-molecule real-time (SMRT) technology. Nucleic Acids Res. (2016) 44:730–43. doi: 10.1093/nar/gkv1498
65. Phelan J, de Sessions PF, Tientcheu L, Perdigao J, MaChado D, Hasan R, et al. Methylation in Mycobacterium tuberculosis is lineage specific with associated mutations present globally. Sci Rep. (2018) 8:160. doi: 10.1038/s41598-017-18188-y
66. Chen L, Li H, Chen T, Yu L, Guo H, Chen Y, et al. Genome-wide DNA methylation and transcriptome changes in Mycobacterium tuberculosis with rifampicin and isoniazid resistance. Int J Clin Exp Pathol. (2018) 11:3036–45.
67. Gong Z, Wang G, Zeng J, Stojkoska A, Huang H, Xie J. Differential DNA methylomes of clinical MDR, XDR and XXDR Mycobacterium tuberculosis isolates revealed by using single-molecule real-time sequencing. J Drug Target. (2021) 29:69–77. doi: 10.1080/1061186X.2020.1797049
68. Ndhlovu V, Kiran A, Sloan DJ, Mandala W, Nliwasa M, Everett DB, et al. Characterization of DNA methylation in Malawian Mycobacterium tuberculosis clinical isolates. PeerJ. (2020) 8:e10432. doi: 10.7717/peerj.10432
69. Tafess K, Ng TTL, Lao HY, Leung KSS, Tam KKG, Rajwani R, et al. Targeted-Sequencing workflows for comprehensive drug resistance profiling of mycobacterium tuberculosis cultures using two commercial sequencing platforms: comparison of analytical and diagnostic performance, turnaround time, and cost. Clin Chem. (2020) 66:809–20. doi: 10.1093/clinchem/hvaa092
70. Zhao K, Tu C, Chen W, Liang H, Zhang W, Wang Y, et al. Rapid identification of drug-resistant tuberculosis genes using direct PCR amplification and oxford nanopore technology sequencing. Can J Infect Dis Med Microbiol. (2022) 2022:7588033. doi: 10.1155/2022/7588033
71. Gliddon HD, Frampton D, Munsamy V, Heaney J, Pataillot-Meakin T, Nastouli E, et al. A rapid drug resistance genotyping workflow for mycobacterium tuberculosis, using targeted isothermal amplification and nanopore sequencing. Microbiol Spectr. (2021) 9:e0061021. doi: 10.1128/Spectrum.00610-21
72. Chan WS, Au CH, Chung Y, Leung HCM, Ho DN, Wong EYL, et al. Rapid and economical drug resistance profiling with Nanopore MinION for clinical specimens with low bacillary burden of Mycobacterium tuberculosis. BMC Res Notes. (2020) 13:444. doi: 10.1186/s13104-020-05287-9
73. Yu MC, Hung CS, Huang CK, Wang CH, Liang YC, Lin JC. Differential Impact of the rpoB Mutant on Rifampin and Rifabutin Resistance Signatures of Mycobacterium tuberculosis Is Revealed Using a Whole-Genome Sequencing Assay. Microbiol Spectr. (2022) 10:e0075422. doi: 10.1128/spectrum.00754-22
74. Gomez-Gonzalez PJ, Campino S, Phelan JE, Clark TG. Portable sequencing of Mycobacterium tuberculosis for clinical and epidemiological applications. Brief Bioinform. (2022) 23:bbac256. doi: 10.1093/bib/bbac256
75. Smith C, Halse TA, Shea J, Modestil H, Fowler RC, Musser KA, et al. Assessing nanopore sequencing for clinical diagnostics: a comparison of next-generation sequencing (NGS) methods for mycobacterium tuberculosis. J Clin Microbiol. (2020) 59:e00583–20. doi: 10.1128/JCM.00583-20
76. Li X, Du W, Wang Y, Liu Z, Li K, Chen H, et al. Rapid diagnosis of tuberculosis meningitis by detecting mycobacterium tuberculosis cell-Free DNA in cerebrospinal fluid. Am J Clin Pathol. (2020) 153:126–30. doi: 10.1093/ajcp/aqz135
77. Shao L, Qiu C, Zheng L, Yang Y, Yang X, Liang Q, et al. Comparison of diagnostic accuracy of the GeneXpert Ultra and cell-free nucleic acid assay for tuberculous meningitis: A multicentre prospective study. Int J Infect Dis. (2020) 98:441–6. doi: 10.1016/j.ijid.2020.06.076
78. Li Z, Pan L, Lyu L, Li J, Jia H, Du B, et al. Diagnostic accuracy of droplet digital PCR analysis of cerebrospinal fluid for tuberculous meningitis in adult patients. Clin Microbiol Infect. (2020) 26:213–9. doi: 10.1016/j.cmi.2019.07.015
79. Ai JW, Zhou X, Xu T, Yang M, Chen Y, He GQ, et al. CRISPR-based rapid and ultra-sensitive diagnostic test for Mycobacterium tuberculosis. Emerg Microbes Infect. (2019) 8:1361–9. doi: 10.1080/22221751.2019.1664939
80. Namuganga AR, Chegou NN, Mayanja-Kizza H. Past and present approaches to diagnosis of active pulmonary tuberculosis. Front Med (Lausanne). (2021) 8:709793. doi: 10.3389/fmed.2021.709793
81. Preez ID, Luies L, Loots DT. Metabolomics biomarkers for tuberculosis diagnostics: current status and future objectives. biomark Med. (2017) 11:179–94. doi: 10.2217/bmm-2016-0287
82. Tornheim JA, Dooley K. Tuberculosis associated with HIV infection. Microbiol Spectr. (2017) 5:1128. doi: 10.1128/microbiolspec.tnmi1127-0028-2016
83. Madadi AK, Sohn M-JJP. Comprehensive therapeutic approaches to tuberculous meningitis: pharmacokinetics, combined dosing, and advanced intrathecal therapies. Pharmaceutics. (2024) 16:540. doi: 10.3390/pharmaceutics16040540
84. Marais S, Cresswell FV, Hamers RL, Te Brake LHM, Ganiem AR, Imran D, et al. High dose oral rifampicin to improve survival from adult tuberculous meningitis: A randomised placebo-controlled double-blinded phase III trial (the HARVEST study). Wellcome Open Res. (2019) 4:190. doi: 10.12688/wellcomeopenres
85. Wasserman S, Davis A, Wilkinson RJ, Meintjes G. Key considerations in the pharmacotherapy of tuberculous meningitis. Expert Opin Pharmacother. (2019) 20:1791–5. doi: 10.1080/14656566.2019.1638912
86. Organization WH. WHO consolidated guidelines on drug-resistant tuberculosis treatment. World Health Organization (2019). Available at: https://www.who.int/publications/i/item/9789241550529.
87. Tucker EW, Guglieri-Lopez B, Ordonez AA, Ritchie B, Klunk MH, Sharma R, et al. Noninvasive (11)C-rifampin positron emission tomography reveals drug biodistribution in tuberculous meningitis. Sci Transl Med. (2018) 10:eaau0965. doi: 10.1126/scitranslmed.aau0965
88. Svensson RJ, Aarnoutse RE, Diacon AH, Dawson R, Gillespie SH, Boeree MJ, et al. A population pharmacokinetic model incorporating saturable pharmacokinetics and autoinduction for high rifampicin doses. Clin Pharmacol Ther. (2018) 103:674–83. doi: 10.1002/cpt.v103.4
89. Ding J, Thuy Thuong Thuong N, Pham TV, Heemskerk D, Pouplin T, Tran CTH, et al. Pharmacokinetics and pharmacodynamics of intensive antituberculosis treatment of tuberculous meningitis. Clin Pharmacol Ther. (2020) 107:1023–33. doi: 10.1002/cpt.v107.4
90. Lee C, Bhakta S. The prospect of repurposing immunomodulatory drugs for adjunctive chemotherapy against tuberculosis: A critical review. Antibiotics (Basel). (2021)10:91. doi: 10.3390/antibiotics10010091
91. Davis AG, Donovan J, Bremer M, Van Toorn R, Schoeman J, Dadabhoy A, et al. Host directed therapies for tuberculous meningitis. Wellcome Open Res. (2020) 5:292. doi: 10.12688/wellcomeopenres
92. WHO consolidated guidelines on tuberculosis: Module 4: Treatment - Drug-resistant tuberculosis treatment. Geneva: WHO Guidelines Approved by the Guidelines Review Committee (2020).
93. WHO consolidated guidelines on drug-resistant tuberculosis treatment. Geneva: WHO Guidelines Approved by the Guidelines Review Committee (2019).
94. Basu Roy R, Seddon JA. Linezolid for children with tuberculous meningitis: more evidence required. Pediatr Infect Dis J. (2017) 36:439. doi: 10.1097/INF.0000000000001464
95. Sun F, Ruan Q, Wang J, Chen S, Jin J, Shao L, et al. Linezolid manifests a rapid and dramatic therapeutic effect for patients with life-threatening tuberculous meningitis. Antimicrob Agents Chemother. (2014) 58:6297–301. doi: 10.1128/AAC.02784-14
96. Li H, Lu J, Liu J, Zhao Y, Ni X, Zhao S. Linezolid is associated with improved early outcomes of childhood tuberculous meningitis. Pediatr Infect Dis J. (2016) 35:607–10. doi: 10.1097/INF.0000000000001114
97. van Well GT, Paes BF, Terwee CB, Springer P, Roord JJ, Donald PR, et al. Twenty years of pediatric tuberculous meningitis: a retrospective cohort study in the western cape of South Africa. Pediatrics. (2009) 123:e1–8. doi: 10.1542/peds.2008-1353
98. Padmapriyadarsini C, Vohra V, Bhatnagar A, Solanki R, Sridhar R, Anande L, et al. Bedaquiline, delamanid, linezolid and clofazimine for treatment of pre-extensively drug-Resistant tuberculosis. Clin Infect Dis. (2022) 76:e938–946. doi: 10.1093/cid/ciac528
99. Rohilla R, Shafiq N, Malhotra S. Efficacy and safety of aspirin as an adjunctive therapy in tubercular meningitis: A systematic review and meta-analysis. EClinicalMedicine. (2021) 34:100819. doi: 10.1016/j.eclinm.2021.100819
100. Murthy JMK. Tuberculous meningitis - adjunctive therapy: corticosteroids, aspirin, or both. Neurol India. (2019) 67:1003–5. doi: 10.4103/0028-3886.266280
101. Misra UK, Kalita J, Kumar M. Safety and efficacy of fludrocortisone in the treatment of cerebral salt wasting in patients with tuberculous meningitis: A randomized clinical trial. JAMA Neurol. (2018) 75:1383–91. doi: 10.1001/jamaneurol.2018.2178
102. Kumar R, Kolloli A, Singh P, Vinnard C, Kaplan G, Subbian S. Thalidomide and phosphodiesterase 4 inhibitors as host directed therapeutics for tuberculous meningitis: insights from the rabbit model. Front Cell Infect Microbiol. (2019) 9:450. doi: 10.3389/fcimb.2019.00450
103. Suarez I, Gruell H, Heyckendorf J, Funger S, Lichtenstein T, Jung N, et al. Intensified adjunctive corticosteroid therapy for CNS tuberculomas. Infection. (2020) 48:289–93. doi: 10.1007/s15010-019-01378-3
104. Liu P, Pei N, Liu X, Huang W, Lu S. Thalidomide in the treatment of human immunodeficiency virus-negative tuberculous meningitis: A case report. Med (Baltimore). (2020) 99:e22639. doi: 10.1097/MD.0000000000022639
105. Arshad A, Dayal S, Gadhe R, Mawley A, Shin K, Tellez D, et al. Analysis of tuberculosis meningitis pathogenesis, diagnosis, and treatment. J Clin Med. (2020)9:2962. doi: 10.3390/jcm9092962
106. Stadelman AM, Ellis J, Samuels THA, Mutengesa E, Dobbin J, Ssebambulidde K, et al. Treatment outcomes in adult tuberculous meningitis: A systematic review and meta-analysis. Open Forum Infect Dis. (2020) 7:ofaa257. doi: 10.1093/ofid/ofaa257
107. Misra UK, Kalita J, Nair PP. Role of aspirin in tuberculous meningitis: a randomized open label placebo controlled trial. J Neurol Sci. (2010) 293:12–7. doi: 10.1016/j.jns.2010.03.025
108. Schoeman JF, Janse van Rensburg A, Laubscher JA, Springer P. The role of aspirin in childhood tuberculous meningitis. J Child Neurol. (2011) 26:956–62. doi: 10.1177/0883073811398132
109. Mai NTH, Dobbs N, Phu NH, Colas RA, Thao LTP, Thuong NTT, et al. A randomised double blind placebo controlled phase 2 trial of adjunctive aspirin for tuberculous meningitis in HIV-uninfected adults. Elife. (2018) 12:e87888. doi: 10.7554/eLife.33478
110. Yadav R. Role of aspirin as an adjuvant therapy in tuberculous meningitis in adults: The time has come for a phase III randomized controlled trial. Neurol India. (2018) 66:1678–9. doi: 10.4103/0028-3886.246225
111. Rizvi I, Garg RK, Malhotra HS, Kumar N, Uniyal R. Role of aspirin in tuberculous meningitis: A systematic review and meta-analysis. Neurol India. (2019) 67:993–1002. doi: 10.4103/0028-3886.266232
112. Murthy JM. Management of intracranial pressure in tuberculous meningitis. Neurocrit Care. (2005) 2:306–12. doi: 10.1385/NCC:2:3:306
113. Loan JJM, Poon MTC, Tominey S, Mankahla N, Meintjes G, Fieggen AG. Ventriculoperitoneal shunt insertion in human immunodeficiency virus infected adults: a systematic review and meta-analysis. BMC Neurol. (2020) 20:141. doi: 10.1186/s12883-020-01713-4
114. Kamat AS, Gretschel A, Vlok AJ, Solomons R. CSF protein concentration associated with ventriculoperitoneal shunt obstruction in tuberculous meningitis. Int J Tuberc Lung Dis. (2018) 22:788–92. doi: 10.5588/ijtld.17.0008
Keywords: tuberculous meningitis, high-throughput, omics, sequencing, diagnosis, treatment
Citation: Lin F (2025) Tuberculous meningitis diagnosis and treatment: classic approaches and high-throughput pathways. Front. Immunol. 15:1543009. doi: 10.3389/fimmu.2024.1543009
Received: 11 December 2024; Accepted: 24 December 2024;
Published: 10 January 2025.
Edited by:
Dan Liu, Wuhan University, ChinaReviewed by:
Zhijia Xia, Affiliated Hospital of Guilin Medical University, ChinaCopyright © 2025 Lin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Fangbo Lin, YXNwbGluQDEyNi5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.